 Percy Herrera-Añazco1,2,3
Percy Herrera-Añazco1,2,3 Diego Urrunaga-Pastor3,4
Diego Urrunaga-Pastor3,4 Vicente A. Benites-Zapata2,5*
Vicente A. Benites-Zapata2,5* Guido Bendezu-Quispe6
Guido Bendezu-Quispe6 Carlos J. Toro-Huamanchumo5,7
Carlos J. Toro-Huamanchumo5,7 Adrian V. Hernandez8,9
Adrian V. Hernandez8,9- 1Universidad Privada San Juan Bautista, Escuela de enfermería, Lima, Peru
- 2Red Internacional en Salud Colectiva y Salud Intercultural, Mexico, Mexico
- 3Instituto de Evaluación de Tecnologías en Salud e Investigación–IETSI, Dirección de Investigación en Salud, EsSalud, Lima, Peru
- 4Universidad Científica del Sur, Facultad de Ciencias de la Salud, Lima, Peru
- 5Universidad San Ignacio de Loyola, Unidad para la Generación y Síntesis de Evidencias en Salud, Lima, Peru
- 6Universidad Privada Norbert Wiener, Centro de Investigación Epidemiológica en Salud Global, Lima, Peru
- 7Clínica Avendaño, Unidad de Investigación Multidisciplinaria, Lima, Peru
- 8Health Outcomes, Policy and Evidence Synthesis (HOPES) Group, University of Connecticut School of Pharmacy, Storrs, CT, United States
- 9Universidad San Ignacio de Loyola, Unidad de Revisiones Sistemáticas y Metaanálisis, Guías de Práctica Clínica y Evaluaciones Tecnológicas Sanitarias, Lima, Peru
Background: Previous studies have suggested that the pandemic impact on mental health could vary according to gender. We aimed to evaluate the gender influence in the prevalence of depressive and anxiety symptoms in Latin American and the Caribbean (LAC) countries in the first stage of the COVID-19 pandemic.
Methods: We conducted a secondary analysis employing the Facebook–COVID-19 Symptom Survey developed by the University of Maryland. We categorized gender as men, women, and non-binary. The outcomes were the presence of anxiety or depressive symptoms, measured with two adapted questions extracted from the Kessler Psychological Distress Scale (K10). We used generalized linear models from the Poisson family, considering the survey's complex sampling. We calculated crude and adjusted prevalence ratios (PR) with their 95% confidence intervals (95% CI) and explored interactions with gender using the adjusted Wald test.
Results: We included 1,338,320 adults from LAC countries; 48.0, 50.6, and 1.4% were men, women, and non-binary participants, respectively. The overall prevalence of anxiety or depressive symptoms was 44.8 and 46.6%, respectively. We found interactions between gender and the rest of the independent variables. In the non-binary group, the association between age and anxiety symptomatology was lost after an age of 55 years. Furthermore, whereas living in a town was associated with a lower prevalence of anxiety and depression symptomatology in men and women, this did not happen among non-binary individuals. Compliance with physical distancing was associated with a lower prevalence of anxiety and depression symptomatology among women (anxiety: PRa = 0.98; 95% CI = 0.97–0.99; p < 0.001, depression: PRa = 0.96; 95% CI = 0.95–0.97; p < 0.001) and only anxiety in non-binary participants (anxiety: PRa = 0.92; 95% CI = 0.88–0.98; p = 0.005). This was not evidenced among men participants (anxiety: PRa = 0.99; 95% CI = 0.96–1.01; p = 0.199, depression: PRa = 0.98; 95% CI = 0.96–1.00; p = 0.084). In addition, compliance with handwashing was associated with a higher prevalence of anxiety symptomatology among men (PRa = 1.06; 95% CI = 1.05–1.11; p < 0.001) and women participants (PRa = 1.03; 95% CI = 1.01–1.05; p = 0.016).
Conclusion: Approximately 4 out of 10 participants had anxiety or depressive symptoms. Women and non-binary gender people had more symptoms of anxiety or depression. The factors associated with these symptoms varied according to gender. It is essential to evaluate gender-related strategies to improve mental health during the COVID-19 pandemic.
Introduction
The COVID-19 pandemic produced substantial adjustments worldwide in people's lifestyles and catastrophic costs to nation's economies (1, 2). To lessen the impact of the pandemic, national quarantines were initiated in the first months of the crisis in the Latin American and the Caribbean (LAC) countries, in order to expand the care capacity of the health systems of these nations, which are characterized by problems of governance and infrastructure, and a lack of qualified human resources limiting patient care during the peak of the pandemic (3–6).
Although not present in LAC, in recent decades, there have been outbreaks of viral infections that have required quarantines in some Asian countries, which increased the presence of factors associated with stress and anxiety described during these periods of quarantine (7–11). These factors include the risk of being infected, death and infection of relatives and friends, feeling of loneliness and social isolation, physical and emotional fatigue of health workers, massive loss of employment, financial insecurity and poverty, and infodemic (12–14). Previous studies involving infected patients and people in quarantine found significant levels of psychological distress, hopelessness, anxiety, depression, anger, and fear of contagion (7–11). Likewise, a meta-analysis involving 25 studies developed in the course of severe acute respiratory syndrome (SARS) and Middle Eastern respiratory syndrome (MERS) outbreaks, both part of the coronavirus family, described that patients experienced significant effects such as anxiety and lack of sleep (7).
During the COVID-19 quarantine, a rise in the prevalence of anxiety and depression symptoms has been reported in comparison with the prevalence in general population prior to the pandemic (15). Several systematic reviews and meta-analyses show that the prevalence of anxiety and depressive symptoms varies between 6.33 and 50.9% and 14.6 and 48.3%, respectively, during the peak of the pandemic (16–23). Although previous studies (15, 24) and studies performed during the pandemic (16, 18, 23) have suggested that women may be more affected by symptoms of anxiety and depression than men, this does not correlate with some systematic reviews during the COVID-19 peak (19, 20), and some studies have even found that men have more anxiety symptoms (25). These controversial findings could be due to sociocultural aspects that do not allow extrapolation of these results in LAC countries. Similarly, people of non-binary gender have a high prevalence of disorders related to mental health (26). A multicenter study in countries in Europe and Southeast Asia suggested that mental health disorders increased during the pandemic (27). However, as with results in women, sociocultural aspects do not allow their extrapolation in countries in Latin America.
Although some studies that evaluate mental health, including depression and anxiety, during the pandemic in the Latin American countries such as Argentina (28), Brazil (29), Mexico (30), and Ecuador have been published (31), the effect of gender on the prevalence of depressive and anxiety symptoms during the pandemic in the LAC countries has not been evaluated. Therefore, our objective was to evaluate this association in the LAC countries during the first stage of the COVID-19 pandemic.
Methods
Design and Study Area
We carried out a secondary analysis of a database generated by social network Facebook (Facebook, Inc.) and the University of Maryland. This database was constructed based on a virtual survey, to obtain relevant information at the population level within the context of the COVID-19 pandemic. The survey included five modules: sociodemographic characteristics, contact report, general health, mental health, and economic security throughout the pandemic. It was initially conducted on April 23, 2020 and was translated and adapted according to the regions that use Facebook (32). We published a previous study using this database (33), in which the methodology was described in greater detail.
Population and Sample
The population for this study included users of the Facebook platform over 18 years of age from the LAC countries, which corresponded to 1,440,586 people from 20 countries. People who answered the modules of mental health and sociodemographic characteristics were considered for the analysis, and our exclusion criterion was the absence of complete information related to the variables of interest. The final sample analyzed included 1,338,320 participants. The analysis period comprised surveys from April 23 to May 23, 2020.
Variables and Procedure
Outcomes
Depressive Symptomatology
This was evaluated using one adapted question from the Kessler Psychological Distress Scale (K10): “In the past seven days, how often did you feel depressed?” This question allowed five answers (all of the time, most of the time, some of the time, a little of the time, and none of the time) (34). The variable was dichotomized as absence of depressive symptoms when the selected answer was “none of the time” and presence of depressive symptoms in any of the four remaining options.
Anxiety Symptomatology
This was evaluated using the K10 adapted question: “During the last seven days, how often did you feel so nervous that nothing could calm you down?” This question allowed five possible answers (all of the time, most of the time, some of the time, a little of the time, and none of the time) (34). This variable was dichotomized considering the absence of anxiety symptoms as none of the time and the presence of anxiety symptoms as any of the four remaining options.
The K10 is a short scale that is easily applied by first-level care personnel and has been used in different studies at the population level. This scale has a Spanish translation and has been applied in various studies in Spain, Colombia, Mexico, and Peru (34, 35), making it an appropriate instrument for the purposes of this research.
Independent Variables
Sociodemographic information was included and categorized as gender (categorized as male, female, and non-binary), age (presented as 18–24, 25–34, 35–44, 45–54, 55–64, 65–74, and 75 or more years), and area of residence (town, rural area, and city).
Likewise, suspicious symptoms of COVID-19 were included as a covariate, defined as the presence of three or more symptoms compatible with an acute infection of COVID-19 (cough, fever, loss of smell, fatigue, chest pain, headache, coryza, respiratory distress, eye pain, sore throat, muscle pain, and nausea) in line with the World Health Organization (WHO) definition of a suspected case (36).
In addition, we considered as covariate the compliance with the principal community mitigation strategies (CMS) (physical distancing, washing of hands, and mask using). Compliance with physical distancing was stablished as not having direct contact (even kissing, touching, hugging, and hand shaking) in the last 24 h for more than 1 min and within 2 m of anyone that does not share the same household. Handwashing compliance was defined as a report of at least one handwash after being in public during the last 7 days. Likewise, compliance with the use of a mask was defined as wearing a mask at least once in public within the prior 7 days.
Food insecurity was evaluated with the question: “How worried are you about having enough to eat in the next week?” which allowed the following responses: very worried, somewhat worried, not too worried, and not worried at all. The first three options were defined as a presence of food insecurity.
The fear that the participant or a member of the participant's family could fall seriously ill from COVID-19 was also included as a covariate and was assessed with the following question: “How worried are you that you or someone in your immediate family might become seriously ill from coronavirus (COVID-19)?,” and its four probable answers: very worried, somewhat worried, not too worried, and not worried at all. Then we stablished “not worried at all” as the lack of fear that the participant or any member of the participant's family could be affected by COVID-19 and any of the other three options as the presence of this condition.
Statistical Analysis
The database was downloaded in Microsoft Excel sheets and imported into the statistical software Stata v14.0 (StataCorp, TX, USA). All analyses considered the survey's complex sampling via the “svy” command.
Qualitative variables were described using weighted proportions according to complex sampling, with their 95% confidence intervals (95% CI) and absolute frequencies. The bivariate analysis between the outcomes (depression and anxiety symptomatology) and the covariates were performed using the Chi-squared test with Rao–Scott correction taking into account the survey's complex sampling. To explore factors associated with anxiety or depression symptomatology, we employed generalized linear models of the Poisson family with logarithmic link function. Crude and adjusted prevalence ratios (PR) and 95% CIs were estimated. In the adjusted model, we included only the variables with a statistically significant p-value (p < 0.05) obtained from the crude model. In addition, we evaluated the possible interaction of gender using the adjusted Wald test.
Ethical Aspects
Authorization was obtained from the University of Maryland to carry out the study and the institution that provided access to the analyzed database. The database was downloaded without identifiers of the survey participants, safeguarding the non-identification of participants.
Results
Characteristics of the Study Population
We analyzed the data of 1,338,320 adults from the LAC countries who answered the survey during April–May 2020. A total of 48.0% (n = 590,950) of the participants were men, while 50.6% (n = 732,701) and 1.4% (n = 14,669) were women and non-binary, respectively. Among the participants, 61.5% (n = 1,012,541) were <45 years of age. Suspected symptoms of COVID-19 were described in 18.6% (n = 280,168), and 75.8% (n = 1,028,162) reported food insecurity. Additionally, 92.3% (n = 1,251,992) reported feeling worried about falling seriously ill or that a family member would fall seriously ill from COVID-19. The prevalence of anxiety and depressive symptoms was 44.8% (n = 640,418) and 46.6% (n = 678,932), respectively (Table 1). The bivariate analysis showed statistically significant differences among anxiety symptoms or depressive symptomatology and the variables of interest (Table 2).
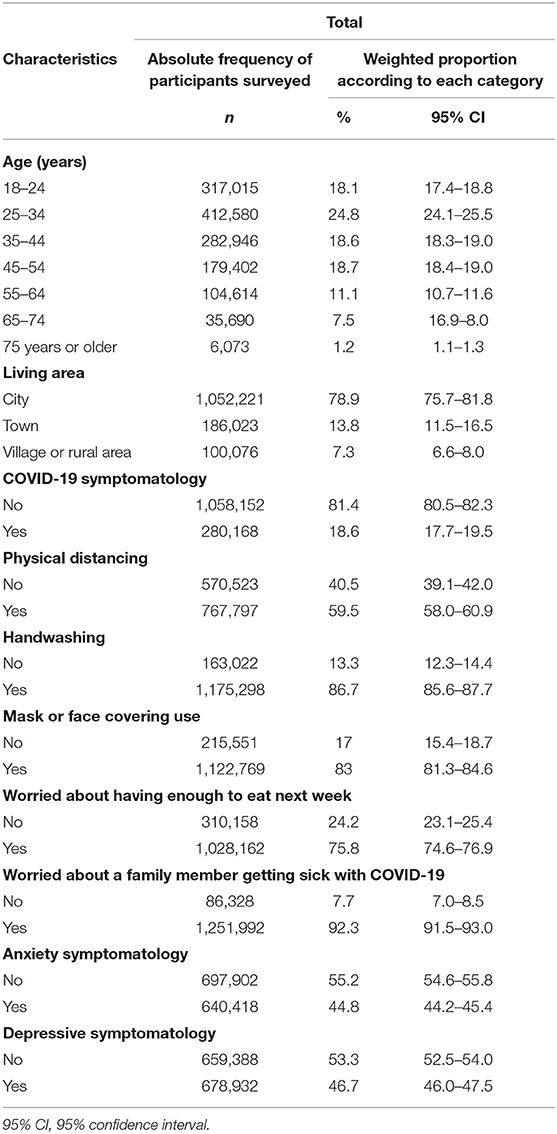
Table 1. Descriptive and bivariate analysis of the study sample characteristics (n = 1,338,320; N = 11,524,713).
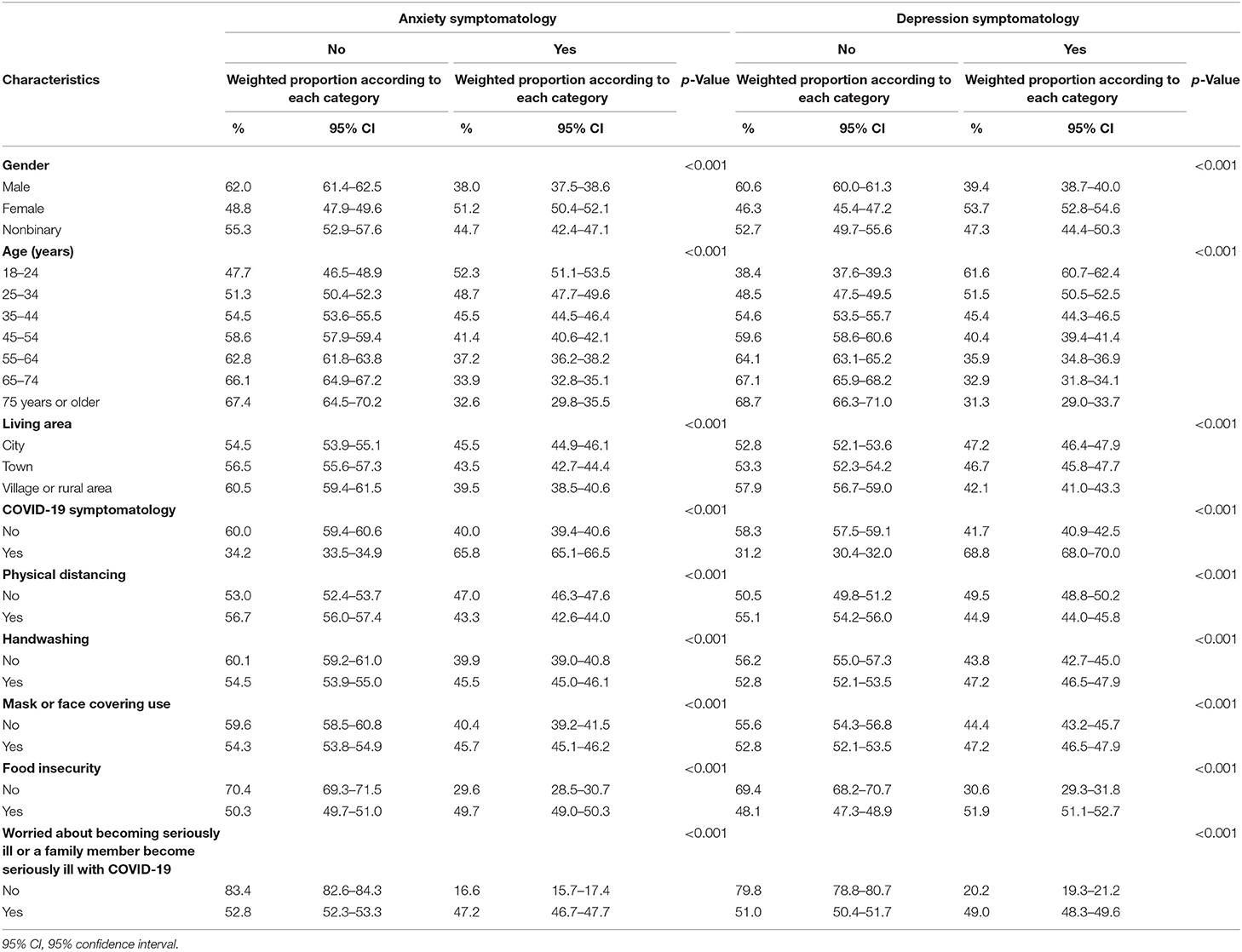
Table 2. Bivariate analysis of the study sample characteristics according to anxiety or depression (n = 1,338,320; N = 11,524,713).
Prevalence of Anxiety and Depressive Symptoms According to Country
Countries with the highest prevalence of both anxiety and depression were Bolivia (43.2%; 95% CI: 42.5–44.0), Chile (41.3%; 95% CI: 40.2–42.5), Ecuador (41.3%; 95% CI: 40.1–42.6), and Peru (40.1%; 95% CI: 39.1–41.1). Likewise, those with the lowest prevalence of both symptoms were Uruguay (27.1%; 95% CI: 25.5–28.7), Dominican Republic (27.1%; 95% CI: 25.7–28.7), Costa Rica (29.0%; 95% CI: 28.2–29.9), and Honduras (29.5%; 95% CI: 28.3–30.8) (Figure 1).
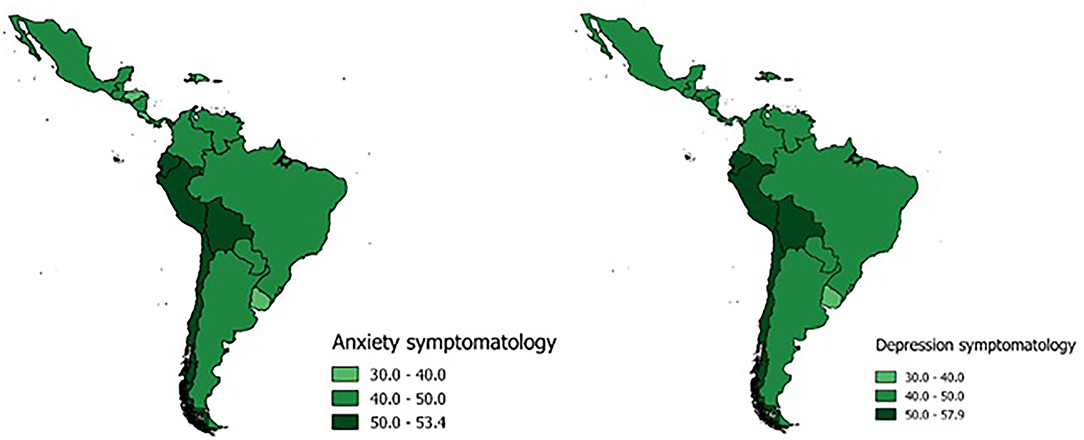
Figure 1. Anxiety and depression prevalences according to the Latin American and the Caribbean countries.
Factors Associated With Anxiety Symptomatology
The adjusted model determined that women (PR = 1.30; 95% CI: 1.28–1.31) and non-binary gender (PR = 1.20; 95% CI: 1.15–1.25) had a higher prevalence of anxiety symptomatology compared with males. In addition, being 25–34 years old (PR = 0.94; 95% CI: 0.93–0.95), 35–44 (PR = 0.91; 95% CI: 0.90–0.92), 45–54 (PR = 0.86; 95% CI: 0.84–0.88), 55–64 (PR = 0.83; 95% CI: 0.80–0.86), 65–74 (PR = 0.82; 95% CI: 0.78–0.86), 75 years or older (PR = 0.86; 95% CI: 0.78–0.95), compared with being 18–24 years old, was associated with a lower prevalence of anxiety symptoms. Similarly, living in a town (PR = 0.96; 95% CI: 0.94–0.98) or in a village or rural area (PR = 0.90; 95% CI: 0.88–0.91) was associated with a lower prevalence of anxiety symptoms when compared with living in a city. In addition, the presence of suspected symptoms of COVID-19 (PR = 1.47; 95% CI: 1.46–1.49), compliance with handwashing (PR = 1.03; 95% CI: 1.02–1.05), use of a mask (PR = 1.07; 95% CI: 1.05–1.09), food insecurity (PR = 1.45; 95% CI: 1.41–1.49), and being worried about falling seriously ill or a family member become seriously ill with COVID-19 (PR = 2.30; 95% CI: 2.20–2.41) had a higher prevalence of anxiety symptoms. In contrast, compliance with physical distancing (PR = 0.98; 95% CI: 0.97–0.99) showed an association with a lower prevalence of anxiety symptoms (Table 3).
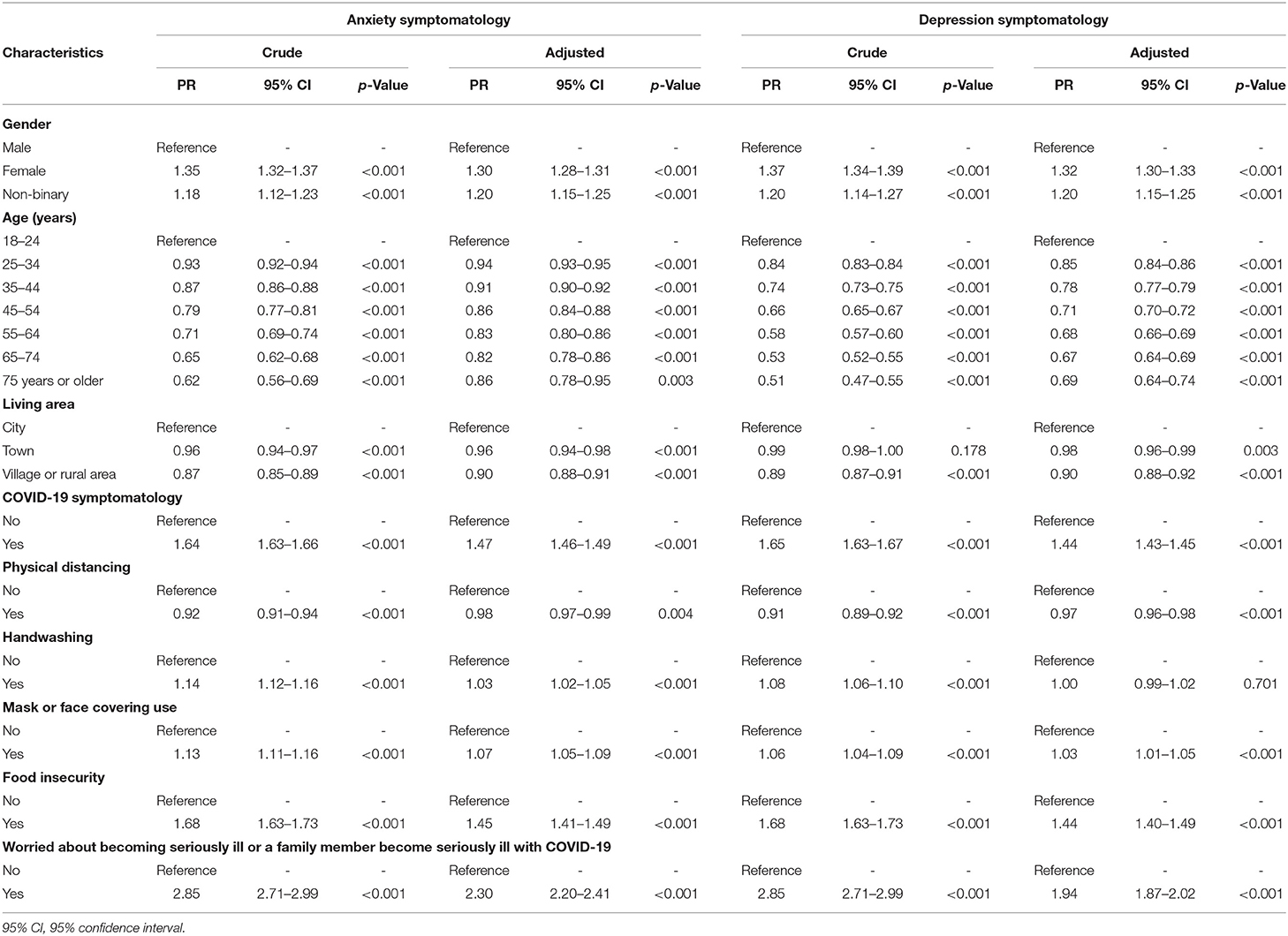
Table 3. Crude and adjusted generalized linear models of Poisson family with logarithmic link to evaluate the factors associated with anxiety or depression in the study sample.
Factors Associated With Depressive Symptomatology
In the adjusted model, women participants (PR = 1.32; 95% CI: 1.30–1.33) and non-binary (PR = 1.20; 95% CI: 1.15–1.25) had a higher prevalence of depressive symptomatology in comparison with males. Alternatively, being 25–34 years old (PR = 0.85; 95% CI: 0.84–0.86), 35–44 (PR = 0.78; 95% CI: 0.77–0.79), 45–54 (PR = 0.71; 95% CI: 0.70–0.72), 55–64 (PR = 0.68; 95% CI: 0.66–0.69), 65–74 (PR = 0.67; 95% CI: 0.64–0.69), 75 years or older (PR = 0.69; 95% CI: 0.64–0.74), compared with being 18–24 years old, was associated with a lower prevalence of this symptomatology. Living in a village or rural area (PR = 0.90; 95% CI: 0.88–0.92) and in a town (PR = 0.98; 95% CI: 0.96–0.99), compared with living in a city, was also associated with a lower prevalence. Meanwhile, having suspected symptoms of COVID-19 (PR = 1.44; 95% CI: 1.43–1.45), use of a mask (PR = 1.03; 95% CI: 1.01–1.05), food insecurity (PR = 1.44; 95% CI: 1.40–1.49), and being worried about becoming seriously ill or a family member become seriously ill with COVID-19 (PR = 1.94; 95% CI: 1.87–2.02) were associated with a higher prevalence of depressive symptomatology. By contrast, compliance with physical distancing (PR = 0.97; 95% CI: 0.96–0.98) was associated with a lower prevalence of depressive symptoms (Table 3).
Factors Associated With Anxiety or Depressive Symptomatology Stratified by Gender
We found interactions between gender and the rest of the independent variables. Compared with the group of men and women, among non-binary participants, after 55 years, the association between age and anxiety symptomatology was lost. Similarly, whereas living in a town was associated with a lower prevalence of anxiety and depression symptomatology in men and women, this did not happen among non-binary participants (anxiety: PRa = 0.97; 95% CI = 0.90–1.05; p = 0.445, depression: PRa = 0.95; 95% CI = 0.88–1.03; p = 0.221) (Tables 4–6).
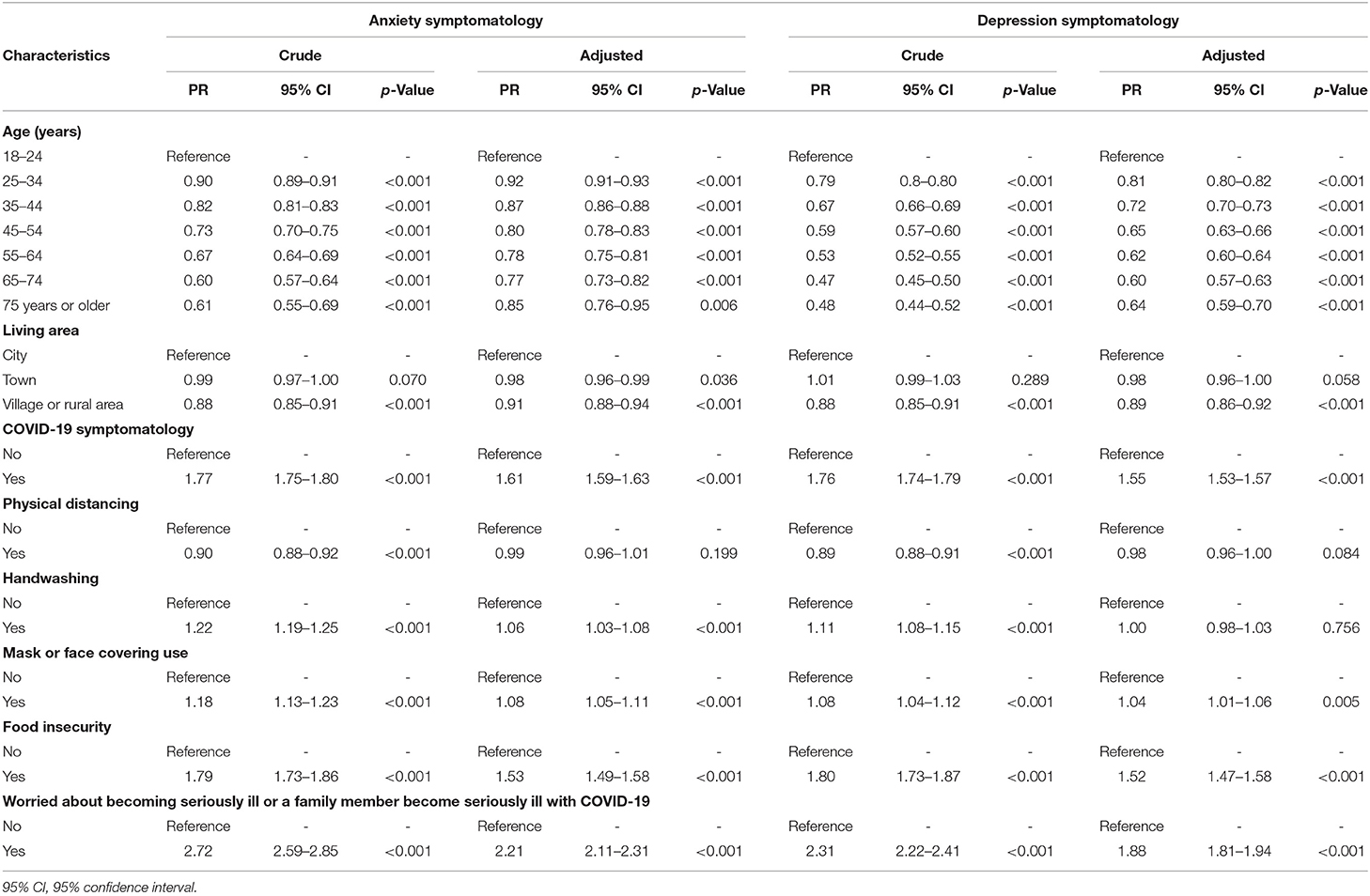
Table 4. Crude and adjusted generalized linear models of Poisson family with logarithmic link to evaluate the factors associated with anxiety or depression in men participants.
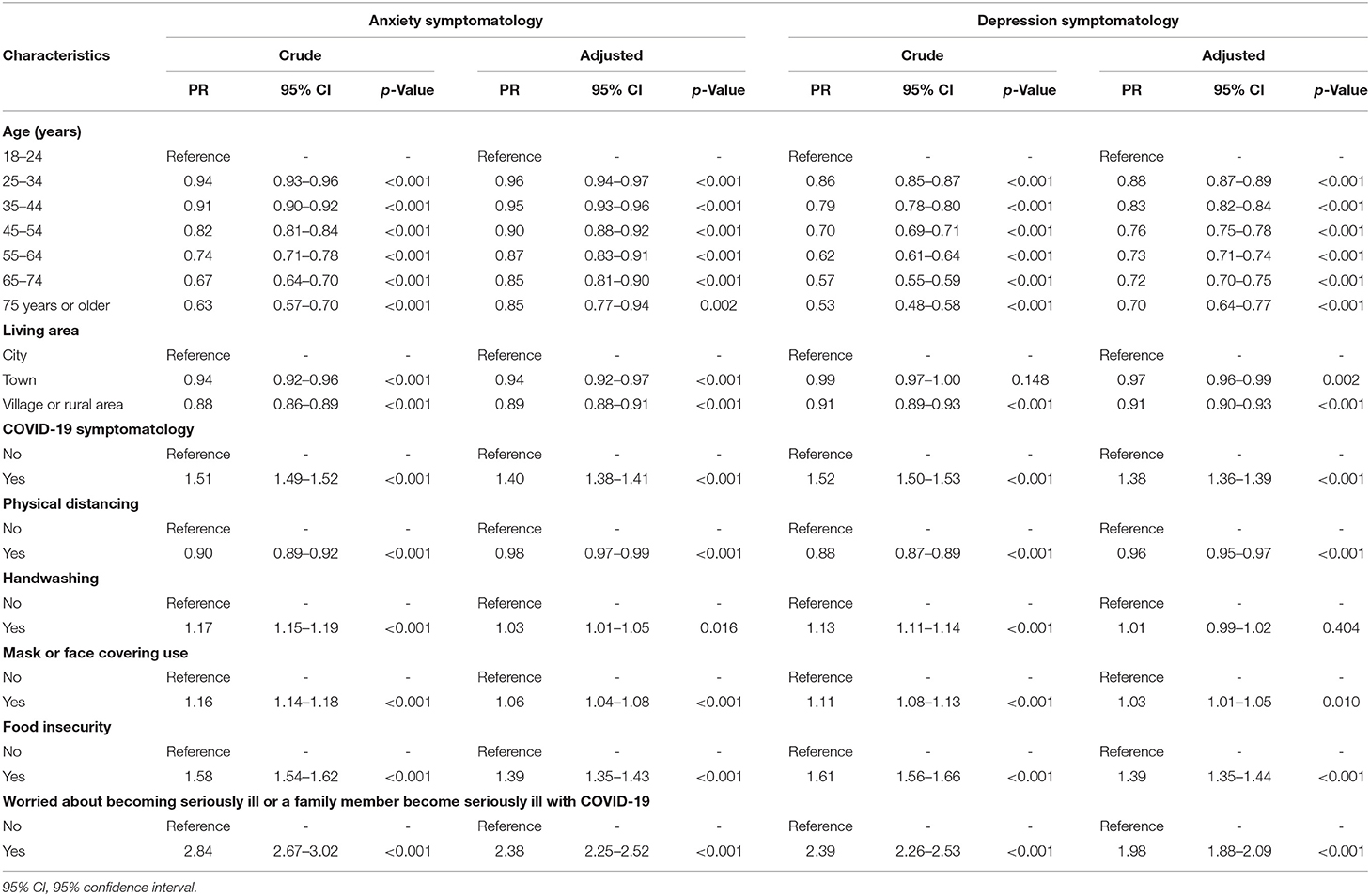
Table 5. Crude and adjusted generalized linear models of Poisson family with logarithmic link to evaluate the factors associated with anxiety or depression in women participants.
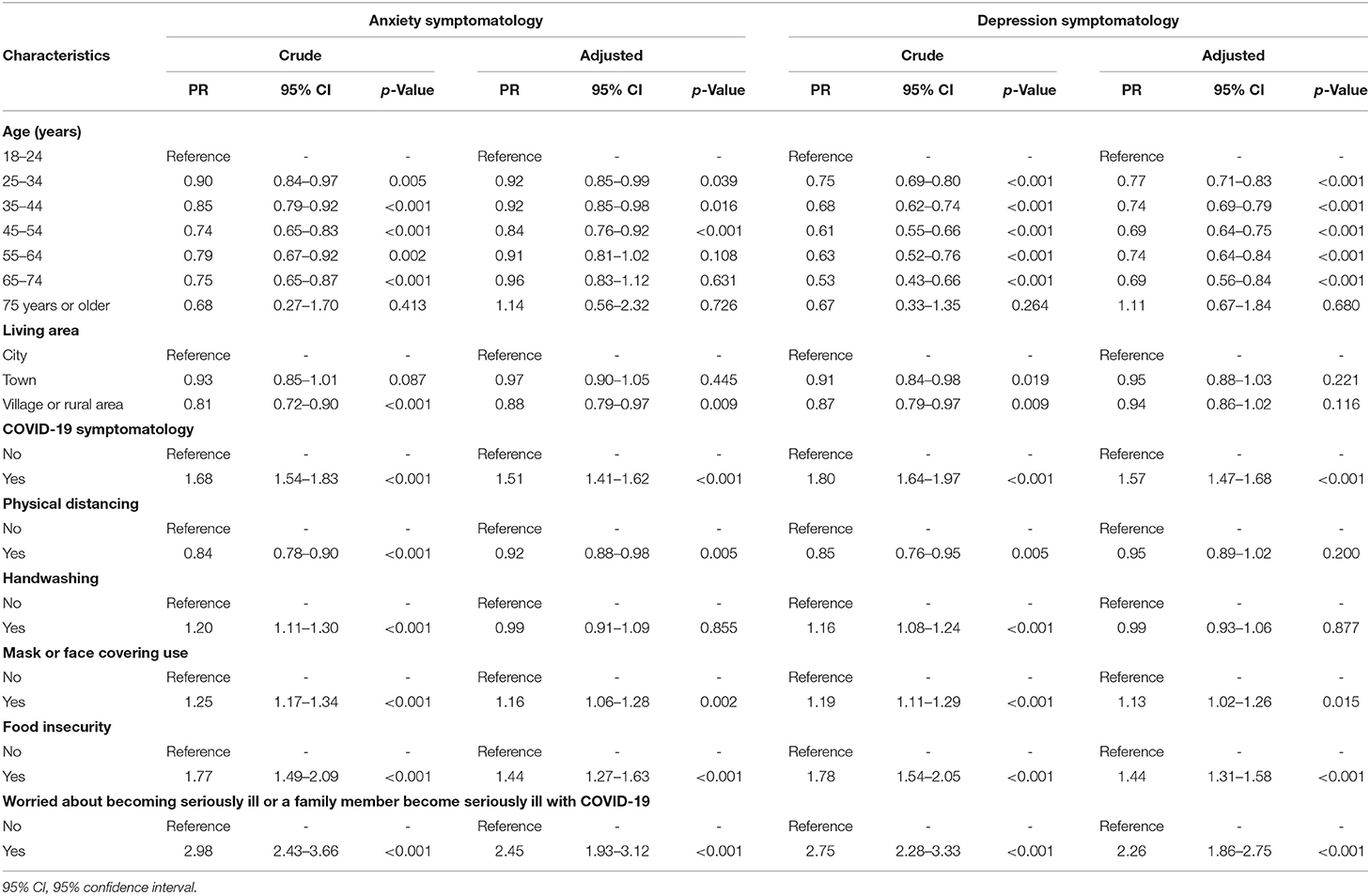
Table 6. Crude and adjusted generalized linear models of Poisson family with logarithmic link to evaluate the factors associated with anxiety or depression in non-binary participants.
Women who complied with physical distancing had a lower prevalence of anxiety and depression symptomatology (anxiety: PRa = 0.98; 95% CI = 0.97–0.99; p < 0.001, depression: PRa = 0.96; 95% CI = 0.95–0.97; p < 0.001), while this was observed only in the case of anxiety for nonbinary participants (anxiety: PRa = 0.92; 95% CI = 0.88–0.98; p = 0.005). Men participants did not show lower prevalence for neither symptomatology (anxiety: PRa = 0.99; 95% CI = 0.96–1.01; p = 0.199, depression: PRa = 0.98; 95% CI = 0.96–1.00; p = 0.084). Yet, we found association between compliance with handwashing and a higher prevalence of anxiety symptomatology among men (PRa = 1.06; 95% CI = 1.05–1.11; p < 0.001) and women participants (PRa = 1.03; 95% CI = 1.01–1.05; p = 0.016), but not among non-binary participants (PRa = 0.99; 95% CI = 0.91–1.09; p = 0.855) (Tables 4–6).
Discussion
Main Findings
The study's goal was to evaluate factors associated with depressive and anxiety symptoms in the LAC countries during the first stage of quarantine due to COVID-19. In addition, we explored the gender differences on the presence of depressive or anxiety symptoms. We found that almost half of the participants had symptoms of anxiety or depression at the beginning of the pandemic. Four countries in the South American region presented the highest prevalence of anxiety or depression symptoms compared with other countries.
Previous Studies
The studies published in some LAC countries showed results that differ from ours, but they also differ in the populations evaluated and the instruments used. A Mexican study carried out in the general population that used the PHQ-9, the GAD-7, and a visual analog scale, found that 20.8% had severe anxiety symptoms, and 27.5% had severe depressive symptoms (30). In Argentina, the Brief-Symptom Inventory-53 was used to evaluate various aspects of mental health, and it was found that, in the general population evaluated, 31.8% presented symptoms of anxiety and 27.5% presented symptoms of depression (28). Finally, a Brazilian study that elaborated its own questionnaire found that 40.4% frequently had feelings of sadness or depression, and 52.6% were frequently nervous or anxious (29). We only found one previous study that evaluated psychological distress using the K10, but it was carried out in college students from Argentina, and then it would not be comparable with our study (37). Our research evaluated the general population, and therefore, it is only comparable with studies from Argentina (28) and Brazil (29).
Previous studies carried out in Spain (38–40), Turkey (41), and China (42) intended to assess factors associated with depressive and anxiety symptomatology with a gender-based approach. However, only one study carried out in Spanish adults evaluated the factors associated with anxiety and depression, stratifying by gender; however, they did not consider the non-binary gender, and measured anxiety and depression with the GAD-7 and PHQ-9, respectively. The rest of the studies considered did not include non-binary gender in their analysis; so, our study will contribute by characterizing this population. In addition, we did not find previous studies with this objective carried out in adults from the LAC countries.
Interpretation of the Results
Although various meta-analyses and systematic reviews have been published in relation to the prevalence of depression and anxiety symptoms during the COVID-19 pandemic, the results among the different studies differ (16–23). These differences could be due to variations in the measurement instruments, cutoffs used to define mild to severe symptoms, and the eligibility criteria (16–23). However, mental health was affected differently according to regions and countries in the LAC countries during the pandemic's first wave (43). Likewise, other factors that influence the results by country included differences in the economies of the nations, government preparation to respond to the crisis, the availability of supplies or medical facilities, as well as cultural differences (16). Similarly, adequate dissemination of information related to COVID-19 in each region also influenced the psychological responses of the population, especially during the introduction of quarantines, when lifestyle was jeopardized by mandatory isolation and unexpected unemployment (14, 17).
Among men participants, compliance of physical distancing had association with a lower prevalence of anxiety or depression symptomatology. This could be related to the fact that men usually have less compliance rates of physical distancing (44). Additionally, during the pandemic, they probably had to continue working, making it even more difficult to achieve this compliance, whereas we found a higher prevalence of both anxiety and depression symptomatology among women participants, with results similar to those found in previous systematic reviews and meta-analyses (16, 18, 23). This could be related to a lack of emotional support during the quarantine or differential neurobiological responses when exposed to stressors (45, 46). Likewise, despite improvements in gender roles, historically, women had limited access to education and are more oriented to household tasks. So, several cases of intimate partner violence during this period have been reported worldwide (47). Another possible explanation could lie in the lockdown effect in the work environment, housework, and childcare. Due to the traditional gender division of labor, most of the increased burden of housework and childcare at home during the COVID-19 pandemic were felt on women (48, 49).
The sexual minority population is exposed to a variety of social stressors, such as discrimination, prejudice, and stigma that contribute to increased mental health problems (26, 27). During the pandemic, a multinational study found that women and non-binary gender people reported a higher prevalence of symptoms in every measure of distress (50). In another multinational study of 76 countries, in which 68.8% of the participant's gender was non-binary, it was found that approximately half of those evaluated had depression and anxiety (27). Then the prevalence of anxiety, depressive symptoms, and suicidal ideation increased during the pandemic (27). We did not find an association between age and anxiety symptoms among non-binary participants after 55 years of age, in contrast to men and women. Although the usual onset for anxiety and depression is young adulthood (51), we consider that our results may also be due to a lack of identification with the non-binary gender in older participants (52). Similarly, we found that in unlike men and women participants, among non-binary participants, living in a town was not significantly associated with a lower prevalence of depression and anxiety symptoms. This could be related to the fact that non-binary individuals who live in town and rural areas are usually more likely to restrain their gender expressions (53).
Among the countries evaluated, we found different prevalences of anxiety and depression symptoms; however, there was a higher prevalence of both parameters in Bolivia. Information on mental health and the impact of mental disorders in Bolivia is scarce. According to statistics reported by admissions from psychiatric hospitals around the country, the leading reason for hospitalization is substance abuse, with alcoholism being responsible for 90%, along with being one of the main causes of deaths in traffic accidents and an important risk factor for domestic violence (54). In 2014, 0.46 psychologist and 1.06 psychiatrists were reported per 100,000 inhabitants. Although Bolivia has a National Mental Health Plan that guides the promotion, prevention, treatment, and rehabilitation of mental health from mental illnesses, resources are limited (54). Hence, there is a need for a mental health and gender approach to promote CMS during the pandemic in Bolivia. This approach will be useful also in other Latin American and Caribbean countries.
Limitations and Strengths
Our study has limitations. Despite being a multinational study with a significant sample, it is based on the users of a social network that not everyone can access. However, it is a widely used social network in Latin America (four out of five Latin American Internet users have a profile on Facebook). Second, the variables included, and their definition, are subject to the pre-established definition of the matrix survey, thus, we could not include culture-related variables. Third, the data were obtained by self-reporting, and therefore, information may be underreported. Fourth, causalities cannot be established between the variables evaluated due to the study design. Fifth, there may be an underreporting of non-binary gender people. Sixth, the questions used are part of a validated instrument; however, they do not constitute one. Finally, the instrument used has not been used in other studies during the pandemic, thereby limiting comparison of the results with other studies. Nonetheless, this is the first multinational study with a significant sample size carried out in the LAC countries.
Conclusions
In conclusion, nearly 4 out of 10 people had symptoms of anxiety, while almost 5 out of 10 had symptoms of depression. Women and non-binary gender people had more symptoms of anxiety and depression. It is necessary to evaluate strategies according to gender to reduce the impact on mental health in the COVID-19 pandemic. The factors associated with symptoms of anxiety or depression varied according to gender.
Data Availability Statement
The datasets presented in this article are not readily available because it is a secondary dataset provided by the Maryland University that cannot be publicly shared due to a signed agreement. Requests to access the datasets should be directed to dmJlbml0ZXN6YXBhdGFAZ21haWwuY29t.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
PH-A, DU-P, VB-Z, GB-Q, CT-H, and AH participated in the conception of the article, the data collection, the writing of the article, and the approval of the final version. DU-P and VB-Z performed the data analysis. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
This research is based on survey results from the University of Maryland.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.727034/full#supplementary-material
References
2. Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int J Surg. (2020) 78:185. doi: 10.1016/j.ijsu.2020.04.018
3. Castro A. Response to the COVID-19 Pandemic In Urban Slums And Rural Populations In Latin America. UNDP In Latin America And The Caribbean (2020).
4. Gonzalez E, Hopkins K, Horwitz L, Nagovitch P, Holly K. Sonneland Z. The Coronavirus in Latin America AS/COA (2020).
5. Burki T. COVID-19 in latin America. Lancet Infect Dis. (2020) 20:547–8. doi: 10.1016/S1473-3099(20)30303-0
6. Andrus JK, Evans-Gilbert T, Santos JI, Guzman MG, Rosenthal PJ, Toscano C, et al. Perspectives on battling COVID-19 in countries of Latin America and the caribbean. Am J Trop Med Hyg. (2020) 103:593. doi: 10.4269/ajtmh.20-0571
7. Rogers JP, Chesney E, Oliver D, Pollak TA, McGuire P, Fusar-Poli P, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. (2020) 7:611–27. doi: 10.1016/S2215-0366(20)30203-0
8. Wu KK, Chan SK, Ma TM. Posttraumatic stress, anxiety, and depression in survivors of severe acute respiratory syndrome (SARS). J Trauma Stress. (2005) 18:39–42. doi: 10.1002/jts.20004
9. Xiang Y-T, Yu X, Ungvari GS, Correll CU, Chiu HF-K. Outcomes of SARS survivors in China: not only physical and psychiatric co-morbidities. East Asian Arch Psychiatry. (2014) 24:37–8. Available online t: https://www.easap.asia/index.php/docman/v24n4-1/478-1401-v24n1-p37
10. Vannucci A, Flannery KM, Ohannessian CM. Social media use and anxiety in emerging adults. J Affect Disord. (2017) 207:163–6. doi: 10.1016/j.jad.2016.08.040
11. Ashour HM, Elkhatib WF, Rahman M, Elshabrawy HA. Insights into the recent 2019 novel coronavirus (SARS-CoV-2) in light of past human coronavirus outbreaks. Pathogens. (2020) 9:186. doi: 10.3390/pathogens9030186
12. Hall RC, Hall RC, Chapman MJ. The 1995 Kikwit Ebola outbreak: lessons hospitals and physicians can apply to future viral epidemics. Gen Hosp Psychiatry. (2008) 30:446–52. doi: 10.1016/j.genhosppsych.2008.05.003
13. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. El impacto psicológico de la cuarentena y cómo reducirla: revisión rápida de las pruebas. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
14. Zarocostas J. How to fight an infodemic. Lancet. (2020) 395:676. doi: 10.1016/S0140-6736(20)30461-X
15. Investigators EM, Alonso J, Angermeyer M, Bernert S, Bruffaerts R, Brugha T, et al. Prevalence of mental disorders in Europe: results from the European study of the epidemiology of mental disorders (ESEMeD) project. Acta Psychiatr Scand. (2004) 109:21–7. doi: 10.1111/j.1600-0047.2004.00327.x
16. Xiong J, Lipsitz O, Nasri F, Lui LM, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. (2020). doi: 10.1016/j.jad.2020.08.001
17. Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. (2020) 16:1–11. doi: 10.1186/s12992-020-00589-w
18. Bareeqa SB, Ahmed SI, Samar SS, Yasin W, Zehra S, Monese GM, et al. Prevalence of depression, anxiety and stress in china during COVID-19 pandemic: a systematic review with meta-analysis. Int J Psychiatry Med. (2021) 56:210–27. doi: 10.1177/0091217420978005
19. Cénat JM, Blais-Rochette C, Kokou-Kpolou CK, Noorishad P-G, Mukunzi JN, McIntee S-E, et al. Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. (2021) 295:113599. doi: 10.1016/j.psychres.2020.113599
20. Deng J, Zhou F, Hou W, Silver Z, Wong CY, Chang O, et al. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: a meta-analysis. Ann N Y Acad Sci. (2020) 1486:90–111. doi: 10.1111/nyas.14506
21. Wu T, Jia X, Shi H, Niu J, Yin X, Xie J, et al. Prevalence of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. (2020) 281:91–8. doi: 10.1016/j.jad.2020.11.117
22. Vindegaard N, Benros ME. COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immun. (2020) 89:531–2. doi: 10.1016/j.bbi.2020.05.048
23. Luo M, Guo L, Yu M, Wang H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public–a systematic review and meta-analysis. Psychiatry Res. (2020) 291:113190. doi: 10.1016/j.psychres.2020.113190
24. Lim GY, Tam WW, Lu Y, Ho CS, Zhang MW, Ho RC. Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci Rep. (2018) 8:1–10. doi: 10.1038/s41598-018-21243-x
25. Shankey V, Aditi M. Depression, anxiety, and stress and socio-demographic correlates among general indian public during COVID-19. Int J Soc Psychiatry. (2020) 66:756–62. doi: 10.1177/0020764020934508
26. Plöderl M, Tremblay P. Mental health of sexual minorities. a systematic review. Int Rev Psychiatry. (2015) 27:367–85. doi: 10.3109/09540261.2015.1083949
27. Jarrett BA, Peitzmeier SM, Restar A, Adamson T, Howell S, Baral S, Beckham SW., et al. Gender-affirming care, mental health, and economic stability in the time of COVID-19: A multi-national, cross-sectional study of transgender and nonbinary people. PloS one. (2021) 16:e0254215. doi: 10.1371/journal.pone.0254215
28. Fernández RS, Crivelli L, Guimet NM, Allegri RF, Pedreira ME. Psychological distress associated with COVID-19 quarantine: latent profile analysis, outcome prediction and mediation analysis. J Affect Disord. (2020) 277:75–84. doi: 10.1016/j.jad.2020.07.133
29. Barros MBdA, Lima MG, Malta DC, Szwarcwald CL, Azevedo RCSd, Romero D, et al. Report on sadness/depression, nervousness/anxiety and sleep problems in the Brazilian adult population during the COVID-19 pandemic. Epidemiol Serv Saúde. (2020) 29:e2020427. doi: 10.1590/s1679-49742020000400018
30. Galindo-Vázquez O, Ramírez-Orozco M, Costas-Muñiz R, Mendoza-Contreras LA, Calderillo-Ruíz G, Meneses-García A. Symptoms of anxiety, depression and self-care behaviors during the COVID-19 pandemic in the general population. Gac Med Mex. (2020) 156:298–305. doi: 10.24875/GMM.M20000399
31. Paz C, Mascialino G, Adana-Díaz L, Rodríguez-Lorenzana A, Simbaña-Rivera K, Gómez-Barreno L, et al. Behavioral and sociodemographic predictors of anxiety and depression in patients under epidemiological surveillance for COVID-19 in Ecuador. PLoS ONE. (2020) 15:e0240008. doi: 10.1371/journal.pone.0240008
32. Barkay N, Cobb C, Eilat R, Galili T, Haimovich D, LaRocca S, et al. Weights and Methodology Brief For the COVID-19 Symptom Survey By University Of Maryland And Carnegie Mellon University, In Partnership With Facebook. arXiv preprint arXiv (2020).
33. Urrunaga-Pastor D, Bendezu-Quispe G, Herrera-Añazco P, Uyen-Cateriano A, Toro-Huamanchumo CJ, Rodriguez-Morales AJ, et al. Cross-sectional analysis of COVID-19 vaccine intention, perceptions and hesitancy across Latin America and the Caribbean. Travel Med Infect Dis. (2021) 41:102059. doi: 10.1016/j.tmaid.2021.102059
34. Andrews G, Slade T. Interpreting scores on the Kessler psychological distress scale (K10). Aust N Z J Public Health. (2001) 25:494–7. doi: 10.1111/j.1467-842X.2001.tb00310.x
35. Vargas Terrez BE, Villamil Salcedo V, Rodríguez Estrada C, Pérez Romero J, Cortés Sotres J. Validación de la escala Kessler 10 (K-10) en la detección de depresión y ansiedad en el primer nivel de atención. Propiedades Psicométricas Salud Mental. (2011) 34:323–31. Available online at: http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S0185-33252011000400005
37. Steinmetz LCL, Leyes CA, Florio MAD, Fong SB, Steinmetz RLL, Godoy JC. Mental health impacts in argentinean college students during COVID-19 quarantine. Front Psychiatry. (2021) 12:557880. doi: 10.3389/fpsyt.2021.557880
38. Jacques-Aviñó C, López-Jiménez T, Medina-Perucha L, De Bont J, Gonçalves AQ, Duarte-Salles T, et al. Gender-based approach on the social impact and mental health in Spain during COVID-19 lockdown: a cross-sectional study. BMJ Open. (2020) 10:e044617. doi: 10.1136/bmjopen-2020-044617
39. Ausín B, González-Sanguino C, Castellanos MÁ, Muñoz M. Gender-related differences in the psychological impact of confinement as a consequence of COVID-19 in Spain. J Gend Stud. (2021) 30:29–38. doi: 10.1080/09589236.2020.1799768
40. García-Fernández L, Romero-Ferreiro V, Padilla S, David López-Roldán P, Monzó-García M, Rodriguez-Jimenez R. Gender differences in emotional response to the COVID-19 outbreak in Spain. Brain Behav. (2021) 11:e01934. doi: 10.1002/brb3.1934
41. Özdin S, Bayrak Özdin S. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int J Soc Psychiatry. (2020) 66:504–11. doi: 10.1177/0020764020927051
42. Hou F, Bi F, Jiao R, Luo D, Song K. Gender differences of depression and anxiety among social media users during the COVID-19 outbreak in China: a cross-sectional study. BMC Public Health. (2020) 20:1–11. doi: 10.1186/s12889-020-09738-7
43. Zhao H, He X, Fan G, Li L, Huang Q, Qiu Q, et al. COVID-19 infection outbreak increases anxiety level of general public in China: involved mechanisms and influencing factors. J Affect Disord. (2020) 276:446–52. doi: 10.1016/j.jad.2020.07.085
44. Pedersen MJ, Favero N. Social distancing during the COVID-19 pandemic: who are the present and future noncompliers? Public Adm Rev. (2020) 80:805–14. doi: 10.1111/puar.13240
45. Panagiotakopoulos L, Neigh GN. Development of the HPA axis: where and when do sex differences manifest? Front Neuroendocrinol. (2014) 35:285–302. doi: 10.1016/j.yfrne.2014.03.002
46. Solomou I, Constantinidou F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: Age and sex matter. Int J Environ Res Public Health. (2020) 17:4924. doi: 10.3390/ijerph17144924
47. Thibaut F, van Wijngaarden-Cremers P. Women's mental health in the time of Covid-19 pandemic. Front Global Womens Health. (2020) 1:17. doi: 10.3389/fgwh.2020.588372
48. Yildirim TM, Eslen-Ziya H. The differential impact of COVID-19 on the work conditions of women and men academics during the lockdown. Gend Work Organ. (2021) 28:243–9. doi: 10.1111/gwao.12529
49. Farré L, Fawaz Y, González L, Graves J. How the COVID-19 Lockdown Affected Gender Inequality In Paid And Unpaid Work In Spain. (2020). doi: 10.2139/ssrn.3643198
50. Prout TA, Zilcha-Mano S, Aafjes-van Doorn K, Békés V, Christman-Cohen I, Whistler K, et al. Identifying predictors of psychological distress during COVID-19: a machine learning approach. Front Psychol. (2020) 11:586202. doi: 10.3389/fpsyg.2020.586202
51. Reisner SL, Katz-Wise SL, Gordon AR, Corliss HL, Austin SB. Social epidemiology of depression and anxiety by gender identity. J Adolesc Health. (2016) 59:203–8. doi: 10.1016/j.jadohealth.2016.04.006
52. Whyte S, Brooks RC, Torgler B. Man, woman, “other”: Factors associated with nonbinary gender identification. Arch Sex Behav. (2018) 47:2397–406. doi: 10.1007/s10508-018-1307-3
53. Suen Y-t, Chan RCH. A nationwide cross-sectional study of 15,611 lesbian, gay and bisexual people in China: disclosure of sexual orientation and experiences of negative treatment in health care. Int J Equity Health. (2020) 19:1–12. doi: 10.1186/s12939-020-1151-7
Keywords: Latin America, anxiety, depression, gender identity, COVID-19
Citation: Herrera-Añazco P, Urrunaga-Pastor D, Benites-Zapata VA, Bendezu-Quispe G, Toro-Huamanchumo CJ and Hernandez AV (2022) Gender Differences in Depressive and Anxiety Symptoms During the First Stage of the COVID-19 Pandemic: A Cross-Sectional Study in Latin America and the Caribbean. Front. Psychiatry 13:727034. doi: 10.3389/fpsyt.2022.727034
Received: 17 June 2021; Accepted: 25 January 2022;
Published: 17 March 2022.
Edited by:
Manasi Kumar, University of Nairobi, KenyaReviewed by:
Aikaterini Arvaniti, Democritus University of Thrace, GreeceLorena García-Fernández, Miguel Hernández University of Elche, Spain
Copyright © 2022 Herrera-Añazco, Urrunaga-Pastor, Benites-Zapata, Bendezu-Quispe, Toro-Huamanchumo and Hernandez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vicente A. Benites-Zapata, dmJlbml0ZXN6YXBhdGFAZ21haWwuY29t