
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 11 August 2022
Sec. Computational Psychiatry
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.883294
This article is part of the Research TopicWomen in Psychiatry 2022: Computational PsychiatryView all 6 articles
 Kristina Todorovic1
Kristina Todorovic1 Erin O’Leary2
Erin O’Leary2 Kaitlin P. Ward3Pratyush P. Devarasetty4
Kaitlin P. Ward3Pratyush P. Devarasetty4 Shawna J. Lee3Michele Knox2
Shawna J. Lee3Michele Knox2 Elissar Andari2*
Elissar Andari2*Background: We are facing an ongoing pandemic of coronavirus disease 2019 (COVID-19), which is causing detrimental effects on mental health, including disturbing consequences on child maltreatment and intimate partner violence.
Methods: We sought to identify predictors of child maltreatment and intimate partner violence from 380 participants (mean age 36.67 ± 10.61, 63.2% male; Time 3: June 2020) using modern machine learning analysis (random forest and SHAP values). We predicted that COVID-related factors (such as days in lockdown), parents’ psychological distress during the pandemic (anxiety, depression), their personality traits, and their intimate partner relationship will be key contributors to child maltreatment. We also examined if there is an increase in family violence during the pandemic by using an additional cohort at two time points (Time 1: March 2020, N = 434; mean age 35.67 ± 9.85, 41.69% male; and Time 2: April 2020, N = 515; mean age 35.3 ± 9.5, 34.33%).
Results: Feature importance analysis revealed that parents’ affective empathy, psychological well-being, outdoor activities with children as well as a reduction in physical fights between partners are strong predictors of a reduced risk of child maltreatment. We also found a significant increase in physical punishment (Time 3: 66.26%) toward children, as well as in physical (Time 3: 36.24%) and verbal fights (Time 3: 41.08%) among partners between different times.
Conclusion: Using modernized predictive algorithms, we present a spectrum of features that can have influential weight on prediction of child maltreatment. Increasing awareness about family violence consequences and promoting parenting programs centered around mental health are imperative.
COVID-19 is an infectious disease that is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and is primarily spread via social interactions and face-to-face exchanges. Prior to the COVID-19 pandemic, family violence was a major public health issue, with 678,000 children as victims of maltreatment in 2018 and one in every four females and one in every nine males as victims of intimate partner violence (IPV) (1). Given this profound prevalence and the current pandemic, the risk of child maltreatment and IPV may be at an elevated risk.
Several factors, such as economic hardship, uncertainty for the future, fear of getting infected, working from home, homeschooling, less support from other caregivers, and social isolation can lead to an increased level of stress and have a negative impact on mental health (2). The COVID-19 pandemic has been associated with psychological difficulties such as depression and anxiety (3–5). Depression and anxiety are associated with an increased risk of child maltreatment and neglect (6). In addition to psychological difficulties, the isolation caused by the pandemic, associated shelter-at-home directives, and school and service closures significantly inhibit our society’s abilities to identify and report family violence. The lack or very limited contact between children and many professionals during the pandemic provides significantly less opportunity for child maltreatment identification and reporting. Parents are having significantly more time with children and less respite and support from other, typical caregivers such as childcare workers, causing increased stress on parents. Many parents are experiencing frustration when trying to work from home while caring for children, managing children’s behaviors, and maintaining work privacy. Children and teens themselves are also more stressed due to worries about the virus, as well as needed adaptations and changes to education. These factors are likely to significantly increase negative parent-child interactions. This, coupled with higher parent stress, may significantly increase the risk of corporal punishment, abuse, and neglect. This is in keeping with evidence from previous pandemics that found parents facing health challenges were more likely to have harsher discipline strategies (7). Also, more recent work has shown that job loss during the COVID-19 pandemic has been found to be a significant risk factor for child maltreatment (8) and IPV (9). Some alarming numbers of child maltreatment during the COVID-19 pandemic have been reported with sixty-one percent of parents using verbal aggression and 1 in 5 parents using physical punishment as their discipline method (3). Therefore, psychological distress can negatively impact parenting practices and may increase the risk of negative parent-child interactions, corporal punishment, neglect, and IPV (10). Protective factors are also important to consider when addressing family violence. Parental empathy involves the ability to understand children’s feelings and intentions, as well as being able to provide comfort and show sensitivity and flexibility to children’s needs. Research has demonstrated poor parental empathy is associated with physical abuse potential and likelihood to punish (11).
The present study investigates mental health consequences of the pandemic, with an emphasis on indicators of child maltreatment and IPV. Specifically, we examined whether the pandemic has a significant impact on verbal aggression and physical punishment toward children and on violence between partners. We first adopted state-of-the-art machine learning approaches to determine the relative contribution of independent factors related to the pandemic among other factors related to mental health and personality traits of parents, to predict verbal aggression and physical punishment toward children, and IPV at Time 3. We used random forest analysis to capture non-linear decision boundaries and nuanced interactions amongst features. We expect COVID-19 related items will be predictive of increased violence, and psychological well-being and emotional empathy will be strong predictors of lower incidence of family violence. Second, we aim to study the potential increase in family violence during the pandemic by comparing participants’ reports of child maltreatment and IPV between different time points of the pandemic, (Time 1: March 2020, Time 2: April 2020, and Time 3: June 2020). We predict that there will be an increase of verbal aggression and physical punishment toward children and IPV over time.
For Time 1, a total of 434 parents or/and participants in a relationship (mean age 35.67 ± 9.85, 41.69% male); and For Time 2, a total of 515 parents or/and participants in a relationship (mean age 35.3 ± 9.5, 34.33% male) were included in the analysis. These participants were recruited via online surveys that were administered through Prolific. Time 1 was collected in March 2020 and Time 2 was collected in April 2020. Participants were United States citizens and were age 18 or older. On average for both times, 74.33% were Caucasian, 9.37% were African American, 8.52% were Hispanic, 3.3% were Asian/Native Hawaiian/Other Pacific Islander, 3.19% were biracial, 0.85% were other and 0.43% were American Indian/Alaskan Native. 37.72% were male participants, 44.28% are from the South state region, 20% from the Midwest, 20% from the West, and 15.72% from Northeast. The distribution of income ranged between $10,000 and more than $90,000. For education level, 25.85% had some college, 35.80% had bachelor’s degree, 10.91% had high school, 10.8% had an associate degree and 15.68% had a Master’s, professional, doctorate, and 0.95% no high school. See Table 1.
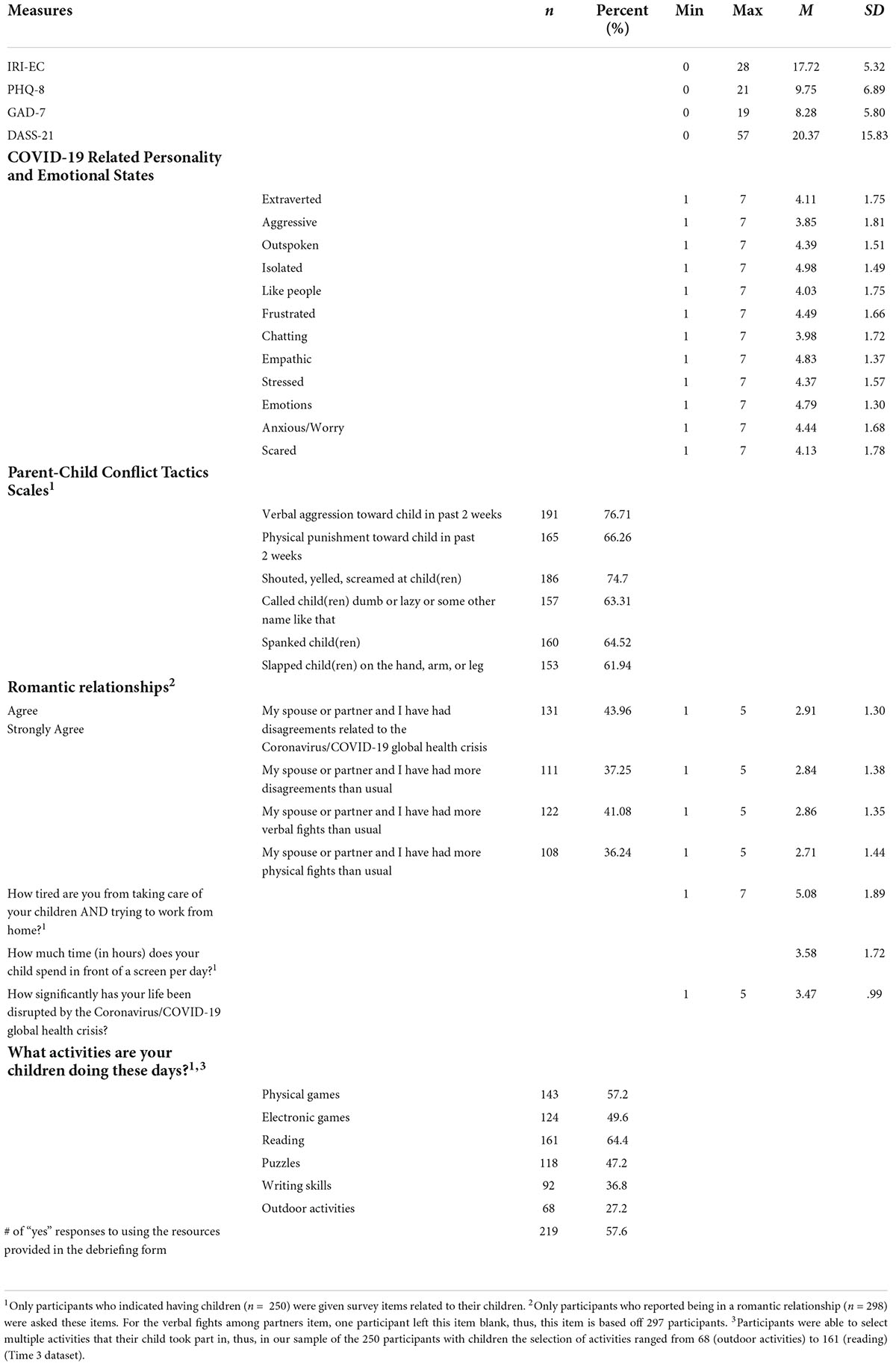
Table 1. Descriptive statistics of measures in the present study.
A total of 380 adults from 43 states in the United States were recruited from Amazon’s Mechanical Turk (Mturk) from June 5, 2020 to June 14, 2020 (Time 3). Mturk is a crowdsourcing website that allows researchers to conduct research including participant recruitment, data collection, and compensating participants. Mturk has been shown to obtain high-quality data from participants and includes a demographically diverse sample (12). The inclusion criteria for the present study included (1) United States resident, (2) at least 95% approval rating as an MTurk worker (e.g., workers with a high completion and quality rating), (3) valid responses on questionnaire. Participants (36.3% female, 63.2% male, 0.3% prefer not to answer) ranged in age from 20 to 73 (M = 36.67, SD = 10.61).
Most participants identified as White/Caucasian (78.7%), followed by Black/African American/African Diaspora (12.1%), Asian/Native Hawaiian/Other Pacific Islander (6.3%), American Indian/Alaskan Native (1.3%), and Other/Prefer not to answer (1.6%). More than half of participants reported living in an urban neighborhood (53.2%), followed by suburban (28.4%) and rural (18.4%). 78.4% of participants reported being in a romantic relationship and 65.8% of participants reported having 1 to 6 children. Our sample represented all regions of the United States: 13.4% Northeast, 16.3% Midwest, 39.2% South, and 30.5% West.
We also collected additional demographics between May 24, 2021 to May 27, 2021 from 106 of the original participants from Time 3. Among parents or/and participants in a relationship (n = 68), around 32.35% have an income that ranges between $40–$50k, 33.82% have an income that ranges between $50–$70k, 13.24% have an income that ranges between $30–$40k, 8.82% that ranges between $70–$90k, and 8.82% that ranges between $20–30k. 60.29% have a bachelor’s degree, 20.59% have some college, 11.76% have a master’s, professional, doctorate, and 4.41% have an associate degree, and 2.94% are in high school.
The average completion time for Time 1 was 33 min and 32 min for Time 2. For Time 2, they were recontacted via the Prolific website. Data from these time points was provided as anonymous therefore, the data was deemed exempt from the first authors university’s Institutional Review Board.
All procedures received approval from the first authors university’s Institutional Review Board. Participants completed a 1-hour survey exploring people’s social and emotional experiences during the COVID-19 pandemic. To ensure that participants provided valid responses on the questionnaires we included 10 explicit request attention check items (e.g., If you are still paying attention, please select “once”). On the consent form, participants were informed that we placed attention check questions throughout the survey and participants had to answer these questions correctly to receive compensation. Participants had to respond correctly to the 10 attention check questions to be included in our sample. Data were collected in blocks of 10 participants then examined by the first author. Participants whose data were believed to be invalid were removed from the study (n = 20 of 400 participants).
Items from the Parent–Child Conflict Tactics Scales were used to assess risk for verbal aggression and physical aggression toward children at all time-points (13). We modified the response scale to ask participants how often behaviors occurred “in the past two weeks” on a 0 (“never”) to 6 (“every day”) scale. We computed dichotomous variables for verbal aggression and physical aggression to indicate no verbal aggression/physical aggression or one or more instances of verbal aggression/physical aggression in the past two weeks. Verbal aggression was measured with two items (i.e., “Shouted, yelled, or screamed at child(ren)” and “Called child(ren) dumb or lazy or some other name like that”). Physical aggression was measured with two items (i.e., “Spanked child(ren)” and “Slapped child(ren) on the hand, arm, or leg”). Internal consistency was excellent (Time 3 α = 0.94).
Information about intimate partner relationships was measured with 6-items about their relationships in the past 2 weeks at all time-points (3). For each item, participants choose one response ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). Sample items include, “My spouse or partner and I have had more verbal fights than usual,” and “My spouse or partner and I have had more physical fights than usual”).
Several questions were asked that are related to the following domains: (1) Empathic concern (Interpersonal Reactivity Index, IRI) (14). At Time 3, empathy was measured with the IRI which is a 28-item scale measuring perspective taking, fantasy, empathic concern, and personal distress. Participants in the present study were only given seven items from the empathic concern subscale. All items were rated on a 0 (“does not describe me well”) to 4 (“describes me very well”) scale. Items were reversed scored as needed. Internal consistency was acceptable (Time 3 α = 0.74); (2) Psychological distress over the last two weeks (depression evaluated with the 8-item Patient Health Questionnaire (PHQ-8); (15), anxiety evaluated with the Generalized Anxiety Disorder Assessment (GAD-7); (16), and 21-items Depression Anxiety Stress Scale (DASS-21); (17) to ensure intra-individual consistency for depression and anxiety) For all time points, severity of depressive symptoms was measured with the 8-item PHQ-8. The PHQ-8 asked participants “Over the last two weeks, how often have you been bothered by any of the following problems?” Participants rated each statement on a 4-point scale ranging from 0 (“not at all”) to 3 (“nearly every day”). A sum of the 8-items was created for data analyses in the present study. Internal consistency in the present sample was excellent (Time 3 α = 0.93). For all time points, anxiety was measured with the Generalized Anxiety Disorder Assessment (GAD-7). The GAD-7 is a 7-item scale assessing severity of generalized anxiety disorder. Participants are asked to rate the severity of symptoms over the past two weeks on a 4-point scale ranging from 0 (“not at all”) to 3 (“nearly every day”). Internal consistency was excellent in the present sample (Time 3 α = 0.91). In addition to separate measure of depression and anxiety, we also included the 21-item Depression Anxiety Stress Scales at Time 3 and 4 (DASS-21) to ensure intra-individual consistency in terms of feelings of depression and anxiety. Participants were given a series of statements and asked to rate each item on a 4-point scale ranging from 0 (“did not apply to me at all”) to 3 (“applied to me most of the time”) to indicate how much the statement applied to them over the past week. Internal consistency was excellent (Time 3 α = 0.97); (3) COVID-19 related daily life (such as days in lockdown, social distancing, life disruption); (4) COVID-19 related childcare (tired of taking care and homeschooling); (5) COVID-19 related personality and emotional states (aggressivity, extraversion, stress, frustration, anxiety, scared, empathy experienced during the COVID-19 pandemic). At Time 3, COVID-19 related personality and emotional states items were coded on a 7-point scale ranging from 1 (“not at all”) to 7 (“extremely”). These items measured participants COVID-19 related experiences via a 17-item measure developed for this study. Participants were asked about their personality and emotional state during the COVID-19 pandemic. The COVID-19 related personality and emotional states questions consisted different questions related to different constructs that are the following: extraversion (“How extraverted [outgoing, sociable] would you rate yourself now?”), aggression (“How aggressive would you rate yourself during the COVID-19 pandemic?”), and empathy (“How empathic would you rate yourself during the COVID-19 pandemic?”), frustrated (“How frustrated would you rate yourself during the COVID-19 pandemic?”), stressed (“How stressed would you rate yourself now?”), anxious/worry (“How often do you feel anxious or worried now?”), and scared (“How often do you feel scared now?”); (6) Children’s activities (such as activities outdoor, writing skills, screen time, reading, puzzles, electronic games), (7) Need for help (interested in requesting help) (8) Intimate partner relationship (COVID-19-related disagreements, disagreements in general, physical fights, and verbal fights since the start of the pandemic), and (9) Number of children.
Models were constructed to predict the probability or classify instances of verbal aggression or physical punishment occurring. As such, we considered three models, an unregularized logistic regression, a regularized multiple logistic regression model, and a random forest model. There were several different types of covariates: continuous, nominal, and ordinal. Nominal variables were dummy-coded, dropping the first value. Ordinal variables were coded by centering at 0, and then performing unit steps in appropriate directions (i.e., –1, 0, 1). Missing data was handled with simple imputation.
The unregularized logistic regression model was constructed to test for each covariate’s individual contribution, while controlling for age, gender, race, income, education, and state region. Next, we considered a regularized logistic regression model that utilized an elastic-net penalty, using scikit-learn to fit this model (18). Finally, we considered a random forest model, again using scikit-learn (19). Random forests are an ensemble supervised learning method non-linear classifier that have been trained on different subsets of the data, often perform extremely well at the cost of model interpretability. While random forests do offer insight into their model by ranking feature importance, we chose instead to use shapley additive explanations (SHAP) values. SHAP values have the advantage of guaranteeing local explanations are consistent and locally accurate, and that the global explanations are built off a series of local explanations.
Final metrics were obtained by using nested cross-validation. Nested cross-validation has been shown to be a robust technique to assess model performance and generalization (20). Instead of using K-fold Cross-Validation which produces biased performance estimates with small sample sizes, we used nested cross- validation and train approaches that can provide unbiased performance estimates regardless of sample size.
When comparing the differences between three time points (Time 1, Time 2, and Time 3), we conducted a logistic regression for the binary-response variables (physical punishment and verbal aggression toward children). In the model, age, race, gender, state region, education, income, and interaction between gender and time were included. We were interested in studying differences in gender with respect to family violence. Time was ordinally encoded. These logistic regressions models were unregularized, which allowed us to generate p-values and confidence intervals (CI) that correspond to the coefficients of the features. We also conducted ordinal regressions on the Likert-scale dependent variables of intimate partner relationships (physical and verbal fights). Same factors above were included in this model.
In aim 1, to determine predictors of family violence, we used dataset of Time 3 which was our main dataset that included many independent factors. In aim 2, to determine family violence prevalence increase, we used datasets of Times 1, 2, and 3 with a focus on dependent factors and demographic information.
Final metrics were obtained by using nested cross-validation. Nested cross-validation has been shown to be a robust technique to assess model performance and generalization. Instead of using K-fold Cross-Validation which produces biased performance estimates with small sample sizes, we used nested cross-validation and train approaches that can provide unbiased performance estimates regardless of sample size.
Briefly, (e.g.) 10-fold cross-validation involves splitting a dataset into 10 equally sized folds. Each fold is treated as a validation once, while the rest of the data is then used for training or hyper-parameter optimization, i.e., the first 10% of the data is withheld, while the remaining 90% of the data is used to train, then the next 10% of the data is withheld, and again, the remaining 90% of the data is used for training. This process continues with each fold being used as a validation set once.
In Nested cross-validation, an additional layer of separation between model performance metrics and hyper-parameter estimation is introduced. Like in (e.g.) 10-fold cross-validation, the dataset is split into 10 equally sized folds. However, instead of immediately using the remaining 9-folds for training, that dataset is further split into another (e.g.) 10-folds. Using these 10 newly created folds (that were generated from the 90% of the data being used for training) regular cross validation is performed, i.e., one (inner) fold is left out for validation, while a model is training on the remaining nine (inner) folds. This process is repeated until all (inner) folds have been used for validation. Once that process has been completed, the resulting model is then validation against the (outer) 10% of the data that has been withheld for validation. In this manner, the model is validated on against a dataset that is has never seen before. This process is repeated once for each of the (e.g.) 10 folds, resulting in a final validation metric. This nested cross-validation approach has been studied, proving to be a nearly unbiased estimate of model performance, while the regular CV approach is shown to be biased.
At Time 3, 76.4% reported one or more instances of verbal aggression toward children, 66% reported one or more instance of physical punishment toward children, 41.08% reported agreeing or strongly agreeing that they had more verbal fights with their partner than usual, and 36.24% reported agreeing or strongly agreeing that they had more physical fights with their partner than usual.
We modeled 32 variables as potential predictors and conducted an unregularized logistic regression to predict verbal aggression toward children while adjusting for age, gender, and state region. The odds ratios (OR) and 99.84% CI for each predictor are shown (Figure 1A; Table 2). Significant results were mainly observed for the intimate partner relationship category (physical fights, verbal fights, COVID-related disagreements, disagreements); for the psychological distress category (GAD-7, DASS-21, PHQ-8); for the empathic concern category (IRI_EC, empathy); for the COVID-19 related personality and emotional states category (aggressivity, extraversion, stress, frustration, anxiety, scared); for the children’s activities category (outdoor activities, physical games, electronic, writing skills); for the COVID-19 related childcare category (tired from childcare, homeschooling); and for need for help category.
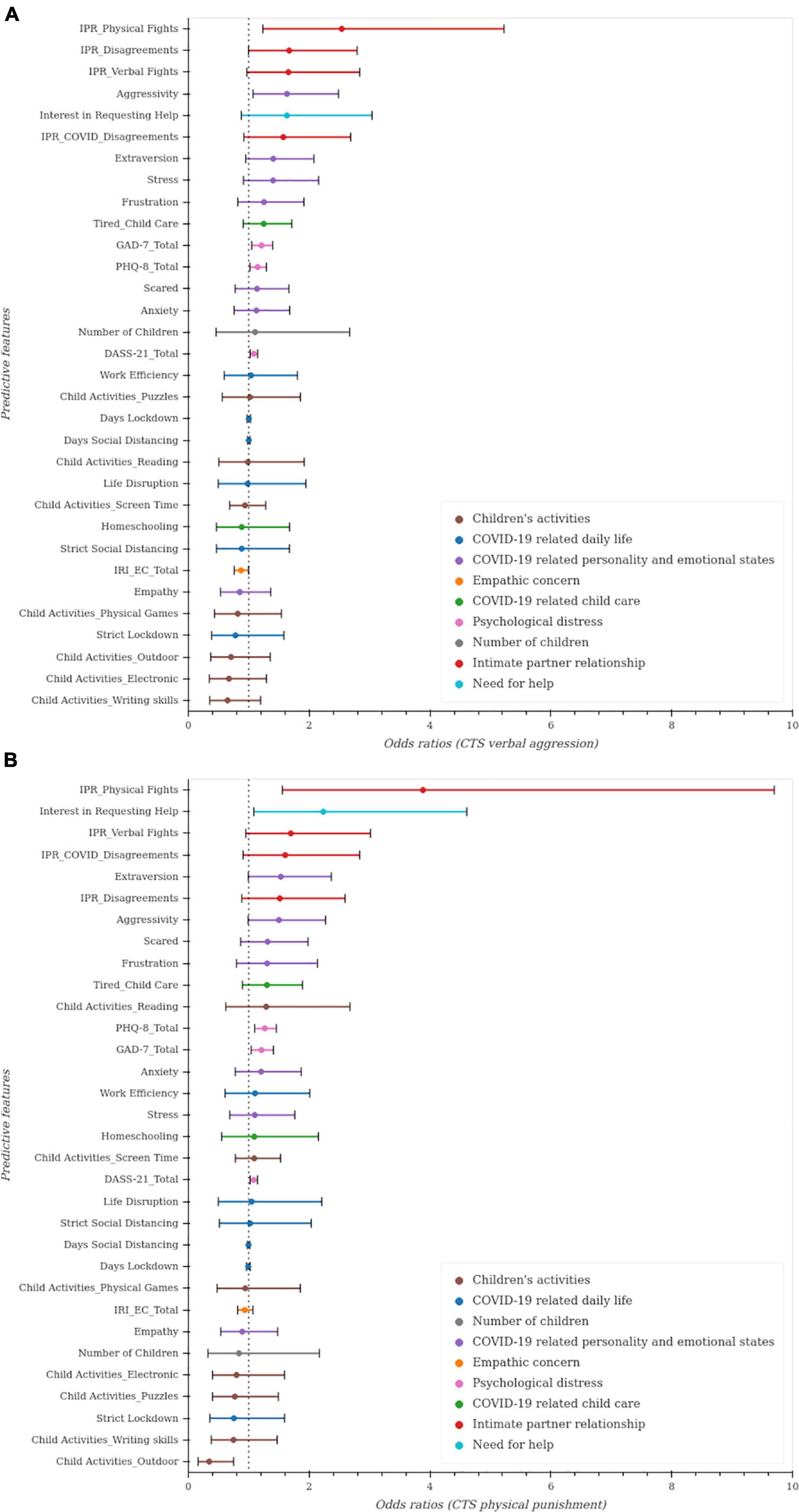
Figure 1. Unregularized regressions to predict indicators of child maltreatment. Unregularized logistic regression was used with 32 predictive factors after adjusting for age, gender and state region. Odds ratios and 99.84% confidence intervals (CI) for each predictor. The OR point estimates are represented by the dots and the line widths for each predictor present the 1- 0.05/32% = 99.84% CI adjusted for multiple comparisons using Bonferroni (as the gold standard method for multiple comparisons). Statistical significance is indicated by CI not including 1 at the 0.05/32 level. (A). Predictors of verbal aggression toward children. (B). Predictors of physical punishment toward children.
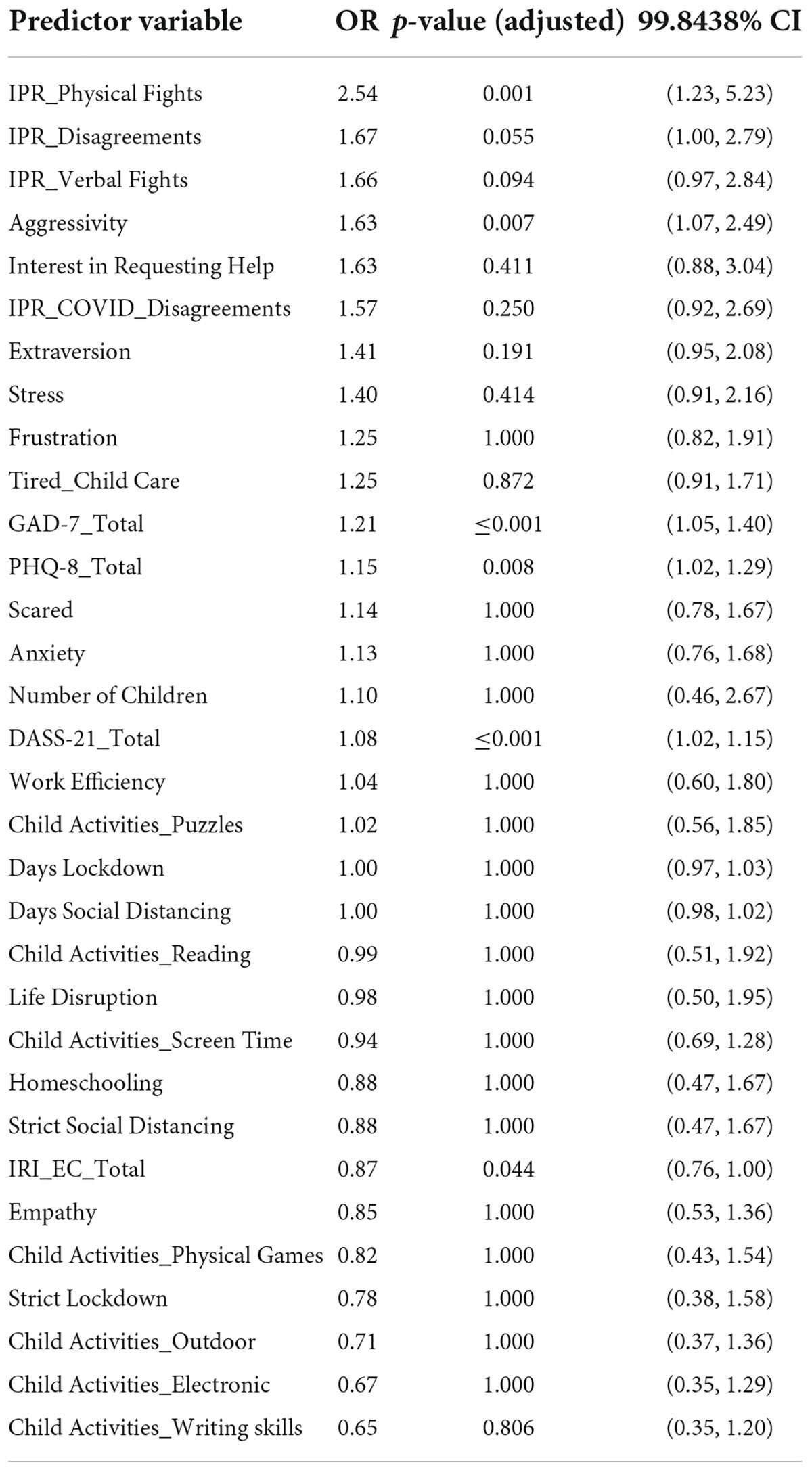
Table 2. (Time 3): Predictors of verbal aggression toward children in the unregularized regression model.
We used similar methods to predict physical punishment (Figure 1B; Table 3). The greatest risk of physical punishment was associated with more physical fights, verbal fights, COVID-related disagreements, and disagreements between partners. Greater risk of physical punishment toward children was also associated with higher levels of anxiety and depression (PHQ-8, DASS-21, GAD-7), and with less empathic concern (IRI). COVID-19-related items to childcare (tired taking care of children), and to personality and emotional states (extraversion, aggressivity, frustration, scared, anxiety and stress) were also significant predictors. Children’s involvement in outdoor activities predicted less risk of physical punishment toward children.
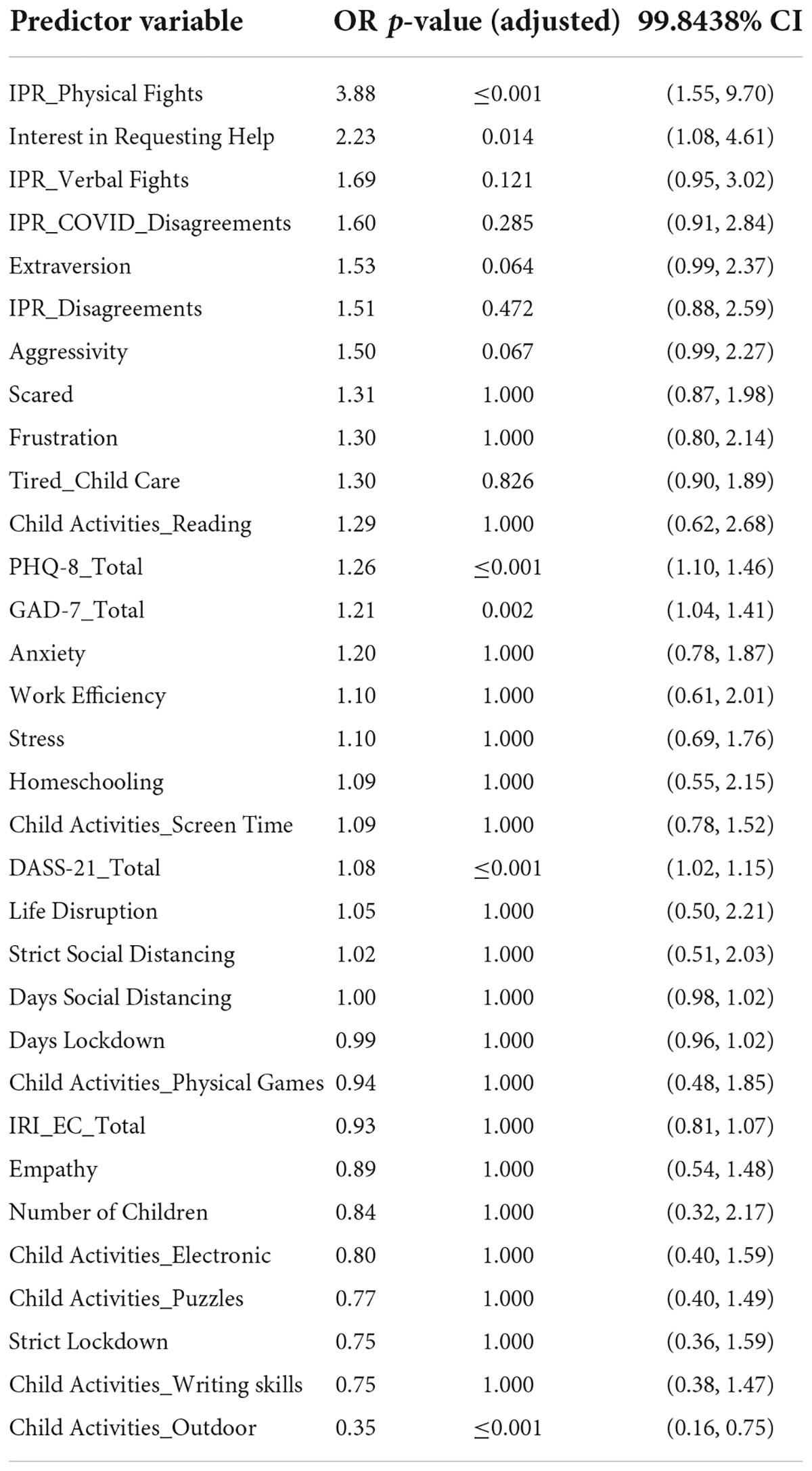
Table 3. (Time 3): Predictors of physical punishment toward children in the unregularized regression model.
We then estimated verbal aggression and physical punishment toward children using regularized logistic with elastic-net penalty, which allows us to account for many features while controlling for overfitting. For verbal aggression, we found empathic concern and DASS-21 scores best predicted verbal aggression (Figure 2). For physical punishment, we found that physical fights among partners, spending time outdoor, empathic concern and psychological distress are among the best predictive in the model (Figure 3). AUROC for cross validation was 0.88 ± 0.09 and 0.94 ± 0.05 with hyperparameters: C = 0.02, l1_ratio = 0.99 and C = 0.20, l1_ratio = 0.99, respectively.
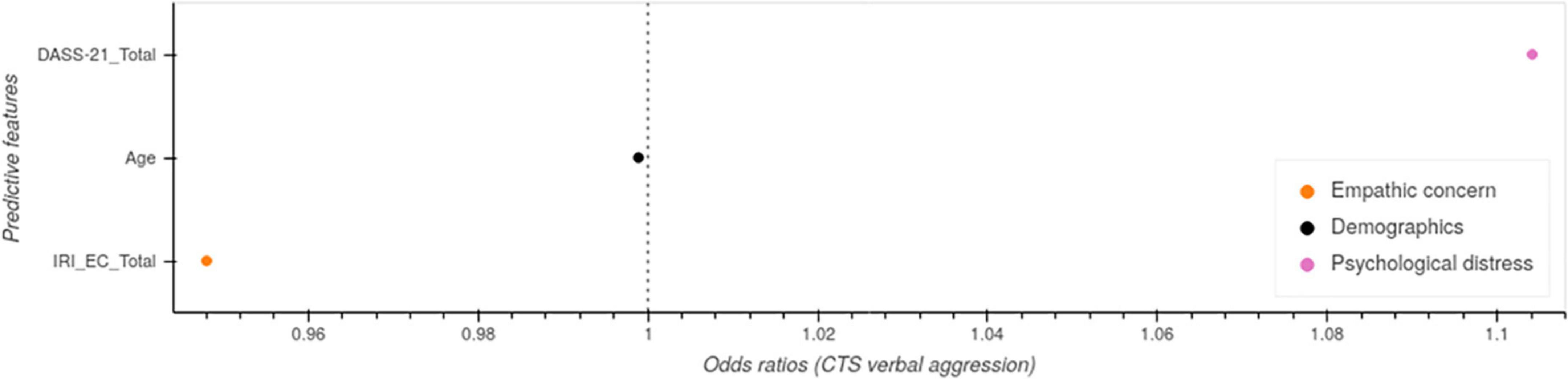
Figure 2. Regularized regression model predicting verbal aggression toward children (Time 3).
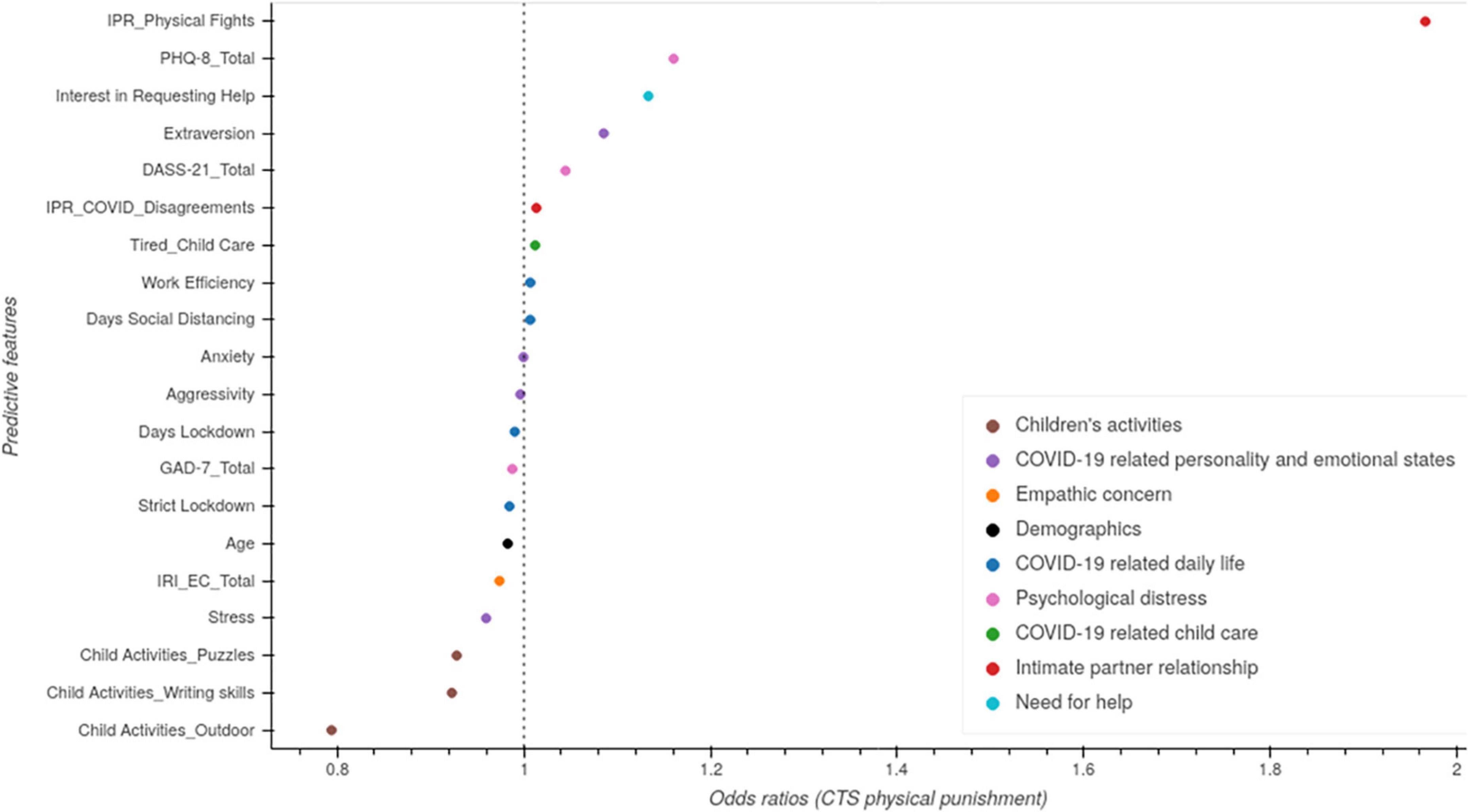
Figure 3. Regularized regression model predicting physical punishment toward children (Time 3).
We then utilized a random forest classification model to determine if there were additional factors identified. For verbal aggression and physical punishment, empathic concern, psychological distress and physical fights among partners were the leading predictor of verbal aggression toward children (Figures 4A,B). Verbal fights among partners, COVID-related disagreements, extraverted personalities, and outdoor activities with children were among important factors that were associated with this physical punishment. The AUROC for the random forest was 0.91 ± 0.06 and 0.93 ± 0.06, with hyperparameters max_features = 0.36 and 0.22 and n_estimators = 211 and 446, respectively.
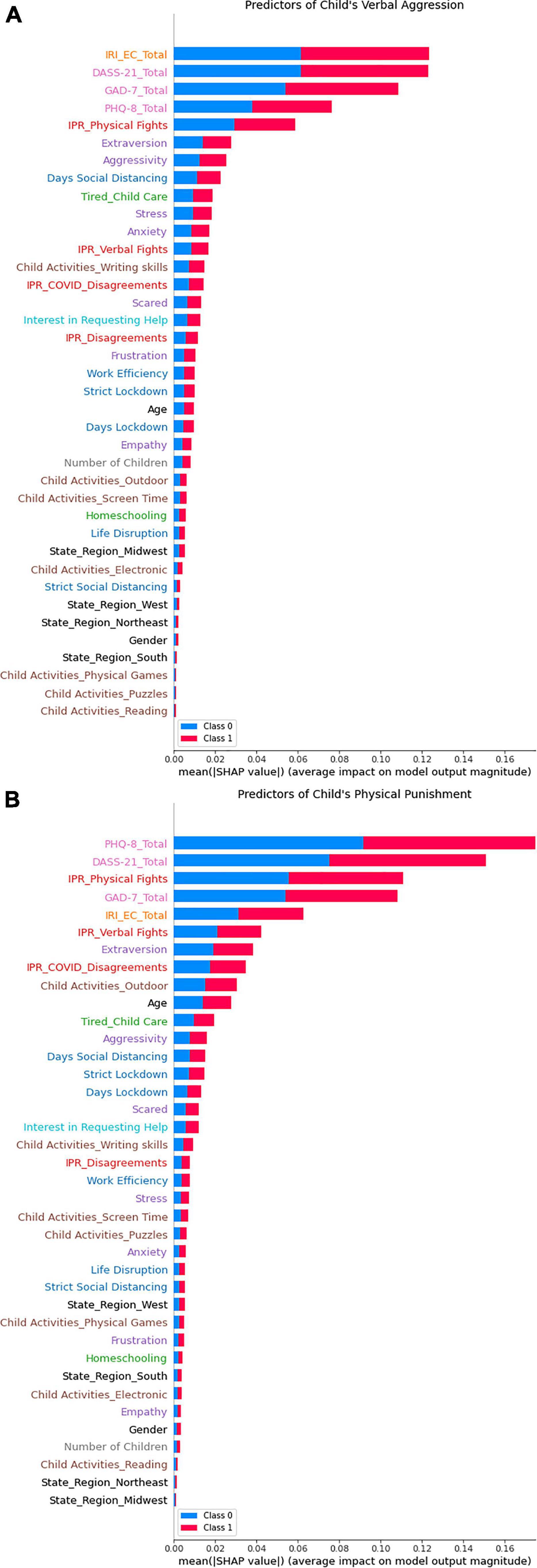
Figure 4. Random forest analysis to predict indicators of child maltreatment. Random forest was conducted with shapely additive explanations (SHAP) values. (A) Predictors of verbal aggression toward children. (B) Predictors of physical punishment toward children.
Unregularized regressions showed that COVID-19 related personality and emotional factors, psychological distress, and empathic concern are among the most predictors of verbal and physical fights (Figures 5A,B). Regularized regressions confirmed these results.
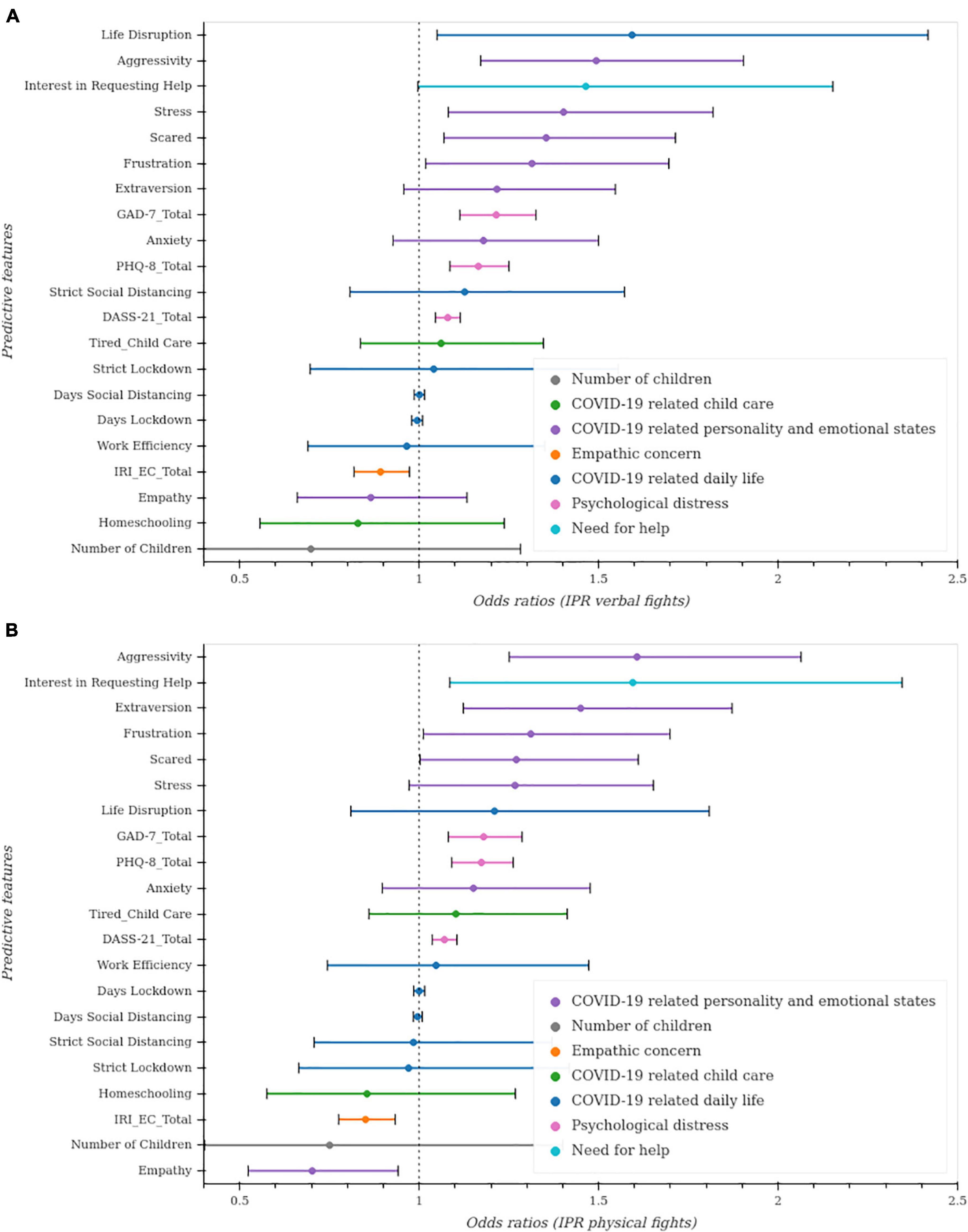
Figure 5. Unregularized regressions to predict intimate partner violence. Unregularized ordinal regressions were conducted. For each covariate of interest, an ordinal regression model was fit while controlling for age, gender, and state region. The p-values and CI for each model were then adjusted for multiple comparisons using the Bonferroni method. (A) Predictive factors of verbal fights between partners. (B) Predictive factors of physical fights between partners.
We conducted both unregularized and regularized ordinal regression models to estimate verbal fights among partners (see Table 4). The unregularized model results demonstrate COVID-19 related personality and emotional factors (Figure 5A) (aggressivity, stressed, scared, frustration, extraversion), and interest in seeking help are among the most significant predictors of verbal fights among partners. Psychological distress (GAD-7, DASS-21, PHQ-8), and empathic concern (IRI_EC) are among the significant factors predicting an increase and a decrease in these verbal fights, respectively.
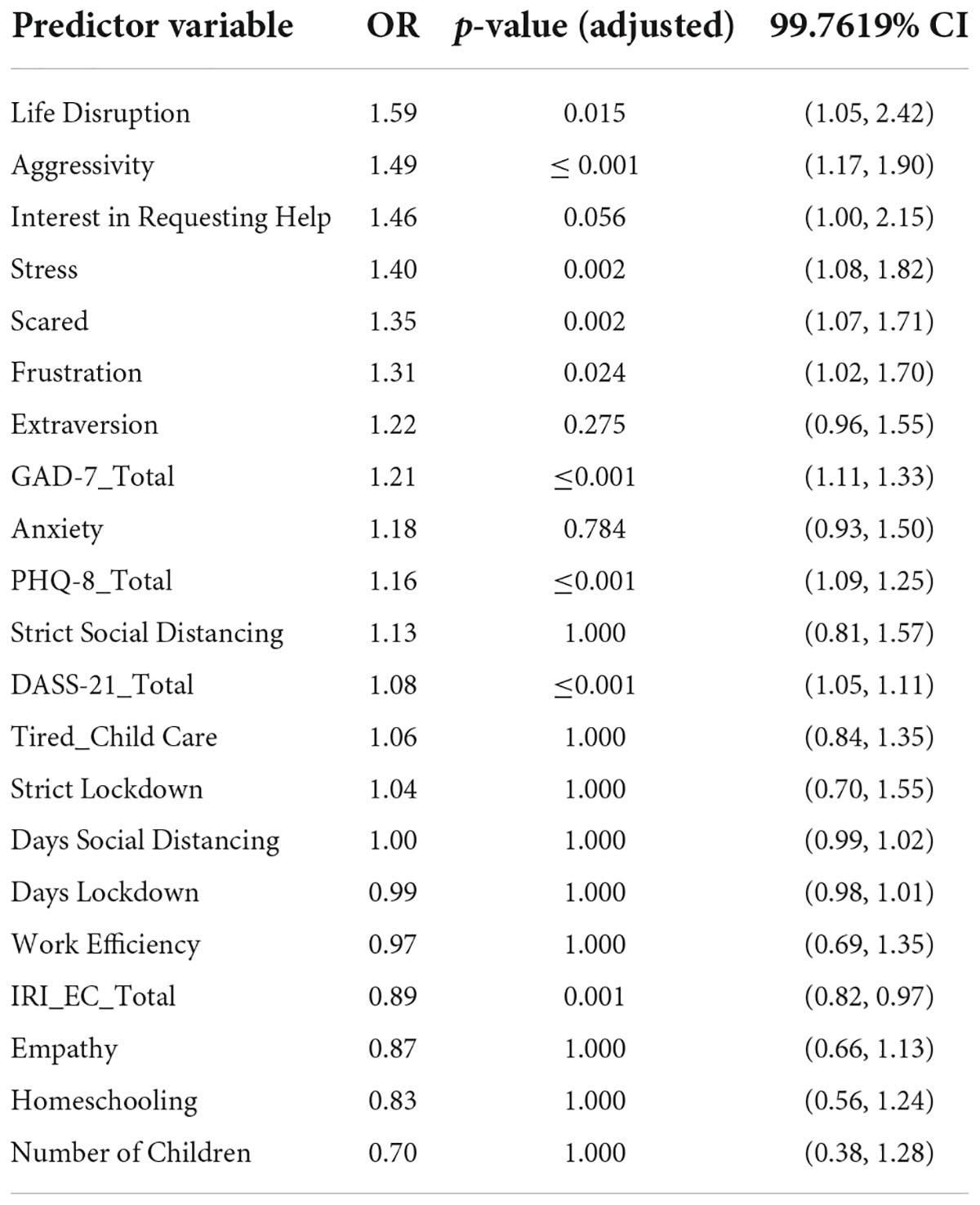
Table 4. (Time 3): Predictors of verbal fights between partners in the unregularized regression model.
The regularized model used an ℓ2 penalty, the mean absolute error (MAE) 0.67=0.11 with a hyperparameter of α= 599.48. Note that this corresponds to the unit encoding of the Likert-scale response. The regularized model identified the same factors as predicting verbal fights (see Figure 6A).
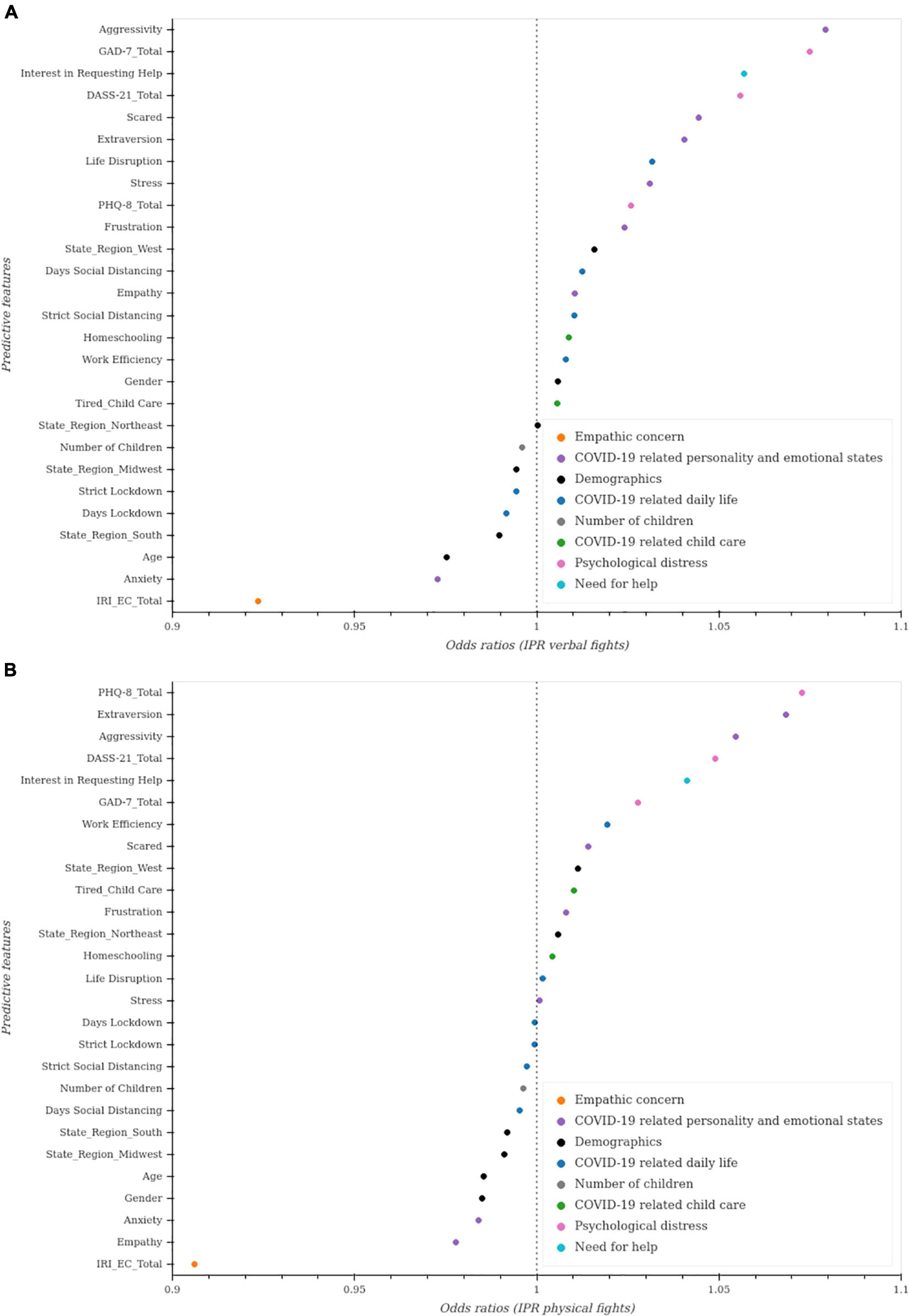
Figure 6. Regularized regression model predicting intimate partner verbal fights (Time 3) (A) and intimate partner physical fights (Time 3) (B).
We examined what factors were associated with increased physical fights among partners by conducting an ordinal regression (see Table 5). Of the factors included in the unregularized model (Figure 5B), the following were associated with increased physical fights among partners: interest in requesting help, COVID-19 related personality and emotional states (aggression, stress), anxious/worry, extraverted, frustrated, scared as well as psychological distress (GAD-7, DASS-21, PHQ-8). Empathic concern (IRI_EC) is predictive of less physical fights between partners. The MAE for the regularized model was 0.670.11 with a hyperparameter of α = 1204.50. Regularized regressions confirm the previous results (see Figure 6B).
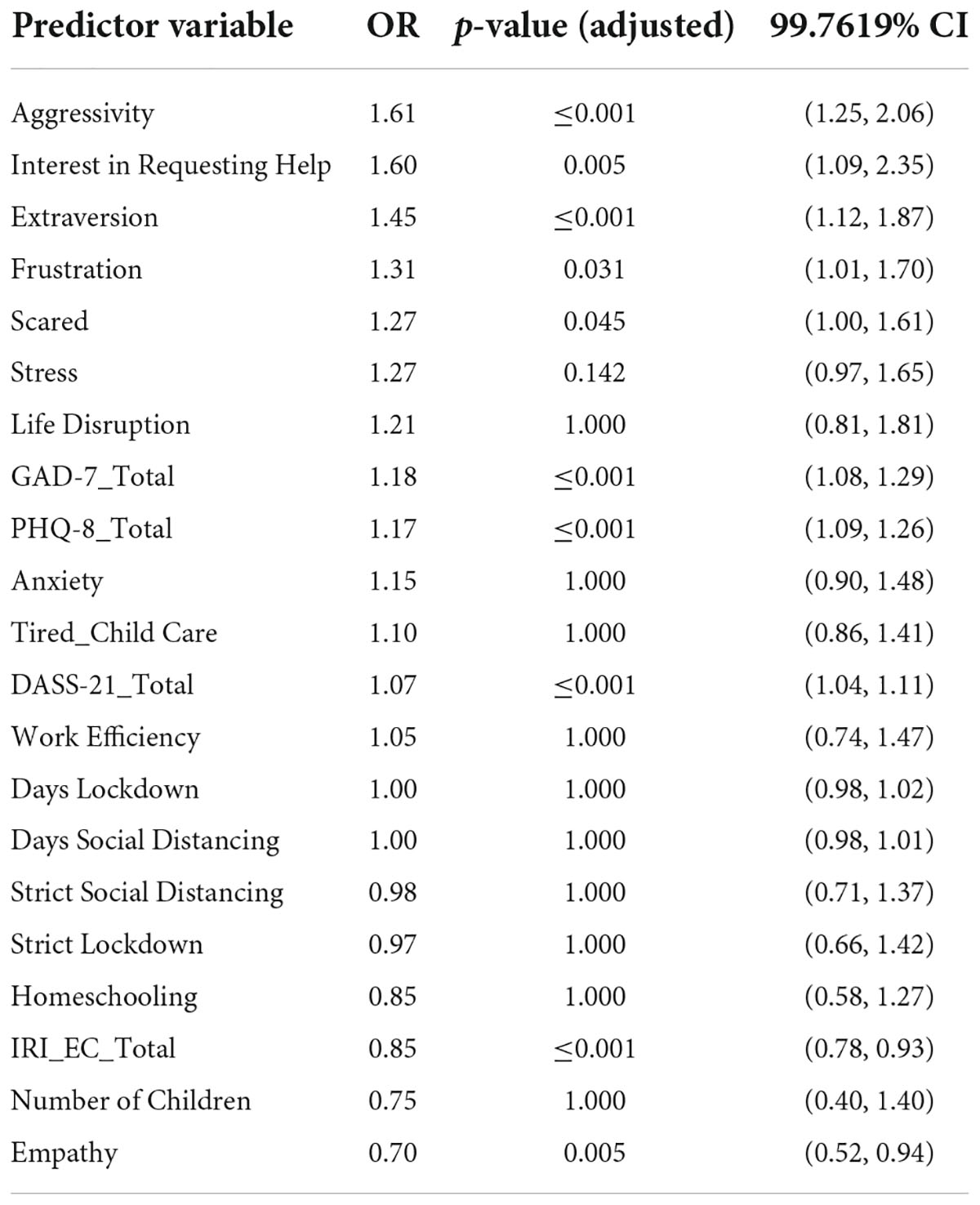
Table 5. (Time 3): Predictors of physical fights between partners in the unregularized regression model.
At Times 1 and 2 on average, 58.63% reported one or more instances of verbal aggression toward children, 22.39% reported one or more instance of physical punishment toward children, 21.46% reported agreeing or strongly agreeing that they had more verbal fights with their partner than usual, and 1.32% reported agreeing or strongly agreeing that they had more physical fights with their partner than usual (more information about each time point in Table 6). We conducted logistic regression for verbal and physical punishment toward children and found a significant increase for physical punishment between Times 1, 2, and 3. There is an increased risk for physical punishment that was associated with time (OR = 4.32; CI = 2.65, 7.02). While there was no effect of time for verbal aggression, there was a significant interaction between male gender and time, signifying an increased risk for verbal aggression over time only in males (OR = 2.4, 2; CI = 1.24, 3.95). Ordinal regressions also revealed a significant increase risk of verbal and physical fights between partners (OR = 2.19, CI = 1.6, 2.99; OR = 5.71, CI = 3.86, 8.45, respectively).
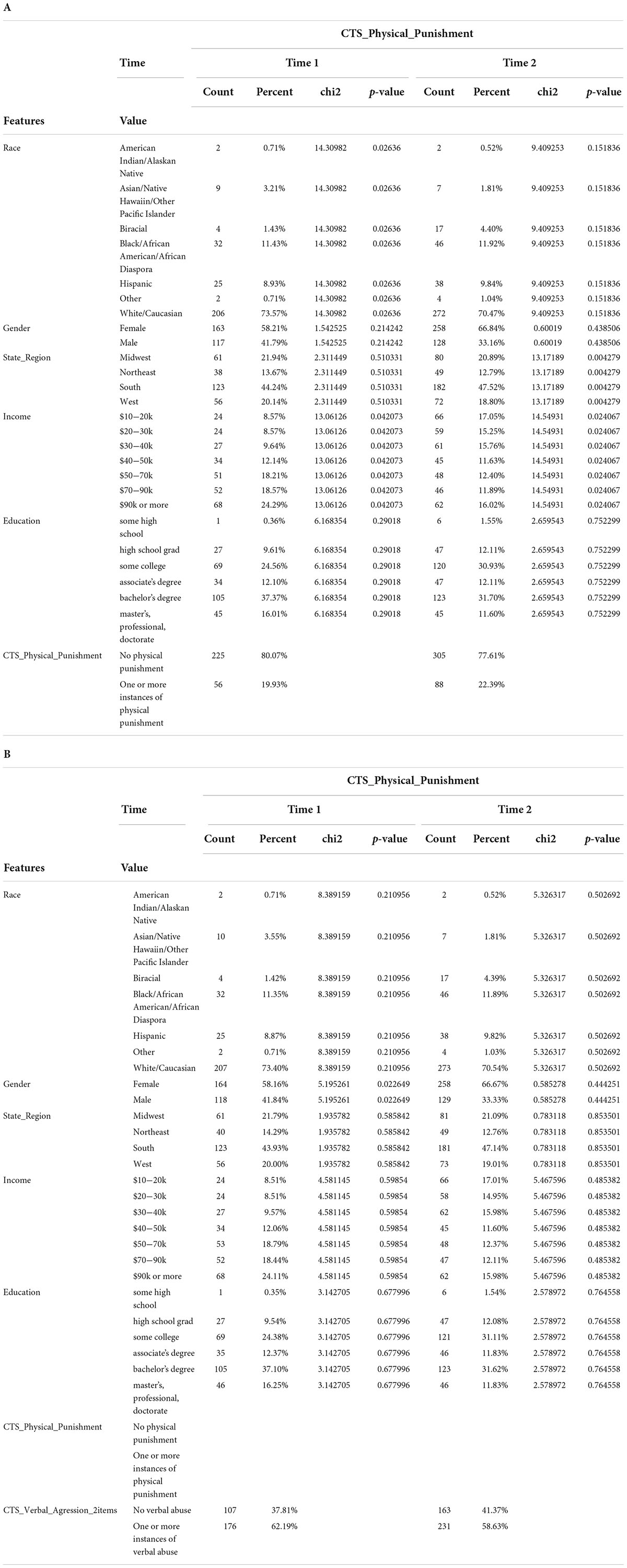
Table 6. Descriptive data for Times 1 and 2.
Logistic regression showed that there is a significant increased risk of physical punishment for certain states [West (OR = 2.81, CI = 1.62, 4.88), South (OR = 2.23, CI = 1.36, 3.68), and Northeast (OR = 2.14, CI = 1.13, 4.04)] as compared to Midwest. Also, larger incomes were associated with less risk of physical punishment (OR = 0.33, CI = 0.17, 0.63). In terms of physical fights between partners, there was a significant increase of risk in the West as compared to Midwest (OR = 2.66, CI = 1.71, 4.14). There was also an increased risk for male reporting on physical fights as compared to females (OR = 1.68, CI = 1.25, 2.27). For physical punishment, verbal aggression toward children and physical fights between partners, there was a significant effect of time (OR = 2.32, CI = 1.55, 3.47; OR = 1.49, CI = 1.06, 2.1; OR = 2.78, CI = 1.96, 3.94), which means that there was a lager increase between Time 3 and Time 2 than Time 2 compared to Time 1.
We used machine learning analysis to assess the strongest predictors of indicators of child maltreatment and intimate partner violence. We found empathic concern and depression and anxiety symptoms were among the strongest predictors of verbal aggression toward children. Physical fights among parents as well as specific traits and behaviors (such as being extraverted and aggressive) were also among the important factors identified in the machine learning model. However, for physical punishment toward children, a greater number of factors related to parents’ relationship such as physical fights, verbal fights, and COVID-19 related disagreements were strongly associated with this form of maltreatment. Indicators of anxiety, depression, lower empathy, and extraversion were among the strongest predictors of increased physical punishment toward children. Finally, children’s outdoor activities were among the strongest predictors of less physical punishment.
Interestingly, for both verbal aggression and physical punishment, parental psychological distress and children’s activities factors were ranked as significantly more important than elements related to strict social distancing or lockdown. However, several other factors that are directly related to the pandemic, such as parents’ disagreements related to COVID-19, being tired from taking care of children during COVID-19, and emotional states during the pandemic are significant contributors to child maltreatment. Research demonstrates past pandemics have had a negative impact on psychological well-being and mental health. During the 2003 SARS outbreak, a 31.2% increase in depression and 28.9% increase in anxiety (21). Recent studies have found increased psychological difficulties during the crisis (22). Psychological difficulties in caregivers are associated with increased risk for child maltreatment (23). Our findings corroborate these studies and show that increased anxiety and depression in parents are correlated with greater risk for child maltreatment. When considered together, results of this study illustrate a concerning picture of increased parental distress relates to increased aggression toward children. Parents’ psychological distress was an even more important predictor than the number of days during lockdown. Therefore, providing support to parents may prevent maltreatment.
Additionally, since lack of empathy is considered one of the roots of aggression (24), empathy training has been used in parenting intervention programs for child maltreatment (25). Abusive fathers were less affectively and cognitively empathic toward their children (26). Other studies found less parental affective but not cognitive empathy was associated with higher risk of child physical abuse (27). The current study suggests empathic concern as well as emotion regulation and non-conflictual relationships between parents may be critical objectives in efforts to prevent child maltreatment.
Our findings demonstrate physical fights among partners and symptoms of depression were the leading predictors of physical punishment and verbal aggression toward children. Isolation poses serious risks for the perpetration of IPV. Factor characteristics of IPV, such as social isolation from supportive peers, functional isolation from support services, and excessive monitoring and control of victims’ activities, are also results of the pandemic and its associated orders (28). Our findings show empathic concern was among the best predictor of lower risk of violence among partners.
Finally, we assessed the effect of time on family violence and found that physical punishment toward children as well as partner violence increased later in the pandemic as compared to the beginning of the pandemic. Given that COVID-19 pandemic is still alarming today, we believe increasing awareness about family violence is crucial.
Even though we are testing here as proxy indicators of child maltreatment, these indicators are not as distinct from physical maltreatment, but instead related to a continuum form of aggressive acts toward children that can impact child’s development (29). We also used yelling/screaming at children as a proxy indicator of emotional abuse that has a negative impact on a child’s emotional health (30).
Our study had several limitations. We used a self-report measurement to acquire predictors of child maltreatment and IPV. Our study is therefore examining indicators of abuse. Our sample is also limited to Amazon’s Mechanical Turk and Prolific. Additionally, for the comparison in child maltreatment between different times of the pandemic, given that we used data of independent samples, there might be other confounders not accounted for that may have impacted the rates of child abuse. We have accounted for different factors such as education and income. However there might be a potential complex dependence structure between these independent factors as they can be correlated.
Given the markedly high rates of both IPV and indicators of child maltreatment compared to the previous years (31), it is critical that educators and professionals actively screen for indicators of abuse. Parenting interventions such as the ACT Parents Raising Safe Kids program (32) aim to improve parental nurturing and emotion regulation. It is also imperative that protective mechanisms are put in place to safeguard children from maltreatment during the pandemic and beyond. Increased efforts to educate healthcare, mental health care, social service providers and other professionals on recognizing and responding to child maltreatment through both in-person and virtual service provision also will be necessary (33). Programs such as the Child Advocacy Studies Training program (CAST) that educate undergraduate and graduate students in a wide variety of fields about child maltreatment identification and responding may effectively begin to address this goal (34). Policy-makers, child welfare and family-serving organizations should prioritize the development of safe and confidential spaces for children to discuss their concerns and experiences; some nations have developed models for this (33). Screening for child maltreatment can be broadened and placed in a variety of institutions including childcare centers, health clinics, and faith-based organizations (35). Innovative methods to reach children during critical times should be identified. For example, social media and virtual platforms are being explored as potential tools for improved understanding and monitoring of children’s experiences with family violence as well as improved accurate reporting of child maltreatment (36, 37). For youths traumatized by child maltreatment, trauma-informed telemental health services and remote case management are critical (8, 37). Lastly, programs addressing parenting practices and parenting stress should be destigmatized, and made to be universally available, including being readily accessible online (8, 35, 37).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Human Research Protection Program at the University of Toledo. The patients/participants provided their written informed consent to participate in this study.
KT designed research, collected data, performed analysis and interpretation, and co-wrote the manuscript. EO’L performed analysis and co-write the manuscript. KW designed study, collected data, and performed analysis. PD collected data and performed analysis. SL designed research, collected data, performed analysis and interpretation. MK designed research, performed analysis and interpretation, and co-wrote the manuscript. EA conceived and designed research, performed data analysis and interpretation, and co-wrote the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the Department of Psychiatry, College of Medicine and Life Sciences, University of Toledo.
We would like to thank all the participants who took part in our study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. U.S. Department of Health and Human Services. Child Maltreatment 2018. Washington, DC: U.S. Department of Health and Human Services (2020).
2. Stuijfzand S, Deforges C, Sandoz V, Sajin CT, Jaques C, Elmers J, et al. Psychological impact of an epidemic/pandemic on the mental health of healthcare professionals: a rapid review. BMC Public Health. (2020) 20:1230. doi: 10.1186/s12889-020-09322-z
3. Lee SJ, Ward KP, Rodriguez CM. Longitudinal analysis of short-term changes in relationship conflict during COVID-19: A risk and resilience perspective. J Interpers Violence. (2022) 37:NP14239–61. doi: 10.1177/08862605211006359
4. Gassman-Pines A, Ananat EO, Fitz-Henley J. COVID-19 and parent-child psychological well-being. Pediatrics. (2020) 146:e2020007294.
5. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. doi: 10.3390/ijerph17051729
6. Espinosa A, Ruglass LM, Dambreville N, Shevorykin A, Nicholson R, Sykes KM. Correlates of child abuse potential among African American and latina mothers: a developmental-ecological perspective. Child Abuse Negl. (2017) 70:222–30. doi: 10.1016/j.chiabu.2017.06.003
7. Green E, Chase RM, Zayzay J, Finnegan A, Puffer ES. The impact of the 2014 Ebola virus disease outbreak in Liberia on parent preferences for harsh discipline practices: a quasi-experimental, pre-post design. Glob Ment Health. (2018) 5:e1. doi: 10.1017/gmh.2017.24
8. Lawson M, Piel MH, Simon M. Child maltreatment during the COVID-19 pandemic: consequences of parental job loss on psychological and physical abuse towards children. Child Abuse Negl. (2020) 110:104709. doi: 10.1016/j.chiabu.2020.104709
9. Bradbury-Jones C, Isham L. The pandemic paradox: the consequences of COVID-19 on domestic violence. J Clin Nurs. (2020) 29:2047–9.
10. Park CL, Russell BS, Fendrich M, Finkelstein-Fox L, Hutchison M, Becker J. Americans’ COVID-19 stress, coping, and adherence to CDC guidelines. J Gen Intern Med. (2020) 35:2296–303. doi: 10.1007/s11606-020-05898-9
11. Rodriguez CM. Analog of parental empathy: association with physical child abuse risk and punishment intentions. Child Abuse Negl. (2013) 37:493–9.
12. Buhrmester M, Kwang T, Gosling SD. Amazon’s mechanical Turk: a new source of inexpensive yet high-quality, data? Perspect Psychol Sci. (2011) 6:3–5. doi: 10.1177/1745691610393980
13. Straus MA, Hamby SL, Finkelhor D, Moore DW, Runyan D. Identification of child maltreatment with the parent-child conflict tactics scales: development and psychometric data for a national sample of American parents. Child Abuse Negl. (1998) 22:249–70.
14. Davis MH. Measuring individual differences in empathy: evidence for a multidimensional approach. J Pers Soc Psychol. (1983) 44:113. doi: 10.3389/fpsyg.2021.588934
15. Kroenke K, Strine TW, Spitzer RL, Williams JB, Berry JT, Mokdad AH. The PHQ-8 as a measure of current depression in the general population. J Affect Disord. (2009) 114:163–73.
16. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7.
17. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behav Res Ther. (1995) 33:335–43. doi: 10.1016/0005-7967(94)00075-u
18. Pedregosa F, Varoquaux G, Gramfort A, Michel V, Thirion B, Grisel O, et al. Scikit-learn: machine learning in python. J Mach Learn Res. (2011) 12:2825–30.
20. Vabalas A, Gowen E, Poliakoff E, Casson AJ. Machine learning algorithm validation with a limited sample size. PLoS One. (2019) 14:e0224365. doi: 10.1371/journal.pone.0224365
21. Hawryluck L, Gold WL, Robinson S, Pogorski S, Galea S, Styra R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg Infect Dis. (2004) 10:1206.
22. Lee SJ, Ward KP, Chang OD, Downing KM. Parenting activities and the transition to home-based education during the COVID-19 pandemic. Child Youth Serv Rev. (2021) 122:105585. doi: 10.1016/j.childyouth.2020.105585
23. Lee SJ, Taylor CA, Bellamy JL. Paternal depression and risk for child neglect in father-involved families of young children. Child Abuse Negl. (2012) 36:461–9. doi: 10.1016/j.chiabu.2012.04.002
24. Miller PA, Eisenberg N. The relation of empathy to aggressive and externalizing/antisocial behavior. Psychol Bull. (1988) 103:324.
25. Bavolek SJ, Kline DF, McLaughlin JA, Publicover PR. Primary prevention of child abuse and neglect: identification of high-risk adolescents. Child Abuse Negl. (1979) 3:1071–80. doi: 10.1136/bmjopen-2017-016140
26. Francis KJ, Wolfe DA. Cognitive and emotional differences between abusive and non-abusive fathers. Child Abuse Negl. (2008) 32:1127–37. doi: 10.1016/j.chiabu.2008.05.007
27. Perez-Albeniz A, de Paul J. Dispositional empathy in high-and low-risk parents for child physical abuse. Child Abuse Negl. (2003) 27:769–80.
28. Van Gelder N, Peterman A, Potts A, O’Donnell M, Thompson K, Shah N, et al. COVID-19: reducing the risk of infection might increase the risk of intimate partner violence. EClin Med. (2020) 21:100348.
29. Gershoff ET, Grogan-Kaylor A. Spanking and child outcomes: old controversies and new meta-analyses. J Fam Psychol. (2016) 30:453. doi: 10.1037/fam0000191
30. Runyan D. Child abuse and neglect by parents and other caregivers. In: Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R editors. World Report on Violence and Health. Geneva: World Health Organization (2002).
31. Finkelhor D, Turner H, Wormuth BK, Vanderminden J, Hamby S. Corporal punishment: current rates from a national survey. J Child Fam Stud. (2019) 28:1991–7. doi: 10.1177/14034948211023634
32. Silva J. ACT Raising Safe Kids Program. Washington, DC: American Psychological Association (2011).
33. Kimber M, McTavish JR, Vanstone M, Stewart DE, MacMillan HL. Child maltreatment online education for healthcare and social service providers: implications for the COVID-19 context and beyond. Child Abuse Negl. (2021) 116:104743. doi: 10.1016/j.chiabu.2020.104743
34. Cross TP, Chiu YL. Mississippi’s experience implementing a statewide child advocacy studies training (CAST) initiative. J Fam Trauma Child Custody Child Dev. (2021) 18:299–318.
35. Musser ED, Riopelle C, Latham R. Child maltreatment in the time of COVID-19: changes in the Florida foster care system surrounding the COVID-19 safer-at-home order. Child Abuse Negl. (2021) 116:104945. doi: 10.1016/j.chiabu.2021.104945
36. Babyey P, Capela F, Cappa C, Lipizzi C, Petrowski N, Ramirez-Marquez J. Using social media data for assessing children’s exposure to violence during the COVID-19 pandemic. Child Abuse Negl. (2021) 116:104747. doi: 10.1016/j.chiabu.2020.104747
Keywords: COVID-19, child maltreatment, intimate partner violence, anxiety, depression, machine learning, random forest
Citation: Todorovic K, O’Leary E, Ward KP, Devarasetty PP, Lee SJ, Knox M and Andari E (2022) Prevalence, increase and predictors of family violence during the COVID-19 pandemic, using modern machine learning approaches. Front. Psychiatry 13:883294. doi: 10.3389/fpsyt.2022.883294
Received: 24 February 2022; Accepted: 12 July 2022;
Published: 11 August 2022.
Edited by:
Tillmann H. C. Kruger, Hannover Medical School, GermanyReviewed by:
Katharina Schüller, Maastricht University, NetherlandsCopyright © 2022 Todorovic, O’Leary, Ward, Devarasetty, Lee, Knox and Andari. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elissar Andari, ZWxpc3Nhci5hbmRhcmlAVXRvbGVkby5lZHU=, ZWFuZGFyaUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.