
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 17 February 2022
Sec. Child and Adolescent Psychiatry
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.736696
This article is part of the Research TopicAntioxidants in Autism Spectrum DisordersView all 6 articles
 Jessica Galli1,2*
Jessica Galli1,2* Erika Loi2,3
Erika Loi2,3 Lucrezia Maria Visconti1
Lucrezia Maria Visconti1 Paola Mattei2Anna Eusebi2
Paola Mattei2Anna Eusebi2 Stefano Calza4
Stefano Calza4 Elisa Fazzi1,2 and ASD Collaborative Group
Elisa Fazzi1,2 and ASD Collaborative GroupBackground: Sleep disturbances are common in children affected by Autism Spectrum Disorder (ASD). The aim of our study was to describe sleep characteristics and disturbances in children with ASD, to evaluate possible related factors, and to assess parental stress.
Methods: Hundred children with a diagnosis of ASD (mean age: 66.7 months, SD: 27.4, range: 24.7–152.1 months, n = 79 males) were included in the study. We collected data on sociodemographic, clinical, genetic and instrumental variables as well as comorbid conditions. Parents filled out the Questionnaire on sleep behavior in the first years of life, the BEARS questionnaire, and the Parenting Stress Index Short Form. From the analysis on sleep characteristics, we excluded 25 children treated with melatonin.
Results: Fifty-seven (57%) out of 100 children met the criteria for insomnia. Sleep disorders were associated with developmental or cognitive delay, emotional and behavioral problems (such as anxiety problems and aggressive behaviors) and absence of strategies for inducing sleep after nocturnal awakenings. From parents' reports, sleep disorders had diurnal repercussions on their offspring; however, we found no statistical correlation between disturbances and family stress. Also, no significant correlation was found between sleep disturbances and epilepsy. Finally, a statistical correlation was found between the regular intake of melatonin and the resolution of insomnia.
Conclusions: Multifactorial variables may be associated to insomnia that could have an impact on the children' behavior. Clinicians need to be aware of the value of screening for sleep disturbance in children with ASD to integrate sleep interventions in the treatment plan.
Autism spectrum disorder (ASD) is a life-long neurodevelopmental condition affecting communication and social interaction across multiple contexts and it includes the presence of atypical and heterogeneous behaviors such as restricted and repetitive patterns of interests or activities manifesting with different degrees of severity; intellectual disability or global developmental delay does not explain it any better (1). Sleep disorders are frequently observed in children with ASD with a higher prevalence (50–80%) (2) compared to that observed in typically developing children (25–40%) (3) and in children affected by other neurodevelopmental disabilities [Down syndrome, 55% or cerebral palsy, 43% (4)]. The type of sleep disturbances is similar in children with and without neurodevelopmental disorders (5). The most described insomnia (6) is onset insomnia or difficulty initiating sleep and sleep maintenance. Besides insomnia, parasomnia such as sleepwalking, nightmare, pavor nocturnus and sleep apnea, enuresis, difficult awakening and daytime sleepiness are also reported (7, 8).
Although children with ASD seem to have a greater vulnerability to sleep problems, the pathophysiology of these difficulties remains unclear. Mazzone et al. (9) offered three hypotheses. First of all, sleep problems may be explained as the consequence of neurobiological and genetic alteration that result in sleep architecture disruption; for instance, abnormal expressions of several neurotransmitters implicated in sleep regulation [such as serotonin, melatonin (10–15), and gamma-aminobutyric acid] (16, 17), and mutations in circadian-relevant genes as NR1D1, CLOCK, ARNTL2 (10), PER1-2-3 (18) have been reported in subjects with ASD. Second, sleep problems may themselves be a core aspect of ASD related to the specific characteristics of the autism. For example, not adhering to bed time rituals, excessive and repetitive activities before bed-time, communication deficits, hypo- or hyper-arousal, sensory dysregulation (19, 20), food selectivity, phobias (21), medical comorbidities and pharmacological treatment as risperidone (9, 22) may cause delayed sleep onset or insomnia. Third, sleep problems could be co-occurring disorders independent from ASD. In addition to the above specific mechanisms, physiological stressors such as being sick, psychological aspects as a difficult day at school (23), child rearing practices (24), and poor sleep hygiene behavior have been suggested as non-specific causes of sleep disturbances.
Sleep disruption may negatively act at neuroanatomical and clinical levels. Research on animals and on typically developing children demonstrated that sleep deprivation may lead to impairments of adequate synaptic development and brain maturation (24, 25); therefore, some authors have speculated that sleep dysfunction in children with ASD could actively cause disorders in synaptic function, potentially creating a maladaptive feed-forward loop of sleep disruption and neural anomalies (24, 25). Furthermore, less sleeping time and worse quality of sleep may affect adaptive behavior (e.g., hygiene, eating, toileting…), cognition, attention, memory, learning (26–30) and executive functioning (31), and increase internalizing and externalizing problems, as depression, anxiety, self-injury, oppositional behavior, irritability, physical aggression (24, 32–35). Sleep problems may also exacerbate the core symptom severity of ASD: poor sleepers were reported to show more restricted and stereotyped behaviors, more severe social skills deficits (2, 26, 36–40) and communication problems (41). However, it is still unclear what daytime implications of sleep disorder are and the direction of their relationship.
Parenting a child with ASD is per se a heavy burden related to emotional, behavioral and communication difficulties (42). In addition, child sleep problems may further increase the family distress affecting the quality of parental sleep (43) and exacerbating offspring symptoms, particularly behavioral problems such as hyperactivity, self-injury, aggressiveness (9).
From a holistic perspective, to our knowledge, there is no study that considers sleep in terms of sleep characteristics (duration, habits and rituals, awakenings), sleep disturbances (insomnia, breathing related sleep disorders or parasomnias) and their impact on child and family life. The aims of our study were: (1) to detail the characteristics of sleep in children with ASD and the type of their sleep disturbances; (2) to evaluate any possible factors (related to ASD condition itself, as severity of autism and comorbidities, and to sleep habits) associated with sleep disturbances; (3) to assess the parents' perception of the sleep disorder of their ASD offspring and whether sleep disturbance has a negative impact on children behavior and parenting stress; (4) to explore the effect of melatonin on sleep disturbances in a small subgroup of ASD children.
We carried out an observational study of 100 children with ASD (mean age: 66.7 months, SD: 27.4, range: 24.7–152.1 months, n = 79 males) recruited at the Unit of Child and Adolescent Neurology and Psychiatry of ASST Spedali Civili of Brescia, Italy, between January 2020 and January 2021. We got a written informed consent from parents and we conducted the study according to the Declaration of Helsinki which was approved by the Institutional Review Board of ASST Spedali Civili of Brescia (Comitato Etico di Brescia, ID number 4085 SLEEPASD). Participation was voluntary, and the data were processed anonymously.
The diagnosis of autism was the only inclusion criterion, previously made in accordance with the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-V) (1) criteria and performed by a multidisciplinary team including a child neuropsychiatrist and an experienced child psychologist.
We collected sociodemographic data as: age and sex of the patient, family structure (siblings: number, sex, age, health condition; parents: age, nationality, marital status, education, and occupation) and family socioeconomic status (SES). The following data on clinical and genetic/instrumental characteristics were obtained from charts: pregnancy, delivery, gestational age, neurological examination (normal or pathological according to the absence/presence of one or more abnormalities concerning cranial nerve, muscle strength, tone and bulk, reflexes and gait), pharmacological treatment, genetic analysis (karyotype, FRAXA, CGH-array), and instrumental examination (brain magnetic resonance imaging and electroencephalogram) defined as “normal” or “altered” in the absence/presence of genetic, structural brain and/or electroencephalographic abnormalities.
We performed the Autism Diagnostic Observation Schedule, 2nd Edition (ADOS-2) (44) to determine the autism symptom severity in 79 children. We collected data on comorbidities as developmental/cognitive delay, emotional and behavioral difficulties and epilepsy. It is noteworthy that epilepsy has been reported to define in children with ASD a different subgroup in terms of clinical characteristics including intellectual disability (45).
Finally, parents filled out three questionnaires at home on: sleep characteristics (duration, habits, rituals and awakenings), sleep disturbances, and parental stress levels. After completion, parents returned the questionnaires during any programmed visits to our Unit. We carried out a diagnosis of sleep disturbances (insomnia, breathing related sleep disorders, or parasomnias) using the findings from the questionnaires and according to the DSM-V criteria.
To avoid a possible bias related to pharmacological intake of hypnotic drugs, we split the total sample in two subgroups: 75 children were not treated with hypnotic drugs and included in the analyses on sleep characteristics, and 25 were treated with melatonin, excluded from the mentioned analyses. In this subgroup, we evaluated the persistence of sleep disturbances after the beginning of the treatment.
We measured family SES by the Hollingshead Scale (Hollingshead, unpublished manuscript)1, which ranks social position based on maternal and paternal occupation and educational attainment. The occupation scores range from 1 to 9 and the education scores from 1 to 7, with lower scores reflecting lower occupational/educational status. We considered the items (Occupation score × 5, Education score × 3) and summed them to produce an Index of Social Position Score (range: 8–66) classified into five categories, with higher scores indicating higher status.
The Autism Diagnostic Observation Schedule 2nd edition (ADOS-2) (44) is a semi-structured, standardized assessment of communication, social interaction, play and restricted and repetitive behaviors. It consists of five modules selected based on the expressive language level and the chronological age and comprises two domains: Social Affect and Restricted Repetitive Behavior. Calibrated Severity Scores were calculated to yield 1 of 3 clinical severity levels: low level of autistic symptoms, medium level, high level.
Developmental profile was evaluated in 81 children using the Griffiths Mental Development Scales Extended Revised (GMDS-ER) (46). It examines six domains of functioning, individually scored: Locomotor, Personal-Social, Hearing and Speech, Eye and Hand Coordination, Performance and Practical Reasoning. A Total Score called Developmental Quotient (DQ) is obtained from the average of the five domains. All the quotients are reported in standard scores (DQ: mean 100, SD 15). Children performances were rated as follows: more than −1 DS, normal; between −1 and −2 DS, borderline; < -2 DS, delay.
Full Intelligence Quotient was evaluated in 19 children using age-appropriate versions of Wechsler intelligence scales IV edition (47). The quotient is reported in standard scores (mean 100, SD 15) rated as follows: more than −1 DS, normal; between −1 and −2 DS, borderline; < -2 DS, delay.
To evaluate the risk of emotional and behavioral difficulties, the parent report Child Behavior Checklist 1½-5 (48, 49) or 6–18 (50) was carried out according to age. The item scores are aggregated in: (1) three composite scales (Internalizing, Externalizing, and Total problems); (2) syndrome scales (CBCL 1½-5: Emotionally reactive, Anxious/Depressed, Somatic complaints, Withdrawn, Sleep problems, Attention problems, and Aggressive behavior; CBCL 6–18: anxious/depressed, withdrawn/ depressed, somatic complaints, social problems, thought problems, attention problems, rule-breaking behavior and aggressive behavior); (3) DSM-oriented scales (CBCL 1½-5: Affective problems, Anxiety problems, Pervasive developmental problems, Attention deficit/Hyperactivity problems, and Oppositional defiant problems; CBCL 6-18: affective problems, anxiety problems, somatic problems, attention deficit/hyperactivity problems, oppositional defiant problems, conduct problems). T scores are created based on a normative sample; the cut-off points were categorized as “normal,” “borderline,” or “clinically significant” according to the tool kit software standards.
The questionnaire (51) elicits assessable information about sleep behavior. It is structured in a series of single answers, multiple and forced choice (YES/NO) questions except for the last part that allows parents to express freely their own opinions on their child's sleep behavior. We chose to administer this questionnaire because it provides: first, sociodemographic data (age, gender, nationality, marital status, education level, and occupation) of the parents and on the family structure; second, a deep and detailed description of sleep behavior since the first years, considering also habits, rituals and any form of strategies adopted by parent to favor sleep; third, information on parents' habits (as waking up during the night to check their baby) and perception of their child sleep (as problematic or not).
The BEARS (52) is a screening tool developed to address the most common sleep issues in toddlers, preschoolers, and school aged children (2–18 year old age range). Five sleep domains are evaluated through a set of age-appropriate “trigger questions”. The five sleep domains are: Bedtime Problems, including difficulty going to bed and falling asleep; Excessive Daytime Sleepiness, which includes behaviors typically associated with daytime somnolence in children; Awakenings during the night; Regularity of sleep/wake cycles (bedtime, wake time) and average sleep duration; Snoring. We chose to use the BEARS questionnaire in order to support the findings obtained from the Questionnaire on sleep behavior in the first years of life because it is a brief and easy tool used to screen sleep problems systematically. Owens and Dalzell (53) in their pilot study demonstrated the usefulness of the questionnaire when compared with the usual consultation because of the increased amount of information on children sleep behavior and problems.
The Parenting Stress Index Short Form (PSI-SF) (54), one of the most widely used tools for measuring parenting stress, was used. It contains 36 items divided into three subscales: “Parental distress” refers to the distress felt by the parent in his/her parental role, “Parent-child dysfunctional interaction” indicates the level of satisfaction perceived by the parent in the relationship with the offspring, and “Difficult child” specifies to the degree of difficulty experienced by the parent regarding the child's behavior. Each item is rated from 1 (strongly disagree) to 5 (strongly agree). The PSI-SF gives three subscores and a total score. Higher scores (at 90th percentile) are associated with significant parental stress level.
Once the questionnaires were returned, we did statistical analyses using R statistical package (version 4.0.3) setting the statistical significance threshold at 5%. We described the qualitative variables as number and percentage and the quantitative variables as mean, standard deviation and range. We applied Pearson's Chi-squared test to study the relationship between sleep disturbances and sociodemographic (age, sex, pregnancy and delivery, gestational age, and family variables), clinical (neurological examination and severity of ASD), and genetic/instrumental data. In addition, we investigated the relationship between sleep disturbances and comorbidities, sleep characteristics, and parental stress index.
In Tables 1, 2, respectively, we report sociodemographic data and children demographic, clinical, genetic and instrumental characteristics; while Table 3 shows comorbid conditions of the sample.
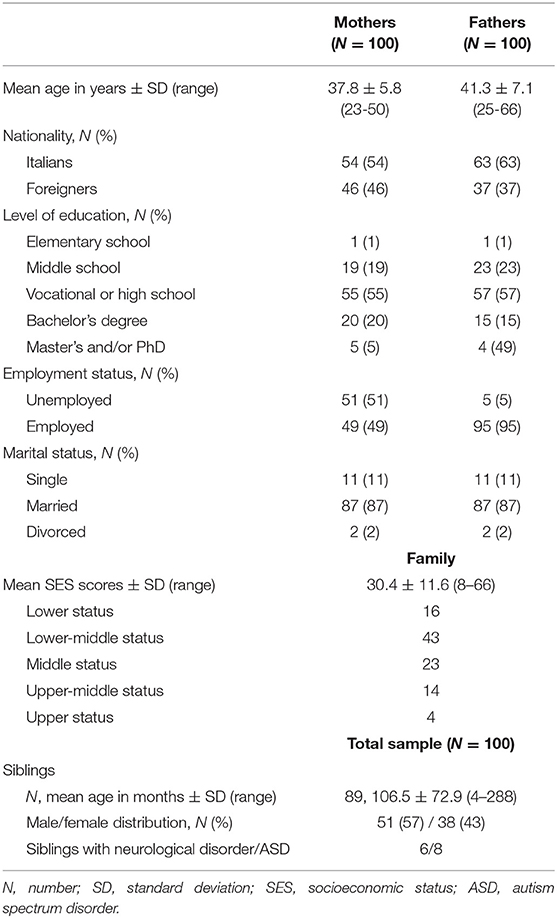
Table 1. Sociodemographic data and family structure.
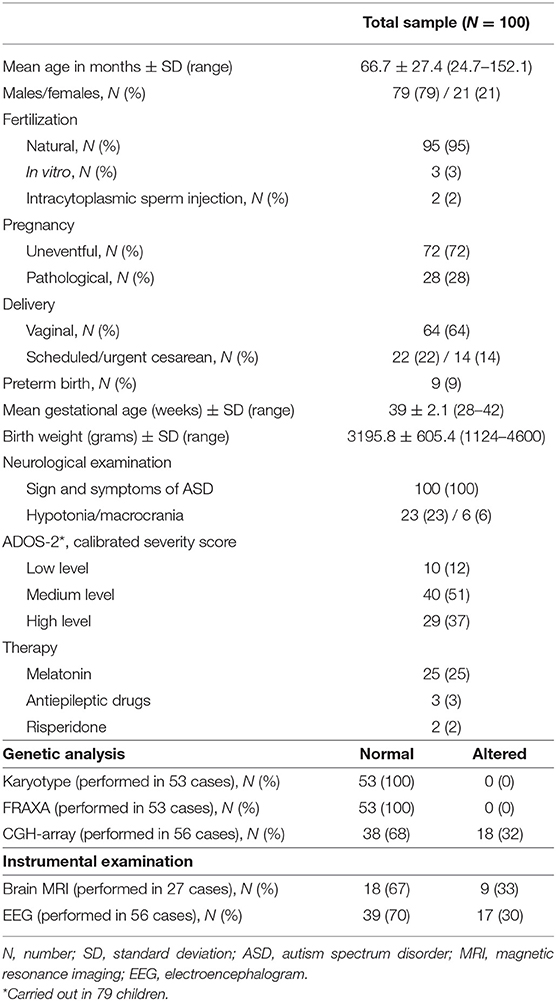
Table 2. Demographic, clinical, and genetic/instrumental data of the total sample.
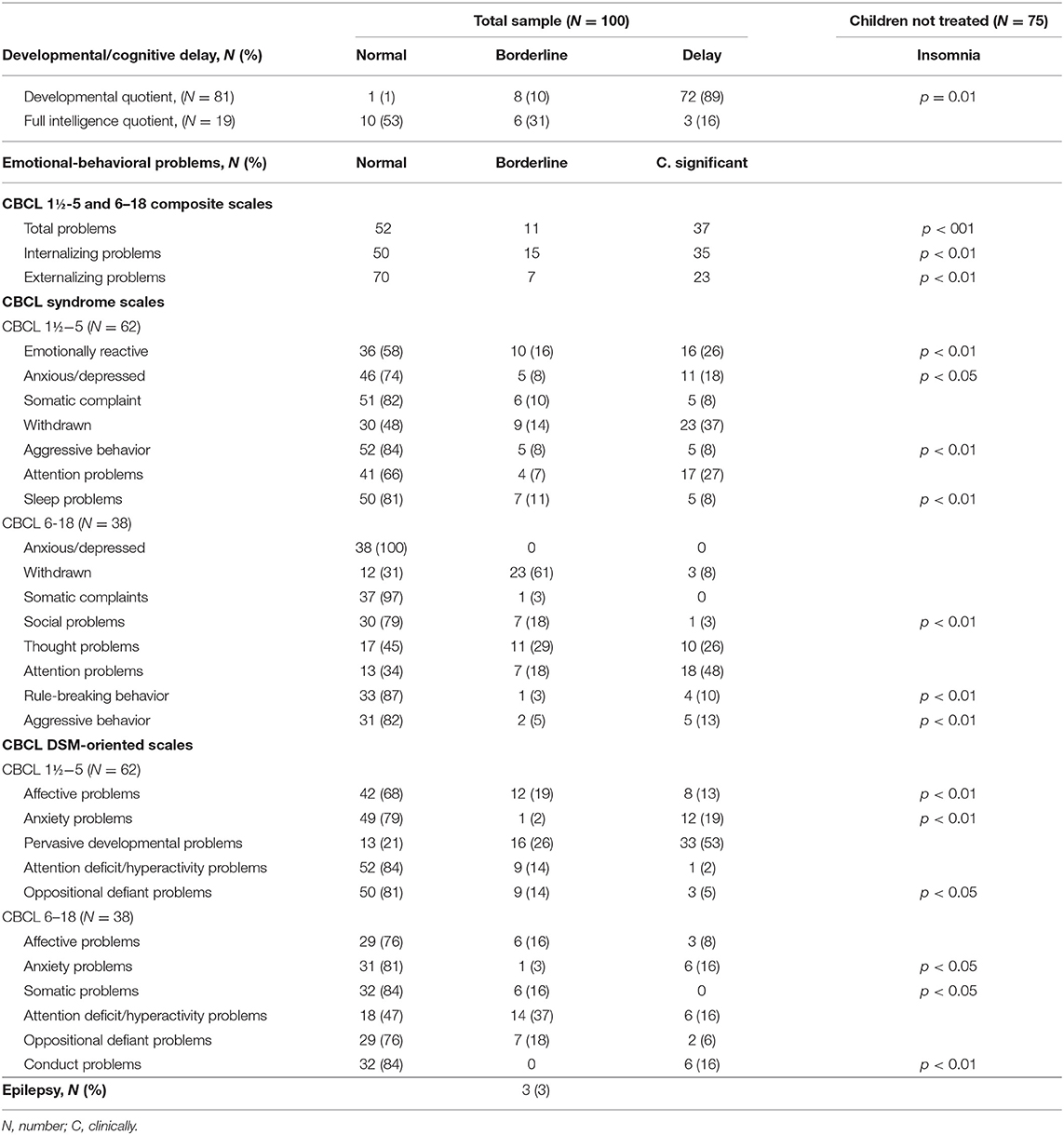
Table 3. Comorbidities of the sample.
Table 4 shows the findings of the Questionnaire on sleep behavior in the first years of life regarding sleep duration, habits and rituals, nocturnal awakenings and waking up time, and it shows the BEARS questionnaire in the 75 subjects not treated with melatonin.
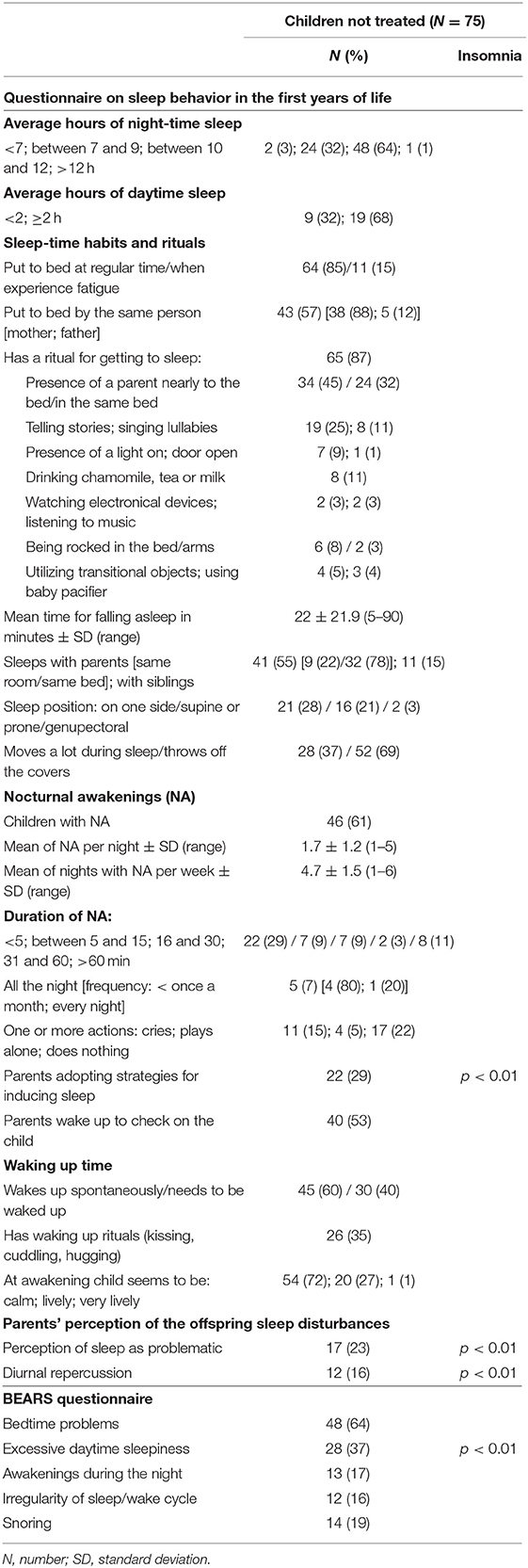
Table 4. Sleep characteristics according to the two sleep questionnaires.
Data collected from both questionnaires helped us to diagnose insomnia, according to DSM-V criteria, in 32 (43%) children: 17 subjects (53%) had difficulty in sleep onset, 5 (16%) difficulty in maintaining sleep due to frequent awakenings or problems returning to sleep after awakenings and 10 (31%) both disturbances. None of the children in our sample presented Breathing-Related Sleep Disorders or Parasomnias.
No sociodemographic data (age, sex, pregnancy, delivery, gestational age, and family variables) of children with ASD seemed to be correlated with the presence of insomnia, as well as the characteristics of neurological examination, the severity of ASD and the genetic/instrumental data.
Correlations between comorbid conditions and insomnia are summarized in Table 3. Specifically, we observed a statistically significant association between sleep disorder and a developmental or cognitive delay (p = 0.01). As regards emotional and behavioral difficulties, considering both CBCL 1½-5 and CBCL 6–18, statistical correlations were found between the presence of insomnia and the occurrence of internalizing, externalizing, and total problems (p < 0.01). Analyzing the syndrome scales, a statistically significant correlation was detected between sleep disturbance and an increased risk of emotionally reactive problems (p < 0.01), anxious/depressed problems (p < 0.05), aggressive behavior and sleep problems (p < 0.01) at CBCL 1½-5, and social problems, rule-breaking behavior, and aggressive behavior (p < 0.01) at CBCL 6–18. Moreover, insomnia correlated with the following DSM-oriented scales: affective problems (p < 0.01), anxiety problems (p < 0.01), and oppositional defiant problems (p < 0.05) at CBCL 1½-5, and anxiety problems (p < 0.05), somatic problems (p < 0.05), and conduct problems (p < 0.01) at CBCL 6–18. Epilepsy did not correlate with sleep disturbances.
Different sleep-time habits and rituals used both by the children themselves and by parents to favor the sleep or places where children sleep during the night did not correlate with the presence or absence of insomnia. However, we found a statistical correlation between the use of strategies and rituals adopted to induce sleep after nocturnal awakenings and the back to sleep (p < 0.01): in fact, children that did not have sleep rituals presented difficulties in going back to sleep.
According to the questionnaire on sleep behavior in the first years of life, 58 (77%) parents did not perceive their offspring sleep as problematic (in 40 cases there was not a sleep disturbance); the remaining 17 (23%) parents judged it as problematic (in 14 cases insomnia was confirmed). A statistically significant association between the presence of insomnia and parents' perception of sleep as problematic was found (p < 0.01). Diurnal repercussions, reported in 12 children (insomnia detected in 10 of them), correlated with the sleep disturbance (p < 0.01): in fact, children with insomnia seemed to be more aggressive and nervous during daytime activities. BEARS questionnaire also confirmed that children with insomnia seemed to be sleepier during the day (p < 0.01). The above correlations are reported in Table 4.
The PSI-SF revealed normal results in 60 (80%) cases, borderline in 5 (7%) and pathological in 10 (13%) at Total Stress Scale. At “Parental Distress” subscale we observed normal scores in 69 (92%) parents, borderline in 1 (1%) and pathological in 5 (7%); at “Parent-Child Dysfunctional Interaction” subscale normal results in 59 (78%) parents, borderline in 5 (7%), and 11 (15%) pathological; and at “Difficult Child” subscale normal scores in 57 (76%) parents, borderline in 7 (9%) and pathological in 11 (15%). No statistical correlation was found between sleep disturbances and PSI-SF total score and each subscale.
As declared in section Materials and Methods we evaluated the persistence of insomnia (already diagnosed at the time of the enrollment) in 25 subjects treated with melatonin (1–3 mg/die, 30 min before falling asleep at about 8.30 p.m., for at least 3 months) to induce sleep. At the time of the questionnaire, insomnia persisted in 10 (40%) cases, 8 (80%) of them assumed melatonin occasionally while 2 (20%) in association with risperidone. The remaining 15 (60%) children took regularly (every night) melatonin without other drugs and they did not present sleep disturbances after the beginning of the treatment. Comparing children who assumed melatonin with regularity and those who took it occasionally, we found a statistical correlation between the regular intake of the drug and the resolution of insomnia (p < 0.01).
The present study arises from the need to describe the sleep characteristics (duration, habits and rituals, and nocturnal awakenings) and the presence of a sleep disturbance in children affected by ASD, to evaluate any possible associated factors, parents' perception of the sleep disorder, and any possible consequences of sleep problems on the child and the family. Finally, we also explored the effect of melatonin on insomnia in a small subgroup of ASD children.
Our study confirms that insomnia is a hallmark of sleep disorder in ASD. Considering children treated with melatonin and those without any hypnotic drug, more than half (57 children, 57%) of our sample suffered from insomnia, specifically sleep onset problems and sleep settling issues, due to frequent awakenings or difficulties returning to sleep after awakenings; our data are in line with those of literature (2, 5, 55, 56). However, we did not observe other sleep disturbances, such as sleep-related breathing and movement disorders probably due to difficulties in making a diagnosis using questionnaires without polysomnography (56).
In accordance with literature (8), night sleep duration was between 9.0 and 12.00 h and the most common habits and rituals involved the presence of parents during the falling asleep phase and nocturnal awakenings in a higher percentage compared to literature (8). The reasons for co-sleeping in ASD subjects are different: firstly, the rate of sleep disturbances is high and consequently this increases the likelihood of wanting to sleep with parents. Moreover, parents themselves may think that the child needs more assistance during the night and therefore they may prefer to sleep with their child; finally the repetitive and limited behaviors characterizing ASD itself could prevent changing this habit (8). In our study there is no evidence that co-sleeping improves the sleep of children; it may be useful to implement behavioral therapies teaching parents the correct strategies to keep toward their children, for example avoiding responding to the child's disruptive bedtime behaviors (crying, calling out, and leaving the bedroom) as well as checking on the child, but only when he/she is showing the desired behaviors (quiet, calm, and in his/her bed) (57). No specific characteristics in bedtime routine or in the rituals performed during the night correlated with the absence of insomnia in our study; hence every behavioral therapy should be personalized keeping in mind the individuality of each child, and needs and preferences of parents, in order to create a balanced routine for the family.
Among comorbid conditions, developmental/cognitive delay and emotional/behavioral difficulties were associated with insomnia. The association between sleep disturbances and cognitive functioning is not well established because some studies reported an increase of sleep difficulties in children with ASD and cognitive deficit (2) while others the occurrence regardless of the cognitive functioning (58). Moreover, the direction of this relationship needs to be clarified (59): do sleep problems cause cognitive deficits or vice versa? Recent researches hypothesized that sleep is essential for optimizing cognitive development, memory and learning (31, 58) and that chronic sleep deprivation has negative effects on cognitive and academic performance (31, 41) probably influencing cerebral connectivity and creating aberrant neural pathways (60).
According to the literature (9, 32), our study revealed that children with insomnia were more likely to exhibit internalizing (as anxious/depressed problems), externalizing (aggressive/social problems and rule-breaking behavior) and total behavior difficulties compared to those without it. Anxiety and mood disorders may be associated with hyperarousal, intrusive thoughts and worries during the pre-sleep time, leading to difficulties in falling asleep and insomnia (9) and at the same time sleep loss may affect behavioral regulation and determine daytime fatigue (32), predisposing to aggression, property destruction (35) and violence (61). The association observed here in children with ASD between insomnia and aggression is of particular interest given the associations found by several authors between aggression and endogenous opioids and steroids in animal models, knowing that abnormalities of the opioid and steroid systems have been reported in ASD (62, 63). This suggests that there is a vulnerability for aggression in ASD, and insomnia may major this vulnerability for aggression or result from it.
In contrast with literature (64), epilepsy did not correlate with sleep disturbances; a possible explanation may be the limited number of subjects affected by epilepsy enrolled in the study.
Sleep rituals and strategies seemed to favor the back to sleep after a nocturnal awakening. According to literature data, sleep problems observed in ASD population may be related also to inadequate “sleep hygiene” (parenting related factors associated with the promotion of the child's sleep) (65), such as inconsistent bedtime routine, delayed or irregular bedtimes, access to electronic media devices (65). Although the exact mechanisms of sleep hygiene practices are still unclear (66), establishing some behavioral conditions, as the reduction of external stimulation, the increase in relaxation, and regular bedtime routine with little variability over nights may play an important role in favoring sleep (7).
In our study, parent's perception of their offspring sleep (judged as “problematic” or “not problematic”) correlated with the diagnosis of insomnia. Moreover, parents reported that sleep disorders have diurnal repercussions as being more aggressive and nervous during activities and excessive daily somnolence; this data confirms other previous findings (32, 67, 68). Interventions addressed to limit sleep disturbances in subjects with ASD improve behavioral problems (69, 70); hence, considering parents' perceptions and experiences of their children' sleep provides insightful information for the clinicians and it helps to identify additional factors that may contribute to insomnia and reduce the efficacy of interventions (71).
In contrast to our hypothesis, poor sleep did not affect parental mental health since no statistical differences were found between the stress levels of parents of children with and without insomnia. Conversely, literature documents that sleep disturbances in children with ASD increase parenting burden and family stress (72). An explanation could be related to the possibility of having developed resilience and adaptive coping strategies to manage difficulties parents face every day, reducing the perception of family distress (73). In fact, less than a third of parents reported being stressed. Another possible explanation could be the fact that parents did not answer authentically to the questionnaire aimed at investigating their challenges, because too focused on problems experienced by their child.
Although the high frequency of insomnia in our sample, only a small number of children took melatonin to favor sleep. The night-time administration of melatonin seemed to lead to improvements of the sleep disturbance in more than half of our cases, but its efficacy was observed in all the children that assumed it every day and without other medications. Melatonin appears to be useful for treatment of sleep disturbances in ASD (56), however its potential mechanism on poor sleep is not completely understood (74, 75). It may help to regulate the circadian rhythm, to act as sedative/hypnotic agent or to replace the melatonin deficiency observed in some ASD children (76). Melatonin may also contribute to reduce the levels of antioxidants (75, 77), particularly high in some children with ASD, and to regulate the synaptic plasticity, altered by an imbalance in excitatory and inhibitory systems (72–76).
The absence of any comparison group and of normative data for the two sleep questionnaires administered may represent potential limitations of the present study. We are aware of the difficulty to evaluate the clinical significance of our findings; however, we made diagnosis of insomnia according to the DSM-V criteria and we assessed comorbid conditions using standardized tests according to normative parameters.
In summary, the results from this study suggest that children affected by ASD showed high prevalence of sleep disturbances, in particular insomnia, which seemed to be associated with developmental/cognitive delay, emotional and behavior problems and poor sleep hygiene, without increasing the family stress. Regular melatonin administration may ameliorate sleep disturbances. As congruence, a screening for sleep disturbance in children with ASD is necessary to integrate sleep interventions in the treatment plan.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comitato Etico di Brescia, ID Number 4085. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Luisa Bonini, Angela Merlini, Laura Pansera, Laura Malerba, and Filippo Gitti, Unit of Child Neurology and Psychiatry, ASST Spedali Civili of Brescia, Brescia, Italy; Silvia Saottini, Department of Clinical and Experimental Sciences, University of Brescia, Brescia, Italy.
JG, EL, and LV wrote the article. LV, PM, and AE collected data and administered the sleep questionnaires. JG, PM, and EF designed the study. SC performed the statistical analysis. All authors contributed to the article, reviewed the manuscript, and approved the submitted version.
Università degli Studi di Brescia provides fees for open access publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors are grateful to children affected by ASD and their families for participation to the study.
1. ^Hollingshead AB. Four factor index of social status. (1975) Unpublished manuscript, Yale University, New Haven, CT.
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Arlington, VA: American Psychiatric Publishing (2013).
2. Richdale AL, Schreck KA. Sleep problems in autism spectrum disorders: prevalence, nature, & possible biopsychosocial aetiologies. Sleep Med Rev. (2009) 13:403–11. doi: 10.1016/j.smrv.2009.02.003
3. Hodge D, Carollo TM, Lewin M, Hoffman CD, Sweeney DP. Sleep patterns in children with and without autism spectrum disorders: developmental comparisons. Res Dev Disabil. (2014) 35:1631–8. doi: 10.1016/j.ridd.2014.03.037
4. Wiggs L, Stores G. Severe sleep disturbance and daytime challenging behaviour in children with severe learning disabilities. J Intellect Disabil Res. (1996) 40:518–28. doi: 10.1111/j.1365-2788.1996.tb00662.x
5. Gail Williams P, Sears LL, Allard A. Sleep problems in children with autism. J Sleep Res. (2004) 13:265–8. doi: 10.1111/j.1365-2869.2004.00405.x
6. Patzold LM, Richdale AL, Tonge BJ. An investigation into sleep characteristics of children with autism and Asperger's disorder. J Paediatr Child Health. (1998) 34:528–33. doi: 10.1046/j.1440-1754.1998.00291.x
7. Singh K, Zimmerman AW. Sleep in autism spectrum disorder and attention deficit hyperactivity disorder. Semin Pediatr Neurol. (2015) 22:113–25. doi: 10.1016/j.spen.2015.03.006
8. Liu X, Hubbard JA, Fabes RA, Adam JB. Sleep disturbances and correlates of children with autism spectrum disorders. Child Psychiatry Hum Dev. (2006) 37:179–91. doi: 10.1007/s10578-006-0028-3
9. Mazzone L, Postorino V, Siracusano M, Riccioni A, Curatolo P. The relationship between sleep problems, neurobiological alterations, core symptoms of autism spectrum disorder, and psychiatric comorbidities. J Clin Med. (2018) 7:102. doi: 10.3390/jcm7050102
10. Yang Z, Matsumoto A, Nakayama K, Jimbo EF, Kojima K, Nagata K, et al. Circadian-relevant genes are highly polymorphic in autism spectrum disorder patients. Brain Dev. (2016) 38:91–9. doi: 10.1016/j.braindev.2015.04.006
11. Kulman G, Lissoni P, Rovelli F, Roselli MG, Brivio F, Sequeri P. Evidence of pineal endocrine hypofunction in autistic children. Neuro Endocrinol Lett. (2000) 21:31–4.
12. Nir I, Meir D, Zilber N, Knobler H, Hadjez J, Lerner Y. Brief report: circadian melatonin, thyroid-stimulating hormone, prolactin, and cortisol levels in serum of young adults with autism. J Autism Dev Disord. (1995) 25:641–54. doi: 10.1007/BF02178193
13. Tordjman S, Anderson GM, Pichard N, Charbuy H, Touitou Y. Nocturnal excretion of 6-sulphatoxymelatonin in children and adolescents with autistic disorder. Biol Psychiatry. (2005) 57:134–8. doi: 10.1016/j.biopsych.2004.11.003
14. Wright B, Sims D, Smart S, Alwazeer A, Alderson-Day B, Allgar V, et al. Melatonin versus placebo in children with autism spectrum conditions and severe sleep problems not amenable to behaviour management strategies: a randomised controlled crossover trial. J Autism Dev Disord. (2011) 41:175–84. doi: 10.1007/s10803-010-1036-5
15. Chaste P, Clement N, Mercati O, Guillaume JL, Delorme R, Botros HG, et al. Identification of pathway-biased and deleterious melatonin receptor mutants in autism spectrum disorders and in the general population. PLoS ONE. (2010) 5:e11495. doi: 10.1371/journal.pone.0011495
16. Gottesmann C. GABA mechanisms and sleep. Neuroscience. (2002) 111:231–9. doi: 10.1016/S0306-4522(02)00034-9
17. McCauley JL, Olson LM, Delahanty R, Amin T, Nurmi EL, Organ EL, et al. A linkage disequilibrium map of the 1-Mb 15q12 GABA(A) receptor subunit cluster and association to autism. Am J Med Genet B Neuropsychiatr Genet. (2004) 131B:51–9. doi: 10.1002/ajmg.b.30038
18. Wimpory D, Nicholas B, Nash S. Social timing, clock genes and autism: a new hypothesis. J Intellect Disabil Res. (2002) 46:352–8. doi: 10.1046/j.1365-2788.2002.00423.x
19. Wiggs L, Stores G. Sleep patterns and sleep disorders in children with autistic spectrum disorders: insights using parent report and actigraphy. Dev Med Child Neurol. (2004) 46:372–80. doi: 10.1017/S0012162204000611
20. Souders MC, Mason TBA, Valladares O, Bucan M, Levy SE, Mandell DS, et al. Sleep behaviors and sleep quality in children with autism spectrum disorders. Sleep. (2009) 32:1566–78. doi: 10.1093/sleep/32.12.1566
21. Schreck KA, Williams K. Food preferences and factors influencing food selectivity for children with autism spectrum disorders. Res Dev Disabil. (2006) 27:353–63. doi: 10.1016/j.ridd.2005.03.005
22. Panju S, Brian J, Dupuis A, Anagnostou E, Kushki A. Atypical sympathetic arousal in children with autism spectrum disorder and its association with anxiety symptomatology. Mol Autism. (2015) 6:64. doi: 10.1186/s13229-015-0057-5
23. Spielman AJ, Caruso LS, Glovinsky PB. A behavioral perpective on insomnia treatment. Psychiatr Clin North Am. (1987) 10:541–53. doi: 10.1016/S0193-953X(18)30532-X
24. Seo WS. An update on the cause and treatment of sleep disturbance in children and adolescents with autism spectrum disorder [published online ahead of print, 2021 Sep 13]. Yeungnam Univ J Med. (2021) 38:275–81. doi: 10.12701/yujm.2021.01410
25. Barone I, Hawks-Mayer H, Lipton JO. Mechanisms of sleep and circadian ontogeny through the lens of neurodevelopmental disorders. Neurobiol Learn Mem. (2019) 160:160–72. doi: 10.1016/j.nlm.2019.01.011
26. Chen H, Yang T, Chen J, Chen L, Dai Y, Zhang J, et al. Sleep problems in children with autism spectrum disorder: a multicenter survey. BMC Psychiatry. (2021) 21:406. doi: 10.1186/s12888-021-03405-w
27. Maquet P. The role of sleep in learning and memory. Science. (2001) 294:1048–52. doi: 10.1126/science.1062856
28. Gozal D. Sleep-disordered breathing and school performance in children. Pediatrics. (1998) 102:616–20. doi: 10.1542/peds.102.3.616
29. Mazurek MO, Petroski GF. Sleep problems in children with autism spectrum disorder: examining the contributions of sensory over-responsivity and anxiety. Sleep Med. (2015) 16:270–9. doi: 10.1016/j.sleep.2014.11.006
30. Mannion A, Leader G. Sleep problems in autism spectrum disorder: a literature review. Rev J Autism Devel Disord. (2014) 1:101–9. doi: 10.1007/s40489-013-0009-y
31. Tesfaye R, Wright N, Zaidman-Zait A, Bedford R, Zwaigenbaum L, Kerns C, et al. Investigating longitudinal associations between parent reported sleep in early childhood and teacher reported executive functioning in school-aged children with autism. Sleep. (2021) 44:zsab122. doi: 10.1093/sleep/zsab122
32. Mazurek MO, Sohl K. Sleep and behavioral problems in children with autism spectrum disorder. J Autism Dev Disord. (2016) 46:1906–15. doi: 10.1007/s10803-016-2723-7
33. Adkins KW, Molloy C, Weiss SK, Reynolds A, Goldman SE, Burnette C, et al. Effects of a standardized pamphlet on insomnia in children with autism spectrum disorders. Pediatrics. (2012) 130(Suppl. 2):S139–44. doi: 10.1542/peds.2012-0900K
34. Sikora DM, Johnson K, Clemons T, Katz T. The relationship between sleep problems and daytime behavior in children of different ages with autism spectrum disorders. Pediatrics. (2012) 130(Suppl. 2):S83–90. doi: 10.1542/peds.2012-0900F
35. Adams HL, Matson JL, Jang J. The relationship between sleep problems and challenging behavior among children and adolescents with autism spectrum disorder. Res Autism Spectr Disord. (2014) 8:1024–30. doi: 10.1016/j.rasd.2014.05.008
36. Krakowiak P, Goodlin-Jones B, Hertz-Picciotto I, Croen LA, Hansen RL. Sleep problems in children with autism spectrum disorders, developmental delays, and typical development: a population-based study. J Sleep Res. (2008) 17:197–206. doi: 10.1111/j.1365-2869.2008.00650.x
37. Kuhn DE, Matson JL. Assessment of feeding and mealtime behavior problems in persons with mental retardation. Behav Modif. (2004) 28:638–48. doi: 10.1177/0145445503259833
38. Schreck KA, Mulick JA, Smith AF. Sleep problems as possible predictors of intensified symptoms of autism. Res Dev Disabil. (2004) 25:57–66. doi: 10.1016/j.ridd.2003.04.007
39. Souders MC, Zavodny S, Eriksen W, Sinko R, Connell J, Kerns C, et al. Sleep in children with autism spectrum disorder. Curr Psychiatry Rep. (2017) 19:34. doi: 10.1007/s11920-017-0782-x
40. Malow BA, Byars K, Johnson K, Weiss S, Bernal P, Goldman SE, et al. A practice pathway for the identification, evaluation, and management of insomnia in children and adolescents with autism spectrum disorders. Pediatrics. (2012) 130(Suppl. 2):S106–24. doi: 10.1542/peds.2012-0900I
41. Taylor MA, Schreck KA, Mulick JA. Sleep disruption as a correlate to cognitive and adaptive behavior problems in autism spectrum disorders. Res Dev Disabil. (2012) 33:1408–17. doi: 10.1016/j.ridd.2012.03.013
42. Dabrowska A, Pisula E. Parenting stress and coping styles in mothers and fathers of pre-school children with autism and Down syndrome. J Intellect Disabil Res. (2010) 54:266–80. doi: 10.1111/j.1365-2788.2010.01258.x
43. Liu R, Dong H, Wang Y, Lu X, Li Y, Xun G, et al. Sleep problems of children with autism may independently affect parental quality of life. Child Psychiatry Hum Dev. (2021) 52:488–99. doi: 10.1007/s10578-020-01035-z
44. Lord C, Rutter M, DiLavore P, Risi S, Gotham K, Bishop SL. Autism Diagnostic Observation Schedule. 2nd ed. Torrence, CA: Western Psychological Services (2012).
45. Amiet C, Gourfinkel-An I, Laurent C, Bodeau N, Génin B, Leguern E, et al. Does epilepsy in multiplex autism pedigrees define a different subgroup in terms of clinical characteristics and genetic risk? Mol Autism. (2013) 4:47. doi: 10.1186/2040-2392-4-47
46. Luiz DM, Kotras N, Barnard A, Knoesen N. Technical Manual of the Griffiths Mental Development Scales–Extended Revised (GMDS–ER). Amersham: ARICD (2004).
47. Wechsler D. Wechsler Intelligence Scale for Children. 4th ed. San Antonio, TX: Harcourt Assessment (2003).
48. Achenbach TM, Rescorla LA. Manual for the ASEBA preschool forms and profiles: An Integrated System of Multi-Informant Assessment. Burlington, VT: University of Vermont, Department of Psychiatry (2000).
49. Frigerio A, Cozzi P, Pastore V, Molteni M, Borgatti R, Montirosso R. La valutazione dei problemi emotivo comportamentali in un campione italiano di bambini in eta prescolare attraverso la Child Behavior Checklist e il Caregiver Teacher Report Form. Infanzia e adolescenza. (2006) 5:24–37. doi: 10.1710/162.1771
50. Achenbach TM, Rescorla LA. Manual for the ASEBA School-Age Forms & Profiles: Child Behavior Checklist for Ages 6-18, Teacher's Report Form, Youth Self-Report: An Integrated System of Multi-Informant Assessment. Burlington: University of Vermont, Research Center for Children Youth & Families (2001).
51. Fazzi E, Zaccagnino M, Capsoni C, Orcesi S, Spada G, Cavallini A, et al. A questionnaire on sleep behaviour in the first years of life: preliminary results from a normative sample. Funct Neurol. (2006) 21:151–8.
52. Mindell JA, Owens JA. Sleep problems in pediatric practice: clinical issues for the pediatric nurse practitioner. J Pediatr Health Care. (2003) 17:324–31. doi: 10.1016/S0891-5245(03)00215-3
53. Owens JA, Dalzell V. Use of the ‘BEARS' sleep screening tool in a pediatric residents' continuity clinic: a pilot study. Sleep Med. (2005) 6:63–9. doi: 10.1016/j.sleep.2004.07.015
54. Abidin RR. Parenting Stress Index. 3rd ed. Professional Manual Lutz, FL: Psychological Assessment Resources Inc (1995).
55. Esposito D, Belli A, Ferri R, Bruni O. Sleeping without prescription: management of sleep disorders in children with autism with non-pharmacological interventions and over-the-counter treatments. Brain Sci. (2020) 10:441. doi: 10.3390/brainsci10070441
56. Guénolé F, Godbout R, Nicolas A, Franco P, Claustrat B, Baleyte JM. Melatonin for disordered sleep in individuals with autism spectrum disorders: systematic review and discussion. Sleep Med Rev. (2011) 15:379–87. doi: 10.1016/j.smrv.2011.02.001
57. Grigg-Damberger M. Ralls F. Treatment strategies for complex behavioral insomnia in children with neurodevelopmental disorders. Curr Opin Pulm Med. (2013) 19:616–25. doi: 10.1097/MCP.0b013e328365ab89
58. Kotagal S. Broomall E. Sleep in children with autism spectrum disorder. Pediatr Neurol. (2012) 47:242–51. doi: 10.1016/j.pediatrneurol.2012.05.007
59. Al Backer NB, Jaafar M, Habibullah H, Bashir S. The Relationship between sleep and cognitive performance in autism spectrum disorder (ASD): a pilot study. Children. (2018) 5:153. doi: 10.3390/children5110153
60. Mughal R, Hill CM, Joyce A, Dimitriou D. Sleep and cognition in children with fetal alcohol spectrum disorders (FASD) and children with autism spectrum disorders (ASD). Brain Sci. (2020) 10:863. doi: 10.3390/brainsci10110863
61. Kamphuis J, Meerlo P, Koolhaas JM, Lancel M. Poor sleep as a potential causal factor in aggression and violence. Sleep Med. (2012) 13:327–34. doi: 10.1016/j.sleep.2011.12.006
62. Le Roy I, Mortaud S, Tordjman S, Donsez-Darcel E, Carlier M, Degrelle H, et al. Genetic correlation between steroid sulfatase concentration and initiation of attack behavior in mice. Behav Genet. (1999) 29:131–6. doi: 10.1023/A:1021664607131
63. Tordjman S, Carlier M, Cohen D, Cesselin F, Bourgoin S, Colas-Linhart N, et al. Aggression and the three opioid families (endorphins, enkephalins, and dynorphins) in mice. Behav Genet. (2003) 33:529–36. doi: 10.1023/A:1025774716976
64. Giannotti F, Cortesi F, Cerquiglini A, Miraglia D, Vagnoni C, Sebastiani T, et al. An investigation of sleep characteristics, EEG abnormalities and epilepsy in developmentally regressed and non-regressed children with autism. J Autism Dev Disord. (2008) 38:1888–97. doi: 10.1007/s10803-008-0584-4
65. van der Heijden KB, Stoffelsen RJ, Popma A, Swaab H. Sleep, chronotype, and sleep hygiene in children with attention-deficit/hyperactivity disorder, autism spectrum disorder, and controls. Eur Child Adolesc Psychiatry. (2018) 27:99–111. doi: 10.1007/s00787-017-1025-8
66. Jan JE, Owens JA, Weiss MD, Johnson KP, Wasdell MB, Freeman RD, et al. Sleep hygiene for children with neurodevelopmental disabilities. Pediatrics. (2008) 122:1343–50. doi: 10.1542/peds.2007-3308
67. Malow BA, Marzec ML, McGrew SG, Wang L, Henderson LM, Stone WL. Characterizing sleep in children with autism spectrum disorders: a multidimensional approach. Sleep. (2006) 29:1563–71. doi: 10.1093/sleep/29.12.1563
68. Johnson CR, Smith T, DeMand A, Lecavalier L, Evans V, Gurka M, et al. Exploring sleep quality of young children with autism spectrum disorder and disruptive behaviors. Sleep Med. (2018) 44:61–6. doi: 10.1016/j.sleep.2018.01.008
69. Goldman SE, Adkins KW, Calcutt MW, Carter MD, Goodpaster RL, Wang L, et al. Melatonin in children with autism spectrum disorders: endogenous and pharmacokinetic profiles in relation to sleep. J Autism Dev Disord. (2014) 44:2525–35. doi: 10.1007/s10803-014-2123-9
70. Papadopoulos N, Sciberras E, Hiscock H, Mulraney M, McGillivray J, Rinehart N. The efficacy of a brief behavioral sleep intervention in school-aged children with ADHD and comorbid autism spectrum disorder. J Atten Disord. (2019) 23:341–50. doi: 10.1177/1087054714568565
71. Kirkpatrick B, Gilroy SP, Leader G. Qualitative study on parents' perspectives of the familial impact of living with a child with autism spectrum disorder who experiences insomnia. Sleep Med. (2019) 62:59–68. doi: 10.1016/j.sleep.2019.01.032
72. Johnson KP. Zarrinnegar P. Autism spectrum disorder and sleep child. Adolesc Psychiatr Clin N Am. (2021) 30:195–208. doi: 10.1016/j.chc.2020.08.012
73. Pyszkowska A, Wrona K. Self-compassion, ego-resiliency, coping with stress and the quality of life of parents of children with autism spectrum disorder. PeerJ. (2021) 9:e11198. doi: 10.7717/peerj.11198
74. Rossignol DA, Frye RE. Mitochondrial dysfunction in autism spectrum disorders: a systematic review and meta-analysis. Mol Psychiatry. (2012) 17:290–314. doi: 10.1038/mp.2010.136
75. Lalanne S, Fougerou-Leurent C, Anderson GM, Schroder CM, Nir T, Chokron S, et al. Melatonin: from pharmacokinetics to clinical use in autism spectrum disorder. Int J Mol Sci. (2021) 22:1490. doi: 10.3390/ijms22031490
76. Melke J, Goubran Botros H, Chaste P, Betancur C, Nygren G, Anckarsäter H, et al. Abnormal melatonin synthesis in autism spectrum disorders. Mol Psychiatry. (2008) 13:90–8. doi: 10.1038/sj.mp.4002016
Keywords: autism spectrum disorder, sleep disturbance, insomnia, parent stress, melatonin
Citation: Galli J, Loi E, Visconti LM, Mattei P, Eusebi A, Calza S, Fazzi E and ASD Collaborative Group (2022) Sleep Disturbances in Children Affected by Autism Spectrum Disorder. Front. Psychiatry 13:736696. doi: 10.3389/fpsyt.2022.736696
Received: 05 July 2021; Accepted: 24 January 2022;
Published: 17 February 2022.
Edited by:
Jean Marc Guile, University of Picardie Jules Verne, FranceReviewed by:
Silvana Markovska-Simoska, Macedonian Academy of Sciences and Arts, North MacedoniaCopyright © 2022 Galli, Loi, Visconti, Mattei, Eusebi, Calza, Fazzi and ASD Collaborative Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessica Galli, amVzc2ljYS5nYWxsaUB1bmlicy5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.