
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Psychiatry, 21 April 2022
Sec. Public Mental Health
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.874128
This article is part of the Research TopicSystematic Reviews of Pharmacological and Non-Pharmacological Psychiatric InterventionsView all 10 articles
 Zuzana Stuchlíková1,2,3
Zuzana Stuchlíková1,2,3 Monika Klírová1,2*
Monika Klírová1,2*
Transcranial direct current stimulation (tDCS) is a non-invasive neurostimulation method that utilizes the effect of low-current on brain tissue. In recent years, the effect of transcranial direct current stimulation has been investigated as a therapeutic modality in various neuropsychiatric indications, one of them being schizophrenia. This article aims to provide an overview of the potential application and effect of tDCS in treating patients with schizophrenia. A literature search was performed using the PubMed, Web of Science, and Google Scholar databases for relevant research published from any date until December 2021. Eligible studies included those that used randomized controlled parallel-group design and focused on the use of transcranial direct current stimulation for the treatment of positive, negative, or cognitive symptoms of schizophrenia. Studies were divided into groups based on the focus of research and an overview is provided in separate sections and tables in the article. The original database search yielded 705 results out of which 27 randomized controlled trials met the eligibility criteria and were selected and used for the purpose of this article. In a review of the selected trials, transcranial direct current stimulation is a safe and well-tolerated method that appears to have the potential as an effective modality for the treatment of positive and negative schizophrenic symptoms and offers promising results in influencing cognition. However, ongoing research is needed to confirm these conclusions and to further specify distinct application parameters.
Schizophrenia is a serious mental illness with an average lifetime prevalence of 6.35 per 1,000 persons (1). Symptoms of schizophrenia may be divided into separate clusters in three main domains that are represented by positive, negative, and cognitive symptoms. Whereas the pharmacological approach is effective mainly in the treatment of positive symptoms, it shows only small benefits in treating negative and cognitive symptoms (2). This is one of the reasons why the scientific focus remains on researching and improving new treatment options and therapeutic modalities. Attenuated cortical activity in prefrontal regions, i.e., hypofrontality (3, 4), and altered inter and intrahemispheric connectivity were described in individuals diagnosed with schizophrenia (5). Frontotemporal and frontoparietal disconnectivity is associated with negative (3, 6) and positive symptoms (3, 7). Hypoactivity of the prefrontal cortex and the disruption of its connection with temporoparietal and contralateral regions were described in relation to the cognitive symptoms (8–10). One of the treatment methods researched for schizophrenia is transcranial direct current stimulation (tDCS) due to its possible effects on the described disrupted cortical mechanisms.
Transcranial direct current stimulation is a non-invasive neuromodulation method based on the use of low-intensity direct current (usually 1–2 mA) and its effect on brain tissue (11). The direct current generated between the surface of electrodes (anode and cathode) placed on the scalp creates cortical changes dependent on the polarity of the applied current. During anodal tDCS (located under the anode), the depolarization of neuronal membranes occurs and thus the cortical excitability rises, meanwhile cathodal tDCS (under the cathode) has the opposite effect (12). Albeit the precise mechanism of the post-modulatory effect of tDCS remains not fully clarified, studies show that direct current stimulation may influence synaptic plasticity and affect remote brain regions by acting on non-synaptic axonal levels (13). The post-modulatory effect on the synaptic level is mediated through the alteration of Ca2+- dependent channels of N-methyl-D-aspartate (NMDA) and amino-3-hydroxy-5-methyl-4-isoxazolepropionate (AMPA) receptors and also through modulating GABA and its interaction with the glutamatergic system (12). These processes further influence brain-derived neutotrophic factor (BDNF) production leading to long-term potentiation (anodal tDCS) or depression (cathodal tDCS) (14, 15), and produce post-modulatory synaptic changes, with long-term potentiation strengthening connections between neurons and long-term depression weakening them (16). Recent research shows BDNF polymorphism to have an impact on the subject sensitivity to tDCS effects (17, 18). Other studies demonstrate a non-synaptic mechanism of tDCS after-effects based on changes in neuronal membrane function (19). tDCS also shows the ability to interfere with functional connectivity, synchronization, and oscillatory action of different cortical and subcortical neuronal networks (16, 17). Additional line of research focuses on possible immunomodulatory effects of tDCS and their importance in overall outcomes (20, 21). Furthermore, tDCS is considered to is considered to also act through induced epigenetic changes, such as histone acetylation and methylation (22, 23).
In recent years, tDCS has been explored as a possible treatment modality for a number of neurological and neuropsychiatric disorders (16, 24). Some of the areas of focus for tDCS application include neurodegenerative diseases such as Parkinson’s disease (25), motor rehabilitation (26), or cognitive improvement (27). One of the investigated disorders in connection to tDCS is also schizophrenia. Previous reviews mainly focused on tDCS efficacy in separate schizophrenic symptom groups such as auditory hallucinations (AH) (28), negative and cognitive symptoms (29, 30). This literature review focuses specifically on the therapeutic application of tDCS in patients with schizophrenia and aims to provide a comprehensive review of tDCS application and its effect on all schizophrenic symptom clusters. Contrary to recent guidelines (24), studies focusing on cognitive function in patients with schizophrenia were also included in this review.
For the purpose of this review, a systematic literature search was performed using electronic databases, namely PubMed and Web of Science, and the Google Scholar search engine. The database search was performed on August 4th and on December 14th, 2021. The second search was performed to identify as recently published trials as possible, providing one additionally selected study. With the use of Boolean operators (tdcs OR “transcranial direct current stimulation” OR “direct current stimulation”) AND (schizophrenia OR “schizophrenic disorder” OR schizophrenic) the search yielded 318 results in the Pubmed database and 381 results in the Web of Science database. The filter to exclude meeting abstracts was used in the search. Subsequently, the Google Scholar search engine was used to identify six more sources from the last year not yet available in the databases.
Inclusion criteria were determined based on the population, intervention, control group, study design, and language used for publication. The population included adults diagnosed with schizophrenia or schizoaffective disorder. The intervention was defined as the use of tDCS for the treatment of positive, negative, or cognitive symptoms of schizophrenia. The control group was set as a sham tDCS application. The study design included randomized blinded studies with parallel arms, therefore excluding any open-label or cross-over trials. Only trials published in English were included. A total of 705 search results were screened based on the titles and/or abstracts. If a trial met inclusion criteria, the full text of the article was retrieved. Full texts were read and reviewed by the first investigator (ZS) with supervision by the senior investigator (MK) who provided subsequent clarification if necessary. Twenty-seven clinical trials were selected following the previously described procedure. A PRISMA flow diagram is available in the Supplementary Material.
Selected trials underwent qualitative analysis. Trials were divided into three groups based on the primary focus on positive, negative, or cognitive symptoms. Studies were categorized into the positive symptom group if the outcomes focused on changes in AH or PANSS total and positive scores. The negative symptom group included outcomes measured by SANS or PANSS negative score. Trials in the cognitive symptom group focused on changes in at least one observed cognitive outcome. Specific stimulation parameters such as total number and frequency of tDCS applications, electrode positioning, and intensity of the electrical current were assessed for each trial. The number of participants in both active and sham stimulation was identified. And primary and secondary clinical outcomes were highlighted. All the information was recorded in comprehensive tables.
The risk of bias was assessed for each of the included trials using the revised Cochrane risk of bias assessment tool (31).
Selected studies focused on the possible effect of tDCS application on the frontotemporal and bifrontal disconnectivity in schizophrenia and on ameliorating schizophrenic symptoms. Different positioning of the electrodes and stimulation protocols were explored. Most of the randomized controlled trials (RCTs) focused on the clinical effect of the stimulation, some of the research also focused on functional changes in distinct brain areas.
Treatment in schizophrenia is often focused on reducing AH as they are frequently present in patients and are often refractory to antipsychotic drugs. Eight of the identified RCTs focused on the reduction of AH as the primary outcome. Two additional trials investigated the effect of tDCS on the reduction of AH in relation to possible modulation of the disrupted neuronal processes in schizophrenia. All 10 studies used similar electrode placement with the anode positioned over the left prefrontal cortex and the cathode over the temporoparietal area. In addition, one study used a bilateral form of stimulation with the second pair of electrodes placed over corresponding contralateral positions (32). All of the studies used the current intensity of 2 mA.
Most of the studies applied tDCS twice daily on five consecutive days (33–39). Two protocols chose to apply stimulation only once per day (32, 40), and two protocols continued to administer stimulation for several weeks (32, 41).
The selected RCT studies do not provide consistent results regarding the efficacy of tDCS on AH intensity. A 2012 study (33) was one of the first to show a significant effect of tDCS in this indication. The effect on AH was also documented in five other studies (34–36, 39, 41). As a secondary outcome, the stimulation protocols reduced the Positive and Negative Syndrome Scale (PANSS) scores (33), and an improvement in working memory was described (41).
Four of the selected studies failed to demonstrate a significant effect of active tDCS stimulation on AH, despite a sufficient sample size and statistical significance being reached (32, 37, 38, 40). Furthermore, two of these RCT studies failed to confirm a significant effect in favor of active stimulation over placebo on any other of the observed symptoms (38, 40). The largest negative study in influencing AH, however, documents improvement in the observed PANSS score and in the level of insight (37). Data from this study were additionally analyzed in two subsequent publications (42, 43). The first paper commented on a trend-level improvement in planning ability, and further specified the positive trends in PANSS score change, where the amelioration of total and general psychopathology did not reach statistical significance compared to sham stimulation (42). The publication in the following year focused on the observed temporary improvement in insight, treatment adherence, and psychological domain of quality of life (43).
Increased activity in the frontal and temporoparietal cortex was previously described in relation to AH (44). A 2016 study (35) showed the effect of tDCS on the resting-state functional connectivity between the frontal and temporoparietal cortex. The reduction of aberrant connectivity positively correlated with the reduction of AH severity (35). These findings may help clarify the positive effect of the preferred frontotemporal stimulation used to improve AH. Subsequent analysis of brain activity in a selected sample from the previous study suggested that the strength of the tDCS-induced electric field reaching the left transverse temporal gyrus may have an important influence on the outcome of frontotemporal stimulation (45).
Impairment of the ability to distinguish between self-generated events and external stimuli was also described in relation to AH in patients with schizophrenia (46). One of the studies showed frontotemporal stimulation to be effective in improving the source-monitoring ability and the improvement positively correlated with a reduction in AH severity (34). A study published in 2019 (47) also explored tDCS application and its ability to influence source-monitoring deficits in a sample of subjects from the 2018 study (36), the findings documented improvement in corollary discharge.
An overview of the selected RCT studies, stimulation parameters, and observed effects is provided in Table 1.
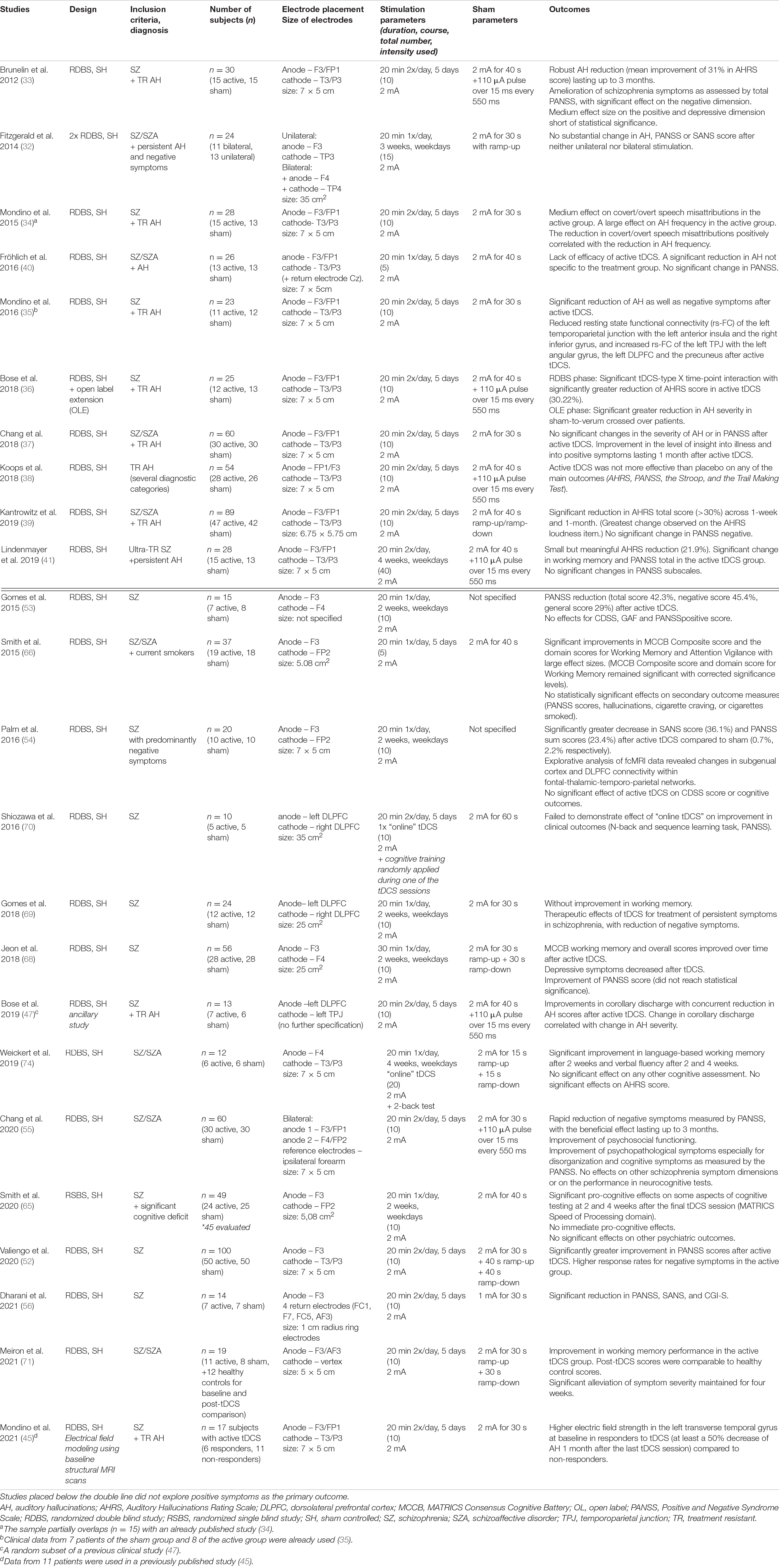
Table 1. Effects of tDCS on positive symptoms.
Key negative symptoms of schizophrenia include blunted affect, alogia, anhedonia, asociality, and avolition (48). Negative symptoms may present as one of the first symptoms of schizophrenia (49) and most antipsychotic drugs have a limited effect on their treatment (50). The search yielded five RCT studies mainly focusing on tDCS application as a possible treatment for negative symptoms. All of the trials demonstrated active stimulation to be at least partially effective in improving the observed outcomes. Based on the assumed association between negative symptoms and neurobiological correlates in the prefrontal cortex (51), the anode was positioned over the corresponding area in all of the studies. One trial protocol placed the cathode over the ipsilateral temporoparietal cortex (52), two over the contralateral prefrontal cortex (53, 54), one protocol used bi-anodal stimulation of the prefrontal cortex bilaterally with cathodes placed on the forearms (55), and one trial used high definition tDCS (HD-tDCS) with four return electrodes positioned around the anode (56). This was the only study using HD-tDCS to be included in this review. All of the selected studies used current intensity of 2 mA for stimulation.
The study using bi-anodal stimulation presented positive outcomes in psychosocial functioning and ameliorated disorganization and cognitive symptoms as measured by PANSS (55). This study showed a rapid reduction in negative symptoms with the beneficial effect lasting up to 3 months (55). Further data analysis, published 1 year later, also documented a significant enhancement of insight and beliefs about medication compliance (57).
In terms of the amelioration of negative symptoms, a 36% reduction in the SANS score (54) and a 45% reduction in the PANSS negative score (53) was described in trials using electrode montage with the cathode placed over the right prefrontal cortex. A significant SANS and PANSS reduction were also documented in a study with HD-tDCS stimulation (56).
A study with frontotemporal electrode montage presented a significantly greater reduction in negative symptoms and the total PANSS score after active stimulation compared to the sham (52). As a secondary outcome, the effect of tDCS on cognitive performance was evaluated in the majority of participants, and no beneficial effect was shown in favor of active stimulation over placebo (58).
Detailed information on the studies mentioned in this section is provided in Table 2.
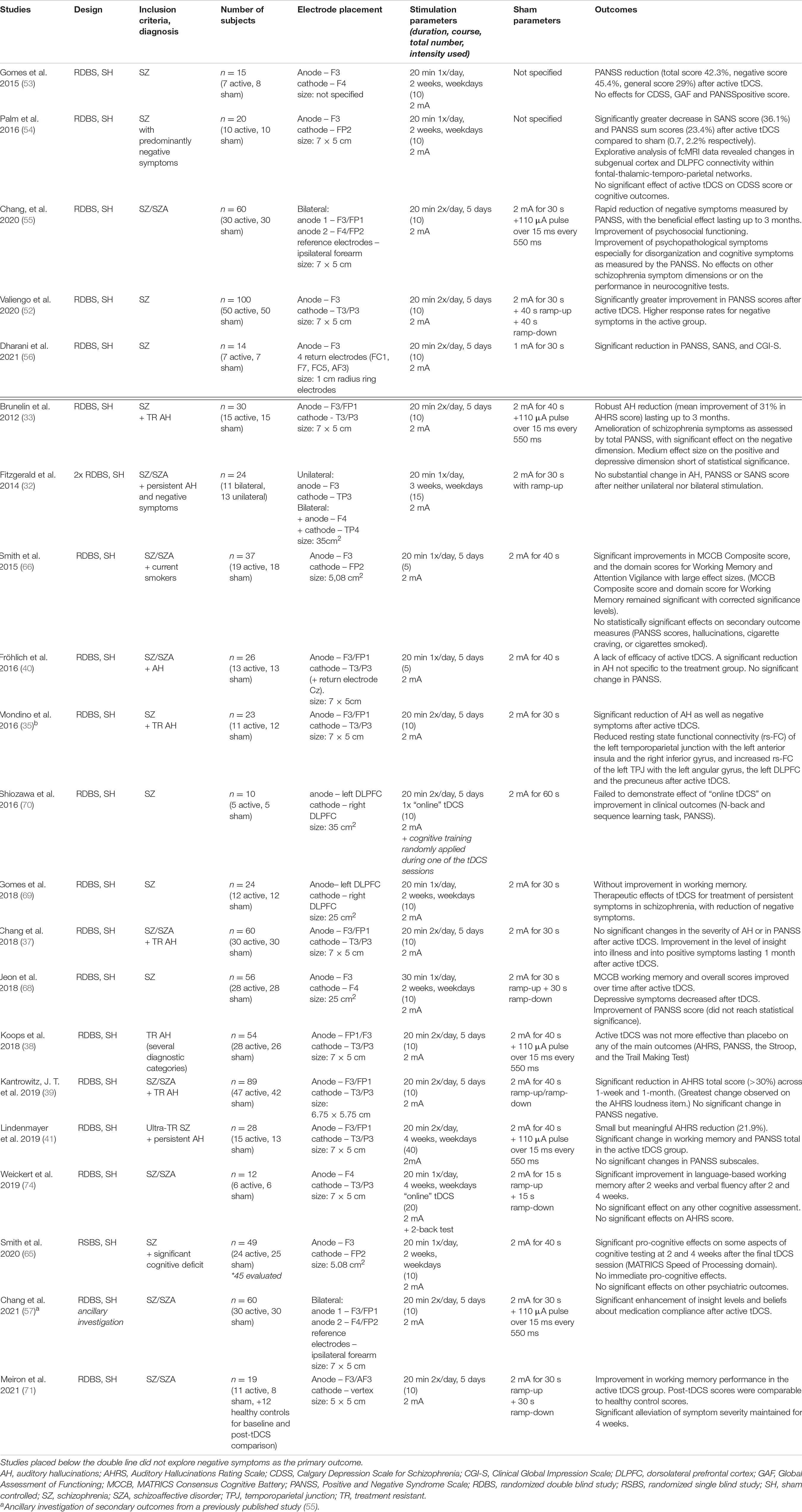
Table 2. Effects of tDCS on negative symptoms.
Cognitive impairment is one of the main intervention targets in the treatment of schizophrenia. Cognitive impairment evolves even before the onset of schizophrenia (prodromal phase), is observable in most patients in the first episode, often persists during symptomatic remissions, and is relatively stable across time (59). Important domains of cognitive deficit in schizophrenia include deficits in working memory, executive functions, attention, and speech (60). However, generalized impairment of various cognitive functions has been described (61). The search identified twelve RTCs with the primary focus on influencing cognitive functions. The selected studies do not provide entirely consistent results, two-thirds of them, nonetheless, reported at least partial improvement in the observed cognitive domains. Anodal tDCS over the left prefrontal cortex appears to be a promising method for improving cognition in neuropsychiatric disorders (11). Most of the studies chose this type of stimulation with the cathode located above the contralateral orbitofrontal area (62–67), contralateral prefrontal area (68–70), or vertex (71). One study placed the anode over the right prefrontal cortex, and one protocol used bi-anodal and bi-cathodal stimulation in the prefrontal area (72). The current intensity of 2 mA was used in all of the studies, except for one trial which applied a lower current intensity of 1 mA (64).
Three studies investigated the cognitive outcomes after a single application of tDCS (63, 67, 72). Only one of them, using bi-anodal stimulation, reported a positive effect on one of the observed parameters, which was emotion identification (72). A second study remained without any positive effect of tDCS on initially significantly reduced visual processing speed and visual short-term memory storage capacity in patients with schizophrenia, and even considered the possibility that tDCS may interfere with practice-dependent improvements in the rate of visual information uptake (67). A third study described a possible impairment of response inhibition after a single tDCS session (63).
Likewise, two of the protocols with multiple tDCS applications – specifically with bi-frontal electrode placement – did not find a significant effect on cognition (69, 70). However, one of the trials reported therapeutic effects of tDCS for the treatment of persistent symptoms in schizophrenia, with a reduction of negative symptoms (69). The applied electrode positioning was the same as in a similar study from 2015 that was reported previously in the section on negative symptoms (53).
The remaining studies with multiple tDCS applications yielded positive results in affecting cognitive functions. Other positive effects of repeated stimulation regimens included a reduction in the PANSS score (68, 71) and alleviation of depressive symptoms (68). Functional magnetic resonance imaging was acquired during tDCS stimulation from some of the participants in a study with a positive effect on working memory (62). Increased activity in the medial prefrontal cortex below the anode was positively correlated with improved working memory, and decreased activity in the anterior cingulate cortex was associated with improved performance on the executive function task, further suggesting the procognitive effects of tDCS applied over the frontal area (73).
A total of four studies used “online” tDCS application, where stimulation is applied at the time of ongoing cognitive training (62, 64, 70, 74). In two cases, “online” tDCS took place during all (74) or more than half of the cognitive training sessions (64). The remaining studies applied stimulation only during one (70) or two appointments (62). By activating the prefrontal cortex, the trials anticipated augmentation of the cognitive training.
An overview of the tDCS use for cognitive symptoms in schizophrenia is provided in Table 3.
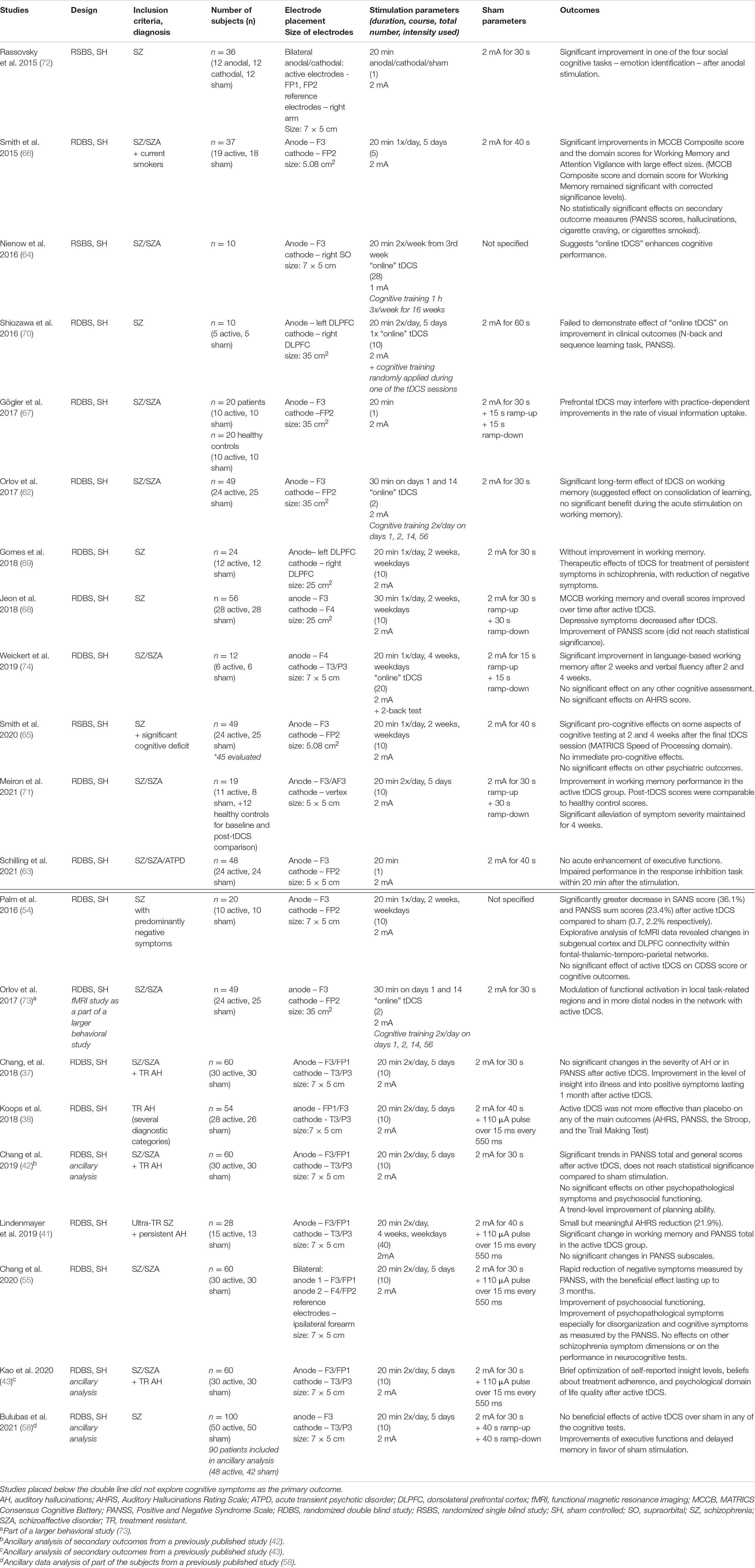
Table 3. Effects of tDCS on cognitive symptoms.
None of the studies reported any serious adverse effects. The most common side effects (SE) documented in the trials included skin redness, tingling or itching sensation under the electrodes, moderate fatigue, tiredness, and headache, all of which were usually well-tolerated and of a mild and transient character. Mostly, there was no significant difference in frequency of SE between active and sham tDCS groups, except for skin redness and a burning sensation under the electrodes with higher frequency in the active tDCS group, which was documented in some of the papers (38, 52, 65). According to recent reviews, there is no evidence for irreversible injury produced by conventional tDCS protocols within a wide range of stimulation parameters (75) and within standard protocols, tDCS is considered a safe method (76).
The Cochrane risk of bias assessment tool was used to evaluate the methodological quality of each trial. Study quality assessment included randomization process, deviations from the intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each domain was scored as “low risk,” “some concerns,” or “high risk.” The level of the risk of bias varied across studies. The most common potential causes of bias were the insufficient description of the randomization and blinding process, dealing with missing data, and unavailability of pre-specified analysis plan (i.e., study protocol) which led to scoring as “some concerns.” A significant number of studies did not provide a sufficient description of blinding of staff delivering intervention and assessors of outcome measures, or did not describe the method used for randomization other than stating the participants were randomized (33–35, 37, 41, 53, 62, 64, 70–72). One of the studies reported only partial effectiveness of blinding since both subjects and testers could correctly guess that the sham group received sham stimulation in most of their guesses (65). There was also missing outcome data in a larger part of the trials mainly due to discontinuation of participants, leading to scoring as “some concerns” in the domain (37, 38, 41, 53, 56, 62, 64–66, 68–72, 74). None of the reviewed studies scored “high” in the overall risk of bias.
This is an up-to-date review article offering a cross-section of current research with a focus on tDCS application in schizophrenia. Following a standardized literature search, we identified 27 randomized controlled trials. A total of 966 patients diagnosed with schizophrenia or schizoaffective disorder participated in these clinical trials. As a primary aim, ten trials examined the effects of tDCS on positive symptoms with six of them yielding positive results. All five trials focusing primarily on negative symptoms showed some improvement in the measured outcomes. Twelve trials explored the impact of tDCS on cognitive functions and out of those, eight trials report beneficial effects in at least one measured aspect of cognition. Overall, we could not establish a reporting bias.
The reviewed studies differed considerably in the experimental design and stimulation protocols. However, all of the clinical trials selected the anode placement to be over the prefrontal cortex. This may be explained by the effort to positively influence the aforementioned attenuated prefrontal activity that is seen in patients with schizophrenia. Nonetheless, the differences between the cortical activity in early-course and chronic schizophrenia may be of consideration in connection to the anode placement. A previous study suggests a difference in the activity of the prefrontal cortex among early-course schizophrenic patients in contrast to attenuation of the activity that is commonly described in patients with chronic illness (77). In such cases, the activation of prefrontal regions by the anodal transcranial stimulation may not be beneficial. None of the reviewed studies reported using neuronavigation for exact electrode positioning, most of them referred to the 10-20 EEG system frequently used for tDCS electrode montage. Nonetheless, due to inter-personal brain variability this method leads to limited targeting accuracy (78). Although neuronavigation methods are not commonplace outside highly specialized research centers, their future implementation could mean achieving more effective stimulation and consequently better clinical outcomes. Another element of tDCS application to consider is the duration of active stimulation. The vast majority of the selected trials used 20 min of stimulation, and only three of them chose to prolong the stimulation up to 30 min. Current research suggests that the effect of anodal tDCS may not be directly proportional to the duration of the active stimulation, and may on the contrary decrease or even reverse with prolonged stimulation (79, 80). However, the studies included in the review that used a 30-min protocol provided positive outcomes with all of them focusing on cognitive measures. Further exploration of the exact electrode placement and duration of the stimulation should be considered in future studies. Additionally, number of sessions in repeated tDCS application protocols and the repetition interval is an important factor to examine. Studies included in this review used stimulation protocols with tDCS applied once or twice daily, usually separating the two stimulation sessions by 2–3 h. Twice-a-day stimulation is used in order to strengthen the effect. Repeated application protocols offer significant opportunities for induction of long-lasting and significant neuroplastic change (81). However, specific timing of repetition intervals is important for optimizing cumulative effects of tDCS (82). Previously published studies indicate that short repetition interval (<30 min) can lead to prolongation of tDCS after-effects (81–83), whereas longer repetition interval (3 or 24 h) result in no excitability-enhancing after effects or can nullify them (83, 84). Current research focuses on accelerated tDCS protocols (85, 86), and future RCT protocols using tDCS as a treatment option for schizophrenia might benefit from their implementation.
In recent years, the emphasis is also placed on gender differences. Brain anatomy, chemistry, and function differ in relation to sex, leading to differences in response to neurostimulation methods in men and women (87, 88). These issues have been addressed and explored in recent studies (89–91). Some of the studies included in this review controlled for potential confounding effects of male to female ratio in trial groups, however, none of them specifically focused on the various effects of tDCS in connection to gender. There was also no consideration of altering stimulation protocols according to sex-related brain differences or examining response to tDCS in women and men separately. In the future, closer exploration of gender-tailored stimulation protocols might be of interest.
The clinical trials included in the review considerably differ in sample size. As the outcomes are not consistent, this makes it difficult to offer clear recommendations for future research. The differences in methodologies, experimental design, and protocols are considerable limitations for selecting an appropriate and most effective design for future trials. More studies with a clear design and robust sample size are needed to better evaluate the clinical effects and possible application of tDCS in treating patients with schizophrenia.
This review has several limitations. Firstly, only randomized controlled double-blind parallel trials were included, which decreased the total number of reviewed studies. Open-label and cross-over studies may play an important role in an overall assessment of tDCS efficacy, and future reviews may consider their inclusion. Secondly, we did not perform a meta-analysis of the selected research, as this article only brings a qualitative overview, and therefore statistical data are not offered for the overall assessment.
This review provides a summary of current research on tDCS application in patients suffering from schizophrenia. Albeit the 2017 guidelines (16) exclude some of the sources on the use of tDCS in schizophrenia as poor evidence, current guidelines list tDCS as a Level B (Probably effective) therapeutic method for the treatment of AH and positive/negative symptoms (24). This review also focused on tDCS application as a treatment for cognitive schizophrenic symptoms, where tDCS appears to be a promising therapeutic method. However, ongoing research is needed to confirm these conclusions and to further specify distinct application parameters.
ZS: conceptualization, methodology, investigation, and writing—original draft preparation. MK: conceptualization, methodology, investigation, supervision, writing—reviewing, and editing. Both authors: contributed to the article and approved the submitted version.
This review was supported by the grant PharmaBrain No. CZ.02.1.01/0.0/0.0/16_0250007444.
ZS was employed by the company Hospital České Budĕjovice, a.s.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.874128/full#supplementary-material
Supplementary Figure 1 | PRISMA 2020 flow diagram for new systematic reviews, which included searches of databases, registers, and other sources [A LiteratureMini-Review of Transcranial Direct Current Stimulation (tDCS) in Schizophrenia]. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit http://www.prisma- statement.org/.
1. Simeone JC, Ward AJ, Rotella P, Collins J, Windisch R. An evaluation of variation in published estimates of schizophrenia prevalence from 1990-2013: a systematic literature review. BMC Psychiatry. (2015) 15:193. doi: 10.1186/s12888-015-0578-7
2. McCutcheon RA, Reis Marques T, Howes OD. Schizophrenia – an overview. JAMA Psychiatry. (2020) 77:201–10.
3. Andreasen NC, O’Leary DS, Flaum M, Nopoulos P, Watkins GL, Boles Ponto LL, et al. Hypofrontality in schizophrenia: distributed dysfunctional circuits in neuroleptic-naive patients. Lancet. (1997) 349:1730–4. doi: 10.1016/s0140-6736(96)08258-x
4. Weinberger DR, Egan MF, Bertolino A, Callicott JH, Mattay VS, Lipska BK, et al. Prefrontal neurons and the genetics of schizophrenia. Biol Psychiatry. (2001) 50:825–44. doi: 10.1016/s0006-3223(01)01252-5
5. Schmitt A, Hasan A, Gruber O, Falkai P. Schizophrenia as a disorder of disconnectivity. Eur Arch Psychiatry Clin Neurosci. (2011) 261(SUPPL. 2):150–4. doi: 10.1007/s00406-011-0242-2
6. Galderisi S, Merlotti E, Mucci A. Neurobiological background of negative symptoms. Eur Arch Psychiatry Clin Neurosci. (2015) 265:543–58. doi: 10.1007/s00406-015-0590-4
7. Ford JM, Mathalon DH. Corollary discharge dysfunction in schizophrenia: can it explain auditory hallucinations? Int J Psychophysiol. (2005) 58:179–89. doi: 10.1016/j.ijpsycho.2005.01.014
8. Glahn DC, Ragland JD, Abramoff A, Barrett J, Laird AR, Bearden CE, et al. Beyond hypofrontality: a quantitative meta-analysis of functional neuroimaging studies of working memory in schizophrenia. Hum Brain Mapp. (2005) 25:60–9. doi: 10.1002/hbm.20138
9. Adhikari BM, Hong LE, Sampath H, Chiappelli J, Jahanshad N, Thompson PM, et al. Functional network connectivity impairments and core cognitive deficits in schizophrenia. Hum Brain Mapp. (2019) 40:4593–605. doi: 10.1002/hbm.24723
10. Lesh TA, Niendam TA, Minzenberg MJ, Carter CS. Cognitive control deficits in schizophrenia: mechanisms and meaning. Neuropsychopharmacology. (2011) 36:316–8. doi: 10.1038/npp.2010.156
11. Hoy KE, Fitzgerald PB. Brain stimulation in psychiatry and its effects on cognition. Nat Publ Gr. (2010) 6:267–75. doi: 10.1038/nrneurol.2010.30
12. Brunoni AR, Nitsche MA, Bolognini N, Bikson M, Wagner T, Merabet L, et al. Clinical research with transcranial direct current stimulation (tDCS): challenges and future directions. Brain Stimul. (2012) 5:175–95. doi: 10.1016/j.brs.2011.03.002
13. Nitsche MA, Cohen LG, Wassermann EM, Priori A, Lang N, Antal A, et al. Transcranial direct current stimulation: state of the art 2008. Brain Stimul. (2008) 1:206–2. doi: 10.1016/j.brs.2008.06.004
14. Fritsch B, Reis J, Martinowich K, Schambra HM, Ji Y, Cohen LG, et al. Direct current stimulation promotes BDNF-dependent synaptic plasticity: potential implications for motor learning. Neuron. (2010) 66:198–204. doi: 10.1016/j.neuron.2010.03.035
15. Medeiros LF, de Souza ICC, Vidor LP, de Souza A, Deitos A, Volz MS, et al. Neurobiological effects of transcranial direct current stimulation: a review. Front Psychiatry. (2012) 3:110. doi: 10.3389/fpsyt.2012.00110
16. Lefaucheur JP, Antal A, Ayache SS, Benninger DH, Brunelin J, Cogiamanian F, et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin Neurophysiol. (2017) 128:56–92. doi: 10.1016/j.clinph.2016.10.087
17. Polanía R, Nitsche MA, Ruff CC. Studying and modifying brain function with non-invasive brain stimulation. Nat Neurosci. (2018) 21:174–87. doi: 10.1038/s41593-017-0054-4
18. Fridriksson J, Elm J, Stark BC, Basilakos A, Rorden C, Sen S, et al. BDNF genotype and tDCS interaction in aphasia treatment. Brain Stimul. (2018) 11:1276–81. doi: 10.1016/j.brs.2018.08.009
19. Ardolino G, Bossi B, Barbieri S, Priori A. Non-synaptic mechanisms underlie the after-effects of cathodal transcutaneous direct current stimulation of the human brain. J Physiol. (2005) 568:653–3. doi: 10.1113/jphysiol.2005.088310
20. Pelletier SJ, Cicchetti F. Cellular and molecular mechanisms of action of transcranial direct current stimulation: evidence from in vitro and in vivo models. Int J Neuropsychopharmacol. (2015) 18:1–13. doi: 10.1093/ijnp/pyu047
21. Rabenstein M, Unverricht-Yeboah M, Keuters MH, Pikhovych A, Hucklenbroich J, Vay SU, et al. Transcranial current stimulation alters the expression of immune-mediating genes. Front Cell Neurosci. (2019) 13:461. doi: 10.3389/fncel.2019.00461
22. Podda MV, Cocco S, Mastrodonato A, Fusco S, Leone L, Barbati SA, et al. Anodal transcranial direct current stimulation boosts synaptic plasticity and memory in mice via epigenetic regulation of BDNF expression. Sci Rep. (2016) 6:1–19. doi: 10.1038/srep22180
23. Wiegand A, Blickle A, Brückmann C, Weller S, Nieratschker V, Plewnia C. Dynamic DNA methylation changes in the comt gene promoter region in response to mental stress and its modulation by transcranial direct current stimulation. Biomolecules. (2021) 11:1726. doi: 10.3390/biom11111726
24. Fregni F, El-Hagrassy MM, Pacheco-Barrios K, Carvalho S, Leite J, Simis M, et al. Evidence-based guidelines and secondary meta-analysis for the use of transcranial direct current stimulation in neurological and psychiatric disorders. Int J Neuropsychopharmacol. (2021) 24:256–313. doi: 10.1093/ijnp/pyaa051
25. Liu X, Liu H, Liu Z, Rao J, Wang J, Wang P, et al. Transcranial direct current stimulation for Parkinson’s disease: a systematic review and meta-analysis. Front Aging Neurosci. (2021) 13:746797. doi: 10.3389/fnagi.2021.746797
26. Mitsutake T, Imura T, Hori T, Sakamoto M, Tanaka R. Effects of combining online anodal transcranial direct current stimulation and gait training in stroke patients: a systematic review and meta-analysis. Front Hum Neurosci. (2021) 15:782305. doi: 10.3389/fnhum.2021.782305
27. Siegert A, Diedrich L, Antal A. New methods, old brains—a systematic review on the effects of tDCS on the cognition of elderly people. Front Hum Neurosci. (2021) 15:730134.
28. Guttesen LL, Albert N, Nordentoft M, Hjorthøj C. Repetitive transcranial magnetic stimulation and transcranial direct current stimulation for auditory hallucinations in schizophrenia: systematic review and meta-analysis. J Psychiatr Res. (2021) 143:163–75. doi: 10.1016/j.jpsychires.2021.09.001
29. Narita Z, Stickley A, DeVylder J, Yokoi Y, Inagawa T, Yamada Y, et al. Effect of multi-session prefrontal transcranial direct current stimulation on cognition in schizophrenia: a systematic review and meta-analysis. Schizophr Res. (2020) 216:367–73. doi: 10.1016/j.schres.2019.11.011
30. Yu L, Fang X, Chen Y, Wang Y, Wang D, Zhang C. Efficacy of transcranial direct current stimulation in ameliorating negative symptoms and cognitive impairments in schizophrenia: a systematic review and meta-analysis. Schizophr Res. (2020) 224:2–10. doi: 10.1016/j.schres.2020.10.006
31. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
32. Fitzgerald PB, McQueen S, Daskalakis ZJ, Hoy KE. A negative pilot study of daily bimodal transcranial direct current stimulation in schizophrenia. Brain Stimul. (2014) 7:813–6. doi: 10.1016/j.brs.2014.08.002
33. Brunelin J, Mondino M, Gassab L, Haesebaert F, Gaha L, Suaud-Chagny MF, et al. Examining transcranial direct-current stimulation (tDCS) as a treatment for hallucinations in schizophrenia. Am J Psychiatry. (2012) 169:719–24. doi: 10.1176/appi.ajp.2012.11071091
34. Mondino M, Haesebaert F, Poulet E, Suaud-Chagny MF, Brunelin J. Fronto-temporal transcranial Direct Current Stimulation (tDCS) reduces source-monitoring deficits and auditory hallucinations in patients with schizophrenia. Schizophr Res. (2015) 161:515–6. doi: 10.1016/j.schres.2014.10.054
35. Mondino M, Jardri R, Suaud-Chagny MF, Saoud M, Poulet E, Brunelin J. Effects of fronto-temporal transcranial direct current stimulation on auditory verbal hallucinations and resting-state functional connectivity of the left temporo-parietal junction in patients with schizophrenia. Schizophr Bull. (2016) 42:318–26. doi: 10.1093/schbul/sbv114
36. Bose A, Shivakumar V, Agarwal SM, Kalmady SV, Shenoy S, Sreeraj VS, et al. Efficacy of fronto-temporal transcranial direct current stimulation for refractory auditory verbal hallucinations in schizophrenia: a randomized, double-blind, sham-controlled study. Schizophr Res. (2018) 195:475–80. doi: 10.1016/j.schres.2017.08.047
37. Chang CC, Tzeng NS, Chao CY, Yeh CB, Chang HA. The effects of add-on fronto-temporal transcranial direct current stimulation (tDCS) on auditory verbal hallucinations, other psychopathological symptoms, and insight in schizophrenia: a randomized, double-blind, sham-controlled trial. Int J Neuropsychopharmacol. (2018) 21:979–87. doi: 10.1093/ijnp/pyy074
38. Koops S, Blom JD, Bouachmir O, Slot MI, Neggers B, Sommer IE. Treating auditory hallucinations with transcranial direct current stimulation in a double-blind, randomized trial. Schizophr Res. (2018) 201:329–6. doi: 10.1016/j.schres.2018.06.010
39. Kantrowitz JT, Sehatpour P, Avissar M, Horga G, Gwak A, Hoptman MJ, et al. Significant improvement in treatment resistant auditory verbal hallucinations after 5 days of double-blind, randomized, sham controlled, fronto-temporal, transcranial direct current stimulation (tDCS): a replication/extension study. Brain Stimul. (2019) 12:981–91. doi: 10.1016/j.brs.2019.03.003
40. Fröhlich F, Burrello TN, Mellin JM, Cordle AL, Lustenberger CM, Gilmore JH, et al. Exploratory study of once-daily transcranial direct current stimulation (tDCS) as a treatment for auditory hallucinations in schizophrenia. Eur Psychiatry. (2016) 33:54–60. doi: 10.1016/j.eurpsy.2015.11.005
41. Lindenmayer JP, Kulsa MKC, Sultana T, Kaur A, Yang R, Ljuri I, et al. Transcranial direct-current stimulation in ultra-treatment-resistant schizophrenia. Brain Stimul. (2019) 12:54–61. doi: 10.1016/j.brs.2018.10.002
42. Chang CC, Kao YC, Chao CY, Chang HA. Enhancement of cognitive insight and higher-order neurocognitive function by fronto-temporal transcranial direct current stimulation (tDCS) in patients with schizophrenia. Schizophr Res. (2019) 208:430–8. doi: 10.1016/j.schres.2018.12.052
43. Kao YC, Tzeng NS, Chao CY, Chang CC, Chang HA. Modulation of self-appraisal of illness, medication adherence, life quality and autonomic functioning by transcranial direct current stimulation in schizophrenia patients. Clin Neurophysiol. (2020) 131:1997–2007. doi: 10.1016/j.clinph.2020.02.029
44. Jardri R, Pouchet A, Pins D, Thomas P. Cortical activations during auditory verbal hallucinations in schizophrenia: a coordinate-based meta-analysis. Am J Psychiatry. (2011) 168:73–81. doi: 10.1176/appi.ajp.2010.09101522
45. Mondino M, Fonteneau C, Simon L, Dondé C, Haesebaert F, Poulet E, et al. Advancing clinical response characterization to frontotemporal transcranial direct current stimulation with electric field distribution in patients with schizophrenia and auditory hallucinations: a pilot study. Eur Arch Psychiatry Clin Neurosci. (2021) 271:85–92. doi: 10.1007/s00406-020-01149-4
46. Waters F, Woodward T, Allen P, Aleman A, Sommer I. Self-recognition deficits in schizophrenia patients with auditory hallucinations: a meta-analysis of the literature. Schizophr Bull. (2012) 38:741–50. doi: 10.1093/schbul/sbq144
47. Bose A, Nawani H, Agarwal SM, Shivakumar V, Kalmady SV, Shenoy S, et al. Effect of fronto-temporal transcranial direct current stimulation on corollary discharge in schizophrenia: a randomized, double-blind, sham-controlled mediation analysis study. Schizophr Res. (2019) 204:411–2. doi: 10.1016/j.schres.2018.07.040
48. Correll CU, Schooler NR. Negative symptoms in schizophrenia: a review and clinical guide for recognition, assessment, and treatment. Neuropsychiatr Dis Treat. (2020) 16:519–34. doi: 10.2147/NDT.S225643
49. An Der Heiden W, Häfner H. The epidemiology of onset and course of schizophrenia. Eur Arch Psychiatry Clin Neurosci. (2000) 250:292–303.
50. Aleman A, Lincoln TM, Bruggeman R, Melle I, Arends J, Arango C, et al. Treatment of negative symptoms: where do we stand, and where do we go? Schizophr Res. (2017) 186:55–62. doi: 10.1016/j.schres.2016.05.015
51. Sanfilipo M, Lafargue T, Rusinek H, Arena L, Loneragan C, Lautin A, et al. Volumetric measure of the frontal and temporal lobe regions in schizophrenia. Arch Gen Psychiatry. (2000) 57:471. doi: 10.1001/archpsyc.57.5.471
52. Valiengo LDCL, Goerigk S, Gordon PC, Padberg F, Serpa MH, Koebe S, et al. Efficacy and safety of transcranial direct current stimulation for treating negative symptoms in schizophrenia: a randomized clinical trial. JAMA Psychiatry. (2020) 77:121–9. doi: 10.1001/jamapsychiatry.2019.3199
53. Gomes JS, Shiozawa P, Dias ÁMH, Valverde Ducos D, Akiba H, Trevizol AP, et al. Left dorsolateral prefrontal cortex anodal tDCS effects on negative symptoms in schizophrenia. Brain Stimul. (2015) 8:989–1. doi: 10.1016/j.brs.2015.07.033
54. Palm U, Keeser D, Hasan A, Kupka MJ, Blautzik J, Sarubin N, et al. Prefrontal transcranial direct current stimulation for treatment of schizophrenia with predominant negative symptoms: a double-blind, sham-controlled proof-of-concept study. Schizophr Bull. (2016) 42:1253–61. doi: 10.1093/schbul/sbw041
55. Chang CC, Kao YC, Chao CY, Tzeng NS, Chang HA. Examining bi-anodal transcranial direct current stimulation (tDCS) over bilateral dorsolateral prefrontal cortex coupled with bilateral extracephalic references as a treatment for negative symptoms in non-acute schizophrenia patients: a randomized, double. Prog Neuro Psychopharmacol Biol Psychiatry. (2020) 96:109715. doi: 10.1016/j.pnpbp.2019.109715
56. Dharani R, Goyal N, Mukherjee A, Umesh S. Adjuvant high-definition transcranial direct current stimulation for negative symptoms in schizophrenia: a pilot study. J ECT. (2021) 37:195–201. doi: 10.1097/YCT.0000000000000756
57. Chang CC, Kao YC, Chao CY, Tzeng NS, Chang HA. The effects of bi-anodal tdcs over the prefrontal cortex regions with extracephalic reference placement on insight levels and cardio-respiratory and autonomic functions in schizophrenia patients and exploratory biomarker analyses for treatment response. Int J Neuropsychopharmacol. (2021) 24:40–53. doi: 10.1093/ijnp/pyaa063
58. Bulubas L, Goerigk S, Gomes JS, Brem A-K, Carvalho JB, Pinto BS, et al. Cognitive outcomes after tDCS in schizophrenia patients with prominent negative symptoms: results from the placebo-controlled STARTS trial. Schizophr Res. (2021) 235:44–51. doi: 10.1016/j.schres.2021.07.008
59. Bozikas VP, Giannakou M, Kosmidis MH, Kargopoulos P, Kioseoglou G, Liolios D, et al. Insights into theory of mind in schizophrenia: the impact of cognitive impairment. Schizophr Res. (2011) 130:130–6. doi: 10.1016/j.schres.2011.04.025
60. Keefe RSE, Harvey PD. Novel antischizophrenia treatments – cognitive impairment in schizophrenia. Handb Exp Pharmacol. (2012) 213:11–37. doi: 10.1007/978-3-642-25758-2
61. Fioravanti M, Bianchi V, Cinti ME. Cognitive deficits in schizophrenia: an updated metanalysis of the scientific evidence. BMC Psychiatry. (2012) 12:64. doi: 10.1186/1471-244X-12-64
62. Orlov ND, Tracy DK, Joyce D, Patel S, Rodzinka-Pasko J, Dolan H, et al. Stimulating cognition in schizophrenia: a controlled pilot study of the effects of prefrontal transcranial direct current stimulation upon memory and learning. Brain Stimul. (2017) 10:560–6. doi: 10.1016/j.brs.2016.12.013
63. Schilling TM, Bossert M, König M, Wirtz G, Weisbrod M, Aschenbrenner S. Acute effects of a single dose of 2 mA of anodal transcranial direct current stimulation over the left dorsolateral prefrontal cortex on executive functions in patients with schizophrenia-a randomized controlled trial. PLoS One. (2021) 16:e0254695. doi: 10.1371/journal.pone.0254695
64. Nienow TM, MacDonald AW, Lim KO. TDCS produces incremental gain when combined with working memory training in patients with schizophrenia: a proof of concept pilot study. Schizophr Res. (2016) 172:218–9. doi: 10.1016/j.schres.2016.01.053
65. Smith RC, Md WL, Wang Y, Jiang J, Wang JJ, Szabo V, et al. Effects of transcranial direct current stimulation on cognition and symptoms in Chinese patients with schizophrenia⋆. Psychiatry Res. (2020) 284:112617. doi: 10.1016/j.psychres.2019.112617
66. Smith RC, Boules S, Mattiuz S, Youssef M, Tobe RH, Sershen H, et al. Effects of transcranial direct current stimulation (tDCS) on cognition, symptoms, and smoking in schizophrenia: a randomized controlled study. Schizophr Res. (2015) 168:260–6. doi: 10.1016/j.schres.2015.06.011
67. Gögler N, Papazova I, Oviedo-Salcedo T, Filipova N, Strube W, Funk J, et al. Parameter-based evaluation of attentional impairments in schizophrenia and their modulation by prefrontal transcranial direct current stimulation. Front Psychiatry. (2017) 8:259. doi: 10.3389/fpsyt.2017.00259
68. Jeon DW, Jung DU, Kim SJ, Shim JC, Moon JJ, Seo YS, et al. Adjunct transcranial direct current stimulation improves cognitive function in patients with schizophrenia: a double-blind 12-week study. Schizophr Res. (2018) 197:378–85. doi: 10.1016/j.schres.2017.12.009
69. Gomes JS, Trevizol AP, Ducos DV, Gadelha A, Ortiz BB, Fonseca AO, et al. Effects of transcranial direct current stimulation on working memory and negative symptoms in schizophrenia: a phase II randomized sham-controlled trial. Schizophr Res Cogn. (2018) 12:20–8. doi: 10.1016/j.scog.2018.02.003
70. Shiozawa P, Gomes JS, Ducos DV, Akiba HT, Dias ÁM, Trevizol AP, et al. Efeito da estimulação transcraniana por corrente contínua (ETCC) sobre o córtex pré-frontal combinada a treinamento cognitivo para o tratamento da esquizofrenia: ensaio clínico randomizado simulação controlado. Trends Psychiatry Psychother. (2016) 38:175–7.
71. Meiron O, David J, Yaniv A. Left prefrontal transcranial direct-current stimulation reduces symptom-severity and acutely enhances working memory in schizophrenia. Neurosci Lett. (2021) 755:135912. doi: 10.1016/j.neulet.2021.135912
72. Rassovsky Y, Dunn W, Wynn J, Wu AD, Iacoboni M, Hellemann G, et al. The effect of transcranial direct current stimulation on social cognition in schizophrenia: a preliminary study. Schizophr Res. (2015) 165:171–4. doi: 10.1016/j.schres.2015.04.016
73. Orlov ND, O’Daly O, Tracy DK, Daniju Y, Hodsoll J, Valdearenas L, et al. Stimulating thought: a functional MRI study of transcranial direct current stimulation in schizophrenia. Brain. (2017) 140:2490–7. doi: 10.1093/brain/awx170
74. Weickert TW, Salimuddin H, Lenroot RK, Bruggemann J, Loo C, Vercammen A, et al. Preliminary findings of four-week, task-based anodal prefrontal cortex transcranial direct current stimulation transferring to other cognitive improvements in schizophrenia. Psychiatry Res. (2019) 280:112487. doi: 10.1016/j.psychres.2019.112487
75. Bikson M, Grossman P, Thomas C, Louis A, Jiang J, Adnan T, et al. Brain stimulation safety of transcranial direct current stimulation: evidence based update 2016. Brain Stimul. (2016) 9:641–1. doi: 10.1016/j.brs.2016.06.004
76. Matsumoto H, Ugawa Y. Adverse events of tDCS and tACS: a review. Clin Neurophysiol Pract. (2017) 2:19–25. doi: 10.1016/j.cnp.2016.12.003
77. Anticevic A, Hu X, Xiao Y, Hu J, Li F, Bi F, et al. Early-course unmedicated schizophrenia patients exhibit elevated prefrontal connectivity associated with longitudinal change. J Neurosci. (2015) 35:267–86. doi: 10.1523/JNEUROSCI.2310-14.2015
78. De Witte S, Klooster D, Dedoncker J, Duprat R, Remue J, Baeken C. Left prefrontal neuronavigated electrode localization in tDCS: 10–20 EEG system versus MRI-guided neuronavigation. Psychiatry Res Neuroimaging. (2018) 274:1–6. doi: 10.1016/j.pscychresns.2018.02.001
79. Vignaud P, Mondino M, Poulet E, Palm U, Brunelin J. Duration but not intensity influences transcranial direct current stimulation (tDCS) after-effects on cortical excitability. Neurophysiol Clin. (2018) 48:89–92. doi: 10.1016/j.neucli.2018.02.001
80. Hassanzahraee M, Nitsche MA, Zoghi M, Jaberzadeh S. Determination of anodal tDCS duration threshold for reversal of corticospinal excitability: an investigation for induction of counter-regulatory mechanisms. Brain Stimul. (2020) 13:832–9. doi: 10.1016/j.brs.2020.02.027
81. Goldsworthy MR, Pitcher JB, Ridding MC. Spaced noninvasive brain stimulation. Neurorehabil Neural Repair. (2015) 29:714–21. doi: 10.1177/1545968314562649
82. Monte-Silva K, Kuo MF, Liebetanz D, Paulus W, Nitsche MA. Shaping the optimal repetition interval for cathodal transcranial direct current stimulation (tDCS). J Neurophysiol. (2010) 103:1735–40. doi: 10.1152/jn.00924.2009
83. Agboada D, Mosayebi-Samani M, Kuo MF, Nitsche MA. Induction of long-term potentiation-like plasticity in the primary motor cortex with repeated anodal transcranial direct current stimulation – Better effects with intensified protocols? Brain Stimul. (2020) 13:987–7. doi: 10.1016/j.brs.2020.04.009
84. Monte-Silva K, Kuo MF, Hessenthaler S, Fresnoza S, Liebetanz D, Paulus W, et al. Induction of late LTP-like plasticity in the human motor cortex by repeated non-invasive brain stimulation. Brain Stimul. (2013) 6:424–32. doi: 10.1016/j.brs.2012.04.011
85. Bystad M, Storø B, Gundersen N, Wiik IL, Nordvang L, Grønli O, et al. Can accelerated transcranial direct current stimulation improve memory functions? An experimental, placebo-controlled study. Heliyon. (2020) 6:0–6. doi: 10.1016/j.heliyon.2020.e05132
86. Mondino M, Poulet E, Brunelin J. Moving to accelerated protocols of tDCS in schizophrenia: a case report. Brain Stimul. (2021) 14:822–4. doi: 10.1016/j.brs.2021.05.006
87. Cahill L. Why sex matters for neuroscience. Nat Rev Neurosci. (2006) 7:477–84. doi: 10.1038/nrn1909
88. Rudroff T, Workman CD, Fietsam AC, Kamholz J. Response variability in transcranial direct current stimulation: why sex matters. Front Psychiatry. (2020) 11:19–22. doi: 10.3389/fpsyt.2020.00585
89. Adenzato M, Brambilla M, Manent R, De Lucia L, Trojano L, Garofalo S, et al. Gender differences in cognitive theory of mind revealed by transcranial direct current stimulation on medial prefrontal cortex. Sci Rep. (2017) 7:41219. doi: 10.1038/srep41219
90. Fehring DJ, Samandra R, Haque ZZ, Jaberzadeh S, Rosa M, Mansouri FA. Investigating the sex – dependent effects of prefrontal cortex stimulation on response execution and inhibition. Biol Sex Differ. (2021) 12:47. doi: 10.1186/s13293-021-00390-3
Keywords: review, neurostimulation, direct current stimulation, tDCS, schizophrenia, schizophrenic
Citation: Stuchlíková Z and Klírová M (2022) A Literature Mini-Review of Transcranial Direct Current Stimulation in Schizophrenia. Front. Psychiatry 13:874128. doi: 10.3389/fpsyt.2022.874128
Received: 11 February 2022; Accepted: 14 March 2022;
Published: 21 April 2022.
Edited by:
Mirko Manchia, University of Cagliari, ItalyReviewed by:
Thorsten Rudroff, The University of Iowa, United StatesCopyright © 2022 Stuchlíková and Klírová. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Monika Klírová, bW9uaWthLmtsaXJvdmFAbnVkei5jeg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.