
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 02 March 2022
Sec. Public Mental Health
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.838239
 Juan D. Molina1,2,3,4*
Juan D. Molina1,2,3,4* Irene Rodrigo Holgado5
Irene Rodrigo Holgado5 Alba Juanes González6
Alba Juanes González6 Carolina Elisa Combarro Ripoll6David Lora Pablos3,7,8
Carolina Elisa Combarro Ripoll6David Lora Pablos3,7,8 Gabriel Rubio2,3,9,10
Gabriel Rubio2,3,9,10 Jordi Alonso11,12Francisco P. J. Rivas-Clemente13
Jordi Alonso11,12Francisco P. J. Rivas-Clemente13Studies specifically designed to determine the profile of psychiatric symptoms among COVID-19 patients are limited and based on case series, self-report questionnaires, and surveys. The objective of the study was to identify and classify the neuropsychological symptoms of hospitalized COVID-19 patients during the first wave of the pandemic in one of the most important front-line tertiary hospitals from Spain, and to analyze its correlation with diagnosed mental disorders, as well as to explore potential risk factors associated with mental health problems. This observational, cohort study involved data from COVID-19 patients at the University Hospital 12 de Octubre (Madrid, Spain) from February to May 2020. First, patients underwent a semistructured phone interview (screening phase), based on the Mini International Neuropsychiatric Interview (MINI). Then the confirmation of the diagnosis (confirmation phase) was performed in patients who reported a mental disorder development or worsening. A factorial analysis was performed to identify groups of symptoms. A tetrachoric matrix was created, and factorial analysis, by a principal component analysis, was employed upon it. Factors showing values >1.0 were selected, and a varimax rotation was applied to these factors. Symptoms most frequently identified in patients were anosmia/ageusia (54.6%), cognitive complaints (50.3%), worry/nervousness (43.8%), slowing down (36.2%), and sadness (35.4%). Four factors were identified after the screening phase. The first (“anxiety/depression”) and second (“executive dysfunction”) factors explained 45.4 and 11.5% of the variance, respectively. Women, age between 50 and 60 years, duration in the hospital (more than 13 days), and psychiatric history showed significant higher levels (number of symptoms) in the factors. This study reports the factor structure of the psychiatric symptoms developed by patients with a confirmed diagnosis of SARS-CoV2 during the first wave of the COVID-19. Three item domains (anxiety, depression, and posttraumatic stress disorder symptoms) were loaded together on one factor, whereas sleep disturbance stood up as a separate factor. Interestingly, the item anosmia/ageusia was not captured by any factor. In conclusion, an increase in neuropsychiatric morbidity is expected in the upcoming months and years. Therefore, screening for early symptoms is the first step to prevent mental health problems associated with this pandemic.
The pandemic, caused by the severe acute respiratory syndrome virus (SARS)-CoV-2, has triggered a deep transformation of societies, with more than 240 million individuals infected worldwide (1) and 3.5 million in Spain (2). Researchers have turned their efforts in the prevention, etiopathology, risk factors, clinical symptoms, treatment, and prognosis of the coronavirus disease 2019 (COVID-19), and the scientific production has increased accordingly in just 1 year (3). Numerous studies have focused on identifying short-term physical complications derived from the disease, such as thromboembolisms or pulmonary fibrosis, for instance (4). Nevertheless, less research has been made about the psychological impact of the pandemic on patients (survivors).
In Spain, 15% of the patients have required hospitalization due to severe COVID-19 (from March 1 to July 31, 2020) (5), and about 10% of them have been admitted at the intensive care unit (ICU) (6). An early study reported that 36.4% of the hospitalized patients experienced neurologic symptoms, involving the central nervous system (especially dizziness and headache), peripheral nervous system (taste or smell impairment), and skeletal muscle injury (7). Moreover, the respiratory distress syndrome, invasive procedures, physical contentions, or the inappropriate management of sedation have been demonstrated to increase the risk of psychologic consequences and, especially, posttraumatic stress disorder (PTSD) in survivors of critical diseases (8), such as COVID-19. Diverse studies have reported additional neuropsychiatric symptoms and complications associated with the disease (including delirium, encephalopathy, olfactory disturbances, acute behavioral changes, headache, and cerebrovascular accidents) (9–11). Indeed, neuropsychiatric symptoms had also been reported after the large viral epidemics in the 19 and 20th centuries (12, 13). For example, 1 year after the SARS pandemic, the prevalence of PTSD in survivors was up to 38%. The prevalence of traumatic memories, anxiety, depression, and PTSD also raised after other coronavirus pandemics (SARS or the Middle East respiratory syndrome-CoV) (9, 14, 15). Moreover, the psychological consequences of patients surviving coronavirus epidemics are stronger than the physical ones (16).
Studies specifically designed to determine the profile of psychiatric symptoms among COVID-19 patients are limited and based on case series, self-report questionnaires, and surveys.
The objective of the present study was to identify and classify the neuropsychological symptoms of hospitalized COVID-19 patients during the first wave of the pandemic, by using screening and diagnosis confirmation, in one of the most important front-line tertiary hospitals in Spain, and to analyze its correlation with diagnosed mental disorders, as well as to explore potential risk factors associated with mental health problems.
This observational, retrospective cohort study involved data from COVID-19 patients admitted at the University Hospital 12 de Octubre (Madrid, Spain) from February to May 2020 with a probable or confirmed diagnosis of SARS-CoV2 infection (by polymerase chain reaction or clinical suspicion). Patients who were not finally diagnosed of the infection during the hospitalization were excluded from the study. After discharge, all eligible patients were invited to participate in the study, and a screening phone interview was administered. Participants who reported the development or worsening of a mental disorder after the hospitalization in the screening phase were offered consultation (in-person) in the hospital to confirm the diagnosis and manage the appropriate approach. This confirmation phase (September 2020–March 2021) was developed by the same clinician who did the screening phase and was conducted through the usual diagnostic procedures in the mental health service, including a complete diagnostic interview based on DSM-5 criteria. Patients who rejected to participate or those with incomplete or unreliable information (language barrier and instrumental difficulties mostly) were excluded from the analysis.
After hospital discharge, two psychiatrics and one psychologist from the hospital evaluated the psychopathological status of the patients (screening phase, July–October 2020). The mental assessment of patients (screening) consisted of a semistructured phone interview, based on the Mini International Neuropsychiatric Interview (MINI) (17), and in persistent symptoms published in the available scientific literature at the time. The survey included a series of questions about the symptoms of different types of mental health problems: depression, panic attacks, generalized anxiety disorder, obsessive–compulsive disorder, PTSD, suicidal risk, substance abuse disorder (SAD) and cognitive complaints, patient sleep or feeding behaviors, and other symptoms, such as pain or anosmia/ageusia. These items were generally named as “symptoms” along the text. Answers included yes or no, and specify, when required. The original (Spanish) and translated (English) versions of the survey provided to patients are shown in Supplementary Table 1.
Demographic, clinical, and survey characteristics of patients and HCWs are expressed with the mean and standard deviation (SD), or with absolute and relative frequencies, when appropriate. A factorial analysis was carried out to group different variables and symptoms from the patient's survey. Given their binary categorical nature, a tetrachoric matrix was created, and factor analysis, by a principal component analysis (PCA), was employed upon it. Factors showing eigenvalues >1.0 were selected. Subsequently, a varimax rotation was applied to these factors in order to facilitate the conceptualization. Variables weighted higher than 0.5 in the axis were considered important for the factor. Constructed factors were related with demographic (gender and age), clinical (psychiatric history), and hospital stay (duration in the hospital and time until the survey). Only associations between the factors of the PCA and the risk factor of the patient showing p < 0.01, using a t-test or analysis of variance (ANOVA), were considered statistically significant. Multiple comparisons were adjusted by the Bonferroni correction. Relevant factors with more than two variables in the factorial analysis were used to determine the risk factors in patients.
Of the 2,486 eligible patients who were initially identified, 1,694 (68.3%) were evaluable for the analysis. Causes of exclusion were not able to be contacted (n = 545), not willing to be interviewed (n = 140), not willing to collaborate in the study (n = 7), aged below 18 (n = 24), and not finally diagnosed of COVID-19 during hospitalization (n = 76). Table 1 shows the characteristics of the participating patients (males 52.3% and females 47.7%, with a mean age of 59.9 years).
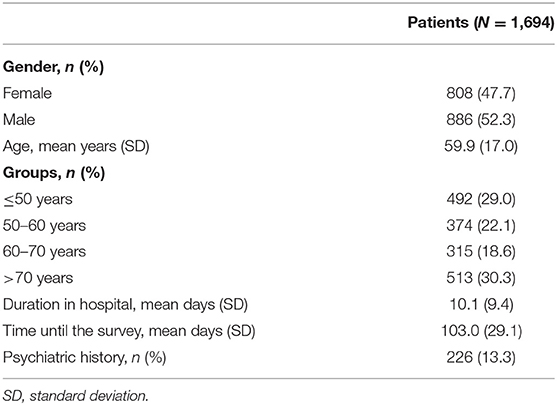
Table 1. Sociodemographic characteristics of the patients.
Table 2 presents the symptoms most frequently identified in patients in the screening phase. These were anosmia/ageusia (54.6% of them), cognitive complaints (50.3%), worry/nervousness (43.8%), slowing down (36.2%), and depression (35.4%). A total of 175 patients (10.3%) reported none of the symptoms.
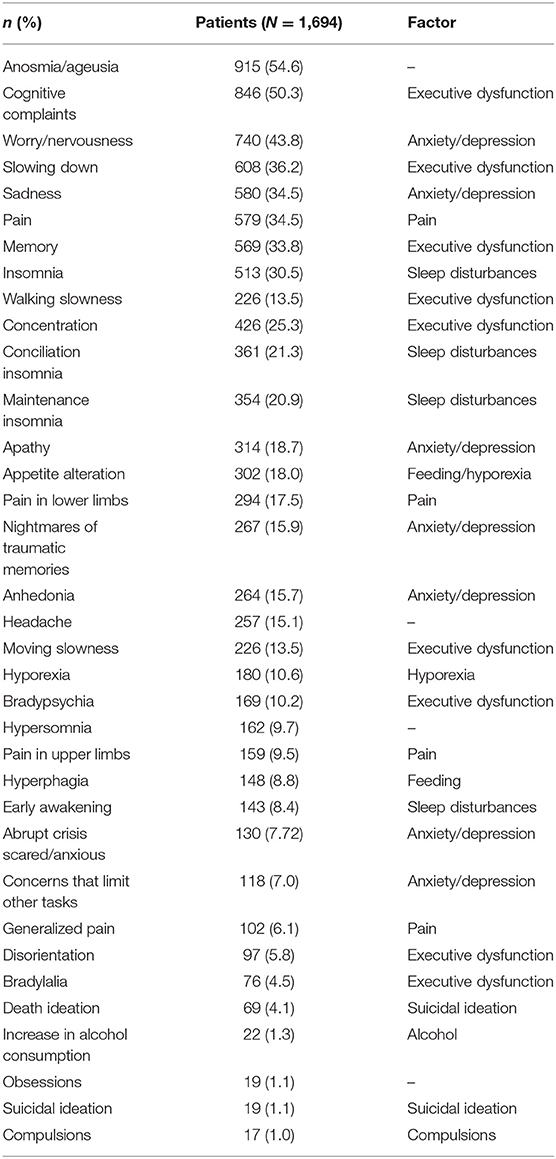
Table 2. Frequency of symptoms identified in patients and aggrupation into factors.
The factorial analysis identified nine factors, of which the first seven factors explained the 87.8% of the variance (Table 3). The first factor was named as “anxiety/depression” and explained 45.4% of the variance. In this factor, items with a weight >0.50 were depression symptoms (anhedonia, sadness, apathy), generalized anxiety symptoms (worry/nervousness, concerns that limit other tasks), nightmares of traumatic memories (PTSD symptom), abrupt crisis scared/anxious, and death ideation. The second factor was conceptualized as “executive dysfunction” and explained 11.5% of the variance. It was composed of the following items (with a weight >0.50): cognitive complaints, slowing down, memory, concentration, disorientation, bradypsychia, and walking slowness. Hypersomnia was the next item with an eigenvalue under 0.5 included in this factor. The third factor was labeled as “pain” and explained 8.2% of the variance. It was composed of the variables generalized pain, pain in the upper limbs, pain in the lower limbs, and pain. Headache was the next item described with a weight under 0.5. Factors four and five explained 6.9% and 6.3% of the variance, respectively. They conformed to the dimension named as “sleep disturbances” and “suicidal ideation,” respectively. Factor six explained 4.8% of the variance and shows that alcohol consumption refusal was correlated with obsessions and suicidal ideation. The inverse correlation failed due to the low frequency of patients who indicated the consumption of alcohol (22 patients, 1.3%).
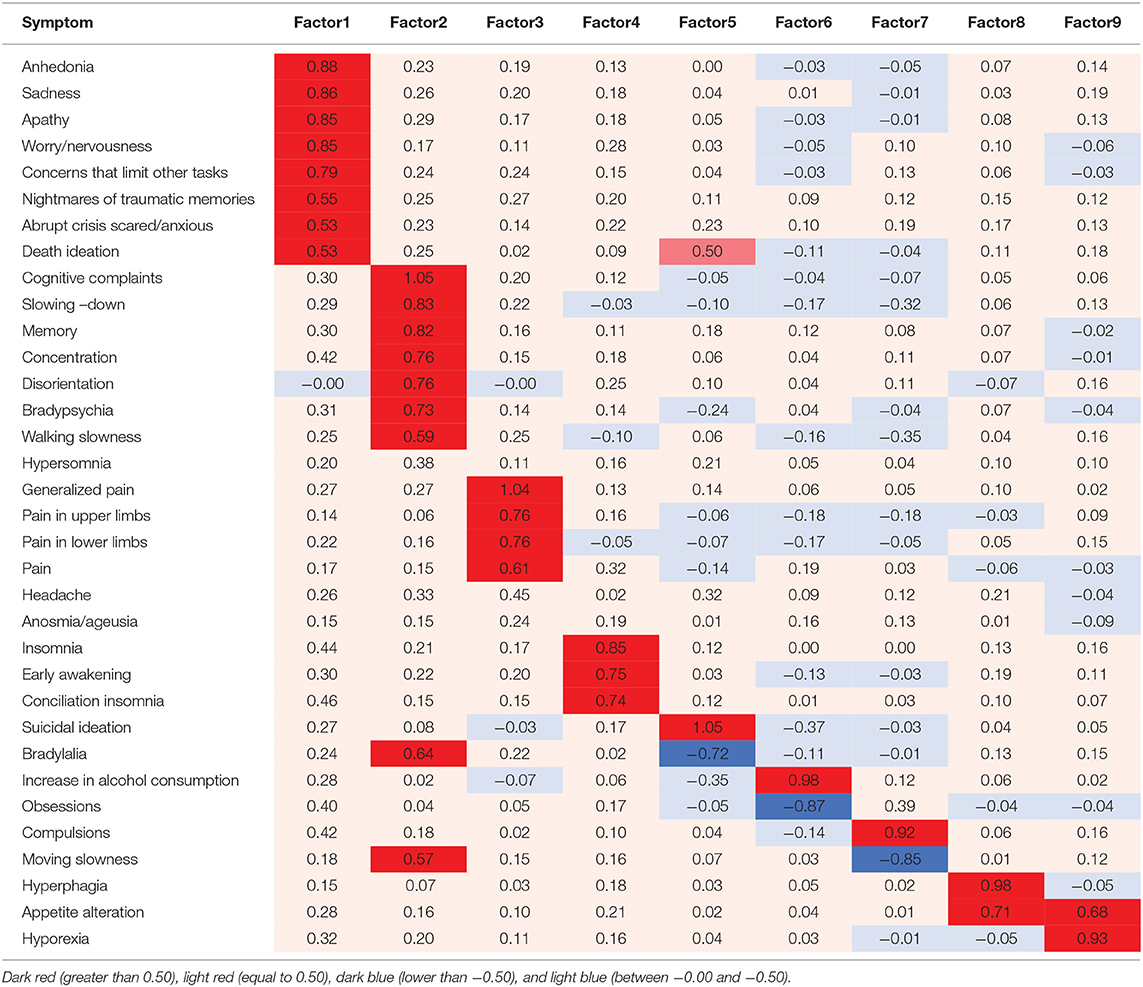
Table 3. Factorial analysis.
Factors seven, eight, and nine explained 4.7%, 3.9%, and 3.3% of the variance, and constituted the dimension “compulsion” with only one item, “feeding,” including the following variables: appetite alteration and hyperphagia, and the latter, “hyporexia,” sharing the appetite alteration item with the previous factor. The remaining and most frequent item anosmia/ageusia was not appropriately explained by the factors included in the factorial analysis (final communalities lower than 0.80). Given that factors one and two grouped eight and seven variables, respectively, patients were distinguished into four groups: those who showed characteristics of both factors; patients who showed characteristics mostly from factor one or factor two, and those who showed none of the characteristics of these factors.
Table 4 shows the mental disorders diagnosed in the confirmation phase, after the screening evaluation. A mental health disorder was confirmed in 14.8% of the participants who experienced significant symptoms in the screening phase. The most frequent confirmed mental problems include anxiety disorders (4.5% of them), depressive disorders (4.2%), and PTSD (2.6%). A significantly greater percentage of patients with confirmed diagnoses showed positive responses for practically all factors (except factors six and seven) than those with no confirmed diagnosis (p < 0.001, Figure 1).
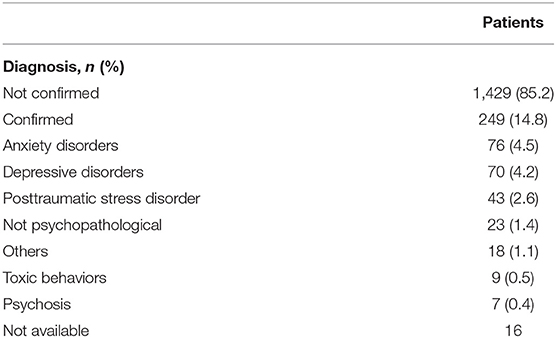
Table 4. Confirmation of diagnoses from the screening phase.
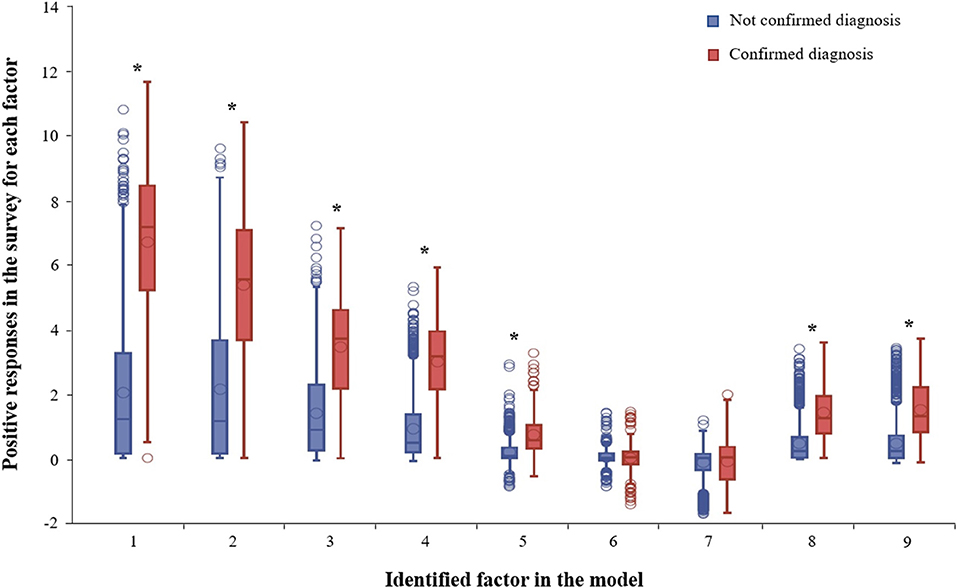
Figure 1. Box plot with positive responses in the survey for each factor identified in the principal component analysis considering the diagnostic confirmation. Asterisks represent statistical differences (Wilcoxon test) found between groups (p < 0.001).
Table 5 shows the positive responses for the first four factors, which were significantly greater in women (vs. men, p < 0.001 in all factors), participants with psychiatric history (vs. those with no history, p < 0.001 in all factors), duration of the hospital stay (especially more than 13 days, p = 0.002, p = 0.001, p = 0.001, and p = 0.021 for the factors, respectively), and age groups (mainly between 50 and 60 years, p < 0.001 in all factors). Regarding the time until the survey, positive responses were significantly higher for the fourth factor, especially when ≤ 92 days (p < 0.001).
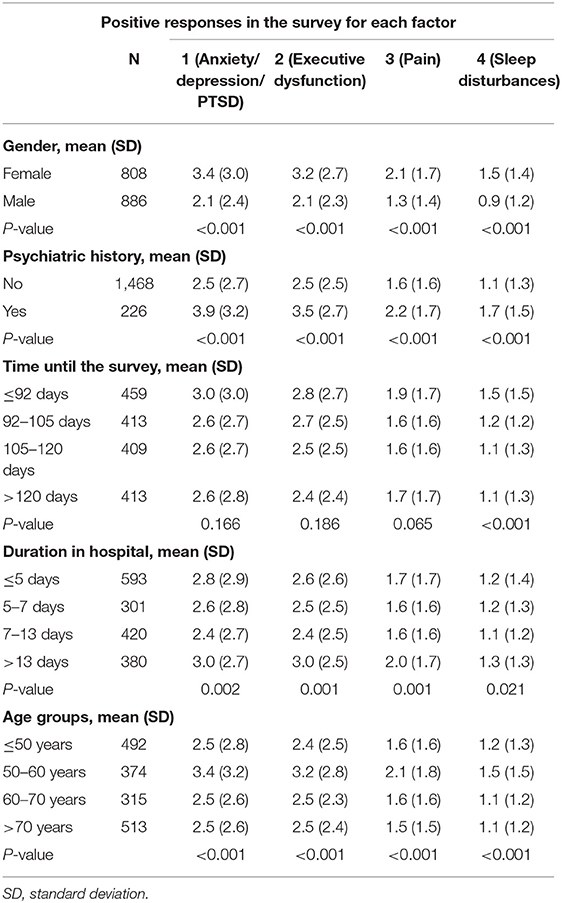
Table 5. Association between patient's risk factors and main factors identified in the principal component analysis.
The results obtained in this study reports the factor structure of the symptoms developed by a large sample of hospitalized patients with a confirmed diagnosis of SARS-CoV2 during the first wave of the COVID-19. The results of the factor analysis revealed that some items loaded strongly on different dimensions, above the 0.5 thresholds (Table 3). Interestingly, three item domains (anxiety, depression, and PTSD symptoms) were loaded together on one factor, whereas sleep disturbances stood up as a separate factor. One explanation could be that these two factors present two different mechanisms that underlie “anxiety–depression.” Another approach could be that “sleep disturbances” is more diagnosis oriented, while the other three item domains are oriented more toward symptoms associated with stress. A symptom dimension comprising items related to “executive dysfunction” is grouped into factor two. The items of symptoms related to pain were grouped into factor three and completed the structure of the four principal factors that accounted for 72% of the variance. Anosmia/ageusia is the most frequent symptom reported (followed by cognitive complaints, worry/nervousness, slowing down, and sadness). It is noteworthy that this neurological item was not captured by any of the factors described.
The strong convergence between the greater percentage of patients with confirmed diagnoses showing positive responses for factors one to four than those with no confirmed diagnosis was interpreted as evidence of validity in this sample.
The COVID-19 pandemic has deeply impacted on numerous facets from our lives (18). One of its consequences is the emerging of mental disorders in the general and specific populations, including COVID-19 patients. Despite the existence of literature, available studies are mainly focused on case series, self-report questionnaires, and surveys. Furthermore, available literature has provided scarce information about subclinical psychiatric symptoms by COVID-19. According to the mental health continuum model by Chen et al. (19), psychiatric symptoms are early signs of mental disorders, and individuals with severe and durable symptoms have a higher likelihood for developing them. Therefore, the early evaluation and identification of psychiatric symptoms have clinical implications for COVID-19 patients. The goals of our study were to identify and classify neuropsychological symptoms of hospitalized COVID-19 patients, study the correlation with diagnosed mental disorders, and explore the potential risk factors associated with mental health problems. The study comprised an initial screening phase and, subsequently, a diagnosis confirmation phase. The screening was conducted in COVID-19 survivors (the entire population) by hospital intern psychiatrists and psychologists. A semistructured phone interview, an ad hoc tool that covers a wide spectrum of psychiatric symptoms, was used. The principal component method yielded two factors that accounted for 45.4% and 11.5% of the variance, respectively. The first factor captured the items of anxiety, depression, and posttraumatic stress disorders, and the second captured the items of executive dysfunction. Factor loading was strong (all eigenvalues >0.5). These items were identified as frequent symptoms reported in patients after hospital discharge. These results are in concordance with previous literature (20–27). A study performed in China has demonstrated that insomnia, anxiety, and depressive symptoms are frequent sequels in patients after 6 months of the hospital discharge, especially in those with severe disease (28). Moreover, it has been shown that one in three survivors show executive dysfunction and mainly alterations in the attention (20). In the US, the number of diagnosed cases of anxiety, mood disorder, cognitive impairment, and insomnia increased in individuals with a diagnosis of COVID-19 (21). In Spain, ~60 and 40% of patients show moderate cognitive alterations and psychiatric morbidity, respectively, after 2 months of hospital discharge (22). Studies have also evidenced a prevalence of more than 95% for posttraumatic symptoms (23) and >30% for depression in patients with COVID-19 who have been hospitalized and stabilized (24). Studies carried out in different countries have reported a PTSD prevalence of ~20% after hospital discharge (25).
Furthermore, our results reveal that the susceptibility was higher in females and individuals aged between 50 and 60 years, after a long hospital stay (more than 13 days). Diverse studies have evidenced the higher psychological impact of the pandemic on young individuals, compared with other age groups, presumably associated with the pronounced change in their life stages (study, work, or social life) (29). Studies have also reported that younger individuals are more likely to experience loneliness than older ones (29, 30). Indeed, loneliness is strongly correlated with the development of psychological disorders (31). Despite the prevalence of confirmed mental disorder diagnosis was low, results suggest higher susceptibility in those with lifetime mental disorders, according to previously described literature. Two studies performed in Italy reported that up to 55% of the survivors have showed psychiatric sequels (PTSD, anxiety, insomnia, and obsessive–compulsive symptoms) 1 and 3 months after the infection, especially in women, young individuals, and those with lifetime mental disorders (26, 27). As documented in the literature (32–35), individuals with psychiatric illnesses are at a higher risk of aggravating their condition with the pandemic, especially among survivors (32). In a study conducted in Spain, the prevalence of cognitive impairment is higher in patients with psychiatric symptoms (22). A systematic review and meta-analysis evaluating the impact of preexisting mental illness in pandemics (including COVID-19, SARS, and influenza ones) revealed a higher development of psychiatric symptoms (mainly anxiety, depression, and insomnia) in individuals with lifetime mental conditions, compared with those without them (33). Furthermore, the authors showed a decrease in the use of psychiatric services and hospitalizations due to psychiatric events during pandemics. Similarly, Gobbi et al. (34) examining the status of 2,734 psychiatric patients worldwide and 318 from the US during the COVID-19 pandemic, concluded that more than 50% of these individuals experienced the worsening of their psychiatric conditions.
Causes associated with the development of short-term mental problems in patients may be derived from the direct effect of the virus in the central nervous system, the neuroinflammation secondary to cytokine dysregulation, the respiratory distress syndrome, the elevated prevalence of delirium, and the treatments used especially at the beginning of the pandemic (such as hydroxychloroquine, lopinavir/ritonavir, and corticoids). On the other hand, symptoms of mental health, such as the anxiety–depression–trauma complex, may be related to the confinement and other emotional stressors and traumatic memories associated with the hospitalization and the severe course of the disease (11, 13, 14, 26). It is well-known that patients remain with anosmia due to the neuronal affection induced by the virus (36). It is thought that one of the mechanisms involved in this manifestation is the disruption of olfactory neurons (37). Therefore, it may explain why that particular symptom is not eligible by any factor in the current analysis.
The main limitation of the study is derived from the methodological design in identifying symptoms associated with mental health, based on a phone interview. Although the use of specific questionnaires for each mental problem could probably strengthen the obtained results, the principal component analysis is a frequent methodology in this kind of studies, used to analyze the internal structure of a relatively large number of variables and develop predictive models. Moreover, patients were retrospectively interviewed. This may have affected the answer given by the patients. Some simplifications in the factorial analysis, useful for the result interpretation, may be poorly reproducible. Nonetheless, our observations are in line with previous studies (20–27, 32–35).
This evidence points out to a presumable increase in neuropsychiatric morbidity in the upcoming months and years. Furthermore, together with the social and economic crisis, it is presumable to expect an increase in suicides in the general population and survivors, similar to that that occurred in previous coronavirus pandemics. Therefore, the multidisciplinary follow-up of patients becomes crucial to guarantee the management of their emotional consequences, with the notable relevance of mental health professionals in this scenario. In this context, screening for early signs or symptoms is the first step to improve the accuracy of early detection and prevent mental health problems. Further prospective, long-term studies, using validated questionnaires, are required to confirm our results and deepen the impact of the pandemic.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval was not provided for this study on human participants because the Ethics Committee of the center in which the study was performed considered there was no need for an evaluation since: (1) it was a retrospective study in which medical records were only reviewed; (2) no intervention was performed; and (3) the database was anonymized to preserve sensitive data from patients. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
JM and IR reviewed the literature. GR, FR-C, and JM conceived and designed the study. IR, AJ, and CC acquired the data. DL, IR, AJ, CC, and JM cleaned and analyzed the data. JM, GR, JA, and FR-C drafted the initial version of the manuscript. All authors reviewed the initial draft and made critical contributions to the interpretation of the data and approved the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.838239/full#supplementary-material
1. World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online at: https://covid19.who.int/ (accessed May 10, 2021).
2. Spanish Spanish Ministry of Health Consumer Affairs and Social Welfare. Current Situation. Available online at: https://www.mscbs.gob.es/en/profesionales/saludPublica/ccayes/alertasActual/nCov/situacionActual.htm (accessed May 10, 2021).
3. Else H. How a torrent of COVID science changed research publishing - in seven charts. Nature. (2020) 588:553. doi: 10.1038/d41586-020-03564-y
4. SeyedAlinaghi S, Afsahi AM, MohsseniPour M, Behnezhad F, Salehi MA, Barzegary A, et al. Late complications of COVID-19; a systematic review of current evidence. Arch Acad Emerg Med. (2021) 9:e14. doi: 10.22037/aaem.v9i1.1058
5. Rubio-Rivas M, Corbella X, Mora-Luján JM, Loureiro-Amigo J, López Sampalo A, Yera Bergua C, et al. Predicting clinical outcome with phenotypic clusters in COVID-19 pneumonia: An analysis of 12,066 hospitalized patients from the Spanish Registry SEMI-COVID-19. J Clin Med. (2020) 9:3488. doi: 10.3390/jcm9113488
6. Spanish Spanish Ministry of Health Consumer Affairs and Social Welfare. Actualization Number 335. Available online at: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_335_COVID-19.pdf (accessed February 11, 2022).
7. Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. (2020) 77:683–90. doi: 10.1001/jamaneurol.2020.1127
8. Bryant SE, McNabb K. Postintensive care syndrome. Crit Care Nurs Clin North Am. (2019) 31:507–16. doi: 10.1016/j.cnc.2019.07.006
9. Banerjee D, Viswanath B. Neuropsychiatric manifestations of COVID-19 and possible pathogenic mechanisms: insights from other coronaviruses. Asian J Psychiatry. (2020) 54:102350. doi: 10.1016/j.ajp.2020.102350
10. Roy D, Ghosh R, Dubey S, Dubey MJ, Benito-León J, Kanti Ray B. Neurological and neuropsychiatric impacts of COVID-19 pandemic. Can J Neurol Sci J Can Sci Neurol. (2021) 48:9–24. doi: 10.1017/cjn.2020.173
11. Borah P, Deb PK, Chandrasekaran B, Goyal M, Bansal M, Hussain S, et al. Neurological consequences of SARS-CoV-2 infection and concurrence of treatment-induced neuropsychiatric adverse events in COVID-19 patients: navigating the uncharted. Front Mol Biosci. (2021) 8:627723. doi: 10.3389/fmolb.2021.627723
12. Stefano GB. Historical insight into infections and disorders associated with neurological and psychiatric sequelae similar to long COVID. Med Sci Monit. (2021) 27:e931447. doi: 10.12659/MSM.931447
13. Troyer EA, Kohn JN, Hong S. Are we facing a crashing wave of neuropsychiatric sequelae of COVID-19? Neuropsychiatric symptoms and potential immunologic mechanisms. Brain Behav Immun. (2020) 87:3439. doi: 10.1016/j.bbi.2020.04.027
14. Rogers JP, Chesney E, Oliver D, Pollak TA, McGuire P, Fusar-Poli P, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. (2020) 7:611–27. doi: 10.1016/S2215-0366(20)30203-0
15. Vindegaard N, Benros ME. COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immun. (2020) 89:531–42. doi: 10.1016/j.bbi.2020.05.048
16. Liu D, Baumeister RF, Zhou Y. Mental health outcomes of coronavirus infection survivors: A rapid meta-analysis. J Psychiatr Res. (2021) 137:542–53. doi: 10.1016/j.jpsychires.2020.10.015
17. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59:22–33.
18. Alzueta E, Perrin P, Baker FC, Caffarra S, Ramos-Usuga D, Yuksel D, et al. How the COVID-19 pandemic has changed our lives: a study of psychological correlates across 59 countries. J Clin Psychol. (2021) 77:556–70. doi: 10.1002/jclp.23082
19. Chen SP, Chang WP, Stuart H. Self-reflection and screening mental health on Canadian campuses: validation of the mental health continuum model. BMC Psychol. (2020) 8:76. doi: 10.1186/s40359-020-00446-w
20. Zhou H, Lu S, Chen J, Wei N, Wang D, Lyu H, et al. The landscape of cognitive function in recovered COVID-19 patients. J Psychiatr Res. (2020) 129:98–102. doi: 10.1016/j.jpsychires.2020.06.022
21. Taquet M, Luciano S, Geddes JR, Harrison PJ. Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry. (2021) 8:130–40. doi: 10.1016/S2215-0366(20)30462-4
22. Méndez R, Balanzá-Martínez V, Luperdi SC, Estrada I, Latorre A, González-Jiménez P, et al. Short-term neuropsychiatric outcomes and quality of life in COVID-19 survivors. J Intern Med. (2021) 3: 13262. doi: 10.1111/joim.13262
23. Bo HX, Li W, Yang Y, Wang Y, Zhang Q, Cheung T, et al. Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychol Med. (2020) 27:1–2. doi: 10.1017/S0033291720000999
24. Parker C, Shalev D, Hsu I, Shenoy A, Cheung S, Nash S, et al. Depression, anxiety, and acute stress disorder among patients hospitalized with COVID-19: a prospective cohort study. J Acad Consult Liaison Psychiatry. (2021) 62:211–19. doi: 10.1016/j.psym.2020.10.001
25. Nakamura ZM, Nash RP, Laughon SL, Rosenstein DL. Neuropsychiatric complications of COVID-19. Curr Psychiatry Rep. (2021) 23:25. doi: 10.1007/s11920-021-01237-9
26. Mazza MG, De Lorenzo R, Conte C, Poletti S, Vai B, Bollettini I, et al. Anxiety and depression in COVID-19 survivors: role of inflammatory and clinical predictors. Brain Behav Immun. (2020) 89:594–600. doi: 10.1016/j.bbi.2020.07.037
27. Mazza MG, Palladini M, De Lorenzo R, Magnaghi C, Poletti S, Furlan R, et al. Persistent psychopathology and neurocognitive impairment in COVID-19 survivors: effect of inflammatory biomarkers at three-month follow-up. Brain Behav Immun. (2021) 94:138–47. doi: 10.1016/j.bbi.2021.02.021
28. Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. (2021) 397:220–32. doi: 10.1016/S0140-6736(20)32656-8
29. Liu MB, Dufour G, Sun ZE, Galante J, Xing CQ, Zhan JY, et al. The impact of the COVID-19 pandemic on the mental health of young people: a comparison between China and the United Kingdom. Chin J Traumatol. (2021) 24:231–6. doi: 10.1016/j.cjtee.2021.05.005
30. Li LZ, Wang S. Prevalence and predictors of general psychiatric disorders and loneliness during COVID-19 in the United Kingdom. Psychiatry Res. (2020) 291:113267. doi: 10.1016/j.psychres.2020.113267
31. Killgore WDS, Cloonan SA, Taylor EC, Lucas DA, Dailey NS. Loneliness during the first half-year of COVID-19 lockdowns. Psychiatry Res. (2020) 294:113551. doi: 10.1016/j.psychres.2020.113551
32. Stamu-O'Brien C, Carniciu S, Halvorsen E, Jafferany M. Psychological aspects of COVID-19. J Cosmet Dermatol. (2020) 19:2169–73. doi: 10.1111/jocd.13601
33. Neelam K, Duddu V, Anyim N, Neelam J, Lewis S. Pandemics and pre-existing mental illness: a systematic review and meta-analysis. Brain Behav Immun Health. (2021) 10:100177. doi: 10.1016/j.bbih.2020.100177
34. Gobbi S, Płomecka MB, Ashraf Z, Radziński P, Neckels R, Lazzeri S, et al. Worsening of preexisting psychiatric conditions during the COVID-19 pandemic. Front Psychiatry. (2020) 11:581426. doi: 10.3389/fpsyt.2020.581426
35. Pera A. Depressive symptoms, anxiety disorder, and suicide risk during the COVID-19 pandemic. Front Psychol. (2020) 11:572699. doi: 10.3389/fpsyg.2020.572699
36. Galougahi MK, Ghorbani J, Bakhshayeshkaram M, Naeini AS, Haseli S. Olfactory bulb magnetic resonance imaging in SARS-CoV-2-induced anosmia: the first report. Acad Radiol. (2020) 27:892–93. doi: 10.1016/j.acra.2020.04.002
Keywords: COVID-19, mental health, women, psychiatric history, screening
Citation: Molina JD, Rodrigo Holgado I, Juanes González A, Combarro Ripoll CE, Lora Pablos D, Rubio G, Alonso J and Rivas-Clemente FPJ (2022) Neuropsychological Symptom Identification and Classification in the Hospitalized COVID-19 Patients During the First Wave of the Pandemic in a Front-Line Spanish Tertiary Hospital. Front. Psychiatry 13:838239. doi: 10.3389/fpsyt.2022.838239
Received: 17 December 2021; Accepted: 14 January 2022;
Published: 02 March 2022.
Edited by:
Lawrence T. Lam, University of Technology Sydney, AustraliaReviewed by:
Suprakash Chaudhury, Hospital and Research Centre, IndiaCopyright © 2022 Molina, Rodrigo Holgado, Juanes González, Combarro Ripoll, Lora Pablos, Rubio, Alonso and Rivas-Clemente. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan D. Molina, anVhbmRlLm1vbGluYUBzYWx1ZC5tYWRyaWQub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.