
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 03 June 2022
Sec. Child and Adolescent Psychiatry
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.756306
This article is part of the Research Topic Adolescence and Risk of Psychopathology: Understanding Trajectories and Early Interventions View all 13 articles
 Fabienne Ligier1,2,3,4,5*
Fabienne Ligier1,2,3,4,5* Festus Body Lawson5Marilou Lamourette5Charles-Edouard Giguère6Alain Lesage1,2,3,7Monique Séguin1,7,8,9
Festus Body Lawson5Marilou Lamourette5Charles-Edouard Giguère6Alain Lesage1,2,3,7Monique Séguin1,7,8,9Objective: Across the globe more than 35,000 children a year are adopted by non-relatives, and some studies suggest that adopted individuals may be more vulnerable to developing mental disorders. To map the differences in suicide risk factors in adopted and non-adopted individuals, this study will compare the development of mental disorders as well as life events occurring before the age of 18 for both adopted and non-adopted individuals deceased by suicide.
Methods: This study included 13 adopted and 26 non-adopted individuals deceased by suicide as well as 26 non-adopted living control individuals. Cases were taken from a data bank created over the last decade by researchers of [our institution] comprising a mixture of 700 suicide cases and living control individuals aged from 14 to 84. Adopted and non-adopted individuals deceased by suicide; adopted individuals deceased by suicide and non-adopted living control individuals were each compared on Axis I and II disorders, early life events, and burdens of adversity.
Results: Results show significant differences, with a higher rate of Attention Deficit Hyperactivity Disorder, mental health comorbidity and Cluster C personality disorders among adopted individuals. Furthermore, adopted individuals have higher adversity scores prior to the age of 15.
Conclusion: This study underlines the fact that adoptive families need to be supported throughout adoption. Health care professionals need specialized training on this matter, and the psychological challenges adopted individuals face need to be treated at the earliest juncture.
Across the globe, more than 35,000 children a year are adopted by non-relatives. Fortunately, the majority of adopted individuals are in good physical and mental health (1, 2). The knowledge that they were given up for adoption, or the experience of adverse early life events may be counteracted by a nurturing family environment (3). Some authors refer to the capacity to overcome early adversity, transforming experiences into resilience, especially when adoptive parents are sensitive to issues relating to the origins of their adopted child (4, 5).
However, when compared to the general population, a significantly large proportion of adopted individuals will develop mental disorders during childhood or later in life, which suggests that adopted individuals may be more prone to developing mental disorders (6–8). Recent data suggests that biological inheritance may be involved in the development of mental disorders among adopted individuals (9, 10); family antecedent of mental disorders accounts for 33–43% of suicide risk in adopted individuals (11, 12) as well as a proportion of mood disorders and substance abuse (9, 10). In addition, early life exposure to institutional deprivation may have a negative effect during the development process, and may increase the presence of mental disorders (13–16). For example, some studies reveal that adopted individuals may have a higher risk of externalizing disorders such as Attention Deficit Hyperactivity Disorder (ADHD) (2, 17), substance abuse (18), as well as a higher risk of suicide attempts (19).
Suicide is the second leading cause of death among people aged 15–24 and suicide prevention is a public health priority (WHO). Since adoption was during several decades an increasing trend worldwide, and adopted individuals may be more vulnerable to suicide, it is important to consider the specific risk variables these individuals may have to bear, and if prevention strategies need to be adapted for this specific population (20).
To map the differences in suicide risk factors in adopted and non-adopted individuals, this study will compare the development of mental disorders as well as life events occurring before the age of 18 for both adopted and non-adopted individuals deceased by suicide.
Thanks to an ongoing partnership between (our institution) and the Quebec Coroner's Office, for the past two decades several research groups [Dumais et al. (21); Kim et al. (22); Séguin et al. (23–25)] have been able to document the life trajectories of individuals deceased by suicide by interviewing their bereaved family members (23, 24, 26). The protocol is as follows: the family receives an introductory letter from the coroner's office, then a research assistant follows up with a telephone call. A trained mental health clinician then contacts the family members in order to present the study. If the family members agree to participate in our study an appointment is made, and the interview process begins 3–4 months after the suicide. Two interviews, each approximately 3 h long, are conducted for each suicide case. Approximately 75% of the close relatives referred by the coroner's office agreed to participate in the study.
Control participants were interviewed over the course of several studies. Most control individuals were participants from the general population identified through a snowball sampling method and an informant who had known the control participants were interviewed (23). This procedure has been previously described by Dumais et al. (21) and Kim et al. (22). All participants signed a consent form and the research held REB approval.
Over the last decade, researchers have created a data bank comprising a mixture of 700 suicide cases and control participants, aged 14–84 (23, 24, 26). In this data bank, we identified 13 cases of adopted individuals deceased by suicide which were compared with 26 non-adopted individuals deceased by suicide, and with 26 non-adopted living control individuals.
Data on common sociodemographic characteristics, life events and mental health characteristics were collected.
The post-mortem diagnosis was assessed using a psychological autopsy method (27). During the interview semi-structured questionnaires were administered using the DSM-IV Structured Clinical Interview for both Axis I and Axis II disorders (SCID I and II) (28), with an informant who had known the deceased well (26). Hospital files were also examined to corroborate this information and determine whether a diagnosis of mental disorder was present.
A case vignette was then drafted and discussed by a panel of experts, to determine the post-mortem diagnosis by consensus. This panel was composed of researchers from our team, clinical practitioners, psychiatrists, and psychologists.
A series of studies over the past decade have established the concordance of DSM diagnoses generated by informant reports in conjunction with chart diagnoses and the psychological autopsy method, which have been proven to have good reliability (27, 29, 30). The same interview methodology was applied to a control group (with a proxy-based interview or direct interview if proxy was unavailable).
The Life Trajectory Calendar interview method was borrowed from Life History Calendar research (30). The questionnaire uses a Life History Calendar to reconstruct the major events in an individual's life as an aid to accurately recall significant life experiences. The calendar explores several clearly described variables from all life spheres; furthermore the frequency, severity and duration of each variable is indicated on the calendar. Narrative methodology requires clinical case histories (case vignettes), and Life History Calendars were drafted after the interviews; the Life History Calendar makes it possible to pinpoint the occurrence of specific events (both positive and negative). The frequency, severity and duration of each event is recorded, and classified in a specific life sphere such as: events associated with early adversity (abuse, neglect, presence of violence, etc.,); events associated with academic life (interruptions, successes, failures, education path etc.); events associated with professional life (unemployment, stress at work, promotions, etc.,); events associated with social life (presence or absence of social support, friends, colleagues, etc.,); events involving the onset of interpersonal difficulties (difficulties associated with mental health, suicide attempts, illness, etc.,). The Life History Calendar approach, as underlined in a previous paper, assists in identifying proximal and distal life events, which helps to understand the life trajectories of individuals deceased by suicide (24). This interesting approach also allows the burden of adversity over the life trajectory to be quantified (24). For this study we targeted the variables occurring before the age of 19 years old.
A variable of 5-year periods for measuring the burden of adversity was developed in order to combine events occurring during a specific period of age into a 'summary variable. The value of this global variable identified as the “burden of adversity” was determined by a panel of experts (25). From clinical case histories, the panel analyzed the life trajectories of each individual and gave an overall adversity rating for each five-year period. The overall burden of adversity assessments ranged from severe (rating 1 or 2), to moderate (3 or 4), to low (5 or 6). In all cases, the experts rated each five-year period independently before reaching a consensus through discussion. When studying the clinical case histories, the intra-pair agreement rating in our panel of experts for each five-year period ranged from 76 to 97%; the lowest agreement was found in the 0–4-year age group studied (24).
In the aforementioned data bank, there were 13 adopted individuals among the 305 suicide cases. Each adopted individual deceased by suicide was matched (1:2) with a non-adopted individual deceased by suicide by age, gender, and region of study (New Brunswick, Ontario, or Québec) at the moment of death. Each adopted individual was also matched with a non-adopted living control individual (1:2) by the same variables (also matched by age, gender and region of study, at the time of interview for the control individuals).
Analyses were made by comparing Axis I and II disorders, early life events, and the burdens of adversity between adopted and non-adopted individuals deceased by suicide, and between adopted individuals deceased by suicide and non-adopted living control individuals. Axis I disorders were distinguished by 2 periods: the 12 months prior to death (individuals deceased by suicide) or the 12 months prior to the interview (living individuals) and the period preceding the12 months prior to the suicide or interview. We also compared the age of suicide of deceased adopted and non-adopted individuals. Comparisons were made using the Chi Square and Student's t-test, with p < 0.05 for significance. Analyses were carried out with SAS 9.4 software.
This study included 65 individual cases: 13 adopted individuals deceased by suicide, 26 non-adopted individuals deceased by suicide, and 26 non-adopted living control individuals. Each group was 54% male.
The mean (SD) age at the time of adoption was 10 months (18), while the mean age of suicide for both adopted and non-adopted individuals (n = 39) was 33.8 (19.6), from 13 to 83.
Comparisons of Axis I or II disorders between adopted and non-adopted individuals deceased by suicide show no difference for Axis I diagnoses in the 12 month period prior to death (Table 1). For the period preceding the 12 months prior to death, Attention Deficit Hyperactivity Disorder (p < 0.0001) and having two or more Axis I diagnoses (p = 0.004) are over-represented among adopted individuals. The same can be said for for Axis II Cluster C personality disorders (p = 0.04).

Table 1. Comparison of an Axis I and II disorders in the 12 months prior to suicide, and the period preceding the 12 months prior to suicide between adopted and non-adopted individuals (n = 39).
As for life events occuring prior to the age of 19 (Table 2), there was no difference between groups.
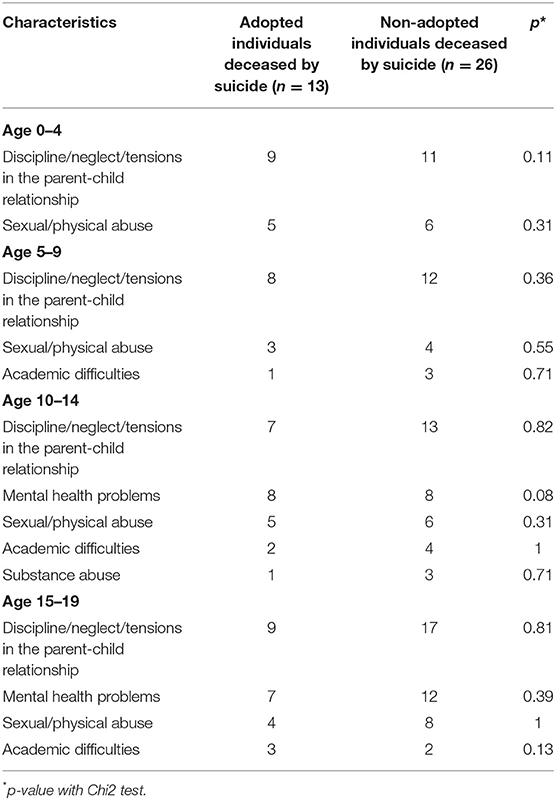
Table 2. Childhood life-events comparison between adopted and non-adopted individuals deceased by suicide (n = 39).
However, adopted individuals deceased by suicide have moderate adversity scores compared with the low adversity scores measured in non-adopted individuals deceased by suicide (see Table 3, Figure 1). The difference in adversity scoring is significant: from age 0 to 4 (3.9 vs. 5.3, p = 0.003), from 5 to 9 years old (3.4 vs. 5.0, p < 0.0001) and from age 10–14 (3.1 vs. 4.7, p < 0.003). The difference is however non-significant in the 15–19 age bracket (p = 0.14).
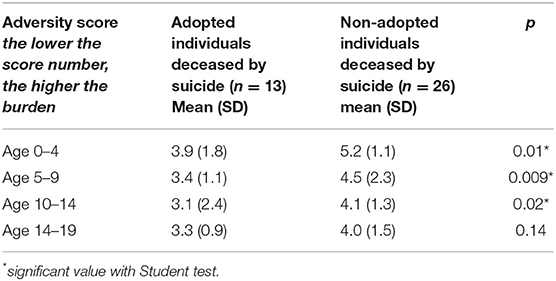
Table 3. Comparison of the burden of adversity score depending on age between adopted and non-adopted individuals deceased by suicide (n = 39).
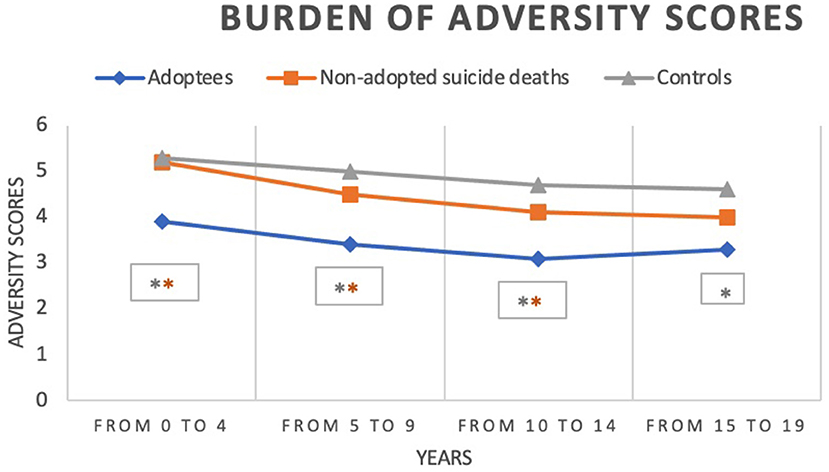
Figure 1. Burden of adversity scores comparing adopted and non-adopted individuals deceased by suicide, and non-adopted living control individuals (n = 65). *p < 0.05. The orange line compares adopted and non-adopted individuals deceased by suicide, and the silver line compares adopted and control individuals. The lower the score number, the higher the burden of adversity.
Lastly, there is no significant difference in the presence and number of past suicide attempts in adopted and non-adopted individuals deceased by suicide (0.07 < p < 0.49).
Comparisons of Axis I or II disorders between adopted individuals deceased by suicide vs. control individuals show significant differences in mood disorders (p < 0.0001), substance abuse (p = 0.04) and the presence of two or more Axis I diagnoses (p = 0.0002). These characteristics are over-represented among adopted individuals deceased by suicide. There is no difference for Axis I diagnoses in the period preceding the 12-months prior to their death or interview (0.06 < p < 1). There are significant differences for Axis II: adopted individuals deceased by suicide have higher incidences of Cluster B and C personality disorders compared with control individuals (p = 0.005 for both).
When looking at life events prior to the age of 19, adopted individuals deceased by suicide have higher rates of the variable “discipline/neglect/tensions in parent-child-relationship” (p = 0.04) and more mental health problems from the age of 10 years old (p = 0.02) compared with non-adopted living control individuals.
Finally, adversity scores are all significantly higher for individuals deceased by suicide with p < 0.003 for each period (see Figure 1).
The aim of this study was to compare adopted with non-adopted individuals deceased by suicide to find a potential specificity in adopted individuals deceased by suicide. Results show significant differences: a higher incidence of ADHD, mental health comorbidity and Cluster C personality disorders among adopted individuals. Moreover, adopted individuals have higher adversity scores prior to the age of 15.
Adopted individuals cumulate two or more Axis I diagnosis in the period preceding the 12 months prior to death, including ADHD. According to the literature, ADHD diagnosis is significantly higher in adopted individuals (17), which may be explained by several factors. One of these factors may be immaturity of the mother: giving up one's baby for adoption may be associated with teenage pregnancy and Halmøy and colleagues (31) concluded from a large population-based study, that adults with ADHD were more likely to be firstborns and to have a younger maternal age at delivery. Another factor may be mental disorders and/or substance abuse, as well as alcohol or drug absorption in utero (32, 33). These factors may in fact be consequences of a history of ADHD in the parents which increases the risk of ADHD in the adopted child (34–36). Equally, if we focus on parental substance abuse, infants may suffer withdrawal symptoms, which is associated with a higher risk of anxiety, a trait shared in the personality disorders found in the adopted individuals examined in this study. Indeed, personality disorders included in Cluster C of Axis II are Avoidant, Dependent, and Obsessive-Compulsive Personality Disorders. The weight of heredity may have both direct and indirect impact in the development of mental disorders among adopted individuals and may partly explain the cumulation of Axis I diagnoses.
Aside from the heredity factor, the early trauma of abandonment in adopted individuals may disturb the quality of attachment and their relationship with adoptive parents. Attachment disorders may also be explained by excessive expectations from the parents that lead to feelings of disappointment. Among the individuals in this study, Cluster B personality disorders were diagnosed in 6 of the 13 adopted individuals. We may hypothesize that, perhaps unsurprisingly, due to early separation from their biological parents some of the individuals studied may have been traumatized at an early stage in life, and may have therefore developed an attachment disorder (1), a characteristic often associated with Cluster B personality disorders such as borderline personality disorder.
If we focus on suicide risk factors, anxiety and borderline personality disorders are both well-known suicide risk factors, as is the impulsivity found in ADHD diagnosis (23, 37). So adopted individuals cumulate Axis I and Axis II mental health disorders for several reasons, and these diagnoses are all associated with a higher risk of suicide.
Furthermore, in all individuals deceased by suicide, mental health problems appear early: between 10 and 14 years old. The mean age of suicide is approximately 33, which underlines that suicide prevention strategies must be embedded from childhood. Of course, family relationships play a buffering role to protect family members against some risk factors, including the risk of suicide and we do not study here the quality of adoptive parents and their child (38).
Even if adopted and non-adopted individuals deceased by suicide have the same types of adverse early life events, adopted individuals have an increased early life adversity burden, even if they were adopted in their first year of the life. May we therefore hypothesize that some adopted individuals were less resilient, and so less able to overcome their early-life trauma (5)?
If we summarize the “profile” of adopted individuals deceased by suicide: they have a greater combination of psychiatric comorbidities and they have higher adversity scores in comparison with non-adopted individuals deceased by suicide compared with the control group. In addition, they have a higher rate of mood disorder and substance abuse during the 12 months prior to suicide compared with individuals from the general population deceased by suicide. They also have higher rate of Cluster B and C personality disorders, as usually described in their life trajectory (23).
That is why it is crucial to be attentive to adopted individuals, a population that may present higher hereditary risk factors for mental disorders, as underlined in the literature (9, 10). The recommendation for special attention may be also linked to this question: do adopted individuals have more psychiatric diagnoses because their parents are more attentive to their psychological development, as described by some authors (8)? Would this explain why adopted individuals often have more diagnoses? In this study, diagnoses have been made in the same way for adopted and non-adopted individuals through interviews of their informants, so the results should have not be influenced by the fact of been or not been adopted. But in situations in which the individual has been adopted, professionals run the risk of trivializing symptoms in saying “it”s just due to their being adopted', as perhaps may occur when dealing with their anxiety issues. We know adopted individuals need care, at least as much if not more than than their non-adopted peers: professionals must therefore be trained specifically to take into account an adopted individual's background when providing care.
This study has some limitations due to the retrospective methods employed, specifically regarding memory biases. However, a series of studies over the past decade have established agreement between DSM diagnoses based on informant report and those based on medical charts (39) and have shown the psychological autopsy method to be reliable (29, 40, 41). As is common in this kind of study, the control individuals are not representative of the general population, as they were generally recruited from friends or neighbors who share environmental and associative mating determinants of mental disorders, which may explain the high rate of mental disorder among control individuals (42). At last, we have no information about adoption between national and international. However, the fact that this is an original study is a strength, as this kind of research has not been done on suicide subjects before, plus we matched individuals on gender, age and region of study to limit biases.
Adopted individuals who die by suicide have higher adversity scores in early life, even if they were adopted in their first year of life. Besides the potential trauma of abandonment, they may have hereditary risk factors for mental disorders. Youth caregivers have to be carefull to these risks of suicide in general and in adopted children in particular.
The adoptive family need to be supported throughout adoption, health care professionals need specific training, and psychological difficulties need to be cared for at the earliest possible juncture.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Research Ethics Boards of the Douglas Mental Health Institute (Montreal) and of the Université du Québec en Outaouais. The patients/participants provided their written informed consent to participate in this study.
FL and MS conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript. C-EG, FL, and AL designed the data collection instruments, collected data, carried out the initial analysis, and reviewed and revised the manuscript. FB and ML critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Many thanks to Nadia Chawky from the McGill Group for Suicide Studies for her kind help during this research and AMC (Association of the Psychotherapy Treatment Centres of Nancy) for its financial contribution to the English language review of this text.
ADHD, Attention Deficit Hyperactivity Disorder.
1. Barcons N, Abrines N, Brun C, Sartini C, Fumadó V, Marre D. Attachment and adaptive skills in children of international adoption. Child Fam Soc Work. (2014) 19:89–98. doi: 10.1111/j.1365-2206.2012.00883.x
2. Bimmel N, Juffer F, van IJzendoorn MH, Bakermans-Kranenburg MJ. Problem behavior of internationally adopted adolescents: a review and meta-analysis. Harv Rev Psychiatry. (2003) 11:64–77. doi: 10.1080/10673220303955
3. Cederblad M, Höök B, Irhammar M, Mercke AM. Mental health in international adoptees as teenagers and young adults. An epidemiological study. J Child Psychol Psychiatry. (1999) 40:1239–48. doi: 10.1111/1469-7610.00540
4. Mohanty J, Newhill C. Adjustment of international adoptees: implications for practice and a future research agenda. Child Youth Serv Rev. (2006) 28:384–95. doi: 10.1016/j.childyouth.2005.04.013
5. Askeland KG, Hysing M, Aarø LE, Tell GS, Sivertsen B. Mental health problems and resilience in international adoptees: Results from a population-based study of Norwegian adolescents aged 16-19 years. J Adolesc. (2015) 44:48–56. doi: 10.1016/j.adolescence.2015.07.001
6. Askeland KG, Hysing M, La Greca AM, Aarø LE, Tell GS, Sivertsen B. Mental health in internationally adopted adolescents: a meta-analysis. J Am Acad Child Adolesc Psychiatry. (2017) 56:203–13. doi: 10.1016/j.jaac.2016.12.009
7. Hjern A, Lindblad F, Vinnerljung B. Suicide, psychiatric illness, and social maladjustment in intercountry adoptees in Sweden: a cohort study. Lancet. (2002) 360:443–8. doi: 10.1016/S0140-6736(02)09674-5
8. Miller BC, Fan X, Grotevant HD, Christensen M, Coyl D, Van Dulmen M. Adopted adolescents' overrepresentation in mental health counseling: adoptees' problems or parents' lower threshold for referral? J Am Acad Child Adolesc Psychiatry. (2000) 39:1504–11. doi: 10.1097/00004583-200012000-00011
9. McAdams TA, Rijsdijk FV, Neiderhiser JM, Narusyte J, Shaw DS, Natsuaki MN, et al. The relationship between parental depressive symptoms and offspring psychopathology: evidence from a children-of-twins study and an adoption study. Psychol Med. (2015) 45:2583–94. doi: 10.1017/S0033291715000501
10. Kendler KS, Ohlsson H, Sundquist K, Sundquist J. The causes of parent-offspring transmission of drug abuse: a Swedish population-based study. Psychol Med. (2015) 45:87–95. doi: 10.1017/S0033291714001093
11. Borczyskowski A, Hjern A, Lindblad F, Vinnerljung B. Suicidal behaviour in national and international adult adoptees: a Swedish cohort study. Soc Psychiatry Psychiatr Epidemiol. (2006) 41:95–102. doi: 10.1007/s00127-005-0974-2
12. Wilcox HC, Kuramoto SJ, Brent D, Runeson B. The interaction of parental history of suicidal behavior and exposure to adoptive parents' psychiatric disorders on adoptee suicide attempt hospitalizations. Am J Psychiatry. (2012) 169:309–15. doi: 10.1176/appi.ajp.2011.11060890
13. Sonuga-Barke EJS, Kennedy M, Kumsta R, Knights N, Golm D, Rutter M, et al. Child-to-adult neurodevelopmental and mental health trajectories after early life deprivation: the young adult follow-up of the longitudinal English and Romanian Adoptees study. Lancet. (2017) 389:1539–48. doi: 10.1016/S0140-6736(17)30045-4
14. Juffer F, van IJzendoorn MH. Behavior problems and mental health referrals of international adoptees: a meta-analysis. JAMA. (2005) 293:2501–15. doi: 10.1001/jama.293.20.2501
15. Rosnati R, Montirosso R, Barni D. Behavioral and emotional problems among Italian international adoptees and non-adopted children. Father's and mother's reports. J Fam Psychol 22. (2008) (3):541–9. doi: 10.1037/0893-3200.22.3.541
16. Harf A, Taïeb O, Moro MR. Troubles du comportement externalisés à l'adolescence et adoptions internationales : revue de la littérature [Externalizing behaviour problems of internationally adopted adolescents: a review]. Encephale. (2007) 33:270–6. French. doi: 10.1016/S0013-7006(07)92039-4
17. Keyes MA, Sharma A, Elkins IJ, Iacono WG, McGue M. The mental health of US adolescents adopted in infancy. Arch Pediatr Adolesc Med. (2008) 162:419–25. doi: 10.1001/archpedi.162.5.419
18. Lindblad F, Hjern A, Vinnerljung B. Intercountry adopted children as young adults - a Swedish cohort study. Am J Orthopsychiatry. (2003) 73:190–202. doi: 10.1037/0002-9432.73.2.190
19. Keyes MA, Malone SM, Sharma A, Iacono WG, McGue M. Risk of suicide attempt in adopted and nonadopted offspring. Pediatrics. (2013) 132:639–46. doi: 10.1542/peds.2012-3251
20. Morgan L. Prevention starts with awareness: adoptive adolescents at high risk for suicidal behavior. NASN Sch Nurse. (2017) 32:302–9. doi: 10.1177/1942602X16672063
21. Dumais A, Lesage AD, Lalovic A, Séguin M, Tousignant M, Chawky N, et al. Is violent method of suicide a behavioral marker of lifetime aggression? Am J Psychiatry. (2005) 162:1375–8. doi: 10.1176/appi.ajp.162.7.1375
22. Kim C, Lesage A, Seguin M, Chawky N, Vanier C, Lipp O, et al. Patterns of co-morbidity in male suicide completers. Psychol Med. (2003) 33:1299–309. doi: 10.1017/S0033291703008146
23. Séguin M, Renaud J, Lesage A, Robert M, Turecki G. Youth and young adult suicide: a study of life trajectory. J Psychiatry Res. (2011) 45:863–70. doi: 10.1016/j.jpsychires.2011.05.005
24. Séguin M, Beauchamp G, Robert M, DiMambro M, Turecki G. Developmental model of suicide trajectories. Br J Psychiatry. (2014) 205:120–6. doi: 10.1192/bjp.bp.113.139949
25. Séguin M, Lesage A, Turecki G, Bouchard M, Chawky N, Tremblay N, et al. Life trajectories and burden of adversity: mapping the developmental profiles of suicide mortality. Psychol Med. (2007) 37:1575–83. doi: 10.1017/S0033291707000955
26. Conner KR, Conwell Y, Duberstein PR. The validity of proxy-based data in suicide research: a study of patients 50 years of age and older who attempted suicide. II Life events, social support and suicidal behavior. Acta Psychiatr Scand. (2001) 104:452–7. doi: 10.1034/j.1600-0447.2001.00091.x
27. Spitzer RL, Williams JBW, Gibbon M, First MB. The structured clinical interview for DSM-III-R (SCID): I: history, rationale, and description. Arch Gen Psychiatry. (1992) 49:624–9. doi: 10.1001/archpsyc.1992.01820080032005
28. First MB, Gibbon M, Spitzer RL, Williams JBW, Benjamin LS. Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II). Washington, DC: American Psychiatric Press, Inc (1997).
29. Kelly TM, Mann JJ. Validity of DSM-III-R diagnosis by psychological autopsy: a comparison with clinician ante-mortem diagnosis. Acta Psychiatr Scand. (1996) 94:337–43. doi: 10.1111/j.1600-0447.1996.tb09869.x
30. Caspi A, Moffitt TE, Thornton A, Freedman D, Amell JW, Harrington H, et al. The life history calendar: a research and clinical assessment method for collecting retrospective event-history data. Int J Methods Psychiatr Res. (1996) 6:101–14.
31. Halmøy A, Klungsøyr K, Skjærven R, Haavik J. Pre- and perinatal risk factors in adults with attention-deficit/hyperactivity disorder. Biol Psychiatry. (2012) 71:474–81. doi: 10.1016/j.biopsych.2011.11.013
32. Landgren M, Svensson L, Strömland K, Andersson Grönlund M. Prenatal alcohol exposure and neurodevelopmental disorders in children adopted from eastern Europe. Pediatrics. (2010) 125:e1178–85. doi: 10.1542/peds.2009-0712
33. Chasnoff IJ, Wells AM, King L. Misdiagnosis and missed diagnoses in foster and adopted children with prenatal alcohol exposure. Pediatrics. (2015) 135:264–70. doi: 10.1542/peds.2014-2171
34. Chang Z, Lichtenstein P, D'Onofrio BM, Almqvist C, Kuja-Halkola R, Sjölander A, et al. Maternal age at childbirth and risk for ADHD in offspring: a population-based cohort study. Int J Epidemiol. (2014) 43:1815–24. doi: 10.1093/ije/dyu204
35. Galbally M, Snellen M, Power J. Antipsychotic drugs in pregnancy: a review of their maternal and fetal effects. Ther Adv Drug Saf. (2014) 5:100–9. doi: 10.1177/2042098614522682
36. Kotelchuck M, Cheng ER, Belanoff C, Cabral HJ, Babakhanlou-Chase H, Derrington TM, et al. The prevalence and impact of substance use disorder and treatment on maternal obstetric experiences and birth outcomes among singleton deliveries in massachusetts. Matern Child Health J. (2017) 21:893–902. doi: 10.1007/s10995-016-2190-y
37. Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. (2016) 387:1227–39. doi: 10.1016/S0140-6736(15)00234-2
38. Melançon F, Cossette L, Smith C, Beauvais-Dubois C, Cyr C, Smolla N. Parenting stress of adoptive mothers, mother-child conflict, and behavior problems during adolescence among international adoptees. J Fam Psychol. (2019) 33:988–93. doi: 10.1037/fam0000542
39. Schneider B, Maurer K, Sargk D, Heiskel H, Weber B, Frölich L, et al. Concordance of DSM-IV Axis I and II diagnoses by personal and informant's interview. Psychiatry Res (2004). (2004) 127:121–36. doi: 10.1016/j.psychres.2004.02.015
40. Dohrenwend BP. Inventorying stressful life events as risk factors for psychopathology: toward resolution of the problem of intracategory variability. Psychol Bull. (2006) 2006. doi: 10.1037/0033-2909.132.3.477
41. Brent DA, Perper JA, Moritz G, Allman CJ, Roth C, Schweers J, et al. The validity of diagnoses obtained through the psychological autopsy procedure in adolescent suicide victims: use of family history. Acta Psychiatr Scand. (1993) 87:118–22. doi: 10.1111/j.1600-0447.1993.tb03341.x
Keywords: adoption, developmental course, risk factors, suicide, youth—young adults
Citation: Ligier F, Body Lawson F, Lamourette M, Giguère C-E, Lesage A and Séguin M (2022) Comparing Childhood Characteristics of Adopted and Non-adopted Individuals Deceased by Suicide. Front. Psychiatry 13:756306. doi: 10.3389/fpsyt.2022.756306
Received: 10 August 2021; Accepted: 27 April 2022;
Published: 03 June 2022.
Edited by:
David Cohen, Sorbonne Universités, FranceReviewed by:
Srinivas Dannaram, Banner Health, United StatesCopyright © 2022 Ligier, Body Lawson, Lamourette, Giguère, Lesage and Séguin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabienne Ligier, ZmFiaWVubmUubGlnaWVyQGNwbi1sYXhvdS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.