 Elena Marcos-Vadillo1Lorena Carrascal-Laso2Ignacio Ramos-Gallego3Andrea Gaedigk4,5Belén García-Berrocal1Eduardo Mayor-Toranzo2Alfonso Sevillano-Jiménez2Almudena Sánchez6María Isidoro-García1,7*Manuel Franco-Martín2
Elena Marcos-Vadillo1Lorena Carrascal-Laso2Ignacio Ramos-Gallego3Andrea Gaedigk4,5Belén García-Berrocal1Eduardo Mayor-Toranzo2Alfonso Sevillano-Jiménez2Almudena Sánchez6María Isidoro-García1,7*Manuel Franco-Martín2- 1Servicio de Bioquímica, Hospital Universitario de Salamanca, Instituto de Investigacion Biomedica de Salamanca, Salamanca, Spain
- 2Servicio de Psiquiatría, Hospital Provincial de Zamora, Instituto de Investigacion Biomedica de Salamanca, Zamora, Spain
- 3Departamento de Fisiología y Farmacología, Universidad de Salamanca, Salamanca, Spain
- 4Division of Clinical Pharmacology, Toxicology and Therapeutic Innovation, Children's Mercy Kansas City, Kansas City, MO, United States
- 5Department of Pediatrics, School of Medicine, University of Missouri-Kansas City, Kansas, MO, United States
- 6Servicio de Farmacia, Hospital Universitario de Salamanca, Instituto de Investigacion Biomedica de Salamanca, Salamanca, Spain
- 7Departamento de Medicina, Universidad de Salamanca, Salamanca, Spain
Precision medicine applied to psychiatry provides new insight into the promising field of precision psychiatry. Psychotic disorders are heterogeneous, complex, chronic, and severe mental disorders. Not only does the prognosis and the course of the disease vary among patients suffering from psychotic disorders, but the treatment response varies as well. Although antipsychotic drugs are the cornerstone of the treatment of schizophrenia, many patients only partially respond to these drugs. Furthermore, patients often experience adverse events which can lead to poor treatment adherence. Interindividual variability in drug response could be related to age, gender, ethnicity, lifestyle factors, pharmacological interactions, obesity, and genetics, all of which influence the process of drug metabolism. Commonly prescribed antipsychotics are metabolized by cytochrome P450 (CYP450) enzymes, and CYP450 genes are highly polymorphic. Pharmacogenetic testing is increasingly being used to predict a patient's drug response and could help to find the most appropriate therapy for an individual patient. In this report, we describe a psychotic patient who did not receive adequate clinical follow-up and subsequently presented adverse events, which could be explained by his pharmacogenetic profile and the drug interactions resulting from the polypharmacy prescribed.
Introduction
An increasing number of children, adolescents, and adults (1) are being diagnosed with mental illness, including depressive disorder, bipolar disorder, and schizophrenia spectrum disorder (2–7). According to the World Health Organization (8), people with mental disorders experience higher rates of disability and mortality compared to the general population, making these conditions a priority of health systems.
Psychotic disorders are a group of heterogeneous, complex, chronic, and severe mental diseases that manifest through positive (hallucinations, delusions, etc.) and negative (impaired motivation, social withdrawal, etc.) symptoms, affecting approximately 1% of the global population (9, 10). Not only are the prognosis and disease course of psychotic disorders variable among patients, but so is treatment response. Antipsychotic drugs comprise the fundamental treatment of schizophrenia and other psychotic disorders (11, 12), but many patients do not only partially respond to drug therapy (13, 14). Furthermore, patients often experience side effects when taking antipsychotics including sedation, cognitive impairment, weight gain and obesity, metabolic syndrome, cardiovascular and neuromotor side effects, among others, which can lead to poor adherence or discontinuation of treatment (15–19).
Interindividual variability in the hepatic metabolism of these drugs may be impacted by several factors including age, gender, ethnicity, lifestyle factors (e.g., tobacco and alcohol consumption, diet), pharmacological interactions (patients taking multiple drugs), obesity, and variation in the genes contributing to the metabolism of the drugs taken (20–22). Many commonly prescribed antipsychotics are metabolized by cytochrome P450 enzymes, mainly CYP2C19 and CYP2D6 (23–26).
CYP genes are highly polymorphic, and patients with extreme phenotypes, i.e., those with no or low activity or increased activity, have been shown to have an increased risk of adverse events or treatment failure due to drug levels that are either too high or too low (27, 28). Thus, pharmacogenetic testing is increasingly utilized to predict a patient's metabolic capacity and utilize this knowledge to inform drug therapy (29–33). Variable enzyme activity can to a large part be explained by the presence of variations on the nucleotide level [i.e., single-nucleotide polymorphisms (SNPs)] but also be caused by gene copy number variation (CNVs), i.e., gene duplications or deletions, and rearrangements (34, 35). Genotype is typically translated into phenotype [i.e., poor metabolizers (PM), intermediate metabolizers (IM), normal metabolizers (NMs), rapid metabolizers (RMs), and ultrarapid metabolizers (UMs)] and therapeutic recommendations based thereof. For CYP2D6 genotype to phenotype translation, recommendations have been published by the Clinical Pharmacogenetics Implementation Consortium (36). Additional details and translation tables for other CYPs can be found on the PharmGKB website at https://www.pharmgkb.org/page/pgxGeneRef.
CYP2D6 is one of the most important and extensively studied CYP450 enzymes (34, 37). It has been shown to contribute to the metabolism of over 20% of commonly prescribed medications (38) including atypical antipsychotics such as aripiprazole, asenapine, clozapine, olanzapine, quetiapine, and risperidone. To date, the Pharmacogene Variation Consortium (39, 40) has described over 140 variant alleles (star alleles) (41). Approximately 5–10% of the European population are poor metabolizers due to having two nonfunctional alleles (42). Additional information regarding allele and genotype frequencies can be found on the PharmGKB website.
In this report, we describe a psychotic patient who did not receive adequate clinical follow-up and presented with side effects, which could have been prevented considering pharmacogenetic test results, complex history, and polypharmacy.
Case Description
The following report describes the situation of a male European patient, who gave us consent to publish his situation, who was born in 1956, and who had been receiving mental health care since 1993, initially under private care, with a diagnosis of schizotypal personality disorder (DSM-V, F21). Regarding the psychiatric family history, his father suffered from bipolar disorder (DSM-V, F31), and his brothers suffered from major depressive disorder (DSM-V, F33). The review of the family history also revealed a psychotic disorder in a second-degree relative (niece). Somatic personal history included hemorrhoids and an anal fissure. The patient did not smoke, drink alcohol, or have a history of substance abuse. During the routine clinical analysis performed throughout the study, there were no ionic, metabolic, or hematological alterations found. In 1994, during his first admission at the University Hospital of Salamanca, he was diagnosed with schizoaffective disorder bipolar type (DSM-V, F25.0). From 1994 to 2015, follow-up treatment was carried out with no hospital admissions and no documented adverse events (AE). In the months following his mother's death and the admission of this father into a care facility, the patient overdosed on lithium with autolytic intention, which required a 3-day stay in intensive care. After this event, the patient clinically deteriorated, and his treatment was changed in seven phases (see Figure 1A):
1st treatment plan (1994–18/01/2016): The first admission was triggered by hypomanic symptoms (expansive mood, ideo-fleeting speech, decreased sleep needs, and maniform symptomatology), after which he was diagnosed with schizoaffective disorder. The treatment prescribed when he was described was as follows: lithium, amisulpride, escitalopram, trazodone, and clobazam. No documented AE. After a sudden change in his familiar environment, the patient overdosed on lithium, with autolytic intention, which required a 3-day stay in intensive care, and was hospitalized for 43 days (6/12/2015–18/01/2016), presenting with rudeness, inappropriate sexual behavior, childish utterances, emotional coldness, and antagonistic behavior. Previous treatment was continued with minor extrapyramidal effects. For pharmacogenetic interactions (see Figure 1B).
2nd treatment plan (18/01/2016–13/06/2016): Based on the adverse effect referred by the patient and taking into account his poor clinical progress during the last hospitalization, the prescriber adjusted the drug treatment upon the patient's release to only include lithium and amisulpride, neither of which is metabolized by a CYP enzyme. Although this adjustment reduced adverse effects, the patient's clinical condition did not improve, and he was readmitted for 49 days (25/04/2016–13/06/2016) due to disturbed behavior with neither depressive nor psychotic symptomatology whereupon he was treated with amisulpride, lorazepam, lormetazepam, quetiapine, and fluoxetine with deep venous thrombosis and gastrointestinal bleeding (melena) as AE.
A pharmacogenetic test [AmpliChip CYP450 Test (43), the Antigenomics platform, MassARRAY 4.2 (Agena), and probed-based assays using the Light-Cycler platform] was performed while the patient was hospitalized. The following allelic variants were tested: CYP2B6 (*6), CYP2C9 (*2 and *3), CYP2C19 (*2, *3, and *17), CYP2D6 (*2, *3, *4, *5, *6, *7, *8, *9, *10, *12, *14, *17, *29, *41, and presence of gene duplication), CYP3A4 (−392 G>A), CYP3A5 (*3), and MDR1 (3435C>T) (Table 1). Allele nomenclature was per the Pharmacogenetic Variation (PharmVar) Consortium (41). The CYP2D6 genotype, however, was returned as a “no call”. Subsequent gene resequencing revealed that the patient had a novel allele, which was submitted to PharmVar (41) and designated CYP2D6*119. The genotype of the patient was revised to CYP2D6*4/*119. The CYP2D6*119 allele shares many sequence variants with the decreased function CYP2D6*41 allele but lacks 2851C>T (p.R296C). Due to the presence of 2989G>A which has been shown to impact splicing, the CYP2D6*119 allele may have decreased function (PMID 33043448); thus we classified the patient as an IM (it is noted though that CPIC classified this alleles as “unknown function”). PM status for CYP3A5 and decreased expression of the MDR1 drug transporter were also discovered.
3rd treatment plan (13/06/2016–04/10/2016): Upon discharge, a treatment readjustment was made, as the potential increase in quetiapine plasma levels due to the quetiapine-fluoxetine pharmacokinetic interaction was thought to be related to the emergence of the deep venous thrombosis, combined with the fact that the hospital stay was prolonged, and the patient could have been bedridden longer than usual. The new prescription consisted of lorazepam, amisulpride, valproate, escitalopram, and trazodone. There were no documented AE, but required two hospitalizations of 9 days (04/07/2016–13/07/2016), due to behavioral disturbances in response to a change of residence, and 21 days (13/09/2016–04/10/2016), due to an exacerbation of the hypomanic symptomatology. Previous treatment was continued with minor extrapyramidal effects and insomnia.
4th treatment plan (October 2016–February 2017): Given the profile of adverse effects reported by the patient (excessive morning sedation and extrapyramidal symptoms) and the fact that the patient was not receiving a satisfactory therapeutic benefit, the pharmacological treatment was readjusted to amisulpride, olanzapine, valproate, and levomepromazine. Hyperprolactinemia was found in a routine clinical analysis, and amisulpride was suspended. The patient was hospitalized for 9 days (22/02/2017–03/03/2017) because of behavioral disturbances and depressed mood with delusions of guilt and harm, exhibiting mutism and a catatonic attitude. Treatment was continued with extrapyramidal effects during the hospitalization.
5th treatment plant (February 2017–May 2017): The patient was discharged with aripiprazole, lithium, clonazepam, lormetazepam, and citalopram. Minor extrapyramidal effects. Hospitalized for 12 days (06/05/2017–18/05/2017), due to disorganized behavior and refusal to take medication, with olanzapine, citalopram, lithium, clonazepam, and lormetazepam.
6th treatment plant (May 2017–December 2017): At discharge, the patient continued with olanzapine, clonazepam, lormetazepam, and lorazepam. The patient presented extrapyramidal symptoms after administration of haloperidol due to a manic episode managed as an outpatient.
7th treatment plant (from December 2017): Given the need to control the patient's sleep pattern and in light of the sedative effects of olanzapine, olanzapine was replaced with aripiprazole, eventually a long-acting injectable (LAI), to ensure adherence and simplify the absorption variables, complementing the therapy with lithium, clonazepam, lormetazepam, and pregabalin. From this point, the patient did not present AE, nor needed hospitalization.
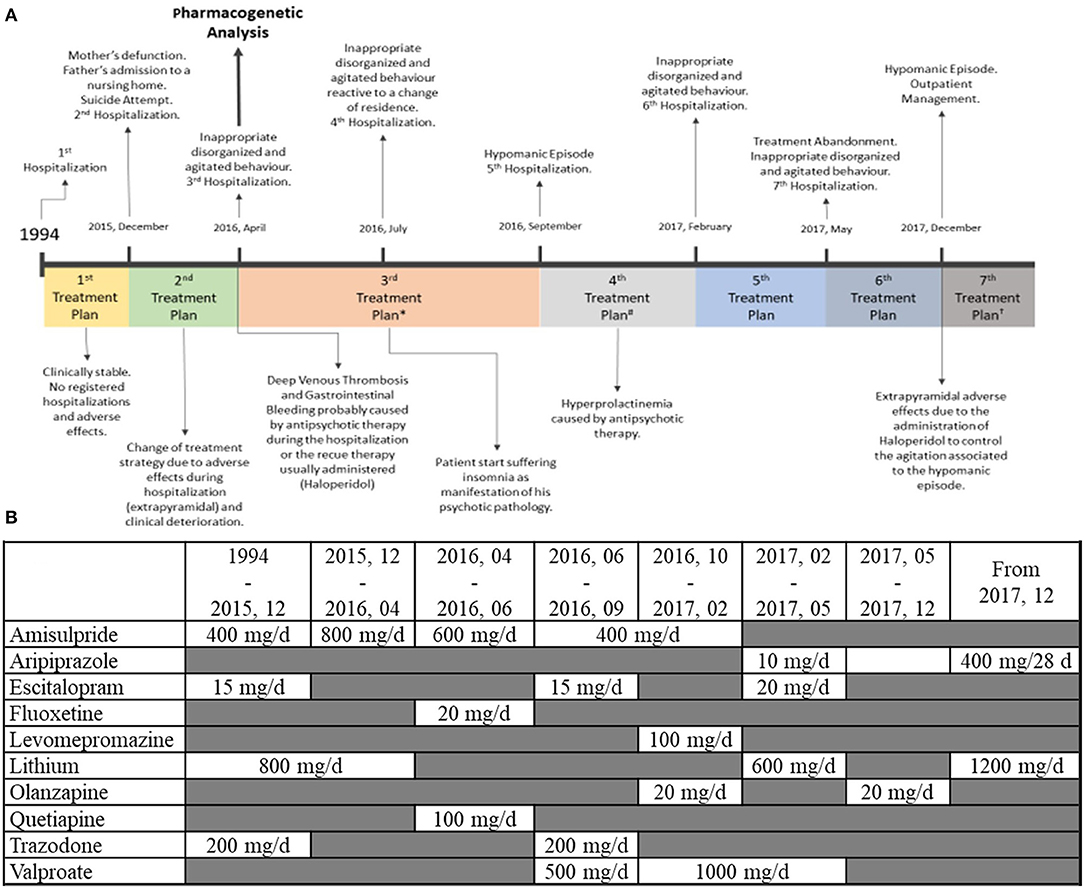
Figure 1. (A) Clinical history of the patient from 1994 to the end of the case study. *Therapeutic plan is slightly modified due to the patient's complaints of insomnia. #One of the antipsychotics used is discontinued due to the appearance of hyperprolactinemia.†After stabilizing a hypomanic episode, olanzapine (oral) is substituted by aripiprazole (LAI), and therapy is readjusted to control insomnia. (B) Pharmacotherapy doses. Daily doses administered through the different stages of the patient clinical evolution. Mg, milligram; D, day.
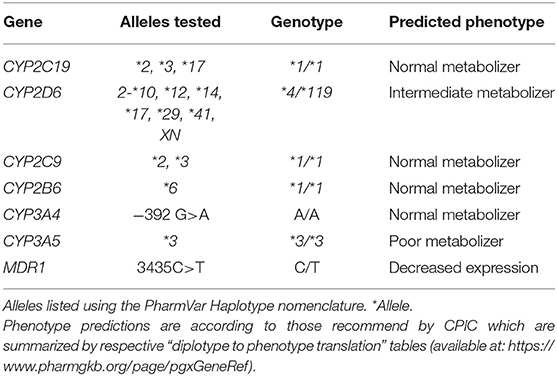
Table 1. Pharmacogenetic analysis.
Discussion
We present a patient with a novel CYP2D6 allele, CYP2D6*119, which was paired with a known non-functional allele. Since the novel allele and CYP2D6*41, a known decreased function allele, essentially only differ by an SNP that is believed to not alter the enzymatic activity, we classified the patient as IM. This phenotype (i.e., decreased CYP2D6 activity) may have contributed to the extrapyramidal AE presented after administration of levomepromazine and haloperidol, and the sedation associated with olanzapine. CYP2D6 has also been described to contribute to the metabolism of quetiapine and aripiprazole. Furthermore, the patient's ABCB1 genotype may have contributed to the hyperprolactinemia associated with amisulpride, to the deep venous thrombosis related to quetiapine, and, together with CYP2D6, to the sedation due to olanzapine. While CYP2D6 and CYP3A5 are not always the major metabolic pathway of drugs associated with AE presented by the patient, there could be a phenocopy effect related to drugs metabolized by these pathways.
This complex case illustrates how AE can impact patient compliance (44), as shown in two hospitalizations (February 2017, May 2017) caused by the patient refusing to continue the treatment. The patient was prescribed antipsychotics, which appeared to have repeatedly caused AE. Pharmacogenetic testing helped to partially understand the origin of his AE; it was possibly caused by a combination of his pharmacokinetic phenotype (reduced CYP2D6 and CYP3A5 enzymatic activity and MDR1 expression) and the phenocopy effect related to pharmacokinetic interactions (Table 2). A treatment plan that was guided by the patient's pharmacogenetic profile and knowledge about the pharmacokinetics of drugs prescribed drastically improved his medical condition. The patient ultimately reported no AE and continued to evolve favorably underscoring the utility of pharmacogenetic testing to guide pharmacotherapy. The application of this methodology could ensure a significant reduction in both pharmaceutical (fewer exacerbations hence less rescue medication, lower dosages, etc.) and hospitalization-related (fewer hospitalizations required to manage adverse effects or achieving better treatment adherence due to the reduction in the emergence of these adverse effects) economical costs. Although the evolution of the patient is not certain, the clinical intervention applied has a lifelong nature, and the results obtained by the pharmacogenetic analysis could be used by other medical areas. These conclusions should be considered taking into account the limitations of this study. Being this case report based on the application of a recently implemented approach to our service, we could not make use of all the possible variables that could be helpful when managing these patients (i.e., antipsychotic plasma levels). Moreover, this methodology was introduced, concurring with the increasing use of LAI presentations, which facilitate therapeutic adherence, and it could be a possible confounder. One of the strong points of this approach is that the decisions concerning the pharmacotherapy of the patient were agreed to by a multidisciplinary team (in which psychiatrists and clinical biochemists, among other clinical specialties, participated), which permitted a more profound knowledge about the drug metabolism and the factors influencing drug varying factors and promoted education on this subject for the bio-sanitary personnel (including psychiatric, nurses, psychologist, etc.).
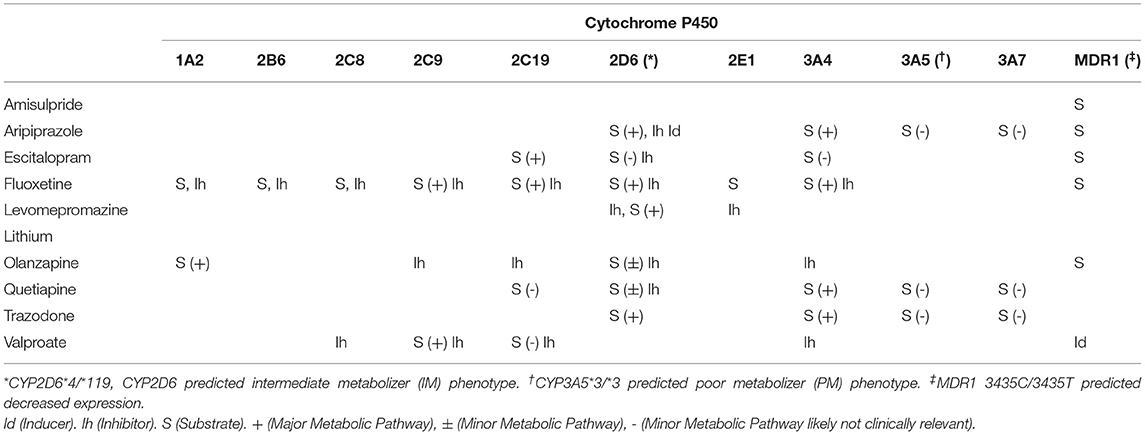
Table 2. Pharmacogenetic interaction of all treatment of the patient.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the University Hospital of Salamanca (CEIC ref.: 107/ 12/2016). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AG, MI-G, and MF-M: conceptualization. EM-V, LC-L, and MI-G: methodology. LC-L and IR-G: software. MI-G, BG-B, and EM-T: validation. EM-V, LC-L, and IR-G: formal analysis, investigation, data curation, and writing-original draft. EM-T and AS-J: resources. AG, AS, MI-G, and MF-M: writing-review and editing. LC-L, IR-G, and MI-G: visualization. MI-G and MF-M: project administration. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hálfdánarson Ó, Zoëga H, Aagaard L, Bernardo M, Brandt L, Fusté AC, et al. International trends in antipsychotic use: a study in 16 countries, 2005-2014. Eur Neuropsychopharmacol. (2017) 27:1064–76. doi: 10.1016/j.euroneuro.2017.07.001
2. McGrath J, Saha S, Chant D, Welham J. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol Rev. (2008) 30:67–76. doi: 10.1093/epirev/mxn001
3. Rintala H, Chudal R, Leppämäki S, Leivonen S, Hinkka-Yli-Salomäki S, Sourander A. Register-based study of the incidence, comorbidities and demographics of obsessive-compulsive disorder in specialist healthcare. BMC Psychiatry. (2017) 17:64. doi: 10.1186/s12888-017-1224-3
4. Rao P, Moore JK, Stewart R, Runions K, Bear N, Wong JWY, et al. Bipolar disorder in children and adolescents: diagnostic inpatient rates from 2000 to 2013 in Germany. Int J Bipolar Disord. (2016) 4:23. doi: 10.1186/s40345-016-0064-2
5. Okkels N, Vernal DL, Jensen SOW, Mcgrath JJ, Nielsen RE. Changes in the diagnosed incidence of early onset schizophrenia over four decades. Acta Psychiatr Scand. (2012) 127:62–8. doi: 10.1111/j.1600-0447.2012.01913.x
6. Kühl JOG, Laursen TM, Thorup A, Nordentoft M. The incidence of schizophrenia and schizophrenia spectrum disorders in Denmark in the period 2000-2012. A register-based study. Schizophr Res. (2016) 176:533–9. doi: 10.1016/j.schres.2016.06.023
7. Olfson M, Druss BG, Marcus SC. Trends in mental health care among children and adolescents. N Engl J Med. (2015) 372:2029–38. doi: 10.1056/NEJMsa1413512
8. WHO. Mental Health Action Plan 2013-2020 WHO. World Health Organization (2015). Available online at: http://www.who.int/entity/mental_health/publications/action_plan/en/index.html (accessed November 25, 2021).
9. Henriksen MG, Nordgaard J, Jansson LB. Genetics of schizophrenia: overview of methods, findings and limitations. Front Hum Neurosci. (2017) 11:322. doi: 10.3389/fnhum.2017.00322
10. Owen MJ, Sawa A, Mortensen PB. Schizophrenia. Lancet. (2016) 388:86–97. doi: 10.1016/S0140-6736(15)01121-6
11. Lally J, MacCabe JH. Antipsychotic medication in schizophrenia: a review. Br Med Bull. (2015) 114:169–79. doi: 10.1093/bmb/ldv017
12. Ozomaro U, Wahlestedt C, Nemeroff CB. Personalized medicine in psychiatry: problems and promises. BMC Med. (2013) 11:132. doi: 10.1186/1741-7015-11-132
13. Martin A, Downing J, Maden M, Fleeman N, Alfirevic A, Haycox A, et al. An assessment of the impact of pharmacogenomics on health disparities: a systematic literature review. Pharmacogenomics. (2017) 18:1541–50. doi: 10.2217/pgs-2017-0076
14. Ravyn D, Ravyn V, Lowney R, Nasrallah HA. CYP450 Pharmacogenetic treatment strategies for antipsychotics: a review of the evidence. Schizophr Res. (2013) 149:1–14. doi: 10.1016/j.schres.2013.06.035
15. Solmi M, Murru A, Pacchiarotti I, Undurraga J, Veronese N, Fornaro M, et al. Safety, tolerability, and risks associated with first- and second-generation antipsychotics: a state-of-the-art clinical review. Ther Clin Risk Manag. (2017) 13:757–77. doi: 10.2147/TCRM.S117321
16. Lieberman JA, Stroup TS, McEvoy JP, Swartz MS, Rosenheck RA, Perkins DO, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. (2005) 353:1209–23. doi: 10.1056/NEJMoa051688
17. Foster A. Pharmacogenetics of antipsychotic adverse effects: case studies and a literature review for clinicians. Neuropsychiatr Dis Treat. (2008) 3:965–73. doi: 10.2147/NDT.S1752
18. Shenoy S, R A, Bhandary RP, Praharaj SK. Frequency, reasons, and factors associated with antipsychotic polypharmacy in Schizophrenia: a retrospective chart review in a tertiary hospital in India. Asian J Psychiatr. (2020) 51:102022. doi: 10.1016/j.ajp.2020.102022
19. Li N, Cao T, Wu X, Tang M, Xiang D, Cai H. Progress in genetic polymorphisms related to lipid disturbances induced by atypical antipsychotic drugs. Front Pharmacol. (2020) 10:1669. doi: 10.3389/fphar.2019.01669
20. Eum S, Lee AM, Bishop JR. Pharmacogenetic tests for antipsychotic medications: clinical implications and considerations. Dialogues Clin Neurosci. (2016) 18:323–37. doi: 10.31887/DCNS.2016.18.3/jbishop
21. Zhuo C, Hou W, Lin C, Hu L, Li J. Potential value of genomic copy number variations in schizophrenia. Front Mol Neurosci. (2017) 10:204. doi: 10.3389/fnmol.2017.00204
22. Mahintamani T, Mitra S, Kavoor A, Nizamie Sh. Negative symptoms in schizophrenia. Ind Psychiatry J. (2016) 25:135. doi: 10.4103/ipj.ipj_30_15
23. Urichuk L, Prior T, Dursun S, Baker G. Metabolism of atypical antipsychotics: involvement of cytochrome P450 enzymes and relevance for drug-drug interactions. Curr Drug Metab. (2008) 9:410–8. doi: 10.2174/138920008784746373
24. Lynch T, Price A. The effect of cytochrome P450 metabolism on drug response, interactions, and adverse effects. Am Fam Physician. (2007) 76:391–6.
25. Sheehan JJ, Sliwa JK, Amatniek JC, Grinspan A, Canuso CM. Atypical antipsychotic metabolism and excretion. Curr Drug Metab. (2010) 11:516–25. doi: 10.2174/138920010791636202
26. Hoffmann MF, Preissner SC, Nickel J, Dunkel M, Preissner R, Preissner S. The transformer database: biotransformation of xenobiotics. Nucleic Acids Res. (2014) 42:D1113–7. doi: 10.1093/nar/gkt1246
27. Gaedigk A, Riffel AK, Berrocal BG, Solaesa VG, Dávila I, Isidoro-García M. Characterization of a complex CYP2D6 genotype that caused an AmpliChip CYP450 Test® no-call in the clinical setting. Clin Chem Lab Med. (2014) 52:799–807. doi: 10.1515/cclm-2013-0943
28. Gaedigk A, Hernandez J, García-Solaesa V, Sánchez S, Isidoro-García M. Detection and characterization of {theCYP}2D6{*}9x2gene duplication in two Spanish populations: resolution of {AmpliChip} {CYP}450 test no-calls. Pharmacogenomics. (2011) 12:1617–22. doi: 10.2217/pgs.11.107
29. Lloret-Linares C, Rollason V, Lorenzini KI, Samer C, Daali Y, Gex-Fabry M, et al. Screening for genotypic and phenotypic variations in {CYP}450 activity in patients with therapeutic problems in a psychiatric setting, a retrospective study. Pharmacol Res. (2017) 118:104–10. doi: 10.1016/j.phrs.2016.07.002
30. Lu YF, Goldstein DB, Angrist M, Cavalleri G. Personalized medicine and human genetic diversity. Cold Spring Harb Perspect Med. (2014) 4:a008581. doi: 10.1101/cshperspect.a008581
31. König IR, Fuchs O, Hansen G, von Mutius E, Kopp M V. What is precision medicine? Eur Respir J. (2017) 50:1–12. doi: 10.1183/13993003.00391-2017
32. Beckmann JS, Lew D. Reconciling evidence-based medicine and precision medicine in the era of big data: challenges and opportunities. Genome Med. (2016) 8:1–11. doi: 10.1186/s13073-016-0388-7
33. Carrasco-Ramiro F, Peiró-Pastor R, Aguado B. Human genomics projects and precision medicine. Gene Therapy. (2017) 24:551–61. doi: 10.1038/gt.2017.77
34. Nofziger C, Turner A, Sangkuhl K, Whirl-Carrillo M, Agúndez J, Black J et al. PharmVar GeneFocus: CYP2D6. Clin Pharmacol Ther. (2019) 107:154–70. doi: 10.1002/cpt.1643
35. Botton M, Whirl-Carrillo M, Del Tredici A, Sangkuhl K, Cavallari L, Agúndez J et al. PharmVar GeneFocus: CYP2C19. Clin Pharmacol Ther. (2020) 109:352–366. doi: 10.1002/cpt.1973
36. Caudle K, Sangkuhl K, Whirl-Carrillo M, Swen J, Haidar C, Klein T et al. Standardizing CYP 2D6 genotype to phenotype translation: consensus recommendations from the clinical pharmacogenetics implementation consortium and dutch pharmacogenetics working group. Clin Transl Sci. (2019) 13:116–24. doi: 10.1111/cts.12692
37. Taylor C, Crosby I, Yip V, Maguire P, Pirmohamed M, Turner R. A review of the important role of CYP2D6 in pharmacogenomics. Genes. (2020) 11:1295. doi: 10.3390/genes11111295
38. Saravanakumar A, Sadighi A, Ryu R, Akhlaghi F. Physicochemical properties, biotransformation, and transport pathways of established and newly approved medications: a systematic review of the top 200 most prescribed drugs vs. the FDA-approved drugs between 2005 and 2016. Clin Pharmacokin. (2019) 58:1281–94. doi: 10.1007/s40262-019-00750-8
39. Gaedigk A, Sangkuhl K, Whirl-Carrillo M, Twist GP, Klein TE, Miller NA. The Evolution of PharmVar. Clin Pharmacol Ther. (2019) 105:29–32. doi: 10.1002/cpt.1275
40. Gaedigk A, Whirl-Carrillo M, Pratt VM, Miller NA, Klein TE. PharmVar and the landscape of pharmacogenetic resources. Clin Pharmacol Ther. (2020) 107:43–6. doi: 10.1002/cpt.1654
41. Gaedigk A, Ingelman-Sundberg M, Miller NA, Leeder JS, Whirl-Carrillo M, Klein TE, et al. The pharmacogene variation (PharmVar) consortium: incorporation of the human cytochrome P450 (CYP) allele nomenclature database. Clin Pharmacol Ther. (2018) 103:399–401. doi: 10.1002/cpt.910
42. Gaedigk A, Sangkuhl K, Whirl-Carrillo M, Klein T, Leeder J. Prediction of CYP2D6 phenotype from genotype across world populations. Genet Med. (2017) 19:69–76. doi: 10.1038/gim.2016.80
43. De Leon J. AmpliChip CYP450 test: personalized medicine has arrived in psychiatry. Expert Rev Mol Diagn. (2006) 6:277–86. doi: 10.1586/14737159.6.3.277
Keywords: antipsychotic agents, pharmacogenetics, cytochrome P450 enzyme system, psychotic disorders, precision medicine
Citation: Marcos-Vadillo E, Carrascal-Laso L, Ramos-Gallego I, Gaedigk A, García-Berrocal B, Mayor-Toranzo E, Sevillano-Jiménez A, Sánchez A, Isidoro-García M and Franco-Martín M (2022) Case Report: Pharmacogenetics Applied to Precision Psychiatry Could Explain the Outcome of a Patient With a New CYP2D6 Genotype. Front. Psychiatry 12:830608. doi: 10.3389/fpsyt.2021.830608
Received: 07 December 2021; Accepted: 30 December 2021;
Published: 25 February 2022.
Edited by:
Mirko Manchia, University of Cagliari, ItalyReviewed by:
Clement Zai, Centre for Addiction and Mental Health (CAMH), CanadaIsa Houwink, Leiden University Medical Center, Netherlands
Copyright © 2022 Marcos-Vadillo, Carrascal-Laso, Ramos-Gallego, Gaedigk, García-Berrocal, Mayor-Toranzo, Sevillano-Jiménez, Sánchez, Isidoro-García and Franco-Martín. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Isidoro-García, misidoro@saludcastillayleon.es