 Zahra Khajali
Zahra Khajali Amin Sayyadi
Amin Sayyadi Zahra Ansari3
Zahra Ansari3 Maryam Aliramezany
Maryam Aliramezany
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 12 January 2023
Sec. Social Psychiatry and Psychiatric Rehabilitation
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.1062386
Introduction: Prevalence of congenital heart disease (CHD) has increased in recent years, and patients with CHD have to deal with sequelae of the multiple medical and surgical treatments that can affect different aspects of their life which could be reflected in their quality of life (QoL). In Iran, to the best of our knowledge, QoL of adult patients with CHD has not been investigated, so this study aimed to investigate the QoL of adult patients with CHD referred to two Iranian outpatient settings.
Methods: In 2022, a double center, cross-sectional study was performed on adult patients with CHD receiving out-patient care at Besat Clinic in Kerman, Iran, and Clinic of Shahid Rajaee Hospital in Tehran, Iran. Inclusion criteria were documented diagnosis of CHD based on guidelines, ejection fraction of above 45% and age of 18–55 years. We recruited a sample of 120 individuals using a simple random sampling method. At the day of referring to the adult congenital heart diseases clinic, after ensuring their written consent to participate in the study, we asked patients to fill in two questionnaires of demographic questionnaire and Persian version of the Ferrans and Powers Quality of Life Index. Data were analyzed using descriptive statistics and chi square via SPSS-22.
Results: A total of 101 patients with a mean age of 31.05 years participated in the study. Demographic and socio-economic factors had no significant relationship with the patients’ QoL. But factors related to the disease were significantly different among QoL groups (P-value > 0.05).
Discussion: Adults with CHD had a low QoL, which is not related to their demographic and socio-economic factors. That is, the existence of the disease alone and its accompanying complications can affect the QoL of these people. Hence, the mental health of adult patients with CHD should be monitored during their routine cardiac care.
Congenital heart diseases (CHD) are on the rise globally. The total number of patients living with CHD has increased from 10,105,235 in 1990 to 11,998,283 in 2017, an increase of 187%. Moreover, the birth prevalence of CHD has increased by 4.2% (17,876 cases per 100,000 babies) (1). Recent diagnostic and therapeutic advances have also increased the number of adults with CHD (2–4). Furthermore, the prevalence of CHD differs among different regions and countries (5), but what is common among adults with CHD is the fact that they all have to deal with sequelae such as heart failure (HF), endocarditis, arrhythmias, and pulmonary hypertension, which can result from multiple medical and surgical treatments received in previous years (6, 7).
Furthermore, studies showed that psychiatric disorders such as anxiety and mood disorders can affect the quality of life in adult patients with congenital heart disease (8). These disorders can negatively affect patients’ employment and social relationships (9). Therefore, screening for psychiatric disorders such as major depressive disorders can help improve the patient’s condition (10).
Furthermore, these patients might also experience mental disorders. Lebherz et al. (6) reported an increased risk of anxiety disorders, regardless of the severity of the heart defect. To show the magnitude, they suggested that it is comparable to the anxiety level of patients with aggressive non-Hodgkin lymphoma. Gleason et al. noted elevated anxiety and depressive symptoms and believed that this combination is associated with unemployment and lower quality of life (QoL) (11).
The World Health Organization (WHO) defined QoL as “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns” (12). For most people, QoL matters more than longevity (13). QoL is an important issue in the field of medicine, but measuring it scientifically is challenging because of its inherent subjectivity (14, 15). Scientists have introduced multiple assessment tools for measuring QoL. Spitzer et al. developed the Quality of Life Index (QLI), which assesses the physical, psychological, and social functioning of patients and yields a score from 0 to 10. The unique feature of the QLI is that it uses multiple resources, including the patient, the physician or other health professional, a relative, or others, and compares the results. Studies in Australia, Canada, and the United States have demonstrated its validity and reliability. Padilla’s Quality of Life Index (1983) is another tool focused on patients’ physical conditions, activities, and attitudes. It was originally developed for patients with cancer, but later, they also used it for patients with colostomy with some disease-specific added items (16).
Truong et al. (17) conducted a cross-sectional study on 109 hospitalized patients with CHD in Vietnam to investigate the QoL of adults. They used the EuroQOL-5D, the Satisfaction with Life Scale, and the Hospital Anxiety and Depression Scale as assessment tools and found that reduced QOL and elevated psychological problems were common among these patients. Unmarried status, unemployment/unstable employment, and complex CHD/pulmonary artery hypertension were found to be related to poor QOL, life dissatisfaction, anxiety, and depression. Rometsch et al. (18) investigated medical and psychosocial risk factors for impaired health-related quality of life (HRQoL) and poor psychological adjustment (PA) in young adults with CHD; their study included 188 patients with CHD and 139 healthy patients, and they discovered that these individuals had impaired physical HRQoL but normal mental HRQoL and PA; they also reported that lower physical exercise capacity, female sex, less social support, and a lower educational level are related to poor QoL.
Various studies proved the negative effects of various heart diseases on patients’ quality of life. For example, it has been shown that heart failure, regardless of the severity of the symptoms, can be a factor that influences the quality of life in an age-dependent manner (19). In addition, the quality of life of patients with coronary artery disease is an important indicator of their prognosis (20). Although the quality of life of patients with congenital heart disease has been investigated in previous studies (17, 18, 20–23), there is no consensus on it. QoL is a multifaceted concept in different countries; age, marital and employment status, and functional class assessment are some of the factors that can be responsible for this diversity (13, 14). To the best of our knowledge, QoL among patients with CHD has not been investigated in Iran. Therefore, considering the rise in the number of patients with CHD and the interaction of mental and physical health, this study aimed to investigate the QoL of adult patients with CHD referred to two Iranian outpatient clinics in 2022.
In 2022, a two-center study was designed on CHD patients receiving outpatient care from the Besat clinic in Kerman, Iran, and the clinic of the Shahid Rajaee hospital in Tehran, Iran. The inclusion criteria were documented diagnoses of CHD based on guidelines, an ejection fraction above 45%, and an age range of 18–55 years. The sample consisted of 120 individuals recruited using simple random sampling. To identify patients, we referred to the outpatient clinic records and randomly selected 60 patients from each clinic (Besat and Shahid Rajaei) based on their registration numbers. Then, we planned to fill in the questionnaires at their routine clinic visit for 6 months (from March 2022 to August 2022). On the day of referral to the adult congenital heart disease clinic, we asked patients to complete questionnaires after explaining the study objectives and obtaining their written consent to participate.
The questionnaire comprised two parts. In the first part, demographic questions (age, sex, level of education, employment, and marital status) were asked. In the second part, the QoL was investigated using the Persian version of Ferrans and Powers’ Quality of Life Index (24). The tool, which was developed in 1999, consists of 35 items on different aspects of life, including health and functioning (HF; 15 items), socioeconomics (SE; 8 items), psychological-spiritual (PS; 7 items), and family (FA; 5 items). Individuals indicated their satisfaction level and the importance of that issue on a scale of 1 to 6, from very dissatisfied/unimportant to very satisfied/important. To measure the scores, at first, we subtracted the constant number of 3.5 from all of the satisfaction scores. Hence, the scores changed to −2.5, −1.5, −0.5, +0.5, +1.5, and +2.5. We multiplied these numbers and importance scores together and added these numbers. To avoid the effect of the questions that remained unanswered, we divided this score by the number of questions. The resulting numbers were on a scale from −15 to +15. To remove negative numbers, we added the constant number of +15 to all numbers and got numbers in the range of 0 to 30. We classified them into three categories: undesirable (0–9), relatively desirable (10–19), and desirable (20–30). We used Cronbach’s alpha to evaluate the scale’s reliability, which was approved with a score of 0.86. We classified the severity of CHD according to the guidelines for the management of adults with CHDs developed by the American College of Cardiology (ACC) and the American Heart Association (AHA) (25): greatly complex, moderately complex, and simple. We also evaluated the patient’s heart function (Table 1) by echocardiography. Additionally, the presence of a residual defect, history of arrhythmia, heart surgery and type of surgery (corrective or palliative), functional class (FC), and blood oxygen level were checked from medical records and put into the questionnaire.

Table 1. Reference value and grading scale for the LVEF.
We used SPSS software, version 22, for statistical analysis. We applied descriptive analysis to the data and conducted the Chi-squared test to examine the relationship between QoL and variables such as age, duration of the disease, and the number of hospitalizations.
This study was approved by the ethical committee of the Rajaei Heart Center (IR.RHC.REC.1400.013). We also ensured that patients had given written informed consent before participating in the study.
A total of 101 (84% response rate) patients (63 women, 62.4%) with a mean age of 31.05 years participated in the study. The number of single and married participants was equal (49 people, 49%). Moreover, there were two divorced participants (2%). More than half of our patients were house wives (81 patients, 58.9%). A lower level of education was more common in our study, (with 80.2% of them not having a university degree). The most common type of CHD among our study participants was moderately complex (45 patients, 44.6%). Approximately one-third of the study population did not suffer from left ventricle dysfunction, but the most common type of dysfunction was mild (43 patients, 42.6%). The number of people in each FC class decreased from 42 (41.6%) in class one to 6 (5.9%) in class four. A history of previous surgery was a common trait (62 participants, 62%), and most surgeries were corrective (53 participants, 53%). More than 60% of our patients (63) had residual defects. For most individuals, cyanosis (86 patients, 85.1%) and arrhythmia (81 patients, 80.2%) were not observed (Figure 1).

Figure 1. Demographic data of the participants. FC, functional class; LV, left ventricle.
While evaluating the relationship between patient characteristics and QoL, we discovered that only disease-specific factors significantly affected QoL (Table 2).
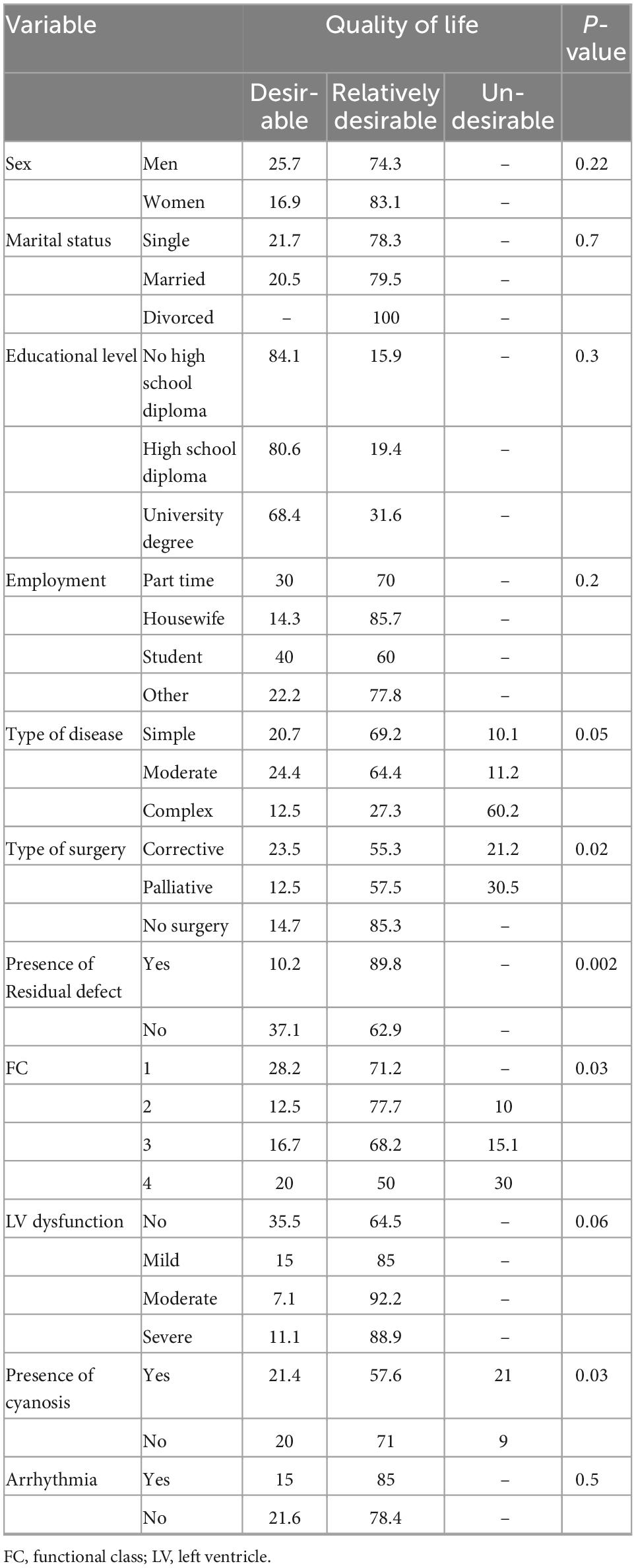
Table 2. Relation between patient’s characteristics and quality of life (QoL).
We had more women in our study than men (63 vs. 38); both sexes had a relatively desirable QoL; however, the ratio of women with better scores of QoL was slightly better than men (83.1 vs. 74.3%). Sex did not have a significant effect on QoL (p-value = 0.224).
The numbers of single and married individuals were the same (49 individuals), and their QoL was very close to each other; we only had two divorced persons in our study, and their scores were both classified as relatively desirable. Marital status was not significantly related to QoL (p-value = 0.726).
Most of our patients had no high school diploma (47.5%); the best QoL was observed in the group with no high school diploma, and the worst was in the group with a university degree. Data for this factor showed that the higher the level of education, the less desirable the life; however, the statistical analysis did not show a statistically significant difference (p-value = 0.372).
Most of our patients were house wives, with the lowest QoL (14.3%), versus students, with the highest number of individuals in the desirable group (40%). The observed difference was not statistically significant (p-value = 0.253).
Simple and moderately complex types of disease had relatively the same QoL, but the complex group had a high ratio of people with an undesirable QoL (60.2%). They also had the lowest ratio of people in the desirable group (12.5%). The effect of the type of CHD was statistically significant (p-value = 0.050).
Most patients had a history of previous surgery, and most surgeries were corrective (51.5%). All patients without a history of previous surgery had a desirable QoL, but 21.2% of patients with previous corrective surgery and 30.5% of patients with previous palliative surgery had undesirable QoL. The type of surgery had a significant effect on QoL (p-value = 0.024).
Another significant factor was the presence of a residual defect (p-value = 0.002). Most of our patients had residual defects (62.4%), and data showed that people with residual defects had significantly lower QoL.
Participants with the lowest FC had the highest ratio of undesirable QoL (30% of the FC group of four); this difference was statistically significant (p-value = 0.031). Dysfunction did not have a significant relationship with QoL (p-value = 0.064). The lowest QoL was observed in the moderate group. This group even had a lower QoL than the group with severe dysfunction (92.2 vs. 88.9%). The presence of cyanosis had a significant impact on QoL (p-value = 0.032), but arrhythmia did not have such an impact (p-value = 0.567).
We performed a descriptive-analytical study on 101 (63 women) adults with CHD to assess the impact of different social, economic, and disease-specific factors on QoL. The statistical analysis did not show any significant relationship between social or economic factors and QoL, but almost all disease-specific factors had a significant relationship with QoL.
Sex, marital status, and educational level constituted the social factors of our study. None of these factors had a significant effect on QoL. The literature is contradictory on the effect of social factors: Jackson et al. (26) had the same results, but Andonian et al. (27) and Rometsch et al. (18) found significantly worse results for female patients. In a study by Apers et al. (13), being married was related to better QoL, but Chen et al. (28) found no relationship between this factor and QoL in their study population. Lower educational level resulted in lower impaired health-related quality of life and psychological adjustment in a study by Rometsch et al. (18); Moons et al. (29) found an association between lower educational level and poorer QoL. The level of education among our participants was low. Cocomello et al. (30) also found a lower level of education among adults with CHD compared to their non-CHD peers.
In addition, it was shown in a previous study that low education can be one of the reasons for these patients not taking medicine, which will ultimately have a negative effect on the disease process and the quality of life of these patients (31).
Students and house wives had the best and worst QoL, respectively, but the statistical analysis did not find a significant difference (P-value = 0.212). Most studies (17, 32) showed that employment results in a significantly higher QoL. Eslami et al. (32) indicated that unemployment is the strongest negative factor associated with dissatisfaction.
The results showed that patients with a complex type of disease had worse QoL compared with those with mild and moderate forms of the disease. Some studies (14, 18) showed no significant difference between the QoL of different types of CHD, while others, including a cross-sectional study conducted by Truong et al. (17), reported the severity of the disease as a significant factor; Moons and Luyckx (33), in their review on the QoL of adults with CHD, found that QoL, when evaluated as physical functioning, is worse in complex cases than mild or moderate ones. It can be said that the type of underlying heart disease and its severity is one of the influencing factors on various factors in adult patients. In addition to the relationship between the type of underlying disease and the quality of life of these patients, a study by Westhoff-Bleck et al. showed that there is a relationship between the severity of heart disease and major depression in these patients (10). A history of previous surgery was another significant factor in determining QoL. Patients who had had corrective surgery had the best QoL, possibly because most of these procedures were curative and allowed the patient to potentially have a relatively normal life afterward. The patients without a history of previous surgery had the worst QoL; this could be due to having an inoperable defect or not following the treatment plan. Wang et al. (34) observed a nonsignificant difference between patients with and those without previous surgery, suggesting that both groups had a good capacity to cope with the disease regardless of this factor. Patients without residual defects can experience significantly better QoL (P-value = 0.002); these defects can deteriorate a patient’s cardiorespiratory function and can therefore lower the QoL. Furthermore, we should pay attention to the fact that most of the patients with residual defects have complex diseases, and these complex situations will result in a worse outcome (35).
Previous studies (13, 36, 37) showed that higher FC leads to worse QoL. In our study, FC had the same significant impact (P-value = 0.032). QoL was significantly lower for cyanotic patients (P-value = 0.031); Simko and McGinnis (38), in their study on QoL between different types of CHDs, reported that all the factors related to QoL, except for job, are worse for patients with cyanosis, but none of these factors were significant; they also mentioned that patients with cyanosis are more likely to have no surgical repairs and to be classified as FC I. We can note that these elements as some of the roots of this difference; Bertoletti et al. (39) did not find a significant difference in cyanosis, while Lane et al. (40) reported a significant difference between these two groups (p < 0.013).
Patients with no dysfunction and those with mild dysfunction had a better QoL. No arrhythmia had the same effect on QoL, but these (dysfunction, P-value = 0.062; arrhythmia, P-value = 0.514) were the only two disease-specific factors whose difference was not statistically significant. Disability has been identified (30, 41) as an unfavorable factor for QoL. The study conducted by Loup et al. (42) had the same nonsignificant result; Neiman et al. (43) showed that sexual dysfunction in women is associated with arrhythmias; Irtel et al. (44) studied the impact of arrhythmias on QoL in adults with CHD; atrial tachyarrhythmias and sinus nodal dysfunction, requiring a pacemaker, were the groups with the most impaired QoL; they also reported that patients without arrhythmias had a QoL comparable to that of the general population.
Congenital heart diseases are severe and, in many cases, life-threatening; they need a remarkable amount of additional care, and they also cause mental distress, but most of our patients had a medium or good QoL; multiple studies (19, 45) have shown the same results. We believe that we should search for the roots of this phenomenon in the socio-psychological components; the authors have cited some of the reasons: Bertoletti et al. (19) believed that this was the result of a good family and social support system. They mentioned that these support systems could help create a suitable environment focused on problem-solving and disease adaptation. They also noted that these could lead to better mental health, but it is noteworthy that unpleasant relationships among the members of the family and parental stress can also have adverse effects. Cocomello et al. (28) described disability paradox, sense of coherence, and response shift as three mechanisms that can contribute to this event.
Another result of our study was that almost all of the disease-specific factors were significantly effective on QoL. Given that disease-specific factors can get worse as the disease progresses over time, early diagnosis and treatment are essential for improving QoL; previous studies (46, 47) suggested using pulse oximetry as a simple, inexpensive, and noninvasive screening approach for this purpose. Bruno and Havranek (48) emphasized the importance of a centralized system for reporting positive CHD results, immediate patient evaluation, and suitable follow up for families.
Because this study was conducted in two academic centers, its results cannot be generalized to all patients. In addition to the abovementioned questionnaire, the Ferrans and Powers Quality of Life Index, which is a subjective assessment tool rather than an objective one, may not be able to examine all aspects of the quality of life. There is a possibility of bias in the study due to the presence of confounding factors such as the city of residence.
To sum up, this study showed that patients with ACHD not only suffer from their main disease but also experience a relatively worse quality of life than the general population. We also found that adults with CHD have a low QoL, which is unrelated to their demographic and socioeconomic factors. This finding suggests that the presence of the disease and its accompanying complications alone can affect these people’s QoL. Therefore, it is crucial to make timely and accurate diagnoses and initiate the appropriate treatment to minimize the complications of the disease as much as possible. This not only reduces the burden of treatment costs but also improves the QoL of these patients.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
This study was approved by the Ethical Committee of Rajaei Heart Center (IR.RHC.REC.1400.013). The patients/participants provided their written informed consent to participate in this study.
MA, ZK, ZA, and AS drafted the manuscript. MA and ZK finalized it. All authors read and approved the final version of the manuscript.
We thank the patients for their consent to participate in this project.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CHD, congenital heart disease; HF, heart failure; QoL, quality of life; PS, psychological-spiritual; SE, socioeconomic; FA, family.
1. Zimmerman M, Smith A, Sable C, Echko M, Wilner L, Olsen H, et al. Global, regional, and national burden of congenital heart disease, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Child Adolesc Health. (2020) 4:185–200. doi: 10.1016/S2352-4642(19)30402-X
2. Nashat H, Habibi H, Heng E, Nicholson C, Gledhill J, Obika B, et al. Patient monitoring and education over a tailored digital application platform for congenital heart disease: a feasibility pilot study. Int J Cardiol. (2022) 362:68–73. doi: 10.1016/j.ijcard.2022.05.002
3. Agasthi P, Graziano J. Catheter Management Pulmonary Valvular Disorders. Treasure Island, FL: StatPearls Publishing (2020).
4. Khajali Z, Maleki M, Amin A, Saedi S, Arabian M, Moosazadeh M, et al. Prevalence of cardiac dysfunction among adult patients with congenital heart disease: a single-center investigation. Iran Heart J. (2019) 20:12–9.
5. Wu W, He J, Shao X. Incidence and mortality trend of congenital heart disease at the global, regional, and national level, 1990–2017. Medicine. (2020) 99:e20593. doi: 10.1097/MD.0000000000020593
6. Lebherz C, Frick M, Panse J, Wienstroer P, Brehmer K, Kerst G, et al. Anxiety and depression in adults with congenital heart disease. Front Pediatr. (2022) 10:906385. doi: 10.3389/fped.2022.906385
7. Ministeri M, Alonso-Gonzalez R, Swan L, Dimopoulos K. Common long-term complications of adult congenital heart disease: avoid falling in a HEAP. Expert Rev Cardiovasc Ther. (2016) 14:445–62. doi: 10.1586/14779072.2016.1133294
8. Westhoff-Bleck M, Briest J, Fraccarollo D, Hilfiker-Kleiner D, Winter L, Maske U, et al. Mental disorders in adults with congenital heart disease: unmet needs and impact on quality of life. J Affect Disord. (2016) 204:180–6. doi: 10.1016/j.jad.2016.06.047
9. Kahl K, Westhoff-Bleck M. Quality of life in adults with congenital heart disease: what matters? J Thorac Dis. (2016) 8:E1379.
10. Mandarano P, Ossola P, Castiglioni P, Faini A, Marazzi P, Carsillo M, et al. Heart rate fractality disruption as a footprint of subthreshold depressive symptoms in a healthy population. Clin Neuropsychiatry. (2022) 19:163. doi: 10.36131/cnfioritieditore20220305
11. Roseman A, Kovacs A. Anxiety and depression in adults with congenital heart disease: when to suspect and how to refer. Curr Cardiol Rep. (2019) 21:1–6. doi: 10.1007/s11886-019-1237-2
12. World Health Organization. WHOQOL: Measuring Quality of Life: World Health Organization. Geneva: World Health Organization (2019).
13. Apers S, Kovacs A, Luyckx K, Thomet C, Budts W, Enomoto J, et al. Quality of life of adults with congenital heart disease in 15 countries: evaluating country-specific characteristics. J Am Coll Cardiol. (2016) 67:2237–45. doi: 10.1016/j.jacc.2016.03.477
14. Martínez-Quintana E, Estupiñán-León H, Rojas-Brito A, Déniz-Déniz L, Barreto-Martín A, Rodríguez-González F. Evaluation of quality of life in patients with congenital heart disease: an observational case control study. Am J Cardiovasc Dis. (2021) 11:73.
15. Haraldstad K, Wahl A, Andenæs R, Andersen J, Andersen M, Beisland E, et al. A systematic review of quality of life research in medicine and health sciences. Qual Life Res. (2019) 28:2641–50. doi: 10.1007/s11136-019-02214-9
16. Lalonde L, Clarke A, Joseph L, Mackenzie T, Grover S. Comparing the psychometric properties of preference-based and nonpreference-based health-related quality of life in coronary heart disease. Qual Life Res. (1999) 8:399–409. doi: 10.1023/a:1008991816278
17. Truong T, Kim N, Nguyen M, Do D, Nguyen H, Le T, et al. Quality of life and health status of hospitalized adults with congenital heart disease in Vietnam: a cross-sectional study. BMC Cardiovasc Disord. (2021) 21:229. doi: 10.1186/s12872-021-02026-1
18. Rometsch S, Greutmann M, Latal B, Bernaschina I, Knirsch W, Schaefer C, et al. Predictors of quality of life in young adults with congenital heart disease. Eur Heart J Qual Care Clin Outcomes. (2019) 5:161–8.
19. Bertoletti J, Marx G, Hattge Junior S, Pellanda L. Quality of life and congenital heart disease in childhood and adolescenc. Arq Bras Cardiol. (2013) 102:192–8. doi: 10.5935/abc.20130244
20. Reiner B, Oberhoffer R, Ewert P, Müller J. Quality of life in young people with congenital heart disease is better than expected. Arch Dis Child. (2019) 104:124–8.
21. Moons P, Van Deyk K, Marquet K, Raes E, De Bleser L, Budts W, et al. Individual quality of life in adults with congenital heart disease: a paradigm shift. Eur Heart J. (2005) 26:298–307. doi: 10.1093/eurheartj/ehi054
22. Silva AM, Vaz C, Areias ME, Vieira D, Proença C, Viana V, et al. Quality of life of patients with congenital heart diseases. Cardiol Young. (2011) 21:670–6.
23. Hunter AL, Swan L. Quality of life in adults living with congenital heart disease: beyond morbidity and mortality. J Thorac Dis. (2016) 8:E1632.
24. Eskandari S, Heravi-Karimooi M, Rejeh N, Ebadi A, Montazeri A. Translation and validation study of the Iranian version of Minnesota living with heart failure questionnaire. Payesh. (2015) 14:475–84.
25. Stout K, Broberg C, Book W, Cecchin F, Chen J, Dimopoulos K, et al. Chronic heart failure in congenital heart disease: a scientific statement from the American heart association. Circulation. (2016) 133:770–801.
26. Jackson J, DeSalvo J, Leslie C, Rausch J. Health-related quality of life declines over three years for congenital heart disease survivors. J Cardiovasc Nurs. (2021) 36:165. doi: 10.1097/JCN.0000000000000764
27. Andonian C, Freilinger S, Achenbach S, Ewert P, Gundlach U, Hoerer J, et al. ‘Well-being paradox’revisited: a cross-sectional study of quality of life in over 4000 adults with congenital heart disease. BMJ Open. (2021) 11:e049531. doi: 10.1136/bmjopen-2021-049531
28. Chen C, Liao S, Wang J, Chang C, Chiu S, Chen Y, et al. Quality of life in adults with congenital heart disease: biopsychosocial determinants and sex-related differences. Heart. (2011) 97:38–43. doi: 10.1136/hrt.2010.200709
29. Moons P, Van Deyk K, Marquet K, De Bleser L, De Geest S, Budts W. Profile of adults with congenital heart disease having a good, moderate, or poor quality of life: a cluster analytic study. Eur J Cardiovasc Nurs. (2009) 8:151–7.
30. Cocomello L, Dimagli A, Biglino G, Cornish R, Caputo M, Lawlor D. Educational attainment in patients with congenital heart disease: a comprehensive systematic review and meta-analysis. BMC Cardiovasc Disord. (2021) 21:549. doi: 10.1186/s12872-021-02349-z
31. Halling T, Akkermann S, Löffler F, Groh A, Heitland I, Haefeli W, et al. Factors that influence adherence to medication in adults with congenital heart disease (ACHD). Front Psychiatry. (2021) 12:788013. doi: 10.3389/fpsyt.2021.788013
32. Eslami B, Macassa G, Sundin Ö, Khankeh H, Soares J. Quality of life and life satisfaction among adults with and without congenital heart disease in a developing country. Euro J Prev Cardiol. (2015) 22:169–79. doi: 10.1177/2047487313514017
33. Moons P, Luyckx K. Quality-of-life research in adult patients with congenital heart disease: current status and the way forward. Acta Paediatr. (2019) 108:1765–72. doi: 10.1111/apa.14876
34. Wang Q, Rouse S, Hay M, Menahem S. Does previous cardiac surgery predict impaired quality of life in adults with congenital heart disease? World J Pediatr Congenit Heart Surg. (2020) 11:304–9. doi: 10.1177/2150135120908185
35. Heusch A, Calaminus G, Kahl J, Schmidt K. Health related quality of life after corrective surgery for congenital heart disease. Klin Padiatr. (2014) 226:281–6.
36. Pragt H, Pieper P, van Slooten Y, Freling H, van Dijk A, Sieswerda G, et al. Quality of life among patients with congenital heart disease after valve replacement. Semin Thorac Cardiovasc Surg. (2019) 31:549–58.
37. Jackson J, Hassen L, Gerardo G, Vannatta K, Daniels C. Medical factors that predict quality of life for young adults with congenital heart disease: what matters most? Int J Cardiol. (2016) 202:804–9. doi: 10.1016/j.ijcard.2015.09.116
38. Simko L, McGINNIS K. What is the perceived quality of life of adults with congenital heart disease and does it differ by anomaly? J Cardiovasc Nurs. (2005) 20:206–14.
39. Bertoletti J, Marx GC, Hattge SP, Pellanda LC. Health-related quality of life in adolescents with congenital heart disease. Cardiol Young. (2015) 25:526–32.
40. Lane D, Lip G, Millane T. Quality of life in adults with congenital heart disease. Heart. (2002) 88:71–5.
41. Robson V. Determinants of Health-Related Quality of Life in Adolescents With Repaired D-Transposition of the Great Arteries. Boston, MA: Harvard Medical School (2018).
42. Loup O, von Weissenfluh C, Gahl B, Schwerzmann M, Carrel T, Kadner A. Quality of life of grown-up congenital heart disease patients after congenital cardiac surgery. Eur J Cardiothorac Surg. (2009) 36:105–11.
43. Neiman A, Ginde S, Earing MG, Bartz PJ, Cohen S. The prevalence of sexual dysfunction and its association with quality of life in adults with congenital heart disease. Int J Cardiol. (2017) 228:953–7.
44. Irtel T, Vetter C, Stuber T, Kuemin A, Heimes T, Pfammater J, et al. Impact of arrhythmias on health-related quality of life in adults with congenital cardiac disease. Cardiol Young. (2005) 15:627–31.
45. Fekkes M, Kamphuis R, Ottenkamp J, Verrips E, Vogels T, Kamphuis M, et al. Health-related quality of life in young adults with minor congenital heart disease. Psychol Health. (2001) 16:239–50.
46. Chamsi-Pasha M, Chamsi-Pasha H. Critical congenital heart disease screening. Avicenna J Med. (2016) 6:65–8.
47. Janjua D, Singh J, Agrawal A. Pulse oximetry as a screening test for congenital heart disease in newborns. J Mother and Child. (2022).
Keywords: congenital heart disease, quality of life, mental health, adult, QoL
Citation: Khajali Z, Sayyadi A, Ansari Z and Aliramezany M (2023) Quality of life in adult patients with congenital heart disease: Results of a double-center study. Front. Psychiatry 13:1062386. doi: 10.3389/fpsyt.2022.1062386
Received: 06 October 2022; Accepted: 19 December 2022;
Published: 12 January 2023.
Edited by:
Ka Yan Ho, Hong Kong Polytechnic University, Hong Kong SAR, ChinaReviewed by:
Constantin-Cristian Topriceanu, University College London, United KingdomCopyright © 2023 Khajali, Sayyadi, Ansari and Aliramezany. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maryam Aliramezany,  bWFsaXJhbWV6YW55QHlhaG9vLmNvbQ==
bWFsaXJhbWV6YW55QHlhaG9vLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.