 Tak Sang Chow
Tak Sang Chow Catherine So Kum Tang
Catherine So Kum Tang Tiffany Sok U. Siu
Tiffany Sok U. Siu Helen Sin Hang Kwok
Helen Sin Hang Kwok
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 13 May 2022
Sec. Public Mental Health
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.845803
This article is part of the Research Topic Neuropsychological Mechanism of Psychological Resilience in Relation to Mental Health Outcomes Across the Lifespan View all 5 articles
Family resilience, which refers to the processes through which a family adapts to and thrives from adversities, has growing importance in recent years. In response to the need for further research on family resilience, the present research aims to abbreviate and validate Sixbey's Family Resilience Assessment Scale (FRAS) into a 16-item version Family Resilience Scale Short Form in the US (FRS16) and Chinese (FRS16_C) samples. The samples included 1,236 (Study 1) and 1,135 (Study 2) participants from the US and China, respectively. Results of confirmatory factor analysis (CFA) supported the proposed three-factor structure of FRS16: Family Communication and Connectedness, Positive Framing, and External Support across two samples. Overall, the reliability and validity of full and subscales of FRS16 and FRS16_C were satisfactory. Multi-group CFA revealed that both configural and metric invariance are supported, suggesting that participants in the US and Chinese samples assign comparable meaning to the latent factors of FRS16. Results suggested that FRS16 and FRS16_C are valid instruments for family resilience in the US and Chinese samples.
Since 1990s, the term “family resilience” has emerged in family sciences to signify family processes that create perseverance, accommodation, and growth in responses to crises and challenges (1–3). The conceptualization of family resilience entails two important features. First, family resilience is more than the average of individual members' resilience, but rather encompasses dynamic, structural features of the family system which could only be understood through a broader, relational framework (4). Second, it involves more than the capacity to survive a crisis, but also to realize the potential for growth out of difficulties (3). Overcoming a challenge together, a family can emerge as more resourceful, connected, and loving in facing future crises.
Building upon earlier strength-based family paradigms which emphasize the interaction between stressors, family perceptions and protective factors in developing resilience (e.g., The Double ABCX model; (5), Walsh (3) proposed a family resilience model that specifies three overarching processes that promote family resilience, each of which consists of several subprocesses. The three overarching processes are Family Belief Systems, Organizational Patterns, and Communication Processes. Family Belief Systems refer to the shared reality that might facilitate normalizing and overcoming a crisis via meaning-making, maintaining positivity, and a transcendent, spiritual grounding. Organizational Patterns refer to the ways families operate during a crisis. Lastly, Communication Processes involve clear communication, open emotional expression, and collaborative problem-solving. In this framework, family resilience is a dynamic process that varies across families, contexts, and time.
This family resilience framework has tremendous implications on how to successfully cope with abrupt and persistent crises including caregiving for a member with chronic illnesses (6), traumatic societal events such as natural disaster (7) and pandemic (8), divorce (9), and the death of a family member (10). Importantly, family resilience influences children's positive development (11, 12). Thus, prevention and intervention programs have been developed to identify and foster family resilience, in the hope of preserving family functioning and well-being during difficult situations [e.g., (13–15)].
In view of the theoretical importance of the family resilience construct and the lack of quantitative measurement of it, Sixbey (16) developed the Family Resilience Assessment Scale (FRAS). The 54-item FRAS was developed upon Walsh (3)'s family resilience model. It includes six subscales, which reflect Walsh's three overarching family resilience processes (Family Belief Systems, Organization Patterns, and Communication Processes). Family Belief Systems are associated with the subscales Maintaining a Positive Outlook, Ability to Make Meaning of Adversity, and Family Spirituality. Organization Patterns are associated with two subscales, Utilizing Social and Economic Resources and Family Connectedness. Finally, Communication Processes are associated with the subscale Family Communication and Problem Solving.
Ever since its birth, researchers have observed the predictive value of the FRAS on mental health measures. For instance, higher score on the FRAS was associated with lower depression, anxiety, stress (17), and higher individual resilience (18, 19). It also served as a protective factor for cancer patients and their spouses (20) as well as young people with severe epilepsy (21). Relevant to the current context, it also mitigated the negative effect of pandemic-related stressors on stress severity (17). Thus, far, the FRAS has been translated to different languages such as Chinese (22–24), Turkish (25), and Polish (26).
The original FRAS consists of 54 items. Its length makes it cumbersome as a process or an outcome measure especially in studies that involve clinical trials, or longitudinal mutli-wave investigation, as researchers are faced with limited assessment time. A brief measure of family resilience is needed to advance the research of family resilience. To our best understanding, the shortest form of FRAS was the Chinese version which still contains 32 items (24), while most other versions have more than 40 items (e.g., (22)). Furthermore, recent studies reveal the possibility of a more parsimonious factor structure of the FRAS. While Kaya and Arici (25) found a 4-factor solution, a 3-factor model showed adequate fit in Li et al. (24)'s study.
As suggested by Burisch (27), acceptable validities and reliabilities can be achieved by a fairly small number of items. The present study proposed a 3-factor model which is built upon Li et al. (24)'s findings. The three proposed factors are (1) Communication and Connectedness; (2) Positive Framing; and (3) External Resources. The first factor combines the Family Communication and Family Connectedness factors in the original scale as effective family communication can only be achieved with an optimal balance of mutual support and respect of individuals' autonomy (28). These two elements are theoretically intertwined. The second factor, Positive framing, refers to the attitudes or beliefs that help a family to maintain positivity during adversities. It combines the subcomponents Maintaining a Positive Outlook and Making Meaning of Adversities in the original FRAS which are two crucial components across different family resilience conceptualizations (29, 30). External Resources are important for families to cope with internal and external crises. Across the literature, social [e.g., neighbor; (31)], economic [e.g., welfare system; (32)], and spiritual [e.g., church or other religious institutions; (33)] resources are important external support for family to function well during crises. Thus, this factor captures the subcomponents Utilizing Social and Economic Resources and Family Spirituality in the original scale. Therefore, the present studies aim to derive a short scale of family resilience with a more parsimonious 3-factor structure to make family resilience research more feasible and less time-consuming. We started with selecting essential items which have the highest factor loadings from the original FRAS and then examined its psychometric properties in a US and then in a Chinese sample. Since past studies found that family resilience was associated with relationship functioning and well-being, the FRAS is hypothesized to be associated with family cohesion (34), relationship satisfaction (35), general health (36), quality of life (37), and perceived community support (38). Overall, the current research aims to abbreviate and validate Sixbey's Family Resilience Assessment Scale (FRAS) into a shorter form and cross-validated it in both the US (study 1) and Chinese (study 2) samples.
Study 1 aims to derive a reliable and valid short scale to measure family resilience based on FRAS in the US sample. We will first identify the most essential items of FRAS according to factor loadings and item-to-subscale correlation. Then, a factorial structure will be identified with CFA. Furthermore, its associations with related variables and the reliability of the composite and subscales will also be examined.
We recruited participants from the US via Amazon's Mechanical Turk (MTurk), a commonly used online crowdsourcing platform that has a diverse and stable subject pool (39). Past studies suggested that participants recruited from MTurk is more representative of the US sample in comparison to face-to-face convenience samples (40). Consent form was presented on the first page of the online survey, participants indicated understanding of their rights and granted consent by pressing “continue to next page.” Participants' confidentiality was guaranteed that personal identities are not traceable, and the data will only be used for research purposes. After data exportation from the platform, data will be stored in a local drive and is solely accessible to members of the research team. Participants must be US citizens aged above 18. They were given 1 week to complete the survey and were compensated with 0.5 USD through the built-in payment system in MTurk upon completion. This study was approved by the Human Research Ethics Committee of the affiliated university of the research team.
After excluding respondents who provided statistical improbable answers (e.g., worked for 500 h on average per week in the past 12 months) and did not provide answers to the key variables (i.e., family resilience and validation instruments), 1,236 participants were available for the CFA analysis. The average age of participants was 36.17 (SD = 10.83, range = 18 to 75), and 63.7% were male. The majority of them were highly educated (92.1 % obtained a bachelor's degree or above), married (79.4%), and with an annual household income of $40,000 or above (71.1%) (see Table 1).
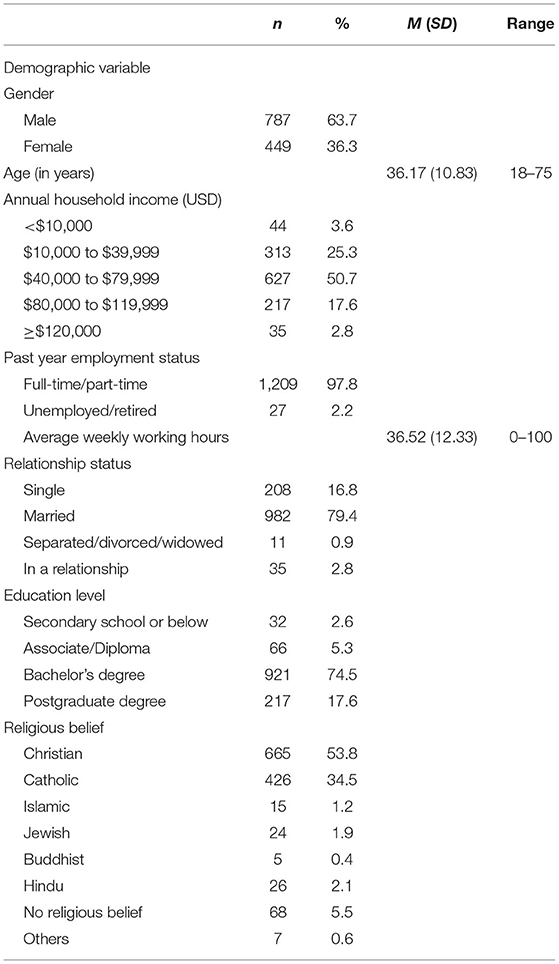
Table 1. Descriptive statistics of demographics of US sample.
First, we selected essential items for the current proposed Family Resilience Scale Short Form from Family Resilience Assessment Scale (FRAS) (16). Considering the original scale has disproportionately large numbers of items in the Family Communication and Problem Solving (FCPS) subscale, the items of our proposed scale were selected with two criteria based on Sixbey's findings in 2005: (1) Two items with the highest factor loadings for each subscale (except for FCPS) (2) For FCPS, 6 items with both factor loadings and item-to-subscale correlation higher than 0.7. As a result, 16 items were selected for the short form (see Appendix A). Thus, the abbreviation for Family Resilience Scale Short Form will be FRS16. Participants indicated their agreement with 16 statements on a 4-point scale (1 = strongly disagree to 4 = strongly agree).
Quality of life was accessed with the 8-item EUROHIS-QOL scale which has been validated across different cultures (41). Participants indicated their satisfaction with different aspects of their lives on a 5-point scale (1 = not at all, 5 = completely).
General health was accessed with the General Health Questionnaire-12 [GHQ-12; (42)] which is intended to tap on respondents' recent functioning such as mood, sleeping quality and concentration compared to their normal state. The items are rated on a 4-point scale (1 = less than usual, 4 = much more than usual), and scores were summed across items with a higher score reflecting worse health.
Relationship satisfaction was accessed with the 7-item Relationship Assessment Scale [RAS; (43)]. Participants indicated how satisfied they were with their partner and relationship based on a 5-point scale (1 = low satisfaction, 5 = high satisfaction).
Family cohesion was accessed with the 9-item family cohesion subscale of the Family Environment Scale (44). Participants indicated their agreement with the statements that described their family (0 = disagree, 1 = agree), with a higher summation score reflecting higher family cohesion.
Perceived community support was assessed with the 2-item integration and need fulfillment subscale of the Brief Sense of Community Scale (45) with a 5-point scale (1 = strongly disagree, 5 = strongly agree) to reflect the degree to which participants felt supported by their community.
The descriptive statistics for demographic and main variables are summarized in Tables 1, 2, respectively.
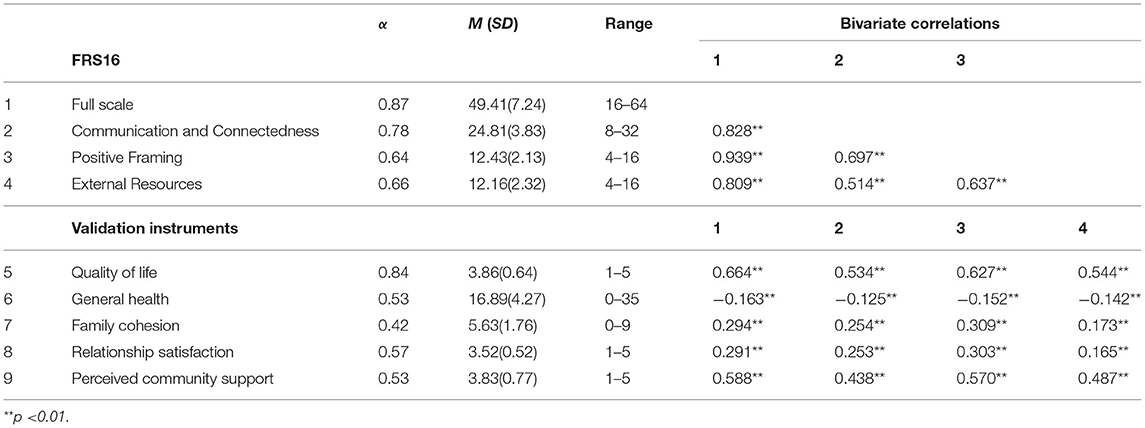
Table 2. Descriptive statistics of main variables of US sample.
The factor structure of the proposed three-factor model was assessed with CFA. CFA was performed with the maximum likelihood estimation in Mplus 8.3 (46). As suggested by the CFA results, the proposed three-factor model has reasonable model fit: χ2 (99) = 699.15, p <0.001; SRMR = 0.046; RMSEA = 0.070, CI = [0.065, 0.075]; TLI = 0.86; CFI = 0.88. The factor solution and standardized factor-loadings of all items are shown in Figure 1. Additionally, four theoretically meaningful alternative models were also examined. In particular, the single-factor model assumes only one underlying latent factor of family resilience. The two-factor model distinguishes items into either external or internal resilience factors. The five-factor model involves problem solving, social and economic resources, positivity, family spiritually, and communication and connectedness. While the six-factor model is the one proposed in the original FRAS. As shown in Table 3, the fit indices improved as the number of factors increased in the model, but this trend slowed down when the number of factors reached to three. Since there were no significant differences in fit indices, the three-factor model seems to have the best balance of parsimony and interpretability of item clustering.
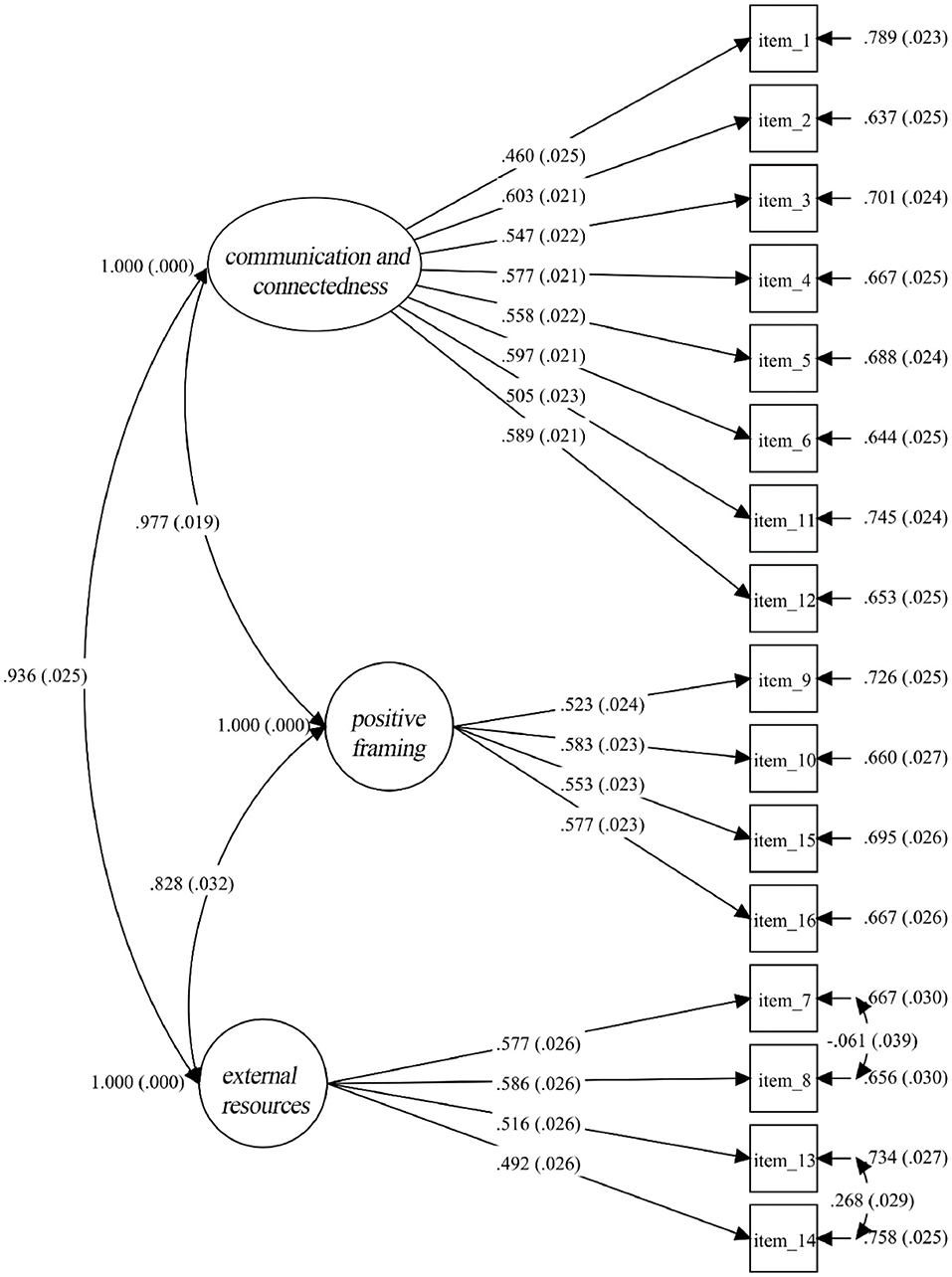
Figure 1. Factor structure and standardized factor loadings of FRS16.

Table 3. Model fit indices of models with different number of factors.
Content validity was examined with the item-to-scale and item-to-subscale correlations. As shown in Table 4, all items were significantly and moderately correlated to both its subscale and full scale (rs ≥ 0.36).
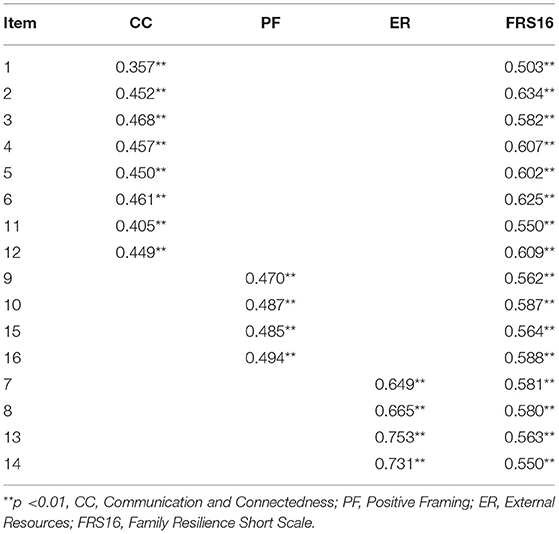
Table 4. Item-to-scale and item-to-subscale correlations.
We also examined whether FRS16 is associated with quality of life, general life and family cohesion, relationship satisfaction and perceived community support. As shown in Table 2, all of the subscales and the full scale of FRS16 were correlated with the proposed variables significantly the expected directions. Whereas, reliabilities of each subscale were above 0.6 and the reliability for the overall FRS16 scale was satisfactory.
Next, we aimed to cross-validate FRS16 with a Chinese sample which was abbreviated as FRS16_C. We first examined the construct validity of the three-factor structure in a Chinese sample with CFA, and conducted content validity tests and examination of the associations between FRS16_C and important outcomes. Additionally, the correlation patterns of the original and two other Chinese versions of FRAS and FRS16_C were examined to evaluate whether they are comparable instruments. Furthermore, test-retest reliability was also examined in a 2-week follow-up. Lastly, measurement invariance analysis was followed to obtain a stronger support that FRS16 operates similarly for both the US and Chinese samples, and participants from the two regions share parallel understandings of the construct.
Procedures were similar to that of Study 1, we recruited participants from mainland China via an online survey distribution platform Credamo (www.credamo.com) which is a professional research data platform with survey distribution and data modeling services. Datasets collected from this platform has been published in well-respected international journals such as Psychological Science and Journal of Consumer Research1. Credamo has over 2 million registered users cover all provincial regions in China which provides researchers a wider reach to participants in different regions within China. Upon completion, participants received 16 CNY in their Credamo account which can be transferred to his or her online payment platform WeChat Pay.
After excluding those who were not residing in mainland China, the final sample consisted of 1,135 participants for the CFA test. On average, participants aged 30.01 (SD = 5.99, range = 18–59) with slightly higher proportion of female (57.4%). The majority of them were married (68.8%), highly educated (85.6% with a bachelor's degree or above), and with a high annual household income within mainland China2 (61%) (see Table 5).
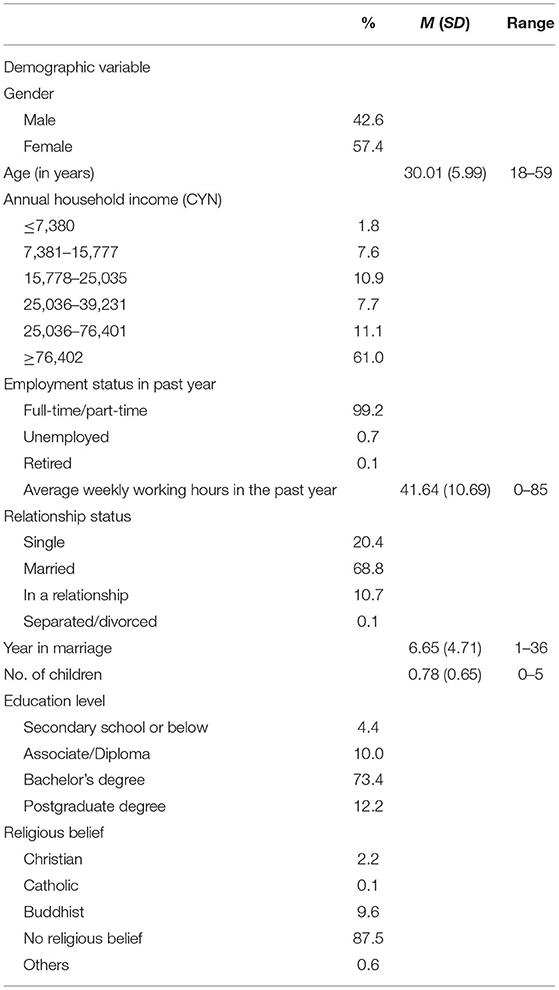
Table 5. Descriptive statistics of demographics (Chinese sample).
This study included available Chinese translations of measures in Study 1. A list of validation studies on these Chinese versions of the measurement scales is available from the corresponding author upon request. In particular, the FRS16_C used the Chinese translation of FRAS by Chiu et al. (22) and refined some wordings to fit the context of mainland China.
All participants completed the full set of questionnaires, including the FRS16_C. Among them, 213 participants filled in the full version of FRAS to test the associations between FRS16_C with the original and two Chinese versions of FRAS and compare their correlations with different demographic and convergent variables as composite scores. Another subsample of 63 participants filled in the same set of measurements 2 weeks later for the temporal consistency test of FRS16_C.
All descriptive statistics for demographic and main variables are summarized in Tables 5, 6, respectively.
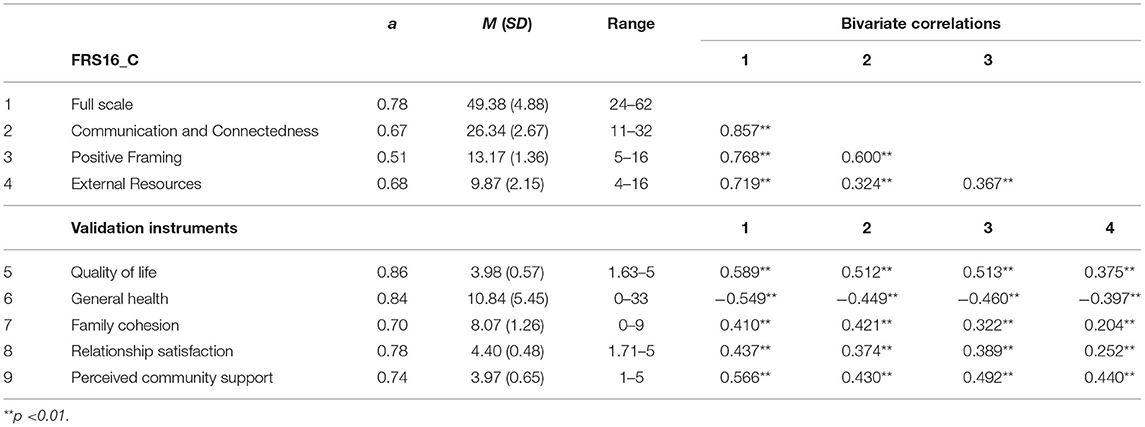
Table 6. Descriptive statistics of main variables (Chinese sample).
Similar to Study 1, CFA was estimated with the maximum likelihood with the aid of Mplus 8.3. CFA results showed that the three-factor model demonstrated excellent model fit: χ2 (99) = 287.84, p <0.001; SRMR = 0.033; RMSEA = 0.041, CI = [0.036, 0.047]; TLI = 0.94; CFI = 0.95 (See Figure 2 for standardized factor loadings). The same set of alternative models were examined, as shown in Table 7, the fit indices of the one- and two-factor models were poor, whereas the five- and six-factor models showed parallel model fits to that of the proposed three-factor model. Considering the three-factor model has both more interpretable and parsimonious factor structure and five- and six-factor models did not show significant improvements in model fit, a holistic evaluation suggests a three-factor model should be adopted.
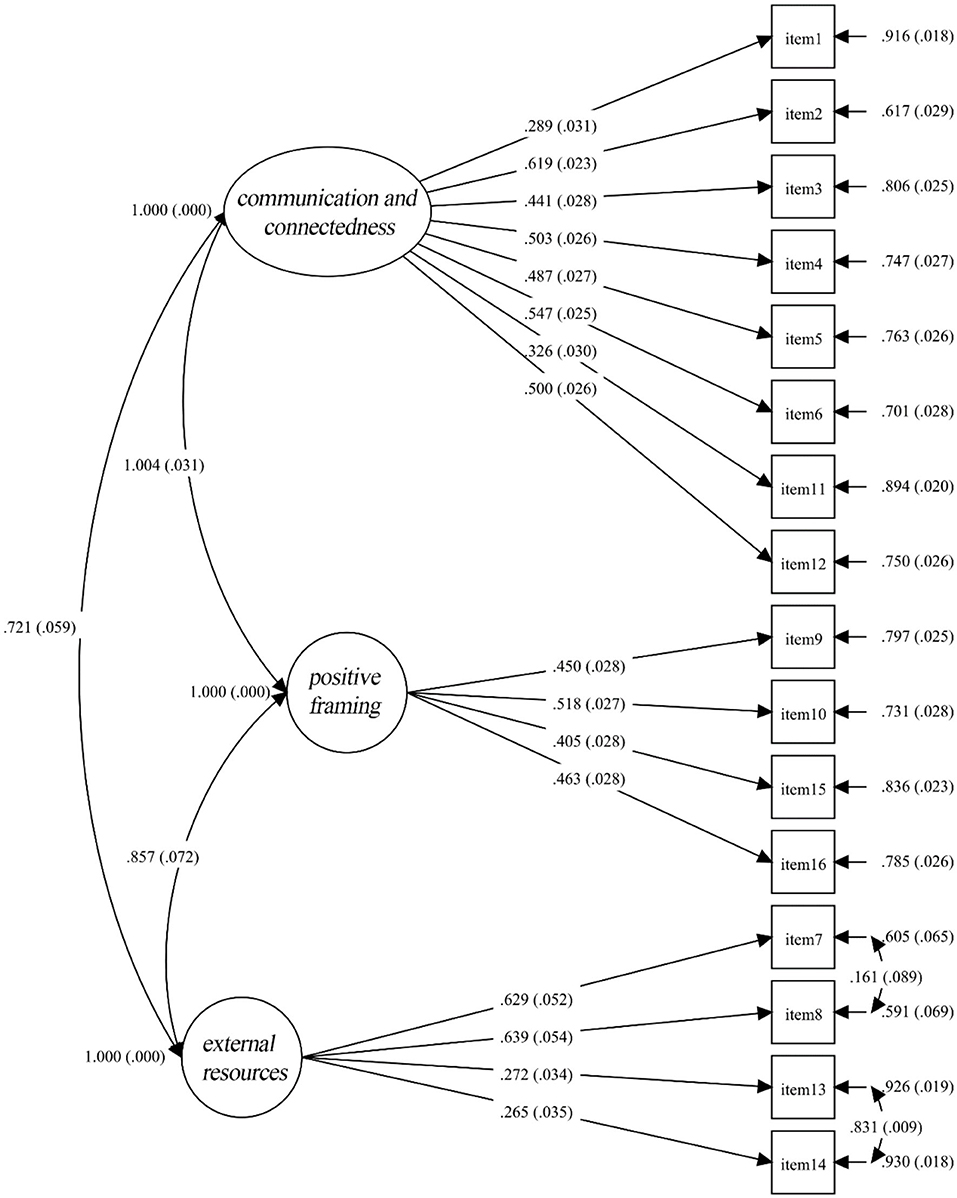
Figure 2. Factor structure and standardized factor loadings of FRS16_C.

Table 7. Model fit indices of models with different number of factors.
As shown in Table 8, all items were significantly correlated to both its subscale and the full scale with a small to moderate strength (rs ≥ 0.31), demonstrating acceptable content validity.
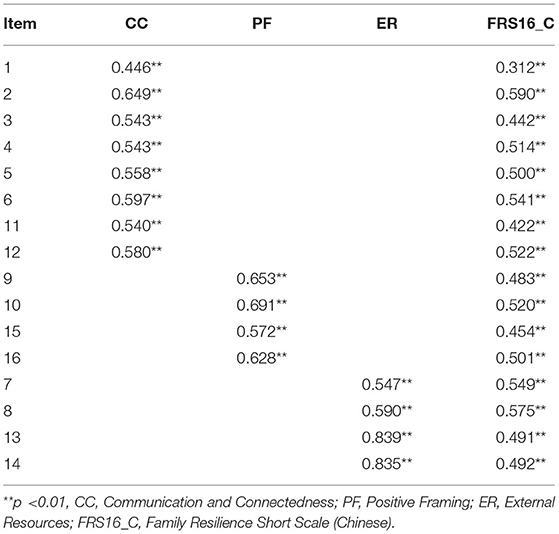
Table 8. Item-to-scale and item-to-subscale correlations.
As shown in Table 6, the full and subscales of FRS16_C were all significantly associated with proposed outcome variables in the expected directions.
To our best knowledge, there are two Chinese versions of FRAS with three- (23) and five-factor models (24) which were validated with family caregivers and university students samples, respectively. Therefore, we would like to compare the performance of FRS16_C in comparison with other existing FRASs by examining the correlation coefficients of FRS16_C with the original FRAS, three-factor FRAS, and five-factor FRAS and compare their correlational patterns with demographic and related variables as a composite. As shown in Table 9, FRS16_C performed similarly to different versions of FRAS. Importantly, we observed that the shortened FRS16_C retained at least 70% of the predictive value of the 54-item scale. This pattern indicated that, given its brevity, the 16-item scale developed in the present study can stand in for the full 54-item scale in terms of predictive value.
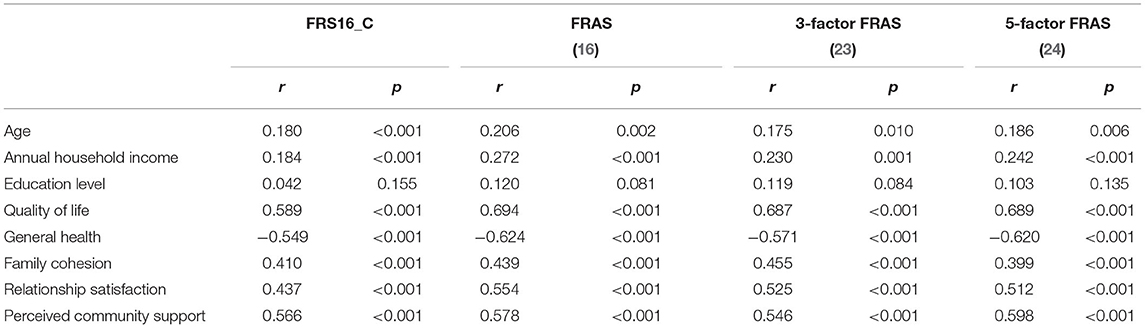
Table 9. Correlations of FRASs and FRS16_C with demographic and outcome variables.
The Cronbach's alphas of Communication and Connectedness, Positive Framing, and External Resources were 0.67, 0.51, and 0.68, respectively. The reliability of overall FRS16_C was 0.78 and the test-retest reliability of FRS16_C in 2-weeks interval was acceptable (ICC = 0.87).
Since the group-level CFA test results were found satisfactory with both the US and Chinese samples separately, configural invariance was established. Thus, the three-factor structure is valid for both groups (47). A multi-group three-factor model was still tested with no parameter constraints, as shown in Table 10, the fit indices of this baseline model were satisfactory, which showed converging support for configural variance. Next, we tried to establish metric variance by running a more stringent multi-group model with the factor loadings coefficients constrained to be equal across groups on top of the baseline model. The multiple-group model showed satisfactory fit (see Table 10), both ΔCFI and ΔRMSEA were below the recommended cut-offs [ΔCFI ≤ 0.010 and ΔRMSEA ≤ 0.015; (48)], suggesting that respondents attributed the same meaning to the latent factor (47).

Table 10. Evaluations of measurement invariance.
To provide a measure of family resilience for contexts in which assessment time is relatively limited, we abbreviated the Family Resilience Assessment Scale [FRAS (16)] to a 16-item version, the FRS16. The proposed 3-factor model was supported across the US and Chinese samples. The 3-factor model consists of easily interpretable factors that cover the most essential components of family resilience, namely, Family Communication and Connectedness, Positive Framing, and External Support (4, 28, 49, 50). These three factors also cover all of the subprocesses in Walsh (28)'s theory and correspond to the different family adaptive subsystems (maintenance system, meaning system, and ecosystem) discussed in Henry et al. (34). Family communication and connectedness signifies the way through which the family members organize and communicate in response to external stressors. It captures the core elements of the maintenance system. Meanwhile, the positive framing factor involves the family world view and the ability to maintain positive strength-based outlook. This factor represents the adaptability of the family meaning system. Finally, the external resources capture positive features and resources in the external ecosystem in which crises and opportunities occur.
We also noticed that the factor loadings of the items related to family spirituality (e.g., item 13: we attend church/synagogue/mosque services) were lower (<0.30) than the two other items about social support (>0.60) in the Chinese sample. Comparatively, the factor loadings of these four items were more homogenous in the US sample. Li et al. (24) suggested that religious support is less significant in Chinese societies. In Chinese culture, the practice of ancestor worship is considered as the most common form of spiritual activity. In a study conducted in Singapore, Chinese participants identified ancestors as their spiritual sources (51), yet prominence and the format of these spiritual activities are diverse even within the Chinese culture. This might explain the more heterogeneous factor loadings of this subscale in the Chinese sample. Since the factor loadings were still statistically significant, and the item-to-subscale and item-to-total correlations remain high, we decided to keep these two items in the External Resources subscale. Nevertheless, future research should further explore the value of religious and spiritual activities in Chinese family resilience.
To assess the psychometric equivalence of the FRS16 across the US and Chinese samples, measurement invariance analyses were conducted. The configural invariance suggested that the basic organization (the 3-factor structure) is supported in both cultures while the metric invariance suggested that the contribution of each item to the latent factor to a similar degree across the two samples. These findings suggested that the proposed FRS16 includes the most essential items that measure the common, fundamental processes of family resilience across cultures. Thus, it is a viable tool for assessing family resilience in cross-cultural studies especially when assessment time is limited. Nevertheless, if cultural sensitivity is the major concern of the research, researchers can consider other longer versions which were developed specifically for a single culture [Chinese: (24)]. We also examined the performance of the FRS16 in comparison with three other versions of FRAS including the full 54-item version. The part-whole correlation between the FRS16 with the original FRAS reaches 0.87. We also observed strong correlations between the FRS16 with other adapted versions of the scale (rs >0.77). Additionally, the FRS16 shares comparable associations with validation instruments with FRAS in three different lengths.
In both samples, the FRS16 demonstrated good internal consistency for the total scale (αs > 0.80). The reliabilities of all subscales were satisfactory except Positive Framing in the Chinese sample. Nevertheless, despite the relatively low Cronbach's α (0.51), the item-to-subscale, and item-to-total correlations were both high and significant. The four items in the Positive Framing subscale were also strongly loaded on the expected latent factor. Given that this subscale consists of only four items that were related to two different types of positive framing—showing high efficacy in problem solving (e.g., Item 10: We can survive if another problem comes up) and normalizing stressors and crises (e.g., Item 15: We accept stressful events as a part of life), the relatively lower alpha was considered acceptable.
The present studies indicated that the FRS16 and its three subscales were all significantly associated with proposed outcome variables (i.e., quality of life, general health, family cohesion, relationship satisfaction, perceived community support) in the expected directions for both the US and Chinese samples. It is noted that the External Resources subscale showed relatively lower correlations with relationship satisfaction and family cohesion in both samples. It might suggest that the ability to utilize external and internal resources to cope with crisis were comparatively less crucial to the cohesion and relationship satisfaction of a family compared to Communication and Connectedness and Positive Framing. However, it does not in any way imply that External Resources was a less important component of family resilience, as it demonstrated correlation with other validation instruments in similar sizes as other components, such as its associations with general health and perceived community support.
The present study has a few limitations. First, the study was conducted on online crowdsourcing samples. Although crowdsourcing data enjoys benefits such as the more diversified demographic background of participants (52), it still cannot represent the general population. This concern has also been reflected in our US sample with higher proportion of male, and in Chinese sample with majority coming from high-annual-household-income family. Efforts should be made in validating the FRS16 with more representative and diverse samples. Additionally, some researchers argued that crowdsourcing data has the problem of cross-contamination and selective dropouts, but these issues are more relevant to experimental studies (53). Afterall, precaution is still needed in interpreting the results obtained from these crowdsourcing platforms. Second, the present study did not focus on populations that are facing acute or chronic stressors and traumatic events (e.g., caregiver of a family member who has chronic illness, recent death of a family member, economic hardship) or populations with different family characteristics (e.g., the number of family members cohabiting). The importance and meaning of family resilience could be different for people who are encountering crises or with different family characteristics. Future research could test the reliability and validity of the FRS16 in diverse populations. Third, we used quality of life, general health, relationship satisfaction, family cohesion, and perceived community support for validating the FRS16. These variables might not fully reflect the three proposed processes in family resilience. Future research might include more theoretically relevant outcome measures such as family and community support [Social Support Index; (54)]. Forth, given that the cross-sectional nature of current studies, the directions of associations between FRS16 and validation instruments remain unknown, future studies are needed to provide support for predictive validations with a longitudinal or experimental design. Fifth, as the measurements were self-reported, responses might be contaminated by social desirability. However, respondents' anonymity is underscored in the beginning of the survey to minimize the influence of social desirability. Lastly, only individual family member's perception of the family dynamics and resilience was captured in this study. Other family members' perceptions may vary. In other words, it might not reflect family resilience comprehensively, as it fails to capture this process positioning families as a unit. Nevertheless, validating a short version of family resilience scale is a starting point to “study resilience in the family as a functional unity” (55) by making the measurement of each family members' perceptions less time-consuming.
Overall, the present study contributes to the literature by developing a short form of family resilience scale and cross-validated it in Western and Eastern cultures. The short version captures the essential items and the most fundamental processes underlying family resilience. Given its brevity, the FRS16 possesses acceptable psychometric properties in both cultures. It is suitable for cross-cultural study and research in which the testing time is limited such as therapy outcome assessment, intensive longitudinal research, and telephone survey.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Human Research Ethics Committee of the Hong Kong Shue Yan University. The patients/participants provided their written informed consent to participate in this study.
TC contributed to study conceptualization, survey design, leading statistical analyses and interpretation of results, and writing the original text. CT contributed to study conceptualization, survey design, results interpretation, administrating and supervising the project, providing comments to revise the manuscript, and refine the data analysis. TS facilitated the data analysis and contributed to reviewing and editing the manuscript. HK provided study measures and contributed to the survey development and refinement. All authors contributed to the article and approved the submitted version.
This study was funded by a matching research grant awarded to the Wan Chow Yuk Fan Centre for Interdisciplinary Evidence-based Practice & Research at the Hong Kong Shue Yan University UL/RS/2021/001.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.845803/full#supplementary-material
1. ^See https://help.credamo.com/web/#/4?page_id=118 for a list of publications in 2020 using Credamo to collect data.
2. ^The categorization of annual household income in 2019 set by National Bureau of Statistics of China was as follow: the lowest 20% cutoff was 7380.4 CNY, following by 15777.0 CNY (mid low), 25034.7 CNY (mid), 39230.5 CNY (upper mid) and 76400.7 CNY (high). See http://www.stats.gov.cn/tjsj/ndsj/2021/indexeh.ht.
1. Ahlert IA, Greeff AP. Resilience factors associated with adaptation in families with deaf and hard of hearing children. Am Ann Deaf. (2012) 157:391–404. doi: 10.1353/aad.2012.1629
2. McCubbin MA, McCubbin HI. Families coping with illness: the resiliency model of family stress, adjustment and adaptation. In: Danielson CB, Hamel-Bissell B, Winstead-Fry P, editors. Families, Health and Illness: Perspectives on Coping and Intervention. St. Louis, MO: Mosby (1993). pp. 21–63.
3. Walsh F. A Family resilience framework: Innovative practice application. Fam Relat. (2002) 51:130–7. doi: 10.1111/j.1741-3729.2002.00130.x
4. Patterson JM. Integrating family resilience and family stress theory. J Marr Fam. (2002) 64:349–60. doi: 10.1111/j.1741-3737.2002.00349.x
5. McCubbin HI, Patterson JM. The family stress process: the Double ABCX Model of adjustment and adaptation. Marr Fam Rev. (1983) 6:7–37. doi: 10.1300/J002v06n01_02
6. Hamall KM, Heard TR, Inder KJ, McGill KM, Kay-Lambkin F. The Child Illness and Resilience Program (CHiRP): a study protocol of a stepped care intervention to improve the resilience and wellbeing of families living with childhood chronic illness. BMC Psychol. (2014) 2:5. doi: 10.1186/2050-7283-2-5
7. Hackbarth M, Pavkov T, Wetchler J, Flannery M. Natural disasters: an assessment of family resiliency following Hurricane Katrina. J Marital Fam Ther. (2012) 38:340–51. doi: 10.1111/j.1752-0606.2011.00227.x
8. Walsh F. Loss and resilience in the time of COVID-19: meaning making, hope, and transcendence. Fam Process. (2020) 59:898–911. doi: 10.1111/famp.12588
9. Shin SH, Choi H, Kim MJ, Kim YH. Comparing adolescents' adjustment and family resilience in divorced families depending on the types of primary caregiver. J Clin Nurs. (2010) 19:1695–706. doi: 10.1111/j.1365-2702.2009.03081.x
10. Hooghe A, Neimeyer RA. Family resilience in the wake of loss: a meaning-oriented contribution. In: Becvar DS, editor. Handbook of Family Resilience. New York, NY: Springer (1993). pp. 269–84. doi: 10.1007/978-1-4614-3917-2_16
11. Masten AS, Monn AR. Child and family resilience: a call for integrated science, practice, professional training. Fam Relat Interdisc J Appl Fam Stud. (2015) 64:5–21. doi: 10.1111/fare.12103
12. Uddin J, Alharbi N, Uddin H, Hossain MB, Hatipoglu SS, Long DL, et al. Parenting stress and family resilience affect the association of adverse childhood experiences with children's mental health and attention-deficit/hyperactivity disorder. J Affect Disord. (2020) 272:104–9. doi: 10.1016/j.jad.2020.03.132
13. Feinberg ME, Boring J, Le Y, Hostetler ML, Karre J, Irvin J, et al. Supporting military family resilience at the transition to parenthood: a randomized pilot trial of an online version of family foundations. Fam Relat. (2020) 69:109–24. doi: 10.1111/fare.12415
14. Lim H, Han K. Effects of the family resilience enhancement program for families of patients with chronic schizophrenia. J Korean Acad Nurs. (2013) 43:133–42. doi: 10.4040/jkan.2013.43.1.133
15. Saltzman WR. The FOCUS family resilience program: an innovative family intervention for trauma and loss. Fam Process. (2016) 55:647–59. doi: 10.1111/famp.12250
16. Sixbey MT,. Development of the Family Resilience Assessment Scale to identify family resilience constructs [Doctorate dissertation, University of Florida]. The University of Florida Digital Collections. Available online at: http://ufdc.ufl.edu/UFE0012882/00001 (2005).
17. Chan ACY, Piehler TF, Ho GWK. Resilience and mental health during the COVID-19 pandemic: findings from Minnesota and Hong Kong. J Affect Disord. (2021) 295:771–80. doi: 10.1016/j.jad.2021.08.144
18. Dong C, Xu R, Xu L. Relationship of childhood trauma, psychological resilience, and family resilience among undergraduate nursing students: a cross-sectional study. Perspect Psychiatr Care. (2021) 57:852–9. doi: 10.1111/ppc.12626
19. Finklestein M, Pagorek-Eshel S, Laufer A. Adolescents' individual resilience and its association with security threats, anxiety and family resilience. J Fam Stud. (2020) 1–17. doi: 10.1080/13229400.2020.1778504 [Epub ahead of print].
20. Chen JJ, Wang QL, Li HP, Zhang T, Zhang SS, Zhou MK. Family resilience, perceived social support, and individual resilience in cancer couples: analysis using the actor-partner interdependence mediation model. Eur J Oncol Nurs. (2021) 52:101932. doi: 10.1016/j.ejon.2021.101932
21. Chew J, Haase AM, Carpenter J. Individual and family factors associated with self-esteem in young people with epilepsy: a multiple mediation analysis. Epilepsy Behav. (2017) 66:19–26. doi: 10.1016/j.yebeh.2016.09.039
22. Chiu SJ, Chou YT, Chen PT, Chien LY. Psychometric properties of the Mandarin version of the family resilience assessment scale. J Child Fam Stud. (2019) 28:354–69. doi: 10.1007/s10826-018-1292-0
23. Chu AMY, Tsang JTY, Tiwari A, Yuk H, So MKP. Measuring family resilience of Chinese family caregivers: psychometric evaluation of the Family Resilience Assessment Scale. Fam Relat. (2021) 70:1297–302. doi: 10.1111/fare.12601
24. Li Y, Zhao Y, Zhang J, Lou F, Cao F. Psychometric properties of the shortened Chinese version of the Family Resilience Assessment Scale. J Child Fam Stud. (2016) 25:2710–17. doi: 10.1007/s10826-016-0432-7
25. Kaya M, Arici N. Turkish version of shortened Family Resiliency Scale (FRAS): the study of validity and reliability. Procedia Soc Behav Sci. (2012) 55:512–20. doi: 10.1016/j.sbspro.2012.09.531
26. Nadrowska N, Błazek M, Lewandowska-Walter A. Polish adaptation of the Family Resilience Assessment Scale (FRAS). Commun Ment Health J. (2021) 57:153–60. doi: 10.1007/s10597-020-00626-3
28. Walsh F. Family resilience: a framework for clinical practice. Fam Process. (2003) 42:1–18. doi: 10.1111/j.1545-5300.2003.00001.x
29. Benzies K, Mychasiuk R. Fostering family resiliency: a review of the key protective factors. Child Fam Soc Work. (2009) 14:103–14. doi: 10.1111/j.1365-2206.2008.00586.x
30. Black K, Lobo M. A conceptual review of family resilience factors. J Fam Nurs. (2008) 14:33–55. doi: 10.1177/1074840707312237
31. VanderWeele TJ. Love of neighbor during a pandemic: Navigating the competing goods of religious gatherings and physical health. Journal of Religion and Health. (2020) 59:2196–202. http://dx.doi.org/10.1007/s10943-020-01031-6
32. Meyer BD, Sullivan JX. The effects of welfare and tax reform: the material well-being of single mothers in the 1980s and 1990s. J Public Econ. (2004) 88:1387–420. doi: 10.1016/S0047-2727(02)00219-0
33. Stone HW, Cross DR, Purvis KB, Young MJ. A study of church nembers during times of crisis. Pastoral Psychol. (2004) 52:405–21. doi: 10.1023/B:PASP.0000020688.71454.3d
34. Henry CS, Sheffield Morris A, Harrist AW. Family resilience: moving into the third wave. Fam Relat. (2015) 64:22–43. doi: 10.1111/fare.12106
35. Izumi M, Gullón-Rivera AL. Family resilience among sojourning Japanese mothers: links to marital satisfaction and children's behavioral adjustment. Fam Consumer Sci Res J. (2018) 46:282–96. doi: 10.1111/fcsr.12247
36. Lester P, Stein JA, Saltzman W, Woodward K, MacDermid SW, Milburn N, et al. Psychological health of military children: longitudinal evaluation of a family-centered prevention program to enhance family resilience. Mil Med. (2013) 178:838–45. doi: 10.7205/MILMED-D-12-00502
37. Huang CY, Mu PF, Jou ST. Relationships between uncertainty, family resilience and quality of life in mothers of children with cancer. Int J Evid Based Healthc. (2011) 9:289. doi: 10.1097/01258363-201109000-00022
38. Garrard ED, Fennell KM, Wilson C. ‘We're completely back to normal, but I'd say it's a new normal': a qualitative exploration of adaptive functioning in rural families following a parental cancer diagnosis. Support Care Cancer. (2017) 25:3561–8. doi: 10.1007/s00520-017-3785-6
39. Mason W, Suri S. Conducting behavioral research on Amazon's Mechanical Turk. Behav Res Methods. (2012) 44:1–23. doi: 10.3758/s13428-011-0124-6
40. Berinsky AJ, Huber GA, Lenz GS. Evaluating online labor markets for experimental research: Amazon.com's Mechanical Turk. Political Anal. (2012) 20:351–68. doi: 10.1093/pan/mpr057
41. Schmidt S, Mühlan H, Power M. The EUROHIS-QOL 8-item index: psychometric results of a cross-cultural field study. Eur J Public Health. (2006) 16:420–8. doi: 10.1093/eurpub/cki155
42. Makowska Z, Merecz D, Moscicka A, Kolasa W. The validity of general health questionnaires, GHQ-12 and GHQ-28, in mental health studies of working people. Int J Occup Med Environ Health. (2002) 15:353–62.
43. Hendrick SS. A generic measure of relationship satisfaction. J Marr Fam. (1988) 50:93–8. doi: 10.2307/352430
44. Moos RR, Moss BS. Family Environment Scale Manual. Palo Alto, CA: Consulting Psychologist Press (1981).
45. Peterson NA, Speer PW, McMillan DW. Validation of A brief sense of community scale: confirmation of the principal theory of sense of community. J Commun Psychol. (2008) 36:61–73. doi: 10.1002/jcop.20217
46. Muthén LK, Muthén BO. Mplus User's Guide. 8th ed. Los Angeles, CA: Muthén and Muthén (1998–2017).
47. van de Schoot R, Lugtig P, Hox J. A checklist for testing measurement invariance. Eur J Dev Psychol. (2012) 9:486–92. doi: 10.1080/17405629.2012.686740
48. Chen FF. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct Equat Model Multidisc J. (2007) 14:464–504. doi: 10.1080/10705510701301834
49. Masten AS, Coatsworth JD. The development of competence in favorable and unfavorable environments: lessons from research on successful children. Am Psychol. (1998) 53:205–20. doi: 10.1037/0003-066X.53.2.205
50. Whitchurch GG, Constantine LL. Systems theory. In: Boss PG, Doherty WJ, LaRossa R, Schumm WR, Steinmetz KS, editors. Sourcebook of Family Theories and Methods: A Contextual Approach. New York, NY: Plenum Press (1993). pp. 325–55.
51. Chang W, Neo A, Fung D. In search of family resilience. Psychology. (2015) 6:1594–607. doi: 10.4236/psych.2015.613157
52. Hauser DJ, Schwarz N. Attentive Turkers: MTurk participants perform better on online attention checks than do subject pool participants. Behav Res Methods. (2016) 48:400–7. doi: 10.3758/s13428-015-0578-z
53. Zhou H, Fishbach A. The pitfall of experimenting on the web: how unattended selective attrition leads to surprising (yet false) research conclusions. J Pers Soc Psychol. (2016) 111:493–504. doi: 10.1037/pspa0000056
54. McCubbin HI, Thompson AI, McCubbin MA editors. Family Assessment: Resiliency, Coping, and Adaptation: Inventories for Research and Practice. 1st ed. Madison, MI: University of Wisconsin Publishers (1996).
Keywords: family resilience, short scale, Chinese, US, measurement validation
Citation: Chow TS, Tang CSK, Siu TSU and Kwok HSH (2022) Family Resilience Scale Short Form (FRS16): Validation in the US and Chinese Samples. Front. Psychiatry 13:845803. doi: 10.3389/fpsyt.2022.845803
Received: 30 December 2021; Accepted: 23 March 2022;
Published: 13 May 2022.
Edited by:
Kangguang Lin, Guangzhou Medical University, ChinaReviewed by:
Intan Hashimah Mohd Hashim, Universiti Sains Malaysia (USM), MalaysiaCopyright © 2022 Chow, Tang, Siu and Kwok. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tak Sang Chow, dHNjaG93QGhrc3l1LmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.