 Arianna Giorgetti
Arianna Giorgetti Francesco Paolo Busardò
Francesco Paolo Busardò Raffaele Giorgetti
Raffaele Giorgetti
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry , 18 April 2022
Sec. Addictive Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.846983
This article is part of the Research Topic Psychiatric and Pharmacotoxicological Insights on Appearance and Performance Enhancing Drugs View all 5 articles
Performance-enhancing drugs (PEDs) are represented by several compounds used to ameliorate the image, the appearance, or an athletic or non-athletic performance. Gamma-hydroxybutyrate (GHB) is an endogenous molecule first used as anesthetic and then marketed as a nutritional supplement with a wide diffusion in the bodybuilding community. The aim of the present work is to provide a toxicological characterization of the use of GHB as a PED, including the scientific basis for its use, the patterns of use/abuse, and the health risks arising from its consumption in this peculiar recreative setting. A literature search was performed on multiple databases including experimental studies on humans and animals as well as epidemiological reports and forensic case reports/series. Experimental studies demonstrated that the use of GHB as a PED is motivated by the release of growth hormone and the induction of sleep. However, the panel of desired performance-related effects was much wider in real cases and epidemiological studies. Even though the use of GHB among bodybuilders has decreased, its use to enhance some kind of performance, particularly sexual ones or social-communicative ones, as well as means to increase mood and perceived energy, is still common.
The term “image-, appearance- or performance-enhancing drug” (IPED, APED, or PED) is used to indicate a wide range of substances used to improve the appearance, to increase musculature as well as self-confidence and self-esteem, and to enhance or increase an athletic performance, which could be professional or non-professional (1, 2). The World Anti-Doping Agency (WADA) has so far included over 192 drugs and methods among the list of banned PEDs, which include androgenic anabolic steroids (AAS), human growth hormone (GH), insulin-like growth factor-1 (IGF-1), and other hormones, but also recreational drugs, such as stimulants, narcotics, cannabinoids, and prescription medications, such as beta agonists and diuretics (3).
However, the universe of APEDs is much wider and complex. Appearance, weight, and eating concerns, rigid or compulsive practices and exercises, body image disturbances and tendencies toward aesthetic and body enhancement are extremely common in western industrial countries (2, 4). Indeed, the use of legal nutritional supplements has been reported to have a prevalence of 49% in the U.S. population and might precede, especially in adolescents, the use of illicit PEDs (2). Moreover, a polypharmacy consumption pattern, with multiple and different substances used to enhance desired effects or counteract the adverse ones, has been demonstrated (5).
Gamma or γ-hydroxybutyrate (GHB) (C4H8O3) is an endogenous short-chain hydroxylated carboxylic acid, exerting a central nervous system (CNS) depressant action (6). This type of effect is thought to be a consequence of its structural similarity to the neurotransmitter gamma-aminobutyric acid (GABA), of which GHB is both a precursor and a metabolite (6, 7). Besides its Food and Drug Administration (FDA) and European agencies approval as treatment of narcolepsy-associated cataplexy and, in some countries, of alcohol dependence (6), GHB has been marketed from 1980 as a performance-enhancer dietary supplement and sold as a pro-drug in products for the gym. Indeed, performance-enhancing and therapeutic effects of GHB, including sleep, vigilance, and mood enhancement, widely overlap. It has been commonly used by body builders (8–11) who acted as early adopters, enhancement drug use innovators, and anticipated an increase in lean muscle mass due to the GHB-induced release of GH (12–15). This lasted until the year 2000, when GHB was listed in the schedule I drugs with the Rape Drug Prohibition Act (6). However, several research projects worldwide are still evaluating therapeutic and possibly performance-enhancing effects.
Renewed attention to the drug has been recently given to GHB as a club drug in various recreational settings (15, 16), in association with the “chemsex” scene (17, 18) or used for drug-facilitated sexual assaults (19).
The aim of the present work is to provide a literature overview of the scientific evidence underlying the use of GHB as a means to enhance the performances, whether connected to appearance, psychomotor, or athletic ones, and to assess the toxicological characteristics and the health risks arising from a specific use of GHB within the framework of PEDs.
A comprehensive literature search was performed on multiple databases (PubMed, Google Scholar, Scopus, ISI Web of Science) focusing on the effects and the use of GHB as a PED. A free-text search with the keywords was done, by combining “GHB,” or “Gamma hydroxybutyrate,” or “sodium oxybate,” and one of the following terms: “performance/-enhancer/PED,” “GH,” or “growth hormone,” “cortisol,” “body building/enhancement,” “weight loss,” “decreased/reduced appetite,” “better sleep,” “self-confidence,” and “muscle growth/strength/tone.”
Keywords were a priori established, but also updated on the basis of the retrieved literature.
Experimental studies, in which previously set and declared GHB doses were administered (20), were included in the present research, prioritizing data from systematic reviews and randomized controlled trials, when available. Both human and animal-based investigations were considered. Data on narcoleptic patients treated with GHB were included, but not randomized controlled trials demonstrating the therapeutical effects of sodium oxybate in these patients. Sexual performances were not specifically targeted by our search and only included when collaterally found.
Studies focused on psychomotor performances already included in the previous paper (20) were not considered, as well as articles specifically focusing on driving abilities.
A second set of information was obtained by epidemiological and forensic case reports/case series of GHB intake.
The search was not restricted to English language documents only, but only papers in which a full-text could be retrieved were included.
Finally, references of the retrieved papers and personal archives of references have been used.
A total of 30 experimental studies were retrieved, including 25 on humans and 5 on animals. A complete list of these studies, including the type, sample, experimental set-up, controlled variables, and main findings, is reported in Table 1, in chronological order.
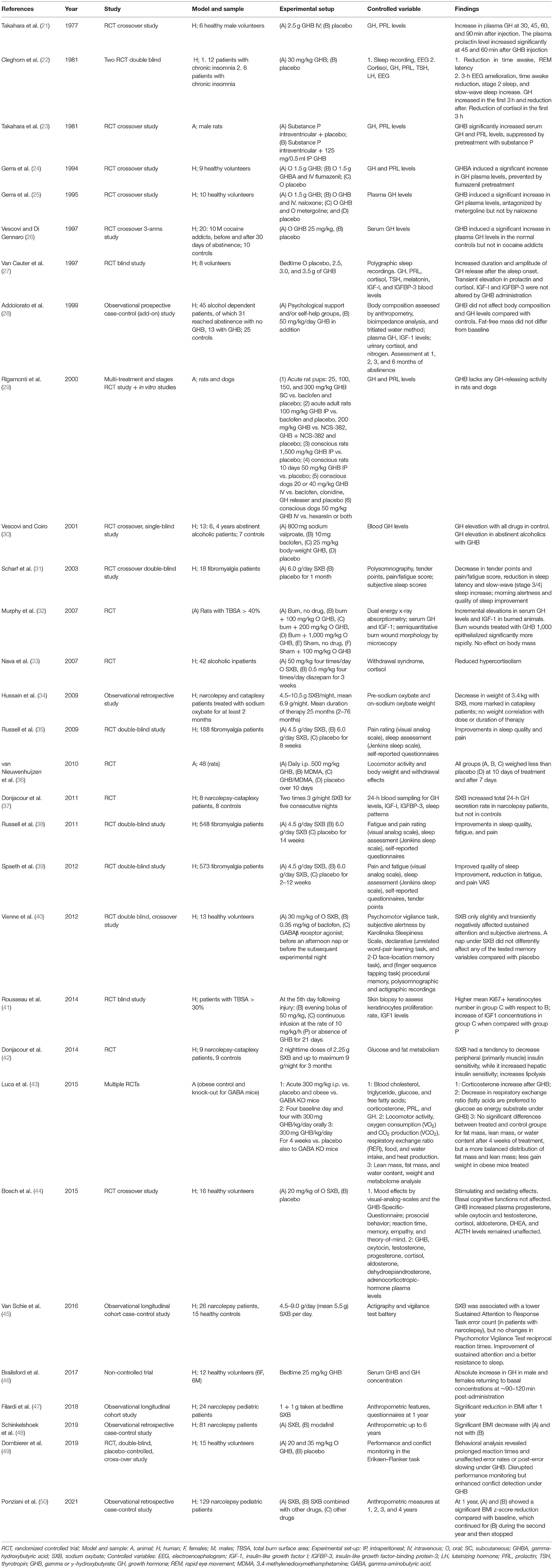
Table 1. Results of the experimental studies.
Most studies corresponded to Randomized Controlled Trial (RCT), with or without a crossover design and the use of placebo or blind/double blind design. Particularly, four studies on fibromyalgia were included, due to the analysis of pain, fatigue, and sleep improvement. One study was a non-controlled trial, six studies were observational, equally distributed between retrospective and longitudinal. Human studies were performed on healthy volunteers, patients with insomnia, or fibromyalgia, narcoleptic patients under sodium oxybate treatment (SXB), including also studies on a pediatric population, and alcohol/substances dependent patients.
Doses of GHB and SXB changed from one study to another, according to the animal/human model, the route of administration and the experimental design. Overall, in humans, GHB/SGB doses tended to be included between 0.8 and 10.5 g, or between 25 and 50 mg/kg, with lower doses in the pediatric population.
Main controlled variables included several hormonal levels, mostly of GH and PRL, but also of cortisol, IGF-1, and many others. Sleep recording and polysomnography were common, also in combination with GH levels to check for an association between variables, or substituted by actigraphy, a validated method to assess sleep parameters. Recently, the latter was also associated with psychomotor abilities test batteries (45). Assessment of body composition and weight was sometimes identified, and performed by means of anthropometry, bioimpedance analysis, and tritiated water method dual-energy x-ray or by simply weighing the body or calculating the BMI. Two articles also performed an extensive and complex evaluation of glucose and lipid metabolism under SXB/GHB treatment (42, 43).
Epidemiological studies and case reports/series are summarized in Table 2. Overall, 24 articles reported the use of GHB or GHB-containing compounds for reasons connected to the enhancing of performance, with a sample number ranging from 1 to 215. When the sample was larger, single information on users were mostly not extractable. The age of users ranged from 17 to 77, with a predominance of around 30 years old, although this could be a bias connected to the study design, which sometimes targeted specifically students. Self-administered doses are often unspecified, the use of a multiple of a “teaspoon” unit or of sips or bottles being reported, with units for retail sale ranging from 30 to 250 g (54). The use of GHB to ameliorate sleep or to resolve insomnia was reported from 1991 to the present. Bodybuilding, ergogenic, and anabolic effects were commonly listed in the desired effects until 2000–2001. Afterward, euphoria, as well as a sensation of increased energy, were more frequently listed as reasons for use (74). Weight loss was both described as a desired and unwanted effect. Curiously, several papers reported the enhancement of communication or of sexual performances as a desired effect, but this was also listed as an unwanted side effect in terms of risky behavior for sexually transmitted infections. Pleasant mood, relaxation, getting rid of daily worries and self-confidence were also listed, as an incentive for use. Finally, the use of GHB as a club drug emerged in connection with the amelioration of dance performance among the desired effects (74).
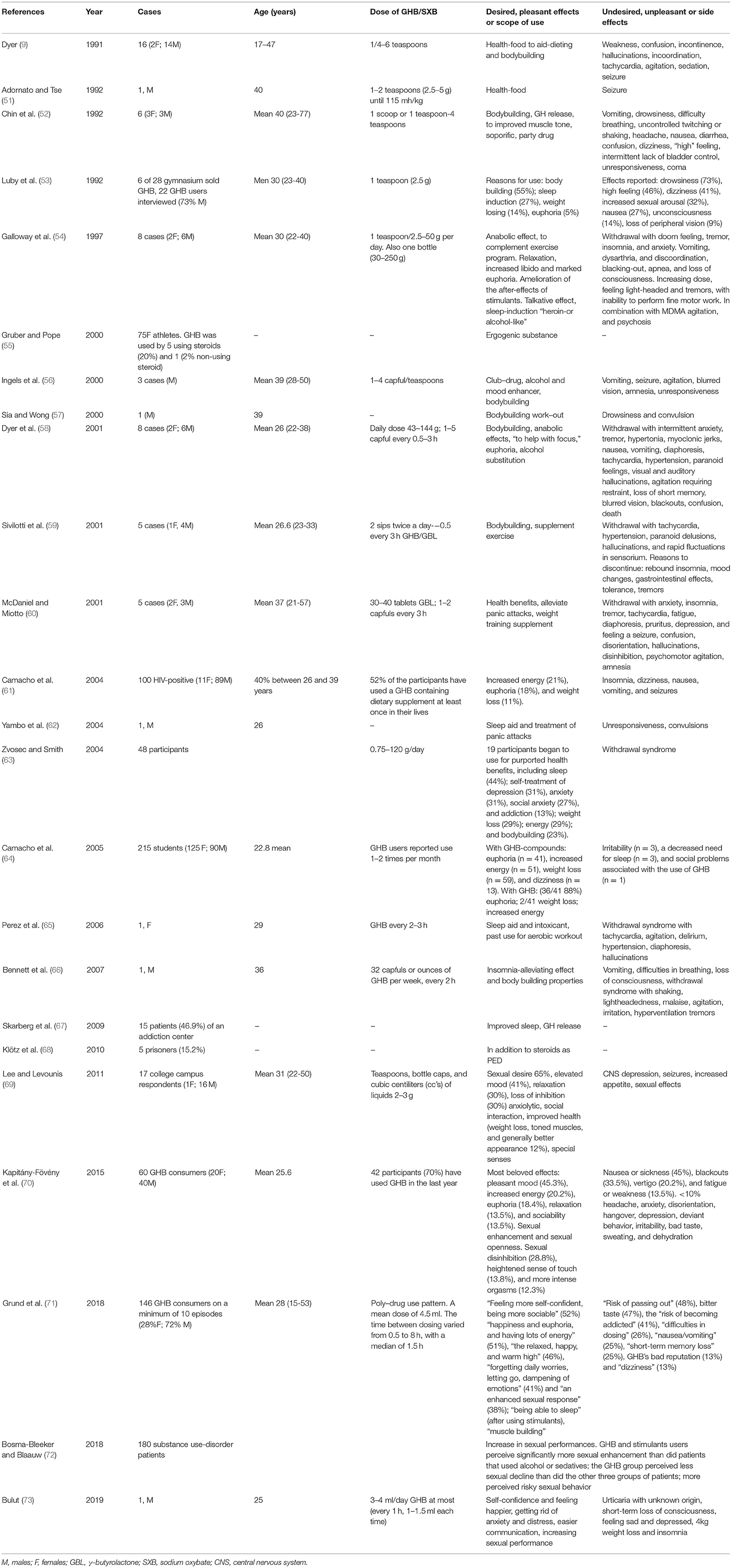
Table 2. Epidemiological and real-case studies.
Adverse effects ranged from urticaria, to headache, weakness, fatigue, irritability, short-term memory losses, nausea, vomiting, loss of weight, diarrhea and incontinence, various grades of central nervous system depression, with dizziness, confusion, hallucinations, incoordination, loss of peripheral vision until unconsciousness, and death. Withdrawal symptoms were commonly described, including a rebound of vomiting, insomnia, anxiety and tremor, psychomotor agitation, or seizures.
After its abandonment as anesthetic agent, GHB was initially introduced in the market for bodybuilding, claiming an anabolic effect, and as a legal nutritional supplement aiding dieting. Our review confirmed that in the past, until the substance was listed among the controlled ones, this application underlined the majority of real case scenarios, resulting in several intoxication cases (9). Although the use in the world of bodybuilding likely decreased over time, the present review highlighted that GHB consumption among users of AAS and of other PEDs is not uncommon also nowadays (5, 55, 57, 59, 63, 68). For example, a publication by Gruber and Pope (55), in the year 2000, highlighted that 20% of woman athletes using steroids also consumed GHB. Bodybuilding was the motivation for use in 63% of cases referred to an emergency department in 2001 for withdrawal syndrome (58). In 2006 and 2007 cases were described with the use of GHB for aerobic workout (65) and bodybuilding properties (66). In 2010 46.9% of the patients of an addiction center and 15.2% of Swedish prisoners responding to surveys/interviews were shown to consume GHB either to improve sleeping or as a PED in addition to steroids (67, 68).
The concept of “performance enhancing” is difficult to define and to distinguish from other kinds of abuse, due to the wide range of aspects to be covered, including image, appearance, athletic, but also self-perception and self-confidence, social or communicative aspects, and sexual performances. The lack of a precise definition, that merges and overlaps with other recreational settings, might partially explain the fact that the issue of the effectiveness of GHB in increasing, and ameliorating performances is still controversial in the literature, and that scientific evidence remains scarce. Considering these limitations, the scope of our study was to provide a toxicological characterization of the use of GHB as a PED, by reviewing the scientific basis as well as desired/undesired effects, patterns of use, and health risks in this peculiar setting.
According to experimental studies and real-case scenarios, the use of GHB among bodybuilders or people seeking an increase in the athletic and muscle-related performance is mainly supported by two types of reasons.
The first one is represented by the release of GH, which has been demonstrated for a short time after the injection or oral administration of GHB in several experimental human and animal settings (21–25, 27, 37, 46). GH is a natural peptide hormone involved in body composition and physical performance, and constitutes one of the PEDs banned by WADA, though the ergogenicity of the substance appears to be weak (75, 76). In the case of GHB, the controversy is way more complex, given the fact that even the GH releasing action has been a matter of debate. Indeed, some studies identified the absence of increase in GH, particularly in cases of cocaine addicts and alcoholics (26, 28) as well as in rats and dogs (29), and the mechanisms underlying this GH secretagog action are not yet fully understood. According to the studies, GHB could stimulate the secretion of GH through the effect on the dopaminergic system, by indirect increase of serotonin levels or by direct effect on the hypothalamus where specific binding sites have been found (21). The role of serotonin emerged by the antagonizing effect of metergoline (a serotonin receptor antagonist) pretreatment (25). However, in both GH and prolactin release, GABA should have a role, as demonstrated by the use of GABA antagonists, such as flumazenil, which prevented hormonal release (24). The difference between GHB and other similar GABA-ergic drugs, such as sodium valproate and baclofen, in the ability of inducing a release of GH in 4-year abstinent alcoholics allows one to hypothesize a different neurotransmitter mediation: GH-releasing activity of GHB might be mediated by muscarinic cholinergic neurotransmission, while GABA might act through a dopaminergic route (30).
The conflicting results obtained by Rigamonti and Móller (29), given the flumazenil-mediated effect (24), were interpreted as if the GH-releasing activity of GHB was mainly due to an endogenous conversion into GABA. Moreover, the absence of GH increase in cocaine addicts and alcoholics might be due to a disruption of the GABAergic system (26, 28).
The disruption of the GABAergic neurotransmission might also hamper the emergence of body modification induced by GHB (28). Indeed, no effect was shown of chronic GHB administration on fat and fat-free mass, wait-to-hip ratio or GH levels in alcoholics. However, this could be due to the low doses of GHB, used to treat alcohol dependency, or to an impairment of the hypothalamic–limbic system and GABAergic neurotransmission in the brain of alcoholics (28). It would be interesting to observe whether these changes in body formation might occur after a longer period of abstinence (4 years), which, as demonstrated by Vescovi and Coiro (30), restored the GHB-mediated release of GH.
Interestingly, a GH release was also seen in animals affected by burn wounds for a total body surface over 40%, in which wound morphology analysis testified a more rapid healing process (epithelialization rates and layer thickness) under high doses of GHB treatment compared with controls (32). Higher keratinocytes proliferation rates were also found in humans with severe burn injuries (41). It has to be underlined that, in the context of athletic performances, a potential for the use of GHB might arise from this skin wound healing effect, once confirmed on a larger scale.
The complexity of the GHB-mediated claimed anabolic or ergogenic effects are also highlighted by the controversial effect on IGF-1, which is physiologically produced in response to GH, and is thought to mediate many of its effects. Indeed, plasma IGF-I and IGFBP-3 levels were not altered by GHB administration in Van Cauter, measured 9 h after drug ingestion (i.e., 7–8 h after the major secretory pulse) (27). No difference was also demonstrated in alcoholics (28) and in the study of Donjacour et al. (37). However, IGF-1 was found increased in burnt animals and humans (32, 41).
Results on cortisol were rather conflicting. Some RCTs found a reduction in cortisol in the first 3 h after GHB administration in patients with chronic insomnia, when GH increased (22), while similar studies, investigating sleep or mood effects in healthy volunteers, reported the opposite (27, 44). In alcoholic inpatients chronically administered GHB, hypercortisolism was reduced (33). Interestingly, one case of Cushing syndrome and one of chorioretinopathy, related to GHB intake, have been reported, suggesting an influence of GHB on cortisol and related hormones (77, 78).
The second type of reasons for GHB use, tightly connected to the previous one, is represented by the sleep-amelioration effect, with a shortening in sleep and rapid eye movement (REM) latency, and increase in slow-wave sleep (22). As shown by experimental studies, GHB administration led to an increase in stages III and IV of non-REM sleep compared with placebo, showing an association, both temporal and quantitative, with GH release. Both EEG amelioration and GH level increase lasted approximately 3 h in patients suffering from chronic insomnia (22). The association was confirmed in healthy volunteers, while prolactin and cortisol levels were not associated with the sleep pattern (27), and in hypocretin-deficient narcolepsy patients, treated with SXB twice a night for 5 days (37). Independently from the GH releasing effect, the induction of sleep, a relaxing effect, and the resolution of insomnia problems were frequently listed as reasons for GHB intake within real cases (52, 53, 62, 63, 65–67). For example, the improvement of sleep was associated with a reduction of fatigue and pain in groups of fibromyalgic patients treated for a month at 4.5 and 6 g SXB daily (31, 37, 73, 75, 76). However, fatigue and weakness were also reported among unpleasant effects of GHB intake (70), and this limits the use of GHB as a muscle-related performance enhancer.
Besides this, experimental studies, epidemiological, and real-cases scenarios also accounted for a wide range of reasons to consume GHB in the amelioration of performances, image, and sociability. The drug is consumed most often in combination with other drugs, as demonstrated by a cross-sectional survey in the Netherlands (71), and the performance enhancing effect of GHB does not only include better sleep and muscle growth, but also weight loss, enhanced sexual desire and performance (70, 72), feeling powerful/stronger, better appearance, toned muscles, increased alertness, general improved health diminished acne, improved social bonding, and increased speech (69).
As for weight loss, a first evidence of a scientific basis for this claiming arose in rats treated daily with GHB and even 7 days after discontinuation of the treatment (36). Patients tend to lose weight (34, 47, 50) as demonstrated in the pediatric population after 1 year of SXB in mono-therapy and after 2 years of combined therapy with other drugs, and this might be connected to an enhanced lipolysis and preferential burning of fatty acids (42, 43). The study of Luca et al. (43) also demonstrated a more balanced distribution of fat and lean mass, together with a reduction in gain weight in obese treated mice. Most of this scientific evidence concern obese patients or those with a baseline altered metabolism. Nevertheless, in real cases, it has been shown that weight loss might be also an unintended effect of SXB (73), with a loss up to approximately 30 kg (79).
Some subjects in the real cases claimed to use GHB “to help focus” in a specific task (58). In contrast with the positive and desired effects reported by some users concerning attention and alertness (69), a study on healthy volunteers monitoring the performance in psychomotor vigilance task and subjective alertness (Karolinska Sleepiness Scale) showed a reduction in attention and alertness after a nap under SXB, although declarative and procedural memory were not affected (40). However, this effect was only transient and the prolonged nap, with increased sleep inertia, might have had a role in the lower psychomotor performance and subjective alertness test. In narcolepsy patients, reaction times were not affected by SXB, while an improvement of sustained attention, with lower error count in a response task, was observed (45). However, once again the ameliorating effect was noted in patients, which were characterized by worse performance compared with controls. A recent randomized control trial on healthy volunteers, conversely, demonstrated prolonged reaction times with altered performance monitoring (49). This might mean that GHB could impair the inner ability of detecting the commission of errors though increasing the visual salience of external stimuli (49).
Beside this, the psychoactive effect of euphoria, connected to an increased confidence and to the feeling of being powerful/stronger represent a sought effect in GHB users (64, 69, 71–73). For example, in one case described by Galloway et al. (54), GHB was initially consumed for anabolic effects, but this was soon superseded by a desire for euphoria. Indeed, as recently shown among participants to a survey, APEDs not only allowed the enhancement of the body and muscles, but were consumed to obtain a psychological effect, such as self-control, the development of knowledge and expertise, sense of meaning, wellbeing, and improved quality of life (80). Euphoria was listed only by 5% of gym GHB users in 1992, but a marked euphoric effect started to be reported in the following studies, reaching 33.5% of respondents (70), 52% of GHB consumers (71) until 88% of respondents among students in 2005 (64). An enhancing effect was also reported in mood, in sociability and in sense of touch, connected to sexual performances (70). Taken together, these data suggests that the reduction in GHB use among bodybuilders might be more related to an unavailability of the drug in health-food stores than to its inefficacy in enhancing some sort of performance (69).
As reported in previous publications (20), in the real-context scenarios, GHB is associated with negative psychomotor performances related to central nervous system depression with altered or impaired vision, drowsiness, incoordination and inability to stand, impaired alertness, blackouts, and memory losses, loss of consciousness until “falling asleep” in unwanted places (9, 51, 53, 56, 61, 62, 69, 71). All these negative effects suggest that GHB has not an objective ameliorative effect on the main psychomotor and psychoactive performances (alertness, memory, vigilance, etc.), except for subjective feelings of increased energy and wellbeing, sociability, and sexual performances. Nevertheless, these effects in self-confidence, sexual performance, communication, and perceived energy cannot be overlooked when talking about GHB and performances, given the fact that these effects are the most desired among GHB users [52% of GHB consumers in a survey of 2018 (71)]. Moreover, as shown by the study of Grund et al. (71), self-confidence-seeking behavior was associated with more coma experiences and the frequency of GHB use correlated with the “enhancing sexual experience” reason for consumption (70). The amelioration of sexual performances is also a reason for use despite the negative effects associated with GHB, including the potential for loss of consciousness (69).
The adverse effects of GHB were at first considered “mild,” as demonstrated in the therapeutical setting. Also, some publications of real-cases intoxication stated that, when discontinuing GHB administration, a full recovery is usual, in the absence of long-term sequelae (52). However, symptoms experienced by users consisted also in severe central nervous system depression with apnea, loss of consciousness, coma (54, 56), and death (58). Our review allowed us to point out some considerations underlining a high risk in a recreational setting, and especially in the context of PEDs.
First of all, when GHB is consumed as a dietary supplement, there is no possibility to accurately control the dosage. In the recreational setting, the use of “teaspoons” of product, as indicated by the bottle of nutritional supplement (53), as well as of scoops, sips, bottle caps, or cubic centiliters (cc's) of liquids were reported, and there is no doubt that a dose can hardly be calculated from this assumption (9, 51, 52, 56, 58–60, 69). The difficulties in self-dosing were also reported by users, who stated that they mostly use plastic vials or bottles, while only a minority tried to reach more accuracy with a syringe (71). On the contrary, in the therapeutic setting, monitoring of the dosages and plasma levels is done, in order to limit potential over- or underdosages.
Real cases also suggest that casual users could self-administer much higher doses than what is actually indicated, from half a teaspoon to four or six, followed by the onset of symptoms such as uncontrolled twitching or difficulty in breathing or unresponsiveness (9, 52). In one case, an entire bottle of GHB was consumed daily (54). In one case presenting to the emergency department for withdrawal symptoms, the higher daily dose was estimated at 43–144 g (58).
Withdrawal symptoms could be severe, spanning from anxiety, hypertonia, myoclonic jerks, and tremors, accompanied by insomnia, gastrointestinal symptoms such as nausea and vomiting, cardiovascular complications such as hypertension and tachycardia, and even confusion, amnesia, psychotic agitation, and delirium (54, 58–60, 65, 66).
Changes in the name of products containing GHB and GBL, homemade, or internet-based preparations further reduce the awareness toward the risks arising from GHB consumption (58, 60, 81). In a recent survey, subjects declared among the benefits of GHB the ease of home-producing the drug (71). It is also perceived as a natural and safe alternative (60), given the fact that it is an endogenous substance and due to the release of GH (24% of respondents in a survey of 2011) (69). In one case described by Galloway et al. (54), a 20-year-old user consumed GHB because he was told that it was an amino acid.
Most of the GHB users, although searching for a health food or natural supplier, experienced a “high” sensation, and 46% of 22 users interviewed in six gyms in 1992, once again disclosing the potential for abuse (52, 53). This is further confirmed by the tendency to escalate self-administered doses (52, 53). Due to the short half-life and rapid metabolism and excretion, the prevention of withdrawal symptoms and the tolerance require the escalation of administrations to every 2 to 4 h in a pattern of “around-the-clock” dosing (54, 58–60, 73, 81). The median gap between doses, in a recent survey, was around 1.5 h (71). This is important since the more frequent the GHB administrations, the higher is the risk for coma (71).
A significant risk hazard is also derived from the combination with other licit or illicit drugs (54, 69–71). While some gymnasium users reported no mixing with other drugs (53, 54, 59), other consumers used GHB in combination with other drugs, from alcohol to methamphetamine, heroin, psychedelics, barbiturates, benzodiazepines, and anti-psychotics (54, 58, 69, 71). The polydrug pattern is sometimes connected to the amelioration of symptoms and after effects either induced by GHB withdrawal, e.g., in the case of alcohol, benzodiazepines, or phenobarbital co-consumption (60); also, GHB could be consumed in the attempt to mitigate the adverse effects produced by other-drugs, especially in the case of methamphetamines (54). The combination of LSD and GHB might be sustained by the anxiolytic effect of GHB, leading to a pleasant experience (54).
Although the consumers are mostly young or middle-aged, and the risk for coma is higher when GHB consumption started at a younger age (71), intoxication cases also highlight that the risk is not only confined to young people but also to older ones, sometimes willing to restore their body appearance and muscular tone (52).
In conclusion, several aspects of the use of GHB as a performance enhancer have been retrieved in the literature, ranging from the more traditional GH release and sleep induction to more recent reasons for use, including the psychoactive subjective effects on mood and energy, and the enhancing of sexual performances. In this view, the term “performance enhancer” should be redefined taking into consideration aspects that transcend only athletic performance. Given the polydrug abuse pattern, the difficulties in the dosages, the tendency to increase the dose until an “around-the-clock” administration is reached, these kinds of recreative consumption appears to be associated with significant health risks.
AG, FB, and RG contributed to the conception and design of the study. AG organized the database and wrote the first draft of the manuscript. RG and FB wrote sections of the manuscript. All authors contributed to the manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Merriam, Webster,. Definition of Performance-Enhancing Drug. Available online at: https://www.merriam-webster.com/dictionary/performance-enhancing+drug (accessed November 29, 2021)
2. Hildebrandt T, Harty S, Langenbucher JW. Fitness supplements as a gateway substance for anabolic-androgenic steroid use. Psychol Addict Behav J Soc. (2012) 26:1–13. doi: 10.1037/a0027877
3. World Anti-Doping Agency. Prohibited List Documents. (2022). Available online at: https://www.wada-ama.org/en/prohibited-list (accessed February 18, 2021).
4. Van Hout MC, Kean J. An exploratory study of image and performance enhancement drug use in a male British South Asian community. Int J Drug Policy. (2015) 26:860–7. doi: 10.1016/j.drugpo.2015.03.002
5. Sagoe D, McVeigh J, Bjørnebekk A, Essilfie MS, Andreassen CS, Pallesen S. Polypharmacy among anabolic-androgenic steroid users: a descriptive metasynthesis. Subst Abuse Treat Prev Policy. (2015) 10:1–19. doi: 10.1186/s13011-015-0006-5
6. White CM. Pharmacologic, pharmacokinetic, and clinical assessment of illicitly used γ-hydroxybutyrate. J Clin Pharmacol. (2017) 57:33–9. doi: 10.1002/jcph.767
7. Felmlee MA, Morse BL, Morris ME. γ-Hydroxybutyric acid: pharmacokinetics, pharmacodynamics, and toxicology. AAPS J. (2021) 23:22. doi: 10.1208/s12248-020-00543-z
8. Friedman J, Westlake R, Furman M. Grievous bodily harm. Neurology. (1996) 46:469–71. doi: 10.1212/WNL.46.2.469
9. Dyer JE. γ-Hydroxybutyrate: A health-food product producing coma and seizurelike activity. Am J Emerg Med. (1991) 9:321–4. doi: 10.1016/0735-6757(91)90050-T
10. Nicholson KL, Balster RL. GHB: a new and novel drug of abuse. Drug Alcohol Depend. (2001) 63:1–22. doi: 10.1016/S0376-8716(00)00191-5
11. Center for Disease Control Prevention (CDC). Epidemiologic Notes and Reports Multistate Outbreak of Poisonings Associated with Illicit Use of Gamma Hydroxy Butyrate. Available online at: https://www.cdc.gov/mmwr/preview/mmwrhtml/00001847.htm (accessed December 29, 2021).
12. Schep LJ, Knudsen K, Slaughter RJ, Vale JA, Mégarbane B. The clinical toxicology of γ-hydroxybutyrate, γ-butyrolactone and 1,4-butanediol. Clin Toxicol Phila Pa. (2012) 50:458–70. doi: 10.3109/15563650.2012.702218
14. McVeigh J, Salinas M, Ralphs R. A sentinel population: the public health benefits of monitoring enhanced body builders. Int J Drug Policy. (2021) 95:102890. doi: 10.1016/j.drugpo.2020.102890
15. Brennan R, Van Hout MC. Gamma-hydroxybutyrate (GHB): a scoping review of pharmacology, toxicology, motives for use, and user groups. J Psychoactive Drugs. (2014) 46:243–51. doi: 10.1080/02791072.2014.921746
16. Trombley TA, Capstick RA, Lindsley CW, DARK. Classics in chemical neuroscience: gamma-hydroxybutyrate (GHB). ACS Chem Neurosci. (2020) 23:3850–9. doi: 10.1021/acschemneuro.9b00336
17. Giorgetti R, Tagliabracci A, Schifano F, Zaami S, Marinelli E, Busardò FP. When “Chems” meet sex: a rising phenomenon called “ChemSex”. Curr Neuropharmacol. (2017) 15:762–70. doi: 10.2174/1570159X15666161117151148
18. Busardò. Replacing GHB with GBL in recreational settings: a new trend in Chemsex. Curr Drug Metab. (2018) 19:1080–5. doi: 10.2174/1389200219666180925090834
19. Carter LP, Pardi D, Gorsline J, Griffiths RR. Illicit gamma-hydroxybutyrate (GHB) and pharmaceutical sodium oxybate (Xyrem®): differences in characteristics and misuse. Drug Alcohol Depend. (2009) 104:1–10. doi: 10.1016/j.drugalcdep.2009.04.012
20. Centola C, Giorgetti A, Zaami S, Giorgetti R. Effects of GHB on psychomotor and driving performance. Curr Drug Metab. (2018) 19:1065–72. doi: 10.2174/1389200219666180124113802
21. Takahara J, Yunoki S, Yakushiji W, Yamauchi J, Yamane Y. Stimulatory effects of gamma-hydroxybutyric acid on growth hormone and prolactin release in humans. J Clin Endocrinol Metab. (1977) 44:1014–7. doi: 10.1210/jcem-44-5-1014
22. Cleghorn JM, Brown GM, Kaplan RD. Effects of Gammahydroxybutyrate (GHB) on sleep and hormones in chronic insomnia. Recent Adv Can Neuropsychopharmacol. (1981) 1981:119–30. doi: 10.1159/000394248
23. Takahara J, Yunoki S, Yamauchi J, Yakushiji W, Hashimoto K, Ofuji T. Inhibitory effects of substance P on the gamma-amino-butyric acid and gamma-hydroxybutyric acid-induced growth hormone and prolactin release in male rats. Life Sci. (1981) 29:1229–31. doi: 10.1016/0024-3205(81)90227-7
24. Gerra G, Caccavari R, Fontanesi B, Marcato A, Fertonani Affini G, Maestri D, et al. Flumazenil effects on growth hormone response to gamma-hydroxybutyric acid. Int Clin Psychopharmacol. (1994) 9:211–5. doi: 10.1097/00004850-199409000-00011
25. Gerra G, Caccavari R, Fontanesi B, Fertonani Affini G, Maestri D, Avanzini P. Naloxone and metergoline effects on growth hormone response to gamma-hydroxybutyric acid. Int Clin Psychopharmacol. (1995) 10:245–50. doi: 10.1097/00004850-199511000-00006
26. Vescovi PP, Di Gennaro C. Failure of gammahydroxy butyric acid to stimulate growth hormone secretion in cocaine addicts. Neuropeptides. (1997) 31:459–62. doi: 10.1016/s0143-4179(97)90040-8
27. Van Cauter E, Plat L, Scharf MB, Leproult R, Cespedes S, L'Hermite-Balériaux M, Copinschi G. Simultaneous stimulation of slow-wave sleep and growth hormone secretion by gamma-hydroxybutyrate in normal young. Men J Clin Invest. (1997) 100:745–53. doi: 10.1172/JCI119587
28. Addolorato G, Capristo E, Gessa GL, Caputo F, Stefanini GF, Gasbarrini G. Long-term administration of GHB does not affect muscular mass in alcoholics. Life Sci. (1999) 65:PL191–6. doi: 10.1016/S0024-3205(99)00395-1
29. Rigamonti AE, Müller EE. Gamma-hydroxybutyric acid and growth hormone secretion studies in rats and dogs. Alcohol Fayettev N. (2000) 20:293–304. doi: 10.1016/s0741-8329(99)00094-4
30. Vescovi PP, Coiro V. Different control of GH secretion by gamma-amino- and gamma-hydroxy-butyric acid in 4-year abstinent alcoholics. Drug Alcohol Depend. (2001) 61:217–21. doi: 10.1016/s0376-8716(00)00149-6
31. Scharf MB, Baumann M, Berkowitz DV. The effects of sodium oxybate on clinical symptoms and sleep patterns in patients with fibromyalgia. J Rheumatol. (2003) 30:1070–4.
32. Murphy KD, Rose MW, Chinkes DL, Meyer WJ, Herndon DN, Hawkins HK, et al. The effects of gammahydroxybutyrate on hypermetabolism and wound healing in a rat model of large thermal injury. J Trauma. (2007) 63:1099–107. doi: 10.1097/TA.0b013e318157d9d0
33. Nava F, Premi S, Manzato E, Campagnola W, Lucchini A, Gessa GL. Gamma-hydroxybutyrate reduces both withdrawal syndrome and hypercortisolism in severe abstinent alcoholics: an open study vs. diazepam. Am J Drug Alcohol Abuse. (2007) 33:379–92. doi: 10.1080/00952990701315046
34. Husain AM, Ristanovic RK, Bogan RK. Weight loss in narcolepsy patients treated with sodium oxybate. Sleep Med. (2009) 10:661–3. doi: 10.1016/j.sleep.2008.05.012
35. Russell IJ, Perkins AT, Michalek JE. Oxybate SXB-26 Fibromyalgia Syndrome Study Group. Sodium oxybate relieves pain and improves function in fibromyalgia syndrome: a randomized, double-blind, placebo-controlled, multicenter clinical trial. Arthritis Rheum. (2009) 60:299–309. doi: 10.1002/art.24142
36. van Nieuwenhuijzen PS, Long LE, Hunt GE, Arnold JC, McGregor IS. Residual social, memory and oxytocin-related changes in rats following repeated exposure to γ-hydroxybutyrate (GHB), 3,4-methylenedioxymethamphetamine (MDMA) or their combination. Psychopharmacology. (2010) 212:663–74. doi: 10.1007/s00213-010-1986-5
37. Donjacour CEHM, Aziz NA, Roelfsema F, Frölich M, Overeem S, Lammers GJ, et al. Effect of sodium oxybate on growth hormone secretion in narcolepsy patients and healthy controls. Am J Physiol Endocrinol Metab. (2011) 300:E1069–1075. doi: 10.1152/ajpendo.00623.2010
38. Russell JI, Holman AJ, Swick TJ, Alvarez-Horine S, Wang GY, Guinta D. Sodium Oxybate 06-008 FM Study Group. Sodium oxybate reduces pain, fatigue, and sleep disturbance and improves functionality in fibromyalgia: results from a 14-week, randomized, double-blind, placebo-controlled study. Pain. (2011) 152:1007–17. doi: 10.1016/j.pain.2010.12.022
39. Spaeth M, Bennett RM, Benson BA, Wang YG, Lai C, Choy EH. Sodium oxybate therapy provides multidimensional improvement in fibromyalgia: results of an international phase 3 trial. Ann Rheum Dis. (2012) 71:935–42. doi: 10.1136/annrheumdis-2011-200418
40. Vienne J, Lecciso G, Constantinescu I, Schwartz S, Franken P, Heinzer R, et al. Differential effects of sodium oxybate and baclofen on EEG, sleep, neurobehavioral performance, and memory. Sleep. (2012) 35:1071–83. doi: 10.5665/sleep.1992
41. Rousseau A-F, Bargues L, Bever HL, Vest P, Cavalier E, Ledoux D, et al. Effect of gamma-hydroxybutyrate on keratinocytes proliferation: a preliminary prospective controlled study in severe burn patients. Int J Crit Illn Inj Sci. (2014) 4:108–13. doi: 10.4103/2229-5151.134150
42. Donjacour CEHM, Aziz NA, Overeem S, Kalsbeek A, Pijl H, Lammers GJ. Glucose and fat metabolism in narcolepsy and the effect of sodium oxybate: a hyperinsulinemic-euglycemic clamp study. Sleep. (2014) 37:795–801. doi: 10.5665/sleep.3592
43. Luca G, Vienne J, Vaucher A, Jimenez S, Tafti M. Central and peripheral metabolic changes induced by gamma-hydroxybutyrate. Sleep. (2015) 38:305–13. doi: 10.5665/sleep.4420
44. Bosch OG, Eisenegger C, Gertsch J, von Rotz R, Dornbierer D, Gachet MS, et al. Gamma-hydroxybutyrate enhances mood and prosocial behavior without affecting plasma oxytocin and testosterone. Psychoneuroendocrinology. (2015) 62:1–10. doi: 10.1016/j.psyneuen.2015.07.167
45. van Schie MKM, Werth E, Lammers GJ, Overeem S, Baumann CR, Fronczek R. Improved vigilance after sodium oxybate treatment in narcolepsy: a comparison between in-field and in-laboratory measurements. J Sleep Res. (2016) 25:486–96. doi: 10.1111/jsr.12386
46. Brailsford A, Bartlett C, Kicman A, Cowan D. Increases in serum growth hormone concentrations associated with GHB administration. J Anal Toxicol. (2017) 41:54–9. doi: 10.1093/jat/bkw107
47. Filardi M, Pizza F, Antelmi E, Ferri R, Natale V, Plazzi G. In-field assessment of sodium oxybate effect in pediatric type 1 narcolepsy: an actigraphic study. Sleep. (2018) 41:zsy050. doi: 10.1093/sleep/zsy050
48. Schinkelshoek MS, Smolders IM, Donjacour CE, van der Meijden WP, van Zwet EW, Fronczek R, et al. Decreased body mass index during treatment with sodium oxybate in narcolepsy type 1. J Sleep Res. (2019) 28:e12684. doi: 10.1111/jsr.12684
49. Dornbierer DA, Kometer M, Von Rotz R, Studerus E, Gertsch J, Gachet MS, et al. Effects of gamma-hydroxybutyrate on neurophysiological correlates of performance and conflict monitoring. Eur Neuropsychopharmacol J Eur Coll Neuropsychopharmacol. (2019) 29:539–48. doi: 10.1016/j.euroneuro.2019.02.004
50. Ponziani V, Pizza F, Zenesini C, Vignatelli L, Pession A, Plazzi G. BMI changes in pediatric type 1 narcolepsy under sodium oxybate treatment. Sleep. (2021) 44:zsaa295. doi: 10.1093/sleep/zsaa295
51. Adornato BT, Tse V. Another health food hazard—gamma-hydroxybutyrate-induced seizures. West J Med. (1992) 157:471.
52. Chin MY, Kreutzer RA, Dyer JE. Acute poisoning from gamma-hydroxybutyrate in California. West J Med. (1992) 156:380–4.
54. Galloway GP, Frederick SL, Staggers FE Jr, Gonzales M, Stalcup SA, Smith DE. Gamma-hydroxybutyrate: an emerging drug of abuse that causes physical dependence. Addiction. (1997) 92:89–96. doi: 10.1111/j.1360-0443.1997.tb03640.x
55. Gruber AJ, Pope HG. Psychiatric and medical effects of anabolic-androgenic steroid use in women. Psychother Psychosom. (2000) 69:19–26. doi: 10.1159/000012362
56. Ingels M, Rangan C, Bellezzo J, Clark RF. Coma and respiratory depression following the ingestion of GHB and its precursors: three cases. J Emerg Med. (2000) 19:47–50. doi: 10.1016/s0736-4679(00)00188-8
57. Sia Y, Wong Y. Case report: gamma-hydroxybutyrate poisoning. Hong Kong J Emerg Med. (2000) 7:166–8. doi: 10.1177/102490790000700308
58. Dyer JE, Roth B, Hyma BA. Gamma-hydroxybutyrate withdrawal syndrome. Ann Emerg Med. (2001) 37:147–53. doi: 10.1067/mem.2001.112985
59. Sivilotti MLA, Burns MJ, Aaron CK, Greenberg MJ. Pentobarbital for severe gamma-butyrolactone withdrawal. Ann Emerg Med. (2001) 38:660–5. doi: 10.1067/mem.2001.119454
60. McDaniel CH, Miotto KA. Gamma hydroxybutyrate (GHB) and gamma butyrolactone (GBL) withdrawal: five case studies. J Psychoactive Drugs. (2001) 33:143–9. doi: 10.1080/02791072.2001.10400479
61. Camacho A, Matthews SC, Dimsdale JE. Use of GHB compounds by HIV-positive individuals. Am J Addict. (2004) 13:120–7. doi: 10.1080/10550490490436019
62. Yambo CM, McFee RB, Caraccio TR, McGuigan M. The inkjet cleaner “Hurricane”—another GhB recipe. Vet Hum Toxicol. (2004) 46:329–30.
63. Zvosec DL, Smith SW. γ-Hydroxybutyrate addiction and withdrawal: from the γ-Hydroxybutyrate addiction study. Ann Emerg Med. (2004) 44:S91. doi: 10.1016/j.annemergmed.2004.07.297
64. Camacho A, Matthews SC, Murray B, Dimsdale JE. Use of GHB compounds among college students. Am J Drug Alcohol Abuse. (2005) 31:601–7. doi: 10.1081/ADA-200062545
65. Perez E, Chu J, Bania T. Seven days of gamma-hydroxybutyrate (GHB) use produces severe withdrawal. Ann Emerg Med. (2006) 48:219–20. doi: 10.1016/j.annemergmed.2006.03.040
66. Bennett WRM, Wilson LG, Roy-Byrne PP. Gamma-hydroxybutyric acid (GHB) withdrawal: a case report. J Psychoactive Drugs. (2007) 39:293–6. doi: 10.1080/02791072.2007.10400616
67. Skarberg K, Nyberg F, Engstrom I. Multisubstance use as a feature of addiction to anabolic-androgenic steroids. Eur Addict Res. (2009) 15:99–106. doi: 10.1159/000199045
68. Klötz F, Petersson A, Hoffman O, Thiblin I. The significance of anabolic androgenic steroids in a Swedish prison population. Compr Psychiatry. (2010) 51:312–8. doi: 10.1016/j.comppsych.2009.05.007
69. Lee SJ, Levounis P. Gamma hydroxybutyrate: an ethnographic study of recreational use and abuse. J Psychoactive Drugs. (2008) 40:245–53. doi: 10.1080/02791072.2008.10400639
70. Kapitány-Fövény M, Mervó B, Corazza O, Kökönyei G, Farkas J, Urbán R, et al. Enhancing sexual desire and experience: an investigation of the sexual correlates of gamma-hydroxybutyrate (GHB) use. Hum Psychopharmacol Clin Exp. (2015) 30:276–84. doi: 10.1002/hup.2491
71. Grund J-P, de Bruin D, van Gaalen S. Going knock-recurrent comatose GHB intoxication in the Netherlands and Flanders (Belgium). Int J Drug Policy. (2018) 58:137–48. doi: 10.1016/j.drugpo.2018.06.010
72. Bosma-Bleeker MH, Blaauw E. Substance use disorders and sexual behavior; the effects of alcohol and drugs on patients' sexual thoughts, feelings and behavior. Addict Behav. (2018) 87:231–7. doi: 10.1016/j.addbeh.2018.07.005
73. Bulut H. A new psychoactive substance, gamma hydroxybutyrate (GHB): a case report. Arch Neuropsychiatry. (2019) 56:229–31. doi: 10.29399/npa.23198
74. Dijkstra BAG, Beurmanjer H, Goudriaan AE, Schellekens AFA, Joosten EAG. Unity in diversity: a systematic review on the GHB using population. Int J Drug Policy. (2021) 94:103230. doi: 10.1016/j.drugpo.2021.103230
75. Erotokritou-Mulligan I, Holt RI, Sönksen PH. Growth hormone doping: a review. Open Access J Sports Med. (2011) 2:99–111. doi: 10.2147/OAJSM.S11626
76. Baumann GP. Growth hormone doping in sports: a critical review of use and detection strategies. Endocr Rev. (2012) 33:155–86. doi: 10.1210/er.2011-1035
77. Busardò FP, Frati P, Sanzo MD, Napoletano S, Pinchi E, Zaami S, et al. The impact of nandrolone decanoate on the central nervous system. Curr Neuropharmacol. (2015) 13:122–31. doi: 10.2174/1570159X13666141210225822
78. Razenberg AJ, Elte JWF, Rietveld AP, van Zaanen HCT, Cabezas MC. A “smart” type of Cushing's syndrome. Eur J Endocrinol. (2007) 157:779–81. doi: 10.1530/EJE-07-0538
79. Noujaim MG, Mourad A, Clough JD. Sodium oxybate: a cause of extreme involuntary weight loss in a young lady. Case Rep Med. (2019) 2019:6537815. doi: 10.1155/2019/6537815
80. Macho J, Mudrak J, Slepicka P. Enhancing the self: amateur bodybuilders making sense of experiences with appearance and performance-enhancing drugs. Front Psychol. (2021) 12:648467. doi: 10.3389/fpsyg.2021.648467
Keywords: gamma hydroxybutyrate (GHB), sodium oxybate, performance-enhancing drugs (PEDs), psychoactive performance, forensic toxicology
Citation: Giorgetti A, Busardò FP and Giorgetti R (2022) Toxicological Characterization of GHB as a Performance-Enhancing Drug. Front. Psychiatry 13:846983. doi: 10.3389/fpsyt.2022.846983
Received: 04 January 2022; Accepted: 25 February 2022;
Published: 18 April 2022.
Edited by:
Fabrizio Schifano, University of Hertfordshire, United KingdomReviewed by:
John Martin Corkery, University of Hertfordshire, United KingdomCopyright © 2022 Giorgetti, Busardò and Giorgetti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raffaele Giorgetti, ci5naW9yZ2V0dGlAdW5pdnBtLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.