 Caroline Schmitt-Koopmann
Caroline Schmitt-Koopmann Carole-Anne Baud2
Carole-Anne Baud2- 1Service of Addiction Medicine, Lausanne University Hospital (CHUV), University of Lausanne, Lausanne, Switzerland
- 2Faculty of Business and Economics, University of Lausanne, Lausanne, Switzerland
- 3Faculty of Law, University of Geneva, Geneve, Switzerland
In 2021, the manufacturer of diamorphine reported a possible impending shortage for Switzerland and Germany. This led us to investigate this controlled medicine’s manufacture, market, and regulatory constraints. Based on our analysis of legal texts and gray literature in the form of reports and documents, we propose recommendations to prevent and address diamorphine shortages in Switzerland. Diamorphine, also known as pharmaceutical “heroin,” is used medically to treat persons with severe opioid use disorder in a handful of countries. The controlled medicine is manufactured from morphine, which, in turn, is extracted from opium poppies. Studying data from the International Narcotics Control Board for 2019, we find that Switzerland accounts for almost half of the worldwide medical consumption of diamorphine. It manufactures more than half of the worldwide total and keeps the largest stocks. Moreover, Switzerland is dependent on a sole supplier of diamorphine (monopoly). As a niche product, diamorphine has an increased risk of shortage. Such a shortage would immediately threaten a valuable public health program for around 1,660 Swiss patients. We believe it is urgent to curtail the monopoly and ensure a stable supply for the future.
Introduction
Diamorphine, also known under its old brand name Heroin, is one of the most controversial substances worldwide. According to the 1961 Single Convention, it is a schedule I drug, meaning it is subject to the highest degree of control (1). In Switzerland, diamorphine is classified as a prohibited controlled substance (schedule d), but it can be used as a medicine under particular conditions (2).
Indeed, the Swiss Agency for Therapeutic Products (Swissmedic) approved diamorphine (under the brand name Diaphin) for treating persons with severe opioid use disorder in 2001 (3). Treatment with diamorphine prescription (TDP) is the only approved effective alternative for persons who do not respond to classic opioid agonist treatments (OAT), such as methadone or buprenorphine treatment (4, 5). It was introduced in 1994 in Switzerland as a pragmatic solution to an AIDS crisis and open drug scenes (6). Under heavy criticism at first, it is now enshrined in Swiss law (6) and recognized internationally as a successful and cost-effective public health program (5, 7, 8). In 2019, 1,663 persons in Switzerland received TDP, which has been reimbursed since 2002 by health insurers (6, 9).
In Switzerland, DiaMo Narcotics GmbH holds the marketing authorization for the only three diamorphine products available: Diaphin i.v. (intravenous), Diaphin IR (immediate-release) tablets, and Diaphin SR (slow-release) tablets (3). DiaMo Narcotics GmbH sources the active ingredient, diamorphine, from two active ingredient manufacturers (10). Two other contract manufacturers then formulate the active ingredient: One contract manufacturer formulates Diaphin i.v., whereas Diaphin IR and SR tablets are formulated by another (10). Due to the small order volume, finding another contract manufacturer is not a realistic option, as noted by a report which analyzed the diamorphine supply situation in January 2021 (10).
In theory, other opioid products could constitute alternatives to diamorphine, but none so far have been authorized for this indication.
The 2021 Diamorphine Supply Disruption
The risk of a diamorphine shortage was already identified in 2016 by the Swiss Federal Council (11). In November 2020 the risk of a supply shortage of Diaphin i.v. became acute, due to the bankruptcy of the contract manufacturer, which formulated Diaphin i.v.: Legacy Pharmaceuticals (10). There were no stocks of Diaphin i.v. because of past difficulties with the contract manufacturer (10).
The impending shortage was not made public, and communication was restricted to the involved Swiss authorities and TDP centers. According to a report on the Swiss TDP, the communication regarding the supply was not transparent enough (10). In contrast to Swiss authorities, the German Medicines Agency announced an impending supply disruption of Diaphin i.v. for the German market in March 2021 (12). Based on publicly available information it is not possible to know if the bankruptcy of Legacy Pharmaceuticals also caused the German Diaphin i.v. supply disruption.
Shortages of diamorphine pose a significant problem for people in TDP and their treating physicians. Risks associated with treatment discontinuation are poorer mental and physical health, increased illegal activities, and consumption of illicit substances (13). Hence, a rapid solution is needed to supply the affected population in case of a shortage.
Structure of the Article
This article describes Switzerland’s dependence on a diamorphine monopoly. We analyzed legal texts and gray literature in the form of reports and documents from Swiss and other authorities. Furthermore, we used reports and data from the International Narcotics Control Board (INCB).
Section “How Did Diamorphine Become a Niche Product?” will describe how the once widely used diamorphine has become a highly regulated niche product. The manufacturing and diamorphine market will be analyzed in sections “How Is Diamorphine Manufactured?” and “How Is the Market for Diamorphine Structured?” In section “Are There Legal or Regulatory Constraints Preventing the Introduction of a Diamorphine Generic in Switzerland?” we identify relevant regulations for diamorphine manufacturers in Switzerland. In section “How Did Switzerland Address the 2021 Supply Disruption?” we analyze the response to the 2021 supply disruption in Switzerland and compare it to the United Kingdom (UK). Lastly, we formulate actionable recommendations in section “What Do We Recommend?”
This research is part of a project funded by the Swiss National Science Foundation (SNSF grant number 182477), which aims to analyze the current controlled medicines legislation in Switzerland.
How Did Diamorphine Become a Niche Product?
Under the brand name heroin, Bayer started commercial production of pharmaceutical diamorphine in 1898; a few years later, other pharmaceutical companies started offering diamorphine as well (14). In the late nineteenth century and early twentieth century, diamorphine was widely used and marketed for “heavy coughs, to relieve the pain of childbirth and serious war injuries, prepare patients for anesthesia, and control certain mental disorders” (15). At the turn of the century, addiction caused by diamorphine was first recognized as a problem; the first so-called “morphine maintenance clinics” were set up to treat persons with opioid use disorder (16, 17).
Internationally, the 1912 International Opium Convention aimed to control opiates strictly but was not implemented globally due to the outbreak of World War I (17). Diamorphine production was limited after the 1931 Geneva Convention established constraints and many countries banned the substance (16, 17). In 1961, the Single Convention on Narcotic Drugs replaced previous treaties and is in its revised version still in force today (1, 18).
At a national level, the United States (US) passed the Harrison Act in 1914, introducing federal narcotics controls (14, 16, 19), followed by an outright ban on diamorphine in 1924 (16, 19).
In contrast, in the United Kingdom (UK), the 1926 Rolleston report laid the groundwork to continue administering morphine or diamorphine to treat persons with an opioid (heroin) use disorder who did not respond to abstinence-based programs (20, 21). The so-called “British system” remained intact until the passing of the Dangerous Drugs Act in 1967, which restricted the right to prescribe diamorphine to specifically licensed doctors only (22). This led to a decrease in people treated with diamorphine (23–25). Clinical guidelines published in 1984 cemented the shift from injectable diamorphine to oral methadone prescription (22). Interestingly, the UK remains the only country in the world to also use diamorphine for severe pain associated with surgical procedures, myocardial infarction, or pain in the terminally ill, and for the relief of dyspnea in acute pulmonary edema (26).
Switzerland passed its first narcotics law that introduced an authorization requirement for manufacturing and trading opiates and cocaine in 1924 (27). Still in force today is the Federal Act on Narcotics and Psychotropic Substances (NarcA), which was passed in 1951 (28). It has often been revised, with the last major change dating to 2011 when the four-pillar policy (prevention, therapy, harm reduction, repression) and TDP were enshrined in the law. Aside from Switzerland, TDP is currently only available in Denmark, Germany, Luxembourg, the Netherlands, the United Kingdom, and Canada (29).
In conclusion, after being widely used, diamorphine is nowadays a niche product in few countries with low production volumes, putting it at high risk of shortage.
How Is Diamorphine Manufactured?
The licit manufacture of diamorphine starts with the cultivation of poppy plants (Papaver somniferum) on licensed fields (30). Papaver somniferum contains, among other alkaloids, morphine, codeine, and thebaine (31). All three are chemically related and easily convertible into one another (31). Breeding allowed for the creation of varieties that yield higher amounts of morphine or other opioid alkaloids (31).
According to the INCB, the main licit cultivation countries are Australia, France, Hungary, India, Slovakia, Spain, and Turkey (Figure 1) (32). In 2019, Spain was the largest producer of morphine-rich raw materials (141 metric tons), followed by Turkey (85 metric tons), Australia (85 metric tons), and France (44 metric tons). Taken together, these four countries were estimated to account for 91% of the licit global production of morphine-rich raw materials in 2020.
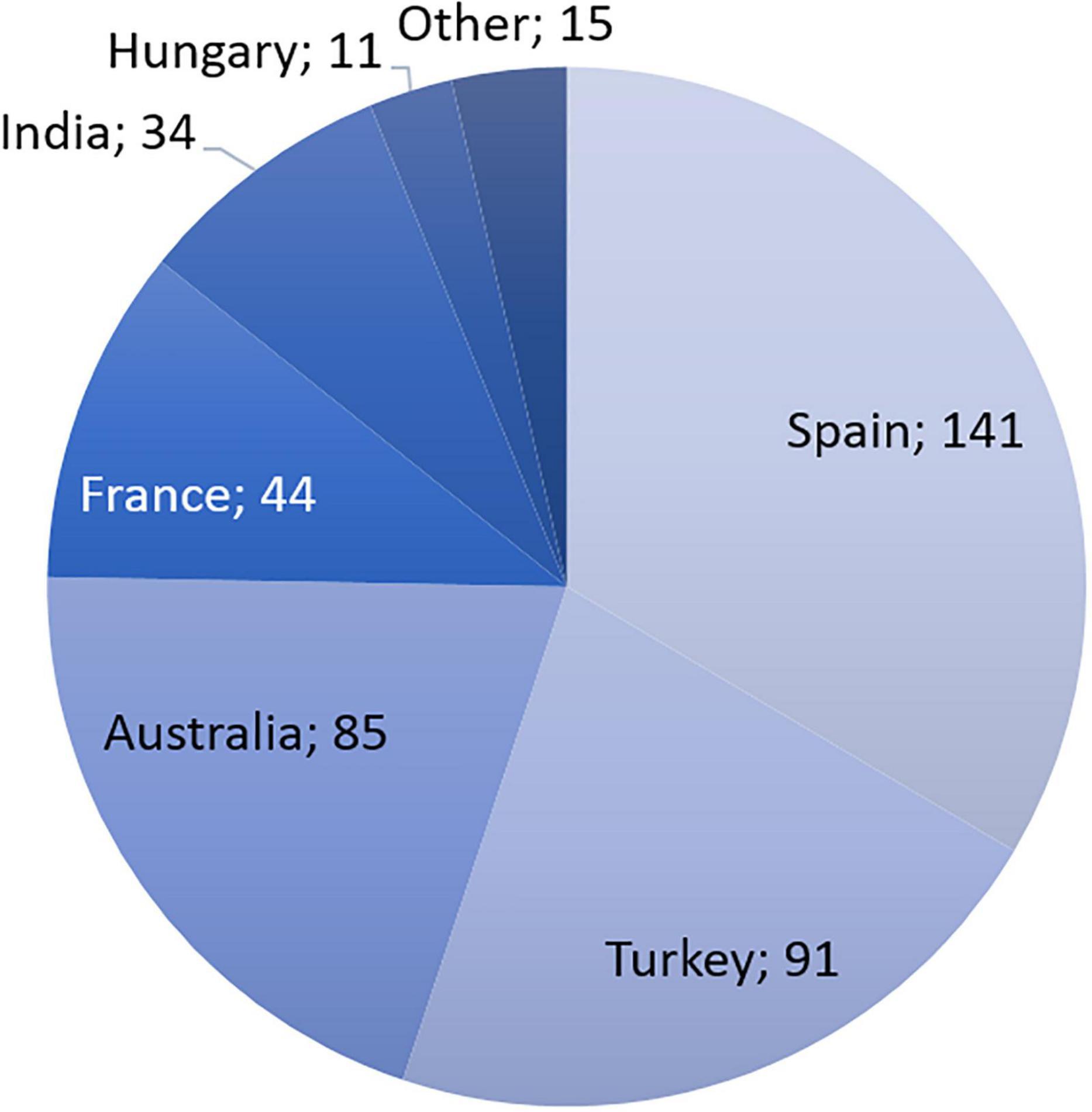
Figure 1. Production of opiate raw materials rich in morphine in tons of morphine equivalent, 2019. Based on data from INCB technical report 2020.
The fully matured poppy plants’ field-dried leaves, stalks, and seedpods are used to make poppy straw concentrate (1). In the next step, morphine is extracted from the poppy straw concentrate before reacting with either acetic acid or acetic anhydride to produce diamorphine. Pure diamorphine, both as a base and as a hydrochloride salt, is a colorless crystalline solid (33). All currently available diamorphine preparations for injection are lyophilized powders because an aqueous solution is not chemically stable enough for storage (34).
Whilst opiates are still manufactured from the opium poppy, advances in synthetic biology enable the creation of a yeast strain capable of making morphine from glucose (35). Four groups of researchers introduced different genetic components into the yeast genome, which combined constitute the entire morphine synthesis pathway (36–41). A morphine manufacturing yeast strain could change the current supply chain, as the manufacture of morphine by self-replicating yeast might be cheaper and more stable than the current processes. However, to the best of our knowledge, no morphine product using this technology has entered the market.
Consequently, the current dependence on the cultivation of Papaver somniferum is a risk factor that could lead to supply disruptions for morphine and diamorphine. The available product on the global market is subject to yearly fluctuations, for example, due to heavy rains or droughts (42). Additionally, the overall demand for opioids is increasing because developing nations require appropriate amounts of opioids to treat pain. For example, in Uganda, opioid analgesic consumption increased by 342% from 2000 to 2015 but overall remained extremely low (43). This leads to more competition on the global market for poppy straw, which can increase prices if the demand is not met with adequate supply (44, 45).
How Is the Market for Diamorphine Structured?
Over the past 20 years, according to the INCB, the licit manufacture of diamorphine worldwide averaged 700 kg annually (32). In 2019, Switzerland manufactured, consumed, and kept the largest stock of diamorphine worldwide (46).
Figure 2C shows that in 2019, a total of 1 metric ton of diamorphine was manufactured by Switzerland and the United Kingdom (557.2 kg, or 55.3%; respectively 450 kg, or 44.7%). Both countries also have the largest stocks of diamorphine in 2019 (Switzerland: 1.2 metric tons; UK 0.8 metric tons), together holding 80.2% of the stocks worldwide (Figure 2A).
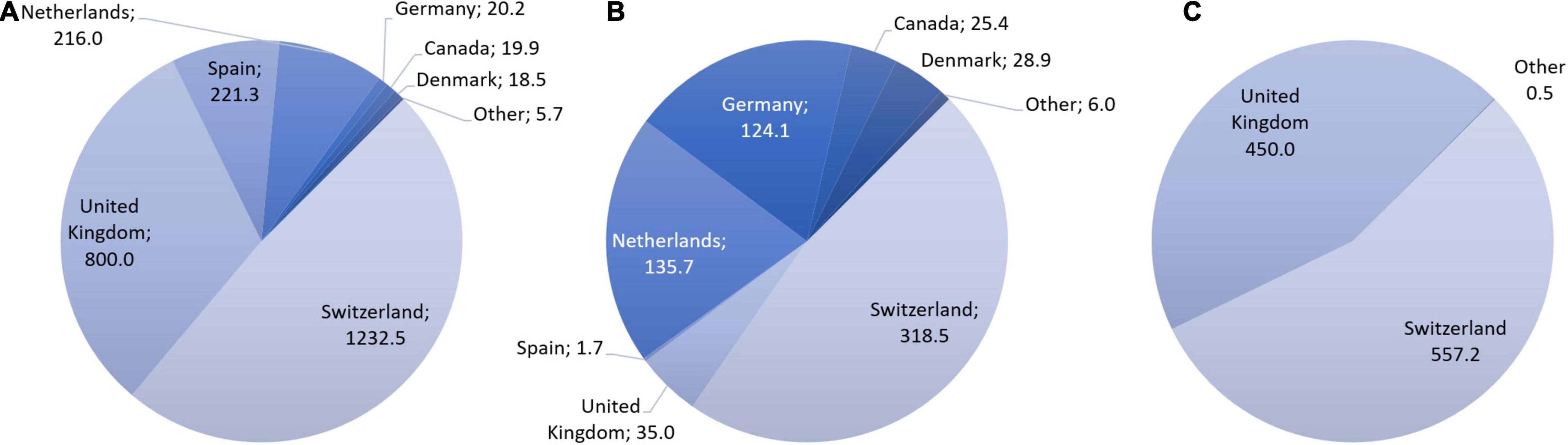
Figure 2. Stocks (A), consumption (B), and manufacture (C) of diamorphine in kg per country, 2019. Based on data requested from INCB.
In 2019, Switzerland accounted for roughly half (318.5 kg, 47.2%) of the global medical diamorphine consumption (675.4 kg). Other countries with significant diamorphine consumption are the Netherlands, Germany, the United Kingdom, Denmark, and Canada (Figure 2B). Table 1 shows that Switzerland’s consumption of diamorphine is extraordinarily high when related to its population size compared with the other countries.

Table 1. Diamorphine consumption and population size of Switzerland, Netherlands, Germany, United Kingdom (UK), Denmark, and Canada in 2019.
Diaphin, is the only authorized diamorphine product in Switzerland, Germany, and Denmark, representing more than two-thirds of the world’s diamorphine consumption (3, 47, 48). Hence, DiaMo holds the monopoly in the cited countries and dominates the world market.
Are There Legal or Regulatory Constraints Preventing the Introduction of a Diamorphine Generic in Switzerland?
Generally, the first constraint for a generic is the existence of a patent. A patent is an intellectual property right for a technical invention, such as a medicine. It allows its owner to prevent others from using the patented invention for commercial purposes for up to 20 years from the patent application (49, 50). In the case of diamorphine, there were no patents on the substance itself. Indeed, Bayer, who started commercial production of diamorphine, could not patent the substance because it was not new, as the English chemist Charles Wright had already synthesized and published a description of diamorphine in 1874 (51).
Another mechanism is document protection, also called marketing exclusivity; it prohibits competitors from relying upon and referring to data submitted to the authority by the originator company. The Swiss Therapeutic Products Act (TPA) allows 10 years of document protection for new medicines (52, 53). Before the expiry of this period, Swissmedic cannot grant a third party a marketing authorization (typically a generic authorization), which relies on the protected data (54). Swissmedic first approved the 10 g i.v. diamorphine formulation in December 2001 (3). Hence, document protection has long run out. More recently, the originator received document protection for a 5 g i.v. formulation, which will last 3 years, until 29.07.2024 (3, 55). However, this should not discourage potential competitors as the document protection only protects the 5 g formulation. Similarly, even though Diaphin has orphan drug status, it was not granted increased document protection of 15 years because it was registered before 2019 (56, 57).
Another administrative hurdle faced by companies wanting to supply diamorphine in Switzerland is applying for a narcotics license from Swissmedic. However, no exceptional license from the Federal Office of Public Health (FOPH) is needed because diamorphine is the active ingredient of an authorized medicinal product (58, 59). Swissmedic will license persons and companies, including brokers, agents, and the army pharmacy, to handle authorized medicinal products containing schedule d substances, such as diamorphine (60). In practice, it considers companies with a license to handle schedule a substances, e.g., morphine, to be also authorize to handle medicinal products containing schedule d substances (i.e., diamorphine) (61). Indeed, 321 companies had a schedule a narcotic license as of mid-December 2021 (62). All of which would, in theory, be allowed to handle diamorphine.
In summary, there is no patent protection on diamorphine, and document protection only covers 5 g Diaphin i.v. Furthermore, we find that diamorphine is subject to constraints similar to substances such as morphine. Hence, in our opinion, there are no regulatory hurdles that should discourage potential competitors from entering the Swiss market.
How Did Switzerland Address the 2021 Supply Disruption?
According to a report on the Swiss TDP, the following actions were taken to mitigate the 2021 shortage: allocation by the manufacturer based on past orders and limitation of purchases; recommendation to switch to Diaphin IR or SR tablets or other OAT; and the postponement of the study on the nasal application of Diaphin i.v. (10). The report also stated that a new manufacturer for Diaphin i.v. had been found in the Netherlands, which resolved the 2021 supply disruption (10).
Compulsory stockpiling is a precautionary measure of import-dependent Switzerland; the stocks can be released as needed when the demand for important basic supplies, including medicines, can no longer be met on the market due to a (temporary) shortage. However, diamorphine is not subject to compulsory stockpiling by the marketing authorization holder, unlike many other opioid medicines such as morphine, fentanyl, and methadone (63). Hence, there were no compulsory stocks that could be released in response to the 2021 supply disruption.
Even though Switzerland seems to have overcome the 2021 supply disruption unscathed, it remains unprepared for a diamorphine shortage.
Compared to Switzerland, the UK has taken a more active approach to managing the risks of a potential diamorphine shortage. In 2006, the UK Office of Fair Trading issued a review that alerted the government of a monopoly situation in the UK (64). The report states: “the Government recognizes that a lack of competition may continue to have a knock-on effect on both downstream prices and the ability of competitors to enter into the market.” Nowadays, the UK has several suppliers for diamorphine (Supplementary Table 1) but still encounters shortages (65, 66). For example, the 5 and 10 mg diamorphine i.v. formulation has intermittently been in short supply since 2018 despite having two suppliers (66). In response to the supply issues, the UK National Health Service (NHS) issued recommendations and implemented medical guidelines to tackle the shortages (67). The NHS recommended switching patients permanently to morphine sulfate solution, where clinically applicable. Primary and secondary care were asked to ensure that no new patients would be started on the diamorphine i.v. strengths with unstable supply; furthermore, patients patients should not be switched to higher strengths, as there were insufficient stocks to support the increased use.
What Do We Recommend?
Based on the information we gathered, authorities in Switzerland have done little to address the diamorphine monopoly and potential shortages. Probably because even though shortages loomed, a rupture of stock never occurred. However, the recent supply chain disruption of diamorphine and the shortage of Sevre-Long (slow-release morphine used in OAT) highlight the importance of preparing for a shortage situation (68, 69). Hence, we recommend several actions to prepare for a potential shortage, sorted by the ease of implementation.
First, authorities and relevant stakeholders should elaborate a plan describing actions to take in a shortage situation. The plan should include a national distribution key to attribute the remaining limited stocks of diamorphine among persons in TDP. This medical-ethical (triage) guideline will help physicians to navigate the shortage. Similar to the SARS-COV2 intensive care triage guidelines, there should be a national ethical, systematic and evidence-based framework to approach the patient allocation of scarce medications in general.
Secondly, diamorphine should be added to the list of compulsory stocked medicines to stabilize the supply. Considering that diamorphine has a long shelf life, this preventive measure could help alleviate short-term ruptures in the supply chain of up to 3 months.
Thirdly, long-term options to reinforce the supply chain of diamorphine should be evaluated. Indeed, the report on the Swiss TDP listed four proposals to reinforce the supply chain: optimization of the current supply by the pharmaceutical industry; decentralized manufacturing by hospital pharmacies; procurement through government; and manufacturing by the government (10).
In our view, these proposed measures are not enough to improve the situation long-term, at least as long as the monopoly remains. Decentralized manufacturing by hospital pharmacies carries logistical issues, especially for TDP centers not in close proximity to hospitals, and would likely not be cheap. Procurement by the government through a tender would likely alleviate some of the risks; however, to be successful there must be interested pharmaceutical companies. Alternatively, Switzerland could evaluate other suppliers, for example, from the UK (Supplementary Table 1). However, this would be problematic even short-term, because Swiss demand would likely extend beyond the available UK supply, as Switzerland uses almost 10 times more diamorphine annually.
Given the perceived “unattractiveness” of manufacturing diamorphine and the current monopoly, manufacturing by the Swiss army pharmacy should be evaluated. The army pharmacy is the only federal administrative unit in Switzerland that holds Swissmedic licenses to manufacture, import, wholesale trade, and export medicinal products (11). Manufacturing of diamorphine by the army pharmacy is the most radical intervention. It would require allowing the Swiss army pharmacy to compete with the pharmaceutical industry, which is unlikely to gather the needed political support (70).
Lastly, injectable hydromorphone should be evaluated as an alternative to diamorphine. The Canadian NAOMI study, a double-blind study with injectable hydromorphone and diamorphine, demonstrated that patients were unable to detect which one they received (71). The authors stated: “the fact that most patients in the hydromorphone group thought they were receiving heroin suggests that hydromorphone can effectively treat and retain opioid-dependent individuals” (71). The SALOME study provided evidence that the injectable hydromorphone was non-inferior to diamorphine for long-term opioid use disorders (72). Nevertheless, it should be kept in mind that the TDP population often has other psychiatric comorbidities (73, 74), including severe chronic anxiety, which can make them more vulnerable to changes. Hence, switching patients from diamorphine to hydromorphone, in case of a shortage, could destabilize a person in treatment. Moreover, reimbursement could be problematic as hydromorphone would be used off-label, and the treatment with hydromorphone instead of diamorphine would be likely several times more expensive. To our knowledge, there has been no large-scale use of hydromorphone for the treatment of opioid use disorders in Switzerland.
In summary, diamorphine should be added to the list of compulsory stocks, and triage guidelines should be elaborated for the allocation of scarce medicines. The potential of the Swiss army pharmacy to manufacture diamorphine should be evaluated if there are not enough pharmaceutical companies interested in bringing other diamorphine products on the market.
Conclusion
In conclusion, Switzerland has so far been lucky in that it has not suffered a shortage of diamorphine; nevertheless, the unstable supply was evidenced recently by reports in Switzerland and Germany. Measures that prevent a shortage in the future and precise planning for a shortage situation must be implemented. TDP is a valuable and successful public health program, and an insufficient supply of diamorphine would affect persons in treatment but also the society as a whole. Switzerland surely does not want to go back to the extreme and very public desperation of the open drug scenes.
Data Availability Statement
The dataset of diamorphine manufacturing, stocks, and consumption in 2019, used in this article, can be requested from the International Narcotics Control Board (INCB). Further enquiries can be directed to the corresponding author.
Author Contributions
CS-K: investigation, data curation, and writing—original draft preparation. CS-K, C-AB, VJ, and OS: writing—review and editing. VJ and OS: supervision and project administration. VJ, C-AB, and OS: funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Schweizerische Nationalfonds zur Förderung der wissenschaftlichen Forschung (Swiss National Science Foundation, SNSF) (grant no. 182477).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank the International Narcotics Control Board (INCB) for providing us with the data for diamorphine, which we use in this publication.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.882299/full#supplementary-material
References
1. Fedlex. SR 0.812.121.0 - Einheits-Übereinkommen von 1961 über die Betäubungsmittel, abgeschlossen am 30. (1961). Available online at: https://www.fedlex.admin.ch/eli/cc/1970/802_803_802/de (accessed November 25, 2020)
2. SR 812.121.11 - Verordnung des Edi vom 30. Mai 2011 über die Verzeichnisse der Betäubungsmittel, psychotropen Stoffe, Vorläuferstoffe und Hilfschemikalien (Betäubungsmittelverzeichnisverordnung, BetmVV-EDI). (2020). Available online at: https://www.admin.ch/opc/de/classified-compilation/20101220/index.html (accessed December 5, 2020]
3. Swissmedic. Lists and directories; 1.1 Authorised Human Medicinal Products. (2021). Available online at: https://www.swissmedic.ch/dam/swissmedic/en/dokumente/internetlisten/zugelassene_arzneimittel_ham.xlsx.download.xlsx/Zugelassene_Arzneimittel_HAM.xlsx (accessed December 20, 2021)
4. Strang J, Groshkova T, Uchtenhagen A, van den Brink W, Haasen C, Schechter MT, et al. Heroin on trial: systematic review and meta-analysis of randomised trials of diamorphine-prescribing as treatment for refractory heroin addiction†. Br J Psychiatry. (2015) 207:5–14. doi: 10.1192/bjp.bp.114.149195
5. Dijkgraaf MGW, van der Zanden BP, de Borgie CAJM, Blanken P, van Ree JM, van den Brink W. Cost utility analysis of co-prescribed heroin compared with methadone maintenance treatment in heroin addicts in two randomised trials. BMJ. (2005) 330:1297. doi: 10.1136/bmj.330.7503.1297
6. Uchtenhagen A. Heroin-assisted treatment in Switzerland: a case study in policy change. Addiction. (2010) 105:29–37. doi: 10.1111/j.1360-0443.2009.02741.x
7. Schaub M, Bolliger H, Hiltebrand D. Heroingestützte Behandlung - Veränderung der Klientel in der Schweiz und Review der Kostenanalysen. Zürich: Institut suisse de recherche sur la santé publique et les addictions (2013).
8. Nosyk B, Guh DP, Bansback NJ, Oviedo-Joekes E, Brissette S, Marsh DC, et al. Cost-effectiveness of diacetylmorphine versus methadone for chronic opioid dependence refractory to treatment. CMAJ. (2012) 184:E317–28. doi: 10.1503/cmaj.110669
9. Gmel G, Labhart F, Maffli E. Heroingestützte/diacetylmorphingestützte Behandlung in der Schweiz - Resultate der Erhebung 2019 (Forschungsbericht Nr. 118). Lausanne: Sucht Schweiz (2020).
10. Frey K, Pestoni A, Häusermann M. Situationsanalyse der heroingestützten Behandlung (HeGeBe). [Schlussbericht]. Zürich: KEK - CDC (2021).
11. Sicherheit in der Medikamentenversorgung. Bericht des Bundesrates in Erfüllung des Postulats Heim (12.3426) vom 4. Juni 2012. (2016). Available online at: https://www.parlament.ch/centers/eparl/curia/2012/20123426/Bericht%20BR%20D.pdf (accessed October 20, 2021)
12. Bundesinstitut für Arzneimittel und Medizinprodukte (BfArM). Lieferengpässe - Ergebnisprotokoll der 4. Sitzung des Beirats nach §52b Absatz 3b AMG zur Bewertung der Versorgungslage mit Arzneimitteln, die zur Anwendung bei Menschen bestimmt sind. (2021). Available online at: https://www.bfarm.de/DE/Arzneimittel/Arzneimittelinformationen/Lieferengpaesse/Beirat/protokolle/protokoll_beirat_4.html (accessed September 16, 2021)
13. van den Brink W, Hendriks VM, Blanken P, Koeter MWJ, van Zwieten BJ, Ree JM. Medical prescription of heroin to treatment resistant heroin addicts: two randomised controlled trials. BMJ. (2003) 327:310. doi: 10.1136/bmj.327.7410.310
15. Hoffmann F. Science History Institute. (2016). Available online at: https://www.sciencehistory.org/historical-profile/felix-hoffmann (accessed September 16, 2021)
16. Sneader W. The discovery of heroin. Lancet. (1998) 352:1697–9. doi: 10.1016/S0140-6736(98)07115-3
17. UNODC. A Century of International Drug Control. World Drug Rep. (2008) 2008:173–222. doi: 10.18356/4713aa6f-en
18. UNODC. The International Drug Control Conventions. (2022). Available online at: https://www.unodc.org/documents/commissions/CND/Int_Drug_Control_Conventions/Ebook/The_International_Drug_Control_Conventions_E.pdf (accessed March 30, 2022)
20. Strang J, Gossop M. Heroin addiction and drug policy: the British system. Oxford: Oxford University Press (1994).
21. Treadway WL. A report of the departmental committee on morphine and heroin addiction to the British ministry of health. Public Health Rep. (1929) 44:1995–2000. doi: 10.2307/4579355
22. Seddon T. Prescribing heroin: john marks, the merseyside clinics, and lessons from history. Int J Drug Policy. (2020) 78:102730. doi: 10.1016/j.drugpo.2020.102730
23. Dennis F. Advocating for diamorphine: cosmopolitical care and collective action in the ruins of the ‘old British system.’. Crit Public Health. (2021) 31:144–55. doi: 10.1080/09581596.2020.1772463
24. Metrebian N, Carnwath T, Stimson GV, Storz T. Survey of doctors prescribing diamorphine (heroin) to opiate-dependent drug users in the United Kingdom. Addiction. (2002) 97:1155–61. doi: 10.1046/j.1360-0443.2002.00193.x
25. Gregory A. Saved from a horrible fate’: Legal heroin prescribed to hundreds of UK drug users, figures reveal. (2019). Available online at: https://www.independent.co.uk/news/uk/home-news/heroin-addiction-diamorphine-treatment-british-system-hat-leap-harm-reduction-a9061556.html (accessed December 20, 2021)
26. Diamorphine. British Electronic Medicines Compendium. (2020). Available online at: https://www.medicines.org.uk/emc/search?q=%22Diamorphine%22 (accessed December 10, 2020)
27. Amtsdruckschriften. Bundesgesetz betreffend Betäubungsmittel (Vom 2. Oktober 1924). (2022). Available online at: https://www.amtsdruckschriften.bar.admin.ch/viewOrigDoc.do?id=10029167 (accessed January 17, 2022)
28. SR 812.121. Federal Act of 3 October 1951 on Narcotics and Psychotropic Substances (Narcotics Act, NarcA). (2021). Available online at: https://www.fedlex.admin.ch/eli/cc/1952/241_241_245/en (accessed December 21, 2021)
29. Harm Reduction International. The Global State of Harm Reduction. (2020). Available online at: https://www.hri.global/files/2021/03/04/Global_State_HRI_2020_BOOK_FA_Web.pdf (accessed September 28, 2021)
30. Art. 23 of the 1961 Single Convention (SR 0.812.121.0). (1961). Available online at: https://www.fedlex.admin.ch/eli/cc/1970/802_803_802/de#art_23
31. International Narcotics Control Board. Narcotic Drugs Report 2020: Part II Comments on the reported statistics on narcotic drugs. New York, NY: United Nations (2021). Available online at: https://www.incb.org/documents/Narcotic-Drugs/Technical-Publications/2020/6_NAR_2020_Part_II_Comments_E.pdf (accessed February 8, 2022)
32. International Narcotics Control Board. Narcotic Drugs Report 2020: Part III Supply and Demand. New York, NY: United Nations (2020).
33. PubChem. Heroin. (2020). Available online at: https://pubchem.ncbi.nlm.nih.gov/compound/5462328 (accessed December 10, 2020).
34. Merves ML, Goldberger BA. Heroin. 2nd ed. In: P Worsfold, A Townshend, C Poole editors. Encyclopedia of Analytical Science. Oxford: Elsevier (2005). p. 260–6. doi: 10.1016/B0-12-369397-7/00456-8
35. Oye KA, Lawson JCH, Bubela T. Drugs: Regulate “home-brew” opiates. Nat News. (2015) 521:281. doi: 10.1038/521281a
36. DeLoache WC, Russ ZN, Narcross L, Gonzales AM, Martin VJJ, Dueber JE. An enzyme-coupled biosensor enables (S)-reticuline production in yeast from glucose. Nat Chem Biol. (2015) 11:465–71. doi: 10.1038/nchembio.1816
37. Fossati E, Ekins A, Narcross L, Zhu Y, Falgueyret J-P, Beaudoin GAW, et al. Reconstitution of a 10-gene pathway for synthesis of the plant alkaloid dihydrosanguinarine in Saccharomyces cerevisiae. Nat Commun. (2014) 5:3283. doi: 10.1038/ncomms4283
38. Fossati E, Narcross L, Ekins A, Falgueyret J-P, Martin VJJ. Synthesis of Morphinan Alkaloids in Saccharomyces cerevisiae. PLoS One. (2015) 10:e0124459. doi: 10.1371/journal.pone.0124459
39. Beaudoin GAW. Characterization of Oxidative Enzymes Involved in the Biosynthesis of Benzylisoquinoline Alkaloids in Opium Poppy (Papaver somniferum). Calgary: University of Calgary (2015). doi: 10.11575/PRISM/25284
40. Hawkins KM, Smolke CD. Production of benzylisoquinoline alkaloids in Saccharomyces cerevisiae. Nat Chem Biol. (2008) 4:564–73. doi: 10.1038/nchembio.105
41. Thodey K, Galanie S, Smolke CD. A microbial biomanufacturing platform for natural and semisynthetic opioids. Nat Chem Biol. (2014) 10:837–44. doi: 10.1038/nchembio.1613
42. Bradsher K. Shake-Up on Opium Island. New York, NY: The New York Times (2014). Available online at: https://www.nytimes.com/2014/07/20/business/international/tasmania-big-supplier-to-drug-companies-faces-changes.html (accessed February 10, 2022)
43. Scholten W, Christensen A-E, Olesen AE, Drewes AM. Analyzing and Benchmarking Global Consumption Statistics for Opioid Analgesics 2015: Inequality Continues to Increase. J Pain Palliat Care Pharmacother. (2020) 34:1–12. doi: 10.1080/15360288.2019.1686098
44. FDA. Drug Shortages: Root Causes and Potential Solutions. (2019). Available online at: https://www.fda.gov/media/131130/download (accessed December 15, 2020)
45. Schweizer Verein der Amts- und Spitalapotheker (GSASA). Empfehlungen zum Umgang mit Lieferengpässen. (2012). Available online at: https://www.gsasa.ch/de/aktivitaeten/oekonomie-versorgung/lieferengpaesse/?oid=10143&lang=de (accessed February 10, 2022)
46. INCB Dataset. Heroin Manufacture, Consumption, Stock, Imports, Exports 2000-2019. Vienna: INCB (2000-2019).
47. Bundesinstitut für Arzneimittel und Medizinprodukte. Diaphin (Reg. Nr. 62906.00.00)- Arzneimittel-Informationssystem. (2022). Available online at: https://portal.dimdi.de/amguifree/am/docoutput/jpadocdisplay.xhtml (accessed February 4, 2022).
48. Danish Medicines Agency. Diaphin (D.SP.NR. 26898) - Produktresumé. (2022). Available online at: http://produktresume.dk/AppBuilder/search?utf8=%E2%9C%93&id=&type=&q=Diaphin&button=S%C3%B8g (accessed February 4, 2022)
49. SR 232.14 Bundesgesetz vom 25. Juni 1954 über die Erfindungspatente (Patentgesetz, PatG) (Stand am 1. April 2019). (2021). Available online at: https://www.fedlex.admin.ch/eli/cc/1955/871_893_899/de (accessed December 21, 2021)
50. Art. 14 PatG (SR 232.14). (2019). Available online at: https://www.fedlex.admin.ch/eli/cc/1955/871_893_899/en#art_14 (accessed April 1, 2019)
51. Wright CRA. XLIX—On the action of organic acids and their anhydrides on the natural alkaloïds. Part I. J Chem Soc. (1874) 27:1031–43. doi: 10.1039/JS8742701031
52. SR 812.21. Federal Act of 15 December 2000 on Medicinal Products and Medical Devices (Therapeutic Products Act, TPA). (2021). Available online at: https://www.fedlex.admin.ch/eli/cc/2001/422/en (accessed December 21, 2021)
53. Art. 11a TPA (SR 812.21). (2022). Available online at: https://www.fedlex.admin.ch/eli/cc/2001/422/en#art_11_a (accessed January 1, 2022)
54. Art. 12 para. 1 let. b TPA (SR 812.21). (2022). Available online at: https://www.fedlex.admin.ch/eli/cc/2001/422/en#art_12 (accessed January 1, 2022)
55. Art. 11b para. 1 TPA (SR 812.21). (2022). Available online at: https://www.fedlex.admin.ch/eli/cc/2001/422/en#art_11_b (accessed January 1, 2022)
56. Swissmedic. Lists and directories; 1.7 Important medicinal products for rare diseases (orphan drugs in the case of human medicines). (2021). Available online at: https://www.swissmedic.ch/dam/swissmedic/en/dokumente/internetlisten/status_orphandrug_ham.xlsx.download.xlsx/Liste_OrphanDrug_Internet.xlsx (accessed December 20, 2021)
57. Art. 11b para. 4 TPA (SR 812.21). (2022). Available online at: https://www.fedlex.admin.ch/eli/cc/2001/422/en#art_11_b (accessed January 1, 2022)
58. Art. 8 para. 5 NarcA (SR 812.121). (2021). Available online at: https://www.fedlex.admin.ch/eli/cc/1952/241_241_245/en#art_8 (accessed May 15, 2021)
59. Art. 8 para. 7 NarcA (SR 812.121). (2021). Available online at: https://www.fedlex.admin.ch/eli/cc/1952/241_241_245/en#art_8 (accessed May 15, 2021)
60. Art. 5 para. 1 let. a BetmKV (SR 812.121.1). (2022). Available online at: https://www.fedlex.admin.ch/eli/cc/2011/362/de#art_5 (accessed January 1, 2022)
61. Swissmedic. Information von BAG, Swissmedic und Kantonsapothekervereinigung zu zugelassenen Arzneimitteln, die kontrollierte Substanzen des Verzeichnisses d enthalten. (2014). Available online at: https://www.swissmedic.ch/dam/swissmedic/de/dokumente/bewilligungen/btm/information_von_bagswissmedicundkantonsapothekervereinigung zuzug.pdf.download.pdf/information_von_bagswissmedicundkantonsapothe kervereinigungzuzug.pdf (accessed December 21, 2021)
62. Swissmedic. Betriebsbewilligung zum Umgang mit kontrollierten Substanzen (Art. 2 Bst. h BetmKV), Liste der Betriebsstandorte Stand: 13.12.2021. (2021). Available online at: https://www.swissmedic.ch/dam/swissmedic/de/dokumente/internetlisten/betriebsbewilligungzumumgangmitkontrollier tensubstanzenart2bsthb.xlsx.download.xlsx/betriebsbewilligungzumumgang mitkontrolliertensubstanzenart2bsthb.xlsx (accessed December 21, 2021)
63. Fedlex. Verordnung über die Meldestelle für lebenswichtige Humanarzneimittel vom 12. August 2015. (2021). Available online at: https://www.fedlex.admin.ch/eli/cc/2015/544/de (accessed September 16, 2021)
64. Opium Derivatives. Government response to OFT review of undertakings by Macfarlan Smith Limited (MSL). (2006). Available online at: https://webarchive.nationalarchives.gov.uk/20090609050344/http://www.berr.gov.uk/files/file33800.pdf (accessed December 10, 2020)
65. Wickware C. NHS trusts forced to use “expensive” pre-filled diamorphine syringes to manage ongoing supply issues. (2022). Available online at: https://pharmaceutical-journal.com/article/news/nhs-trusts-forced-to-use-expensive-pre-filled-diamorphine-syringes-to-manage-ongoing-supply-issues (accessed February 15, 2022).
66. PSNC. Medicine Supply Notification: Diamorphine 5mg and 10mg powder for solution for injection ampoules - Updated. (2022). Available online at: https://psnc.org.uk/our-news/medicine-supply-notification-diamorphine-5mg-powder-for-solution-for-injection-ampoules/ (accessed February 15, 2022).
67. SEHD. Medicine Supply Alert Notice Diamorphine Hydrochloride powder for reconstitution and injection 5mg & 10mg ampoules. (2022). Available online at: https://www.sehd.scot.nhs.uk/publications/MSAN(2020)10update.pdf (accessed February 15, 2022)
68. Praxis-suchtmedizin. Update Lieferunterbrechung von Sevre-Long§. (2022). Available online at: https://www.praxis-suchtmedizin.ch/praxis-suchtmedizin/index.php/de/heroin/srom-sevre-long-kapanol (accessed January 18, 2022)
69. Bundesamt für wirtschaftliche Landesversorgung (BWL). Aktuelle Versorgungsstörungen, Versorgungsenpässe Arzneimittel (14.02.2022). (2022). Available online at: https://www.bwl.admin.ch/bwl/de/home/themen/heilmittel/meldestelle/aktuelle_versorgungsstoerungen.html (accessed February 16, 2022)
70. Parlament. Bericht der Kommission für soziale Sicherheit und Gesundheit des Nationalrats vom 5. November 2020: 19.465 Volksapotheke zur Sicherung der Versorgung der Bevölkerung mit Medikamenten und Impfstoffen. (2022). Available online at: https://www.parlament.ch/centers/kb/Documents/2019/Kommissionsbericht_SGK-N_19.465_2020-11-05.pdf (accessed February 21, 2022)
71. Oviedo-Joekes E, Guh D, Brissette S, Marsh DC, Nosyk B, Krausz M, et al. Double-blind injectable hydromorphone versus diacetylmorphine for the treatment of opioid dependence: a pilot study. J Substance Abuse Treat. (2010) 38:408–11. doi: 10.1016/j.jsat.2010.03.003
72. Oviedo-Joekes E, Guh D, Brissette S, Marchand K, MacDonald S, Lock K, et al. Hydromorphone compared with diacetylmorphine for long-term opioid dependence: a randomized clinical trial. JAMA Psychiatry. (2016) 73:447–55. doi: 10.1001/jamapsychiatry.2016.0109
73. Steffen T, Berthel T, Zimmer A, Gutzwiller F, Uchtenhagen A. Die Entwicklung der psychischen Gesundheit in der heroingestützten Behandlung - Ergebnisse aus der schweizerischen Studie PROVE. Suchttherapie. (2000) 1:27–33. doi: 10.1055/s-2000-13255
Keywords: diamorphine, Switzerland, market, manufacturing, shortages
Citation: Schmitt-Koopmann C, Baud C-A, Junod V and Simon O (2022) Switzerland’s Dependence on a Diamorphine Monopoly. Front. Psychiatry 13:882299. doi: 10.3389/fpsyt.2022.882299
Received: 23 February 2022; Accepted: 11 April 2022;
Published: 09 May 2022.
Edited by:
Kenneth Michael Dürsteler, University Psychiatric Clinic Basel, SwitzerlandReviewed by:
Luis Falcato, Arud Centre for Addiction Medicine, SwitzerlandMaximilian Meyer, University Psychiatric Clinic Basel, Switzerland
Daniel Ciccarone, University of California, San Francisco, United States
Copyright © 2022 Schmitt-Koopmann, Baud, Junod and Simon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Caroline Schmitt-Koopmann, Y2Fyb2xpbmUuc2NobWl0dEBjaHV2LmNo