
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 16 June 2022
Sec. Addictive Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.862858
This article is part of the Research Topic Methods and Applications in Addiction Psychiatry Research: 2021 View all 13 articles
 Asunción Santos-de-Pascual1
Asunción Santos-de-Pascual1 Luis Miguel López-Cano1Mavi Alcántara-López2
Luis Miguel López-Cano1Mavi Alcántara-López2 Antonia Martínez-Pérez2*
Antonia Martínez-Pérez2* Maravillas Castro-Sáez2
Maravillas Castro-Sáez2 Visitación Fernández-Fernández2
Visitación Fernández-Fernández2 Concepción López-Soler2
Concepción López-Soler2The aim of this study is to explore the effects of a residential multimodal treatment intervention for an addict population. We gathered participants from the “Programa Base” (n = 166) of the Solidarity and Reinsertion Foundation of Murcia, and assessed the various problematic areas with the EuropASI at baseline level, 6 months and 12 months of treatment. We found improved outcomes in every area except for Legal Status. In addition, we found differences between male and female participants in their baseline evaluation, as well as between completers and non-completers. In conclusion, this data shows us some changes which occurred in individuals with problematic drug use during treatment, going further into the complex social reality which causes great suffering and damage to people and their families.
Drug use continues to be one of the most persistent threats to health in Spain and Europe, directly and indirectly affecting the well-being of millions of people in our country (1). Understanding of the phenomenon of addictions has increased in recent years, thanks to the continuous effort of professionals and researchers to elucidate the most relevant treatment factors as well as the current commitment to investing in effective treatment approaches (1–3).
There have been several publications over the last 30 years on the evidence of the effectiveness of Therapeutic Communities (TCs) for addiction treatment with publications on this subject in systematic reviews and meta-analyzes (4–11).
The review by Malivert et al. (6), aimed to assess the effectiveness of TC treatment on abstinence and determine its predictive factors. Twelve studies were selected in which 3,271 patients from 61 TCs participated. All studies showed a reduction in substance use during treatment and following discharge. Treatment completion was the best predictor of abstinence at follow-up, though long-term benefits were uncertain. There were important complications when comparing data due to the large diversity between treatment modalities evaluated, duration, and characteristics of the population who attended.
Various studies have found a strong link between treatment duration in TCs and completion, with greater recovery than when treatment is abandoned prematurely (12–17). Therefore, treatment abandonment is of great concern in all addiction treatment modalities (18), and is often most common in the first months (11). This is particularly relevant when we consider that TCs appear less effective than other forms of intervention regarding treatment adherence (18), and that results improve every 3 months that a person remains (7, 19, 20).
In addition to treatment, type and duration influence outcome and results. Recent research indicates that addiction severity, gender, attachment, comorbidity with personality disorders, therapeutic alliance, relationships within TCs, and social and occupational integration are highly relevant variables when predicting treatment results and adherence in the first months (21–34).
The vast majority of studies in systematic reviews and meta-analytic studies were carried out on the American and Australian population, although 2 studies on the Spanish population are also mentioned. In the work by Fernández-Montalvo et al. (35), a long-term follow-up was performed (a mean of 6 years following treatment) of a TC treatment for addictions. A comparison was made between those who completed and who abandoned treatment. The sample comprised 155 subjects (113 who completed and 42 who dropped out). The latter showed a higher and earlier rate of both relapses (83.3 vs. 32.7%) and new treatments for their addiction than the completion group (66.7 vs. 23%). The program was also effective in reducing illegal behavior and improving health status. In the second study by Fernández-Hermida et al. (36), the authors found significant reductions in the use of alcohol and illegal drugs, in illegal behavior, and a large percentage of those assessed, achieved and maintained stable employment at the 3-year follow-up. The main differences were found between the completion group and those who abandoned it with the latter suffering relapses in a much shorter period than the rest.
As well as studies included in reviews, there are relevant works by López-Goñi et al. (37), Pérez del Río (38) and Valero-Agüayo (39), for treatments similar to those analyzed in previous meta-analytical studies (35, 36). López-Goñi et al. (37), described the pre-post treatment evolution of a sample of 112 patients observed in two Spanish TCs. Sample evaluation was with the Addiction Severity Index (ASI), at start and finish of treatment. Sixty nine point seven percent of the sample completed treatment and 30.3% abandoned it. Results showed a statistically significant improvement in eight of the nine areas evaluated. Only in Physical Health were there no significant changes. The authors highlight that this is possibly due to the high rate of chronic physical illnesses presented by those evaluated. Pérez del Río (38) found that people with better prognosis and who complete 6 months of treatment tend to respond to less unstructured profiles at the social and relational level, have experienced longer abstinence periods, and had significantly lower drug use. On the other hand, Valero-Agüayo et al. (39) observed that the presence of polydrug use, emotional and physical abuse, and numerous family conflicts were factors closely related to abandonment, thus suggesting treatment models that take these variables into account.
Our main aim is to analyze the efficacy of a multicomponent treatment protocol in people with severe substance use disorder, as well as to observe the influence of time in treatment in critical areas (medical health, employment problems, alcohol problems and illegal drugs, social and family relationships, and psychopathological state). Our main hypothesis is that the longer a person remains in treatment, the more pronounced the decrease in addiction severity and other associated problems.
Our second aim is to analyze the relationship between women and men, type of completion, and number of treatments with addiction severity and other associated problems.
The study simple was drawn from the 322 cases attended to between January 2017 and January 2019 in the base program of the Solidarity and Reintegration Foundation of the Region of Murcia. Inclusion criteria were: (a) have substance use problems, (b) participate voluntarily. An exclusion criterion was that participants had not been in treatment for substance use disorder in the previous 6 months.
On applying these criteria, the selected sample was 166 participants (51.55% of the initial population). The mean age of people in treatment was 40.17 years. 22.3% were women. The main substance of consumption in the sample was cocaine (29.5%), followed by joint consumption of alcohol and other drugs (22.9%), and alcohol alone (16.3%). 38.6% reported having received some prior treatment. The mean age and standard deviation at the start of consumption was 26.37 (SD = 21.36) and 21 years of habitual consumption (Table 1).
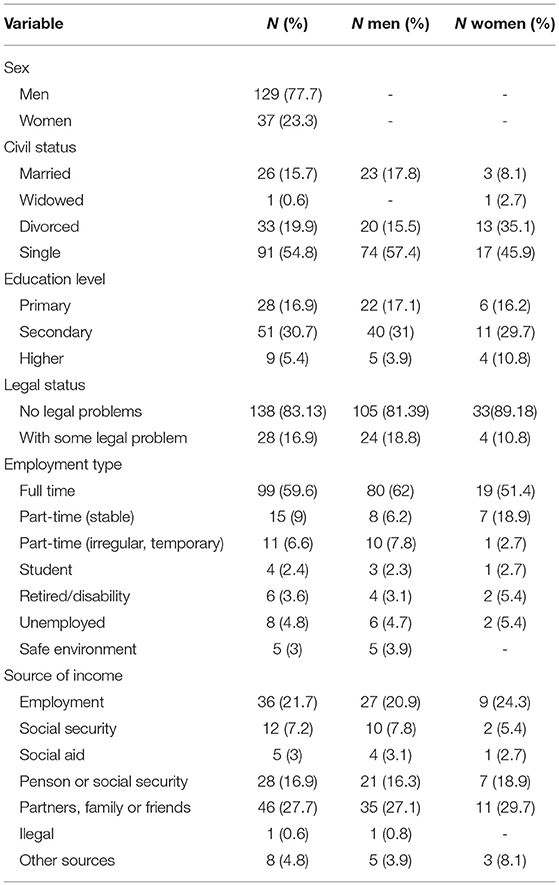
Table 1. Sociodemographic characteristics of sample.
The absence of substance use was assessed by self-report and by random urine sample tests throughout the therapeutic process.
Sociodemographic variables: information on user status was gathered through a semi-structured registry interview developed for this work. Sociodemographic data were gathered (gender, age, educational level, employment, legal records) and clinically relevant variables (substances used, family history of use, type of main substance used, years of use, number of previous treatments).
The EuropASI: is the European Version of the Addiction Severity Index, ASI (40) and the Spanish version was used for this study (41), which presents high internal consistency (α = 0.70). It is a hetero-applied, semi-structured, clinical interview totaling 159 items, widely used for evaluation and diagnosis of patients upon admission to treatment programs, which explores six areas of special relevance to addiction problems: physical health, employment and resources, alcohol and/or drug consumption, legal status, family and social relationships and psychopathological state. As well as different items for each of these areas, the instrument provides a severity index ranging from 0 (no problem) to 9 (extreme problem), with highest scores indicating the need for treatment.
The Solidarity and Reintegration Foundation is a non-governmental organization providing treatment and rehabilitation programs for those with substance use problems and behavioral addictions. The program evaluated in this study, the Base Program (BP), is a semi-residential treatment program whose intervention is based on the biopsychosocial model, and whose aims are: (a) achievement and maintenance of abstinence by users, (b) normalization and social reintegration of user regarding work and family, and (c) The adoption of a lifestyle promoting personal autonomy.
The treatment program comprises two phases. The reception phase lasts between 4 and 6 months approximately and is characterized by intensive group work of a cognitive-behavioral type oriented toward maintaining abstinence and adherence to treatment. Users were divided according to therapeutic criteria, providing access to residential treatments to more serious cases, people who could not stay on their own or the family home, or did not have a person of reference to help during the process.
The therapeutic community (TC) phase is conducted in a residential way, providing a micro-society where residents and a team of professionals, as a facilitating instrument, assume different roles and are governed by clear and specific rules, designed to promote the personal evolution of residents. Intervention is focused on analysis of various factors involved in relapse prevention and lasts between 6 and 8 months.
The treatment program consists of various components mainly developed through group dynamics, in daily group and individual support sessions when required, throughout the process. Components are: Coexistence program; Cognitive restructuring; Social skills training; Self-regulation/self-control; Recognition and emotional expression; Reconstitution of personal identity; Restructuring of securities; Relapse prevention; Family therapy; Contingency management.
Descriptive statistics were first obtained from sociodemographic data and the clinical variables of the sample. To analyze the relationship between sociodemographic and clinical characteristics, independent mean comparisons were performed using the Mann-Whitney U test. To assess results of the program, analysis of comparison of means related by the Wilcoxon signed-rank test was conducted. To calculate the effect size of the non-parametric tests, r (r = Z / √N) was used in accordance with the procedure described by Rosenthal (1994) when assumptions to calculate Cohen's cannot be fulfilled.
All analyzes and data treatments were performed using the statistical package SPSS 21.0.
Of the 166 people evaluated at start of treatment, 42.8% abandoned treatment before completion, while 50% remained to the end (see Table 2). In the longitudinal analysis of the different moments of evaluation of treatment (baseline, 6 months and 12 months), relevant data was found on the effect of treatment on severity of patients' problems. In comparison between baseline and 6 months, significant differences were found in Physical Health indices (Z = 5.290, p < 0.01, r = 0.526), Employment Problems (Z = 4.033, p < 0.01, r = 0.401), Alcohol Use (Z = 5.778, p < 0.01, r = 0.575), Drug Use (Z = 7.029, p < 0.01, r = 0.699), Social / Family Relations (Z = 4.873, p < 0.01, r = 0.485), and Psychopathological State (Z = 5.853, p < 0.01, r = 0.582) (see Table 3), 42.8% abandoned treatment before completion.
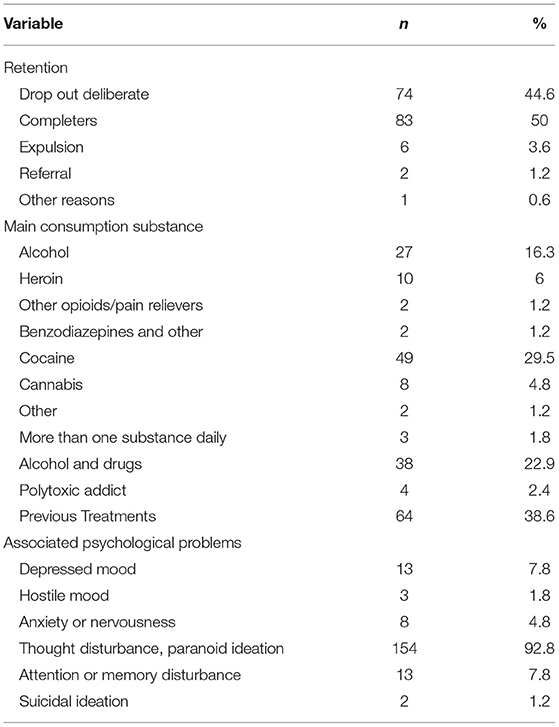
Table 2. Substance use and clinically relevant variables.

Table 3. Differences between baseline evaluations and 6 months.
Similar decreases were found in severity indices on comparing evaluation at 6 months with that of 12 months, in Physical Health indices (Z = 3,163, p < 0.01, r = 0.356), Employment Problems (Z = 5,028, p < 0.01, r = 0.566), Alcohol Use (Z = 5.207, p < 0.01, r = 0.586), Drug Use (Z = 6.797, p < 0.01, r = 0.511), Social / Family Relations (Z = 4.455, p < 0.01, r = 0.501), and Psychopathological State (Z = 4.988, p < 0.01, r = 0.561) (see Table 4).

Table 4. Differences between 6-month and 12-month evaluations.
As for treatment effects when comparing the initial and 12-month evaluations, significant differences were found in Physical Health indices (Z = 5.091, p < 0.01, r = 0.566), Employment Problems (Z = 5.369, p < 0.01, r = 0.597), Alcohol Use (Z = 6.735, p < 0.01, r = 0.748), Drug Use (Z = 6.797, p < 0.01, r = 0.748), Social/Family Relations (Z = 4.873, p < 0.01, r = 0.631), and Psychopathological State (Z = 4.988, p < 0.01, r = 0.702) (see Table 5).
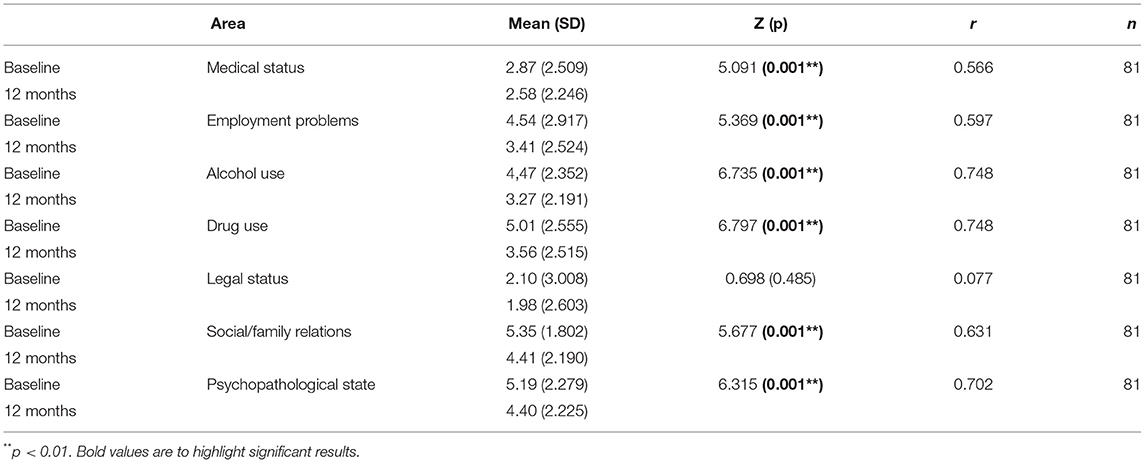
Table 5. Differences between baseline and 12-month evaluations.
Significant differences were found between men and women in several of the EuropASI severity indices (see Table 6). A greater severity of problems was observed among women in the Physical Health index (UMW = 1667.5; p < 0.01; r = 0.29), Social/Family Relations (UMW = 1762.0; p < 0.05; r = 0.19), and Psychopathological State (UMW = 1756.0, p < 0.012, r = 0.19), and a greater severity in the group of men in Drug Use (UMW = 1876.0; p < 0.05; r = 0.16), and Legal Status (UMW = 1903.0; p < 0.05; r = 0.16).
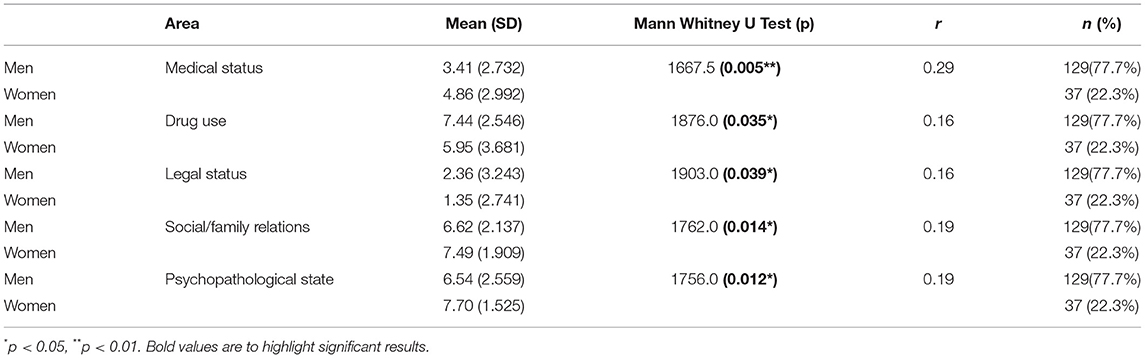
Table 6. Differences by sex.
On analyzing differences found at the start of treatment of those who completed and who abandoned treatment, differences were only seen in Social / Family Relations (UMW = 2349.5; p < 0.05; r = 0.18) (see Table 7). On comparing the group who had previously received treatment with those starting treatment for the first time, significant differences were found in Drug Use at 6 months of treatment (UMW = 934.50; p < 0.05; r = 0.21) and at 12 months (UMW = 529.00; p < 0.05; r = 0.28), but notat the beginning.
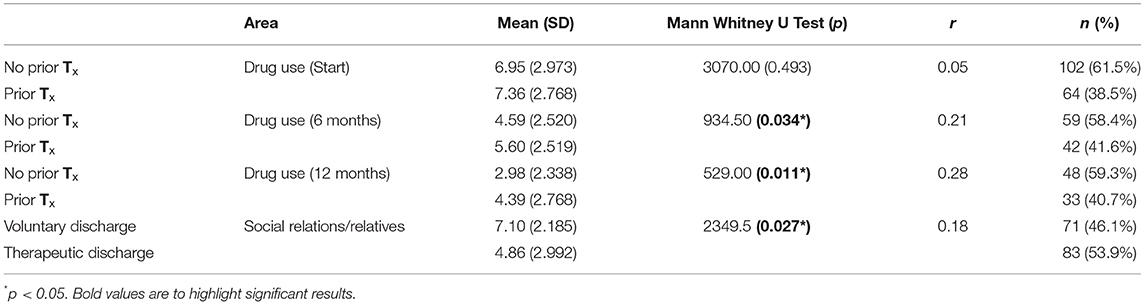
Table 7. Differences by number of previous treatments, and type of discharge.
There are no significant differences between the Medication/No-Medication groups for any EuropASI indices at any evaluation time (Baseline, 6 months, 12 months), except for the index of legal problems at Baseline evaluation (UMW = 2456, p < 0.05, r = 0.17) and at 12 months (UMW = 438.5, p < 0.05, r = 0.29), and the index of psychological problems at 6 months (UMW = 709, p < 0.01, r = 0.29) (see Table 8).

Table 8. Differences by medication status.
There are differences in the EuropASI index of psychological problems in the evaluation of Start (UMW = 2,372, p < 0.05, r = 0.16) between people who manifested problems with concentration in the previous month and those who did not, and in problems 12 months after treatment (UMW = 435, p < 0.05, r = 0.29).
No significant differences were found for any of the indices between people who experienced severe depression and those who did not. Nor for those who manifested severe anxiety or who experienced violent behavior.
The difference between pretreatment (baseline) and posttreatment (12 months), in substance use was 3.4 (SD: 2.83), effect size is equal to 1.2 (d), and power is 1 for the final sample.
The evaluated sample is similar to those found in other articles in the field of addictions (4, 6–8, 18, 42), commonly finding a high percentage of men, cocaine and alcohol users, and polydrug users. The retention ratio in this study is in line with other research (6, 8, 18).
It is worth noting the high percentage of users presenting psychopathological problems, 92.8% symptoms of mental pathology, far from that found in other studies, which report prevalences of around 50% (24, 43–47). This difference might be due to the ASI not being a diagnostic tool and that its psychopathological area is limited to exploring and providing information on possible problems, i.e., it is a screening tool, although it may also be explained by the fact that those who choose this resource (Foundation for Reintegration...) have a longer and more complex history of consumption. Thus, these data must be taken with caution and this area should be explored in future studies with standardized diagnostic tests that can more reliably estimate psychological pathology.
The most striking treatment results have always been found when comparing severity of problems of profiles at start of treatment with results after 12 months. These data correspond to those in other studies on the importance of time spent in treatment (12–17). In this study, the severity of medical problems and those related to illegal substances (EuropASI Medical and EuropASI Drugs) reduced considerably in the first 6 months of treatment. Contrarily, in severity of family/social and employment problems, greater treatment effects are observed in the second period (6–12 months). This more pronounced decrease in the last stage might be due to the fact that vocational training and/or employability workshops do not begin until severity of alcohol and drug use has decreased, as occurs within the area of relationship problems between users and their family members (6, 8, 18). These data, added to the fact that the only difference we found between those completing treatment and those not, was greater severity of family/social problems, supporting the need for treatment modalities that include interventions in this area. These must be developed from the very start as delay until later intervention stages can cause intense emotional burden in users that can lead to premature abandonment of treatment. This is relevant if we consider that the person's level of social and family integration plays a key role in whether they remain in treatment (6, 8, 32, 34, 48, 49).
No variations were found regarding legal problems throughout treatment. We understand this is caused by the low severity of legal problems presented by the collected sample, since other treatment modalities in TCs did find a marked reduction in these problems among prison populations that present high levels of this type PODEMOS QUITAR CONCHA? (8, 50–52).
There are considerable differences between men and women in the entry profile as regards severity of medical, family, psychological, legal problems, and dependence on illegal substances. As the percentage of women in the sample was low, data should be viewed with caution.
In this study, it was found that patients with a history of previous treatments obtain worse results at 6 months and 12 months in the EuropASI Drug Use Index, corresponding to data that indicate better results with fewer treatment episodes (53–56). Some studies mention the difficulty of profiles with several previous failed treatment schedules (54, 55, 57, 58) which may be due to greater severity at start of treatment. Darke et al. (59), found that users who had stayed longer in the same treatment itinerary obtained better results, while those presenting a longer history of previous treatments, and with a similar or even longer time in treatment often achieved much worse treatment results (26, 29, 54, 55, 57, 58).
As for the study's limitations, a control group could not be included in the research due to the desire to provide users with the best possible treatment without delay, which is a methodological weakness, as well as the absence of longer follow-up. Nevertheless, it provides relevant data on two treatment stages which can help improve the applied protocols.
The main conclusions are as follows: (a) longer treatment time brings better therapeutic results; (b) severity of treatment areas related to substances and physical health greatly improve in the first months of treatment, while social/ family and employment problems require longer for improvement to be effective; (c) Patient gender influences severity of consumption problems, legal situation, physical health, and the social/family relationships presented and these must be considered when designing interventions; (d) Social-family problems influence retention of treatment and these problems must be addressed from the start to try and prevent premature abandonment of treatment; (e) Those with a longer history of treatment present additional difficulties and these must be determined to avoid early abandonment.
The main aim of this research was to assess the efficacy of the multimodal cognitive-behavioral treatment protocol applied at the Solidarity & Reinsertion Foundation of Murcia (Murcia), and is a first step toward knowing the effects throughout treatment for 1 year in people with consumption problems, delving into this social reality that brings so much suffering and deterioration to people and their families. Information on follow-up at 18 and 24 months is being gathered in this sample, owing to the importance of maintaining improvement achieved by treatment and of obtaining more information on differences between men and women.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by University of Murcia. The patients/participants provided their written informed consent to participate in this study.
AS-d-P carried out the treatment protocol, collaborated on its application as clinical supervisor, corrected the evidence included in the research, and is a collaborator in the writing of the article. LL-C performed statistical treatment and collaborated in the review of articles. MA-L collaborated in the bibliographic search and writing of the introduction, results, and bibliographical references of the article. AM-P, MC-S, and VF-F carried out part of the search for articles, writing of results, and preparation of tables. CL-S designed the research and collaborated in the proofreading and writing of the article. All authors contributed to the article and approved the submitted version.
This research was carried out with the support of the Solidarity and Reinsertion Foundation (Murcia) and research funds from the UM.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to acknowledge the collaboration and support provided by the technical teams of the Solidarity and Reinsertion Foundation of Murcia that performed data collection for this study.
1. European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). Informe Europeo sobre Drogas: tendencias y novedades (2019). Available online at: http://www.emcdda.europa.eu/publications/edr/trends-developments/2019 (accessed September 3, 2019).
2. Delegación del Gobierno para el Plan Nacional sobre Adicciones (PNSD). Estrategia Nacional sobre Drogas 2017-20124 (2017). Available online at: http://www.pnsd.mscbs.gob.es/pnsd/estrategiaNacional/home.htm (accessed November 21, 2019).
3. National Institute of Drug Abuse (NIDA). Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition) (2018). Available online at: https://www.drugabuse.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition/principles-effective-treatment (accessed February 2, 2021).
4. Henderson A, Stenfert Kroese B. Group interventions for trauma and substance misuse available for women in criminal justice services: a systematic review of the literature. J Forensic Pract 1 de enero de. (2020) 22:235–49. doi: 10.1108/JFP-05-2020-0024
5. Magor-Blatch L, Bhullar N, Thomson B, Thorsteinsson E. A systematic review of studies examining effectiveness of therapeutic communities. Ther Communities. (2014) 35:168–84. doi: 10.1108/TC-07-2013-0024
6. Malivert M, Fatséas M, Denis C, Langlois E, Auriacombe M. Effectiveness of therapeutic communities: a systematic review. Eur Addict Res. (2012) 18:1–11. doi: 10.1159/000331007
7. Perry AE, Martyn-St JM, Burns L, Hewitt C, Glanville JM, Aboaja A, et al. Interventions for female drug-using offenders. Cochrane Database Syst Rev. (2020) 1:1–109. doi: 10.1002/14651858.CD010910.pub3
8. Perry AE, Martyn-St JM, Burns L, Hewitt C, Glanville JM, Aboaja A, et al. Interventions for drug-using offenders with co-occurring mental health problems. Corchane Database Systematic Review. (2019) 10:1–96. doi: 10.1002/14651858.CD010901.pub3
9. Sacks S, McKendrick K, Sacks JY, Cleland CM. Modified therapeutic community for co-occurring disorders: single investigator meta analysis. Subst Abus julio de. (2010) 31:146–61. doi: 10.1080/08897077.2010.495662
10. Smith LA, Gates S, Foxcroft D. Therapeutic communities for substance related disorder. Cochrane Database Syst Rev. (2006) 1:CD005338. doi: 10.1002/14651858.CD005338.pub2
11. Vanderplasschen W, Colpaert K, Autrique M, Rapp RC, Pearce S, Broekaert E, et al. Therapeutic communities for addictions: a review of their effectiveness from a recovery-oriented perspective. Sci World J. (2013) 2013:427817. doi: 10.1155/2013/427817
12. Greenfield L, Burgdorf K, Chen X, Porowski A, Roberts T, Herrell J. Effectiveness of long-term residential substance abuse treatment for women: findings from three national studies. Am J Drug Alcohol Abuse. (2004) 30:537–50. doi: 10.1081/ADA-200032290
13. Ormbostad HAK, Ormbostad E, Stallvik M. Investigating patients' perceptions of residential substance use treatment is drop out a deliberate or impulsive act? J Soc Work Pract Addict. (2021) 21:255–72. doi: 10.1080/1533256X.2021.1933850
14. Teesson M, Mills K, Ross J, Darke S, Williamson A, Havard A. The impact of treatment on 3 years' outcome for heroin dependence: findings from the Australian Treatment Outcome Study (ATOS). Addiction. (2008) 103:80–8. doi: 10.1111/j.1360-0443.2007.02029.x
15. Teesson M, Marel C, Darke S, Ross J, Slade T, Burns L, et al. Long-term mortality, remission, criminality and psychiatric comorbidity of heroin dependence: 11-year findings from the Australian Treatment Outcome Study. Addiction. (2015) 110:986–93. doi: 10.1111/add.12860
16. Turner B, Deane FP. Length of stay as a predictor of reliable change in psychological recovery and well being following residential substance abuse treatment. Ther Communities. (2016) 37:112–20. doi: 10.1108/TC-09-2015-0022
17. Zhang Z, Friedmann PD, Gerstein DR. Does retention matter? Treatment duration and improvement in drug use. Addiction. (2003) 98:673–84. doi: 10.1046/j.1360-0443.2003.00354.x
18. Minozzi S, Saulle R, De Crescenzo F, Amato L. Psychosocial interventions for psychostimulant misuse. Cochrane Database Syst Rev. (2016) 9:CD011866. doi: 10.1002/14651858.CD011866.pub2
19. Ernst & Young. Review of Long Term Residential treatment for People with Alcohol and Other Drug Use Problems. National Drug Strategy, Commonwealth Department of Human Services and Health of Australia. (1996).
20. Simpson DD, Joe GW, Fletcher BW, Hubbard RL, Anglin MD. A national evaluation of treatment outcomes for cocaine dependence. Arch Gen Psychiatry. (1999) 56:507–14. doi: 10.1001/archpsyc.56.6.507
21. Adamson SJ, Sellman JD, Frampton CMA. Patient predictors of alcohol treatment outcome: a systematic review. J Subst Abuse Treat. (2009) 36:75–86. doi: 10.1016/j.jsat.2008.05.007
22. Christensen HN, Diderichsen F, Hvidtfeldt UA, Lange T, Andersen PK, Osler M, et al. Joint effect of alcohol consumption and educational level on alcohol-related medical events: a Danish register-based cohort study. Epidemiology. (2017) 28:872–9. doi: 10.1097/EDE.0000000000000718
23. Dacosta-Sánchez D, Díaz-Batanero C, Fernandez-Calderon F, Lozano ÓM. Impact of cluster B personality disorders in drugs therapeutic community treatment outcomes: a study based on real world data. J Clin Med. (2021) 10:2572. doi: 10.3390/jcm10122572
24. Daigre C, Perea-Ortueta M, Berenguer M, Esculies O, Sorribes-Puertas M, Palma-Alvarez R, et al. Psychiatric factors affecting recovery after a long term treatment program for substance use disorder. Psychiatry Res. (2019) 276:283–9. doi: 10.1016/j.psychres.2019.05.026
25. Fuchshuber J, Hiebler-Ragger M, Ragger K, Rinner A, Kapfhammer HP, Unterrainer HF. Increased attachment security is related to early therapy drop-out in substance use disorders. BMC Res. (2018) 11:141. doi: 10.1186/s13104-018-3251-7
26. Harley M, Pit SW, Rees T, Thomas S. Completion rates and psychosocial intervention effectiveness in an Australian substance use therapeutic community. Subst Abuse: Treat Prev Policy. (2018) 13:33. doi: 10.1186/s13011-018-0170-5
27. McCaul ME, Svikis DS, Moore RD. Predictors of outpatient treatment retention: patient versus substance use characteristics. Drug Alcohol Depend. (2001) 62:9–17. doi: 10.1016/S0376-8716(00)00155-1
28. Mulder RT, Frampton CMA, Peka H, Hampton G, Marsters T. Predictors of 3-month retention in a drug treatment therapeutic community. Drug Alcohol Rev. (2009) 28:366–71. doi: 10.1111/j.1465-3362.2009.00050.x
29. Papamalis FE. Examining the relationship of personality functioning and treatment completion in substance misuse treatment. Subst Abuse: Res Treat. (2020) 14:1–19. doi: 10.1177/1178221820951777
30. Roncero C, Rodríguez-Cintas L, Barral C, Fuste G, Daigre C, Ramos-Quiroga JA, et al. Treatment adherence to treatment in substance users referred from Psychiatric Emergency service to outpatient treatment. Actas Esp Psiquiatr. (2012) 40:63–9. https://pubmed.ncbi.nlm.nih.gov/22508071/
31. Rübig LL, Fuchshuber J, Köldorfer P, Rinner A, Fink A, Unterrainer H-F. Attachment and therapeutic alliance in substance use disorders: initial findings for treatment in the therapeutic community. Front Psychiatry. (2021) 12:730876. doi: 10.3389/fpsyt.2021.730876
32. Schaefer DR, Davidson KM, Haynie DL, Bouchard M. Network integration within a prison-based therapeutic community. Soc Netw. (2021) 64:16–28. doi: 10.1016/j.socnet.2020.07.007
33. Vismara L, Presaghi F, Bocchia M, Ricci RV, Ammaniti M. Attachment patterns in subjects diagnosed with a substance use disorder: a comparison of patients in outpatient treatment and patients in therapeutic communities. Front Psychiatry. (2019) 10:807. doi: 10.3389/fpsyt.2019.00807
34. Warren K, Campbell B, Cranmer S, De Leon G, Doogan N, Weiler M, et al. Building the community: Endogenous network formation, homophily and prosocial sorting among therapeutic community residents. Drug Alcohol Depend. (2020) 207:107773. doi: 10.1016/j.drugalcdep.2019.107773
35. Fernández-Montalvo J, López-Goñi JJ, Illescas C, Landa N, Lorea I. Evaluation of a therapeutic community treatment program: a long-term follow-up study in Spain. Subst Use Misuse. (2008) 43:1362–77. doi: 10.1080/10826080801922231
36. Fernández-Hermida J-R, Secades-Villa R, Fernández-Ludeña J-J, Marina-González P-A. Effectiveness of a therapeutic community treatment in Spain: a long-term follow-up study. Eur Addict Res. (2002) 8:22–9. doi: 10.1159/000049484
37. López-Goñi JJ, Fernández-Montalvo J, Menéndez JC, Yudego F, García AR, Esarte S. Group and individual change in the treatment of drug addictions: a follow-up study in therapeutic communities. Span J Psychol. (2010) 13:906–13. doi: 10.1017/S1138741600002559
38. Pérez del Río F. En qué cambian los pacientes drogodependientes a los seis meses de tratamiento en la comunidad terapéutica. Rev Asoc Esp Neuropsiq. (2012) 32:287–303. doi: 10.4321/S0211-57352012000200006
39. Valero-Aguayo L, Ortiz-Tallo M, Parra-García M, del M, Jiménez-Guerra M. Valoración de resultados y perfil psicosocial de un programa de rehabilitación de personas con drogodependencias. Anal Psicol enero de. (2013) 29:38–47. doi: 10.6018/analesps.29.1.159131
40. McLellan AT, Kushner H, Metzger D, Peters R, Smith I, Grissom G, et al. the fifth edition of the addiction severity index. J Subst Abuse Treat. (1992) 9:199–213. doi: 10.1016/0740-5472(92)90062-S
41. Bobes J, González MP, Sáiz P, Bousoño M. Índice Europeo de Severidad de la Adicción: EuropASI. Versión española. Actas de la IV Reunión Interregional de Psiquiatría (1996).
42. Observatorio Proyecto Hombre. Informe 2018: sobre el perfil de las personas con problemas de adicción en tratamiento. (2019). Available online at: http://proyectohombre.es/informe-observatorio/ (accessed May 13, 2021).
43. Araos P, Vergara-Moragues E, González-Saiz F, Pedraz M, García-Marchena N, Romero-Sanchiz P, et al. Differences in the Rates of Drug Polyconsumption and Psychiatric Comorbidity among Patients with Cocaine Use Disorders According to the Mental Health Service. J Psychoactive Drugs. (2017) 49:306–15. doi: 10.1080/02791072.2017.1342151
44. Arias F, Szerman N, Vega P, Mesias B, Basurte I, Morant C, et al. Estudio Madrid sobre prevalencia y características de los pacientes con patología dual en tratamiento en las redes de salud mental y de atención al drogodependiente. Adicciones. (2013) 25:118–27. doi: 10.20882/adicciones.59
45. Miovský M, Lukavská K, Rubášová E, Štastná L, Šefránek M, Gabrhelík R. Attention deficit hyperactivity disorder among clients diagnosed with a substance use disorder in the therapeutic communities: prevalence and psychiatric comorbidity. Eur Addict Res. (2021) 27:87–96. doi: 10.1159/000508571
46. Simonelli A, Parolin M, Mapelli D, Cristofalo P, Cimino S, Cerniglia L. Cognitive functioning, clinical profile and life events in young adults addicted to drugs. Does being a girl make a difference? Clin Neuropsychiatry. (2017) 14:226–38. https://psycnet.apa.org/record/2017-31745-005
47. Szerman N, Arias F, Vega P, Babín F, Mesías B, Basurte I, et al. Estudio piloto sobre la prevalencia de patología dual en pacientes en tratamiento en la Comunidad de Madrid. Adicciones. (2011) 23:249–55. doi: 10.20882/adicciones.149
48. Broekaert E. What future for the Therapeutic Community in the field of addiction? A view from Europe. Addiction. (2006) 101:1677–8. doi: 10.1111/j.1360-0443.2006.01646.x
49. Mandell W, Lidz V, Dahl JJ. Experimental evaluation of a vocationally integrated therapeutic community. Ther Communities. (2015) 36:173–85. doi: 10.1108/TC-06-2014-0021
50. Messina N, Grella CE, Cartier J, Torres S A. Randomized Experimental Study of Gender-Responsive Substance Abuse Treatment for Women in Prison. J Subst Abuse Treat. (2010) 38:97. doi: 10.1016/j.jsat.2009.09.004
51. Welsh WN. A multisite evaluation of prison-based therapeutic community drug treatment. Crim Justice Behav. (2007) 34:1481–98. doi: 10.1177/0093854807307036
52. Zhang SX, Roberts REL, McCollister KE. Therapeutic Community in a California prison: treatment outcomes after 5 years. J Res Crime Delinq. (2011) 57:82–101. doi: 10.1177/0011128708327035
53. Bruguera E, Heredia M, Llavayol E, Pujol T, Nieva G, Valero S, et al. Integral Treatment Programme for Addicted Physicians: Results from The Galatea Care Programme for Sick Physicians. Eur Addict Res. (2020) 26:122–30. doi: 10.1159/000505914
54. Darke S, Ross J, Teesson M, Ali R, Cooke R, Ritter A, et al. Factors associated with 12 months continuous heroin abstinence: findings from the Australian Treatment Outcome Study (ATOS). J Subst Abuse Treat. (2005) 28:255–63. doi: 10.1016/j.jsat.2005.01.006
55. Darke S, Ross J, Mills KL, Williamson A, Havard A, Teesson M. Patterns of sustained heroin abstinence amongst long-term, dependent heroin users: 36 months findings from the Australian Treatment Outcome Study (ATOS). Addict Behav. (2007) 32:1897–906. doi: 10.1016/j.addbeh.2007.01.014
56. Gossop M, Marsden J, Stewart D, Rolfe A. Treatment retention and 1 year outcomes for residential programmes in England. Drug Alcohol Depend. (1999) 57:89–98. doi: 10.1016/S0376-8716(99)00086-1
57. Anglin MD, Hser Y-I, Grella CE. Drug addiction and treatment careers among clients in the Drug Abuse Treatment Outcome Study (DATOS). Psychology of Addictive Behaviors. (1997) 11:308–23. doi: 10.1037/0893-164X.11.4.308
58. Hser YI, Grella CE, Hsieh SC, Anglin MD, Brown BS. Prior treatment experience related to process and outcomes in DATOS. Drug Alcohol Depend. (1999) 57:137–50. doi: 10.1016/S0376-8716(99)00081-2
Keywords: addiction, substance-related disorders, treatment, retention, gender
Citation: Santos-de-Pascual A, López-Cano LM, Alcántara-López M, Martínez-Pérez A, Castro-Sáez M, Fernández-Fernández V and López-Soler C (2022) Effects of a Residential Multimodal Psychological Treatment in an Addicted Population, at 6 and 12 Months: Differences Between Men and Women. Front. Psychiatry 13:862858. doi: 10.3389/fpsyt.2022.862858
Received: 26 January 2022; Accepted: 24 May 2022;
Published: 16 June 2022.
Edited by:
Marco Colizzi, University of Udine, ItalyReviewed by:
Farhana Sabri, Islamic Science University of Malaysia, MalaysiaCopyright © 2022 Santos-de-Pascual, López-Cano, Alcántara-López, Martínez-Pérez, Castro-Sáez, Fernández-Fernández and López-Soler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonia Martínez-Pérez, YW1wZXJlekB1bS5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.