
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 21 December 2022
Sec. Autism
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.1038223
This article is part of the Research Topic Emotion Regulation in Neurodevelopmental Disorders: Current Understanding and Treatments View all 10 articles
 Nawelle Famelart1*
Nawelle Famelart1* Gwenaelle Diene2Sophie Çabal-Berthoumieu2Mélanie Glattard2Catherine Molinas2Maithe Tauber2,3†Michèle Guidetti1†
Gwenaelle Diene2Sophie Çabal-Berthoumieu2Mélanie Glattard2Catherine Molinas2Maithe Tauber2,3†Michèle Guidetti1†Background: This study aimed to test the effect of a new training programme on emotional competencies, named EMO-T, and to show the value of an integrative developmental approach. This approach postulates that the emotion regulation disturbances commonly observed in neurodevelopmental disorders are the consequence of potential disruptions in the prerequisite emotion skills. This integrative approach is particularly suitable in the case of complex and multidimensional disorders such as Prader–Willi syndrome (PWS), a rare genetic disease.
Methods: We examined the emotion expression, recognition, comprehension, and regulation skills in 25 PWS children aged 5–10 and 50 typically developing children (TD) aged 3–10. After a pre-test session, half of the PWS children participated in the EMO-T programme with their regular therapist for 6 weeks, while the other half continued their usual rehabilitation programme. Two post-test sessions were conducted, one at the end of the programme and one 3 months later.
Results: At pre-test, PWS children displayed a deficit in the four emotional competencies (EC). PWS children who participated in the EMO-T programme showed a significant and sustainable post-test improvement regarding voluntary expression and emotion recognition abilities, such that the level reached was no longer different from the baseline level of TD children. They also tended to improve in their emotion regulation, although they received no specific training in this skill.
Discussion: These results support that emotion regulation abilities require prerequisite emotion skills, which should be more fully considered in current training programmes. Because emotion regulation disorders strongly impact all areas of life, an integrative developmental approach appears crucial especially in the case of neurodevelopmental disorders. Further studies should be conducted to explore this perspective.
In the last two decades, there has been growing interest in the study of emotional competencies (EC) for their key role in social adaptation. EC refer to the ability to use emotions daily, including their expression, recognition, comprehension, and regulation (1). Most studies tend to focus on these various aspects of EC independently, without considering what underlies them and how they interact during development. Disturbances in these EC are commonly observed in neurodevelopmental disorders. Notably, emotion regulation disturbances can strongly impact daily life (2). To improve the effectiveness of assessment tools and training programmes, it appears important to adopt an integrative developmental approach, i.e., an approach that tackles all areas of emotional competencies, considering their development timeline, and including the child’s various caregivers.
From a developmental perspective, the different EC emerge in a hierarchical manner across childhood and adolescence (3–5). Expression and recognition abilities, which are the pillars on which interpersonal relationships are established, emerge very early during the first months of life (6). They can be considered as the basis of the development of emotion comprehension (7). This skill refers to comprehension of the causes and consequences of emotions according to the context and emerges later, at the end of the first year (8). Through the expression, recognition and comprehension skills, the individual gradually conceives of emotion as a concept (9). The construction of this “emotion theorizing” is closely linked to the emergence of the theory of mind for which a pivotal phase is typically observed from the age of 4. “Emotion theorizing” also appears necessary for the regulation of emotions and, by extension, adaptation in general (7, 8, 10–12). Emotion regulation skills develop more steadily across childhood and adolescence (4). In the early years, emotion is mostly co-regulated by parents or caregivers. Interpreting their child’s expressions, parents implement strategies to help regulate them (e.g., trying to distract the child’s attention to stop them crying). Over the course of development, a child broadens its repertoire, regulating emotions by increasingly sophisticated strategies. At first, this goes through a co-regulating process, but it also involves learning how to recognize and to emotionally master daily life situations. At the end of the second year, children begin to mobilize some regulation strategies on their own initiative (13–16). They are gradually able to manage their reactions through improved voluntary control of expression, an ability that starts to be particularly efficient from the age of 4 (17–20).
Given this developmental model, emotion regulation abilities seem to be strongly dependent on the expression, recognition, and comprehension skills, which can be considered as prerequisites (9). In this perspective, emotion regulation disorders–the most common reason for complaints by the entourage (2, 21)—might be the consequence of potential disruptions in the prerequisite skills. Thus, there is much to gain by basing EC training programmes on this developmental perspective.
To date, various intervention programmes have been developed to improve EC in children. For the most part, they were developed to prevent (e.g., school context, at-risk populations) or to remedy (e.g., populations with neurodevelopmental disorders) behavioral and social adjustment problems.
Integrative programmes such as the Social-Emotional Intervention (13), the Preschool PATHS (22), the SMILE (23) or the RULER (24) programme showed the value of including parents or teachers in the promotion of emotion abilities in children. The Emotion-Based Prevention programme (25), which included school and family, showed an improvement in the emotion knowledge and the regulation abilities in children after training in the identification and comprehension of emotions. The study also revealed that the level of emotion knowledge moderated the effect of the programme on both regulation abilities and on social skills. These results once again reinforce the developmental model of EC. The main challenge of training programmes is to promote the transfer of skills acquired during the training sessions into all areas of daily life. The integration of most of the child’s caregivers (i.e., family, teachers, therapists) into the programme appears to be crucial, as highlighted in Hadwin, Howlin, and Baron–Cohen’s programme (26).
Immersive programmes also showed their ability to remediate emotional difficulties. Computer programmes such as Emotion Trainer (27), Mind Reading (28), or FaceSay (29) were specifically developed to train emotion recognition and comprehension abilities in children with Autistic Spectrum Disorders (ASD). The main advantage of the computer format is the possibility of regular use at home. These training programmes are progressive and game-based, which adds an ecological value to the tool. Indeed, the game context (especially board games) seems to be relevant to promote the development of emotion regulation competencies in young children (30).
However, a developmental approach may be lacking in many of these programmes. Several of them focus only on one specific competence, and most of them do not include voluntary expressive skills, which are key for emotion regulation and social adjustment abilities. As a few studies have shown, it is advantageous to consider all the prerequisite skills required to develop a competence. For instance, the programme developed by Begeer et al. (31) aimed to improve social cognition in children with ASD, including therapists and families. The protocol started by a reinforcement of competencies considered as precursors of theory of mind (including imitation, perception, interactions with others). In the following steps, sessions focused on training the comprehension of social situations, the thoughts of others, and lastly the ability to reason from another person’s perspective. Results showed a significant improvement in basic skills and the conceptual comprehension of theory of mind. The authors also observed a lack of transfer of the skills acquired into daily life, however, due to the generalization difficulties of individuals with ASD.
As mentioned in the review by Mazefsky et al. (21), a holistic approach to EC is crucial in the case of neurodevelopmental disorders. Emotion regulation difficulties should rather be considered as a symptom because they are part of a broader, multidimensional problem. An integrative programme based on a developmental model appeared particularly suitable for complex neurodevelopmental disorders such as Prader–Willi syndrome.
Prader–Willi syndrome (PWS) is a rare genetic disease related to the loss of expression of paternally-inherited genes on chromosome 15 in the region q11–13. PWS is a complex neurodevelopmental disorder characterized by a significant dysfunction of the endocrine system, leading to neonatal hypotonia, growth retardation, eating disorders, and sleep disturbances (32). The phenotype also comprises learning difficulties and many psychological dysfunctions. People with PWS display a mild or moderate intellectual disability (average IQ of 60–70), memory, executive, and perceptive dysfunctions (33–35). They exhibit a language and a motor delay (36–38). In terms of social abilities, people with PWS show social maladjustment and many behavioral disorders, with several autistic features (39, 40). The literature describes a symptomatology such as tantrums, emotional lability, impulsive behavior, lack of empathy and of emotional regulation, anxiety and difficulties of social adaptation (35, 37, 40, 41), suggesting disturbances in social and emotional competencies. These problems strongly impact daily life, constituting the main reason besides hyperphagia for the family burden (42).
Regarding EC, the literature reports difficulties in the recognition and comprehension of basic emotions. Individuals with PWS make on average 10–20% more errors in identifying and assigning emotions than the typical population, even when matched for developmental age (35, 43). They take very little information into account to judge a situation, with difficulties accessing a global representation, focusing instead on details that are mostly irrelevant (39, 43, 44). The same difficulties are observed in face and voice processing (45, 46). This particularity is likely to compromise their capacity for emotional recognition and thus to place them at a disadvantage in everyday situations. In addition, the emotional expressions of PWS children are particularly poor and equivocal, making it difficult to interpret them (9).
Very few intervention programs aimed at directly improving EC in the PWS population exist, however. Most of the studies focus on hormonal treatments [Ghrelin, Oxytocin (47, 48)] or medical protocols [vagus nerve stimulation—tVNS (49)], showing some beneficial effects on social and emotional skills. Recently, two studies reported promising results on two online intervention programs aimed at developing social skills. The BOSS program (50) was offered to adolescents and young adults with PWS. The sessions were collective and took place by videoconference, 3 times a week for 10 weeks. The results showed an interesting effect of the program on socialization (friendly relations and quality of interactions with peers). The PRETEND (42) program was aimed at 3–5 year-old children with PWS and the play skills intervention work was done through the parents. The online coaching sessions took place weekly for 8 weeks. Again, the results were promising, showing interesting improvements in cognitive and affective play skills for some of the children with PWS.
To date, however, no intervention program specifically addressing EC in children with PWS has been tested, despite the need. Considering the complexity and the multidimensional disorders related to PWS, the extent of the EC difficulties involved, and their consequences on daily life, the aim of the present study was to test the effect of a training programme on EC, named EMO-T. We focused on a relatively narrow age range, which is rare in studies of PWS. The period of school age is typically a pivotal phase in emotional development. During this period, the process of “emotion theorizing” is strongly accentuated in the light of the development of other skill areas [cognitive, socialization, learning, autonomy; (3, 7)]. We postulated that a programme based on an integrative developmental approach would enable children to make significant and lasting progress in EC.
The study population was composed of 25 children with PWS aged 5;5–10;5 years. The average IQ was 75.7 and the average intellectual developmental age was 5;7 years. The children were divided into two groups, one experimental group (PWS-EG) and one control group (PWS-CG) (see Table 1 for details). The distribution was quasi-randomized. It was carried out in such a way that at any time of inclusion (spanned 18 months), the two groups were comparable in terms of sex ratio, chronological age, and IQ. Group comparison analysis (Student t-test) showed that the two groups had equivalent IQ, but showed a slight difference—albeit not significant—in term of age (see Table 1). The parents were not informed which group their child was assigned to. The families socioeconomic status (SES) was measured by the Hollingshead scale (51), which is based on marital status, education level and current occupation. SES levels range between 1 and 5, 1 corresponding to a low SES and 5 to a high one. The families in the PWS sample had a median of 4 (middle-high SES). There was no significant difference between the PWS-EG and PWS-CG groups (see Table 1).

Table 1. Descriptive characteristics for PWS and TD groups.
Fifty children with typical development (TD) also participated in the study, divided into two groups (see Table 1). The first group consisted of 25 children matched to PWS children by sex and chronological age (TD-CA group). The second group consisted of 25 other children matched to PWS children by sex and intellectual developmental age (TD-DA group). Group comparison analysis (Student t-test) confirmed that the mean age of the TD-CA group was equivalent to the mean chronological age of the PWS group [t(48) = 0.072; ns; d = 0.020]. The mean age of the TD-DA was similar to the mean developmental age of the PWS group [t(48) = −0.025; ns; d = 0.007]. None of the TD children had any academic or learning delays. The SES levels of families in the TD-DA group were higher (median = 5) than the TD-CA and PWS groups (median = 4) [Kruskal–Wallis test: χ2(2, N = 75) = 7.898, p = 0.019; see Table 1]. However, this difference cannot explain the results obtained in experimental tasks, which varied in the other direction (see Section “Results”).
A power analysis was conducted on emotion regulation rate. The estimation of the delta and the standard deviation was based on previous studies with individuals suffering from neurodevelopmental disorders on the one hand, and with typically developing individuals on the other hand. Setting the alpha at 0.05 and power at 0.80 yielded a total sample size of 32 (16 for each group). The recruitment of PWS children was carried out through the PWS French National Reference Centre and the French National Association of PWS. Initially, 29 families were enrolled in the study, corresponding to 12% of the target population. One family stopped its participation before the end of the protocol. Three children were not able to fully follow the assessment sessions and were removed from the analysis because of missing data. The participation of PWS families in the EMO-T programme was established in collaboration with one of each child’s therapists (speech therapist, psychomotor therapist, or psychologist). The programme was included in the child’s regular care programme (see the flowchart in Figure 1).
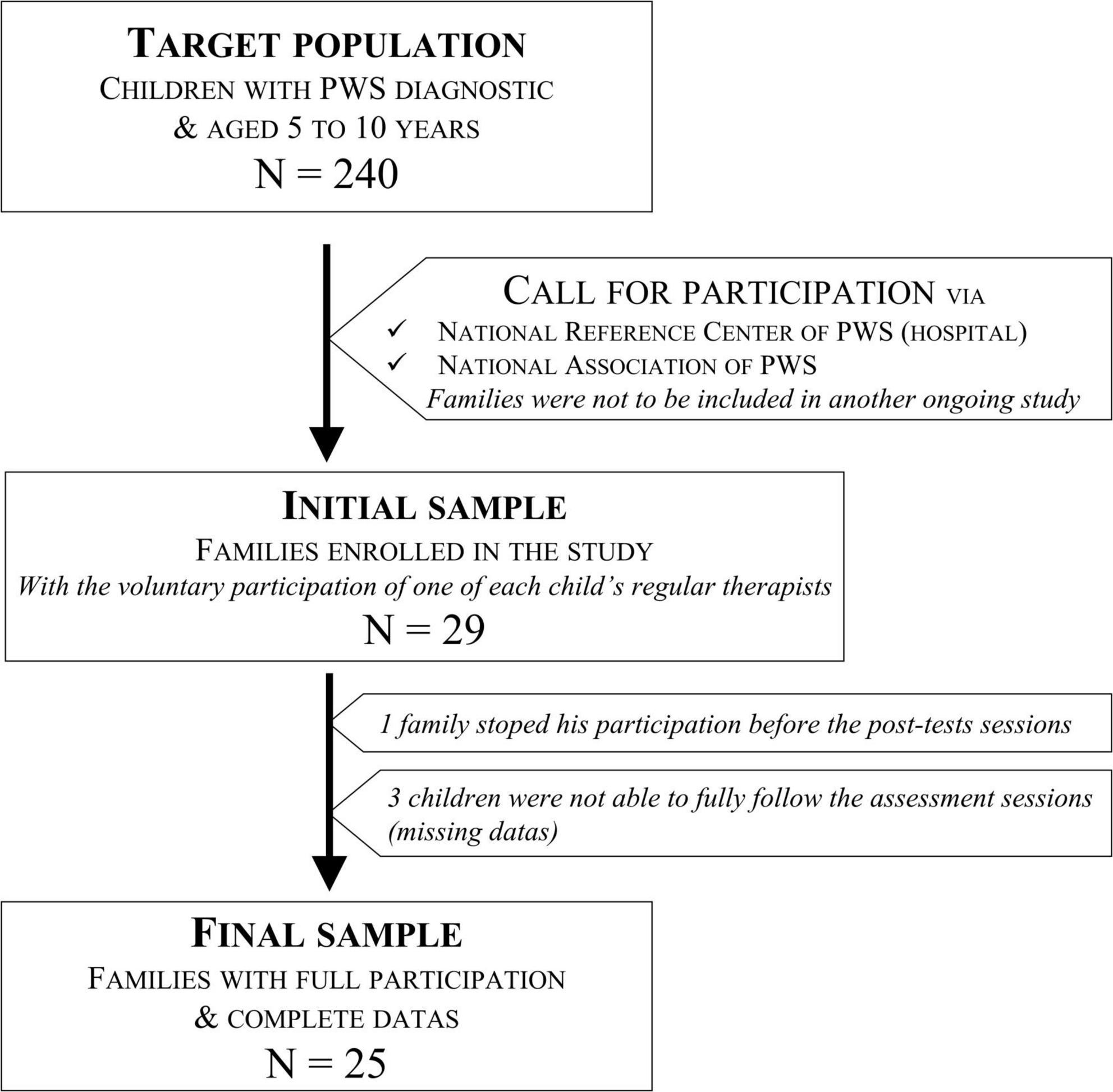
Figure 1. Prader–Willi syndrome (PWS) participants flow chart.
Given our objectives, the challenge was two-fold. The first task was to assess the children with respect to four emotional competencies: expression, recognition, comprehension, and regulation. The assessment tasks used were created or adapted from previous studies. The second challenge was to develop a training programme consisting of exercises aiming to improve emotional competencies. As the developmental model considers expression, recognition and comprehension as prerequisite skills for emotion regulation, the exercises of the EMO-T programme focused exclusively on these three competencies. The exercises used were created or adapted from previous studies in order to maintain consistency with the assessment tasks, without being identical.
The tasks and exercises are presented briefly below (for more details, see Supplementary Appendix A).
The two tasks used were created to assess spontaneous emotional reactions and voluntary production of emotional expressions [from Famelart et al.’s (9) study]. Scores are expressed as a proportion between 0 and 1, 1 meaning that the emotion is fully detectable and matches the theoretical pattern. The EMOrea Task consisted in recording the facial reactions of the child while he/she was watching a funny video clip (that was likely to induce the emotion of joy in children). The EMOmim Task consisted in asking the child to produce emotional facial expressions (voluntary expressions) of joy, sadness, fear, and anger.
Three tasks with different levels of complexity were used to assess the ability to recognize and name the emotions of joy, sadness, fear, and anger. Scores are presented in percentage of correct responses. In the Identification task, the participant had to point out the picture of the person expressing the emotion specified in the verbal instruction. In the Matching task, the participant had to select the picture of the person expressing the same emotion as in the target picture presented at the top of the screen. In the Naming task, the participant had to say which emotion the person was feeling in a short video.
The AJQ task (Affective Judgment Questionnaire) was used to assess the ability to attribute an emotion according to the context of stories. The AJQ task consisted in presenting short illustrated stories and asking the child to say which emotion the character felt (emotions targeted: joy, sadness, fear, and anger) and to justify their response. Scores were based on emotion attribution and kind of justifications, and they are presented as the percentage of correct responses.
To assess the emotion regulation skills, we used the Emotion Regulation Checklist (ERC—French version), which is a questionnaire completed by parents. Scores of the composite scale range between 0 and 4, and the higher the score, the better the regulation abilities.
The EMO-T programme was conducted by one of the child’s therapists (speech therapist, psychomotor therapist, or psychologist) and was included in the child’s regular care programme. The therapist received a half-day training session on the programme proposed by the researchers. The programme was applied weekly over six 30-min sessions. Each session consisted of the same exercises; however, the supports and stimuli evolved so that the task became more complex as the sessions progressed.
Each session included exercises to train the abilities of expression, recognition, and comprehension of emotions. All the exercises were based on the child’s justifications and arguments and the discussion with the therapist. The sessions followed the same sequence of five exercises:
(1) Sorting of static emotional facial expressions–Recognition;
(2) Naming of dynamic emotional expressions (vocal and facial) –Recognition;
(3) Mimicking emotions and recognizing them–Expression;
(4) Emotion attribution–Comprehension;
(5) Narration of emotional experience–Comprehension.
For each test session, the children were individually interviewed in a quiet room at home. All the children were met by the same experimenter, a researcher trained as a psychologist. The tasks were always presented in the same order: EMOrea, EMOmim, Matching, Identification, Naming, and AJQ. During this phase, the parents completed the ERC questionnaire.
All the children–PWS and TD children–were first assessed in a pre-test session. The PWS children included in the experimental group (PWS-EG) then received the training programme conducted by the previously trained therapist (see above), over 6 weeks (weekly 30-min sessions). During this phase, PWS children from the control group (PWS-CG) continued their usual rehabilitation with their therapist. In the third step, all the PWS children were retested, immediately after the end of the programme (post-test 1) and again 3 months later (post-test 2). Children in the PWS-CG group followed the training programme at the end of the protocol and their therapist was trained only at this time.
To test the efficiency of the EMO-T programme on the children’s EC, analyses were conducted in three steps for each task, considering the PWS Experimental Group as a reference for analyses: (1) comparison of PWS groups with the TD groups at the pre-test session (group effect); (2) comparison of the trajectory evolution of the two PWS groups between the pre- and the two post-test sessions (interaction effect); (3) comparison of the PWS groups at the second post-test session with the TD groups considered as a baseline (from the pre-test session). We used a Generalised Linear Mixed Model (GLMM) to adapt the analytical model to the specificity of the variable distribution and to integrate random effects (repeated measures). Preliminary analyses showed that age, IQ, and sex had no significant interaction or influence on any of the main effect shown.
Figure 2 and Table 2 summarize the results and statistical analyses for each task. All the details are presented in the Supplementary Appendix B.
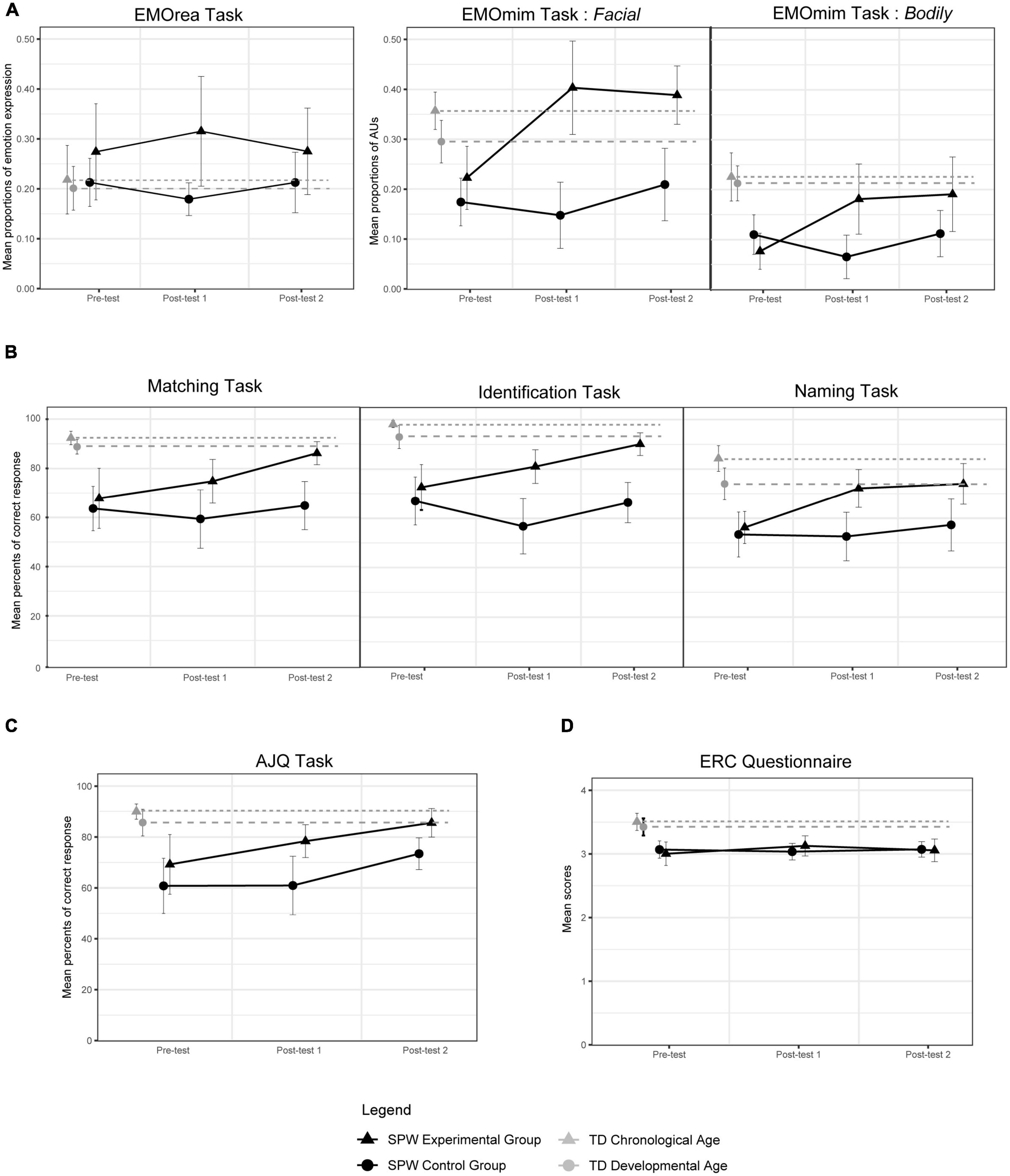
Figure 2. Graphical results of the three test sessions for each task. (A) Expression. (B) Recognition. (C) Comprehension. (D) Regulation.
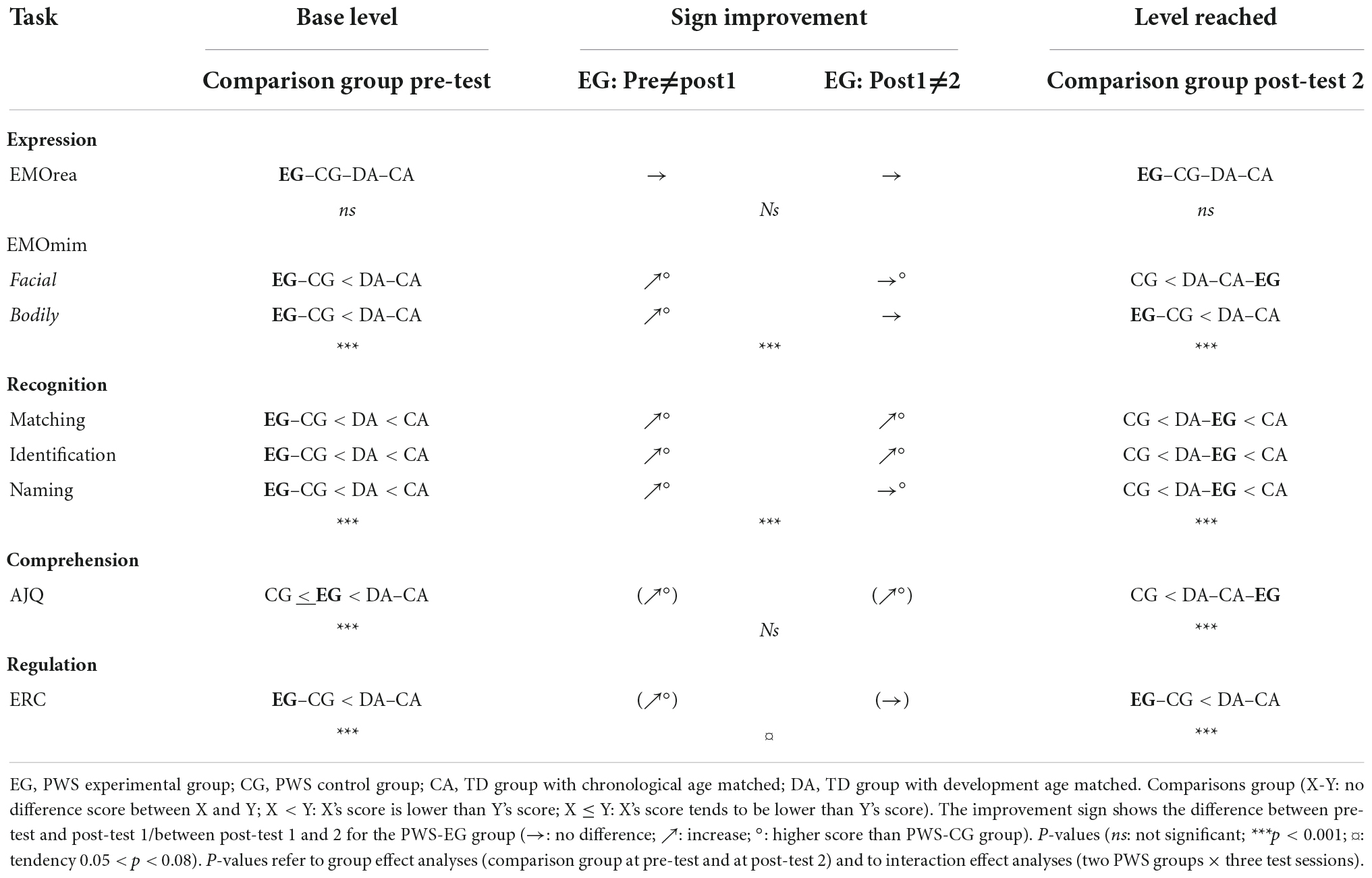
Table 2. Summary of results of the three steps of analyses for each task.
Regarding the first step of analyses, results from the pre-test session indicated a strong group effect for all tasks, except for the EMOrea task. The scores of the two PWS groups were significantly lower than those of the two TD groups. In addition, analyses showed that the scores of the two PWS groups were statistically similar. However, for the AJQ task, the scores of the PWS-EG group tended to be higher than the scores of the PWS-CG group.
In the second step, results revealed a strong interaction between the PWS groups and the test sessions for the EMOmim task and the three recognition tasks. The scores of the PWS-EG group increased significantly between the pre-test session and the first post-test session, in which they achieved significantly higher scores than the PWS-CG group. The scores of the PWS-EG group between the two post-test sessions remained statistically unchanged in the EMOmim task and the Naming task, while the group showed a significant increase in the Matching and Identification tasks.
No significant interaction was observed for the EMOmim task and the AJQ task. Nevertheless, results from the AJQ task indicated a group effect, with the PWS-EG group mainly displaying higher scores than the PWS-CG group. Results also highlighted an effect of the test session independently of the group. Specifically in the PWS-EG group, analyses showed a significant increase in scores between the pre-test session and the first post-test session, and a strong tendency to increase between the first and the second post-test session.
In the ERC questionnaire, analyses showed a strong tendency toward interaction. Scores in the PWS-EG group increased between the pre-test session and the first post-test session, without any significant differences between the two post-test sessions.
Lastly, in the third step of the analyses, we observed a significant group effect for the EMOmim task (Facial modality only), the three recognition tasks and the AJQ tasks. Scores in the PWS-EG group were significantly higher than those in the PWS-CG group at the second post-test session. The scores of the PWS-EG group no longer statistically differed from those of the two TD groups in the EMOmim task (Facial modality only) and in the AJQ task. In the three recognition tasks, the scores of the PWS-EG group no longer statistically differed from those of the TD-DA group, but they remained significantly lower than those of the TD-CA group. In the ERC questionnaire, scores in the PWS-EG group remained significantly lower than those of the two TD groups and statistically similar to those of the PWS-CG group. In the EMOrea task, the four groups remained statistically similar.
This study aimed to test the effect of the EMO-T programme on EC, based on an integrative developmental approach. The programme was applied to children with PWS as they display specific patterns of emotion regulation which are part of a broader and multidimensional problem.
Analyses showed four main results. First, PWS children displayed a specific deficit in the four EC (i.e., expression, recognition, comprehension, and regulation of emotions). Second, at post-test 2, PWS children who benefited from the EMO-T programme showed a significant improvement in their voluntary expression and recognition abilities. Third, this level reached was maintained over time, and even continued to increase beyond the programme (recognition). Fourth, the post-programme level of PWS children was no longer different from the baseline level of TD children matched by intellectual developmental age, nor even of TD children matched by chronological age (voluntary expression and comprehension).
Lastly, PWS children in the experimental group tended to improve in their emotion regulation, although they received no specific training in this skill. These results support the developmental model of EC, showing that emotion regulation abilities require expression, recognition, and comprehension skills. Such prerequisite skills should be more fully considered in current training programmes.
Nevertheless, the improvement in emotion regulation was limited and was not sustained over time, which can be attributed to several reasons. First and foremost, the mixed results regarding emotion comprehension could be a cause of this. Since comprehension abilities require several skills in many areas, especially cognitive skills, they are considered as the pillar of emotional development (7, 8, 11). In this light, the programme should include the remediation of cognitive and executive abilities, which are also heavily involved in EC, as highlighted in the study by Li et al. (52) or the study by Weiss et al. (53).
The limited sample size could also have made the results less consistent. The fact that the theoretical sample determined from the power analysis could not be reached may also explain the trend results in the emotion regulation scale. In addition, the great variability of profiles existing in PWS (35) made it more complex to set up suitable tasks. This can be illustrated by the three children who were withdrawn from the analyses because they showed too low a level of understanding and were not able to follow the instructions.
The unsustainable improvement in emotion regulation could also be due to the programme format. The EMO-T programme was applied over 6 weeks, a choice that was determined by organizational constraints, but this can be considered as a minimum duration. From the other programmes, a longer period of 3 months seems to offer a better opportunity of stabilizing the progression (25, 26, 31). Additionally, the EMO-T programme could be made more progressive, focusing initially on the ability to express and recognize emotions, since they are prerequisites for social perception skills (43). From this basis, the sessions could then include exercises on social cognition (emotion comprehension, ToM, etc.). The work on emotion regulation could then be initiated in a final stage. Feedback from therapists supports this proposition, although they also highlighted that a certain degree of redundancy may be relevant for some children who need a routine.
Lastly, the issue of how to measure emotional regulation in children remains unresolved. It is still difficult to develop a standardized methodology to carry out direct observations to measure how and when regulatory strategies are used, and to assess their effectiveness (11). It would be worthwhile further investigating board games in this respect because they create a specific context that requires regulation skills in children (30). The coding system used in Hagstrøm et al.’s (54) study or in Penela et al. (55) also shows interesting possibilities.
To conclude, this study underlined the value of considering a developmental model to promote an EC training programme. This appears crucial especially in the case of neurodevelopmental disorders with multidimensional dysfunctions. The study also showed the importance of adopting an integrative approach, by including the training programme in regular care. The EMO-T programme delivered in a therapeutic context showed an improvement through assessment sessions conducted in the family context. Interestingly, the results on the emotion regulation questionnaire completed by parents showed a potential impact of the programme on daily life. The transfer of acquisitions could be even stronger, however, by considering the “caregiver triad”: family, school, and therapists. Further studies should be conducted to explore this perspective.
The raw data supporting the conclusions of this article are available from the corresponding author on reasonable request.
Ethical review and approval was not required for the current study in accordance with the local legislation and institutional requirements. Only voluntary children with informed parental consent participated in the study. In line with the latest Declaration of Helsinki (2013), all the children, parents and therapists were fully informed of the nature and characteristics of the study. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
NF: elaboration of the study and the method, data collection, data analysis, and writing the manuscript. MT and MGu: study supervision and writing the manuscript. GD, SÇ-B, MGl, and CM: help with the recruitment of participants and the data collection. All authors contributed to the article and approved the submitted version.
This study was supported by grants from the University of Toulouse and the Occitanie Region (France). This work was also supported by funding from the Prader–Willi Syndrome French Reference Center and the French Prader–Willi Association.
We thank all the participants and their families included in this study, as well as the therapists who agreed to collaborate on this project. We are deeply grateful to the National Reference Center and the French Prader-Willi Association for financial support and for their help in recruiting the participants. We also thank the CLLE Laboratory for assistance with the statistical analysis and equipment.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.1038223/full#supplementary-material
1. Mikolajczak M. Emotional Competence. In: Carducci B, Nave C editors. The wiley encyclopedia of personality and individual differences. New Haven, CT: Wiley (2020). p. 137–41. doi: 10.1002/9781118970843.ch200
2. Hsiao Y. Parental stress in families of children with disabilities. Interv Sch Clin. (2018) 53:201–5. doi: 10.1177/1053451217712956
3. Decety J. The neurodevelopment of empathy in humans. Dev Neurosci. (2010) 32:257–67. doi: 10.1159/000317771
4. Denham S. Emotional Competence During Childhood and Adolescence. In: LoBue V, Pérez-Edgar K, Buss K editors. Handbook of emotional development. Cham: Springer International Publishing (2019). p. 493–541. doi: 10.1007/978-3-030-17332-6_20
5. Pollak S, Camras L, Cole P. Progress in understanding the emergence of human emotion. Dev Psychol. (2019) 55:1801–11. doi: 10.1037/dev0000789
6. Walle E, Reschke P, Camras L, Campos J. Infant differential behavioral responding to discrete emotions. Emotion. (2017) 17:1078–91. doi: 10.1037/emo0000307
7. Denham S, Blair K, DeMulder E, Levitas J, Sawyer K, Auerbach-Major S, et al. Preschool emotional competence: pathway to social competence? Child Dev. (2003) 74:238–56. doi: 10.1111/1467-8624.00533
8. Camras L, Halberstadt A. Emotional development through the lens of affective social competence. Curr Opin Psychol. (2017) 17:113–7. doi: 10.1016/j.copsyc.2017.07.003
9. Famelart N, Diene G, Çabal-Berthoumieu S, Glattard M, Molinas C, Guidetti M, et al. Equivocal expression of emotions in children with prader-willi syndrome: what are the consequences for emotional abilities and social adjustment? Orphanet J Rare Dis. (2020) 15:55. doi: 10.1186/s13023-020-1333-9
10. Flournoy J, Pfeifer J, Moore W, Tackman A, Masten C, Mazziotta J, et al. Neural reactivity to emotional faces may mediate the relationship between childhood empathy and adolescent prosocial behavior. Child Dev. (2016) 87:1691–702. doi: 10.1111/cdev.12630
11. Nader-Grosbois N, Mazzone S. Validation of the french version of the emotion regulation checklist (ERC-vf). Eur Rev Appl Psychol. (2015) 65:29–41. doi: 10.1016/j.erap.2014.10.002
12. Parsafar P, Davis E. Intrapersonal emotion regulation processes influence what children remember about their emotional experiences. Child Dev. (2019) 90:1935–51. doi: 10.1111/cdev.13070
13. Denham S, Burton R. Social and emotional prevention and intervention programming for preschoolers. Boston, MA: Springer (2003). doi: 10.1007/978-1-4615-0055-1
14. Izard C, Stark K, Trentacosta C, Schultz D. Beyond emotion regulation: emotion utilization and adaptive functioning. Child Dev Perspect. (2008) 2:156–63. doi: 10.1111/j.1750-8606.2008.00058.x
15. Stegge H, Meerum Terwogt M. Awareness and regulation of emotion in typical and atypical development. In: Gross J editor. Handbook of emotion regulation. New York, NY: Guilford Press (2007). p. 288–305.
16. Thompson R. Emotion and emotion regulation: two sides of the developing coin. Emot Rev. (2011) 3:53–61. doi: 10.1177/1754073910380969
17. Cole P, Jacobs A. From children’s expressive control to emotion regulation: looking back, looking ahead. Eur J Dev Psychol. (2018) 15:658–77. doi: 10.1080/17405629.2018.1438888
18. Famelart N, Guidetti M. The effect of laughter expression modulation on emotional experience in 4 to 10 year-old children. Eur J Dev Psychol. (2017) 14:311–23. doi: 10.1080/17405629.2016.1201474
19. Gross J, Thompson R. Emotion Regulation: Conceptual Foundations. In: Gross J editor. Handbook of emotion regulation. New York, NY: Guilford Press (2007). p. 3–24.
20. Gross J, Cassidy J. Expressive suppression of negative emotions in children and adolescents: theory, data, and a guide for future research. Dev Psychol. (2019) 55:1938–50. doi: 10.1037/dev0000722
21. Mazefsky C, Pelphrey K, Dahl R. The need for a broader approach to emotion regulation research in autism: applying an emotion regulation framework in ASD. Child Dev Perspect. (2012) 6:92–7. doi: 10.1111/j.1750-8606.2011.00229.x
22. Domitrovich C, Cortes R, Greenberg M. Improving young children’s social and emotional competence: a randomized trial of the preschool “PATHS” curriculum. J Primary Prevent. (2007) 28:67–91. doi: 10.1007/s10935-007-0081-0
23. Pons F, Harris P, Doudin P. Teaching emotion understanding. Eur J Psychol Educ. (2002) 17:293–304. doi: 10.1007/BF03173538
24. Brackett M, Bailey C, Hoffmann J, Simmons D. RULER: a theory-driven, systemic approach to social, emotional, and academic learning. Educ Psychol. (2019) 54:144–61. doi: 10.1080/00461520.2019.1614447
25. Izard C, King K, Trentacosta C, Morgan J, Laurenceau J, Krauthamer-Ewing E, et al. Accelerating the development of emotion competence in head start children: effects on adaptive and maladaptive behavior. Dev Psychopathol. (2008) 20:369–97. doi: 10.1017/S0954579408000175
26. Hadwin J, Howlin P, Baron-Cohen S. Teaching children with autism to mind-read: the workbook. Hoboken, NJ: John Wiley & Sons (2015). p. 156.
27. Silver M, Oakes P. Evaluation of a new computer intervention to teach people with autism or asperger syndrome to recognize and predict emotions in others. Autism. (2001) 5:299–316. doi: 10.1177/1362361301005003007
28. Baron-Cohen S, Golan O, Wheelwright S, Hill J. Mind reading: the interactive guide to emotions. London: Jessica Kingsley Publishers (2004).
29. Hopkins I, Gower M, Perez T, Smith D, Amthor F, Casey Wimsatt F, et al. Avatar assistant: improving social skills in students with an ASD through a computer-based intervention. J Autism Dev Disord. (2011) 41:1543–55. doi: 10.1007/s10803-011-1179-z
30. Dell’Angela L, Zaharia A, Lobel A, Vico Begara O, Sander D, Samson A. Board games on emotional competences for school-age children. Games Health J. (2020) 9:187–96. doi: 10.1089/g4h.2019.0050
31. Begeer S, Gevers C, Clifford P, Verhoeve M, Kat K, Hoddenbach E, et al. Theory of mind training in children with autism: a randomized controlled trial. J Autism Dev Disord. (2011) 41:997–1006. doi: 10.1007/s10803-010-1121-9
32. Cassidy S, Schwartz S, Miller J, Driscoll D. Prader-willi syndrome. Genet Med. (2012) 14:10–26. doi: 10.1038/gim.0b013e31822bead0
33. Chevalère J, Jauregi J, Copet P, Laurier V, Thuilleaux D, Postal V. Investigation of the relationship between electrodermal and behavioural responses to executive tasks in prader-willi syndrome: an event-related experiment. Res Dev Disabil. (2019) 85:229–42. doi: 10.1016/j.ridd.2018.11.013
34. Copet P, Jauregi J, Laurier V, Ehlinger V, Arnaud C, Cobo A, et al. Cognitive profile in a large french cohort of adults with prader-willi syndrome: differences between genotypes. J Intellect Disabil Res. (2010) 54:204–15. doi: 10.1111/j.1365-2788.2010.01251.x
35. Whittington J, Holland A. Cognition in people with prader-willi syndrome: insights into genetic influences on cognitive and social development. Neurosci Biobehav Rev. (2017) 72:153–67. doi: 10.1016/j.neubiorev.2016.09.013
36. Akefeldt A, Åkefeldt B, Gillberg C. Voice, speech and language characteristics of children with prader-willi syndrome. J Intellect Disabil Res. (2007) 41:302–11. doi: 10.1111/j.1365-2788.1997.tb00713.x
37. Dimitropoulos A, Ferranti A, Lemler M. Expressive and receptive language in prader–willi syndrome: report on genetic subtype differences. J Commun Disord. (2013) 46:193–201. doi: 10.1016/j.jcomdis.2012.12.001
38. Pansy J, Barones C, Urlesberger B, Pokorny F, Bartl-Pokorny K, Verheyen S, et al. Early motor and pre-linguistic verbal development in prader-willi syndrome – A case report. Res Dev Disabil. (2019) 88:16–21. doi: 10.1016/j.ridd.2019.01.012
39. Koenig K, Klin A, Schultz R. Deficits in social attribution ability in prader-willi syndrome. J Autism Dev Disord. (2004) 34:573–82. doi: 10.1007/s10803-004-2551-z
40. Reddy L, Pfeiffer S. Behavioral and emotional symptoms of children and adolescents with prader-willi syndrome. J Autism Dev Disord. (2007) 37:830–9. doi: 10.1007/s10803-006-0210-2
41. Dykens E, Roof E. Behavior in prader-willi syndrome: relationship to genetic subtypes and age. J Child Psychol Psychiatry. (2008) 49:1001–8. doi: 10.1111/j.1469-7610.2008.01913.x
42. Dimitropoulos A, Doernberg E, Russ S, Zyga O. Intervention response by genetic subtype: pretend-preschool program for children with prader-willi syndrome via remote parent training. J Autism Dev Disord. (2022) 52:5191–206. doi: 10.1007/s10803-022-05695-9
43. Dykens E, Roof E, Hunt-Hawkins H, Daniell C, Jurgensmeyer S. Profiles and trajectories of impaired social cognition in people with prader-willi syndrome. PLoS One. (2019) 14:e0223162. doi: 10.1371/journal.pone.0223162
44. Feldman B, Dimitropoulos A. Face discrimination skills in prader-willi syndrome and autism spectrum disorder. J Mental Health Res Intellect Disabil. (2014) 7:264–85. doi: 10.1080/19315864.2013.857744
45. Debladis J, Valette M, Strenilkov K, Mantoulan C, Thuilleaux D, Laurier V, et al. Face processing and exploration of social signals in prader-willi syndrome: a genetic signature. Orphanet J Rare Dis. (2019) 14:262. doi: 10.1186/s13023-019-1221-3
46. Strenilkov K, Debladis J, Salles J, Valette M, Mantoulan C, Thuilleaux D, et al. A study of voice and non-voice processing in prader-willi syndrome. Orphanet J Rare Dis. (2020) 15:22. doi: 10.1186/s13023-020-1298-8
47. Mahmoud R, Swanson H, Butler M, Flodman P, Gold J, Miller J, et al. Molecular classes and growth hormone treatment effects on behavior and emotion in patients with prader–willi syndrome. JCM. (2022) 11:2572. doi: 10.3390/jcm11092572
48. Tauber M, Boulanouar K, Diene G, Çabal-Berthoumieu S, Ehlinger V, Fichaux-Bourin P, et al. The use of oxytocin to improve feeding and social skills in infants with prader–willi syndrome. Pediatrics. (2017) 139:1–11. doi: 10.1542/peds.2016-2976
49. Holland A, Manning K. t-VNS to treat disorders of behaviour in prader-willi syndrome and in people with other neurodevelopmental conditions. Auto Neurosci. (2022) 239:102955. doi: 10.1016/j.autneu.2022.102955
50. Dykens E, Roof E, Hunt-Hawkins H, McDonald C. The feasibility and effectiveness of a novel, on-line social skills intervention for individuals with prader-willi syndrome. Front Psychiatry. (2022) 13:863999. doi: 10.3389/fpsyt.2022.863999
51. Hollingshead A. Four factor index of social status. Unpublished working paper. New Haven, CT: Yale University (1975).
52. Li Q, Liu P, Yan N, Feng T. Executive function training improves emotional competence for preschool children: the roles of inhibition control and working memory. Front Psychol. (2020) 11:347. doi: 10.3389/fpsyg.2020.00347
53. Weiss J, Thomson K, Burnham Riosa P, Albaum C, Chan V, Maughan A, et al. A randomized waitlist-controlled trial of cognitive behavior therapy to improve emotion regulation in children with autism. J Child Psychol Psychiatr. (2018) 59:1180–91. doi: 10.1111/jcpp.12915
54. Hagstrøm J, Spang K, Vangkilde S, Maigaard K, Skov L, Pagsberg A, et al. An observational study of emotion regulation in children with tourette syndrome. J Child Psychol Psychiatr. (2021) 62:790–7. doi: 10.1111/jcpp.13375
Keywords: emotion competencies, developmental model, Prader–Willi syndrome, training programme, integrative approach, children
Citation: Famelart N, Diene G, Çabal-Berthoumieu S, Glattard M, Molinas C, Tauber M and Guidetti M (2022) What underlies emotion regulation abilities? An innovative programme based on an integrative developmental approach to improve emotional competencies: Promising results in children with Prader–Willi syndrome. Front. Psychiatry 13:1038223. doi: 10.3389/fpsyt.2022.1038223
Received: 06 September 2022; Accepted: 28 November 2022;
Published: 21 December 2022.
Edited by:
Ru Ying Cai, Autism Spectrum Australia, AustraliaReviewed by:
Christiane E. Kehoe, The University of Melbourne, AustraliaCopyright © 2022 Famelart, Diene, Çabal-Berthoumieu, Glattard, Molinas, Tauber and Guidetti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nawelle Famelart, bmF3ZWxsZS5mYW1lbGFydEB1bml2LXRsc2UyLmZy
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.