 Falk W. Lohoff
Falk W. Lohoff
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Psychiatry , 09 June 2022
Sec. Addictive Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.767506
This article is part of the Research Topic Molecular Aspect of Alcohol Addiction and its Comorbidities with Affective Disorders View all 6 articles
Alcohol Use Disorder (AUD) is a chronic psychiatric disorder marked by impaired control over drinking behavior that poses a significant challenge to the individual, their community, the healthcare system and economy. While the negative consequences of chronic excessive alcohol consumption are well-documented, effective treatment for AUD and alcohol-associated diseases remains challenging. Cognitive and behavioral treatment, with or without pharmaceutical interventions, remain the most commonly used methods; however, their efficacy is limited. The development of new treatment protocols for AUD is challenged by difficulty in accurately measuring patterns of alcohol consumption in AUD patients, a lack of a clear understanding of the neuropsychological basis of the disorder, the high likelihood of AUD patients relapsing after receiving treatment, and the numerous end-organ comorbidities associated with excessive alcohol use. Identification and prediction of patients who may respond well to a certain treatment mechanism as well as clinical measurement of a patient's alcohol exposure are bottlenecks in AUD research which should be further addressed. In addition, greater focus must be placed on the development of novel strategies of drug design aimed at targeting the integrated neural pathways implicated in AUD pathogenesis, so that next-generation AUD treatment protocols can address the broad and systemic effects of AUD and its comorbid conditions.
Alcohol use disorder (AUD) is a common chronic disorder that is estimated to account for approximately 5% of the global disease burden (1, 2), an estimated 3.8% of global deaths (3), and which is associated with 88,000 deaths annually in the United States (4). AUD is also associated with several psychiatric and physical comorbidities and represents a high cost to society, estimated at ~$250 billion a year in the United States (5). The 12 month prevalence for AUD ranges from 5 to 14%, (6–8) and despite this high occurrence, significant unmet clinical needs exist in the management of AUD. Current medical treatment protocols have only limited efficacy in reducing the burden of the disorder. Further, AUD is a highly comorbid disorder, with strong associations between other psychiatric and downstream physical conditions. Treatment of AUD must therefore incorporate treatment for the systemic effects of the disorder and not simply the behavioral aspects of addiction or dependence. Addressing these critical needs is important to reduce overall illness associated morbidity and mortality. This article will succinctly review and summarize key unmet needs in AUD.
AUD is commonly treated with cognitive or behavioral interventions, pharmacological treatment, or a combination of these. The U.S. Food and Drug Administration (FDA) has approved three medications for the treatment of AUD expressly: disulfiram, acamprosate, and naltrexone, including an injectable form of naltrexone. Additionally, several drugs have been used off-label to treat AUD, such as topiramate, gabapentin, baclofen, ondansetron, and varenicline, among others (9). While these drugs have been used to treat AUD, and some patients do respond well to treatment, their efficacy is limited and none have been demonstrated to systematically and dramatically outperform placebo in reducing AUD symptoms, with many studies reporting a positive effect finding statistically significant but small effect sizes (10–13). Some studies have suggested that topiramate might outperform placebo in reducing drinking and craving, but the effect was minimal and not indicative of significant clinical potential (12, 14). The best support for effective pharmacological treatment of AUD exists currently for naltrexone and acamprosate, although meta-analyses of randomized double-blind placebo-controlled trials (RCTs) of those drugs found that in 40% to 70% of individuals taking either medication, there were no measurable positive outcomes, a finding not unusual for psychiatric mediations (12, 13, 15–17).
AUD patients' response to pharmacological treatment is also considerably heterogeneous, and clinical, environmental, genetic, and social factors can all contribute to variance in drug response in patients. Patients can exhibit varying degrees of clinical response and side effects, even to the same dose of the same drug, and some patients may respond very well to one treatment protocol but poorly to another. How success is defined in the context of pharmacological treatment also impacts the reported efficacy of different treatments. For instance, certain drugs may promote abstinence from drinking, while others may reduce the incidence of heavy drinking or end-organ comorbidities (18). Identifying what external factors may mediate patients' response to specific medicines remains a key challenge in the development of efficacious treatment for AUD.
In addition to pharmacological treatment, several options exist for psychotherapy or non-pharmacological treatments, such as individual psychotherapy, Cognitive-Behavioral Therapy (CBT), and 12-step facilitation groups including Alcoholics Anonymous (AA). Pharmacological and non-pharmacological interventions which have been assessed for use in treating AUD are summarized in Table 1. These interventions can be administered at the individual or group level and can help address problematic drinking by targeting maladaptive thought and behavior patterns or environmental triggers. Overall, studies have found psychological interventions for AUD to be somewhat effective compared to nonspecific controls, but also generally report that effect sizes are small, they do not work for all patients, and are no more effective than current pharmacological options (19, 20).
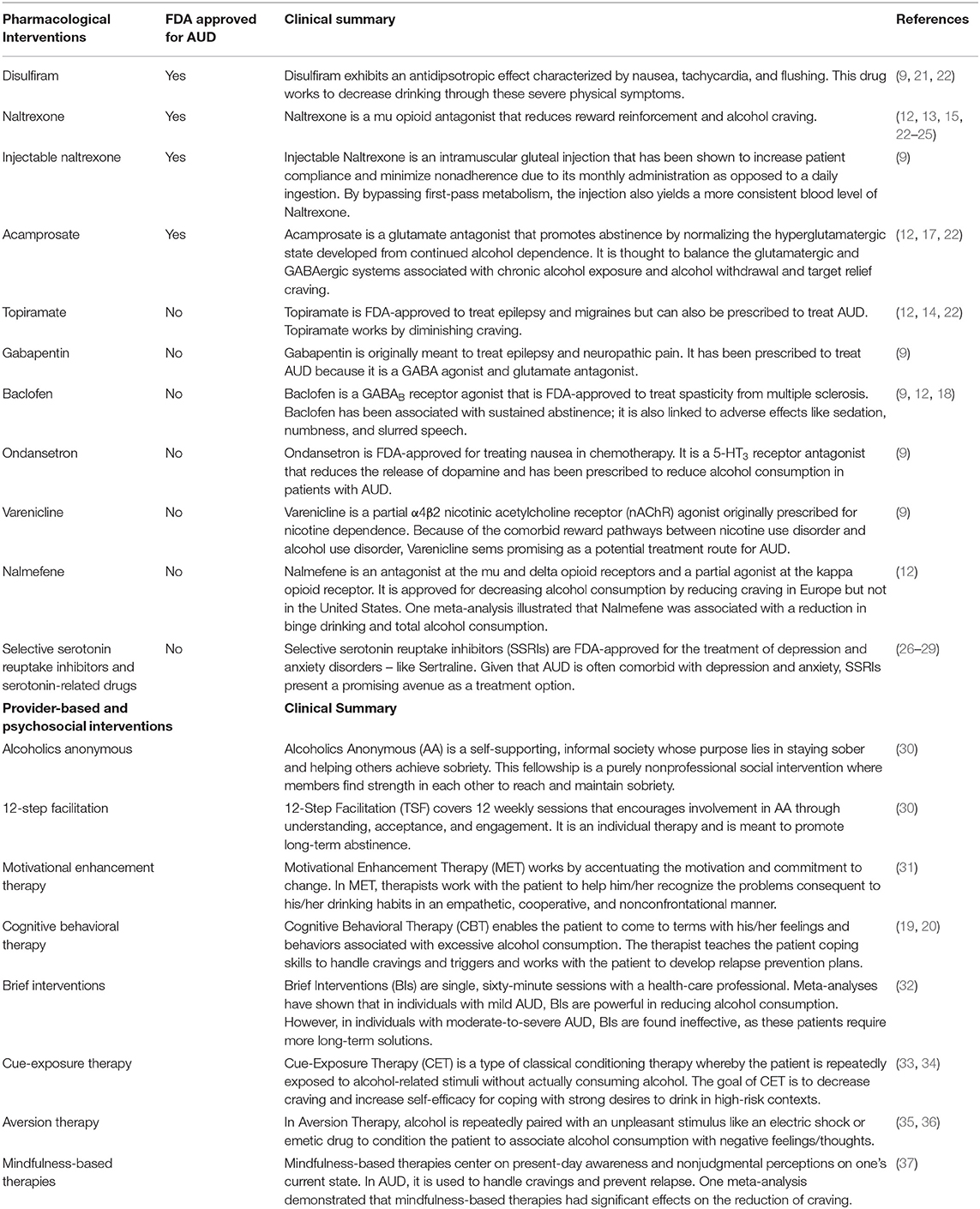
Table 1. Summary of currently available pharmacological and psychosocial interventions of AUD.
Behavioral interventions can be used as standalone treatment or in conjunction with pharmacological treatment, and while there is some evidence for their efficacy as a standalone treatment, research suggests that the greatest efficacy results from a combination of pharmacological and non-pharmacological treatment (19, 38, 39). The COMBINE study recruited 1383 recently alcohol-abstinent patients with primary alcohol dependence diagnoses and found that patients receving naltrexone, behavioral interventions, or both fared better on drinking outcomes, while acamprosate was ineffective with or without cognitive intervention (23). Interestingly, placebo pills and meetings with healthcare professionals both had a greater effect on drinking behavior than cognitive-behavioral approaches alone. The COMBINE study highlights the immense variation in responses to both behavioral and pharmacological interventions for AUD, and underscores the importance of finding new, highly effective medications that work for large groups of patients. While some medication may be effective for certain patients, it is clear that current pharmacological interventions cannot address the immense heterogeneity in the clinical presentation of AUD patients.
Despite the high prevalence and associated adverse effects of AUD, less than 20% of individuals with the disorder get any treatment, and of those <10 percent (i.e., 2% overall) get pharmacological treatment. Only a fraction of patients receive subspecialty treatment (9, 40). Treatment for AUD frequently consists of specialized cognitive, behavioral, or pharmacological interventions, oftentimes in combinations (Table 1). However, current forms of AUD treatment have often shown limited success in randomized controlled trials (10, 11). It should be noted, however, that blinding factors may play a role in the outcomes of these studies; disulfiram, for example, was associated positively with abstinence and negatively with relapse in open-label studies (9). A meta-analysis of randomized controlled trials of disulfiram found that open-label studies alone reported significant effects compared to placebo, possibly due to patients' fear of adverse reactions (21).
In addition, most individuals with AUD first present to their general practitioner, but often do not have access to specialized addiction treatment (41, 42). This represents a missed opportunity to provide the best specialized care if clinically indicated. The National Institute of Alcohol Abuse and Alcoholism (NIAAA) is addressing this important aspect of access to care by providing information on available treatment options. The NIAAA Alcohol Treatment Navigator is an online tool that guides individuals toward evidence-based treatment from providers near their area; this is especially relevant because access to care is one of the main barriers to AUD treatment access (https://alcoholtreatment.niaaa.nih.gov/). The American College of Academic Addiction Medicine also offers fellowship programs and other training resources for clinicians to become trained and certified in addiction medicine. As AUD grows in prevalence and severity, it is all the more crucial for physicians to be able to recognize and effectively treat this patient population.
Like many other substance abuse and psychiatric disorders, treatment response to medication for AUD is heterogeneous; individual patients can exhibit divergent treatment responses and side effects when treated with the same drug, and even at the same dosage, with some patients responding favorably to one treatment but not another. The inability to identify prior to initiating treatment who will respond to and tolerate a chosen AUD medication often leads to a prescribing process of trial-and-error, adverse therapeutic outcomes, and unnecessary prolongation of AUD disease activity, which can promote the progression of comorbidities and negative health outcomes.
The promise of personalized medicine and pharmacogenomics brings the possibility of identifying a priori which drugs might work best for a specific individual with AUD (43). Pharmacogenomics refers to the testing of genetic markers (single nucleotide polymorphisms – SNPs) that can predict treatment response and adverse event profiles by altering pharmacokinetic and pharmacodynamic processes. While several products in the psychiatric space have claimed to offer improved targeting of initial medication choices based on pharmacogenetic testing profiles, current data in AUD does not support routine pharmacogenetic testing (44, 45). More AUD-specific genomic investigation is needed to determine whether any SNP drug targets have potential for targeted medications, which could allow for new, gene-specific mechanisms of pharmacological interventions.
Treatments for AUD rely on accurate measures of alcohol consumption and drinking behaviors. Researchers have broadly utilized retrospective self-report evaluations like the Timeline Follow-Back (TLFB) to measure alcohol intake and patterns. While the TLFB has been linked to valid assessments of short and long-term estimations of alcohol consumption, self-report evaluations tend to systematically underestimate drinking due to the unreliability of human memory, namely recall bias (46). Considering that participants using TLFB evaluations consistently underreport their drinking, the field should move toward more reliable objective measures to assess alcohol consumption (46). For example, daily drinking diaries can be used to decrease the amount of time for which participants must recall their drinking behavior relative to longer-term measurements such as the TLFB, which may improve participants' ability to accurately recall their drinking behavior. The advance of modern consumer technology and the proliferation of mobile devices such as smartphones has also enabled real-time self-report methods that can account for situational variables and may be more accurate than traditional memory-based recall measures such as the TLFB. These methods are part of the collective framework known as Ecological Momentary Assessment (EMA), which incorporates technology into self-report measures to allow for more accurate reports of drinking patterns in the short term (47). However, while these methods may be more valid than traditional recall questionnaires, they are still subject to inherent limitations of self-report assessments, including behavioral reactivity (i.e., the “observer effect”) and a reliance on participant compliance (47). Real-time daily assessments for alcohol consumption using biosensors that can continuously monitor alcohol levels may alleviate these concerns, and should be further explored as an objective assessment of drinking behavior (48). The use of objective alcohol consumption level monitoring could also improve efficiency and predictive validity in standard medication testing paradigms by providing detailed consumption data for outcome measures (48).
The heterogenic nature of AUD requires a multi-disciplinary treatment approach to address the many unmet medical needs among those with AUD. Current pharmacotherapies are often characterized by limited efficacy and fail to show promising results in clinical use (49). Further, the considerable heterogeneity of AUD patients makes it especially challenging to design a single drug capable of treating AUD patients as a whole. This inability of existing medications to effectively treat AUD illustrates the need to pursue new neuroscience-based pharmacotherapies that target the various neural and molecular pathways of addiction individually (49). These strategies may yield drugs which can target specific neurological AUD characteristics to more effectively treat individual patients.
Better understanding of the neurofunctional domains underlying AUD by assessing severity, modeling heterogeneity, predicting course, and targeting treatments can lead to improved medications (50). Previous studies have mainly focused on single domains of function such as cognitive control or social/emotional processing. A comprehensive framework can capture essential factors of neuropsychological functioning in people with varying degrees of AUD, which is crucial for developing effective treatments.
Kwako et al. (50) developed the Addictions Neuroclinical Assessment (ANA), a neuroscience-based framework that proposes that 3 domains are implicated in substance use disorders: incentive salience, negative emotionality, and executive function. These 3 neurofunctional factors are interrelated because of their shared underlying neural circuitry and shared genetic and environmental risk factors.
The incentive salience construct refers to the psychological “wanting” that is driven by both physiological factors and learned associations about a reward cue, prompting compulsive habits (51). Cue exposure is related to increased craving and changes in the neural reward system, facilitating chemical dependence (52). In AUD, factors like depression, trait anxiety scores, and items from the Obsessive Compulsive Drinking Scale load onto the incentive salience domain (50).
The negative emotionality domain, which proposes that a decrease in negative affect drives excessive alcohol consumption, encompasses markers including increased scores in neuroticism, aggression, trait anxiety, and overall difficulties in emotion regulation, which are often exhibited by AUD patients (50). As in the incentive salience factor, craving also maps onto negative emotionality; the desire to avoid withdrawal is mediated by the associated negative affect. More specifically, it is believed that individuals with AUD drink for the sole purpose of avoiding the negative emotionality states associated with withdrawal shifting from pleasant feelings following consumption to feelings of relief instead (52).
Finally, the executive function domain encompasses the higher-order mental processes involved in cognitive control and future planning. Subdomains in this field relevant for addiction include items like response inhibition, working memory, impulsivity, and premeditation (50, 51). Inefficient executive cognitive functioning puts the maintenance of abstinence at risk, thereby increasing the likelihood of relapse.
Using an extensive range of scales and neuropsychological tests, it was found that these 3 neurofunctional domains differ between individuals with and without AUD, which further accentuates the pertinence of these factors for addiction (50). Other authors have analyzed the ANA framework and found that it can inform alcohol-specific outcomes and treatments; classifying patient groups using ANA-like qualitative classifications can serve as a useful mechanism for predicting drug efficacy (53). The negative functionality domain, in particular, was associated with drinking intensity at 12 months and coping motives at 6 months post-treatment for AUD (54). While more work is needed to conclude the extent to which the ANA framework can effectively predict treatment outcomes or identify treatment responders or nonresponses, it is a useful tool for informing hypotheses for ongoing drug and clinical research.
At present, medication development for AUD is marked by slow pace and high costs due to the failure of many compounds to succeed in clinical trials. Despite exploring potential molecular targets, many studies report little to no effect sizes using these medications. Therefore, novel strategies are needed to identify new treatments that address how the target interacts with other pathways and mechanisms. One such method focuses on the integration of biomolecular and cellular networks that are imperative for detecting multiple targets that drive AUD (55). By evaluating how these networks are connected in the neurocircuits integral to the underlying domains of AUD, researchers can formulate better therapies through a multi-disciplinary approach.
Chronic AUD is a progressive neurodegenerative disease with no definitive cure. Even with the few approved psychotropic medications, many people still suffer from AUD due to factors like social stigma, expense, and transient effects of currently available pharmacotherapy. For instance, a multivariate meta-analysis of 41 pharmacotherapy trials conducted from 1992 to 2009 found that the effect size for naltrexone, one of the FDA approved drugs, has steadily diminished in promoting abstinence and reducing heavy drinking since the earliest studies (56).
Some studies have found that pharmacological interventions are effective in reducing drinking behavior in AUD patients, with certain medications generally promoting certain improved outcomes. The Alcohol Clinical Trials Initiative (ACTIVE) workgroup and its members have reviewed clinical trials of AUD medications and found that some drugs are effective for certain patient populations (57). For instance, disulfiram has been found by some open-label studies to reduce drinking, and while the results of clinical trials investigating acamprosate have been mixed, it may be more effective in preventing relapse among detoxified patients than reducing drinking for general AUD patients (22). Similarly, naltrexone may be more effective in reducing relapse to heavy drinking than in promoting abstinence (22, 24, 25, 58). Further, while these medications have been found to help reduce AUD symptoms in some people and trials, no medication has been shown to work consistently and with large effect sizes across patient groups; future drug discovery efforts should seek to identify novel compounds and drug targets with large effect sizes and which are easier to use clinically (55, 58).
Relapse also complicates AUD treatment; studies of relapse rates in AUD patients and in studies of different interventions have yielded varying estimates on the prevalence and significance of relapse. Some studies indicate that between 20 and 80% of individuals who receive treatment and experience short-term remission are expected to relapse long-term (59). Other authors have argued that relapse is not absolute; the rate of reported relapse is substantially heterogeneous and can be influenced by demographics, framing, and interpretation of data (60, 61). Moreover, many study designs, particularly randomized controlled trials, do not typically assess long-term outcomes, such as total reduction in drinking behavior over several years and improvement of comorbid symptoms. Further research is needed to clearly establish the role of current pharmacological interventions in treating AUD in the long term. With such high relapse-rates, AUD is in critical need of effective and long-lasting therapeutic interventions so that people who do pursue treatment can continue to manage their condition after the initial treatments have run their course.
Besides being a complex substance use disorder itself, AUD is highly comorbid with other psychiatric disorders, including major depressive disorder (MDD) and anxiety disorders (62–64). A diagnosis of MDD or an anxiety disorder increases the likelihood of developing AUD (65) and common underlying biological and/or genetic factors are suspected to play a role in these relationships (66, 67). Identification of common predispositional genetic factors is crucial for the development of novel treatments for AUD, MDD, and/or anxiety (26).
One-third of AUD individuals also exhibit depressive symptoms (27). Selective serotonin reuptake inhibitors (SSRIs) are widely used to treat depression, and while clinical trials have examined their efficacy in treating comorbid AUD, these trials have failed to find a clinically significant effect. Sertraline, an FDA-approved SSRI for the treatment of depression, was associated with lowered alcohol consumption compared to placebo, but there was no difference in other drinking measures (28). A later study found no significant effect of sertraline on depressive symptoms or alcohol consumption (68). However, it has been reported that a combination of sertraline and naltrexone may have a significant effect on AUD-depression comorbidity; a treatment group receiving both medications exhibited a greater rate of abstinence from alcohol, greater time to relapse in heavy drinking, less depressive symptoms, and fewer adverse events compared to other treatment groups (69). The presentation of AUD patients varies considerably due to individual-level differences, and combining medications that target different domains of neuropsychiatric impairment may increase the therapeutic effect of a medication regiment while also allowing for effective treatment of a wider range of patients.
Comorbid anxiety disorders, including generalized anxiety disorder (GAD), panic disorder (PD), social phobia, specific phobia, post-traumatic stress disorder (PTSD), and obsessive-compulsive disorder (OCD), occur in approximately 5 to 30% of AUD patients. Conversely, among anxiety disorder patients, the prevalence of AUD ranges from 7 to 10%, with approximately 50% of patients using alcohol to self-medicate their anxiety symptoms (29). Further, a diagnosis of an anxiety disorder predicts development of AUD in patients non-pathologically misusing alcohol, and AUD diagnosis predicts GAD and SP diagnoses and onset of PD (29). Studies of sertraline in comorbid PTSD/AUD patients found that sertraline may have a limited effect on a small subset of patients, but could not conclude an overall beneficial effect (70). Further studies failed to find significant reduction in comorbid symptoms in patients treated with SSRIs or norepinephrine reuptake inhibitors (71). However, there is considerable heterogeneity in the clinical presentation of individuals suffering from AUD and comorbid psychiatric disorders, and different patterns of diagnoses necessitate different treatment options. Long-term studies with more complex statistical models are needed in order to better estimate the potential of pharmacological interventions for treating AUD and comorbid diagnoses together. Addressing both AUD and its comorbid psychiatric disorders is crucial in alleviating alcohol-associated pathologies and to achieve better treatment outcomes.
Approximately 50% of all liver disease mortality is currently attributable to alcohol misuse (72–76), yet there are no FDA approved treatment options for alcohol-associated liver disease (ALD). ALD causes significant morbidity and mortality and is the leading cause of cirrhosis, liver cancer, and acute/chronic liver failure (72–76). Although the pathophysiology of ALD is clearly linked to excessive alcohol consumption, the exact mechanisms remain elusive and span domains of behavior as well as environmental, genetic and epigenetic factors (77, 78). Treatment options for ALD are limited and ultimately include abstinence from alcohol – a goal that is difficult to achieve for most individuals with ALD and/or AUD. Presently, there are only limited pharmacological treatment options available for ALD, which, depending on the degree of liver damage, may include corticosteroids, pentoxifylline and N-acetylcysteine (79–84). Once liver damage progresses to cirrhosis, liver transplant is often the only option. Given the large unmet clinical need for effective new pharmacological interventions for ALD, innovative approaches to identify novel targets and treatments are needed (85). Similarly, alcohol can damage the cardiovascular, metabolic, and gastrointestinal systems and lead to various cancers, all of which contribute significantly to the overall morbidity and mortality of AUD. Given this, pharmacological treatment of AUD cannot be developed isolated from related downstream organ systems affected by alcohol metabolism and comorbidities. Coordination of care between medical specialties is necessary to provide individuals suffering from AUD/ALD integrative care to maximize preventive measures and to minimize adverse health outcomes.
There is also the issue of patient treatment goals and the role of end-organ function and harm reduction endpoints in defining therapeutic success for individual patients. While many clinical trials of new medications and treatment programs for AUD use abstinence as a primary outcome measure, an excessive focus on abstinence as the only relevant outcome for AUD treatment could overshadow treatments that tangibly reduce the harmful physiological effects of drinking; this may also partially explain the failure of several clinical trials despite robust preclinical findings indicating potential in human subjects (86–88). Many treatments are available which facilitate some degree of drinking behavior symptom improvement, and several other medications can treat downstream, end-organ damage resulting from drinking, and these drugs should be given appropriate attention by researchers and clinicians to improve patient outcome when abstinence cannot be achieved.
AUD is a chronic, often disabling disease with significant morbidity and mortality. Despite non-pharmacological and pharmacological treatment options, most individuals with AUD don't achieve their therapeutic goals, often due to limited efficacy of available treatments. New efforts using precision medicine approaches and novel molecular-based drug discovery efforts are needed to address the complex nature of AUD and its associated psychiatric and end-organ comorbidities.
FL designed, drafted, and wrote the manuscript.
This work was supported by the National Institutes of Health (NIH) intramural funding [ZIA-AA000242 to FL]; Division of Intramural Clinical and Biological Research of the National Institute on Alcohol Abuse and Alcoholism (NIAAA).
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The author thanks Andrew Bell, Joyce Yoo, and Diane Cooper for helpful comments and editing of the manuscript.
1. Alcohol GBD and CDrug Use. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry. (2018) 5: 987–1012. doi: 10.1016/S2215-0366(18)30337-7
2. G. B. D. A. Collaborators. Alcohol use and burden for 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. (2018) 392:1015–1035. doi: 10.1016/s0140-6736(18)31310-2
3. Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet. (2009) 373:2223–33. doi: 10.1016/S0140-6736(09)60746-7
4. Gonzales K, Roeber J, Kanny D, Tran A, Saiki C, Johnson H, et al., C. Centers for Disease and Prevention. Alcohol-attributable deaths and years of potential life lost−11 States, 2006-2010. MMWR Morb Mortal Wkly Rep. (2014) 63:213–6.
5. Sacks JJ, Gonzales KR, Bouchery EE, Tomedi LE, Brewer RD. 2010 National and state costs of excessive alcohol consumption. Am J Prev Med. (2015) 49:e73–9. doi: 10.1016/j.amepre.2015.05.031
6. Grant BF, Hasin DS, Chou SP, Stinson FS, Dawson DA. Nicotine dependence and psychiatric disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions. Arch Gen Psychiatry. (2004) 61:1107–15. doi: 10.1001/archpsyc.61.11.1107
7. Grant BF, Goldstein RB, Saha TD, Chou SP, Jung J, Zhang H, et al. Epidemiology of DSM-5 Alcohol Use Disorder: Results From the National Epidemiologic Survey on Alcohol and Related Conditions III. JAMA Psychiatry. (2015) 72:757–66. doi: 10.1001/jamapsychiatry.2015.0584
8. Grant BF, Chou SP, Saha TD, Pickering RP, Kerridge BT, Ruan WJ, et al. Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV Alcohol Use Disorder in the United States, 2001-2002 to 2012-2013: Results From the National Epidemiologic Survey on Alcohol and Related Conditions. JAMA Psychiatry. (2017) 74:911–23. doi: 10.1001/jamapsychiatry.2017.2161
9. Kranzler HR, Soyka M. Diagnosis and pharmacotherapy of alcohol use disorder: a review. JAMA. (2018) 320:815–24. doi: 10.1001/jama.2018.11406
10. Anton RF, Schacht JP, Book SW. Pharmacologic treatment of alcoholism. Handb Clin Neurol. (2014) 125:527–42. doi: 10.1016/B978-0-444-62619-6.00030-6
11. Muller CA, Geisel O, Banas R, Heinz A. Current pharmacological treatment approaches for alcohol dependence. Expert Opin Pharmacother. (2014) 15:471–81. doi: 10.1517/14656566.2014.876008
12. Palpacuer C, Duprez R, Huneau A, Locher C, Boussageon R, Laviolle B, et al. Pharmacologically controlled drinking in the treatment of alcohol dependence or alcohol use disorders: a systematic review with direct and network meta-analyses on nalmefene, naltrexone, acamprosate, baclofen and topiramate. Addiction. (2018) 113:220–37. doi: 10.1111/add.13974
13. Ray LA, Green R, Roche DJO, Magill M, Bujarski S. Naltrexone effects on subjective responses to alcohol in the human laboratory: a systematic review and meta-analysis. Addict Biol. (2019) 24:1138–52. doi: 10.1111/adb.12747
14. Blodgett JC, Del Re AC, Maisel NC, Finney JW. A meta-analysis of topiramate's effects for individuals with alcohol use disorders. Alcohol Clin Exp Res. (2014) 38:1481–8. doi: 10.1111/acer.12411
15. Srisurapanont M, Jarusuraisin N. Opioid antagonists for alcohol dependence. Cochrane Database Syst Rev. (2005) CD001867. doi: 10.1002/14651858.CD001867.pub2
16. Rosner S, Hackl-Herrwerth A, Leucht S, Vecchi S, Srisurapanont M, Soyka M. Opioid antagonists for alcohol dependence. Cochrane Database Syst Rev. (2010) CD001867. doi: 10.1002/14651858.CD001867.pub3
17. Rosner S, Hackl-Herrwerth A, Leucht S, Lehert P, Vecchi S, Soyka M. Acamprosate for alcohol dependence. Cochrane Database Syst Rev. (2010) CD004332 doi: 10.1002/14651858.CD004332.pub2
18. Kumar A, Sharma A, Bansal PD, Bahetra M, Gill HK, Kumar R, et al. comparative study on the safety and efficacy of naltrexone versus baclofen versus acamprosate in the management of alcohol dependence. Indian J Psychiatry. (2020) 62:650–8. doi: 10.4103/psychiatry.IndianJPsychiatry_201_19
19. Magill M, Ray L, Kiluk B, Hoadley A, Bernstein M, Tonigan JS, et al. meta-analysis of cognitive-behavioral therapy for alcohol or other drug use disorders: treatment efficacy by contrast condition. J Consult Clin Psychol. (2019) 87:1093–105. doi: 10.1037/ccp0000447
20. Kiluk BD, Ray LA, Walthers J, Bernstein M, Tonigan JS, Magill M. Technology-delivered cognitive-behavioral interventions for alcohol use: a meta-analysis. Alcohol Clin Exp Res. (2019) 43:2285–95. doi: 10.1111/acer.14189
21. Skinner MD, Lahmek P, Pham H, Aubin HJ. Disulfiram Efficacy in the treatment of alcohol dependence: a meta-analysis. PLoS ONE. (2014) 9:e87366. doi: 10.1371/journal.pone.0087366
22. Leggio L, Falk DE, Ryan ML, Fertig J, Litten RZ. Medication development for alcohol use disorder: A focus on clinical studies. In: Nader MA, Hurd YL, editors. Substance Use Disorders: From Etiology to Treatment. Cham: Springer International Publishing (2020).
23. Anton RF, O'Malley SS, Ciraulo DA, Cisler RA, Couper D, Donovan DM, et al. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial. JAMA. (2006) 295:2003–17. doi: 10.1001/jama.295.17.2003
24. Maisel NC, Blodgett JC, Wilbourne PL, Humphreys K, Finney JW. Meta-analysis of naltrexone and acamprosate for treating alcohol use disorders: when are these medications most helpful? Addiction (Abingdon, England). (2013) 108:275–93. doi: 10.1111/j.1360-0443.2012.04054.x
25. Mann K, Aubin HJ, Witkiewitz K. Reduced drinking in alcohol dependence treatment, what is the evidence? Eur Addict Res. (2017) 23:219–30. doi: 10.1159/000481348
26. Helton SG, Lohoff FW. Serotonin pathway polymorphisms and the treatment of major depressive disorder and anxiety disorders. Pharmacogenomics. (2015) 16:541–53. doi: 10.2217/pgs.15.15
27. Bradizza CM, Stasiewicz PR, Paas ND. Relapse to alcohol and drug use among individuals diagnosed with co-occurring mental health and substance use disorders: a review. Clin Psychol Rev. (2006) 26:162–78. doi: 10.1016/j.cpr.2005.11.005
28. Moak DH, Anton RF, Latham PK, Voronin KE, Waid RL, Durazo-Arvizu R. Sertraline and cognitive behavioral therapy for depressed alcoholics: results of a placebo-controlled trial. J Clin Psychopharmacol. (2003) 23:553–62. doi: 10.1097/01.jcp.0000095346.32154.41
29. Vorspan F, Mehtelli W, Dupuy G, Bloch V, Lepine JP. Anxiety and Substance Use Disorders: Co-occurrence and Clinical Issues. Curr Psychiatry Rep. (2015) 17:544. doi: 10.1007/s11920-014-0544-y
30. Kelly JF, Abry A, Ferri M, Humphreys K. Alcoholics anonymous and 12-step facilitation treatments for alcohol use disorder: a distillation of a 2020 cochrane review for clinicians and policy makers. Alcohol Alcohol. (2020) 55:641–51. doi: 10.1093/alcalc/agaa050
31. Cornelius JR, Douaihy A, Bukstein OG, Daley DC, Wood SD, Kelly TM, et al. Evaluation of cognitive behavioral therapy/motivational enhancement therapy (CBT/MET) in a treatment trial of comorbid MDD/AUD adolescents. Addict Behav. (2011) 36:843–8. doi: 10.1016/j.addbeh.2011.03.016
32. Kaner EF, Beyer C FR, Muirhead, Campbell F, Pienaar ED, Bertholet N, et al. Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database Syst Rev. (2018) 2:CD004148. doi: 10.1002/14651858.CD004148.pub4
33. Mellentin AI, Skøt L, Nielsen B, Schippers GM, Nielsen AS, Stenager E, et al. Cue exposure therapy for the treatment of alcohol use disorders. A meta-analytic review. Clin Psychol Rev. (2017) 57:195–207. doi: 10.1016/j.cpr.2017.07.006
34. Byrne SP, Haber P, Baillie A, Giannopolous V, Morley K. Cue Exposure therapy for alcohol use disorders: what can be learned from exposure therapy for anxiety disorders? Subst Use Misuse. (2019) 54:2053–63. doi: 10.1080/10826084.2019.1618328
35. Elkins RL, Richards TL, Nielsen R, Repass R, Stahlbrandt H, Hoffman HG. The Neurobiological Mechanism of Chemical Aversion (Emetic) Therapy for Alcohol Use Disorder: an fMRI Study. Front Behav Neurosci. (2017) 11:182. doi: 10.3389/fnbeh.2017.00182
36. Goltseker K, Handrus H, Barak S. Disruption of relapse to alcohol seeking by aversive counterconditioning following memory retrieval. Addict Biol. (2021) 26:e12935. doi: 10.1111/adb.12935
37. Cavicchioli M, Movalli M, Maffei C. The clinical efficacy of mindfulness-based treatments for alcohol and drugs use disorders: a meta-analytic review of randomized and nonrandomized controlled trials. Eur Addict Res. (2018) 24:137–62. doi: 10.1159/000490762
38. Gao J, Cao J, Guo T, Xiao Y. Association between alcoholic interventions and abstinence rates for alcohol use disorders: a meta-analysis. Medicine. (2018) 97:e13566–e13566. doi: 10.1097/MD.0000000000013566
39. Ray LA, Bujarski S, Grodin E, Hartwell E, Green R, Venegas A, et al. State-of-the-art behavioral and pharmacological treatments for alcohol use disorder. Am J Drug Alcohol Abuse. (2019) 45:124–40. doi: 10.1080/00952990.2018.1528265
40. Park-Lee E, Lipari RN, Hedden SL, Kroutil LA, Porter JD. Receipt of services for substance use and mental health issues among adults: results from the 2016 national survey on drug use and health. In: CBHSQ Data Review. Rockville, MD: Substance Abuse and Mental Health Services Administration (US) (2017).
41. Williams EC, Achtmeyer CE, Young JP, Berger D, Curran G, Bradley KA, et al. Barriers to and facilitators of alcohol use disorder pharmacotherapy in primary care: a qualitative study in five VA clinics. J Gen Intern Med. (2018) 33:258–67. doi: 10.1007/s11606-017-4202-z
42. Hagedorn HJ, Brown R, Dawes M, Dieperink E, Myrick DH, Oliva EM, et al. Enhancing access to alcohol use disorder pharmacotherapy and treatment in primary care settings: ADaPT-PC. Implement Sci. (2016) 11:64. doi: 10.1186/s13012-016-0431-5
43. Lohoff FW, Ferraro TN. Pharmacogenetic considerations in the treatment of psychiatric disorders. Expert Opin Pharmacother. (2010) 11:423–39. doi: 10.1517/14656560903508762
44. Hartwell EE, Kranzler HR. Pharmacogenetics of alcohol use disorder treatments: an update. Expert Opin Drug Metab Toxicol. (2019) 5:553–64. doi: 10.1080/17425255.2019.1628218
45. Lohoff FW. Pharmacotherapies and personalized medicine for alcohol use disorder: a review. Pharmacogenomics. (2020) 21:2020–79. doi: 10.2217/pgs-2020-0079
46. Dulin PL, Alvarado CE, Fitterling JM, Gonzalez VM. Comparisons of alcohol consumption by time-line follow back vs. smartphone-based daily interviews. Addict Res Theory. (2017) 25:195–200. doi: 10.1080/16066359.2016.1239081
47. Wray TB, Merrill JE, Monti PM. Using Ecological Momentary Assessment (EMA) to assess situation-level predictors of alcohol use and alcohol-related consequences. Alcohol Res. (2014) 36:19–27.
48. Roberts W, McKee SA. Mobile alcohol biosensors and pharmacotherapy development research. Alcohol. (2019) 81:149–60. doi: 10.1016/j.alcohol.2018.07.012
49. Heilig M, Augier E, Pfarr S, Sommer WH. Developing neuroscience-based treatments for alcohol addiction: a matter of choice? Transl Psychiatry. (2019) 9:255. doi: 10.1038/s41398-019-0591-6
50. Kwako LE, Schwandt ML, Ramchandani VA, Diazgranados N, Koob GF, Volkow ND, et al. Neurofunctional domains derived from deep behavioral phenotyping in alcohol use disorder. Am J Psychiatry. (2019) 176:744–53. doi: 10.1176/appi.ajp.2018.18030357
51. Kwako LE, Momenan R, Litten RZ, Koob GF, Goldman D. Addictions neuroclinical assessment: a neuroscience-based framework for addictive disorders. Biol Psychiatry. (2016) 80:179–89. doi: 10.1016/j.biopsych.2015.10.024
52. Jurado-Barba R, Sion A, Martinez-Maldonado A, Dominguez-Centeno I, Prieto-Montalvo J, Navarrete F, et al. Neuropsychophysiological measures of alcohol dependence: can we use EEG in the clinical assessment? Front Psychiatry. (2020) 11:676. doi: 10.3389/fpsyt.2020.00676
53. Nieto SJ, Grodin EN, Green R, Ray LA. Evaluation of the Addictions Neuroclinical Assessment (ANA) framework through deep phenotyping of problem drinkers. Drug Alcohol Depend. (2021) 221:108603. doi: 10.1016/j.drugalcdep.2021.108603
54. Votaw VR, Stein ER, Witkiewitz K. A longitudinal mediation model of negative emotionality, coping motives and drinking intensity among individuals receiving community treatment for alcohol use disorder. Alcohol Alcohol. (2021) 56:573–80. doi: 10.1093/alcalc/agab012
55. Litten RZ, Falk DE, Ryan ML, Fertig J, Leggio L. Five priority areas for improving medications development for alcohol use disorder and promoting their routine use in clinical practice. Alcohol Clin Exp Res. (2020) 44:23–35. doi: 10.1111/acer.14233
56. Del Re AC, Maisel N, Blodgett J, Finney J. The declining efficacy of naltrexone pharmacotherapy for alcohol use disorders over time: a multivariate meta-analysis. Alcohol Clin Exp Res. (2013) 37:1064–8. doi: 10.1111/acer.12067
57. Anton RF, Litten RZ, Falk DE, Palumbo JM, Bartus RT, Robinson RL, et al. A W. the: The Alcohol Clinical Trials Initiative (ACTIVE) purpose and goals for assessing important and salient issues for medications development in alcohol use disorders. Neuropsychopharmacology. (2012) 37:402–11. doi: 10.1038/npp.2011.182
58. Anton RF, Schacht JP, Book SW. Pharmacologic treatment of alcoholism. In: Sullivan EV, Pfefferbaum A, editors. Handbook of Clinical Neurology. Amsterdam; Kodlington; Waltham, MA: Elsevier (2014).
59. Moos RH, Moos BS. Rates and predictors of relapse after natural and treated remission from alcohol use disorders. Addiction. (2006) 101:212–22. doi: 10.1111/j.1360-0443.2006.01310.x
60. MacKillop J. Is addiction really a chronic relapsing disorder? Alcohol Clin Exp Res. (2020) 44:41–4. doi: 10.1111/acer.14246
61. Kelly JF, Greene MC, Bergman BG, White WL, Hoeppner BB. How many recovery attempts does it take to successfully resolve an alcohol or drug problem? Estimates and correlates from a national study of recovering US adults alcoholism: Clin Exp Res. (2019) 43:1533–44. doi: 10.1111/acer.14067
62. Grant BF, Harford TC. Comorbidity between Dsm-Iv Alcohol-Use Disorders and Major Depression - Results of a National Survey. Drug Alcohol Depend. (1995) 39:197–206. doi: 10.1016/0376-8716(95)01160-4
63. Buckley PF, Brown ES. Prevalence and consequences of dual diagnosis. J Clin Psychiatry. (2006) 67:e01. doi: 10.4088/JCP.0706e01
64. Jane-Llopis E, Matytsina I. Mental health and alcohol, drugs and tobacco: a review of the comorbidity between mental disorders and the use of alcohol, tobacco and illicit drugs. Drug Alcohol Rev. (2006) 25:515–36. doi: 10.1080/09595230600944461
65. Martins SS, Gorelick DA. Conditional substance abuse and dependence by diagnosis of mood or anxiety disorder or schizophrenia in the US population. Drug Alcohol Depend. (2011) 119:28–36. doi: 10.1016/j.drugalcdep.2011.05.010
66. Tawa EA, Hall SD, Lohoff FW. Overview of the genetics of alcohol use disorder. Alcohol Alcohol. (2016) 51:507–14. doi: 10.1093/alcalc/agw046
67. Helton SG, Lohoff FW. Pharmacogenetics of alcohol use disorders and comorbid psychiatric disorders. Psychiatry Res. (2015) 230:121–9. doi: 10.1016/j.psychres.2015.09.019
68. Kranzler HR, Mueller T, Cornelius J, Pettinati HM, Moak D, Martin PR, et al. Sertraline treatment of co-occurring alcohol dependence and major depression. J Clin Psychopharmacol. (2006) 26:13–20. doi: 10.1097/01.jcp.0000194620.61868.35
69. Pettinati HM, Oslin DW, Kampman KM, Dundon WD, Xie H, Gallis TL, et al. double-blind, placebo-controlled trial combining sertraline and naltrexone for treating co-occurring depression and alcohol dependence. Am J Psychiatry. (2010) 167:668–75. doi: 10.1176/appi.ajp.2009.08060852
70. Brady KT, Sonne S, Anton RF, Randall CL, Back SE, Simpson K. Sertraline in the treatment of co-occurring alcohol dependence and posttraumatic stress disorder. Alcohol Clin Exp Res. (2005) 29:395–401. doi: 10.1097/01.ALC.0000156129.98265.57
71. Petrakis IL, Ralevski E, Desai N, Trevisan L, Gueorguieva R, Rounsaville B, et al. Noradrenergic vs serotonergic antidepressant with or without naltrexone for veterans with PTSD and comorbid alcohol dependence. Neuropsychopharmacology. (2012) 37:996–1004. doi: 10.1038/npp.2011.283
72. Gao B, Bataller R. Alcoholic liver disease: pathogenesis and new therapeutic targets. Gastroenterology. (2011) 141:1572–85. doi: 10.1053/j.gastro.2011.09.002
73. Li TK. Quantifying the risk for alcohol-use and alcohol-attributable health disorders: Present findings and future research needs. J Gastroenterol Hepatol. (2008) 23:S2–8. doi: 10.1111/j.1440-1746.2007.05298.x
74. Rehm J, Samokhvalov AV, Shield KD. Global burden of alcoholic liver diseases. J Hepatol. (2013) 59:160–8. doi: 10.1016/j.jhep.2013.03.007
75. Centre N.I., Statistics on alcohol: England. (2009). Available online at: https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-alcohol
76. Seitz HK, Bataller R, Cortez-Pinto H, Gao B, Gual A, Lackner C, et al. Alcoholic liver disease. Nat Rev Dis Primers. (2018) 4:16. doi: 10.1038/s41572-018-0014-7
77. Anstee QM, Daly AK, Day CP. Genetics of alcoholic liver disease. Semin Liver Dis. (2015) 35:361–74. doi: 10.1055/s-0035-1567832
78. Villanueva A, Portela A, Sayols S, Battiston C, Hoshida Y, Méndez-González J, et al. DNA methylation-based prognosis and epidrivers in hepatocellular carcinoma. Hepatology. (2015) 61:1945–56. doi: 10.1002/hep.27732
79. Lee WM, Hynan LS, Rossaro L, Fontana RJ, Stravitz RT, Larson AM, et al. Intravenous N-Acetylcysteine improves transplant-free survival in early stage non-acetaminophen acute liver failure. Gastroenterology. (2009) 137:856–864.e1. doi: 10.1053/j.gastro.2009.06.006
80. Parker R, Armstrong MJ, Corbett C, Rowe IA, Houlihan DD. Systematic review: pentoxifylline for the treatment of severe alcoholic hepatitis. Aliment Pharmacol Ther. (2013) 37:845–54. doi: 10.1111/apt.12279
81. Lucey MR. Liver transplantation for alcoholic liver disease. Nat Rev Gastroenterol Hepatol. (2014) 11:300. doi: 10.1038/nrgastro.2013.247
82. Forrest EH, Morris AJ, Stewart S, Phillips M, Oo YH, Fisher NC, et al. The Glasgow alcoholic hepatitis score identifies patients who may benefit from corticosteroids. Gut. (2007) 56:1743–6. doi: 10.1136/gut.2006.099226
83. Singal AK, Shah VH. Current trials and novel therapeutic targets for alcoholic hepatitis. J Hepatol. (2019) 70:305–13. doi: 10.1016/j.jhep.2018.10.026
84. Mitchell MC, Friedman LS, McClain CJ. Medical management of severe alcoholic hepatitis: expert review from the clinical practice updates committee of the AGA institute. Clin Gastroenterol Hepatol. (2017) 15:5–12. doi: 10.1016/j.cgh.2016.08.047
85. Bataller R, Arteel GE, Moreno C, Shah V. Alcohol-related liver disease: Time for action. J Hepatol. (2019) 70:221–2. doi: 10.1016/j.jhep.2018.12.007
86. Huhn AS, Gipson CD. Promoting harm reduction as a treatment outcome in substance use disorders. Exp Clin Psychopharmacol. (2021) 29:217–8. doi: 10.1037/pha0000494
87. Jones JD, Varshneya NB, Hudzik TJ, Huhn AS. Improving translational research outcomes for opioid use disorder treatments. Curr Addict Rep. (2021) 8:109–21. doi: 10.1007/s40429-020-00353-5
Keywords: alcohol, addiction, treatment, Personalized and Precision Medicine (PPM), mood disorder
Citation: Lohoff FW (2022) Targeting Unmet Clinical Needs in the Treatment of Alcohol Use Disorder. Front. Psychiatry 13:767506. doi: 10.3389/fpsyt.2022.767506
Received: 30 August 2021; Accepted: 29 April 2022;
Published: 09 June 2022.
Edited by:
Joshua Gowin, University of Colorado, United StatesReviewed by:
Lea M. Hulka, University of Zurich, SwitzerlandCopyright © 2022 Lohoff. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Falk W. Lohoff, ZmFsay5sb2hvZmZAbmloLmdvdg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.