 Christine Adamus
Christine Adamus Sonja Mötteli
Sonja Mötteli Matthias Jäger
Matthias Jäger Dirk Richter
Dirk Richter- 1Centre for Psychiatric Rehabilitation, Universitäre Psychiatrische Dienste Bern (UPD), Bern, Switzerland
- 2University Hospital of Psychiatry and Psychotherapy, University of Bern, Bern, Switzerland
- 3Department of Psychiatry, Psychotherapy and Psychosomatics, Psychiatric University Hospital Zurich, Zürich, Switzerland
- 4Psychiatrie Baselland, Liestal, Switzerland
- 5Department of Health Professions, Bern University of Applied Sciences, Bern, Switzerland
Background: No randomised controlled study (RCT) on the effectiveness of Independent Supported Housing (ISH) vs. housing as usual (HAU) settings for non-homeless individuals with severe mental illness (SMI) has been conducted to date because of limited feasibility. Alternative designs, such as observational studies, might be suitable for providing adequate evidence if well conducted. To test this hypothesis, this article reports on a prospective, direct comparison of the designs of two parallel studies in this field.
Methods: A two-centre, parallel-group non-inferiority effectiveness study was conducted at two locations in Switzerland using identical instruments and clinical hypotheses. One centre applied an RCT design and the other an observational study (OS) design with propensity score methods (ClinicalTrials.gov: NCT03815604). The comparability of the two study centres was investigated in terms of participants, procedures, and outcomes. The primary outcome was social inclusion and the secondary outcomes were quality of life and psychiatric symptoms.
Results: The study included 141 participants (RCT: n = 58; OS: n = 83). Within one year, 27% study dropouts occurred (RCT: 34%; OS: 22%). A similar balance of sample characteristics was achieved in the RCT and the OS using propensity score methods (inverse probability of treatment weighting). After one year, ISH was non-inferior to the control condition regarding social inclusion (mean differences [95% CI]) in the RCT (6.28 [–0.08 to 13.35]) and the OS (2.24 [–2.30 to 6.77]) and showed no significant differences in quality of life (RCT: 0.12 [–0.52 to 0.75]; OS: 0.16 [–0.26 to 0.58]) and symptoms (RCT: –0.18 [–0.75 to 0.40]; OS: 0.21 [–0.17 to 0.60]) in both study centres. However, strong and persistent preferences for ISH in the RCT control group reduced participants’ willingness to participate. Because of several limitations in the RCT, the results of the RCT and the OS are not comparable.
Conclusion: Participants were comparable in both study sites. However, there were significant problems in conducting the RCT because of strong preferences for ISH. The OS with propensity score methods provided results of more stable groups of participants and revealed balanced samples and valid outcome analysis. Our results do not support further investment in RCTs in this field.
Introduction
Housing rehabilitation of people with severe mental illness (SMI) has been a major element of mental healthcare since the deinstitutionalisation process started in the 1980s and 1990s. Different housing rehabilitation settings aim to help people with SMI gain housing skills, manage their illness, and foster their social inclusion. While housing rehabilitation usually takes place in inpatient housing settings such as residential care homes or sheltered apartments (1–4), Independent Supported Housing (ISH) provides outreach support in an independent accommodation. The UN Convention on the Rights of Persons with Disabilities (UN CRPD) demands free choice in one’s place of residence (5) and most persons with SMI strongly prefer to live independently (6, 7).
Many arguments advocate increased implementation of ISH to support people with SMI in their direct living environment. ISH interventions originate from the ‘Housing First’ approach for homeless persons, which has been successful in supporting them in finding, getting, and retaining an independent accommodation (8–10). ISH is also increasingly being offered in several countries for the support of non-homeless persons with mental illness (11). Furthermore, treatment guidelines for people with SMI recommend providing ISH as well as a broad range of in-home and community support services as the first choice, as it allows greater active participation in the community than institutionalised settings (12, 13). However, in many countries, institutionalised settings are still more prevalent in the housing rehabilitation provided to people with SMI, and evidence regarding the effectiveness of ISH for non-homeless individuals is still weak. There are only a small number of studies, which have a quality rating of weak-to-moderate and show no consistent results regarding the effectiveness of different housing settings (9, 10, 14). A more recent observational study showed no differences between ISH and residential care settings for non-homeless individuals with respect to multiple outcomes (15). More significantly, no randomised controlled study (RCT) have investigated the effectiveness of ISH in supporting non-homeless individuals. Due to these methodological limitations, it is still unclear whether the effectiveness of ISH is comparable to that of institutionalised residential settings in the housing rehabilitation provided to non-homeless service users.
Generally, the RCT design is considered the ‘gold standard’ for intervention studies. With the random allocation of participants to the study conditions, sample characteristics are assumed to be balanced and do not confound the results. Therefore, RCTs have high internal validity and the results allow drawing causal inferences regarding the effectiveness (or efficacy) of the intervention. In contrast, in the naturalistic observational study (OS) design, participants are ‘naturally’ allocated to study conditions, for example, by participants’ self-selection or on the referral of their treating therapists instead of randomisation. This makes the OS more user-friendly and more acceptable to participants, especially in the case of strong preferences for one of the conditions (16, 17). However, owing to the natural allocation, the baseline characteristics of the participants may differ systematically between the treatment and control conditions (18). Therefore, the observed outcome may be confounded by these baseline differences instead of representing a true treatment effect. Because of the inherent risk of confounding bias, many researchers still question the ability of OS to build causal inferences (19). There is a wide and persistent consensus that unidentified confounders in OS generally lead to an overestimation of treatment effects and that this weakness can only be overcome by random allocation of participants.
However, some evidence suggests the contrary (20–22). A large meta-analysis of the Cochrane collaboration compared the quantitative effect size estimates of interventions tested with randomised and observational studies in 228 medical conditions (20). No significant differences in effect size were found between the two study designs. Other methodological study characteristics seem to be confounded with the allocation method (23, 24), and many other sources of bias may be inherent in both OS and RCT (23, 25). In addition, significant research has been conducted on methodological and statistical methods to reduce confounding and improve the validity of observational intervention studies (16, 24, 26). Among many other sophisticated statistical methods, propensity score (PS) methods are increasingly applied to control confounding in observational intervention studies. There is evidence indicating that they are successful in balancing the confounding effect of the covariates on the outcome, enabling the estimation of unbiased treatment effects (18, 27). Accordingly, there are conditions under which observational studies can provide adequate evidence and approximate results from randomised studies, especially when the evidence suggests little or no harm from a feasible and acceptable intervention (16, 20).
There are situations in which random allocation is impossible or difficult to achieve, thus creating an urgent need for alternative study designs. Such situations include 1) conditions that make a random allocation ethically questionable, as in the case of housing settings for persons with mental illness; 2) intervention effects that occur over a long time frame, such as rehabilitation effects (16, 23); 3) mental healthcare interventions relying on interpersonal interactions and subjects’ active participation (28) and therefore on participants’ motivation and compliance (29); and 4) strong preferences of participants for one of the study conditions, as is common in psychiatric housing rehabilitation (6, 7, 17). Strong preferences limit the external validity of RCTs if many eligible participants refuse to be randomised and, therefore, cannot be included in the study. Strong preferences also limit internal validity if participants consent to randomisation despite their preference for one of the conditions, because motivation and compliance may systematically differ between conditions and may bias the estimated treatment effect by a high dropout rate or low in-treatment compliance in the non-preferred condition (17, 29).
In the case of strong preferences, a comprehensive cohort design as a partial RCT is recommended to enhance participation rates (30). Under the comprehensive cohort design, participants not consenting to randomisation are treated according to their preferences, while consenting participants are randomly assigned. However, in a recent housing rehabilitation feasibility trial, only 17 out of 1,432 screened, non-homeless persons with SMI agreed to participate, with only eight of them agreeing to randomisation (31). The main impediments to recruitment were located in the service users’ preferences and the staffs’ ‘gate keeping’ behaviour. Despite the clinical equipoise of the residential conditions, the staff assumed different support intensities and considered service users unsuitable for either service and therefore for study participation. Consequently, the first attempt to conduct a randomised study on housing rehabilitation settings for non-homeless persons with SMI failed to support its feasibility (31).
In our two-centre study on the effectiveness of ISH for non-homeless persons with SMI (32), one centre made a second attempt to conduct an RCT in this field (33), while the other centre conducted an OS with PS methods. Random allocation was possible at one of the two sites due to the new introduction of ISH and the scarcity of comparable services in the region, which allowed limited access of ISH only to study participants (33). Both study centres prospectively conducted concurrently the same investigation on the effectiveness of the same intervention as assessed with the same outcome measures in two cities in Switzerland. The only difference between the two study centres was supposed to be the allocation procedure. The present paper provides a direct comparison of the two study centres and reports on the hypothesis that the OS will provide similar results as the RCT.
Materials and methods
Study design
The present paper reports on the ongoing prospective, two-year, two-centre, non-blinded, parallel-groups, non-inferiority cohort field study conducted according to the published protocol (32) to investigate the effects of ISH for non-homeless individuals with SMI applying two different study designs. The study was registered on ClinicalTrials.gov (NCT03815604) and approved by the Swiss Association of Research Ethics Committees (Swissethics; reference No. 2018–02381).
Setting and study conditions
The study was conducted at two sites in Switzerland (RCT in Zurich; OS in Bern) that provided ISH to non-homeless individuals with SMI. Both locations also have a broad range of other residential rehabilitation settings that address the same population and follow the traditional approach of a continuum of care.
Intervention condition
Independent Supported Housing is a community-based outreach residential rehabilitation service for non-homeless adults with SMI who need housing support. It follows the principles of the ‘Housing First’ paradigm (34) and offers flexible, targeted and individual support according to the service users’ needs in their own accommodation that is rented independently of treatment and care at the service users’ own expenses. Individuals receive housing support without prior treatment or preparatory house training, including help in finding or retaining an accommodation, and facilitation of contact with social insurance, landlords, mental health services, and social relationships. The main goals of ISH are the social inclusion of service users and facilitation of independent and stable housing. Support is provided by mostly non-medical staff with nursing or social work training for up to four (Zurich) or eight (Berne) hours per week with no prospective time limitation or move-on orientation (see control condition below). There is also an option to consult with an ISH-related psychiatrist. ISH, however, is independent of treatment and care, which are performed by appropriate specialists outside the intervention. According to the STAX-SA taxonomy (35), ISH corresponds to a type 4 service with no staff on-site, providing low to moderate (sometimes also high) level of outreaching support at the service users’ own accommodation without any emphasis on moving-on.
In this RCT, the intervention was newly introduced in 2017. It was provided as a pilot support service by the Center for Acute Mental Illness, Mobile Service for Residential Care of the Psychiatric University Hospital Zurich, Switzerland.
ISH has been well established in the OS study and has been provided since 2012 by the Center of Psychiatric Rehabilitation of the University Hospital Universitäre Psychiatrische Dienste (UPD) in Bern, Switzerland.
Control condition
The control condition, housing as usual (HAU), contains different residential rehabilitation settings that follow the traditional continuum rehabilitation approach. This continuum includes various housing settings that provide (mostly) inpatient rehabilitation support of varying support intensities. Each setting aims to help service users stabilise and gain housing skills to enable them to live independently. Some traditional housing settings have a ‘move-on’ orientation (35, 36); once their needs decrease and functioning improves, service users are expected to graduate into a less supported setting. According to the STAX-SA taxonomy (35), the control condition contains supported accommodation services of types 1, 2, and 3, with staff on-site providing moderate to high (sometimes low) level of support in a congregate setting with limited or strong (sometimes also no) emphasis on moving-on. In addition, the control conditions contained host families (not covered in the STAX-SA typology) providing moderate support on-site and by outreach staff with limited emphasis on moving-on.
In the RCT, participants randomised to the control condition could use any HAU setting for residential support available in the canton of Zurich. A list with addresses provided orientation about available forms of support, and social workers helped them access the support services.
In the OS, the control condition mainly consisted of residential care services, complemented by assisted living communities and host family settings, to which the study team had good connections.
The two conditions showed similar fidelity with the criteria for self-determined living regarding the provided support and staff, with ISH allowing more self-determination to service users regarding housing conditions and social inclusion (37).
Procedure
Recruitment began in April 2019 at both the study centres. Sample size calculation was conducted in order to test the non-inferiority hypothesis of the effectiveness of ISH to HAU regarding the primary outcome measure (see outcome measures below) with the application ‘Power and Sample Size’ (38) and the following parameters: Power: 0.9; significance level: 0.025; non-inferiority margin: 15; group means: 111.2–106.7; SD: 12; allocation ratio: 1:1. This yielded a sample size of 28 participants in each RCT (allocation ratio 1:1) and the OS intervention condition. The OS control condition was supposed to be two- to three-fold larger (intended allocation ratio 1:3) to facilitate many-to-one PS matching (32, 39, 40). This sample size was not reached, whereupon an alternative PS method was applied (see statistical methods below).
In the RCT, all individuals with interest in ISH were screened for eligibility and consecutively recruited by a study collaborator. During the recruitment period, access to ISH was limited only to the study participants, which was possible due to the pilot status of the ISH service and the scarcity of comparable services. After participants provided informed consent, the study collaborator randomly assigned them to ISH or HAU according to the block-randomisation results that were concealed in closed envelopes, separately for each participant (detailed description of the random sequence generation and allocation procedure is provided in the protocol (32) and publication (33)). Then, participants were interviewed by the study collaborator. Following the baseline assessment, allocated treatment conditions were implemented. Recruitment for the RCT was completed by March 2020. In deviation to the protocol (32), the participants were not required to live in a particular setting. Instead, participants allocated to the ISH condition had the (optional) possibility of using ISH; participants allocated to the HAU condition were supported to receive established standard housing rehabilitation services according to their choice (except ISH). Due to control participants’ strong and persistent preference for ISH (33), they were further given the opportunity to be waitlisted and allowed to start with ISH after the first follow-up assessment.
In the OS, residential rehabilitation staff consecutively recruited participants after their admission to respective rehabilitation services (ISH or HAU setting). Interested participants were contacted and asked by a study collaborator to provide informed consent. Consenting participants were enrolled in the study. In the ISH condition, recruitment was completed by March 2020. Under the HAU condition, the target sample size could not be reached during the recruitment phase and recruitment was stopped by December 2020.
Follow-up assessments were conducted 6 months (T1) and 12 months (T2; primary outcome assessment) after baseline assessment (T0) at both locations. Follow-up assessments were intended to continue even after withdrawal from or moving between housing settings. In order to prevent confusion, we refer to ‘dropouts’ only with regard to a termination of study participation. Any withdrawal from the intervention will be referred to as ‘discharge’.
Participants
All the housing rehabilitation settings included in this study targeted similar populations. The inclusion and exclusion criteria were defined in accordance with the criteria of the included service providers to identify eligible participants.
Participants who were aged between 18 and 65 years, had a psychiatric diagnosis, were able to communicate in German, were able to take prescribed medication if indicated, had a source of income to pay for housing (including social insurance benefits), were in need of housing support, and were able to provide written informed consent were considered eligible.
Participants were excluded if they lacked the capacity to provide consent, had impaired cognitive abilities that affected the feasibility and validity of assessment interviews, including intoxication, delirium, and dementia, and if they were in need of acute psychiatric treatment at the time of admission to the residential service.
Data collection and outcome measures
The data were collected through interviews and questionnaires. Face-to-face interviews were conducted and continued via phone while the coronavirus pandemic containment measures were in place. In periods when the measures were stopped, participants could choose between face-to-face or phone interviews. The questionnaires were filled out by participants, or were assessed by interviews conducted with the study collaborators as per the participants’ preferences.
Sample characteristics
Demographic and clinical information were collected during the interviews with the participants. Demographic information included participants’ age (in years), gender (female or male), nationality (Swiss or non-Swiss), highest education (no graduation, elementary school, vocational education, and higher education), and the number and duration (in years) of previous stays in residential rehabilitation settings. Clinical information included the participants’ main psychiatric diagnosis categories according to the ICD-10 (41). Diagnoses were retrieved either from patient medical records or from participants’ self-reports according to their wishes. Some participants did not know and few participants did not accept their main diagnosis.
Primary outcome variable
The primary outcome of ‘social inclusion’ was measured using the German version of the Social Functioning Scale (SFS) (42, 43). In accordance with the UN CRPD, the goal of service users’ social inclusion and participation has highest priority in the rehabilitation of persons with SMI (5). The 76-item self-report questionnaire provides a measure of participants’ social inclusion and participation among seven subscales (social engagement, interpersonal behaviour, pro-social activities, recreational activities, independence-competence, independence-performance, and employment/occupation). Most items could be answered on a four point Likert scale. Raw subscale scores were transformed into standardised scale scores with m = 100 and SD = 15, with higher scores indicating better social inclusion.
Secondary outcome variables
Participants’ subjective quality of life was measured using the German Manchester Short Assessment of Quality of Life (MANSA) (44). The questionnaire assesses satisfaction with twelve life domains on a seven-point Likert scale, which are summarised as total mean scores between 1 and 7, with higher scores indicating a higher quality of life.
The severity of psychiatric symptoms was assessed using the nine-item Symptom Checklist (SCL-K-9) (45, 46). The questionnaire asked participants to assess the severity of their mental health symptoms within the past 7 days on a five-point Likert scale. A higher total mean score between 0 and 4 indicates more severe symptoms.
Statistical methods
Sample characteristics were examined for both conditions (ISH and HAU) at the two study centres (RCT and OS). Statistical testing of differences in sample characteristics was performed using an unpaired t-test (numeric variables) and Chi-square tests (categorical variables).
In the case of missing items in the primary and secondary outcome measures, available items were averaged to build raw (sub-) scale scores where possible (47, 48). Missing (sub-) scale scores at baseline were replaced with the sample means of the respective study sites (RCT or OS). The number of missing scale scores was low (RCT: 1.7% SFS independence-performance missing; OS: 1.2% SFS employment/occupational and 1.2% SCL-K-9 missing, each n = 1). No missing outcome data (T2) were imputed.
Propensity score methods
To balance the important baseline covariates between the two OS conditions, inverse probability of treatment weighting (IPTW) based on propensity scores (PS) was applied (49) and described according to published guidelines (50). The IPTW method was chosen because it suits the sample size well (27) and does not require the exclusion of cases (49). Covariates for the PS model were iteratively selected using theoretical and analytical approaches to find the best covariate balance between the OS conditions (18). Categorical covariates were dichotomised according to cut-offs (ordinal) or based on the frequency of occurrence in the two conditions (nominal; see Table 1) to achieve maximal balance in the OS. The final PS model included the covariates gender (female vs. male), age (in years), main psychiatric diagnosis (ICD-10 categories [F3, F4, and F6] vs. [F1, F2, and ‘other,’ which included the categories F7, F8, F9, and F0]), highest education (vocational training or higher vs. elementary school or below), and number of previous stays in residential rehabilitation settings. To estimate the PS, these covariates were inserted as predictors of treatment assignment in a logistic regression. PS estimation was separately applied for both study centres. There were no missing values in the baseline covariates.
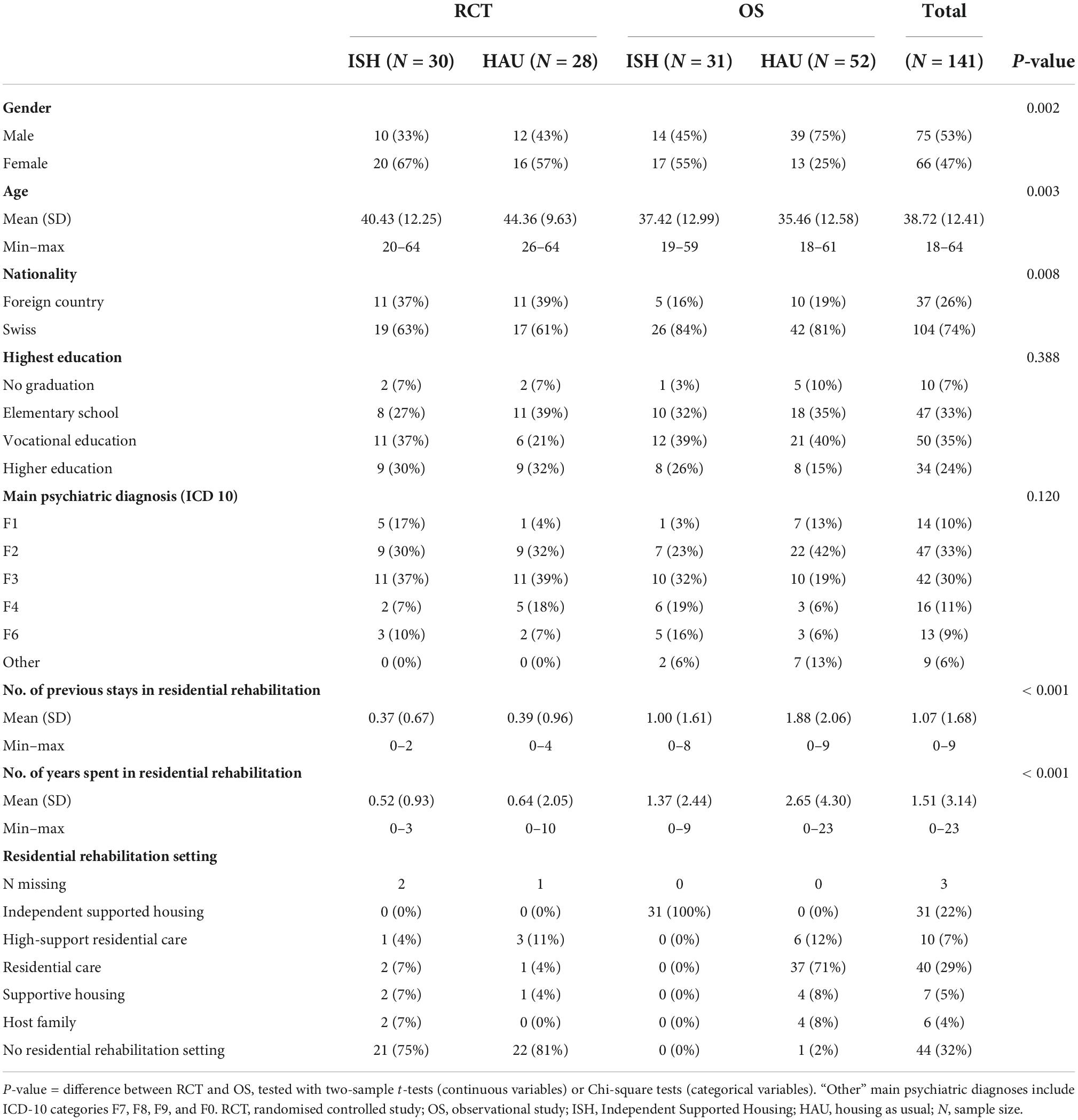
Table 1. Sample characteristics at baseline.
Based on the PS, IPTW was computed to estimate the average treatment effect (ATE) for the OS using the following formula (49) with Z denoting the study condition (Z = 1 intervention; Z = 0 control condition): . To avoid very large weights in the OS (> 9), which would increase the variability of the treatment effect (49), the resulting weights (mean IPTWISH = 2.84; range: 1.21–13.13; mean IPTWHAU = 1.56; 1.02–4.27) were truncated at the 2nd and 98th percentiles (truncated mean IPTWISH = 2.53; 1.21–8.02; mean IPTWHAU = 1.56; 1.04–4.27).
Balance in baseline covariates between the conditions was assessed using standardised differences d using the formulae derived by Austin (49, 51). The propensity-adjusted covariate balance (weighted d) in the OS was compared with the covariate balance in the RCT (unweighted d). A d below 10% indicates negligible imbalance (49, 51).
Outcome analyses
The main analyses focus on the primary outcome point T2 (12 months after baseline). The outcome analyses were conducted using 95% confidence interval (CI) testing on all outcome measures with PS-based IPT-weighted values in the OS and unweighted values in the RCT. To test the non-inferiority hypothesis, we tested whether the lower bound of the 95% CI of the mean differences (meanISH-meanHAU, with pooled SDs) of the SFS scale scores at T2 was above the non-inferiority margin of Δ = –15 in both intent-to-treat (ITT) and per-protocol (PP) analysis samples (52). The margin refers to one SFS standard deviation (for rationale of the margin see (32)). The ITT analysis included all participants with available outcome data in their assigned conditions, regardless of whether they used a residential rehabilitation support service. The PP analysis included all available data of participants who used the assigned housing rehabilitation setting (ISH or HAU) for at least 90 days between T0 (RCT) or admission (OS) and T2. Participants were also included in the PP analysis if they moved from one HAU setting to another and if their overall stay in HAU settings lasted for at least 90 days. In the case of proven non-inferiority, testing superiority is acceptable (53). Differences between conditions regarding the primary and secondary outcome measures was also assessed with a 95% CI of mean differences.
All statistical analyses were performed using the statistical software R (54). The significance level was set to α = 0.05 (two-tailed) for all analyses. For PS estimation, the glm function of the package stats was applied. IPT-weighted means were computed using ddply of the package plyr. IPTW and 95% CI were computed using the base R.
Results
Sample characteristics
Figure 1 shows the flowchart of participants’ recruitment and follow-up in the two study centres. The RCT included 58 participants (n = 30 in ISH; n = 28 in HAU) and the OS included 83 participants (n = 31 in ISH; n = 52 in HAU). In the RCT, two individuals declined to participate directly after randomisation (one in each condition), and two participants had to be excluded (both in HAU). Reasons for exclusion were non-compliance in assessment and having already started with ISH (each n = 1).
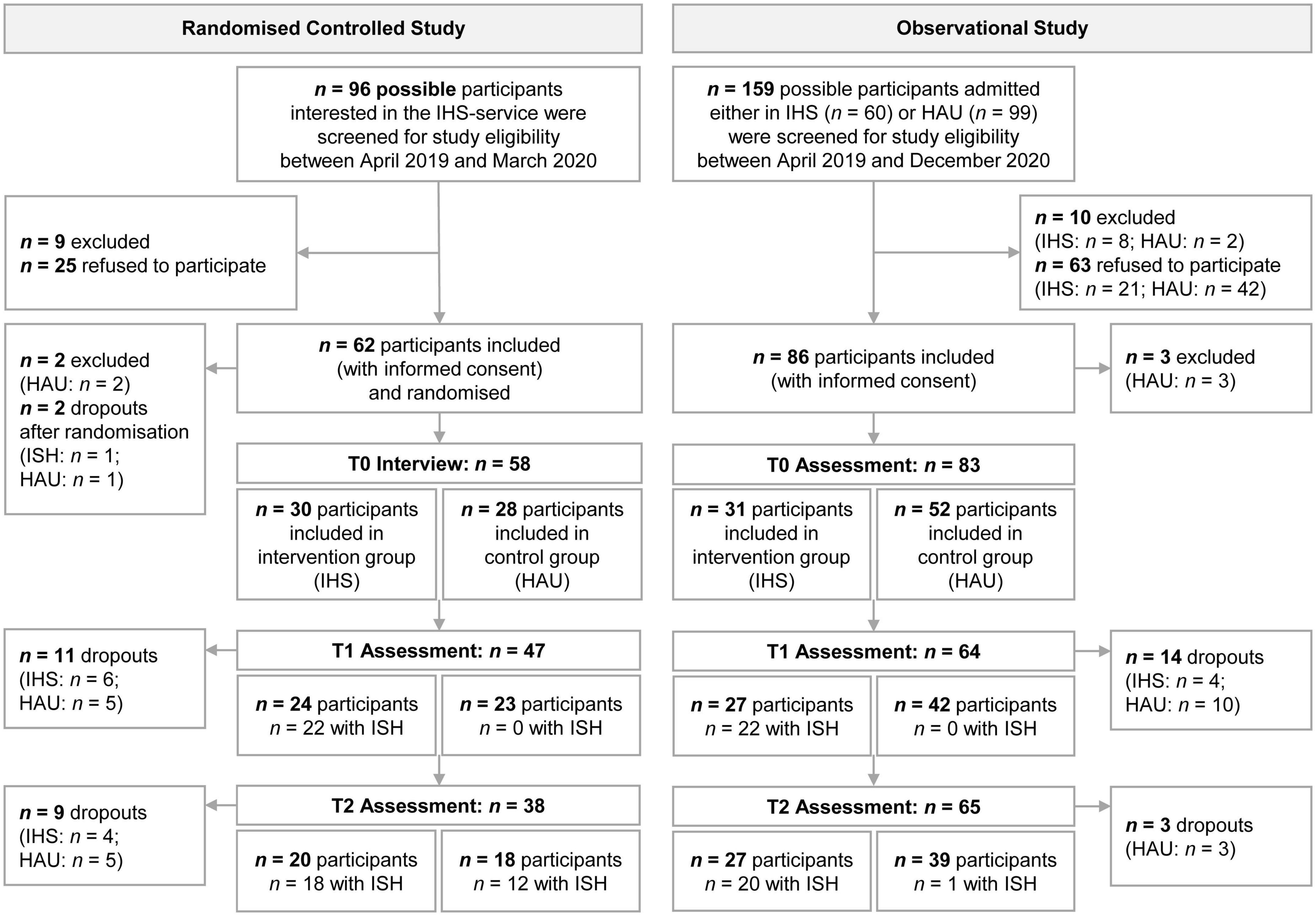
Figure 1. Flow chart of participants’ recruitment and follow-up. ISH, Independent Supported Housing; HAU, housing as usual; n, sample size.
Table 1 presents the participants’ baseline characteristics at both study centres. Participants had a mean age of m = 38.72 years (SD = 12.41), were mostly male (53%), had a Swiss nationality (74%), a vocational or higher education (59%), and a primary psychotic or schizophrenic (33%) or an affective diagnosis (30%), and had lived m = 1.07 (1.68) times in housing rehabilitation settings for m = 1.51 (3.14) years.
Participants in the OS significantly differed from participants in the RCT in their gender, age, nationality, and number and duration of previous stays in residential rehabilitation settings. The OS ISH condition did not significantly differ from the RCT samples in terms of gender and age (see Supplementary Table A).
In the RCT, most allocated participants used ISH support services (T1: n = 22 of the 24 participants; T2: n = 18 out of 20). Participants in the control condition who still preferred the ISH service had to be waitlisted at T1 because of ethical reasons (no longer deny participants the needed support considering the scarcity of comparable service). One year after randomisation (T2), 12 of the remaining 18 participants in the control group had started using the ISH service. Thus, at T2, the majority of participants in both conditions (ISH and HAU) used the ISH intervention. Even when service utilisation has only started recently, this compromises the purpose of the RCT design and the validity of its outcome analyses below. Most ISH participants (95%, 19 out of 20 participants at T2) met the PP definition of having utilised the allocated housing rehabilitation service for at least 90 days (mean duration = 266, SD = 112 days). However, only very few control participants lived in a HAU setting for 90 days or more (17%, 3 out of 18 participants at T2, mean duration = 240, SD = 168 days). Of the initial sample, 34.5% dropped out from the study by T2 (T1: n = 11; T2: n = 9), and 70% of the ISH dropouts occurred after their ISH discharge.
In the OS, most ISH participants still used ISH during follow-up (T1: n = 22 of the 27 participants; T2: n = 20 out of 27). At T2, one participant in the control condition started using ISH. All participants who discharged from ISH service still lived independently in their homes and continued to participate in the study. Of the included participants, 20.5% dropped out from the study (T1: n = 14; T2: n = 3). Some participants missed an assessment without dropping out (T1: n = 5; T2: n = 1; therefore, in Figure 1, the number of assessments does not equal the number of participants). The PP definition was met by most participants in both conditions (ISH: 96%, 25 out of 26 participants at T2; HAU: 95%, 37 out of 39 participants at T2) and utilisation duration was high in both conditions (ISH: mean = 365, SD = 112 days; HAU: mean = 333, SD = 119 days). Most dropouts occurred in the HAU group (HAU: 25%; ISH: 12.9%).
In both study sites, those who completed the study significantly differed from dropouts only with regard to their main psychiatric diagnoses at T1 and T2 (OS: p = 0.009 and p = 0.003, RCT: p = 0.004 and p = 0.010; details are shown in Supplementary Table B).
Propensity score
In both study sites (RCT and OS), the PS distribution showed a good overlap between the conditions (Figure 2). The larger the overlapping region of the PS in the histogram, the more comparable were the conditions in terms of the covariate distribution. The RCT showed a better PS balance than the OS due to random allocation.
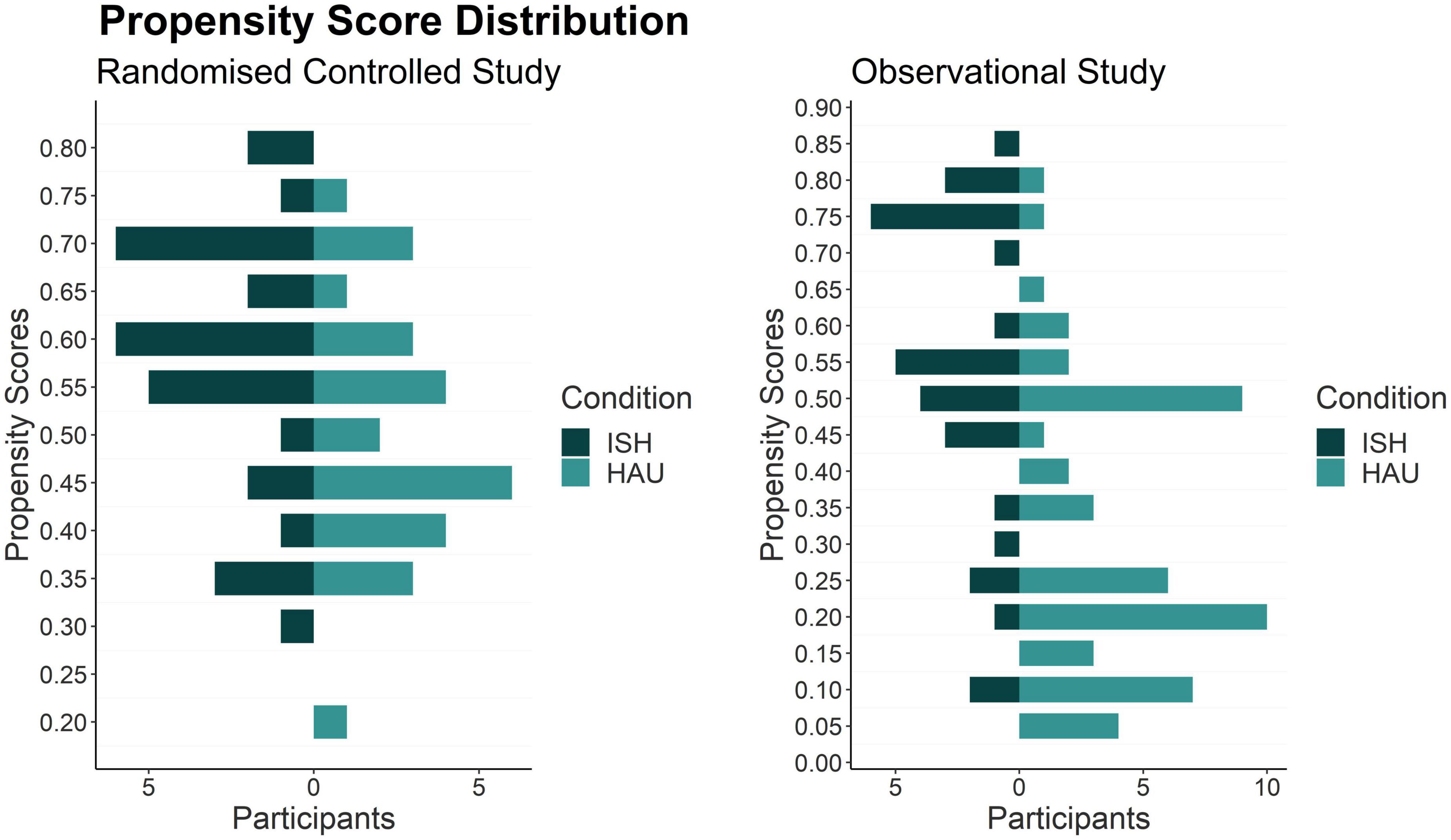
Figure 2. Histogram of PS-distribution between study conditions in the RCT and the OS. ISH, Independent Supported Housing; HAU, housing as usual.
The standardized differences in the RCT presented in Figure 3 show moderate covariate balance with d ranging between 2.5 (previous stays in ISH/HAU) and 30.3 (age). The unweighted covariates in the OS showed a high imbalance, with d ranging between 12.6 (age) and 65.1 (psychiatric diagnosis). Good covariate balance in the OS could be achieved with weighting based on PS, with weighted d ranging between 5.2 (education) and 8.7 (previous stay in ISH/HAU).
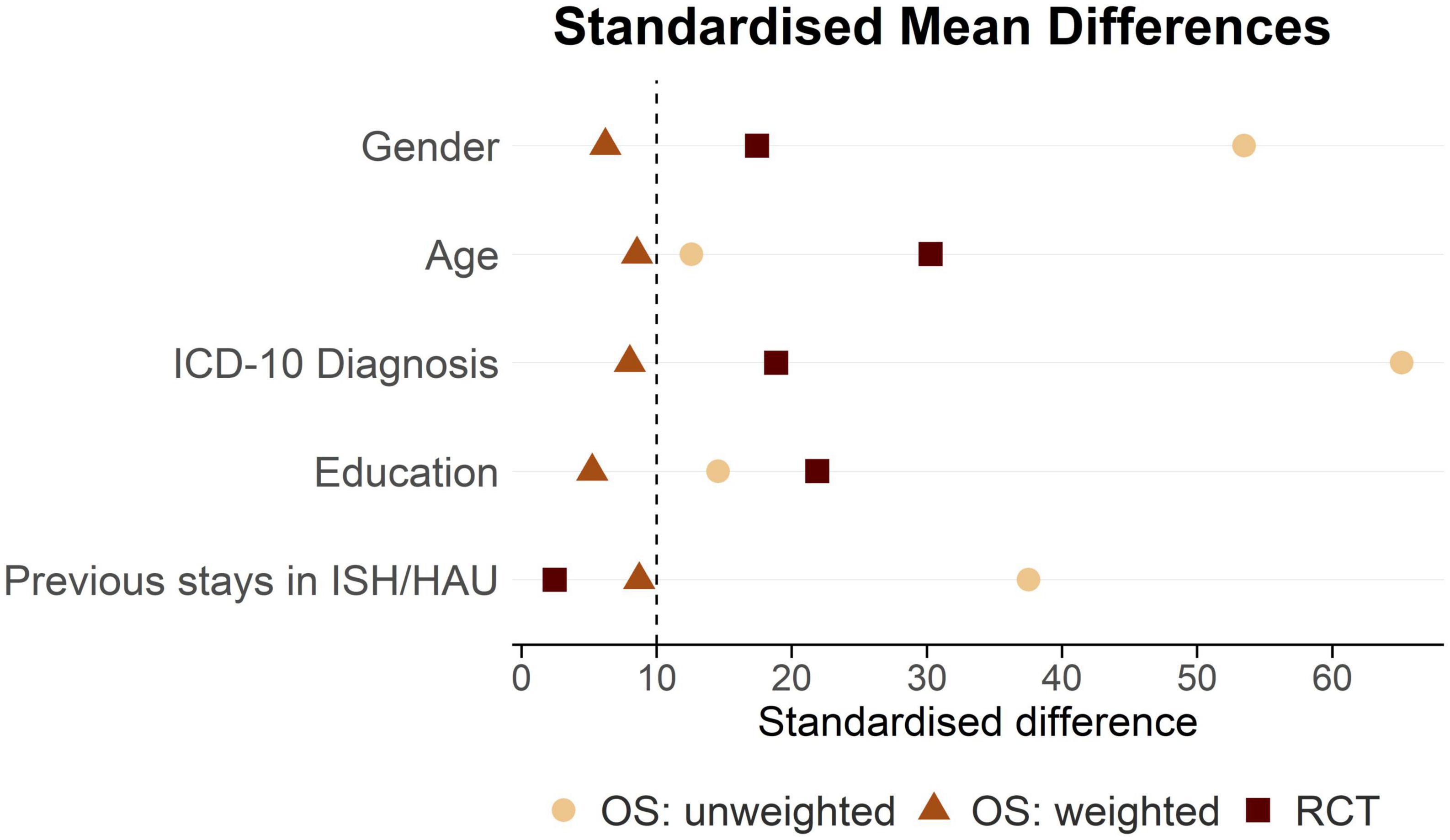
Figure 3. Standardised differences of unweighted and IPTW-weighted covariates included in the PS-model. RCT, randomised controlled study; OS, observational study; ISH, Independent Supported Housing; HAU, housing as usual; IPTW, inverse probability of treatment weighting; PS, propensity score.
Outcome analysis
Figure 4 shows the mean differences and 95% CI of the outcome variables at baseline (T0) and after 12 months (T2) for the two study sites (RCT and OS; for means and SDs of the outcome measures, see Supplementary Table C).
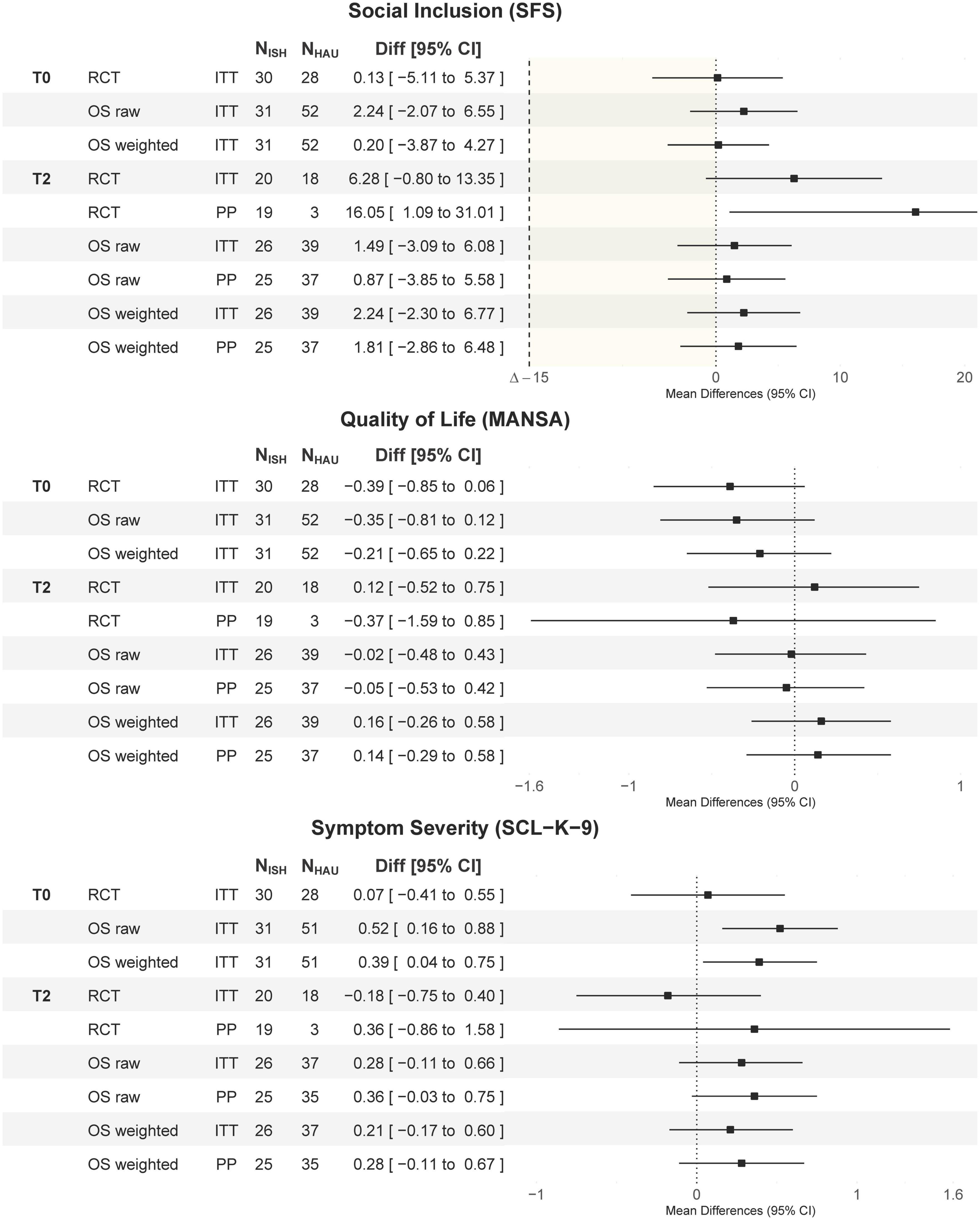
Figure 4. Mean differences (meanISH-meanHAU) and 95% CI of differences. Outcome analysis in social inclusion, quality of life, and psychiatric symptoms at baseline (T0) and after 12 months (T2) separately for the RCT, the unweighted, and IPTW-weighted OS study arms. Every analysis was conducted for both the ITT and the PP sample. RCT, randomized controlled study; OS, observational study; ITT, intent to treat; PP, per-protocol; N, sample size; ISH, Independent Supported Housing; HAU, housing as usual; Diff, mean differences; SFS, Social Functioning Scale, MANSA, Manchester Short Assessment of Quality of Life; SCL-K-9, 9-item Symptom Checklist; IPTW, inverse probability of treatment weighting.
The non-inferiority test of the primary outcome variable SFS showed the lower level of the 95% CI of meanISH-meanHAU above the non-inferiority margin of Δ = –15 in both the ITT and PP samples in both study sites (RCTITT: –0.80 to 13.35; RCTPP: 1.09 to 31.01; OSITT: –2.30 to 6.77; OSPP: –2.86 to 6.48), indicating that ISH is not inferior to HAU settings in terms of social inclusion. When testing for differences, only the RCT PP analysis at T2 showed superiority (95% CI: 1.09 to 31.01). However, this analysis only included n = 3 HAU participants who fulfilled the PP definition. All other comparisons showed no significant SFS differences between ISH and HAU, indicating no superiority of either condition.
There were also no significant mean differences [95% CI] between ISH and HAU in terms of quality of life (MANSA: RCTITT: 0.12 [–0.52 to 0.75]; RCTPP: –0.37 [–1.59 to 0.85]; OSITT: 0.16 [–0.26 to 0.58]; OSPP: 0.14 [–0.29 to 0.58]) and symptoms (SCL-K-9: RCTITT: –0.18 [–0.75 to 0.40]; RCTPP: 0.36 [–0.86 to 1.58]; OSITT: 0.21 [–0.17 to 0.60]; OSPP: 0.28 [–0.11 to 0.67]) after 12 months. However, there were significant differences in baseline symptoms in the OS, with higher SCL-K-9 scores in the ISH group than in the HAU group (ISH: m = 1.44, SD = 0.86; HAU: m = 1.04, SD = 0.72; 95% CI: 0.04 to 0.75).
Discussion
Two centres concurrently conducted the same prospective study on the effectiveness of ISH versus HAU in non-homeless individuals with SMI, applying two different study designs. The comparison of the two study centres showed significant problems in the conduction of the RCT due to participants’ strong and persisting preferences for ISH. In contrast, the OS achieved a very good covariate balance after PS-based weighting, which allows a valid estimation of the ISH effectiveness. Because of several limitations in the RCT, the results of the RCT and the OS are not comparable. Thus, the comparison of the two studies did not confirm the hypothesis that the OS provides as good evidence as the RCT. Although the OS design is not an equivalent option to the RCT, the OS showed to be a valid option in complex situations when RCTs are not feasible as it was the case with the strong preferences for one of the two housing rehabilitation settings for persons with SMI.
In the RCT, there was a strong and persistent preference for ISH. Only three participants in the control condition fulfilled the PP criteria of residing in a residential setting for at least 90 days until T2 (four until T1). Instead, for ethical reasons and prevention of a high dropout rate, 70% of the HAU participants were waitlisted at T1, and two-thirds started with ISH before T2. Therefore, the control condition was a waitlist control rather than an active control, as was the case in the OS. This introduced severe problems in the RCT study. On the one hand, non-inferiority hypothesis testing requires an active control condition, which was not the case here. Furthermore, the need to allow control participants to start with ISH before the primary outcome point T2 undermined the purpose of the RCT of investigating controlled effectiveness of ISH vs. HAU. In addition, it did not allow proceeding the study for another year. However, because most ISH participants were still using ISH after one year, the intended study spanning of at least two years would have been required to investigate the intervention’s effectiveness (32). Participants who discharged from the ISH service commonly also dropped out from the study, while most waitlisted participants remained in the study. This indicates that participants’ motivation to participate at the study seemed strongly influenced by their motivation to use ISH, since study participation was a precondition. Limiting access to a strongly preferred intervention only to study participants puts their voluntary participation into question. Consequently, although it was somewhat possible to perform the first RCT on the effectiveness of ISH for non-homeless individuals with SMI, it did not work as intended or as would have been necessary for valid conclusions from an RCT study.
In contrast, the OS design provides a much higher potential for conducting a longitudinal investigation of housing rehabilitation settings. The OS design showed to be much more user friendly because study participation was not a precondition for access to specific support during the entire study. Accordingly, willingness to participate was much higher in the OS, as reflected in the large PP sample and low dropout rates in both conditions. All but three (one ISH and two HAU) participants fulfilled the PP criteria, and study dropouts were not related to service utilisation; most occurred due to a loss of motivation. Study participation remained high among those who discharged from their housing rehabilitation settings. The effectiveness results of the OS showed non-inferiority of ISH to HAU regarding social inclusion and showed no significant differences in quality of life and symptoms after one year.
This study has some limitations. Deviations from the study protocol (32) occurred in the following aspects. First, RCT participants in the control group were given the opportunity to be waitlisted after T1 because of their strong and persistent preference for ISH. Second, two third of the wait-listed participants already started with ISH before T2, which may have affected the results at T2 and made it impossible for the RCT to proceed for another year as planned. Finally, the intended sample size for the OS control group was not reached after the recruitment phase. Consequently, the PS-based IPTW method was applied instead of the planned many-to-one matching. However, this had important advantages, as IPTW seems to perform better than matching in small samples (27, 55, 56). In addition, IPTW allows the analysis of the entire sample without excluding unmatched subjects (57). Other limitations besides the protocol deviations should further be noted. There were some regional differences in the supply of the ISH service (e.g., maximal amount of weekly support) and in participant characteristics between the RCT and the OS. Regional differences will always be an issue in ISH studies and may introduce a large amount of heterogeneity. In addition, sociodemographic and clinical data were assessed through interviews with participants and there was not always an opportunity to externally verify participants’ self-reported diagnosis. Although the vast majority of diagnoses were verified by a clinician or their case reports, this may be a source of potential bias. Our results complement the results of a recent feasibility trial which also did not support the implementation of randomised trials on ISH for non-homeless persons (31). The feasibility trial failed to recruit sufficient participants to conduct an effectiveness trial because of participants’ and staff members’ strong preferences. Our randomised study site was only able to randomise participants due to the scarcity of housing rehabilitation interventions similar to ISH in the area. Therefore, it was possible to limit access to ISH to only the study participants. However, strong preferences for ISH did not allow ensuring service utilisation in the control condition in an ethical manner. As a result, we were able to recruit sufficient participants, but the control group resulted in a passive waitlist condition rather than an active control. Furthermore, allowing control participants to start with the intervention before the primary outcome assessment invalidate the comparison of the two conditions. Based on this, it seems impossible to conduct an RCT on the effectiveness of ISH compared to an active residential rehabilitation condition for non-homeless persons. Although a passive control group could allow an RCT to be conducted, this would deny access to the needed support, which is ethically questionable.
Randomised trials as the ‘gold standard’ in intervention studies generally provide much better prevention of alternative explanations for a resulting effect estimation than other study designs. However, strong preferences impede the possibility of conducting RCTs on psychiatric rehabilitation interventions or may bias the results (17). A meta-analysis showed positive effects on treatment outcomes when participants were allocated the preferred treatment (preference effect: d = 0.18) or had an opportunity to choose a treatment in the study (choice effect: d = 0.14) (58). The preference effect was more apparent in mental health interventions than in pain and functional therapies (d = 0.23 vs. d = 0.09). Several extensions of the RCT design have been proposed to accommodate preferences (59); however, their application has not succeeded in the feasibility trial (31). Therefore, alternatives to the randomised design are needed to foster evidence regarding the effectiveness of ISH, and the OS proved to produce valid results in the present study as well as in many preceding studies (20). The applied PS-based IPTW method produced a good balance of sample covariates, and evidence suggests a good bias reduction in the case of a rather small sample size (27, 49). In addition to the OS design, other quantitative study designs should be explored to complement existing evidence. For example, the self-controlled mirror-image design known from pharmacology has been shown to overcome the risk of confounding owing to time-invariant sample characteristics because every subject acts as its own control (60, 61). This design allows for causal inference when time-variant confounding (i.e., regression toward the mean) is adequately addressed (60). Evidence is generally better when the results of different study designs agree (23) and most convincing when the weaknesses of the design are well understood, measured, and controlled (16). To increase evidence-based knowledge on ISH for non-homeless individuals, methodological strategies to enhance the quality of a given design that suits the investigational conditions seem much more appropriate than investing again in an RCT.
Finally, strong preferences for ISH over HAU settings are also a major reason for the recommendation in the guidelines to offer access to ISH as the first choice, despite its mixed and weak evidence regarding the non-homeless population (5, 12, 13). Service users’ preferences should be the decisive factor in the choice of housing support form. In addition, person-centred mental health care and interventions to improve personal recovery, empowerment, and social inclusion are based on informed decisions and thus on service users’ preferences. Thus, if a newer intervention shows to be non-inferior to the standard intervention, it does not matter which intervention service users choose to use.
Conclusion
While the RCT showed major limitations because of strong preferences for the intervention condition ISH, the OS with propensity score methods showed very good feasibility, revealed balanced sample characteristics and valid outcome analyses. Our results should encourage researchers to apply well-conducted alternative study designs that allow service users the right to choose their place of residence and needed support services. These findings do not support further investment in randomised trials to investigate the effectiveness of housing rehabilitation settings. In addition, our results support the treatment guidelines’ prioritisation of ISH over HAU and advocate its wider implementation in psychiatric rehabilitation to allow freedom of choice regarding one’s place of residence. According to our results, a preference-driven supply of residential rehabilitation services is the most appropriate.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the corresponding author after a written agreement between the authors and researchers who wish to access the data.
Ethics statement
This study received ethical approval from the Swiss Association of Research Ethics Committees (Swissethics), Reference No. 2018–02381. All participants provided written informed consent for participation.
Author contributions
MJ and DR: conceptualization, funding acquisition, project administration, and supervision. CA and SM: data curation and investigation. CA: formal analysis, visualization, and writing—original draft preparation. SM, MJ, and DR: writing—review and editing. CA, SM, MJ, and DR: methodology. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by a grant from the Swiss National Science Foundation https://snf.ch/de (10531C_179451). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments
We are grateful to all participants, service providers, and staff of the participating housing rehabilitation settings.
Conflict of interest
Authors CA, SM, and DR are affiliated with institutions that also provide some of the participating housing rehabilitation services.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.1033328/full#supplementary-material
Abbreviations
ISH, Independent Supported Housing; HAU, Housing as usual; SMI, Severe mental illness; RCT, Randomised controlled study; OS, Observational study; PS, Propensity Score; IPTW, Inverse probability of treatment weighting.
References
1. Dalton-Locke C, Marston L, McPherson P, Killaspy H. The effectiveness of mental health rehabilitation services: a systematic review and narrative synthesis. Front Psychiatry. (2021) 11:607933. doi: 10.3389/fpsyt.2020.607933
2. Priebe S, Badesconyi A, Fioritti A, Hansson L, Kilian R, Torres-Gonzales F, et al. Reinstitutionalisation in mental health care: comparison of data on service provision from six European countries. BMJ. (2005) 330:123–6. doi: 10.1136/bmj.38296.611215.AE
3. Fakhoury W, Priebe S. Deinstitutionalization and reinstitutionalization: major changes in the provision of mental healthcare. Psychiatry. (2007) 6:313–6. doi: 10.1016/j.mppsy.2007.05.008
4. Richter D, Hoffmann H. Die deinstitutionalisierung der psychiatrischen versorgung ist nicht gelungen. Sozialpsychiatrische Informationen. (2016) 2:11–3.
5. United Nations. Convention on the Rights of Persons with Disabilities. New York: United Nations. (2006).
6. Richter D, Hoffmann H. Preference for independent housing of persons with mental disorders: systematic review and meta-analysis. Adm Policy Ment Health. (2017) 44:817–23. doi: 10.1007/s10488-017-0791-4
7. Tanzman B. An overview of surveys of mental health consumers’ preferences for housing and support services. Psychiatr Serv. (1993) 44:450–5. doi: 10.1176/ps.44.5.450
8. Aubry T, Bloch G, Brcic V, Saad A, Magwood O, Abdalla T, et al. Effectiveness of permanent supportive housing and income assistance interventions for homeless individuals in high-income countries: a systematic review. Lancet Public Health. (2020) 5:e342–60. doi: 10.1016/S2468-2667(20)30055-4
9. McPherson P, Krotofil J, Killaspy H. Mental health supported accommodation services: a systematic review of mental health and psychosocial outcomes. BMC Psychiatry. (2018) 18:128. doi: 10.1186/s12888-018-1725-8
10. Richter D, Hoffmann H. Independent housing and support for people with severe mental illness: systematic review. Acta Psychiatr Scand. (2017) 136:269–79. doi: 10.1111/acps.12765
11. Martinelli A, Iozzino L, Ruggeri M, Marston L, Killaspy H. Mental health supported accommodation services in England and in Italy: a comparison. Soc Psychiatry Psychiatr Epidemiol. (2019) 54:1419–27. doi: 10.1007/s00127-019-01723-9
12. World Health Organization [WHO]. Guidance on community mental health services: Promoting person-centred and rights-based approaches. Geneva: World Health Organization (2021).
13. Gühne U, Weinmann S, Riedel-Heller SG, Becker T. S3-Leitlinie psychosoziale Therapien bei schweren psychischen Erkrankungen: S3-Praxisleitlinien in Psychiatrie und Psychotherapie. DGPPN, editor. Berlin: Springer-Verlag (2019).
14. Gühne U, Stein J, Weinmann S, Becker T, Riedel-Heller SG. wohninterventionen für menschen mit schweren psychischen störungen – internationale evidenz aus RCTs. Psychiatr Prax. (2017) 44:194–205. doi: 10.1055/s-0042-118594
15. Dehn LB, Beblo T, Richter D, Wienberg G, Kremer G, Steinhart I, et al. Effectiveness of supported housing versus residential care in severe mental illness: a multicenter, quasi-experimental study. Soc Psychiatry Psychiatr Epidemiol. (2022) 57:927–37. doi: 10.1007/s00127-021-02214-6
16. Bonell CP, Hargreaves J, Cousens S, Ross D, Hayes R, Petticrew M, et al. Alternatives to randomisation in the evaluation of public health interventions: design challenges and solutions. J Epidemiol Community Health. (2011) 65:582–7. doi: 10.1136/jech.2008.082602
17. Macias C, Gold PB, Hargreaves WA, Aronson E, Bickman L, Barreira PJ, et al. Preference in random assignment: implications for the interpretation of randomized trials. Adm Policy Ment Health. (2009) 36:331–42. doi: 10.1007/s10488-009-0224-0
18. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. (2011) 46:399–424. doi: 10.1080/00273171.2011.568786
19. Trentino K, Farmer S, Gross I, Shander A, Isbister J. Observational studies – should we simply ignore them in assessing transfusion outcomes? BMC Anesthesiol. (2016) 16:96. doi: 10.1186/s12871-016-0264-4
20. Anglemyer A, Horvath HT, Bero L. Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials. Cochrane Database Syst Rev. (2014) 4:MR000034. doi: 10.1002/14651858.MR000034.pub2
21. Ioannidis JP, Haidich A-B, Pappa M, Pantazis N, Kokori SI, Tektonidou MG, et al. Comparison of evidence of treatment effects in randomized and nonrandomized studies. JAMA. (2001) 286:821–30. doi: 10.1001/jama.286.7.821
22. Concato J, Shah N, Horwitz RI. Randomized, controlled trials, observational studies, and the hierarchy of research designs. N Engl J Med. (2000) 342:1887–92. doi: 10.1056/NEJM200006223422507
23. Gershon AS, Jafarzadeh SR, Wilson KC, Walkey AJ. Clinical knowledge from observational studies. Everything you wanted to know but were afraid to ask. Am J Respir Crit Care Med. (2018) 198:859–67. doi: 10.1164/rccm.201801-0118PP
24. Shadish WR. Randomized controlled studies and alternative designs in outcome studies: challenges and opportunities. Res Soc Work Pract. (2011) 21:636–43. doi: 10.1177/1049731511403324
25. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
26. Cousens S, Hargreaves J, Bonell C, Armstrong B, Thomas J, Kirkwood B, et al. Alternatives to randomisation in the evaluation of public-health interventions: statistical analysis and causal inference. J Epidemiol Community Health. (2011) 65:576–81. doi: 10.1136/jech.2008.082610
27. Pirracchio R, Resche-Rigon M, Chevret S. Evaluation of the propensity score methods for estimating marginal odds ratios in case of small sample size. BMC Medical Res Methodol. (2012) 12:70. doi: 10.1186/1471-2288-12-70
28. Duncan C, Weich S, Fenton S-J, Twigg L, Moon G, Madan J, et al. A realist approach to the evaluation of complex mental health interventions. Br J Psychiatry. (2018) 213:451–3. doi: 10.1192/bjp.2018.96
29. Staines GL, Cleland CM. Observational studies versus randomized controlled trials of behavioral interventions in field settings. Rev Gen Psychol. (2012) 16:37–58. doi: 10.1037/a0026493
30. Olschewski M, Scheurlen H. Comprehensive cohort study: an alternative to randomized consent design in a breast preservation trial. Methods Inf Med. (1985) 24:131–4. doi: 10.1055/s-0038-1635365
31. Killaspy H, Priebe S, McPherson P, Zenasni Z, McCrone P, Dowling S, et al. Feasibility randomised trial comparing two forms of mental health supported accommodation (supported housing and floating outreach); a component of the QuEST (quality and effectiveness of supported tenancies) study. Front Psychiatry. (2019) 10:258. doi: 10.3389/fpsyt.2019.00258
32. Adamus C, Mötteli S, Jäger M, Richter D. Independent housing and support for non-homeless individuals with severe mental illness: randomised controlled trial vs. observational study – study protocol. BMC Psychiatry. (2020) 20:319. doi: 10.1186/s12888-020-02712-y
33. Mötteli S, Adamus C, Deb T, Fröbel R, Siemerkus J, Richter D, et al. Independent supported housing for non-homeless people with serious mental illness: a pragmatic randomized controlled trial. Front Psychiatry. (2022) 12:798275. doi: 10.3389/fpsyt.2021.798275
34. Tsemberis S. From streets to homes: an innovative approach to supported housing for homeless adults with psychiatric disabilities. J Community Psychol. (1999) 27:225–41. doi: 10.1002/(SICI)1520-6629(199903)27:23.0.CO;2-Y
35. McPherson P, Krotofil J, Killaspy H. What works? Toward a new classification system for mental health supported accommodation services: the simple taxonomy for supported accommodation (STAX-SA). Int J Environ Res Public Health. (2018) 15:190. doi: 10.3390/ijerph15020190
36. Chan KPK, Kathryn K, Igoumenou A, Killaspy H. Predictors of successful move-on to more independent accommodation amongst users of the community mental health rehabilitation team: a prospective cohort study in inner London. Soc Psychiatry Psychiatr Epidemiol. (2021) 56:75–84. doi: 10.1007/s00127-020-01910-z
37. Richter D, Adamus C, Motteli S, Myszor F, Wienberg G, Steinhart I. [Supported housing - development and validation of the “supported housing fidelity scale” for people with mental health problems]. Psychiatr Prax. (2021) 49:103–6. doi: 10.1055/a-1509-4666
38. HyLown Consulting LLC. Power and Sample Size. (2013). Available online at: http://powerandsamplesize.com/Calculators/Compare-2-Means/2-Sample-Non-Inferiority-or-Superiority (accessed October 2, 2017).
39. Bai H. Methodological considerations in implementing propensity score matching. In: Pan W, Bai H editors. Propensity score analysis: Fundamentals and developments. New York: Guilford (2015). p. 74–88. doi: 10.1016/j.zefq.2011.12.007
40. Austin PC. Statistical criteria for selecting the optimal number of untreated subjects matched to each treated subject when using many-to-one matching on the propensity score. Am J Epidemiol. (2010) 172:1092–7. doi: 10.1093/aje/kwq224
41. World Health Organization [WHO]. The ICD-10 classification of mental and behavioural disorders. Genève: World Health Organization (1993).
42. Birchwood M, Smith J, Cochrane R, Wetton S, Copestake S. The social functioning scale – the development and validation of a new scale of social adjustment for use in family intervention programmes with schizophrenic patients. Br J Psychiatry. (1990) 157:853–9. doi: 10.1192/bjp.157.6.853
43. Iffland JR, Lockhofen D, Gruppe H, Gallhofer B, Sammer G, Hanewald B. Validation of the German version of the social functioning scale (SFS) for schizophrenia. PLoS One. (2015) 10:e0121807. doi: 10.1371/journal.pone.0121807
44. Priebe S, Huxley P, Knight S, Evans S. Application and results of the manchester short assessment of quality of life (MANSA). Int J Soc Psychiatry. (1999) 45:7–12. doi: 10.1177/002076409904500102
45. Klaghofer R, Brähler E. Konstruktion und teststatistische prüfung einer kurzform der SCL-90-R. Z klin Psychol Psychiatr Psychother. (2001) 49:115–24.
46. Prinz U, Nutzinger D, Schulz H, Petermann F, Braukhaus C, Andreas S. Die symptom-checkliste-90-r und ihre kurzversionen: psychometrische analysen bei patienten mit psychischen erkrankungen. Phys Medizin Rehabilitationsmedizin Kurortmedizin. (2008) 18:337–43. doi: 10.1055/s-0028-1093323
47. Newman DA. Missing data: five practical guidelines. Organ Res Methods. (2014) 17:372–411. doi: 10.1177/1094428114548590
48. Parent MC. Handling item-level missing data: simpler is just as good. Couns Psychol. (2013) 41:568–600. doi: 10.1177/0011000012445176
49. Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med. (2015) 34:3661–79. doi: 10.1002/sim.6607
50. Ali MS, Groenwold RH, Belitser SV, Pestman WR, Hoes AW, Roes KC, et al. Reporting of covariate selection and balance assessment in propensity score analysis is suboptimal: a systematic review. J Clin Epidemiol. (2015) 68:122–31. doi: 10.1016/j.jclinepi.2014.08.011
51. Austin PC. Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Commun Stat Simul Comput. (2009) 38:1228–34. doi: 10.1080/03610910902859574
52. Rehal S, Morris TP, Fielding K, Carpenter JR, Phillips PP. Non-inferiority trials: are they inferior? A systematic review of reporting in major medical journals. BMJ Open. (2016) 6:e012594. doi: 10.1136/bmjopen-2016-012594
53. Piaggio G, Elbourne DR, Pocock SJ, Evans SJ, Altman DG, Consort Group. Reporting of noninferiority and equivalence randomized trials: extension of the consort 2010 statement. JAMA. (2012) 308:2594–604. doi: 10.1001/jama.2012.87802
54. R Core Team. R: a language and environment for statistical computing. R version 4.0. 3 ed. Vienna, Austria: R Foundation for Statistical Computing (2020).
55. Holmes W, Olsen L, editors. Using propensity scores with small samples. San Antonio: Annual meetings of the American Evaluation Association (2010).
56. Parks D, Lin X, Lee K. Assessing statistical methods for causal inference in observational data. Value Health. (2014) 17:A731. doi: 10.1016/j.jval.2014.08.084
57. Allan V, Ramagopalan SV, Mardekian J, Jenkins A, Li X, Pan X, et al. Propensity score matching and inverse probability of treatment weighting to address confounding by indication in comparative effectiveness research of oral anticoagulants. J Comp Eff Res. (2020) 9:603–14. doi: 10.2217/cer-2020-0013
58. Delevry D, Le QA. Effect of treatment preference in randomized controlled trials: systematic review of the literature and meta-analysis. Patient. (2019) 12:593–609. doi: 10.1007/s40271-019-00379-6
59. Ismaila AS, Walter SD. Review of Designs for Accommodating Patients’ or Physicians’ Preferences in Randomized Controlled Trials. In: van Montfort, K., Oud, J., Ghidey, W editors. Developments in Statistical Evaluation of Clinical Trials. Berlin: Springer (2014). p. 305–33.
60. Kishimoto T, Nitta M, Borenstein M, Kane JM, Correll CU. Long-acting injectable versus oral antipsychotics in schizophrenia: a systematic review and meta-analysis of mirror-image studies. J Clin Psychiatry. (2013) 74:957–65. doi: 10.4088/JCP.13r08440
Keywords: Independent Supported Housing, psychiatric rehabilitation, effectiveness study, study design, randomised controlled study, observational study, propensity score, preference
Citation: Adamus C, Mötteli S, Jäger M and Richter D (2022) Independent Supported Housing for non-homeless individuals with severe mental illness: Comparison of two effectiveness studies using a randomised controlled and an observational study design. Front. Psychiatry 13:1033328. doi: 10.3389/fpsyt.2022.1033328
Received: 31 August 2022; Accepted: 24 October 2022;
Published: 10 November 2022.
Edited by:
Tilman Steinert, ZfP Südwürttemberg, GermanyReviewed by:
Helen Killaspy, University College London, United KingdomIda Haussleiter, Ruhr University Bochum, Germany
Copyright © 2022 Adamus, Mötteli, Jäger and Richter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christine Adamus, Y2hyaXN0aW5lLmFkYW11c0B1cGQudW5pYmUuY2g=