
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 01 December 2022
Sec. Autism
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.1026191
 Mathilde Berard1,2
Mathilde Berard1,2 Marianne Peries1,2,3Julie Loubersac1,2,3Marie-Christine Picot2,3,4
Marianne Peries1,2,3Julie Loubersac1,2,3Marie-Christine Picot2,3,4 Jonathan Y. Bernard5,6
Jonathan Y. Bernard5,6 Kerim Munir7
Kerim Munir7 Amaria Baghdadli1,2,3,8*
Amaria Baghdadli1,2,3,8*  for the ELENA study group
for the ELENA study groupBackground: The COVID-19 pandemic may affect the screen time of children and adolescents with Autism Spectrum Disorders (ASD). This study aimed to examine the screen time of children and adolescents with ASD during a discrete lockdown period in France and identify risk factors for excessive screen time.
Methods: The study sample consisted of 249 ASD subjects, 3–17 years of age, enrolled in the ELENA cohort. Information about the screen time was collected using the COVID-19 questionnaire specially created for this study. The clinical, socio-demographic and familial characteristics were collected from the last ELENA follow-up visit.
Results: More than one third of subjects exceeded recommended levels of screen time and almost half of parents reported that their child spent more time using screen since COVID-19 pandemic beginning. Excessive screen time was significantly related to age with higher screen time in adolescents. Risk factors for excessive screen time were high withdrawn behaviors and low socioeconomic status for children, and older age and male gender for adolescents.
Conclusion: These results imply to adapt the recommendations already formulated in general population concerning the good use of screens in youth with ASD. Specific recommendations and suitable guidance are needed to help children and adolescents with ASD and their parents implement the more optimal use of screen time activities for educational, therapeutic and social goals.
Trial registration number: NCT02625116.
The use of television and mobile devices by children and adolescents with autism spectrum disorders (ASD) occupies a central place in their everyday lives. Current measure of screen time is the total duration (usually in hours/day) of time spent viewing programs, or playing video games, on television, a computer, or a mobile device. Other consistent finding is that, over the ensuing decades, the screen time among children and adolescents has been increasing. To date, studies of screen time of children and adolescents in the general population pointed to poorer health outcomes in terms of sedentary health risks, behavioral strengths and difficulties scores, prosocial behaviors (1, 2), psychological wellbeing, quality of life (3), sleep (4), as well as depressive (3, 5), and anxiety disorders (6). It has also been suggested that excessive screen time can lead to worsening of autism-like symptoms (7–10), attention deficit hyperactivity disorder (ADHD) (11, 12), dyslexia (13), as well as language, cognitive, and motor acquisition delays (14, 15).
To date, the indicators of risk for excessive screen time in children and adolescents in the general population have included male gender, older age, urban residence, insufficient home living and play space, lower parental education, lower household income, and inconsistent parenting practice in terms of ability to control screen time behaviors (16–20).
Given the concerns about the negative impact of excessive screen time of children and adolescents, a number of international guidelines have been proposed (21–24). The guidelines consistently recommend for children and adolescents not to exceed an hour of screen time daily for ages 2–5 years, and 2 h daily for ages older than 5 years. Surprisingly, studies have consistently found that at least half the children in the general population exceed these limits (19, 25, 26) increasing with age (25, 27).
Although currently there are no specific recommendations on acceptable screen time in children and adolescents with ASD, studies consistently show that they spend more screen time compared to their typically developing peers (28–32) and may therefore be at greater risk of becoming dependent (33–35), or attracted to video gaming that may correspond to their solitary and repetitive social patterns of interaction (36). Number of studies have also pointed to unfavorable effects of excessive screen time in children and adolescents with ASD that included enhanced sedentary behavior (29, 31, 32), ADHD symptoms (33), reduced mother-child reciprocal interaction (30) and sleep problems (37–39). The National Survey of Children's Health (26) involving a representative sample of U.S. children, age 6–17 years, showed that although more than half of children with ASD were high users (more than 2 h/day), nevertheless compared to non-ASD children, they had similar amounts of screen time. Montes (26) has further cautioned against assumption of increased risk of excessive screen time among children and adolescents with ASD especially given the utility of visual electronic devices in ASD as communication and teaching aids.
A recent study examining the impact of the COVID-19 pandemic on health behaviors among adolescents with ASD reported significant increase in screen times in terms of both weekday (3.7 h/week) and weekend (5.9 h/week) use (39). Others studies also emphasized the negative effect of the COVID-19 lockdown on youth physical activity and recreational opportunities during the lockdown (40, 41). The stay-home orders during the COVID-19 pandemic have led to doubling or tripling of screen time among children and adolescents with ASD (16, 19, 39–46).
The purpose of the current study was to examine and describe screen time in a sample of children and adolescents with validated ASD diagnoses enrolled in the ELENA cohort study in France during a discrete lockdown period, and to identify clinical and socio-demographic risk factors for excessive screen time.
We first hypothesized that screen time of children with ASD will increase during the lockdown period, as observed by previous studies. Moreover, based on prior studies, we expect to identify several risk factors for excessive screen time in these children, both clinical (severe autistic symptoms, low intellectual and adaptive functioning and behavioral issues) and socio-demographic (low parental educational levels and socioeconomic status).
The present study is a cross-sectional survey of parent-informants of children and adolescents with ASD enrolled in the ELENA regional cohort in France carried out between November 5 and December 18, 2020 corresponding to the second COVID-19 lockdown in France. The participants were recruited from the ELENA cohort, an ongoing, prospective, and multicenter study of developmental trajectories in ASD. The subjects followed in the study were 2–16 years at inclusion (V0), all with confirmed ASD according to DSM5 criteria and multidimensional assessments including ADOS, ADI, and psychological assessments. Inclusions in ELENA were carried out over a period from 2013 to 2019. Thereafter, all children are followed for 72 months with standardized clinical data collection times at 36 (V1) and 72 months (V2) after inclusion. The clinical data collected at these times are similar. Complete details about the ELENA protocol have been published elsewhere (47).
For the present study, the participants consisted of children with a confirmed diagnosis of ASD and fulfilled the following inclusion criteria: (1) active follow-up in the ELENA cohort; (2) aged 3–17 years; (3) completed COVID-19 questionnaire; and (4) living full-time or shared custodial arrangement with the responding parent.
The 249 children and adolescents were mainly boys (80.3%) and their mean age was 9.1 years (SD = 3.8). Fifty height percent of children had a middle or high parental socioeconomic status (SES). Over half of the mothers (62.2%) and the fathers (53%) had a college or university education. Children involved in this study were younger and had a higher estimate intellectual level and VABS-II scores for communication and daily living skills then the other children included in the ELENA cohort (Supplementary Table 1).
For the present study, parents were invited by a letter to complete an online questionnaire related to the specified lockdown period via the ELENA cohort database electronic system. A reminder was sent to parents 2 weeks later by e-mail or telephone. Only one questionnaire was completed per child by corresponding parent. As the COVID study was carried out in addition to the ELENA follow-up, we did not automatically collect the motives for declining to participate in this survey, but the few families who did cite a lack of time. Signed informed consent has been obtained from all participating families included in the ELENA cohort. This study was approved by the Internal Review Board of the University Hospital of Montpellier and was conducted according to the recommendations of the Declaration of Helsinki.
The COVID-19 questionnaire included: (i) child characteristics, education and leisure activities, specialized care (i.e., speech therapy, occupational therapy, psychosocial intervention; social skills training), sleep (within the last 15 days), social home environment and relationships; and (ii) child screen time from the inclusion of the pandemic in March 2020: average screen time (hours/day) assessed on a 5-point Likert response scale (none; <1 h/day; 1–2 h/day; 2–4 h/day; >4 h/ day), change in screen time since the COVID-19 lockdown (November 5–December 18, 2020), assessed as increased, decreased, same as before, or not applicable (i.e., “my child does not spend any time on screens”).
The clinical characteristics of subjects have been previously assessed by licensed study psychologists using standardized tools within the ELENA Cohort. The child and adolescent adaptive skills were assessed with the Vineland Adaptive Behavior Scales, Second Edition (VABS-II) (48). Autism symptom severity was measured using the calibrated severity score (CSS) of the Autism Diagnostic Observation Schedule-2 (ADOS-2) (49, 50). A best estimate intellectual functioning was calculated using standardized and validated instruments [Brunet-Lézine R (51); BECS (52); PEP-3 (53); WPPSI-IV (54); WISC-V (55); WAIS-IV (56); K-ABC (57)] based on child age and level, according to the approach of Howlin et al. (58). Psychiatric comorbidities were assessed using the Child Behavior Checklist [CBCL; (59)], a norm-referenced measure assessing emotional and behavioral disorders in children. A CBCL score <65 corresponds to a normal range and a score greater or equal to 65 corresponds to a borderline or clinical range. Children and adolescents responses to sensory stimuli were assessed by the Sensory Profile (SP), a parent-reported 125-items questionnaire (60) for which a total score (SP total score) was calculated from 36 items (61), lower scores indicating greater SP difficulties. The tools and measures have been described in detail in the ELENA protocol (47). The clinical characteristics used in this paper were collected at the last ELENA follow-up visit closest to the beginning of the containment with a mean delay of 12 months between these times (standard deviations ± 10.7).
The socio-demographic and familial characteristics included: sibship size, household composition, parental ages, educational levels and socioeconomic status (SES) studied as a composite variable based on the mother and/or the father's professional background. When the parents were living together, the highest SES in the household was taken into consideration; when separated, the SES of parent with whom the child lived most of the time was taken into consideration. Only current occupational professional activities were considered; if a parent did not work at the time of the study, her/his SES was not taken into account. Parental SES was scored as high (business owners, professionals, executives), middle (farmers, supervisors, skilled craftsmen), or low (farm workers, laborers, service employees, and unemployed). Middle and high SES classes were grouped to increase the power of data. All data about socio-demographic and familial characteristics used in this paper were extracted from the last ELENA follow-up visit.
The outcome variable was screen time of children and adolescents during the specified COVID-19 lockdown period, defined as greater than recommended (21, 23) (<1 h/day for 2–5-year-old group, and <2 h/day for >5-year-old group). The following potential explanatory variables were considered for the analysis: (i) data from ELENA follow-up: for the child (gender and clinical characteristics: CSS, VABS-II, CBCL and SP scores, best estimate intellectual functioning), and the parents (number of siblings, parental SES and educational level); and (ii) data collected during lockdown: for the child (age, education, leisure activities, weekly social relationships with peers and family and continuation of specialized care) and the parents (age, household composition and perception of their child's sleep).
Descriptive analysis was performed according three age subgroups identified according to school levels (preschool, elementary and beyond than middle school, respectively): <6 years old, 6–11 years old and ≥12 years old. Means with ± standard deviations (SDs) were reported for continuous variables. Categorical variables were described into frequency and percentage. Pearson chi-square or Fisher exact tests and ANOVA tests were used to compare sub-groups characteristics. Pairwise comparisons were performed using the Bonferroni post-hoc test. Chi square test was used to compare the excessive screen time between groups.
The risk factors analysis was performed for the subgroups: children (<12 years) and adolescents (≥12 years). The groups <6 years, and 6–11 years, were pooled into a group < 12 years, because of (1) the homogeneous prevalence of screen time for the age subgroups <6 years and 6–11 years and to address (2) the limited sample size of the age subgroup <6 years.
The association between potential explanatory factors and screen time during the lockdown was studied using Pearson chi-square or Fisher exact tests for the categorical variables and T-Test or Kruskal-Wallis tests for continuous variables. The following effect sizes, Cramer's V, Cohen's d and eta2, were calculated as appropriate (62).
For the multivariable logistic regression models of excessive screen time risk factors, variables with a p <0.20 according to the univariate analysis were included in the model and the model that minimized the Akaike Information Criterion (AIC) was selected using a backward selection. The multivariable model for the <12 years group was adjusted with the delay between the date of the last CBCL and the filling time of the COVID-19 questionnaire. The adjusted odds ratios (aORs) with 95% confidence intervals (CIs) are presented. The goodness-of-fit of the models was assessed using the Hosmer and Lemeshow test. A sensitivity analysis was performed using chained equation missing data method to impute the missing explanatory variables (100 imputation datasets), assuming that the data were missing at random. All statistical tests were considered significant for p < 0.05. Statistical analyses were performed using SAS Enterprise Guide V7.13 (SAS Institute Inc., Cary, NC, USA).
The sample study included 249 children and adolescents who were mainly boys (80.3%). The caregivers who filled the COVID-19 questionnaire were mothers for 202 participants (81.2%), fathers for 20 of them (8%) and both parents combined for 27 of them (10.8%). The means ADOS-2 CSS was 7.37 (SD = 1.8) and the mean estimate intellectual functioning was 79.1 (SD = 30.2). The mean VABS-II scores were 73.3 (SD = 17.4) for communication, 73.0 (SD = 15.7) for daily living skills and 69.1 (SD = 14.3) for socialization. The three age groups considered for this study: <6 years (n = 40, 16.1%); 6–11 years (n = 143, 57.4%); and ≥12 years (n = 66, 26.5%) were comparable on CSS and VABS-II scores but significantly different on intellectual level (p < 0.001, eta2 = 0.17), that increased with age. Most children were in school (N = 225, 90.4%) and had no leisure activities (n = 169, 67.9%). Specialized care was maintained for most children and adolescents (n = 227, 91.2%) but it was significantly more frequent in 6–11 years than ≥12 years subgroup (94.4 and 83.3%, respectively; p = 0.01). More details are presented in Table 1.
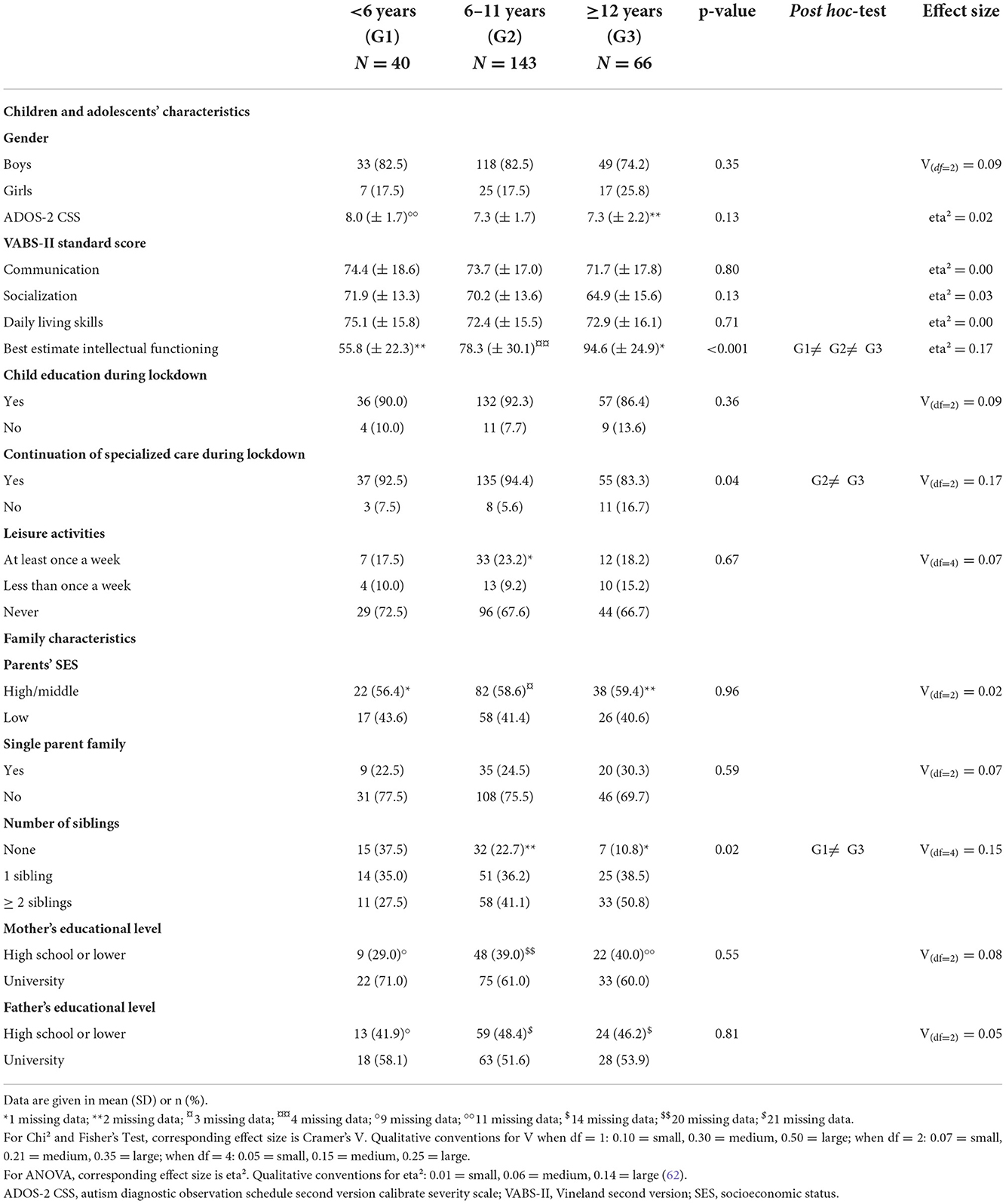
Table 1. Children, family, and socio-demographic characteristics.
Excessive screen time was found in 37.4% (n = 93) of our sample and was significantly related to age [p < 0.001, Cramer's V(df = 2) = 0.33] as follows: 63.6%, ≥12 year (n = 42); 27.3%, 6–11 year (n = 39) groups; and 30%, <6 years group (n = 12). Gender was linked to excessive screen time for the ≥12 years group [p = 0.03, Cramer's V(df = 1)= −0.28], with males more likely to have excessive screen time (83.3%) than females (16.7%). Highest screen times (>4 h/day) were: 16.7%, <6 year; 20.5%, aged 6–11 year; and 50.0%, ≥12 year groups. Almost half of parents (48.8%) reported that their child spent more time using screen since COVID-19 pandemic beginning as 44.0 % reported no change and only 4.0 % reported a screen time decrease.
Children (<12 years) with excessive screen time vs. within recommended level had significantly: lower VABS-II scores for Daily Living Skills [mean = 69.5 (SD = 14.6) vs. 74.28 (SD = 15.8), respectively; p = 0.02, Cohen's d = 0.31], higher CBCL scores for withdrawn [70.7% with borderline or clinical range vs. 53.9%, respectively; p = 0.06, Cramer's V(df = 1) = −0.15] and lower parental SES [58.0 vs. 35.7%, respectively; p = 0.01, Cramer's V(df = 1) = 0.20].
Adolescents (≥12 years) with excessive screen time vs. within recommended level had: older age [mean = 14.7 years (SD = 1.5) vs. 13.4 years (SD = 1.9), respectively; p = 0.002, Cohen's d = −0.76]; male gender (83.3 vs. 58.3%, respectively; p = 0.03, Cramer's V(df = 1) = −0.28]; higher CSS [mean = 7.7 (SD = 2.2) vs. 6.7 (SD = 2.01), respectively; p = 0.04, Cohen's d = −0.45] and CBCL score for withdrawn (65.7% with borderline or clinical range vs. 35.3% respectively; p = 0.04, Cramer's V(df = 1)= −0.29]. In addition, they received less specialized care services during lockdown [76.2 vs. 95.8%, respectively, p = 0.05, Cramer's V(df = 1)= −0.25] and had lower maternal education level [p = 0.09, Cramer's V(df = 1)= −0.23].
Children (<12 years): after adjustment, higher withdrawn CBCL score (borderline/clinical range) and low parental SES were both noted to increase risk of excessive screen time: (ORa = 2.39 (95%CI 1.06–5.36, p = 0.04); and ORa = 2.67 (95%CI 1.25–5.71, p = 0.01]), respectively. Using multiple imputation of missing data, the sensitivity analysis confirms the result of the complete case multivariable analysis in children (Table 2).
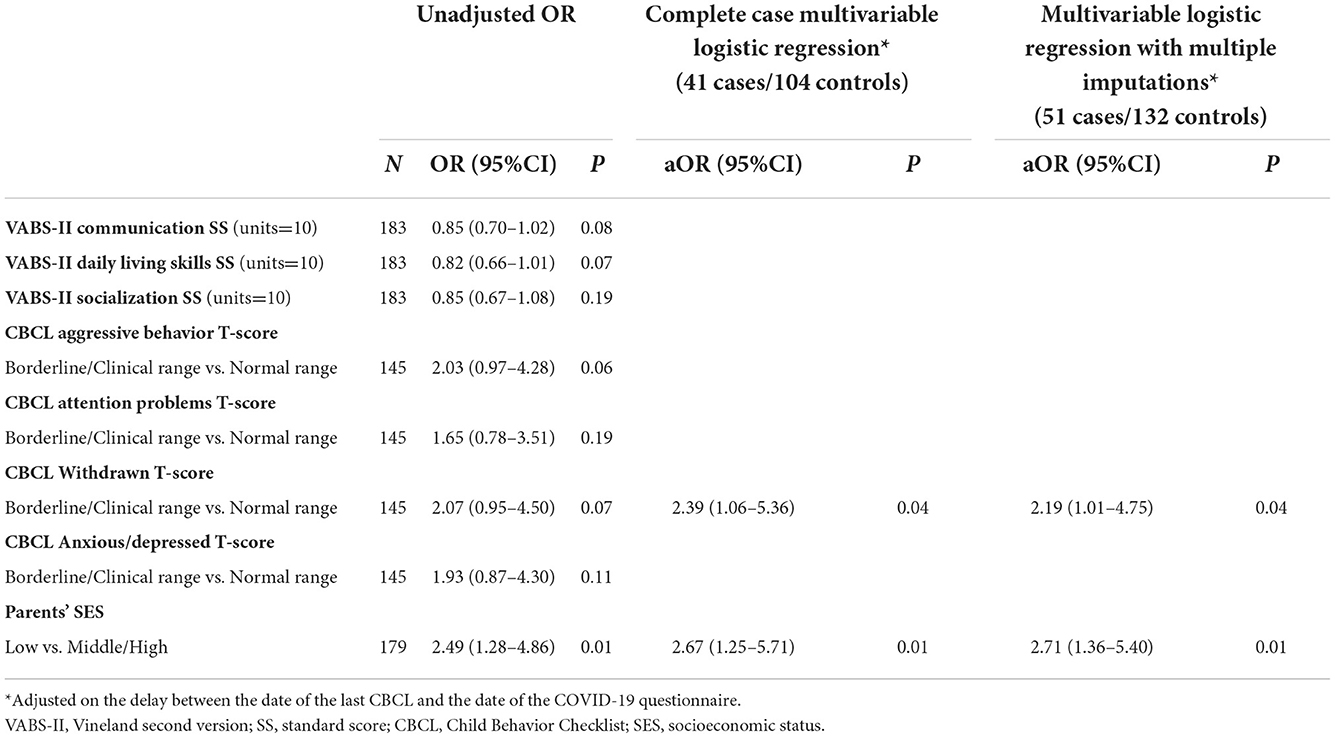
Table 2. Risk factors for excessive screen time in children bellow 12 years old.
Adolescents (≥12 years): after backward selection, only older age was a risk factor of excessive screen time [OR = 2.24 (1.30–3.86), p = 0.04]. The sensitivity analysis conducted on imputed data showed that child age and male gender were significant risk factors for excessive screen time in adolescents: ORa = 1.64 (95%CI: 1.53–2.34; p = 0.01) and ORa = 4.25 (95%CI: 1.67–15.47; p = 0.03), respectively (Table 3).
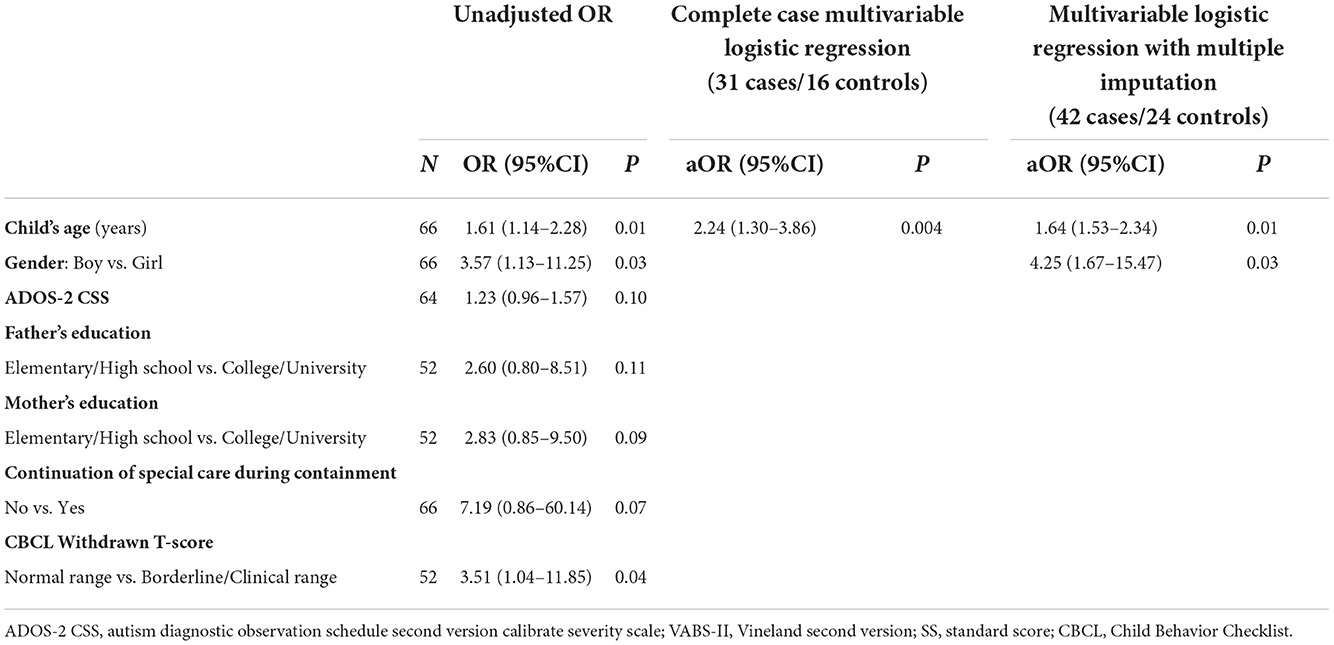
Table 3. Risk factors for excessive screen time in adolescents aged 12 years old and over.
The current study provided a unique opportunity to examine screen time during a discrete COVID-19 lockdown period among a sample of 249 children and adolescents with well-characterized diagnosis of ASD enrolled in a regional ASD cohort in France. We found that 37.4% of subjects had above recommended levels of screen time during lockdown. This figure is comparable to that obtained in the U.S. general population in the National Health and Nutrition Examination Survey that reported sedentary behavior profiles comprised of television viewing or engaging with electronic media that exceeded 2-h/day or more of screen time for 47% of the population of 2–15 year old children and adolescents (27). It is notable that the latter study classified sedentary behaviors depending on the screen time activities involved as “productive” (e.g., computer use for homework or reading, or other educational activity) or “leisure” (e.g., viewing television or playing computer or video games).
Regarding the impact of lockdown on children's screen time, half of parents reported an increase since the beginning of the pandemic, which is congruent with previous studies (39). This indicates that screen time measured during the pandemic does not necessarily represent the usual screen time of children. In particular, children and adolescents had to adapt to a new virtual system for education and work purposes, so that “excessive” screen time can be biased by this constrains during the lock-down.
The results of the current study were consistent with that of Must et al. (32) that compared children with ASD and typically developing children under 12 years of age. Must et al. (32) reported significantly elevated screen times, 2.5 vs. 1.6 h/day, among ASD and non-ASD children, respectively, albeit during a non-lockdown period. A study by Krupa et al. (30) involving 2–4 year-old children with ASD vs. typically developing non-ASD children also reported significantly elevated weekly screen times, 8.4 vs. 6.9 h, respectively, that did not exceed recommended levels. Nonetheless, although not at excessive screen time levels, for these young children, the Krupa et al. (30) study emphasized the importance of joint family-child screen time that had an impact on mother-child reciprocal interaction.
The present study allowed to identify factors associated to excessive screen time. First, above recommended screen time was higher for adolescents (63%), almost double that of under 12-year-olds. Excessive screen time experience among adolescents is also supported by prior studies and likely relate to ease of screen access, attraction to social networks, and difficulty in implementing stricter controls (19, 63). Second, our analysis found that children with excessive screen time had lower daily living skills (as assessed with VABS-II). This is consistent with the previously reported association of excessive screen time with negative health conditions in children and adolescents with ASD (29, 33, 37). Third, children and adolescents with ASD with excessive screen time were significantly more withdrawn (as assessed with CBCL) suggesting that children with these clinical characteristics may are more likely to have greater screen time. However, it is difficult to understand the true nature of this interaction, which can reflect either greater interest in solitary screen-based activities, or adverse effect of excessive screen time on prosocial behavior. Alternatively, the degree of withdrawal observed in children and adolescents with excessive screen time could be related to greater autism severity, as noted by Dong et al. (64), who found that children with significant sensory characteristics, were more likely to be fascinated by the visual stimuli of screens. It is also possible that they were given these devices because it was a convenient way to keep them occupied during the lockdown. Fourth, the univariate analysis found that adolescents with excessive screen time were not only older but were more likely to be males, a finding again consistent with previous literature (19, 63). Fifth, the adolescents with excessive screen time received less special care services and less educational resources at home. In such uniformed circumstances, it has also been noted that parents themselves may be involved in excessive screen time (65). As already been reported in previous studies (19) low parental SES has also been noted to be a risk factor for excessive screen time among children with less opportunities for non-screen based leisure and vocational activities.
Finally, the multivariable and sensitivity analyses, underscored that be more withdrawn and had lower parental SES were the risk factors for excessive screen time among children. Among adolescents, older age and male gender were the risk factors for excessive screen time, two factors commonly supported by prior population based studies (17–20, 63). Number of limitations of the study should be noted. The subsample of children and adolescents examined for the present study were younger and had higher intellectual and adaptive functioning scores than in the overall ELENA cohort, which limits the generalization of our results. ELENA is a regional cohort and not a nationally representative sample, which may bias our results on the link between socio-economic status and screen time and therefore we cannot generalize. Data on socio-familial characteristics were only available for a subset of children, who did not differ from the whole cohort on these variables. We do not have a measurement of the screen exposure before confinement or a comparison to the population without ASD or the general population. Part of the clinical data used in this article was collected at the last visit in ELENA about 12 months before our COVID-19 survey. However, the clinical presentation in other cohorts with ASD (66) was found to be stable in the short term. Nevertheless, an important strength of the current study included the use of a large sample of children and adolescents with confirmed ASD diagnosis with consideration of a wide range of clinical and socio-familial variables collected using validated instruments and potential risk factors. Although the sample size was limited, the significance of the findings for a relatively small subgroup was important and consistent with prior research. Given the positive relationship found between age and excessive screen time, future research is needed to examine long-term effects of excessive screen time from adolescence onwards.
The experience of above recommended level of screen time among children and adolescents with ASD is equally important with consequent negative effects of excessive screen time on health. It is therefore paramount to develop recommendations on screen time and to provide guidance to parents of children and adolescents with ASD. Further studies are needed to examine the relationship between sedentary behaviors, screen time and healthy and behavioral outcomes in children and adolescents with ASD. The clinical and social risk factors identified in the current study also make it possible for professionals to consider measures to implement the more optimal use of screen time activities for educational, therapeutic and social goals. It is particularly important to encourage the access of children to non-screen time based leisure and cultural activities that complement educational interventions in particular during period of lockdowns.
The datasets presented in this article are not readily available because Research data are not shared due to the need for confidentiality. The corresponding author, AB, confirms that she had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Requests to access the datasets should be directed to AB, cmVjaC1jbGluaXF1ZS1hdXRpc21lQGNodS1tb250cGVsbGllci5mcg==.
This study involving human participants was reviewed and approved by Internal Review Board of the University Hospital of Montpellier. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Signed informed consent is obtained from all participating families included in the ELENA cohort.
Amaria Baghdadli, Catherine Chabaux, Clarisse Chatel, David Cohen, Emmanuel Damville, Marie-Maude Geoffray, Ludovic Gicquel, Renaud Jardri, Thierry Maffre, Alexandre Novo, Roxane Odoyer, Marie-Joëlle Oreve, Didier Périsse, François Poinso, Julien Pottelette, Laurence Robel, Catherine Rolland, Marie Schoenberger, Sandrine Sonié, Mario Speranza, and Stéphanie Vespérini.
MB and AB conceived the study, contributed to the collection, analysis, interpretation of the data, and drafted the manuscript. AB is the PI of the ELENA cohort. JL contributed to the collection of the data. MP and M-CP analyzed and interpreted the data and critically revised it for the principal intellectual content. All authors reviewed and approved the final version.
This work was supported by the French Health Ministry (DGOS) PHRCN 2013 [Grant No 1: 13-0232] and the Caisse Nationale de Solidarité pour l'Autonomie (CNSA) [Grant No 2: 030319]. The CHU of Montpellier (AOI) provided additional support. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
We warmly thank the contributing families, the ELENA staff, and the ELENA consortium. We also express gratitude to the funders.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.1026191/full#supplementary-material
1. Carson V, Hunter S, Kuzik N, Gray CE, Poitras VJ, Chaput J-P, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Physiol Nutr Metab. (2016) 41:S240–65. doi: 10.1139/apnm-2015-0630
2. Sultana RN, Sabag A, Keating SE, Johnson NA. The effect of low-volume high-intensity interval training on body composition and cardiorespiratory fitness: a systematic review and meta-analysis. Sports Med. (2019) 49:1687–721. doi: 10.1007/s40279-019-01167-w
3. Suchert V, Hanewinkel R, Isensee B. Sedentary behavior and indicators of mental health in school-aged children and adolescents: a systematic review. Prev Med. (2015) 76:48–57. doi: 10.1016/j.ypmed.2015.03.026
4. Belmon LS, van Stralen MM, Busch V, Harmsen IA, Chinapaw MJ. What are the determinants of children's sleep behavior? A systematic review of longitudinal studies. Sleep Med Rev. (2019) 43:60–70. doi: 10.1016/j.smrv.2018.09.007
5. Hoare E, Milton K, Foster C, Allender S. The associations between sedentary behaviour and mental health among adolescents: a systematic review. Int J Behav Nutr Phys Act. (2016) 13:1–22. doi: 10.1186/s12966-016-0432-4
6. Stanczykiewicz B, Banik A, Knoll N, Keller J, Hohl DH, Rosińczuk J, et al. Sedentary behaviors and anxiety among children, adolescents and adults: a systematic review and meta-analysis. BMC Public Health. (2019) 19:1–22. doi: 10.1186/s12889-019-6715-3
7. Harlé B. Intensive early screen exposure as a causal factor for symptoms of autistic spectrum disorder: the case for ≪Virtual autism≫. Trends Neurosci Educ. (2019) 17:100119. doi: 10.1016/j.tine.2019.100119
8. Jahan A, Parvin SR, Bugum D. Familial, social and environmental risk factors in autism: a case-control study. Bangladesh Med Res Counc Bull. (2014) 40:113–7. doi: 10.3329/bmrcb.v40i3.25233
9. Kushima M, Kojima R, Shinohara R, Horiuchi S, Otawa S, Ooka T, et al. Association between screen time exposure in children at 1 year of age and autism spectrum disorder at 3 years of age: the Japan environment and children's study. JAMA Pediatr. (2022) 176:384-−91. doi: 10.1001/jamapediatrics.2021.5778
10. Marcelli D, Bossière M-C, Ducanda A-L. L'exposition précoce et excessive aux écrans (EPEE): un nouveau syndrome. Devenir. (2020) 32:119–37. doi: 10.3917/dev.202.0119
11. Ra CK, Cho J, Stone MD, De La Cerda J, Goldenson NI, Moroney E, et al. Association of digital media use with subsequent symptoms of attention-deficit/hyperactivity disorder among adolescents. JAMA. (2018) 320:255–63. doi: 10.1001/jama.2018.8931
12. Swing EL, Gentile DA, Anderson CA, Walsh DA. Television and video game exposure and the development of attention problems. Pediatrics. (2010) 126:214–21. doi: 10.1542/peds.2009-1508
13. He Z, Shao S, Zhou J, Ke J, Kong R, Guo S, et al. Does long time spending on the electronic devices affect the reading abilities? A cross-sectional study among Chinese school-aged children. Res Dev Disabil. (2014) 35:3645–54. doi: 10.1016/j.ridd.2014.08.037
14. Lin L-Y, Cherng R-J, Chen Y-J, Chen Y-J, Yang H-M. Effects of television exposure on developmental skills among young children. Infant Behav Dev. (2015) 38:20–6. doi: 10.1016/j.infbeh.2014.12.005
15. Martinot P, Bernard JY, Peyre H, De Agostini M, Forhan A, Charles M-A, et al. Exposure to screens and children's language development in the EDEN mother–child cohort. Sci Rep. (2021) 11:11863. doi: 10.1038/s41598-021-90867-3
16. Aguilar-Farias N, Toledo-Vargas M, Miranda-Marquez S, Cortinez-O'Ryan A, Cristi-Montero C, Rodriguez-Rodriguez F, et al. Sociodemographic predictors of changes in physical activity, screen time, and sleep among toddlers and preschoolers in chile during the covid-19 pandemic. Int J Environ Res Public Health. (2021) 18:176. doi: 10.3390/ijerph18010176
17. Bleakley A, Jordan AB, Hennessy M. The relationship between parents' and children's television viewing. Pediatrics. (2013) 132:e364–71. doi: 10.1542/peds.2012-3415
18. Carson V, Janssen I. Associations between factors within the home setting and screen time among children aged 0–5 years: a cross-sectional study. BMC Public Health. (2012) 12:1–8. doi: 10.1186/1471-2458-12-539
19. Eyimaya AO, Irmak AY. Relationship between parenting practices and children's screen time during the COVID-19 Pandemic in Turkey. J Pediatr Nurs. (2021) 56:24–9. doi: 10.1016/j.pedn.2020.10.002
20. Lloyd AB, Lubans DR, Plotnikoff RC, Collins CE, Morgan PJ. Maternal and paternal parenting practices and their influence on children's adiposity, screen-time, diet and physical activity. Appetite. (2014) 79:149–57. doi: 10.1016/j.appet.2014.04.010
21. Council on communications and media, Hill D, Ameenuddin N, Chassiakos RYL, Cross C, Hutchinson J, et al. Media and young minds. Pediatrics Am Acad Pediatrics. (2016) 138:e20162591. doi: 10.1542/peds.2016-2591
22. Picherot G, Cheymol J, Assathiany R, Barthet-Derrien M-S, Bidet-Emeriau M, Blocquaux S, et al. Children and screens: groupe de Pédiatrie Générale (Société française de pédiatrie) guidelines for pediatricians and families. Arch Pédiatrie. (2018) 25:170–4. doi: 10.1016/j.arcped.2017.12.014
23. World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children Under 5 Years of Age. World Health Organization (2019). Available online at: https://apps.who.int/iris/handle/10665/311664 (accessed November 14, 2022).
24. World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour: Web Annex: Evidence Profiles (2020). Available online at: https://apps.who.int/iris/handle/10665/336656 (accessed November 14, 2022).
25. Fakhouri TH, Hughes JP, Brody DJ, Kit BK, Ogden CL. Physical activity and screen-time viewing among elementary school–aged children in the United States from 2009 to 2010. JAMA Pediatr. (2013) 167:223–9. doi: 10.1001/2013.jamapediatrics.122
26. Montes G. Children with autism spectrum disorder and screen time: results from a large, nationally representative US study. Acad Pediatr. (2016) 16:122–8. doi: 10.1016/j.acap.2015.08.007
27. Sisson SB, Church TS, Martin CK, Tudor-Locke C, Smith SR, Bouchard C, et al. Profiles of sedentary behavior in children and adolescents: the US National Health and Nutrition Examination Survey, 2001–2006. Int J Pediatr Obes. (2009) 4:353–9. doi: 10.3109/17477160902934777
28. Chonchaiya W, Nuntnarumit P, Pruksananonda C. Comparison of television viewing between children with autism spectrum disorder and controls. Acta Paediatr. (2011) 100:1033–7. doi: 10.1111/j.1651-2227.2011.02166.x
29. Healy S, Haegele JA, Grenier M, Garcia JM. Physical activity, screen-time behavior, and obesity among 13-year olds in Ireland with and without autism spectrum disorder. J Autism Dev Disord. (2017) 47:49–57. doi: 10.1007/s10803-016-2920-4
30. Krupa M, Boominathan P, Ramanan PV, Sebastian S. Relationship between screen time and mother-child reciprocal interaction in typically developing children and children with autism spectrum disorders. Indian J Pediatr. (2019) 86:394. doi: 10.1007/s12098-018-02844-w
31. Mazurek MO, Wenstrup C. Television, video game and social media use among children with ASD and typically developing siblings. J Autism Dev Disord. (2013) 43:1258–71. doi: 10.1007/s10803-012-1659-9
32. Must A, Phillips SM, Curtin C, Anderson SE, Maslin M, Lividini K, et al. Comparison of sedentary behaviors between children with autism spectrum disorders and typically developing children. Autism. (2014) 18:376–84. doi: 10.1177/1362361313479039
33. Kawabe K, Horiuchi F, Miyama T, Jogamoto T, Aibara K, Ishii E, et al. Internet addiction and attention-deficit/hyperactivity disorder symptoms in adolescents with autism spectrum disorder. Res Dev Disabil. (2019) 89:22–8. doi: 10.1016/j.ridd.2019.03.002
34. Liu S, Yu C, Conner BT, Wang S, Lai W, Zhang W. Autistic traits and internet gaming addiction in Chinese children: the mediating effect of emotion regulation and school connectedness. Res Dev Disabil. (2017) 68:122–30. doi: 10.1016/j.ridd.2017.07.011
35. So R, Makino K, Fujiwara M, Hirota T, Ohcho K, Ikeda S, et al. The prevalence of internet addiction among a Japanese adolescent psychiatric clinic sample with autism spectrum disorder and/or attention-deficit hyperactivity disorder: a cross-sectional study. J Autism Dev Disord. (2017) 47:2217–24. doi: 10.1007/s10803-017-3148-7
36. Paulus FW, Sander CS, Nitze M, Kramatschek-Pfahler A-R, Voran A, von Gontard A. Gaming disorder and computer-mediated communication in children and adolescents with autism spectrum disorder. Z Für Kinder- Jugendpsychiatrie Psychother. (2019). doi: 10.1024/1422-4917/a000674
37. Aishworiya R, Kiing JS, Chan YH, Tung SS, Law E. Screen time exposure and sleep among children with developmental disabilities. J Paediatr Child Health. (2018) 54:889–94. doi: 10.1111/jpc.13918
38. Engelhardt CR, Mazurek MO, Sohl K. Media use and sleep among boys with autism spectrum disorder, ADHD, or typical development. Pediatrics. (2013) 132:1081–9. doi: 10.1542/peds.2013-2066
39. Garcia JM, Lawrence S, Brazendale K, Leahy N, Fukuda D. Brief report: The impact of the COVID-19 pandemic on health behaviors in adolescents with Autism Spectrum Disorder. Disabil Health J. (2021) 14:101021. doi: 10.1016/j.dhjo.2020.101021
40. López-Bueno R, López-Sánchez GF, Casajús JA, Calatayud J, Gil-Salmerón A, Grabovac I, et al. Health-related behaviors among school-aged children and adolescents during the Spanish Covid-19 confinement. Front Pediatr. (2020) 8:573. doi: 10.3389/fped.2020.00573
41. Schmidt SC, Anedda B, Burchartz A, Eichsteller A, Kolb S, Nigg C, et al. Physical activity and screen time of children and adolescents before and during the COVID-19 lockdown in Germany: a natural experiment. Sci Rep. (2020) 10:21780. doi: 10.1038/s41598-020-78438-4
42. Bates LC, Zieff G, Stanford K, Moore JB, Kerr ZY, Hanson ED, et al. COVID-19 impact on behaviors across the 24-hour day in children and adolescents: physical activity, sedentary behavior, and sleep. Children. (2020) 7:138. doi: 10.3390/children7090138
43. Moore SA, Faulkner G, Rhodes RE, Brussoni M, Chulak-Bozzer T, Ferguson LJ, et al. Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: a national survey. Int J Behav Nutr Phys Act. (2020) 17:85. doi: 10.1186/s12966-020-00987-8
44. Pietrobelli A, Pecoraro L, Ferruzzi A, Heo M, Faith M, Zoller T, et al. Effects of COVID-19 lockdown on lifestyle behaviors in children with obesity living in Verona, Italy: a longitudinal study. Obesity. (2020) 28:1382–5. doi: 10.1002/oby.22861
45. Together P. Survey Shows Parents Alarmed as Kids' Screen Time Skyrockets During COVID-19 Crisis (2020). Available online at: https://parents-together.org/survey-shows-parents-alarmed-as-kids-screen-time-skyrockets-during-covid-19-crisis/ (accessed November 14, 2022).
46. Xiang M, Zhang Z, Kuwahara K. Impact of COVID-19 pandemic on children and adolescents' lifestyle behavior larger than expected. Prog Cardiovasc Dis. (2020) 63:531. doi: 10.1016/j.pcad.2020.04.013
47. Baghdadli A, Miot S, Rattaz C, Akbaraly T, Geoffray M-M, Michelon C, et al. Investigating the natural history and prognostic factors of ASD in children: the multicEntric Longitudinal study of childrEN with ASD - the ELENA study protocol. BMJ Open. (2019) 9:e026286. doi: 10.1136/bmjopen-2018-026286
48. Sparrow SS, Cicchetti DV, Balla DA, Doll EA. Vineland Adaptive Behavior Scales: Survey Forms Manual. American Guidance Service (2005). doi: 10.1037/t15164-000
49. Gotham K, Risi S, Dawson G, Tager-Flusberg H, Joseph R, Carter A, et al. A replication of the Autism Diagnostic Observation Schedule (ADOS) revised algorithms. J Am Acad Child Adolesc Psychiatry. (2008) 47:642–51. doi: 10.1097/CHI.0b013e31816bffb7
50. Lord C, Rutter M, Di Lavore P, Risi S, Gotham K, Bishop S. Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) Manual (Part I): Modules 1–4. Torrance, CA: Western Psychological Services (2012).
51. Brunet O, Lézine I, Josse D. Brunet-Lézine révisé: échelle de développement psychomoteur de la première enfance : manuel BLR-C. Issy-Les-Moulineaux: Etablissements d'Applications Psychotechniques (1997).
52. Adrien J. Batterie d'évaluation cognitive et socio-émotionnelle. BECS Prat Psychol Rech Clin Auprès D'enfants Atteints TED (2008).
53. Schopler E, Lansing M, Reichler R, Marcus L. Psychoeducational Profile Third Edn (PEP-3). (2004). (Pro-Ed ed. USA). doi: 10.1037/t52601-000
56. Wechsler D. Wechsler adult intelligence scale–Fourth Edition (WAIS–IV). San Antonio TX NCS Pearson. (2008) 22:816–27. doi: 10.1037/t15169-000
57. Kaufman AS. K-ABC: Kaufman assessment battery for children: Interpretive manual. Am Guidance Service. (1983). doi: 10.1037/t27677-000
58. Howlin P, Savage S, Moss P, Tempier A, Rutter M. Cognitive and language skills in adults with autism: a 40-year follow-up. J Child Psychol Psychiatry. (2014) 55:49–58. doi: 10.1111/jcpp.12115
59. Achenbach TM, Ruffle TM. The child behavior checklist and related forms for assessing behavioral/emotional problems and competencies. Pediatr Rev. (2000) 21:265–71. doi: 10.1542/pir.21.8.265
60. Dunn W. Sensory Profile: User's Manual San Antonio. TX Psychol Corp. (1999). doi: 10.1037/t15155-000
61. McIntosh D, Miller L, Shyu V, Dunn W. Development and validation of the short sensory profile. Sens Profile Man. (1999) 59–73.
63. Hu BY, Johnson GK, Wu H. Screen time relationship of Chinese parents and their children. Child Youth Serv Rev. (2018) 94:659–69. doi: 10.1016/j.childyouth.2018.09.008
64. Dong H-Y, Wang B, Li H-H, Yue X-J, Jia F-Y. Correlation Between Screen Time and Autistic Symptoms as Well as Development Quotients in Children With Autism Spectrum Disorder. Front Psychiatry. 2021;12:140. doi: 10.3389/fpsyt.2021.619994
65. Dong H-Y, Feng J-Y, Wang B, Shan L, Jia F-Y. Screen Time and Autism: Current situation and risk factors for screen time among preschool children with ASD. Front Psychiatry. 2021;1332. doi: 10.3389/fpsyt.2021.675902
Keywords: autism spectrum disorder, COVID-19, lockdown, screen time, children, adolescents
Citation: Berard M, Peries M, Loubersac J, Picot M-C, Bernard JY, Munir K and Baghdadli A (2022) Screen time and associated risks in children and adolescents with autism spectrum disorders during a discrete COVID-19 lockdown period. Front. Psychiatry 13:1026191. doi: 10.3389/fpsyt.2022.1026191
Received: 23 August 2022; Accepted: 04 November 2022;
Published: 01 December 2022.
Edited by:
Lucia Margari, University of Bari Aldo Moro, ItalyReviewed by:
Betty Vohr, Women and Infants Hospital of Rhode Island, United StatesCopyright © 2022 Berard, Peries, Loubersac, Picot, Bernard, Munir and Baghdadli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amaria Baghdadli, cmVjaC1jbGluaXF1ZS1hdXRpc21lQGNodS1tb250cGVsbGllci5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.