
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 13 April 2022
Sec. Psychopathology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.874183
This article is part of the Research Topic Violent Relationships: Acute and Long-term Implications View all 8 articles
 Freya Thiel1,2†
Freya Thiel1,2† Verena C. S. Büechl1,2†Franciska Rehberg1,2Amera Mojahed1
Verena C. S. Büechl1,2†Franciska Rehberg1,2Amera Mojahed1 Judith K. Daniels3,4
Judith K. Daniels3,4 Julia Schellong5
Julia Schellong5 Susan Garthus-Niegel1,2,6*
Susan Garthus-Niegel1,2,6*Background: To contain the spread of COVID-19, governmental measures were implemented in many countries. Initial evidence suggests that women and men experience increased anger and aggression during COVID-19 lockdowns. Not surprisingly, media reports and initial empirical evidence highlight an increased risk for domestic violence (DV) during the pandemic. Nonetheless, a systematic review of studies utilizing participants' reports of potential changes in DV prevalence and severity during the pandemic as compared to pre-pandemic times is needed.
Objective: To examine empirical, peer-reviewed studies, pertaining to the potential change in prevalence and severity of different types of DV during the COVID-19 pandemic, as reported by study participants.
Data Sources: Electronic EMBASE, MEDLINE, PsycINFO, and CINAHL searches were conducted for the period between 2020 and January 5, 2022. References of eligible studies were integrated by using a snowballing technique.
Study Selection: A total of 22 primary, empirical, peer-reviewed studies published in English or German were included.
Results: Of the 22 studies, 19 were cross-sectional whereas 3 included both pre-pandemic and during pandemic assessments. Data synthesis indicates that severity of all types of DV as well as the prevalence of psychological/emotional and sexual DV increased for a significant number of victims in the general population during the pandemic. Evidence for changes in prevalence regarding economic/financial, physical, and overall DV remains inconclusive. There was considerable between-study variation in reported prevalence depending on region, sample size, assessment time, and measure.
Conclusions: Data synthesis partly supports the previously documented increase in DV. Governmental measures should consider the availability of easily accessible, anonymous resources. Awareness and knowledge regarding DV need to be distributed to improve resources and clinical interventions.
In order to contain the global spread of COVID-19, measures such as social isolation/distancing, quarantine, and stay-at-home orders have been implemented in many countries (1, 2). Although effective in decelerating the spread of COVID-19 (3, 4), these measures also have major social consequences, which may have a substantial impact on mental health, wellbeing, and life satisfaction (5, 6). Empirical research pertaining to mental health during the COVID-19 pandemic indicates increased levels of anxiety, depression, insomnia, and psychological distress (7). Feelings of loneliness resulting from measures such as social isolation or stay-at-home orders, may not only lead to an increase in depressive symptoms (8), but may also impair self-regulation abilities (9), which can lead to dysfunctional behavioral patterns, such as alcohol and drug abuse (10, 11), as well as violent behavior (12). Initial evidence suggests that during the first COVID-19 lockdown in Germany, both women and men experienced increased anger and aggression and tended to direct their anger at others (13). Over the course of the pandemic, media reports have highlighted an alarming increase in rates of domestic violence among intimate partners and against children during lockdown periods (14–16) and web searches related to support for domestic abuse have expanded since the beginning of the pandemic (17).
Domestic violence (DV) is defined as “a pattern of behavior that is used to gain or maintain power and control over an intimate partner in a relationship, a child, another relative or any other household member” (18). DV may affect anyone, regardless of age, gender, ethnic or socioeconomic background, religious or sexual orientation, or type of relationship (18, 19). To this end, DV can also include intimate partner violence (IPV). According to the World Health Organization (WHO), IPV pertains to “any act or behavior within a present or former intimate relationship that causes physical, psychological, or sexual harm” (20). Among others, these behaviors may include (a) psychological/emotional or verbal violence (e.g., insulting, threatening, humiliating), (b) sexual violence (e.g., forced sexual intercourse), (c) physical violence (e.g., beating, kicking), (d) economic/financial violence (20, 21).
Reports on DV or IPV have largely focused on violence committed against women. To this end, it has been documented that globally one in three women will experience physical or sexual violence committed by an intimate partner during her life (20), making IPV the most common form of violence against women. Nonetheless, public, empirical, and clinical attention toward DV or IPV against men has grown. Similar to violence against women, it is estimated that one in four men will experience physical violence by an intimate partner during his life (22–25). As described above, governmental restrictions to slow down the spread of COVID-19, such as social isolation, have been linked to increased anger and aggression (13), which may in turn increase the risk for DV victimization and/or perpetration. Finally, a recent review documents that both social and geographic isolation represent crucial risk factors for IPV (1).
Despite the positive effects of governmental restrictions on containment of the virus, these measures also deteriorated conditions for victims of DV, finding them trapped at home with their perpetrators and minimizing their access to social support systems like friends and family outside the abusive relationship (15, 26). Further, stay-at-home orders and lockdowns might make it easier for perpetrators to socially isolate and surveil their victim, which may be used to control intimate partners or family members (26). Thus, during the pandemic, the risk of DV may have increased because of domestic confinement with possible perpetrators, while at the same time access to private and public help resources such as protection services has been limited (2, 15, 26). Regional and societal factors may further impact victims' and perpetrators' access to help resources. For instance, in many settings around the world, patriarchal views of the family, social norms, or geographical distance from professional and private support resources may offer potential explanations for the increased risk of IPV (1, 27–29).
Although worldwide media reports suggest increasing rates of DV over the course of the pandemic (14–16) and initial empirical evidence highlights that social and geographical isolation may augment DV (1), empirical studies pertaining to a potential increase in DV cases or severity during the pandemic had to be designed, conducted, and had to undergo rigorous peer-review processes before publication. Since the global onset of the COVID-19 pandemic in March 2020, the amount of empirical, peer-reviewed studies has grown.
To date, several reviews focusing on a change in DV prevalence are available. First, an initial systematic review of 32 studies published until July 2020 documented evidence for an increase in DV cases, specifically during the first week of COVID-19 lockdowns in various countries. Nonetheless, this review was conducted in the early stages of the pandemic—thus, the majority of included studies reported on police or helpline reports to assess DV prevalence and not all included reports and studies had been peer-reviewed (30). Second, a systematic review and meta-analysis of 18 studies published until January 2021 focused exclusively on administrative/official data (e.g., police records), documenting an increase in DV following stay-at-home orders or lockdown, with the majority of studies stemming from the U.S. (31). Third, a systematic review focused solely on IPV, including 19 studies, eight of which focused on reports by victims and 11 on reports by help professionals (i.e., police officers, DV resource center staff, healthcare providers). Results outlined an increase in the episodes of IPV as reported by victims (i.e., cross-sectional studies) and help professionals (32). Fourth, a systematic review focusing on IPV as well as sexual functioning during the COVID-19 pandemic included 11 cross-sectional studies published until the end of 2020, 5 of which reported on IPV. The authors showed that IPV against women increased during the COVID-19 pandemic (33). Taken together, all prior reviews suggest an increase in DV during the pandemic. It should however be noted that prior reviews were limited by the timing of literature and it can be assumed that additional literature has been published since. Further, initial research primarily focused on administrative/official reports to assess a potential change in DV during the COVID-19 pandemic. Nevertheless, initial studies focusing on administrative/official reports may reflect changes in help-seeking behavior rather than changes in prevalence, highlighting the importance for empirical studies assessing participants.
We therefore set forth to examine empirical, peer-reviewed studies reporting on original participant data regarding a change in the prevalence and/or severity of DV over the course of the pandemic as compared to pre-pandemic times. Given the acute nature of the topic and the time needed to plan, conduct, and publish relevant data, we expected the majority of studies to have employed cross-sectional designs. Nonetheless, we also expected initial evidence from longitudinal studies or those with repeated pre-pandemic and during pandemic assessments to be available by the time of the current literature search.
In order to examine the research question of whether there was a change in DV prevalence and/or severity during the COVID-19 pandemic as compared to pre-pandemic times, we followed the PRSIMA (34) approach: Electronic EMBASE, MEDLINE, PsycINFO, and CINAHL searches were conducted from 2020 to January 5, 2022 to identify research articles for inclusion in this review. Separate searches for each primary database combined terms relating to DV and the COVID-19 pandemic, applying the Boolean operators (AND) and (OR), accordingly. For MEDLINE, PsycINFO, and CINAHL searches, we used the search string “TI (domestic OR intimate OR interpersonal OR partner OR marital OR couple OR relationship) AND TI (violence or abuse) AND TI (covid* OR pandemic OR corona)”. For EMBASE, the string was adapted to “((domestic OR interpersonal OR intimate OR partner OR marital OR couple OR relationship) AND (violence OR abuse) AND (covid OR pandemic OR corona)).ti.”. Additionally, references of eligible studies were integrated by using a snowballing technique.
For inclusion in this review, we considered primary, peer-reviewed, empirical studies pertaining to a potential change in DV prevalence and/or severity during the COVID-19 pandemic as reported by participants, published in English or German. Studies examining participant-reported violence in a domestic context during the pandemic, including different age groups, genders, and any form of intimate relationship (e.g., intimate partner, relationship, marital or couple violence, violence against children in the household) were incorporated. Thus, studies utilizing official records (e.g., police, helpline, or hospital records) without participant assessment were excluded in order to focus specifically on the potential change in DV prevalence rather than a change in help-seeking behavior. Empirical quantitative studies, such as cross-sectional, longitudinal, and clinical studies, published in peer-reviewed journals were included. Qualitative studies, conference abstracts, case studies, and dissertations/theses with a peer-reviewed published version were excluded.
All studies identified through the database searches were imported into the systematic review tool Rayyan QRCI (35). Titles and abstracts were screened by two reviewers (VCSB and FR). Studies which did not meet eligibility criteria were excluded. In case of any uncertainties, a third reviewer (FT) was consulted. Subsequently, full texts were reviewed by the same reviewers as above (VCSB and FR) and screened for final inclusion in the current review. Again, a third reviewer (FT) was consulted in case of insecurities. Included studies were then retained for data extraction.
Studies identified for inclusion in the current review were assessed for risk of bias using the JBI critical appraisal checklist for prevalence studies (36). It includes nine appraisal criteria pertaining to the appropriateness of a study's (1) target population (i.e., sample frame addresses target population), (2) recruitment method (i.e., appropriate to recruit representative sample), (3) sample size (i.e., power calculation provided), (4) description of subjects and setting (i.e., sufficient detail on sample and setting), (5) data analyses (i.e., sufficient coverage of all subgroup samples), (6) measurement validity (i.e., validated measure used to assess DV), (7) measurement reliability (i.e., DV measured in same way for all participants), (8) statistical analyses (i.e., significance test for change in DV prevalence/severity), and (9) response rate. The full checklist and a detailed description of appraisal criteria are available at https://jbi.global/critical-appraisal-tools. After a pilot trial on one included study to ensure feasibility of the JBI checklist for the current purpose, each study was assessed for risk of bias by two independent reviewers (FT and VCSB/FR). Initial inter-rater agreement was high (93%) and disagreements were discussed to reach consensus. Of the nine checklist criteria, appropriateness of the sample size as well as measurement validity and reliability were considered particularly relevant for the current review and thus defined as major domains. Overall, we considered a study to present low risk of bias if at least five of the JBI checklist criteria were fulfilled, including at least one of the three major domains.
Results were synthesized narratively and in tabular form. Studies on DV prevalence can be expected to exhibit high heterogeneity pertaining to target population as well as conceptualization and assessment of violence. We therefore did not conduct any quantitative analyses for this review. Data from identified studies were tabulated in a data extraction form developed by FT and VCSB. With the help of AM, data pertaining to author and year of publication, country, setting (e.g., clinical or population-based) and study period (i.e., time point of COVID-19 pandemic), study design, sample size and characteristics (e.g., final sample, target population, age, gender), measure used to assess DV (e.g., validated measure, self-generated questions), direction of DV (i.e., victimization, perpetration), DV prevalence estimates, and type of DV (i.e., psychological/emotional or verbal, sexual, physical, economic/financial) were extracted. Further, results from risk of bias assessments were visualized and synthesized in tabular form.
Electronic EMBASE, MEDLINE, PsycINFO, and CINAHL searches revealed a total of 521 studies. After exclusion of duplicates, titles and abstracts of 262 studies were screened. Based on title/abstract screening, 171 studies were discarded. The remaining 91 studies were retained for full-text screening. Based on full-text screening, 69 studies were excluded because they did not fulfill the eligibility criteria outlined above. Hence, the screening process resulted in the identification and inclusion of 22 studies (13, 37–57). An overview of the study selection process is provided in Figure 1.
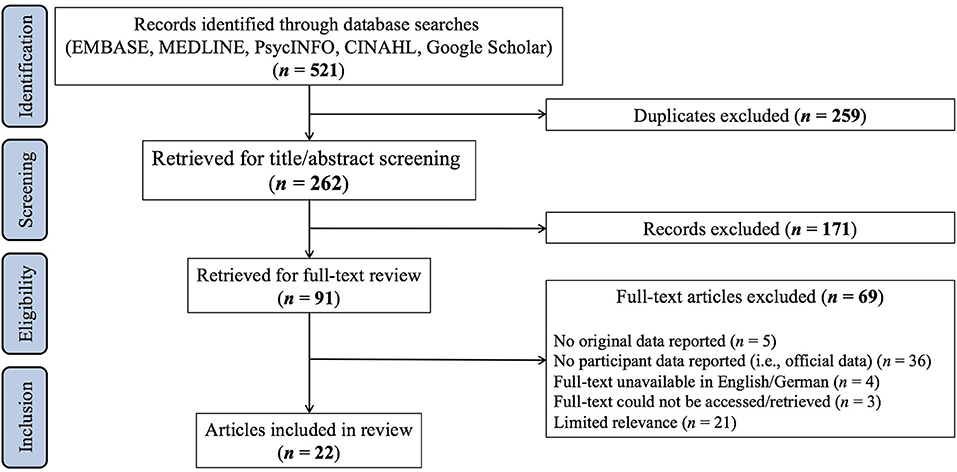
Figure 1. Study selection process.
All 22 studies were written in English and published between October 2020 and December 2021, with n = 3 published in 2020 and n = 19 published in 2021. The studies originated from various countries, with the majority coming from the U.S. (n = 4), followed by India (n = 3), Germany (n = 2), and Bangladesh (n = 2). Further studies in this review were conducted in Austria, the Czech Republic, Egypt, Ethiopia, Iraq, Jordan, Nigeria, Peru, Saudi Arabia, Switzerland, and Tunisia. Ten studies included only females (37, 41–43, 46–49, 51, 54), 10 further studies included both female and male participants (13, 39, 44, 45, 50, 52, 53, 55–57), and two studies assessed DV in males only (38, 40). Without exception, all studies reported on DV against adults, with only one study further reporting on violence against children (55). Most studies were cross-sectional (n = 19) (13, 37–54), while only few longitudinal studies or studies with repeated pre-pandemic and during pandemic assessments were identified (n = 3) (55–57) (see Table 1).
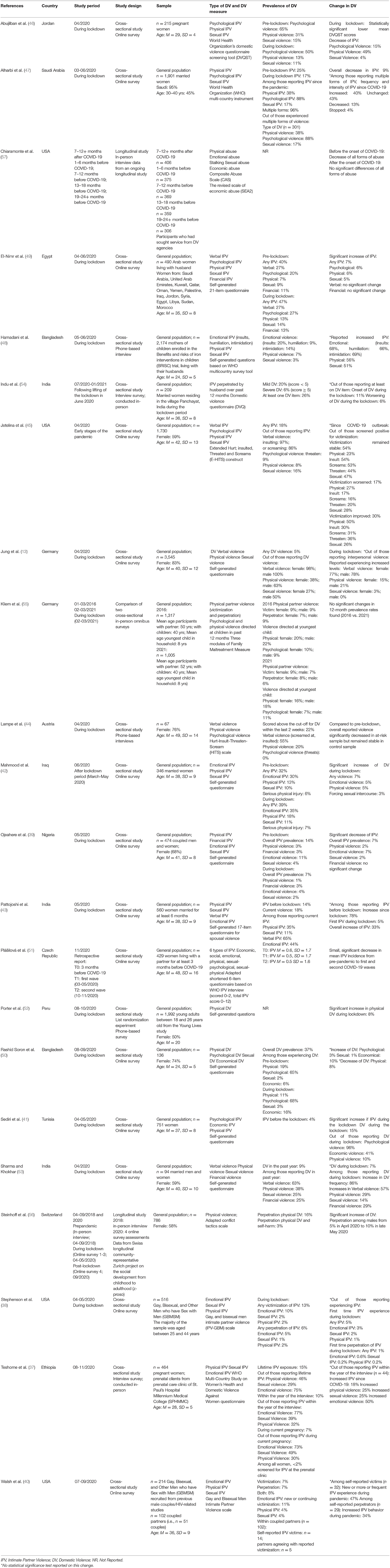
Table 1. Study characteristics.
The majority of the n = 19 cross-sectional studies assessed different types of DV. To this end, 12 studies reported on changes in psychological/emotional or verbal DV (13, 37–40, 42, 45, 46, 48–50, 53), 11 on sexual DV (13, 37–39, 42, 45, 46, 48–50, 53), 12 reported on physical DV (13, 37–39, 42, 45, 46, 48–50, 52, 53), and 4 included economic/financial DV (39, 49, 50, 53). One study did not provide a differentiation of DV type (54). All cross-sectional studies included participant report on DV victimization, whereas two studies further included assessment of DV perpetration (38, 40). Most cross-sectional studies investigated DV in the general population (n = 14) (13, 39, 41–43, 45, 47–54), while some studies focused on specific samples (n = 5) (37, 38, 40, 44, 46). Assessment of DV was heterogeneous regarding the methodological approach—five studies used validated questionnaires [i.e., (Extended-) Hurt, Insult, Threaten, Scream Scale [(E-)HITS]; Composite Abuse Scale Revised Short Form (CASR-SF); Domestic Violence Questionnaire (DVQ); Gay and Bisexual Men Intimate Partner Violence scale (IPV-GBM)] (38, 40, 44, 45, 54), nine studies relied on self-generated questions (13, 39, 41–43, 49, 50, 52, 53), five studies used scales from the “WHO Multi-Country Study on Women's Health and Domestic Violence Against Women” (37, 47), the “World Health Organization's Domestic Violence Questionnaire Screening Tool” (46), or DV self-generated questionnaires based on questionnaires developed by the WHO (48, 51). Further, the majority utilized online surveys (n = 14) (13, 38–43, 45–47, 49–51, 53), whereas some studies conducted in-person (n = 2) (37, 54) or telephone interviews (n = 3) (44, 48, 52).
Compared to the numerous cross-sectional studies, studies with repeated pre-pandemic and during pandemic assessments were still scarce at the time of literature search for the current review. Three empirical, peer-reviewed studies were identified. Of these, two employed longitudinal designs (56, 57) and one compared two representative population surveys from 2016 to 2021 (55). Two studies utilized samples from the general population in Germany and Switzerland (55, 56), with one solely focusing on perpetration of physical DV but not victimization (56), and the other focusing on victimization and perpetration of physical IPV and perpetration of physical and psychological/emotional violence against children in the household (55). The third study was conducted in the U.S. and focused specifically on DV survivors in precarious or unstable housing conditions (57). While two studies conducted in-person interviews at all measurement points (55, 57), one study supplemented pre-pandemic interviews with data collected via online surveys during the pandemic (56).
Of the 22 studies, half were rated as having high risk of bias (13, 37, 39, 41–43, 45, 48, 50, 53, 55) and half were rated as having low risk of bias (38, 40, 44, 46, 47, 49, 51, 52, 54, 56, 57). The distribution of ratings on each of the nine JBI checklist criteria (36) can be found in Figure 2. Participant recruitment was rated as holding high risk of bias for 13 of the included studies. This risk of bias mostly pertained to potential selection bias given recruitment for online surveys using snowballing sampling and/or survey distribution via various (social) media sites. Sample size was rated as holding low risk of bias only if a power analysis was provided by the original authors and an appropriate sample size was reached. More than half of the included studies (n = 12) did not report a power calculation and were consequently rated as “unclear”. Measurement validity was assessed based on the utilization of a generally validated DV measure, without guaranteeing the instrument's validation for use in specific populations or validation of specific translated or adapted versions. Consequently, risk of bias pertaining to measurement validity was rated as low for 11 of the included studies. Although some of the included cross-sectional studies utilizing online surveys reported how many individuals accessed their survey in comparison to the number of completed surveys, an actual response rate cannot be provided—for these studies, the response rate criterion was thus not applicable. Further, because some studies only reported a change in DV prevalence and/or severity in a descriptive manner and did not provide tests of statistical significance for change estimates, 10 of the included studies were rated as holding high risk regarding the statistical analysis criterion. Risk of bias assessment by JBI checklist items for each included study can be found in Supplementary Table S1.
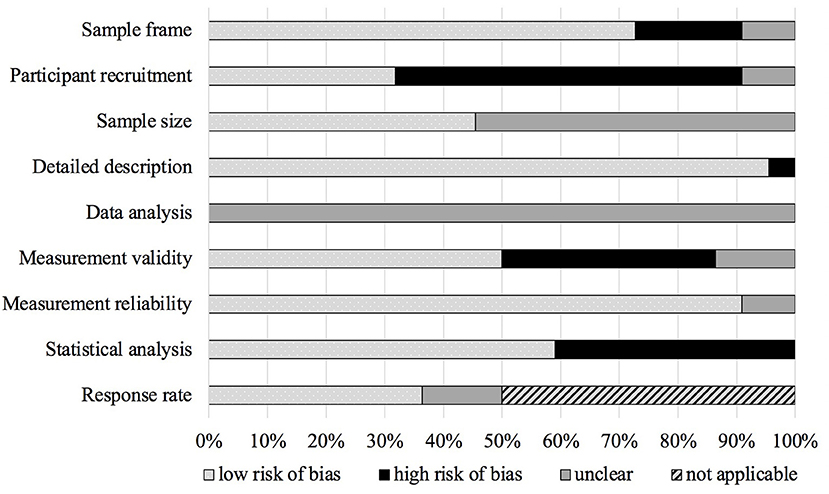
Figure 2. Risk of bias of included studies with percentages of ratings on JBI checklist.
Without exception, all cross-sectional as well as two of the three studies with longitudinal/repeated pre-pandemic and during pandemic assessments reported on changes in DV in the context of victimization (for reports pertaining to DV perpetration, please refer to Section Perpetration of Violence). In the following, we will report results pertaining to changes in each type of DV (i.e., psychological/emotional or verbal, sexual, physical, economic/financial) and changes in overall DV. In each section, we will first present results from studies with longitudinal/repeated pre-pandemic and during pandemic assessments, followed by results from cross-sectional studies. For cross-sectional studies, we will first focus on the change in prevalence and the change in severity in samples from the general population, followed by studies utilizing specific samples. As outlined in the introduction, some studies investigated IPV, which we here conceptualize as a specific type of DV (n = 14). We will therefore refer to either IPV or DV depending on the particular focus of the original study.
Prevalence of current psychological/emotional or verbal violence varied widely across studies, depending on region, sample size, assessment time, and assessment measure. Only one longitudinal study investigated psychological/emotional violence. Chiaramonte et al. (57) used data from an ongoing longitudinal study in the U.S. to examine the impact of the COVID-19 stay-at-home order (March 15, 2020) on DV survivors who had sought service from DV agencies and were currently in precarious or unstable housing conditions. Five in-person interviews were conducted every 6 months over a 2-year period, assessing psychological/emotional violence via the Composite Abuse Scale (CAS). In this specific sample of DV survivors, there was a significant decrease in psychological/emotional DV in the 24 months prior to the onset of the COVID-19 pandemic—thus, since seeking help from a DV agency. No significant changes were found after the onset of the pandemic (57).
Among the n = 10 cross-sectional studies reporting on psychological/emotional DV, n = 6 studies reported a specific change in psychological/emotional DV prevalence or severity compared to pre-pandemic levels in samples from the general population (39, 42, 45, 48–50), with three studies documenting an increase in overall prevalence and one study documenting a decrease. Two studies reported a significant increase in psychological/emotional DV between 5 and 6% during or after the first lockdown in samples of 346 married women in the Kurdistan region of Iraq (42) and 490 Arab women from 14 different countries (see Table 1) (49). An additional study reported an increase of 3% in a sample of 136 Bangladeshi females and males, but did not report a significance test for this potential increase (50). In contrast, Ojeahere et al. reported a decrease of 7% in a Nigerian sample of 474 female and male participants during the first lockdown using self-generated questions in an online survey (39). All four studies utilized self-generated questions to assess DV via online surveys (39, 42, 49, 50).
Regarding a change in severity, two cross-sectional studies specifically reported on changes in psychological/emotional violence among those experiencing DV in samples from the general population (45, 48). To this end, Hamadani et al. differentially examined insults, humiliation, and intimidation as specific types of psychological/emotional IPV via telephone interviews in a sample of 2,174 mothers in Bangladesh, recruited from a study in which their children were enrolled. Of those reporting IPV, 68, 66, and 69% reported insults, humiliation, and intimidation to have increased during the first lockdown, respectively (48). Additionally, Jetelina et al. found that among those reporting psychological/emotional IPV in an online survey of 1,730 female and male participants in the U.S., 20% reported violence to have worsened since the COVID-19 outbreak, whereas 36% reported violence to have improved, and 44% reported violence to not have changed (45).
Further, n = 4 cross-sectional studies focused on specific populations, namely currently pregnant women in Ethiopia (37) and Jordan (46), as well as gay, bisexual, and other men who have sex with men (GBMSM) in the U.S. (38, 40). Regarding psychological/emotional DV among pregnant women, Abujilban et al. reported a 15% decrease during the first lockdown in an Jordanian sample of 215 pregnant women when using the World Health Organization's Domestic Violence Questionnaire Screening Tool (DVQST) in an online survey (46). Conversely, using in-person interviews, Teshome et al. documented that among those reporting IPV within the last year (i.e., 2020) in their sample of 464 pregnant Ethiopian women, half the women reported psychological/emotional violence to have increased after the COVID-19 outbreak (37). Regarding psychological/emotional DV among gay, bisexual, and other men who have sex with men (GBMSM) in the U.S., using the Gay, and Bisexual Men Intimate Partner Violence Scale in an online survey, Walsh et al. documented that out of those reporting psychological/emotional IPV, 11% reported experiencing new or more frequent psychological/emotional IPV during the pandemic (40). Further, Stephenson et al. report that 1% of the 516 men in their sample indicated having experienced psychological/emotional violence for the first time during the first lockdown (38).
In addition, n = 4 cross-sectional studies reported a specific change in verbal DV prevalence to pre-pandemic levels in the general population (13, 45, 49, 53). To this end, two studies indicated verbal DV among 3,545 females and males in Germany (13) and 94 females and males in India (53) who reported experiencing IPV or DV to have increased by 57–78% during the first lockdown. Both studies relied on self-generated questions to assess verbal IPV/DV in online surveys (13, 53). Jetelina et al., however, documented that among those reporting verbal IPV in an online survey of 1,730 female and male participants in the U.S., 17% reported violence to have worsened since the COVID-19 outbreak, whereas 31% reported violence to have improved, and 54% reported violence to not have changed (45). In contrast, El-Nimr et al. found no significant change in verbal IPV during the first lockdown in a sample of 490 Arab women (49). No studies with longitudinal/repeated pre-pandemic and during pandemic assessments of verbal violence were identified.
Taken together, included studies suggest an increase in cases and severity of psychological/emotional DV in the general population during the COVID-19 pandemic. The limited number of studies focusing on specific samples point toward unchanged or even decreased psychological/emotional DV cases, whereas severity of DV may have increased for a significant proportion of victims. Studies pertaining to verbal DV were limited to reports on severity, suggesting verbal DV to have worsened for many victims since the COVID-19 outbreak.
Only one longitudinal study investigated sexual violence. Chiaramonte et al. (57) used data from an ongoing longitudinal study in the U.S. to examine the impact of the COVID-19 stay-at-home order (March 15, 2020) on DV survivors who had sought service from DV agencies and were currently in precarious or unstable housing conditions (see above). In this specific sample of DV survivors, there was a significant decrease in sexual DV in the 24 months prior to the onset of the COVID-19 pandemic—thus, since seeking help from a DV agency. No significant changes were found after the onset of the pandemic (57).
Among the n = 11 cross-sectional studies reporting on sexual DV, n = 8 studies reported a specific change in sexual DV prevalence or severity to pre-pandemic levels in samples from the general population (13, 39, 42, 45, 48–50, 53), of which three indicated an increase and one a decrease in overall prevalence. Two studies reported significant overall increases of sexual DV by 3–5% during the first lockdown in samples of Arab women (49) and women in the Kurdistan region of Iraq (42). An additional study reported an increase of 1% in a sample of 136 Bangladeshi females and males, but did not report a significance test for this potential increase (50). In contrast, Ojeahere et al. documented a decrease of 2% in a sample of 474 females and males during the lockdown in Nigeria (39). All four studies utilized self-generated questions to assess sexual DV via online surveys (39, 42, 49, 50).
Regarding a change in severity, four studies specifically reported on changes in sexual violence during the first lockdown among those experiencing DV (13, 45, 48, 53). In a sample of 3,545 females and males in Germany, 3% of the women reported sexual violence to have worsened (13). Similarly, in a sample of 94 Indian females and males, 14% of those experiencing DV reported an increase of sexual violence (53). Hamadani et al. reported that out of those experiencing IPV in a sample of 2,174 mothers in Bangladesh, 51% reported sexual violence to have increased (48). Even more specifically, Jetelina et al. documented that among those experiencing sexual IPV in a sample of 1,730 females and males in the U.S., 28% reported violence to have worsened since the COVID-19 outbreak, whereas 26% reported violence to have improved, and 47% reported violence to not have changed (45).
The remaining n = 3 cross-sectional studies focused on specific populations, namely currently pregnant women in Ethiopia (37) and Jordan (46), and GBMSM in the U.S. (38). Regarding sexual DV among pregnant women, Abujilban et al. reported a 4% decrease during the first lockdown in a Jordanian sample of 215 pregnant women when using the World Health Organization's Domestic Violence Questionnaire Screening Tool (DVQST) in an online survey (46). Nonetheless, using in-person interviews, Teshome et al. documented that among those reporting IPV within the last year (i.e., 2020) in their sample of 464 pregnant Ethiopian women, 25% reported sexual violence to have increased after the COVID-19 outbreak (37). In the sample of GBMSM men in the U.S., Stephenson et al. documented that 2% indicated having experienced sexual violence for the first time during lockdown (38).
Overall, included studies suggest an increase in cases and severity of sexual DV in the general population during the COVID-19 pandemic. Similar to studies on psychological/emotional violence, the limited number of studies focusing on specific samples point toward unchanged or even decreased sexual DV cases, whereas severity of sexual DV may have increased for a significant proportion of victims.
Two studies with longitudinal/repeated pre-pandemic and during pandemic assessments reported on changes in physical violence. First, Kliem et al. (55) utilized data from in-person interviews between January and March 2016 (i.e., pre-pandemic) and February and March 2021 (i.e., during-pandemic) in representative samples of 1,317 (2016) and 1,005 (2021) participants from the general German population. At both time points, participants reported on physical IPV within the past 12 months. No significant difference between 12-month prevalence from 2016 vs. 2021 were found regarding physical IPV, with the 12-month prevalence remaining stable at around 9% for women and 7–9% for men (55). Second, Chiaramonte et al. (57) used data from an ongoing longitudinal study in the U.S. to examine the impact of the COVID-19 stay-at-home order (March 15, 2020) on DV survivors (see above). In this specific sample of DV survivors, there was a significant decrease in physical DV in the 24 months prior to the onset of the COVID-19 pandemic—thus, since seeking help from a DV agency. No significant changes were found after the onset of the pandemic (57).
Among the n = 12 cross-sectional studies reporting on physical DV, n = 9 studies reported a specific change in physical DV prevalence to pre-pandemic levels in samples from the general population (13, 39, 42, 45, 48–50, 52, 53), with three studies documenting an increase in overall prevalence and two studies documenting a decrease. Three studies reported significant overall increases of physical DV by 5–8% during the first lockdown in samples of 490 Arab women (49), 346 women in the Kurdistan region of Iraq (42), and 1,992 young Peruvian female and male adults (52). Two studies utilized self-generated questions to assess physical DV via online surveys (42, 49), whereas one study conducted phone interviews (52). In contrast, using self-generated questions in an online survey, Ojeahere et al. documented a slight decrease of 2% in a sample of 474 females and males during the lockdown in Nigeria (39). Further, Rashid Soron et al. reported a decrease of 8% in a sample of 136 Bangladeshi females and males, but did not report a significance test for this potential decrease (50).
Regarding a change in severity, four studies specifically reported on changes in physical violence among those experiencing DV (13, 45, 48, 53). Among those reporting DV in a sample of 3,545 females and males in Germany, severity of physical DV increased by almost 15% in females and 21% in males during the first lockdown (13). Similarly, in a sample of 94 Indian females and males, 29% of those experiencing DV reported physical violence to have increased during the first lockdown (53). Hamadani et al. reported higher numbers, documenting that out of those experiencing IPV in a sample of 2,174 mothers in Bangladesh, 56% reported physical violence to have increased during the lockdown using self-generated questions in a phone-based survey (48). Even more specifically, Jetelina et al. documented that among those experiencing physical IPV in a sample of 1,730 females and males in the U.S., 27% reported violence to have worsened since the COVID-19 outbreak, whereas 50% reported violence to have improved, and 23% reported violence to not have changed (45).
The remaining n = 3 cross-sectional studies focused on specific populations, namely currently pregnant women in Ethiopia (37) and Jordan (46), and GBMSM in the U.S. (38). Regarding currently pregnant women, Abujilban et al. reported a 49% decrease during the first lockdown in an Jordanian sample of 215 pregnant women when using the World Health Organization's Domestic Violence Questionnaire Screening Tool (DVQST) in an online survey (46). Nonetheless, using in-person interviews, Teshome et al. documented that among those reporting IPV within the last year (i.e., 2020) in their sample of 464 pregnant Ethiopian women, 25% reported physical violence to have increased since the COVID-19 outbreak (37). In the sample of GBMSM in the U.S., Stephenson et al. documented that 1% indicated having experienced physical violence for the first time during the lockdown (38).
Taken together, regarding changes in cases of physical DV in the general population, three cross-sectional studies reported increases, whereas two studies reported decreases during the pandemic. The two studies with longitudinal/repeated pre-pandemic and during pandemic assessments reported no change in cases of physical DV in the general population and among DV survivors. It should however be noted that all studies originated in different countries, making direct comparison difficult. Regarding changes in severity of physical DV, included studies highlight that during the pandemic, physical violence worsened for a significant number of victims. Again, the limited number of studies focusing on specific samples point toward an unchanged or even decreased number of physical DV cases, whereas severity of DV may have increased for a significant proportion of victims.
Only one longitudinal study investigated economic violence. Chiaramonte et al. (57) used data from an ongoing longitudinal study in the U.S. (see above), assessing economic violence via The Revised Scale of Economic Abuse (SEA2). In this specific sample of DV survivors, there was a significant decrease in economic DV in the 24 months prior to the onset of the COVID-19 pandemic—thus, since seeking help from a DV agency. No significant changes were found after the onset of the pandemic (57).
Without exception, all n = 4 cross-sectional studies reporting a specific change in economic/financial DV prevalence to pre-pandemic levels utilized samples from the general population (39, 49, 50, 53). Rashid Soron et al. reported a 10% increase during the first lockdown in a sample of 136 Bangladeshi females and males using self-generated questions in an online survey, although no significance test was performed for this potential increase (50). In contrast, also utilizing self-generated questions in online surveys, the two remaining studies did not find any significant change in economic/financial DV during the lockdown in samples of 474 females and males in Nigeria (39) and 490 Arab women (49). Nonetheless, of those experiencing DV in a sample of 94 females and males, 29% reported economic violence to have increased during the first lockdown in India (53).
Overall, three of the four cross-sectional studies as well as the only longitudinal study identified for this review reported no change in economic/financial DV cases during the COVID-19 pandemic in the general population. Nonetheless, for many of those experiencing DV, severity of economic/financial violence may have increased.
A total of n = 14 cross-sectional studies documented changes in overall DV, i.e., regardless of DV type, either through participants' retrospective reports for a time point prior to the pandemic (38–43, 45, 47, 49, 51, 53, 54) or through comparison of cross-sectional data to data collected as part of a prior study (44). Of these, n = 10 studies utilized samples from the general population. Four studies reported significant increases in overall DV of 7–33% during the first lockdown in samples of 490 Arab women (49), 346 women in the Kurdistan region of Iraq (42), 751 Tunisian (41), and 560 Indian women (43). All four studies utilized self-generated questions to assess DV via online surveys and exclusively focused on violence against women. In contrast, three studies documented decreases in overall DV. To this end, Ojeahere et al. reported a 7% decrease of any type of DV during the first lockdown as compared to pre-lockdown times in a Nigerian sample of 474 females and males using self-generated questions in an online survey (39). Similarly, Alharbi et al. documented an overall 9% decrease of IPV during the first lockdown in a Saudi Arabian sample of 1,901 married women using the WHO multi-country instrument in an online survey (47). Although utilizing mean IPV scores rather than prevalence rates, Plášilová et al. found a small, significant decrease in mean IPV incidence from 3 months prior to the pandemic to measurement time points during the first and second COVID-19 waves in a sample of 429 women in the Czech Republic (51).
Regarding a change in severity, n = 4 cross-sectional studies documented changes in those with DV experiences specifically. To this end, Pattojoshi et al. reported that among the 560 women in their sample who experienced IPV before the first lockdown in India, 78% reported an increase in violence since the beginning of the lockdown (43). Similarly, in a sample of 94 females and males, Sharma and Khokhar documented that of those experiencing DV during the lockdown in India, 86% reported increased violence as compared to the time before the pandemic (53). Slightly lower increases were reported by Indu et al. who found that among those having experienced DV perpetrated by their husbands within the previous 12 months in a sample of 209 Indian women, 6% indicated violence to have worsened during the lockdown and 11% reported violence to have begun during the pandemic (54). Even more specifically, Jetelina et al. documented that among those experiencing IPV in a sample of 1,730 females and males in the U.S., 17% reported violence to have worsened since the COVID-19 outbreak, whereas 30% reported violence to have improved, and 54% reported violence to not have changed (45). Further, Alharbi et al. found that among those indicating ever having experienced IPV in a sample of 1,901 married women in Saudi Arabia, 40% reported violence to have increased since the COVID-19 outbreak, whereas 13% reported a decrease, 43% reported no change, and 4% reported violence to have stopped (47).
Four cross-sectional studies focused on specific populations, namely currently pregnant women in Ethiopia (37), GBMSM in the U.S. (38, 40), and participants with a history of DV in Austria (44). Using in-person interviews, Teshome et al. documented that out of those reporting IPV within the last year (i.e., 2020) in their sample of 464 pregnant Ethiopian women, 18% reported experiencing increased violence (37). Two studies investigated IPV in U.S. samples of 516 (38) and 214 (40) GBMSM. Stephenson et al. reported that among self-reported victims of IPV, 5% indicated having experienced IPV for the first time during the first lockdown (38). Walsh et al. documented that among self-reported victims of IPV, 47% reported experiencing new or more frequent IPV since the COVID-19 outbreak (40). Finally, Lampe et al. (44) compared DV during the lockdown in Austria in a sample of female and male participants with (n = 34) or without (n = 33) prior DV experiences. Those with prior DV experiences reported more DV than those without prior DV experiences. Importantly, while DV remained stable compared to pre-lockdown values for those without prior DV experiences, it decreased in the group with prior DV experiences. Nonetheless, DV during the lockdown remained significantly higher in the group with prior DV experiences (44). No studies with repeated longitudinal/pre-pandemic and during pandemic assessments of overall violence were identified.
Taken together, evidence pertaining to changes in overall DV cases remains inconclusive with four cross-sectional studies reporting increases and three cross-sectional studies reporting decreases. Regarding changes in DV severity however, across different samples from the general population in various countries, 6–86% of those experiencing DV reported violence to have worsened during the first lockdown in their respective country or since the COVID-19 outbreak. Again, the limited number of studies focusing on specific samples does not allow for conclusions regarding changes in the number of overall DV cases, while severity of DV may have increased for a significant proportion of victims.
Besides the focus on victims of DV, n = 2 studies with longitudinal/repeated pre-pandemic and during pandemic assessments reported on DV perpetration. First, Steinhoff et al. (56) used interview data from a Swiss longitudinal study to compare DV perpetration in a representative sample of 786 young adults. To this end, pre-pandemic in-person interview reports from 2018 and four during-pandemic online survey measurements between spring and fall 2020 were included. The risk of DV perpetration doubled over the early course of the pandemic from 5% in April 2020 to 10% in May 2020 for men, but no change was observed for women (56). Second, Kliem et al. (55) utilized data from in-person interviews between January and March 2016 (i.e., pre-pandemic) and February and March 2021 (i.e., during-pandemic) in representative samples of 1,317 (2016) and 1,005 (2021) participants from the general German population. At both time points, participants reported on physical IPV perpetration and physical or psychological violence against the youngest child in the household within the past 12 months. No significant difference in the 12-month prevalence from 2016 vs. 2021 were found regarding IPV perpetration or for physical or psychological violence directed against children. IPV 12-month prevalence remained stable with around 6% of women and 6–9% of men reporting IPV perpetration in 2016 and 2021. Similarly, DV directed against children over the past 12 months remained stable with 16–20% of women and 18–22% of men indicating having been physically violent and 7–10% of women and 9–11% of men indicating psychological violence against a child in 2016 and 2021 (55).
Further, n = 2 cross-sectional studies examined rates in DV perpetration during the pandemic, both utilizing U.S. samples of GBMSM (38, 40). In their sample of 516 men, Stephenson et al. (38), 6% of participants reported having perpetrated any type of IPV, with emotional IPV being the most common type. Only 1% of men indicated first-time perpetration during the lockdown (38). Reports of perpetration were slightly higher in Walsh et al.'s (40) sample of 214 men, recruited from two previous male couples/HIV-related studies. Overall, 15% reported IPV perpetration, with 7% reporting perpetration but not victimization and 8% reporting both perpetration and victimization. Among the self-reported perpetrators, around a third indicated their behavior to have increased since the COVID-19 outbreak. Interestingly, however, Walsh et al. further documented that among couples within the sample, reports of perpetration and victimization were not always congruent (40).
Overall, the limited number of included studies reporting on DV perpetration does not allow for definite conclusions. Nonetheless, across studies, self-reported perpetration seems to have remained unchanged as compared to pre-pandemic times. The single study documenting perpetration across the pandemic however, indicates that for men, risk of DV perpetration may have increased over time since the COVID-19 outbreak. This finding highlights the need for data from multiple measurement points over the course of the pandemic rather than solely comparing pre-pandemic levels to during-pandemic levels.
The aim of our review was to examine the change in prevalence of domestic violence during the COVID-19 pandemic in empirical, peer-reviewed studies. We opted to only include self-report studies to approximate prevalence rates not biased by help seeking behavior, which in itself might have been altered by the pandemic. Overall, 22 studies were included-−19 were cross-sectional whereas 3 included both pre-pandemic and during pandemic assessments. Of the 22 studies, 17 utilized samples from the general population, while 5 included samples from specific populations [i.e., DV survivors; pregnant women; gay, bisexual, and other men who have sex with men (GBMSM)].
Taken together, these studies suggest (1) an increase in cases and severity of psychological/emotional and sexual DV in the general population, (2) no change in number of economic/financial DV cases in the general population, and (3) an increase in severity of DV of any type for a significant number of victims during the pandemic. Evidence for changes in prevalence regarding verbal DV remains inconclusive because of the limited number of studies reporting on verbal DV. Further, despite a larger number of available studies, evidence for changes in prevalence regarding physical and overall DV remains inconclusive.
As mentioned above, only five of the 22 included studies focused on samples from specific populations, namely DV survivors, pregnant women, and GBMSM. Although it should be assumed that individuals from these three groups would be included in representative samples from the general population, several considerations should be noted. First, although valuable information pertaining to a change in DV severity may be drawn from studies utilizing samples of DV survivors, given the fact that prior DV experience is a risk factor for future DV experiences, a potential change in DV prevalence from pre-pandemic to pandemic times in these samples may not be generalizable to the general nor other populations. Second, we here treated studies on pregnant women as a specific sample because of the additional stress pregnancy and the transition to parenthood may represent for the entire family. To this end, pregnancy-specific factors, such as becoming a first-time parent and the pregnancy being unwanted have been found to put pregnant women at an increased risk for DV victimization (58). Further, violence during pregnancy may have severe adverse consequences for both, the mother and the unborn child. For instance, while physical violence against the pregnant woman may also lead to injuries of the unborn child, implications of maternal mental health complications during pregnancy, potentially resulting from violence victimization, may bear further adverse implications for pregnancy and birth outcomes, as well as child development (59–63). Third, we also treated studies on GBMSM as a specific sample because prior research indicates higher risk for IPV and/or DV among GBMSM than among heterosexual men (64–66). In addition, it has been suggested that sexual minorities may be disproportionately affected by pandemic-related stressors relating to employment, finances, and (mental) health (40). For these reasons, it is noteworthy that only a very limited number of studies on specific (at-risk) groups was available for inclusion in this review. Examinations of other at-risk groups, such as sexual minorities apart from GBMSM and investigations of at-risk samples in different countries is currently still lacking. Thus, changes in DV prevalence and severity in specific (at-risk) groups requires additional scientific attention.
Similarly, it should be highlighted that the majority of included studies reporting on samples from the general population focused on violence against women, with 10 studies exclusively assessing females. Although 10 further studies included both, females and males, there is currently a lack of studies reporting on male victimization. This lack however does not only pertain to DV during the pandemic, but can be pointed out as a gap in the current literature pertaining to DV in general. Additionally, only one of the included studies reported on DV against children. On the one hand, this may be attributable to the current inclusion criterion of solely incorporating studies which presented participant reports. For instance, studies utilizing official/administrative data indicate that DV against children may oftentimes be reported by third parties and that opportunities for third-party observations and report are limited by governmental measures such as social distancing, school closures, and lockdown (67, 68). On the other hand, this may be at least partially explained by the current focus on DV victimization. Only few studies in this review included participant reports regarding DV perpetration. Although not surprising given the topic's sensitive nature and potential biases in self-reports, such as social desirability, examining victimization and perpetration in isolation may not reflect the true complexity and oftentimes bidirectionality of DV, where many individuals may, at least temporarily, be victim and perpetrator rather than one of the two exclusively (69, 70). Nevertheless, a clear picture of DV perpetration and its risk factors is crucial for the development and implementation of resources and (preventive) interventions as well as de-stigmatization of help seeking among perpetrators.
As noted above, at the time of the literature search for this review, only three studies with longitudinal/repeated pre-pandemic and during pandemic assessments were identified. Of these, two utilized samples from the general population in Germany and Switzerland (55, 56), with one solely focusing on perpetration of physical DV but not victimization (56), and the other focusing on victimization and perpetration of physical IPV and perpetration of psychological/emotional and physical violence against children in the household (55). The third study focused specifically on U.S. DV survivors in precarious or unstable housing conditions (57). Without question, more time is required for studies utilizing repeated assessments over time to be conducted and for results to be published. Nonetheless, studies identified for this review highlight a need for data pertaining to prevalence and severity of different types of DV from multiple timepoints prior to the COVID-19 outbreak and over the course of the pandemic with multiple measurements during the pandemic. Repeated assessments over the course of the pandemic are further warranted given different pandemic phases and waves, which in turn may be characterized by differential stressors (71, 72). For instance, the COVID-19 outbreak and immediate governmental measures represented an entirely new and unknown situation for most of the global population, characterized by uncertainty and an immediate increase in stress related to employment and finances for many. Although this initial uncertainty may by now have decreased, long-term adjustment to the pandemic and the ever-changing implications for day-to-day life may vary considerably among individuals given their specific experiences and living conditions. Thus, repeated assessments of DV over the course of the pandemic may offer the opportunity to distinguish between the pandemic's initial stress, potentially resulting in emotional turmoil, in turn increasing the risk for interpersonal aggression, vs. long-term stress, potentially resulting in emotional depletion/depression in turn also increasing the risk for interpersonal aggression (71, 72).
In light of the fast, global spread of COVID-19 and the time needed to design, authorize, and conduct empirical studies, it is not surprising that the majority of studies identified for this review were cross-sectional and utilized online surveys to assess DV. We noted a large between-study heterogeneity regarding study country of origin, sample size, participant inclusion criteria, and/or measure used to assess DV. Taking this into account, results of individual studies should thus be interpreted with caution and may not be generalizable to different regions or samples and are limited regarding the validity of reported changes over time. In addition, few studies reported on self-reported DV perpetration, suggesting that perpetration seems to have remained unchanged as compared to pre-pandemic times.
Putting our results into the context of previous reports using official/administrative data highlights an additional concern. Although studies included in the current review focusing on self-reported DV suggest increased DV experience for a significant amount of people around the world, prior studies utilizing police and helpline call data and formal police reports are not fully congruent with this increase. To this end, several studies have documented decreases in formal DV-related police reports, whereas sharp increases in numbers of DV-related emergency calls to the police and helplines have been documented (73–81). Importantly, the reported reduction in formal police reports may not reflect a decrease in DV prevalence but rather a decrease in reporting DV incidences. Being constrained to the domestic setting and isolation from other social or work contexts due to stay-at home orders or lockdowns may be linked to reduced or altered help-seeking behaviors. Prior research suggests a shift in help-seeking behavior where victims may seek help in acute emergency situations but may not follow through with formal police reporting during stay-at-home orders and lockdown (2). Nonetheless, social isolation may make reporting of DV more difficult given that the perpetrator cannot be separated. Thus, many victims may only have limited or no access to help resources and may further be limited in their ability to participate in research studies and/or to complete online surveys in a safe, unhindered environment. Because this may not be conveyed in crime statistics, empirical studies regarding DV-related help-seeking behavior and potential changes resulting from governmental measures in response to the spread of COVID-19 are needed in order to improve assistance for victims.
The aforementioned changes in help-seeking behavior and restricted or limited resource availability are of particular importance because of the detrimental side effects of DV victimization. For instance, Iob et al. document that half of those experiencing psychological or physical DV reported thoughts pertaining to suicide and self-harm. Alarmingly, during the first U.K. lockdown, a quarter of those experiencing psychological/emotional or physical DV indicated having harmed themselves during the past week (82). Besides the previously documented increase in DV-related homicide during the COVID-19 pandemic (83–85), victims may thus further be at high risk for self-harm and/or suicide, highlighting the crucial need for easily accessible DV resources and (preventive) interventions for both, victims and perpetrators.
Several strengths and limitations of the included literature should be acknowledged. It is crucial to highlight the important contributions of the studies included in this review, given the initial reliance on official/administrative records to assess the potential change in DV during the COVID-19 pandemic. Studies included in this review utilized participant reports and may thus more accurately reflect changes in DV prevalence and severity rather than changes in help-seeking behavior. Limitations of included studies pertain to the reliance on cross-sectional designs (viz. introducing potential biases given retrospective self-report) and online surveys (viz. introducing self-selection bias within the sample). Although noted as a limitation in the majority of studies, generalizability of individual results may be limited given concerns regarding sample representativeness of the intended target population. Further, not all studies utilized measures to assess DV which had previously been validated in the language used or for the population investigated. Additionally, the majority of studies focused on DV victimization and only few studies investigated both, victimization and perpetration. Nonetheless, the cultural diversity represented within the identified studies is remarkable, particularly given the timely nature of the topic.
Strengths of the current review are the systematic search for and identification of relevant literature, the systematic processes of data extraction and quality assessment, as well as its focus on participant-reported changes in specific types of DV prevalence and severity estimates and its bi-directionality (i.e., victimization vs. perpetration). Several limitations should be noted. First, given the expectation that studies on DV prevalence tend to exhibit high heterogeneity regarding target population and conceptualization and assessment of violence, we synthesized extracted data narratively and did not conduct any quantitative analyses of reported changes in DV prevalence or severity. Thus, we do not present pooled estimates and our assumption that the considerable variation of changes in prevalence and severity estimates observed may be attributable to between-study variation was not tested. Second, the current review was not pre-registered and no formal protocol was put into writing. Third, although we conducted this systematic review in line with PRISMA guidelines and utilized the JBI checklist for risk of bias assessment, we did not conduct certainty assessments. Fourth, quality assessment presented herein was limited by methodological limitations and lacking information in the original articles. Our risk of bias assessment resulted in the appraisal of half the included studies as presenting high risk. It should therefore be noted that our review may be affected by publication and/or reporting biases.
In this review, we focused our attention on changes in prevalence and severity of different types of DV during the COVID-19 pandemic. To this end, we examined empirical studies utilizing self-reported participant data, published in peer-reviewed journals. Given the considerable between-study heterogeneity pertaining to region, sample size and characteristics, assessment time, and assessment measure, results of individual studies may not be directly comparable and should be interpreted with caution because of limited generalizability. Overall, our data synthesis of 22 studies indicates increases in cases of psychological/emotional and sexual DV as well as increases in severity of DV of any type for a significant number of victims during the pandemic in the general population. Our findings thus partially support the previously documented increase in DV during stay-at-home orders and lockdown. Nonetheless, evidence for changes in prevalence regarding economic/financial, physical, and overall DV remains inconclusive. Prior research suggests that many victims may only have limited or no access to help resources and that social isolation may make reporting of DV more difficult given that the perpetrator cannot be separated. This highlights an important public and clinical concern, indicating a potential change in help-seeking behavior among victims of DV during the COVID-19 pandemic. Restricted or limited access to help resources and social isolation from friends, family, or co-workers resulting from governmental measures to contain the spread of the virus likely impacts millions of individuals at risk for DV around the world. Governmental measures should thus take into account the availability of easily accessible, anonymous help resources for DV victims and perpetrators, in particular during times of social isolation, stay-at-home orders, and lockdown. Finally, DV awareness and knowledge needs to be distributed in order to improve formal and informal resources as well as (preventive) interventions for both, victims and perpetrators.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
FT, VB, and SG-N designed and conceptualized the present study. FT, VB, and FR conducted manuscript screening, data extraction, and risk of bias (quality) assessment. AM aided in data extraction. FT and VB wrote the first draft of the manuscript. SG-N supervised data extraction and drafting of the manuscript. FT, VB, FR, AM, JD, JS, and SG-N contributed to the analysis and interpretation. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors received funds for open access publication fees by the Norwegian Institute of Public Health.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.874183/full#supplementary-material
1. Mojahed A, Brym S, Hense H, Grafe B, Helfferich C, Lindert J, et al. Rapid review on the associations of social and geographical isolation and intimate partner violence: implications for the ongoing COVID-19 pandemic. Front Psychiatry. (2021) 12:578150. doi: 10.3389/fpsyt.2021.578150
2. Garthus-Niegel S, Seefeld L, Mojahed A, Schellong J. Häusliche Gewalt im Kontext der COVID-19-Pandemie = Domestic violence in the context of the COVID-19 pandemic. Trauma Gewalt. (2021) 15:200–10. doi: 10.21706/tg-15-3-200
3. Nussbaumer-Streit B, Mayr V, Dobrescu AI, Chapman A, Persad E, Klerings I, et al. Quarantine alone or in combination with other public health measures to control COVID-19: a rapid review. Cochrane Database Syst Rev. (2020) 4:Cd013574. doi: 10.1002/14651858.CD013574
4. Lau H, Khosrawipour V, Kocbach P, Mikolajczyk A, Schubert J, Bania J, et al. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J Travel Med. (2020) 27:taaa037. doi: 10.1093/jtm/taaa037
5. Vindegaard N, Benros ME. COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immun. (2020) 89:531–42. doi: 10.1016/j.bbi.2020.05.048
6. Ammar A, Chtourou H, Boukhris O, Trabelsi K, Masmoudi L, Brach M, et al. COVID-19 home confinement negatively impacts social participation and life satisfaction: a worldwide multicenter study. Int J Environ Res Public Health. (2020) 17:6237. doi: 10.3390/ijerph17176237
7. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. (2020) 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
8. Cacioppo JT, Hughes ME, Waite LJ, Hawkley LC, Thisted RA. Loneliness as a specific risk factor for depressive symptoms: cross-sectional and longitudinal analyses. Psychol Aging. (2006) 21:140–51. doi: 10.1037/0882-7974.21.1.140
9. Hawkley LC, Cacioppo JT. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med. (2010) 40:218–27. doi: 10.1007/s12160-010-9210-8
10. Lauder W, Mummery K, Jones M, Caperchione C. A comparison of health behaviours in lonely and non-lonely populations. Psychol Health Med. (2006) 11:233–45. doi: 10.1080/13548500500266607
11. Åkerlind I, Hörnquist JO. Loneliness and alcohol abuse: a review of evidences of an interplay. Soc Sci Med. (1992) 34:405–14. doi: 10.1016/0277-9536(92)90300-F
12. Lieberman JA, Olfson M. Meeting the mental health challenge of the COVID-19 pandemic. Psychiatric Times. (2020). Available online at: https://www.psychiatrictimes.com/view/meeting-mental-health-challenge-covid-19-pandemic (accessed February 11, 2022).
13. Jung S, Kneer J, Kruger THC. Mental health, sense of coherence, and interpersonal violence during the covid-19 pandemic lockdown in Germany. J Clin Med. (2020) 9:1–12. doi: 10.3390/jcm9113708
14. Campbell AM. An increasing risk of family violence during the Covid-19 pandemic: strengthening community collaborations to save lives. Foren Sci Int Rep. (2020) 2:100089. doi: 10.1016/j.fsir.2020.100089
15. WHO. Addressing Violence Against Children, Women and Older People During the COVID-19 Pandemic: Key Actions. WHO (2020).
16. Fraser E. Impact of COVID-19 Pandemic on Violence Against Women Girls. London: Department for International Development. (2020). Available online at: https://www.sddirect.org.uk/media/1881/vawg-helpdesk-284-covid-19-and-vawg.pdf (accessed February 11, 2022).
17. Poate S,. 75% Increase in Domestic Violence Searches Since Coronavirus. (2020). Available online at: https://www.nbnnews.com.au/2020/03/31/dvsearches-coronavirus/ (accessed February 11, 2022).
18. UN. What is Dometic Abuse?. Available online at: https://www.un.org/en/coronavirus/what-is-domestic-abuse (accessed February 11, 2022).
19. Mojahed A, Alaidarous N, Kopp M, Pogarell A, Thiel F, Garthus-Niegel S. Prevalence of intimate partner violence among intimate partners during the perinatal period: a narrative literature review. Front Psychiatry. (2021) 12:601236. doi: 10.3389/fpsyt.2021.601236
20. WHO. Understanding and Addressing Violence Against Women: Intimate Partner Violence. WHO (2012).
21. van Gelder N, Peterman A, Potts A, O'Donnell M, Thompson K, Shah N, et al. COVID-19: reducing the risk of infection might increase the risk of intimate partner violence. EClinicalMedicine. (2020) 21:100348. doi: 10.1016/j.eclinm.2020.100348
22. Kolbe V, Büttner A. Domestic violence against men - prevalance and risc factors. Dtsch Artzebl International. (2020) 117:534–41. doi: 10.3238/arztebl.2020.0534
23. Black MC, Basile KC, Breiding MJ, Smith SG, Walters ML, Merrick MT, et al. The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 Summary Report. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (2011).
24. Walter W, Lenz H-J, Puchert R. Gewalt gegen Männer Personale Gewaltwiderfahrnisse von Männern in Deutschland: Pilotstudie im Auftrag des Bundesministeriums für Familie, Senioren, Frauen und Jugend. (2004). Available online at: https://www.bmfsfj.de/resource/blob/84590/a3184b9f324b6ccc05bdfc83ac03951e/studie-gewalt-maenner-langfassung-data.pdf (accessed February 11, 2020).
25. NCADV NCADV. Domestic Violence. (2020). Available online at: https://www.ncadv.org/statistics (accessed February 11, 2022).
26. Peterman A, Potts A, O'Donnell M, Thompson K, Shah N, Oertelt-Prigione S, et al. Pandemics and Violence Against Women and Children (2020).
27. Mojahed A, Alaidarous N, Shabta H, Hegewald J, Garthus-Niegel S. Intimate partner violence against women in the Arab countries: a systematic review of risk factors. Trauma Viol Abuse. (2020) 1524838020953099. doi: 10.1177/1524838020953099. [Epub ahead of print].
28. Riddell T, Ford-Gilboe M, Leipert B. Strategies used by rural women to stop, avoid, or escape from intimate partner violence. Health Care Women Int. (2009) 30:134–59. doi: 10.1080/07399330802523774
29. Shamu S, Abrahams N, Temmerman M, Musekiwa A, Zarowsky C. A systematic review of African studies on intimate partner violence against pregnant women: prevalence and risk factors. PLoS ONE. (2011) 6:e17591. doi: 10.1371/journal.pone.0017591
30. Kourti A, Stavridou A, Panagouli E, Psaltopoulou T, Spiliopoulou C, Tsolia M, et al. Domestic violence during the COVID-19 pandemic: a systematic review. Trauma Viol Abuse. (2021) 15248380211038690. doi: 10.1177/15248380211038690. [Epub ahead of print].
31. Piquero AR, Jennings WG, Jemison E, Kaukinen C, Knaul FM. Domestic violence during the COVID-19 pandemic - evidence from a systematic review and meta-analysis. J Crim Justice. (2021) 74:101806. doi: 10.1016/j.jcrimjus.2021.101806
32. Lausi G, Pizzo A, Cricenti C, Baldi M, Desiderio R, Giannini AM, et al. Intimate partner violence during the covid-19 pandemic: a review of the phenomenon from victims' and help professionals' perspectives. Int J Environ Res Public Health. (2021) 18:6204. doi: 10.3390/ijerph18126204
33. Bazyar J, Chehreh R, Sadeghifar J, Karamelahi Z, Ahmadimazhin S, Vafery Y, et al. Effects of the COVID-19 pandemic on the intimate partner violence and sexual function: a systematic review. Prehosp Disaster Med. (2021) 36:593–8. doi: 10.1017/S1049023X21000789
34. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. (2021) 88:105906. doi: 10.1186/s13643-021-01626-4
35. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
36. Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int J Evid Based Healthc. (2015) 13:147–53. doi: 10.1097/XEB.0000000000000054
37. Teshome A, Gudu W, Bekele D, Asfaw M, Enyew R, Compton SD. Intimate partner violence among prenatal care attendees amidst the COVID-19 crisis: the incidence in Ethiopia. Int J Gynaecol Obstet. (2021) 153:45–50. doi: 10.1002/ijgo.13566
38. Stephenson R, Chavanduka TMD, Rosso MT, Sullivan SP, Pitter RA, Hunter AS, et al. COVID-19 and the risk for increased intimate partner violence among gay, bisexual and other men who have sex with men in the United States. J Interpers Viol. (2021) 886260521997454. doi: 10.1177/0886260521997454. [Epub ahead of print].
39. Ojeahere MI, Kumswa SK, Adiukwu F, Plang JP, Taiwo YF. Intimate partner violence and its mental health implications amid COVID-19 lockdown: findings among Nigerian Couples. J Interpers Viol. (2021) 8862605211015213. doi: 10.1177/08862605211015213. [Epub ahead of print].
40. Walsh AR, Sullivan S, Stephenson R. Intimate partner violence experiences during COVID-19 among male couples. J Interpers Viol. (2021) 8862605211005135. doi: 10.1177/08862605211005135. [Epub ahead of print].
41. Sediri S, Zgueb Y, Ouali U, Jomli R, Nacef F, Ouanes S, et al. Women's mental health: acute impact of COVID-19 pandemic on domestic violence. Arch Womens Mental Health. (2020) 23:749–56. doi: 10.1007/s00737-020-01082-4
42. Mahmood KI, M-Amen KM, Hussain SS, Kako DA, Shabu SA, Shabila NP, et al. The impact of COVID-19 related lockdown on the prevalence of spousal violence against women in Kurdistan Region of Iraq. J Interpers Viol. (2021) 886260521997929. doi: 10.1177/0886260521997929. [Epub ahead of print].
43. Pattojoshi A, Sidana A, Garg S, Mishra SN, Singh LK, Goyal N, et al. Staying home is NOT ‘staying safe': a rapid 8-day online survey on spousal violence against women during the COVID-19 lockdown in India. Psychiatry Clin Neurosci. (2021) 75:64–6. doi: 10.1111/pcn.13176
44. Lampe A, Trawoger I, Beck T, Riedl D, Daniels JK. Did domestic violence really increase in the early phase of the covid-19 pandemic? Results of an interview-based observational study. Zeitschrift Psychosom Med Psychother. (2021) 67:303–14. doi: 10.13109/ZPTM.2021.67.OA8
45. Jetelina KK, Knell G, Molsberry RJ. Changes in intimate partner violence during the early stages of the COVID-19 pandemic in the USA. Inj Prev. (2021) 27:93–7. doi: 10.1136/injuryprev-2020-043831
46. Abujilban S, Mrayan L, Hamaideh S, Obeisat S, Damra J. Intimate partner violence against pregnant jordanian women at the time of COVID-19 pandemic's quarantine. J Interpers Viol. (2021) 37:886260520984259. doi: 10.1177/0886260520984259
47. Alharbi FF, Alkheraiji MA, Aljumah AA, Al-Eissa M, Qasim SS, Alaqeel MK. Domestic violence against married women during the COVID-19 quarantine in Saudi Arabia. Cureus. (2021) 13:e15231. doi: 10.7759/cureus.15231
48. Hamadani JD, Hasan MI, Baldi AJ, Hossain SJ, Shiraji S, Bhuiyan MSA, et al. Immediate impact of stay-at-home orders to control COVID-19 transmission on socioeconomic conditions, food insecurity, mental health, and intimate partner violence in Bangladeshi women and their families: an interrupted time series. Lancet Global Health. (2020) 8:e1380–e9. doi: 10.1016/S2214-109X(20)30366-1
49. El-Nimr NA, Mamdouh HM, Ramadan A, El Saeh HM, Shata ZN. Intimate partner violence among Arab women before and during the COVID-19 lockdown. J Egypt Public Health Assoc. (2021) 96:15. doi: 10.1186/s42506-021-00077-y
50. Rashid Soron T, Ashiq MAR, Al-Hakeem M, Chowdhury ZF, Uddin Ahmed H, Afrooz Chowdhury C. Domestic violence and mental health during the COVID-19 pandemic in Bangladesh. JMIR Format Res. (2021) 5:e24624. doi: 10.2196/24624
51. Plášilová L, Hula M, Krejčová L, Klapilová K. The COVID-19 pandemic and intimate partner violence against women in the Czech Republic: incidence and associated factors. Int J Environ Res Public Health. (2021) 18:502. doi: 10.3390/ijerph181910502
52. Porter C, Favara M, Sánchez A, Scott D. The impact of COVID-19 lockdowns on physical domestic violence: evidence from a list randomization experiment. SSM Popul Health. (2021) 14:100792. doi: 10.1016/j.ssmph.2021.100792
53. Sharma P, Khokhar A. Domestic violence and coping strategies among married adults during lockdown due to Coronavirus disease (COVID-19) pandemic in India: a cross-sectional study. Disaster Med Public Health Prepared. (2021) 1–29. doi: 10.1017/dmp.2021.59. [Epub ahead of print].
54. Indu PV, Tharayil HM, Ayirolimeethal A, Vidyadharan V, Vijayan B. Domestic violence and psychological problems in married women during COVID-19 pandemic and lockdown: a community-based survey. Asian J Psychiatr. (2021) 64:102812. doi: 10.1016/j.ajp.2021.102812
55. Kliem S, Baier D, Kroger C. Domestic violence before and during the COVID-19 pandemic - a comparison of two representative population surveys. Dtsch Arztebl Int. (2021) 118:483–4. doi: 10.3238/arztebl.m2021.0267
56. Steinhoff A, Bechtiger L, Ribeaud D, Murray AL, Hepp U, Eisner M, et al. Self-injury and domestic violence in young adults during the COVID-19 pandemic: trajectories, precursors, and correlates. J Res Adolesc. (2021) 31:560–75. doi: 10.1111/jora.12659
57. Chiaramonte D, Simmons C, Hamdan N, Ayeni OO, López-Zerón G, Farero A, et al. The impact of covid-19 on the safety, housing stability, and mental health of unstably housed domestic violence survivors. J Community Psychol. (2021). doi: 10.1002/jcop.22765. [Epub ahead of print].
58. James L, Brody D, Hamilton Z. Risk factors for domestic violence during pregnancy: a meta-analytic review. Violence Vict. (2013) 28:359–80. doi: 10.1891/0886-6708.vv-d-12-00034
59. Thiel F, Eberhard-Gran M, Garthus-Niegel S. The impact of perinatal life stress on infant temperament and child development: a 2-year follow-up cohort study. J Dev Behav Pediatr. (2021) 42:299–306. doi: 10.1097/DBP.0000000000000887
60. Thiel F, Iffland L, Drozd F, Haga SM, Martini J, Weidner K, et al. Specific relations of dimensional anxiety and manifest anxiety disorders during pregnancy with difficult early infant temperament: a longitudinal cohort study. Arch Women's Mental Health. (2020) 23:535–46. doi: 10.1007/s00737-019-01015-w
61. Junge C, Garthus-Niegel S, Slinning K, Polte C, Simonsen TB, Eberhard-Gran M. The impact of perinatal depression on children's social-emotional development: a longitudinal study. Matern Child Health J. (2017) 21:607–15. doi: 10.1007/s10995-016-2146-2
62. Polte C, Junge C, von Soest T, Seidler A, Eberhard-Gran M, Garthus-Niegel S. Impact of maternal perinatal anxiety on social-emotional development of 2-year-olds, a prospective study of Norwegian mothers and their offspring. Matern Child Health J. (2019) 23:386–96. doi: 10.1007/s10995-018-2684-x
63. Martini J, Petzoldt J, Knappe S, Garthus-Niegel S, Asselmann E, Wittchen H-U. Infant, maternal, and familial predictors and correlates of regulatory problems in early infancy: the differential role of infant temperament and maternal anxiety and depression. Early Hum Dev. (2017) 115:23–31. doi: 10.1016/j.earlhumdev.2017.08.005
64. Finneran C, Stephenson R. Intimate partner violence among men who have sex with men: a systematic review. Trauma Viol Abuse. (2013) 14:168–85. doi: 10.1177/1524838012470034
65. Stephenson R, Finneran C. The IPV-GBM scale: a new scale to measure intimate partner violence among gay and bisexual men. PLoS ONE. (2013) 8:e62592. doi: 10.1371/journal.pone.0062592
66. Rollè L, Sechi C, Patteri L, Costa G, Bergaglia M, Menzio L, et al. Intimate partner violence: attitudes in a sample of Italian students. Cogent Psychol. (2018) 5:1514960. doi: 10.1080/23311908.2018.1514960
67. Baron EJ, Goldstein EG, Wallace CT. Suffering in silence: how COVID-19 school closures inhibit the reporting of child maltreatment. J Public Econ. (2020) 190:104258. doi: 10.1016/j.jpubeco.2020.104258
68. McLay MM. When ‘shelter-in-place' isn't shelter that's safe: a rapid analysis of domestic violence case differences during the covid-19 pandemic and stay-at-home orders. J Fam Violence. (2021) 1–10. doi: 10.1007/s10896-020-00225-6. [Epub ahead of print].
69. Bates EA. Current controversies within intimate partner violence: overlooking bidirectional violence. J Fam Violence. (2016) 31:937–40. doi: 10.1007/s10896-016-9862-7
70. Langhinrichsen-Rohling J, Misra TA, Selwyn C, Rohling ML. Rates of bidirectional versus unidirectional intimate partner violence across samples, sexual orientations, and race/ethnicities: a comprehensive review. Partner Abuse. (2012) 3:199–230. doi: 10.1891/1946-6560.3.2.199
71. Belz M, Hessmann P, Vogelgsang J, Schmidt U, Ruhleder M, Signerski-Krieger J, et al. Evolution of psychosocial burden and psychiatric symptoms in patients with psychiatric disorders during the Covid-19 pandemic. Eur Arch Psychiatry Clin Neurosci. (2022) 272:29–40. doi: 10.1007/s00406-021-01268-6
72. Bartels C, Hessmann P, Schmidt U, Vogelgsang J, Ruhleder M, Kratzenberg A, et al. Medium-term and peri-lockdown course of psychosocial burden during the ongoing COVID-19 pandemic: a longitudinal study on patients with pre-existing mental disorders. Eur Arch Psychiatry Clin Neurosci. (2021) 1–15. doi: 10.1007/s00406-021-01351-y. [Epub ahead of print].
73. Bullinger LR, Carr JB, Packham A. COVID-19 and crime: effects of stay-at-home orders on domestic violence. Am J Health Econ. (2021) 7:249–80. doi: 10.1086/713787
74. Leslie E, Wilson R. Sheltering in place and domestic violence: evidence from calls for service during COVID-19. J Public Econ. (2020) 189:104241. doi: 10.1016/j.jpubeco.2020.104241
75. Mohler G, Bertozzi AL, Carter J, Short MB, Sledge D, Tita GE, et al. Impact of social distancing during COVID-19 pandemic on crime in Los Angeles and Indianapolis. J Crim Justice. (2020) 68:101692. doi: 10.1016/j.jcrimjus.2020.101692
76. Nix J. Richards TN. The immediate and long-term effects of COVID-19 stay-at-home orders on domestic violence calls for service across six US jurisdictions. Police Pract Res. (2021) 22:1443–51. doi: 10.1080/15614263.2021.1883018
77. Silverio-Murillo A, Balmori de la Miyar JR, Hoehn-Velasco L. Families under Confinement: COVID-19 Domestic Violence. Andrew Young School of Policy Studies Research Paper Series. (2021). Available online at: https://ssrn.com/abstract=3688384 (accessed February 11, 2022).
78. Armbruster SK. Lost in Lockdown? COVID-19, Social Distancing, and Mental Health in Germany. Freiburg i Br: Albert-Ludwigs- Universität Freiburg, Wilfried-Guth-Stiftungsprofessur für Ordnungs- und Wettbewerbspolitik (2020).
79. Perez-Vincent SM, Carreras E, Gibbons MA, Murphy TE, Rossi MA. Covid-19 Lockdowns and Domestic Violence. Washington, DC: Inter-American Development Bank (2020). p. 4.
80. Rengasamy ER, Long SA, Rees SC, Davies S, Hildebrandt T, Payne E. Impact of covid-19 lockdown: domestic and child abuse in bridgend. Child Abuse Negl. (2021) 105386. doi: 10.1016/j.chiabu.2021.105386
81. Torrubiano-dominguez J, Vives-cases C, La Parra-Casado D, Estevez JF, Sanz-barbero B. Intimate partner violence against women during the COVID-19 lockdown in Spain. Int J Environ Res Public Health. (2021) 18:4698. doi: 10.3390/ijerph18094698
82. Iob E, Steptoe A, Fancourt D. Abuse, self-harm and suicidal ideation in the UK during the COVID-19 pandemic. Br J Psychiatry. (2020) 217:543–6. doi: 10.1192/bjp.2020.130
83. Bradbury-Jones C, Isham L. The pandemic paradox: the consequences of COVID-19 on domestic violence. J Clin Nurs. (2020) 29:2047–9. doi: 10.1111/jocn.15296
84. Das M, Das A, Mandal A. Examining the impact of lockdown (due to COVID-19) on Domestic Violence (DV): an evidences from India. Asian J Psychiatr. (2020) 54:102335. doi: 10.1016/j.ajp.2020.102335
Keywords: pandemic, domestic, intimate, partner, violence, abuse, COVID-19
Citation: Thiel F, Büechl VCS, Rehberg F, Mojahed A, Daniels JK, Schellong J and Garthus-Niegel S (2022) Changes in Prevalence and Severity of Domestic Violence During the COVID-19 Pandemic: A Systematic Review. Front. Psychiatry 13:874183. doi: 10.3389/fpsyt.2022.874183
Received: 11 February 2022; Accepted: 21 March 2022;
Published: 13 April 2022.
Edited by:
Ravi Philip Rajkumar, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), IndiaReviewed by:
Obasanjo Afolabi Bolarinwa, University of KwaZulu Natal, South AfricaCopyright © 2022 Thiel, Büechl, Rehberg, Mojahed, Daniels, Schellong and Garthus-Niegel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susan Garthus-Niegel, c3VzYW4uZ2FydGh1cy1uaWVnZWxAdW5pa2xpbmlrdW0tZHJlc2Rlbi5kZQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.