
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 18 April 2022
Sec. Public Mental Health
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.814242
This article is part of the Research Topic Mental Health Promotion and Protection View all 34 articles
 Zhipeng Wu1,2
Zhipeng Wu1,2 Zhengqian Jiang3
Zhengqian Jiang3 Zhipeng Wang3Yuqiao Ji3
Zhipeng Wang3Yuqiao Ji3 Feiwen Wang1,2
Feiwen Wang1,2 Brendan Ross4Xiaoqi Sun5
Brendan Ross4Xiaoqi Sun5 Zhening Liu1,2
Zhening Liu1,2 Yicheng Long1,2*
Yicheng Long1,2*
Introduction: Wisdom has been empirically researched as a complex psychological characteristic that is associated with many mental health outcomes. However, its association with psychotic-like experiences (PLEs) remains unclear. This is the first work to assess wisdom, explore its association with PLEs, and test its moderating effect on the relation between the frequency of PLEs and their associated distress in the general population.
Methods: From January 29th to February 5th, 2021, our online self-administered survey recruited 927 participants (ages 14 to 65) from thirteen Chinese provinces. Convenience sampling was employed. We measured wisdom with the 12-item three-dimensional wisdom scale (3D-WS-12) and PLEs with the 15-item positive subscale of the Community Assessment of Psychic Experiences (CAPE-P15).
Results: Using the cut-off value of 1.47 in the mean frequency score, we divided our participants into high-PLEs group (188, 22.1%) and low-PLEs group (663, 77.9%). Three-dimensional wisdom score was decreased in the high-PLEs group compared to the low-PLEs group (Kruskal-Wallis t = 59.9, p < 0.001). Wisdom was associated with less frequent PLEs (Spearman’s rho = −0.21, p < 0.01) and lower distress related to PLEs (Spearman’s rho = −0.28) in the high-PLEs group (all above p < 0.001), which were replicated in the low-PLEs group. Notably, wisdom significantly attenuated the distress associated with PLEs [coefficient = −0.018, Bootstrap 95% CI (−0.029, −0.008)], but only in the low-PLEs group.
Conclusion: Our results implicated that wisdom could protect individuals from distressful subclinical psychotic symptoms and wiser individuals have better general mental health.
Wisdom, a complex and trait-based psychological construct that has been consistently discussed in religious and philosophical texts for centuries, has emerged as a new field of empirical research since the 1970s (1). The essence of wisdom research lies in the definition of wisdom and its empirical measurement. Baltes and Staudinger posited that wisdom was embedded in extensive pragmatic knowledge, concentrating on the cognitive and intellectual aspect (2). Clayton supplemented reflective and affective domains to the components of wisdom (3). Sternberg postulated that wisdom derived from an employment of knowledge regarding to the balance of personal and societal interests (4). Josefsson and colleagues’ research on wisdom stressed some aspects related to wellbeing (5). Ardelt developed a three-dimension model to assess wisdom from cognitive (a deep understanding of human existence and relationships), reflective (accurate/unbiased introspection and perspective-taking), and affective (an emotional affinity for others) domains (6). Wang and Chen claimed that wisdom is a comprehensive psychological construct integrating intelligence and morality (7). Although wisdom might be perceived differently in western and eastern cultures, Jeste and Vahia found that the ancient eastern wisdom components are largely in line with modern view of western wisdom, such as emotion regulation and insight (8).
The assessment of wisdom can be based on interviews by experts, such as the Berlin Wisdom Paradigm (9), or self-reported questionnaires, such as the well-recognized 30-item Self-Assessed Wisdom Scale (SAWS) measuring wisdom from five factors: critical life experiences, emotions, reminiscence, openness, and humor; the 39-item Three-Dimensional Wisdom Scale (3D-WS-39) based on the three-dimensional wisdom model (6, 10); and the newly emerged 28-item San Diego Wisdom Scale (SD-WISE) consisting of six domains: social advising, emotional regulation, pro-social behaviors, insight, tolerance for divergent values, and decisiveness (11). It should be noted that self-reported wisdom is highly related to interview-based wisdom and thus suggests an applicability of using self-reported measures in large-scale studies (1). However, these self-administered questionnaires are lengthy and thus limited in use for multifactorial assessments in psychiatric epidemiology. Hence, Thomas et al. developed a 12-item abbreviated Three-Dimensional Wisdom scale (3D-WS-12) that can be administered quickly within the context of epidemiological surveys and show considerable efficiency and validity (12).
A growing body of studies have found that wisdom is associated with multiple health-related outcomes, encompassing better general physical and mental health (13), wellbeing (14), happiness (15), life satisfaction, successful aging, and resilience (11, 16), as well as lower degree of loneliness (17) in the general population. However, the psychiatric assessments involved in these studies mainly covered subclinical anxiety, depressive symptoms, or common positive domains including wellbeing and resilience, while missing the inclusion of psychotic phenomena, a spectrum of less prevalent but even more debilitating subclinical symptoms. Thus, studies covering psychotic phenomena are warranted to get a more comprehensive picture of the association between wisdom and mental health at subclinical level.
Psychotic-like experiences (PLEs), usually known as subclinical delusions or hallucinations, are common in the general population (18–21). In line with the psychosis continuum model, healthy individuals reporting these symptoms are considered to represent a non-clinical psychosis phenotype and thus supposed to be at high risk of schizophrenia-spectrum disorder (20, 22, 23). More recently, under the notion that PLEs usually coexist with affective symptoms including depression and anxiety (24–27), it is also suggested that PLEs are more likely to serve as an indicator of common mental distress, instead of a single risk state for psychosis (28). For both perspectives, psychotic phenomena such as PLEs are recommended to be included as a significant part of assessment in psychiatric epidemiology.
In addition to depressive and anxiety symptoms, previous studies demonstrated that individuals with PLEs, especially delusional experiences, are prone to cognitive bias, for instance, jump to conclusion (JTC), belief inflexibility (BIB) and aberrant salience bias (ASB) (29–31), in line with well-established findings in patients with full-blown psychosis (32–35). Moreover, it was found that patients at ultra-high risk for psychosis showed significant impairments in social cognition that involves the cognitive processes of perceiving, interpreting, and processing social information (36). Further, adults with PLEs presented dysfunction in emotion regulation (ER), which can be regarded as an element of wisdom; and ER is associated with the frequency and distress level of their PLEs (37). However, these studies are not comprehensive since they did not target wisdom as a whole and thus limited in shedding light on the relation between wisdom and subclinical psychotic symptoms. Further studies investigating wisdom as a unitary psychological construct in the population with PLEs are in pressing need because wisdom could protect high-risk individuals for full-onset psychosis.
To the best of our knowledge, this is the first study to investigate the association between wisdom and PLEs and test its moderating role in the relation between frequency of PLEs and their associated distress in the general population. Specifically, adopting the three-dimensional wisdom model, we tested the following hypotheses: (1) wisdom level is decreased in the population with high-level PLEs compared with those having less PLEs; (2) wisdom is negatively associated with the frequency of PLEs and their associated distress; and (3) wisdom attenuates the relation between frequency of PLEs and their associated distress. We expected to see that although wisdom might decrease with the existence of PLEs, wiser individuals may have less frequent and lower distress related to PLEs. Hence, wisdom might be a good intervention target for lowering the social burden of psychosis in the future.
This study was designed as an online cross-sectional survey. We adopted a self-reported questionnaire link at the largest online survey platform in China called “Questionnaire Star1”. Our online-based data collection was performed between January 29th and February 5th, 2021. A set of self-rating assessments were distributed to students, corporate staff and retired population from 13 different provinces in China (Hunan, Shanghai, Shanxi, Heilongjiang, Jiangsu, Henan, Guangdong, Shandong, Yunnan, Chongqing, Shaanxi, Anhui, and Jiangxi provinces) using convenience sampling method (38). Specifically, we employed thirteen volunteers, who were college students from above-mentioned provinces, to disseminate the questionnaire link and each volunteer reached at least 100 individuals through WeChat (the largest social media application in China) message. Each participant was electronically informed about the purpose of our study and asked to complete an electronic consent inform, and consent from guardians was also requested for those below 18 years old. With their consent, participants completed all the questionnaires before uploading their answers. Each participant who completed our survey was reimbursed five RMB for their time. On average, it took 10 min for each participant to finish these questionnaires.
Our participants were recruited using the following criteria. Inclusion criteria of the study included: (i) able to understand and complete these questionnaires using electronic devices, (ii) consented to participate in this study, and (iii) without history of psychiatric diagnosis. The study was approved by the Ethics Committees of the Second Xiangya Hospital of Central South University.
The abbreviated Three-Dimensional Wisdom Scale (3D-WS-12) was refined from the original three-dimensional wisdom scale (3D-WS-39) (6, 12). It contains 12 items covering affective, reflective, and cognitive dimensions of wisdom, and each domain contains 4 items. Answers to each item include range from 1 = strongly agree or definitely true of myself to 5 = strongly disagree or not true of myself. This wisdom screening tool has been translated into Chinese and shown to be valid to assess wisdom in Chinese population (39). Cronbach’s alpha for the total score of 3D-WS-12 in our sample was 0.79, which were 0.71, 0.75, 0.72 for cognitive, reflective, and affective subscales, respectively.
The 15-item positive subscale of the Community Assessment of Psychic Experiences (CAPE-P15) contains two dimensions: frequency and associated distress of PLEs. Each subscale measures the frequency or associated distress of PLEs from three positive psychotic domains: persecutory ideation (PI, 5 items), bizarre experiences (BE, 7 items), and perceptual abnormalities (PA, 3 items) (40). The psychometric properties of the Chinese version of CAPE-P15 were validated (41). Participants completed the questionnaire based on their past 3 months’ experiences. Answers in the frequency subscale include: 1-never, 2-sometimes, 3-often, and 4-nearly always. Answers in the distress subscale include: 1-not distressed, 2-a bit distressed, 3-quite distressed, and 4-very distressed. The total frequency score was divided by the number of valid answers to reach an average frequency score for each participant. An average frequency score of 1.47 was adopted as the cut-off value for participants with high-level PLEs (high-PLEs group) versus participants with low-PLEs (41, 42). In our sample, Cronbach’s alpha for the total frequency score was 0.88, which was 0.87 for the total distress score.
We obtained the following demographic information from participants: age, sex, education years, and personal history of psychiatric illness. We screened participants’ personal history of psychiatric diagnoses with the question: “Have you ever been diagnosed with any mental disorder?”.
Before statistical analysis, we excluded participants with any previous psychiatric diagnosis to focus on studying subclinical symptoms. We also eliminated subjects whose age apparently did not match their education years and those who spent very little time (less than 3 min in total) on the survey, to filter out those potentially flawed samples.
Our analysis included three major steps. First, we examined the normality and skewness of all measurements using the Shapiro–Wilk test. Since these variables did not meet the assumption of normality (p < 0.05), we employed non-parametric methods in the following analysis. Then descriptive analysis was used to present the characteristics of our sample. Second, we divided the participants into two groups (the high-PLEs and the low-PLEs group) using the cut-off value of 1.47 in the mean frequency score of CAPE-P15 (41, 42) and compared the group difference in all variables using Chi-squared test or Kruskal-Wallis test. Then, Spearman correlation was employed to investigate the association between wisdom and frequency and associated distress of PLEs in the whole population and in two separate groups. Considering that demographic variables, such as age, might correlate both with wisdom and PLEs, we also tested the interaction between demographic variables and wisdom in the association between wisdom and frequency/distress of PLEs in each group using moderation models. Finally, we conducted moderation analysis to explore the moderating effect of wisdom on the relationship between the frequency of PLEs and associated distress in the whole group or in each of the two groups alone after controlling the demographic variables. PROCESS for Windows was used to build a moderation model (43). Bootstrap inference with 5,000 samples and heteroskedasticity-consistent standard error estimator (HC4) were adopted considering the violation of normal distribution, which was in accordance with our previous study (44). IBM SPSS 24.0 for Windows (45) was used for other statistical analyses.
Our online survey recruited 927 participants from thirteen Chinese provinces in total. We eliminated: 35 subjects for their previous diagnosis of any psychiatric illness, 37 subjects for spending less than 3 min on this survey, and 4 subjects for apparent mismatch between reported age and education years. No participant was discarded for missing value because the online survey can only be submitted with every question completed. After cleaning the data, a total of 851 participants entered the final data analysis, including 7.6% middle school students, 69.5% undergraduate students, 4.8% graduate students, 13.3% employed staff, and 4.8% the retired. Other details of sample characteristics are shown in Table 1.

Table 1. Sample characteristics.
Using the cut-off value of 1.47 in the mean frequency score of CAPE-P15 (41, 42), we identified 188 individuals with high-level PLEs (PLEs group, 22.1%) and 663 individuals with low-level PLEs (low-PLEs group, 77.9%). Three-dimensional wisdom total score was lower in the high-PLEs group, along with the cognitive, affective and reflective components (Table 2).
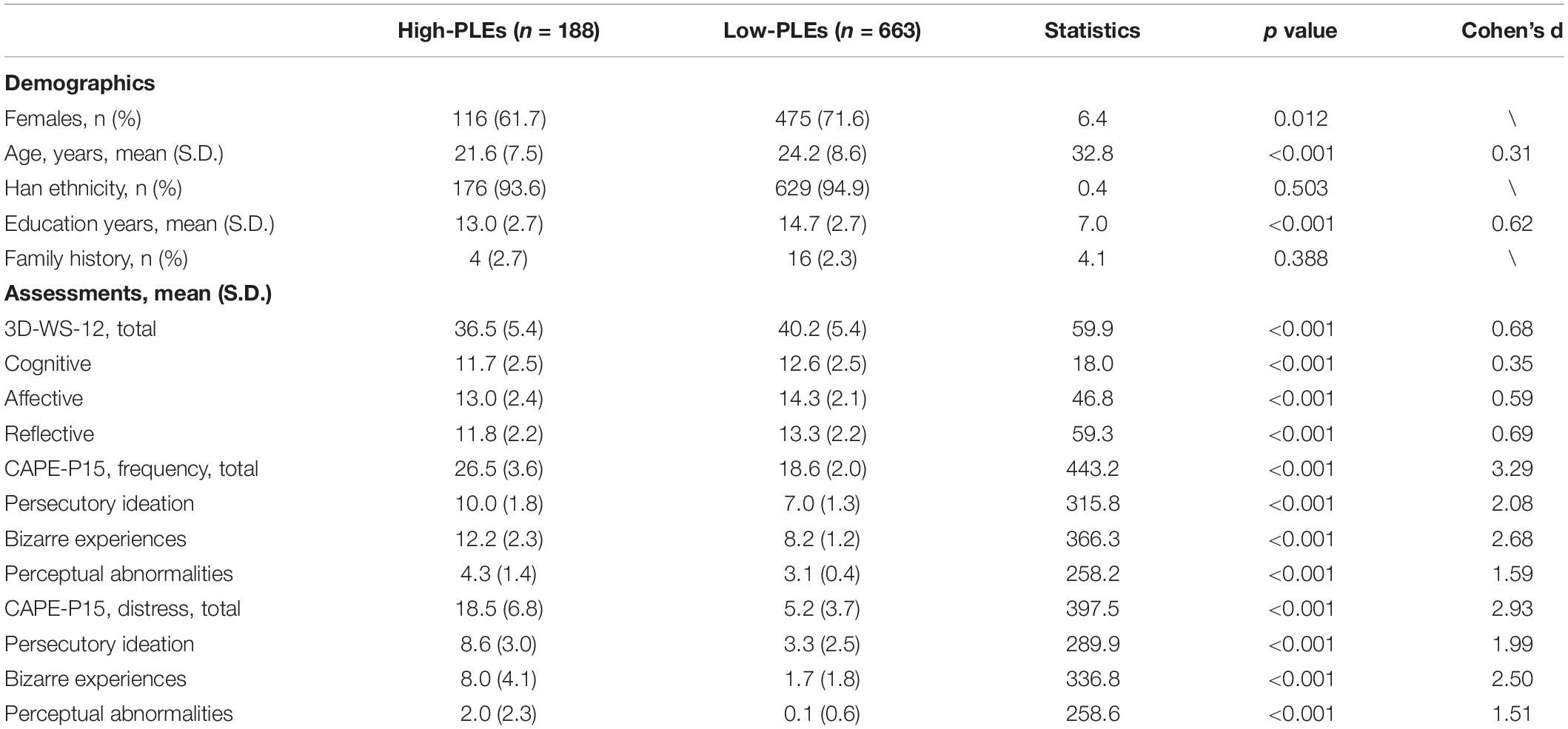
Table 2. Difference between high-PLEs and low-PLEs group in demographics and assessments.
At the population level, wisdom was negatively correlated with total frequency and associated distress of PLEs, which was replicated in three subtypes of PLEs: persecutory ideation (PI), bizarre experiences (BE), and perceptual abnormalities (PA). These results were verified in each dimension of wisdom (cognitive, affective, and reflective) (Table 3).
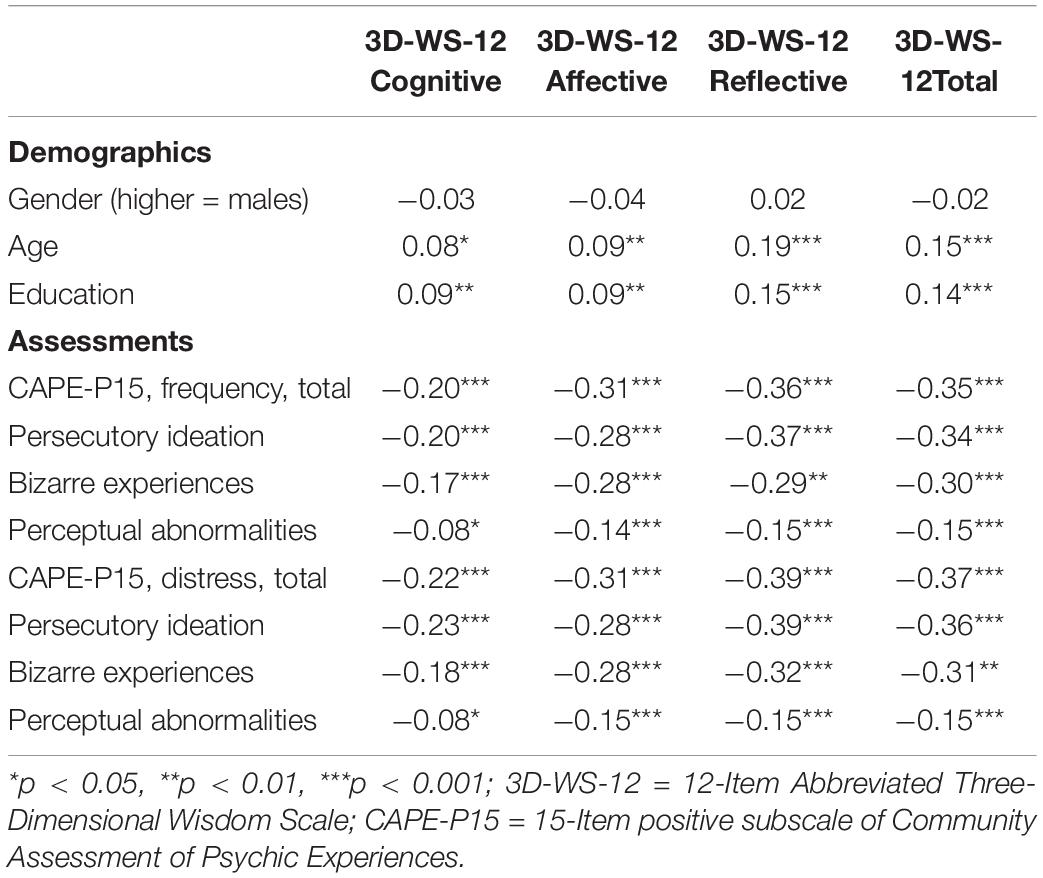
Table 3. Spearman’s correlations between wisdom and other variables in the whole population.
In the high-PLEs group, correlations between wisdom and frequency/distress of PLEs were still significant at the total score level, but wisdom was not correlated with the frequency and distress of perceptual abnormalities (PA), nor in any of the three wisdom subscales. It should be noted that reflective wisdom showed a slightly strong negative correlation with the total frequency and distress score of PLEs compared to cognitive and affective wisdom (Table 4).
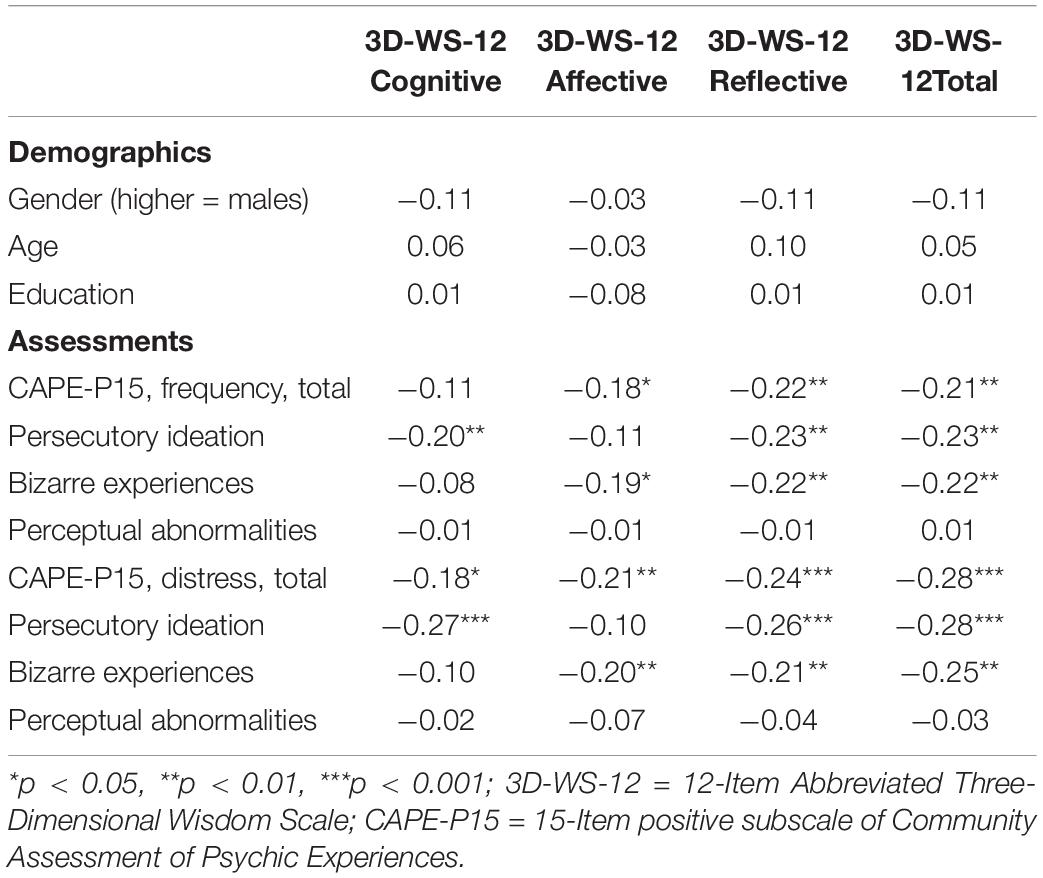
Table 4. Spearman’s correlations between wisdom and other variables in the high-PLEs group.
In the low-PLEs group, the total three-dimensional wisdom score was correlated with the total frequency and distress score of PLEs and PI/BE subscales except PA, as seen in the high-PLEs group. Other results were similar to findings in the high-PLEs group and the whole population (Table 5). Further analysis revealed that no significant interaction between demographic variables (age, gender, education) and total wisdom score was observed in the association between wisdom and frequency/distress of PLEs.
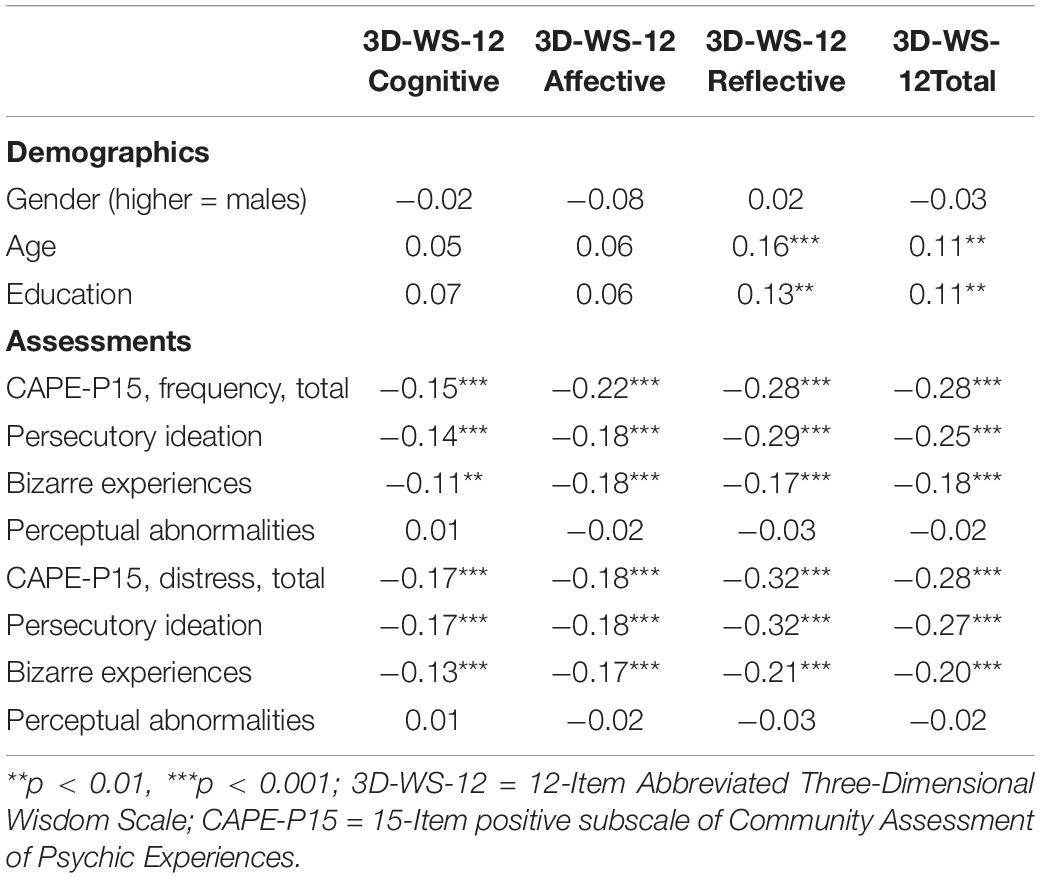
Table 5. Spearman’s correlations between wisdom and other variables in the low-PLEs group.
At the whole population level, after controlling for age, sex, and educational years, we observed no significant moderating effect of wisdom total score on the relation between PLEs frequency and associated distress, nor that of any of the three subscales of wisdom score. This was replicated in the high-PLEs group. However, in the low-PLEs group, total wisdom score significantly attenuated the relation between total PLEs frequency and associated distress [coefficient = −0.018, Bootstrap 95% CI (−0.029, −0.008)]. At the subscales level, this moderation existed in the cognitive [coefficient = −0.033, Bootstrap 95% CI (−0.058, −0.008)] and reflective [coefficient = −0.052, Bootstrap 95% CI (−0.079, −0.024)] wisdom but not in affective wisdom (Figure 1). We further tested this moderation on the subscales of CAPE-P15 (PI, BE, and PA), but the moderation of wisdom was only significant at the total frequency and distress level of PLEs.
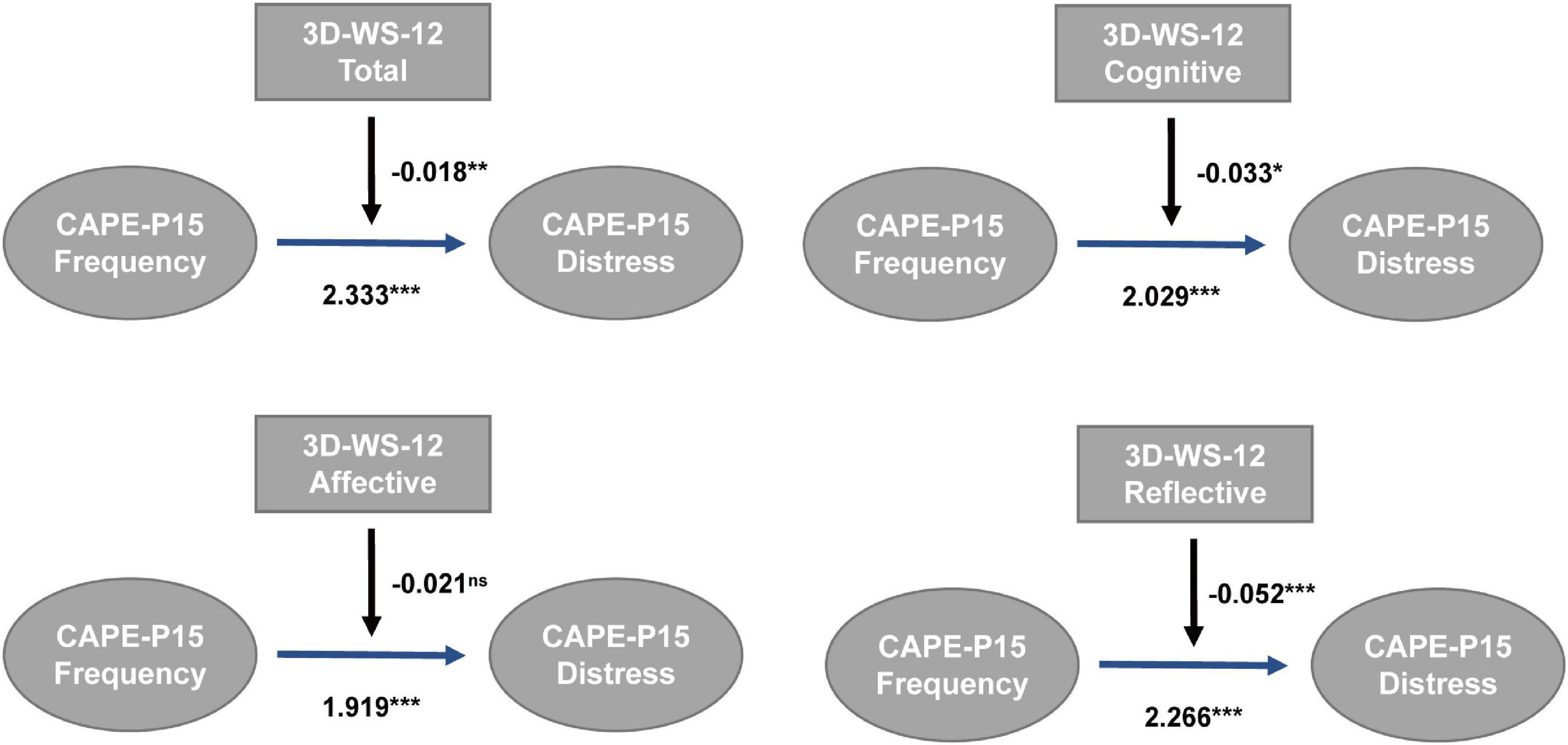
Figure 1. Moderation of wisdom in the relation between PLEs frequency and associated distress in low-PLEs group (N = 663, PROCESS Model 1, ns, not significant, *p < 0.05, **p < 0.01, ***p < 0.001).
To the best of our knowledge, this is the first work to investigate the association between wisdom and subclinical psychotic symptoms, and has three major findings. First, the three-dimensional wisdom level was decreased in participants with high-level PLEs compared to those with less PLEs. Second, wisdom was negatively associated with frequency and associated distress of PLEs. Third, wisdom attenuated the relation between the frequency of PLEs and their associated distress, but only when the frequency was relatively low.
To date, three-dimensional wisdom has not been measured in the subclinical psychotic population, but a previous study suggested that schizophrenia patients had lower wisdom scores (including cognitive, affective, and reflective wisdom) than the control group (46); our findings of decreased wisdom in the subclinical psychotic population highly resonate with these findings. Studies investigating the wisdom level as a whole in the subclinical psychotic population are still lacking. However, some aspects of wisdom were covered in previous studies. A large body of research concluded that many forms of cognitive biases were observed in individuals with PLEs, such as jumping to conclusions (JTC), aberrant salience (ASB), attention to threat (ATB), externalizing bias (ETB), and belief inflexibility (BIB) (30, 47–50). Notably, it is also well-established that patients with psychosis presented cognitive dysfunction that could precede the onset of full-blown disease with debilitating positive symptoms and cognitive distortion even contribute to the maintenance of psychotic symptoms (51). This suggests that the clinical and subclinical psychotic population might share similar alterations in cognitive function but with varying degrees. Cognitive wisdom, however, refers to an individual’s ability to understand life, to comprehend the significance and deeper meaning of phenomena and events, especially with regard to intrapersonal and interpersonal matters, such as the knowledge of the positive and negative aspects of human nature (6). Decreased cognitive wisdom in the population with high-level PLEs is likely to explain the existence of cognitive biases or distortions, which can possibly translate to cognitive symptoms of psychotic patients.
Notably, our results highlight the critical role of reflective wisdom in terms of association with common mental health domains covered in this study. Reflective wisdom is considered to be a prerequisite for developing cognitive wisdom. Perception of reality without any major distortions is mandatory to reach a deeper understanding of life. Wise individuals would engage in reflective thinking by looking at phenomena and events from different perspectives to develop self-awareness and self-insight (3, 6). Previous studies found that individuals with PLEs are prone to poor reflective reasoning and biased self-reflection (52, 53). In clinical settings, a large portion of patients with full-blown psychosis suffer from impaired insight and thus are difficult to reach a rational understanding of their conditions (54, 55). Our work provided further evidence that individuals with more PLEs showed undermined reflective capability, which can be explained by decreased reflective wisdom.
Affective wisdom represents positive emotions and behavior toward others, such as sympathy and compassion. Dysfunction in empathy can be observed in individuals at high risk for psychosis (56). At clinical settings, patients at risk for psychosis showed significant impairment in social cognition, specifically including difficulties in emotion recognition and social skills (36). Further, dysfunction in emotion regulation was associated with the frequency and distress of PLEs (37). In line with these findings, our results provided evidence that individuals with PLEs were in lack of affective wisdom, which is critical in forming social bonds with others.
Furthermore, individuals with higher wisdom tended to have less frequent PLEs and lower degrees of associated distress in the PLEs group. Notably, these findings also apply to the low-PLEs group, suggesting a general protective effect of wisdom for mental health. In these associations, reflective wisdom seemed to play a more significant role among the three wisdom dimensions, which was also observed in a wisdom study on schizophrenia patients (46) and can possibly be explained by the prerequisite role of reflective wisdom for generating cognitive and affective wisdom (6). For the three domains of PLEs, compared to persecutory ideation and bizarre experiences, it should be noted that wisdom showed little ameliorating effect on perceptual abnormalities, which implies that subclinical hallucinations and delusions might share a different nature.
Notably, the moderation results revealed that wiser individuals tended to have lower distress even with the same frequency of PLEs. However, this moderation was only significant among the participants who reported lower levels of PLEs (the low-PLEs group). It could be interpreted that wisdom can attenuate the distress associated with PLEs when the frequency is relatively low. When the frequency reaches a specific threshold, this moderation would no longer work due to the general deterioration of the individual’s condition and the possible loss of insight. Further, this moderation seemed more stronger for reflective wisdom, in accordance with its critical role in three-dimensional wisdom as aforementioned. Our findings were also supported by previous works. Cognitive biases moderated the relation between negative affective states and PLEs in non-clinical adults (57). Individuals having difficulties in emotion regulation showed more frequent PLEs and distress (37).
Our findings may have important implications for clinical practices. Wisdom is considered to be amenable to intervention (58) and thus can be trained and cultivated, just like resilience (59). Under this notion, tailored intervention targeting three dimensions of wisdom can potentially ameliorate the frequency and associated distress of PLEs in this non-clinical population, and meanwhile contribute to a better general mental health outcome. For instance, it could be hypothesized that enhancement of cognitive wisdom could prevent cognitive biases, reflective wisdom could improve the self-reflection, and affective wisdom may boost one’s empathy and compassion and finally improve social cognition and function. Works examining these promising hypotheses are highly recommended to lower the debilitating burden of full-onset psychosis to the individual family and to society as a whole.
Finally, our results should be interpreted with several limitations. First, the cross-sectional design limited the conclusion of causal relationship, and further cohort studies following the outcomes of individuals with different levels of wisdom is recommended. Second, the convenience sampling method may incur bias and have less generalizability. For instance, we recruited more females possibly because women are more likely to seek mental health services and participate in psychiatric studies (60, 61). Thus, works using probability sampling (62) to target more representative population are warranted. Third, the sample size of participants with high-level PLEs are relatively modest, future replication in larger population is also needed. Lastly, wisdom may be taken in a different manner since a previous work failed to replicate the three-dimension structure of 3D-WS-12 (63), thus, the interpretation of our results should be cautious, and further validation of three-dimensional wisdom structure is warranted to get a better understanding of its utility in Chinese culture.
Together, our work investigated the association between wisdom and PLEs for the first time, finding that wisdom ameliorated the frequency/distress of PLEs, and attenuated the distress associated with PLEs. Our findings have good implications for clinical practice since wisdom serves as a protective role for PLEs and could be a promising target in preventing the transition from high-risk state to full-blown psychosis.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of The Second Xiangya Hospital of Central South University. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
ZL, YL, and ZWu designed the study. ZJ, FW, ZWa, and YJ collected the data and double-checked the data input. ZWu and XS finished the statistical analysis and drafted the manuscript. ZL, YL, ZJ, and BR revised the manuscript. All authors agreed on the final version of the manuscript.
This work was supported by the National Natural Science Foundation of China (Grant Number 82071506 to ZL) and the Natural Science Foundation of Hunan Province, China (2021JJ40851 to YL).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all volunteers and participants for their contribution to this work.
1. Bangen KJ, Meeks TW, Jeste DV. Defining and assessing wisdom: a review of the literature. Am J Geriatr Psychiatry. (2013) 21:1254–66. doi: 10.1016/j.jagp.2012.11.020
2. Baltes PB, Staudinger UM. Wisdom: a metaheuristic (pragmatic) to orchestrate mind and virtue toward excellence. Am Psychol. (2000) 55:122–36. doi: 10.1037//0003-066x.55.1.122
3. Clayton V. Wisdom and intelligence: the nature and function of knowledge in the later years. Int J Aging Hum Dev. (1982) 15:315–21. doi: 10.2190/17tq-bw3y-p8j4-tg40
4. Sternberg JR. A balance theory of wisdom. Rev Gen Psychol. (1998) 2:347–65. doi: 10.1037/1089-2680.2.4.347
5. Josefsson K, Cloninger CR, Hintsanen M, Jokela M, Pulkki-Råback L, Keltikangas-Järvinen L. Associations of personality profiles with various aspects of well-being: a population-based study. J Affect Disord. (2011) 133:265–73. doi: 10.1016/j.jad.2011.03.023
6. Ardelt M. Empirical assessment of a three-dimensional wisdom scale. Res Aging. (2003) 25:275–324.
7. Chen H, Wang F. Wisdom: structure, category, measurement, and relationships to related variables. Adv Psychol Sci. (2013) 21:108–17. doi: 10.3724/sp.j.1042.2013.00108
8. Jeste DV, Vahia IV. Comparison of the conceptualization of wisdom in ancient Indian literature with modern views: focus on the Bhagavad Gita. Psychiatry. (2008) 71:197–209. doi: 10.1521/psyc.2008.71.3.197
9. Staudinger UM, David FL, Paul BB. The psychometric location of wisdom-related performance: intelligence, personality, and more?. Pers Soc Psychol Bull. (1997) 23:1200–14. doi: 10.1177/01461672972311007
10. Webster JD. An exploratory analysis of a self-assessed wisdom scale. J Adult Dev. (2003) 10:13–22.
11. Thomas ML, Bangen KJ, Palmer BW, Sirkin Martin A, Avanzino JA, Depp CA. A new scale for assessing wisdom based on common domains and a neurobiological model: the San Diego Wisdom Scale (SD-WISE). J Psychiatr Res. (2019) 108:40–7. doi: 10.1016/j.jpsychires.2017.09.005
12. Thomas ML, Bangen KJ, Ardelt M, Jeste DV. Development of a 12-item abbreviated three-dimensional wisdom scale (3D-WS-12): item selection and psychometric properties. Assessment. (2015) 24:71–82.
13. Webster JD, Westerhof GJ, Bohlmeijer ET. Wisdom and mental health across the lifespan. J Gerontol B Psychol Sci. (2014) 69:209–18. doi: 10.1093/geronb/gbs121
14. Ardelt M, Jeste DV. Wisdom and hard times: the ameliorating effect of wisdom on the negative association between adverse life events and well-being. J Gerontol B Psychol Sci. (2018) 73:1374–83. doi: 10.1093/geronb/gbw137
15. Bergsma A, Ardelt M. Self-reported wisdom and happiness: an empirical investigation. J Happiness Stud. (2012) 13:481–99. doi: 10.1007/s10902-011-9275-5
16. Ardelt M. Antecedents and effects of wisdom in old age: a longitudinal perspective on aging well. Res Aging. (2000) 22:360–94. doi: 10.1177/0164027500224003
17. Lee EE, Lee EE, Depp C, Palmer BW, Glorioso D, Daly R, et al. High prevalence and adverse health effects of loneliness in community-dwelling adults across the lifespan: role of wisdom as a protective factor. Int Psychogeriatr. (2019) 31:1447–62. doi: 10.1017/S1041610218002120
18. Kelleher I, Cannon M. Psychotic-like experiences in the general population: characterizing a high-risk group for psychosis. Psychol Med. (2011) 41:1–6. doi: 10.1017/S0033291710001005
19. Kelleher I, Connor D, Clarke MC, Devlin N, Harley M, Cannon M. Prevalence of psychotic symptoms in childhood and adolescence: a systematic review and meta-analysis of population-based studies. Psychol Med. (2012) 42:1857–63. doi: 10.1017/S0033291711002960
20. Van Os J, Hanssen M, Bijl RV, Ravelli A. Strauss (1969) revisited: a psychosis continuum in the general population?. Schizophr Res. (2000) 45:11–20. doi: 10.1016/s0920-9964(99)00224-8
21. Van Os J, Linscott RJ, Myin-Germeys I, Delespaul P, Krabbendam L. A systematic review and meta-analysis of the psychosis continuum: evidence for a psychosis proneness-persistence-impairment model of psychotic disorder. Psychol Med. (2009) 39:179–95. doi: 10.1017/S0033291708003814
22. Yung AR, Nelson B, Baker K, Buckby JA, Baksheev G, Cosgrave EM. Psychotic-like experiences in a community sample of adolescents: implications for the continuum model of psychosis and prediction of schizophrenia. Aust N Z J Psychiatry. (2009) 43:118–28. doi: 10.1080/00048670802607188
23. Poulton R, Caspi A, Moffitt TE, Cannon M, Murray R, Harrington H. Children’s self-reported psychotic symptoms and adult schizophreniform disorder: a 15-year longitudinal study. Arch Gen Psychiatry. (2000) 57:1053–8. doi: 10.1001/archpsyc.57.11.1053
24. Wu Z, Liu Z, Zou Z, Wang F, Zhu M, Zhang W, et al. Changes of psychotic-like experiences and their association with anxiety/depression among young adolescents before COVID-19 and after the lockdown in China. Schizophr Res. (2021) 237:40–6. doi: 10.1016/j.schres.2021.08.020
25. Armando M, Nelson B, Yung AR, Ross M, Birchwood M, Girardi P, et al. Psychotic-like experiences and correlation with distress and depressive symptoms in a community sample of adolescents and young adults. Schizophr Res. (2010) 119:258–65. doi: 10.1016/j.schres.2010.03.001
26. Chan SKW, Lee KKW, Chan VHY, Pang HH, Wong CSM, Hui CLM, et al. The 12-month prevalence of psychotic experiences and their association with clinical outcomes in Hong Kong: an epidemiological and a 2-year follow up studies. Psychol Med. (2020) 51:2501–8. doi: 10.1017/S0033291720001452
27. Yamasaki S, Usami S, Sasaki R, Koike S, Ando S, Kitagawa Y, et al. The association between changes in depression/anxiety and trajectories of psychotic-like experiences over a year in adolescence. Schizophr Res. (2018) 195:149–53. doi: 10.1016/j.schres.2017.10.019
28. Stochl J, Khandaker GM, Lewis G, Perez J, Goodyer IM, Zammit S, et al. Mood, anxiety and psychotic phenomena measure a common psychopathological factor. Psychol Med. (2015) 45:1483–93. doi: 10.1017/S003329171400261X
29. Livet A, Navarri X, Potvin S, Conrod P. Cognitive biases in individuals with psychotic-like experiences: a systematic review and a meta-analysis. Schizophr Res. (2020) 222:10–22. doi: 10.1016/j.schres.2020.06.016
30. Gawęda Ł, Prochwicz K. A comparison of cognitive biases between schizophrenia patients with delusions and healthy individuals with delusion-like experiences. Eur Psychiatry. (2015) 30:943–9. doi: 10.1016/j.eurpsy.2015.08.003
31. Cicero DC, Cohn JR. The role of ethnic identity, self-concept, and aberrant salience in psychotic-like experiences. Cultur Divers Ethnic Minor Psychol. (2018) 24:101–11. doi: 10.1037/cdp0000160
32. Dudley R, Taylor P, Wickham S, Hutton PJSB. Psychosis, delusions and the “jumping to conclusions” reasoning bias: a systematic review and meta-analysis. Schizophr Bull. (2016) 42:652–65. doi: 10.1093/schbul/sbv150
33. McLean BF, Mattiske JK, Balzan RP. Association of the jumping to conclusions and evidence integration biases with delusions in psychosis: a detailed meta-analysis. Schizophr Bull. (2017) 43:344–54. doi: 10.1093/schbul/sbw056
34. Woodward TS, Moritz S, Menon M, Klinge RJCN. Belief inflexibility in schizophrenia. Cogn Neuropsychiatry. (2008) 13:267–77. doi: 10.1080/13546800802099033
35. Janssen I, Versmissen D, Campo J, Myin-Germeys I, Van Os J, Krabbendam LJPM. Attribution style and psychosis: evidence for an externalizing bias in patients but not in individuals at high risk. Psychol Med. (2006) 36:771–8. doi: 10.1017/S0033291706007422
36. Glenthøj LB, Fagerlund B, Hjorthøj C, Jepsen JRM, Bak N, Kristensen TD, et al. Social cognition in patients at ultra-high risk for psychosis: what is the relation to social skills and functioning? Schizophr Res Cogn. (2016) 5:21–7. doi: 10.1016/j.scog.2016.06.004
37. Osborne KJ, Willroth EC, Devylder JE, Mittal VA, Hilimire MR. Investigating the association between emotion regulation and distress in adults with psychotic-like experiences. Psychiatry Res. (2017) 256:66–70. doi: 10.1016/j.psychres.2017.06.011
38. Elfil M, Negida A. Sampling methods in clinical research; an educational review. Emergency. (2017) 5:e52.
39. Liu J, Chen H. The relationship between wisdom and happiness in college students. Campus Life Ment Health. (2017) 15:323–7.
40. Capra C, Kavanagh DJ, Hides L, Scott J. Brief screening for psychosis-like experiences. Schizophr Res. (2013) 149:104–7. doi: 10.1016/j.schres.2013.05.020
41. Sun M, Wang D, Jing L, Xi C, Dai L, Zhou L. Psychometric properties of the 15-item positive subscale of the community assessment of psychic experiences. Schizophr Res. (2020) 222:160–6. doi: 10.1016/j.schres.2020.06.003
42. Bukenaite A, Stochl J, Mossaheb N, Schäfer MR, Klier CM, Becker J, et al. Usefulness of the CAPE-P15 for detecting people at ultra-high risk for psychosis: psychometric properties and cut-off values. Schizophr Res. (2017) 189:69–74. doi: 10.1016/j.schres.2017.02.017
43. Hayes A. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling. (2012). Available online at: https://www.semanticscholar.org/paper/PROCESS-%3A-A-Versatile-Computational-Tool-for-%2C-%2C-1-Hayes/aa753b543c78d6c4f344fb431c6683edaa062c07
44. Wu Z, Zou Z, Wang F, Xiang Z, Zhu M, Long Y, et al. Family functioning as a moderator in the relation between perceived stress and psychotic-like experiences among adolescents during COVID-19. Compr Psychiatry. (2021) 111:152274. doi: 10.1016/j.comppsych.2021.152274
46. Van Patten R, Lee EE, Daly R, Twamley E, Tu XM, Jeste DV. Assessment of 3-dimensional wisdom in schizophrenia: associations with neuropsychological functions and physical and mental health. Schizophr Res. (2019) 208:360–9. doi: 10.1016/j.schres.2019.01.022
47. Gawęda Ł, Pionke R, Arciszewska A, Prochwicz K, Frydecka D, Misiak B, et al. A combination of self-disturbances and psychotic-like experiences. A cluster analysis study on a non-clinical sample in Poland. Psychiatry Res. (2019) 273:394–401. doi: 10.1016/j.psychres.2019.01.044
48. Cicero DC, Becker TM, Martin EA, Docherty AR, Kerns JG. The role of aberrant salience and self-concept clarity in psychotic-like experiences. Personal Disord. (2013) 4:33. doi: 10.1037/a0027361
49. So SH, Tang V, Leung PW. Dimensions of delusions and attribution biases along the continuum of psychosis. PLoS One. (2015) 10:e0144558. doi: 10.1371/journal.pone.0144558
50. Daalman K, Sommer I, Derks E, Peters EJPM. Cognitive biases and auditory verbal hallucinations in healthy and clinical individuals. Psychol Med. (2013) 43:2339–47. doi: 10.1017/S0033291713000275
51. Garety PA, Kuipers E, Fowler D, Freeman D, Bebbington PJPM. A cognitive model of the positive symptoms of psychosis. Psychol Med. (2001) 31:189–95. doi: 10.1017/s0033291701003312
52. Mækelæ MJ, Moritz S, Pfuhl G. Are Psychotic Experiences Related to Poorer Reflective Reasoning?. Front Psychol. (2018) 9:122. doi: 10.3389/fpsyg.2018.00122
53. Modinos G, Renken R, Ormel J, Aleman A. Self-reflection and the psychosis-prone brain: an fMRI study. Neuropsychology. (2011) 25:295–305. doi: 10.1037/a0021747
54. Amador XF, David AS. Insight and Psychosis: Awareness of Illness in Schizophrenia and Related Disorders. Oxford: Oxford University Press (2004).
55. Van Der Meer L, De Vos AE, Stiekema APM, Pijnenborg GHM, Van Tol M-J, Nolen WA. Insight in Schizophrenia: involvement of Self-Reflection Networks? Schizophr Bull. (2013) 39:1288–95. doi: 10.1093/schbul/sbs122
56. Derntl B, Michel TM, Prempeh P, Backes V, Finkelmeyer A, Schneider F, et al. Empathy in individuals clinically at risk for psychosis: brain and behaviour. Br J Psychiatry. (2015) 207:407–13. doi: 10.1192/bjp.bp.114.159004
57. Prochwicz K, Kłosowska J. The moderating role of cognitive biases on the relationship between negative affective states and psychotic-like experiences in non-clinical adults. Psychiatry Res. (2018) 265:118–27. doi: 10.1016/j.psychres.2018.04.023
58. Lee EE, Bangen KJ, Avanzino JA, Hou B, Ramsey M, Eglit G, et al. Outcomes of randomized clinical trials of interventions to enhance social, emotional, and spiritual components of wisdom: a systematic review and meta-analysis. JAMA Psychiatry. (2020) 77:925–35. doi: 10.1001/jamapsychiatry.2020.0821
59. Adler AB, Williams J, Mcgurk D, Moss A, Bliese PD. Resilience training with soldiers during basic combat training: randomisation by platoon. Appl Psychol Health Well Being. (2015) 7:85–107. doi: 10.1111/aphw.12040
60. Galdas PM, Cheater F, Marshall P. Men and health help-seeking behaviour: literature review. J Adv Nurs. (2005) 49:616–23. doi: 10.1111/j.1365-2648.2004.03331.x
61. Woodall A, Morgan C, Sloan C, Howard L. Barriers to participation in mental health research: are there specific gender, ethnicity and age related barriers?. BMC Psychiatry. (2010) 10:103. doi: 10.1186/1471-244X-10-103
62. Taherdoost H. Sampling Methods in Research Methodology; How to Choose a Sampling Technique for Research. Int J Acad Res. (2016) 5:18–27.
Keywords: wisdom, psychotic-like experiences, mental health, psychosis prevention, epidemiology
Citation: Wu Z, Jiang Z, Wang Z, Ji Y, Wang F, Ross B, Sun X, Liu Z and Long Y (2022) Association Between Wisdom and Psychotic-Like Experiences in the General Population: A Cross-Sectional Study. Front. Psychiatry 13:814242. doi: 10.3389/fpsyt.2022.814242
Received: 13 November 2021; Accepted: 11 March 2022;
Published: 18 April 2022.
Edited by:
Giorgio Di Lorenzo, Tor Vergata University of Rome, ItalyReviewed by:
Michel Ferrari, University of Toronto, CanadaCopyright © 2022 Wu, Jiang, Wang, Ji, Wang, Ross, Sun, Liu and Long. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yicheng Long, eWljaGVuZ2xvbmdAY3N1LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.