
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 25 April 2022
Sec. Public Mental Health
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.860683
This article is part of the Research TopicAdaption to Change and Coping Strategies: New Resources for Mental HealthView all 29 articles
 Mohamed Elsayed1*
Mohamed Elsayed1* Carlos Schönfeldt-Lecuona1,2†
Carlos Schönfeldt-Lecuona1,2† Xenia Anna Welte1
Xenia Anna Welte1 Khaled Tarek Dardeer3
Khaled Tarek Dardeer3 Manar Ahmed Kamal4
Manar Ahmed Kamal4 Ramy Abdelnaby5
Ramy Abdelnaby5 Markus A. Rudek6
Markus A. Rudek6 Evelyne Riedel7
Evelyne Riedel7 Michael Denkinger2,8
Michael Denkinger2,8 Maximilian Gahr1
Maximilian Gahr1 Bernhard J. Connemann1
Bernhard J. Connemann1 Sheikh M. Alif9
Sheikh M. Alif9 Biswajit Banik10
Biswajit Banik10 Wendy Cross10
Wendy Cross10 Muhammad Aziz Rahman10,11*†
Muhammad Aziz Rahman10,11*†Background: The COVID-19 pandemic has imposed enormous psychological discomfort and fear across the globe, including Germany.
Objectives: To assess the levels of COVID-19 associated psychological distress and fear amongst Southern German population, and to identify their coping strategies.
Methods: A cross-sectional survey using an online questionnaire was conducted in healthcare and community settings in the region of Ulm, Southern Germany. Assessment inventories were the Kessler Psychological Distress Scale (K-10), the Brief Resilient Coping Scale (BRCS), and the Fear of COVID-19 Scale (FCV-19S), which were valid and reliable tools.
Results: A total of 474 Individuals participated in the study. The mean age was 33.6 years, and 327 (69%) were females. Most participants (n = 381, 80.4%) had high levels of psychological distress, whereas only 5.1% had high levels of fear, and two-thirds of participants showed higher levels of coping. Moderate to very high levels of psychological distress were associated with being female, living alone, distress due to employment changes, experiencing financial impact, having multiple co-morbidities, being a smoker, increased alcohol use over the previous 6 months, contact with COVID-19 cases and healthcare providers for COVID-19-related stress. Individuals who were ≥60 years, lived with non-family members, had co-morbidities and visited a healthcare provider had higher levels of fear. Higher levels of education and income showed better coping amongst participants.
Conclusion: Psychological distress was very high during the COVID-19 pandemic in Germany and associated with low levels of coping. This study identified vulnerable groups of people, who should be given priorities for addressing their health and wellbeing in future crisis periods.
The coronavirus disease (COVID-19) has spread into 222 countries and territories worldwide and the World Health Organization (WHO) declared a global public health emergency on 30 January 2020 (1). As of 23 November 2021, Germany reported more than five million confirmed cases and almost 100,000 deaths from COVID-19 (2). This led to enact public health measures by the Government such as physical distancing, canceling large gatherings, imposing travel restrictions and lockdown in large cities, ensuring obligatory quarantine for positive cases, primary close contacts, along with closing of educational institutions. The lockdown also resulted in the closure of many small businesses, and the unemployment rate increased to 4.1% in summer 2020 compared to 3.1% just before the pandemic (3). Ongoing restrictions also impacted on the physical and mental health of the population, especially older adults with multiple comorbidities (4). Ongoing social isolation and uncertainty of further COVID-19 pandemic waves could potentially trigger long-term mental disorders (5).
Furthermore, Unemployment and social isolation were associated with risky behaviors such as increased tobacco and alcohol consumption (6). Lockdown measures and social distancing restrictions caused a shift to telehealth facilities (7). Previous studies showed that healthcare workers engaged in the diagnosis and management of COVID-19 patients were more prone to psychological distress and various mental disorders, such as depression, anxiety, anger, fear of spreading the infection to their relatives, friends, or colleagues (8, 9).
Studies from several countries around the world including Germany found that the pandemic caused higher psychological distress, anxiety, and depression amongst a large proportion of community members (10–16). Studies also showed that depression, stress, and anxiety during the pandemic triggered sleep disorders and increased consumption of tobacco and alcohol (17). However, with increased vaccination rates and easing of restrictions, impacts may change during the current pandemic waves. Although there are previously published studies that assessed anxiety, fear and distress amongst community members and healthcare workers in Germany during the COVID-19 pandemic, the existing evidence lacks a full understanding of the impacts of the pandemic on mental health and coping strategies amongst the public in Germany and identification of the relevant predictors. Therefore, this study aimed to assess the levels of psychological distress, fear of the COVID-19 disease, and coping strategies among a wide range of population in Germany; it also aimed to identify critical factors associated with those outcomes. The population subgroups who were at higher risk of developing poor mental health outcomes would be identified in this study, which would enable the policymakers to optimize psychosocial interventions targeted to those vulnerable groups of population and guide resource planning to avoid long-term mental health impacts.
A cross-sectional study was conducted according to The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement Checklist (18). This study was a part of a large study involving 17 countries and was led by the last author (10). Participants were informed about the study using social media and received the link of the questionnaire through social media or by emails. In addition, Quick Response (QR) codes were used on professional posters in outpatient clinics to inform patients about the study and invite participation. Data were collected from healthcare settings, including General Practices, hospitals, allied health professionals, and community settings, using a structured self-administered online questionnaire (10, 13, 14, 19).
Adult participants who were ≥18 years old with the capacity to respond to an online questionnaire in German language were included in three main groups: (a) patients who attended a healthcare setting, either for face-to-face or telehealth consultation in the last 4 weeks irrespective of respiratory/COVID-19 symptoms, (b) healthcare workers (full time, part-time or casual) who have been in contact with patients in the last 4 weeks in a healthcare setting (doctor, nurses, allied health professionals, technicians, patient service attendants, receptionists, etc.) irrespective of caring for respiratory/COVID-19 patients, and (c) community members who did not consult any healthcare provider in the last 4 weeks.
An online link to the web-based questionnaire was developed using Google forms to collect data from February to April 2021 during the second and third waves of the COVID-19 pandemic. According to Robert Koch Institute, the second German wave began in October 2020 (https://www.shorturl.at/shortener.php), while the third wave started in March 2021 (https://www.shorturl.at/loqHP). Initially, there was a screening question related to age to confirm eligibility; subsequently data were collected on: (a) socio-demographics as age, gender, location of residence, marital status, living conditions (alone or with families), the highest level of education, country of birth; (b) profession as a primary occupation, the impact of COVID-19 on occupation, identification as a frontline healthcare worker; (c) self-reported comorbidities as hypertension, cardiovascular diseases, chronic respiratory diseases, diabetes, cancer; (d) behavioral risk factors as current smoking, alcohol intake; (e) health service utilization (in the last 4 weeks) as consultation with a healthcare provider for any symptom, admission to the hospital including reasons for admission; (f) exposure and contact history of COVID-19, test and diagnosis of COVID-19, close contact, isolation and quarantine status; (g) psychological impact measured by the Kessler Depression Scale (K-10) (20), and fear measured by the Fear of COVID-19 Scale (FCV) (21); (h) coping strategies measured by the Brief Resilient Coping Scale (BRCS) (22); and (j) access to mental health resources (in the last four weeks) (see Appendix 1).
The K10 scale is a 10-item self-rated questionnaire that measures distress based on depressive and anxiety symptoms. Each item has five possible answers (none of the time = 1, a little of the time = 2, some of the time = 3, most of the time = 4, all of the time = 5) allowing for a total score of 50. A score of 10–15 is likely to be well, 16–29 is medium risk for anxiety or depression and 30–50 is high risk for anxiety or depressive symptoms (20). Cronbach's alpha for this tool was 0.902, which was satisfactory.
The FCV-19S is a seven-item scale that assesses fear of COVID-19 among the general population. Each item has five possible answers (strongly disagree = 1 disagree = 2 neutral = 3 agree = 4 strongly agree = 5) allowing for a maximum score of 35, a score of 7-22 is considered low fear and 23–35 is considered high fear of COVID-19 (21). Cronbach's alpha for this tool was 0.82, which was satisfactory.
The BRCS is a 4-item scale that measures a psychological well-being construct: resilience. Each item is a 5-point response (does not describe me at all = 1, does not describe me = 2, neutral = 3, describes me = 4, describes me very well = 5). The maximum possible score is 20, and it is categorized into low resilience (score 4–13), medium resilience (score 14–16) and high resilience (Score 17–20) (22). Cronbach's alpha for this tool was 0.758, which was satisfactory.
All participants fulfilling the inclusion criteria were invited to participate. Considering Germany's population of 84 million according to World Population Prospects (23), the prevalence of lifetime mental health issues amongst Germans was 31.1% (24), at 95% confidence intervals, margin of error (5%), and 80% power, the required sample size was 329. The sample size was calculated using Open Epi Info software version 7.2. Convenient sampling was used to recruit the study participants by following snowball sampling.
Ethical approval was obtained from the Research Ethical Committee (REC) of the Ulm University (Ethical Approval Number 448/20 – FSt/Sta).
International Business Machines Corporation (IBM) Statistical Package for the Social Sciences (SPSS) statistics software version 25 was used for data analysis. Descriptive analyses were conducted and followed by inferential analyses. Continuous variables were presented as mean ± standard deviation (SD), while categorical variables were presented as numbers and percentages. Internal consistency of the instruments was calculated using Cronbach's alpha. The study outcomes were categorized into binary variables as follows: K-10 score was categorized into low (score 10–15) and moderate to very high (score 16–50), FCV-19S score was categorized into low (score 7–21) and high (score 22–35) and BRCS score was defined into low (score 4–13) and medium to high (score 14–20) resilient copers. Univariate and multivariate logistic regression (adjusted for age, gender, born in Germany, living status, employment status, level of education) were performed to explore the association between population characteristics and the study's outcomes. Odds ratios (ORs), adjusted odds ratios (AORs) and 95% confidence intervals (95% CIs) were obtained. Firth logistic regression with penalized maximum likelihood was used for fear of COVID-19 outcome as the number of events was relatively low for the number of adjusted variables. To measure the association between distress, fear and coping, partial rank correlation was conducted on the overall score as a continuous variable for each scale. This was done after controlling for potential confounding factors (age, gender, born in Germany, living status, employment status and level of education). P values less than 0.05 were considered statistically significant.
A total of 474 people participated in the study. The mean age of the participants was 33.6 (13.3) years, and 327 (69%) were females. Most of them were born in Germany (89.9%, n=426), and around half lived with family members (48.5%, n = 230). Two-thirds (62.4%, n = 296) of the participants had a source of income during the pandemic, and only 2.1% (n = 10) had their jobs affected by the pandemic. Half of the participants (57%, n = 270) reported change in the employment situation, and half of them (49.4%, n = 196) had higher perceived distress due to that change. About half participants (47.3%, n = 224) self-identified as essential service workers and 54.6% (n = 259) reported being healthcare workers. Only 7.4% (n = 35) participants reported having psychiatric or mental health issues, although a quarter of the participants (24.1%, n = 114) perceived their mental health status as poor to fair. Table 1 shows the characteristics of included participants, and Tables 2–4 shows multivariate analyses of psychological distress, fear, and coping.

Table 1. Baseline demographic characteristics of the participants (N = 474).
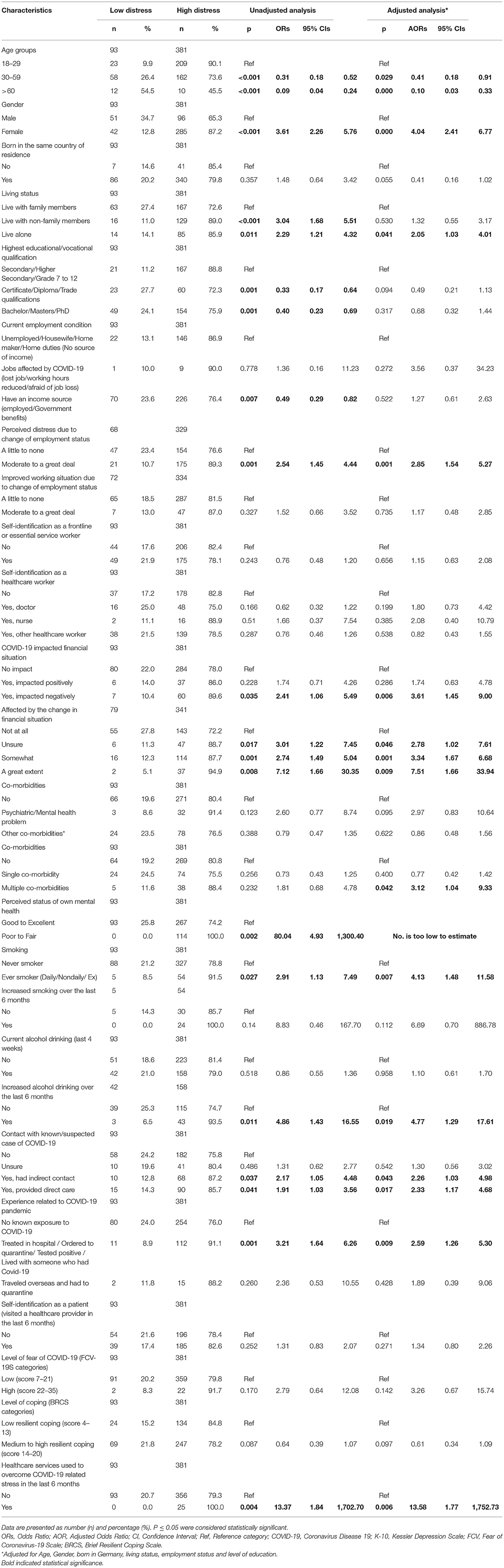
Table 2. Factors associated with high psychological distress among the study population (based on K10 scoring).
After adjusting for potential confounders, multivariate analyses showed that being a female, living alone, those with distress due to employment change, worsened financial situation, having multiple co-morbidities, smoking, increased alcohol consumption over the last 6 months, contact with COVID-19 case whether direct or indirect, direct experience of COVID-19 and healthcare use to overcome pandemic stress in the last 6 months were associated with moderate to very high levels of psychological distress (Table 2).
Multivariate logistic regression showed that being over 60, living with non-family members, those having a diploma or a trade qualification, those with single or multiple comorbidities, perceived mental health status as poor to fair, direct experience of COVID-19, visiting a health care provider in the past 6 months and using healthcare service to overcome pandemic related stress in the last 6 months were associated with higher levels of fear of COVID-19 (Table 3).
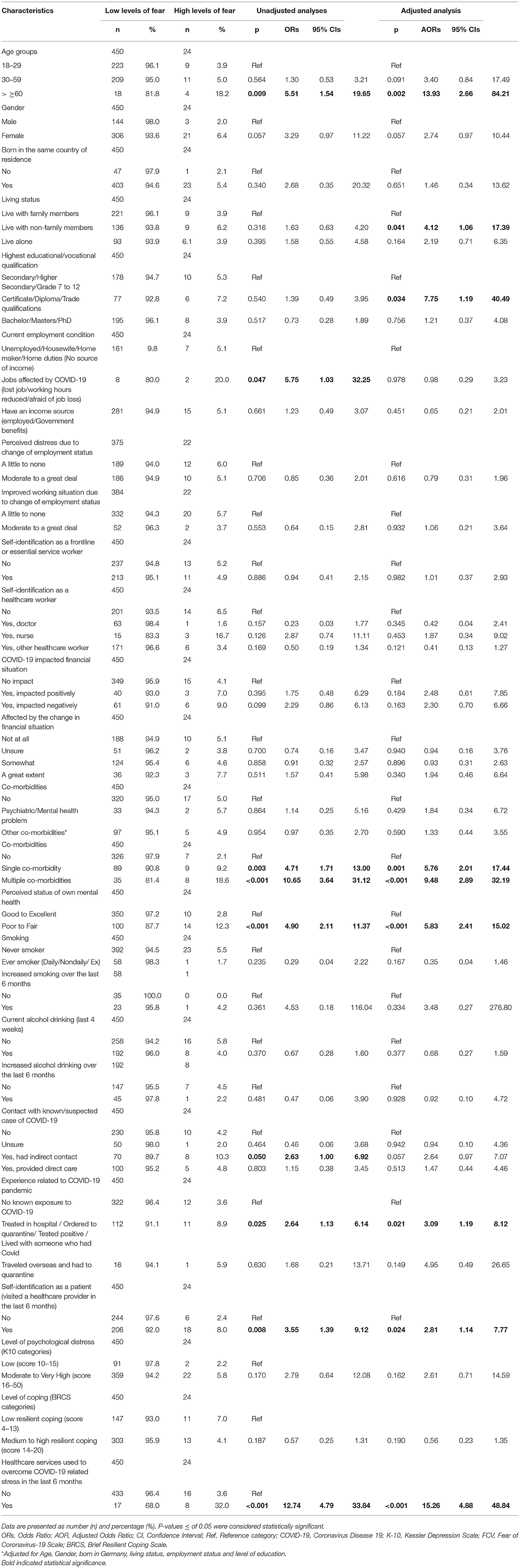
Table 3. Factors associated with high levels of fear of COVID-19 among the study population (based on FCV-19S scoring).
Multivariate analyses revealed that having an income source and being a healthcare worker were associated with higher levels of coping. Conversely, higher levels of education, distress due to change in employment, worsened financial situation due to the pandemic, and perceived status of mental health as poor to fair were the factors that predicted lower levels of coping amongst the study participants (Table 4).
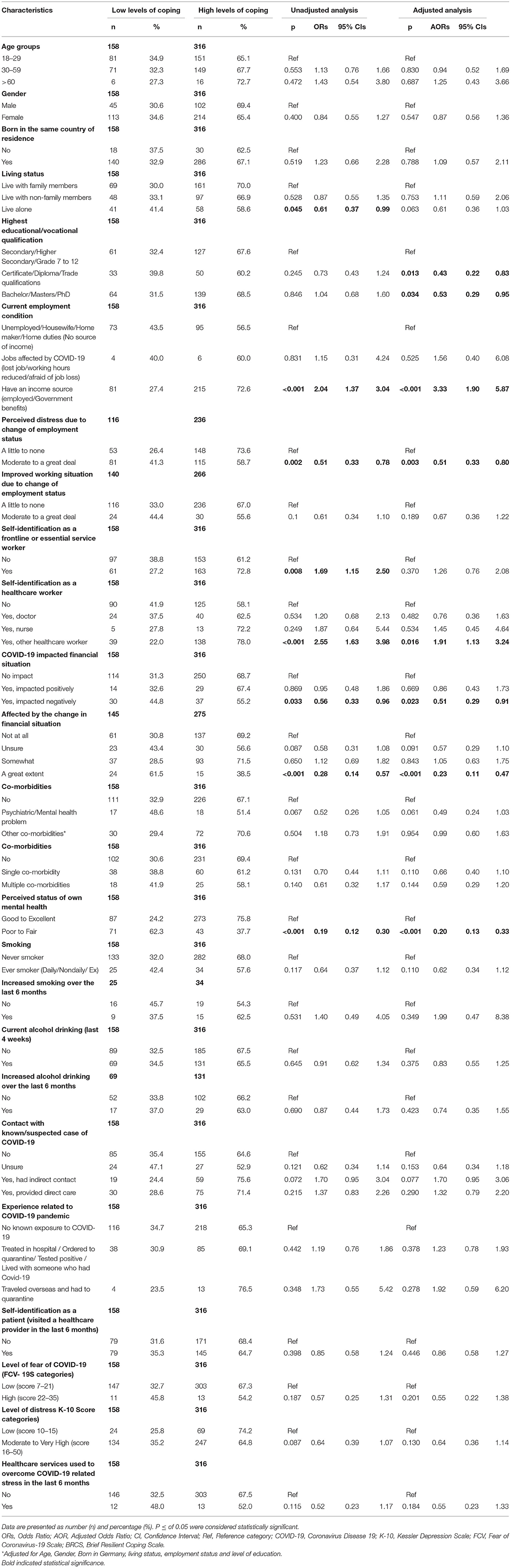
Table 4. Factors associated with coping among the study population (based on BRCS scoring).
The K-10 distress score correlated significantly with the FCV-19S score (spearman's r = 0.331, p < 0.001), the BRCS score showed an inverse relationship with the distress and fear scores (spearman's r = −0.276 and – 0.173, p < 0.001). People with higher distress had higher levels of fear of COVID-19 and lower coping. On the other hand, people with better coping had lower distress and fear of COVID-19 (Table 5).
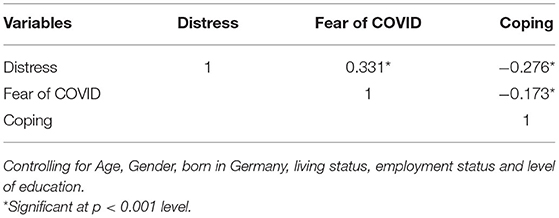
Table 5. Association between psychological distress, coping and fear of COVID-19 using spearman's partial rank correlation.
Moderate to very high levels of psychological distress were associated with being a female, living alone, suffering employment change or worsening the financial situation, and poor mental health, smoking and alcohol consumption. Higher levels of fear of COVID-19 were markable in people of ≥60 years, or those with comorbidities or poor mental health. Having an income source and being a healthcare worker was associated with higher levels of coping.
During the COVID-19 pandemic, the course of psychological disturbances which were associated with psychological distress, fear, and coping strategies among the community members including healthcare workers across the world were well-studied (25). Our study can be seen as a supplement to a global cross-sectional study involving 17 countries (10). The same online instruments were used like the prior global study led by the last author (MAR), but the current study adapted German language. In this study, more females participated than males, which was in line with other similar German studies (16, 26–28) in the first wave of the pandemic, and also supports an Australian (10), Egyptian (15), Bangladeshi (14), Malaysian (13), and global study (10). A possible explanation might be that women were more inclined to share their experiences by participating in the study or women were more impacted due to the pandemic, lockdown or financially that prompted them to participate in the study. The mean age (33.6 years) showed that the study participants of this study were younger than those who were included in similar German studies (16, 26, 27).
For the issue of psychological distress in this study, there were more participants with moderate to very high distress, which was in line with the results of previous studies conducted in Germany (27), Australia (10), Malaysia (13), Bangladesh (14), Hong Kong (19) and globally (10), as well as other studies (28–31). Furthermore, similar to this study, previous studies (10, 13, 14, 27) also reported that females and younger respondents had higher psychological distress compared to the reference group. A previous study showed that women seemed to be more impacted by the pandemic in terms of wellbeing than men (32). According to the findings of this study, the common factors associated with moderate to very high levels of psychological distress were being females, those with change in the employment status, and worsening the financial situation, which was supported by earlier evidence (10, 13, 14). Similarly, Hetkamp and Schweda (33) found that respondents reported reduced sleep quality and moderate generalized anxiety and psychological burdens. A possible explanation could be that participants might experience crucial interference with their everyday lives, which was likely to increase psychological distress while the accessibility of conventional mental health care was limited (25). It could also be assumed that uncertainties about the novel coronavirus, its progression, and variable nature of pandemic, and availability and access to the varied range of evidence also could contribute to the report of various country-wise reports of moderate to a high level of psychological stress. There was also a higher correlation between potential contact with COVID-19 cases, whether direct or indirect, experience with the pandemic, and healthcare use to overcome pandemic stress.
Regarding the issue of fear in this study, there were more participants with low fear, which supports studies conducted in Bangladesh (14), Australia (10), Malaysia (13), and globally (10). That indicated habituation to the threatening situation of the pandemic. However, generalized anxiety could remain elevated over time due to the ongoing nature of pandemic (33). Similarly, a largescale German study among 3,500 randomly selected participants reported mental health (anxiety, depression) impact shortly after the lockdown came into effect (34). This study identified the factors associated with higher fear of COVID-19, which were similar as reported in the earlier studies: being female, and middle-aged, or over 60 (10, 13, 14). Being born in the same country of residence, and having at least a trade/certificate/diploma or bachelor degree were associated with higher levels of fear in this study, which were similar to the study conducted in Bangladesh (14).
Regarding the issue of coping in this study, there were more participants with high levels of coping, which is supported by the previous Malaysian (13) and the global study (10). High resilience coping could be explained by the long period of pandemic in Germany. Having an income source and being a healthcare worker were associated with higher levels of coping, findings of which were different compared to the previous studies (10, 13, 14). Finally, results showed that the COVID-19 pandemic and subsequent lockdown measures in early 2020 might slow the spread of the virus. However, those restrictions forced a sudden and dramatic change to the daily routines of community people, although not all individuals were impacted in the similar way. Some situational factors such as occupation, family status, financial and health impact, personality traits could influence individuals' experience during the ongoing COVID crisis in Germany (35).
This study had few limitations. The participants were included from the Ulm region in Southern Germany, which limits the generalizability across the whole German territory. Furthermore, it wasn't possible to exclude more responses from distressed individuals than non-distressed individuals, potentially resulting in selection bias. Finally, the study findings were limited to individuals who could access to online platforms in order to participate; therefore, there was limited generalizability due to the focus to internet-literate people. However, due to the lockdown measures applied during data collection, an online survey was the only available option to perform this study. One of the most crucial points in our study was collecting the targeted sample size during the pandemic lockdown period. Lastly, this study was the only German study that assessed the factors associated with psychological distress, fear, and coping strategies during the second and third waves of the COVID-19 pandemic. The data collection period coincided with the transition between the second and third waves in Germany, therefore, it was also not unlikely to have increased prevalence of psychological distress amongst the participants who participated in this study.
This study identified levels of psychological distress, fear and coping amongst the community members during the COVID-19 pandemic in the Ulm region in Southern Germany. In addition, several factors and risk groups that were associated with those outcomes, were identified. The identified higher risk groups should be prioritized for receiving mental health support from the relevant healthcare providers such as family physicians and psychiatrists, and automated follow-up reminders could be sent through text messages which would prevent further deterioration of mental health conditions.
The original contributions generated for this study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by the Research Ethical Committee (REC) of the Ulm University (Ethical Approval Number 448/20 – FSt/Sta). The patients/participants provided their written informed consent to participate in this study.
ME had substantial contribution to the conception or design of the study, data collection, and scientific writing of the manuscript. CS-L contributed to the conception and revised the manuscript critically. XW coordinated data collection. KD performed the statistical analysis. MK took part in scientific writing. ER, RA, MD, MG, and BC revised the manuscript critically for important intellectual content. SA, BB, and WC provided critical feedback on the narrative structure and methods and results. MAR conceptualized the study, coordinated data collection, provided critical feedback, and revised the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to acknowledge the support of the study participants, who donated their valuable time to respond to our survey.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.860683/full#supplementary-material
1. COVID Live Update: 230 496 379 Cases and 4 725 702 Deaths from the Coronavirus - Worldometer. Available online at: https://www.worldometers.info/coronavirus/?utm_campaignhomeAdvegas1? (accessed November 23, 2021).
2. Germany COVID: 4 167 891 Cases and 93 736 Deaths - Worldometer. Available from: https://www.worldometers.info/coronavirus/country/germany/ (accessed November 23, 2021).
3. Anderton R, Botelho V, Consolo A, Da Silva AD, Foroni C, Mohr M, et al. The impact of the COVID-19 pandemic on the euro area labour market. Available online at: https://www.ecb.europa.eu/pub/economic-bulletin/articles/2021/html/ecb.ebart202008_02~bc749d90e7.en.html (accessed November 23, 2021).
4. Martins Van Jaarsveld G. The Effects of COVID-19 Among the Elderly Population: A Case for Closing the Digital Divide. Front Psychiatry. (2020) 0:1211. doi: 10.3389/fpsyt.2020.577427
5. Giallonardo V, Sampogna G, Vecchio DV, Luciano M, Albert U, Carmassi C, et al. The impact of quarantine and physical distancing following COVID-19 on mental health: study protocol of a multicentric italian population trial. Front Psychiatry. (2020). 11:533. doi: 10.3389/fpsyt.2020.00533
6. Grossman ER, Benjamin-Neelon SE, Sonnenschein S. Alcohol Consumption during the COVID-19 Pandemic: A Cross-Sectional Survey of US Adults. Int J Environ Res Public Health. (2020) 17:1–10. doi: 10.3390/ijerph17249189
7. Monaghesh E, Hajizadeh A. The role of telehealth during COVID-19 outbreak: a systematic review based on current evidence. BMC Public Heal. (2020). 20:1–9. doi: 10.1186/s12889-020-09301-4
8. Di Tella M, Romeo A, Benfante A, Castelli L. Mental health of healthcare workers during the COVID-19 pandemic in Italy. J Eval Clin Pract. (2020) 26:1583–7. doi: 10.1111/jep.13444
9. Cabarkapa S, Nadjidai SE, Murgier J, Ng CH. The psychological impact of COVID-19 and other viral epidemics on frontline healthcare workers and ways to address it: A rapid systematic review. Brain, Behav Immun - Heal. (2020) 8:100144. doi: 10.1016/j.bbih.2020.100144
10. Rahman MA, Islam SMS, Tungpunkom P, Sultana F, Alif SM, Banik B, et al. COVID-19: Factors associated with psychological distress, fear, and coping strategies among community members across 17 countries. Global Health. (2021) 17:1–19. doi: 10.1186/s12992-020-00624-w
11. Guerrini CJ, Schneider SC, Guzick AG, Amos Nwankwo GN, Canfield I, Fedson S. et al. Psychological distress among the US general population during the COVID-19 pandemic. Front Psychiatry. (2021) 0:810. doi: 10.3389/fpsyt.2021.642918
12. Kosic A, Ignjatović TD, Petrović N. A cross-cultural study of distress during COVID-19 pandemic: some protective and risk factors. Int J Environ Res Public Heal. (2021) 18:7261. doi: 10.3390/ijerph18147261
13. Moni ASB, Abdullah S, Abdullah MFIL, Bin Kabir MS, Alif SM, Sultana F, et al. Psychological distress, fear and coping among Malaysians during the COVID-19 pandemic Gori A, editor. PLoS ONE. (2021) 16:e0257304. doi: 10.1371/journal.pone.0257304
14. Rahman MA, Rahman S, Wazib A, Arafat SMY, Chowdhury ZZ, Uddin BMM, et al. COVID-19 related psychological distress, fear and coping: identification of high-risk groups in Bangladesh. Front Psychiatry. (2021) 12:1399. doi: 10.3389/fpsyt.2021.718654
15. Shehata GA, Gabra R, Eltellawy S, Elsayed M, Gaber DE, Elshabrawy HA. Assessment of anxiety, depression, attitude, and coping strategies of the egyptian population during the COVID-19 pandemic. J Clin Med. (2021) 10:3989. doi: 10.3390/jcm10173989
16. Petzold MB, Bendau A, Plag J, Pyrkosch L, Mascarell Maricic L, Betzler F, et al. Risk, resilience, psychological distress, and anxiety at the beginning of the COVID-19 pandemic in Germany. Brain Behav. (2020) 10:e01745. doi: 10.1002/brb3.1745
17. Stanton R, To QG, Khalesi S, Williams SL, Alley SJ, Thwaite TL, et al. Depression, anxiety and stress during COVID-19: associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int J Environ Res Public Health. (2020) 17:1–13. doi: 10.3390/ijerph17114065
18. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC VJ. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. STROBE Statement—Checklist of items that should be included in reports of cross-sectional studies. Univ los Andes. (2020) 1–2. doi: 10.1016/j.jclinepi.2007.11.008
19. Chair SY, Chien WT, Liu T, Lam L, Cross W, Banik B, et al. Psychological distress, fear and coping strategies among hong kong people during the COVID-19 pandemic. Curr Psychol. (2021) 1:1–20. doi: 10.1007/s12144-021-02338-7
20. Oakley Browne MA, Wells JE, Scott KM, McGee MA. The kessler psychological distress scale in te rau hinengaro: the New Zealand mental health survey. Aust N Z J Psychiatry. (2010) 44:314–22. doi: 10.3109/00048670903279820
21. Ahorsu DK, Lin CY, Imani V, Saffari M, Griffiths MD, Pakpour AH. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addict. (2020). doi: 10.1007/s11469-020-00270-8. [Epub ahead of print].
22. Sinclair VG, Wallston KA. The development and psychometric evaluation of the Brief Resilient Coping Scale. Assessment. (2004) 11:94–101. doi: 10.1177/1073191103258144
24. Baumeister H, Härter M. Prevalence of mental disorders based on general population surveys. Soc Psychiatry Psychiatr Epidemiol. (2007) 42:537–46. doi: 10.1007/s00127-007-0204-1 [Online ahead of print].
25. Kaess M, Moessner M, Koenig J, Lustig S, Bonnet S, Becker K, et al. Editorial perspective: a plea for the sustained implementation of digital interventions for young people with mental health problems in the light of the COVID-19 pandemic. J Child Psychol Psychiatry. (2021) 62:916–18. doi: 10.1111/jcpp.13317
26. Liu S, Heinzel S, Haucke MN, Heinz A. Increased psychological distress, loneliness, and unemployment in the spread of COVID-19 over 6 months in Germany. Med. (2021) 57:1–11. doi: 10.3390/medicina57010053
27. Bendau A, Plag J, Kunas S, Wyka S, Ströhle A, Petzold MB. Longitudinal changes in anxiety and psychological distress, and associated risk and protective factors during the first three months of the COVID-19 pandemic in Germany. Brain Behav. (2021) 11:1–11. doi: 10.1002/brb3.1964
28. Bäuerle A, Steinbach J, Schweda A, Beckord J, Hetkamp M, Weismüller B, et al. Mental health burden of the COVID-19 outbreak in germany: predictors of mental health impairment. J Prim Care Community Heal. (2020) 11:1–8. doi: 10.1177/2150132720953682
29. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatry. (2020) 33:e100213. doi: 10.1136/gpsych-2020-100213
30. Gausman J, Langer A. Sex and gender disparities in the COVID-19 pandemic. J Womens Health (Larchmt). (2020) 29:465–6. doi: 10.1089/jwh.2020.8472
31. French MT, Mortensen K, Timming AR. Psychological distress and coronavirus fears during the initial phase of the COVID-19 pandemic in the United States. J Ment Health Policy Econ. (2020) 23:93–100.
32. Engels ES, Mutz M, Demetriou Y, Reimers AK. Levels of physical activity in four domains and affective wellbeing before and during the Covid-19 pandemic. Arch Public Heal. (2021) 79:1–9. doi: 10.1186/s13690-021-00651-y
33. Hetkamp M, Schweda A, Bäuerle A, Weismüller B, Kohler H, Musche V, et al. Sleep disturbances, fear, and generalized anxiety during the COVID-19 shut down phase in Germany: relation to infection rates, deaths, and German stock index DAX. Sleep Med. (2020) 75:350–3. doi: 10.1016/j.sleep.2020.08.033
34. Mata J, Wenz A, Rettig T, Reifenscheid M, Möhring K, Krieger U, et al. Health behaviors and mental health during the COVID-19 pandemic: A longitudinal population-based survey in Germany. Soc Sci Med. (2021) 287:114333. doi: 10.1016/j.socscimed.2021.114333
Keywords: COVID-19, psychological distress, fear, cross-sectional survey, coping, mental health, Germany
Citation: Elsayed M, Schönfeldt-Lecuona C, Welte XA, Dardeer KT, Kamal MA, Abdelnaby R, Rudek MA, Riedel E, Denkinger M, Gahr M, Connemann BJ, Alif SM, Banik B, Cross W and Rahman MA (2022) Psychological Distress, Fear and Coping Strategies During the Second and Third Waves of the COVID-19 Pandemic in Southern Germany. Front. Psychiatry 13:860683. doi: 10.3389/fpsyt.2022.860683
Received: 23 January 2022; Accepted: 22 March 2022;
Published: 25 April 2022.
Edited by:
Mohammadreza Shalbafan, Iran University of Medical Sciences, IranReviewed by:
Nabi Nazari, Lorestan University, IranCopyright © 2022 Elsayed, Schönfeldt-Lecuona, Welte, Dardeer, Kamal, Abdelnaby, Rudek, Riedel, Denkinger, Gahr, Connemann, Alif, Banik, Cross and Rahman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohamed Elsayed, bW9oYW1lZC5lbHNheWVkQG1laW4uZ214; Muhammad Aziz Rahman, bWEucmFobWFuQGZlZGVyYXRpb24uZWR1LmF1; YXppei5yYWhtYW5AeTdtYWlsLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.