
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry, 10 January 2022
Sec. Schizophrenia
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.813590
This article is part of the Research TopicReviews in Psychiatry 2022: SchizophreniaView all 9 articles
 Xin-Yang Zhang1,2†
Xin-Yang Zhang1,2† Huo-Di Chen3†Wan-Nian Liang4†Xin-Hu Yang1Dong-Bin Cai5Xiong Huang1
Huo-Di Chen3†Wan-Nian Liang4†Xin-Hu Yang1Dong-Bin Cai5Xiong Huang1 Xing-Bing Huang1
Xing-Bing Huang1 Cheng-Yi Liu2
Cheng-Yi Liu2 Wei Zheng1*
Wei Zheng1*Objective: The efficacy and safety of adjunctive magnetic seizure therapy (MST) for patients with schizophrenia are unclear. This systematic review was conducted to examine the efficacy and safety of adjunctive MST for schizophrenia.
Methods: Chinese (WanFang and Chinese Journal Net) and English (PubMed, EMBASE, PsycINFO, and the Cochrane Library) databases were systematically searched.
Results: Two open-label self-controlled studies (n = 16) were included and analyzed in this review. In these studies, the Positive and Negative Syndrome Scale (PANSS) total scores and Brief Psychiatric Rating Scale (BPRS) total scores significantly decreased from baseline to post-MST (all Ps < 0.05), without serious adverse neurocognitive effects. Mixed findings on the neurocognitive effects of adjunctive MST for schizophrenia were reported in the two studies. A discontinuation rate of treatment of up to 50% (4/8) was reported in both studies. The rate of adverse drug reactions (ADRs) was evaluated in only one study, where the most common ADRs were found to be dizziness (25%, 2/8) and subjective memory loss (12.5%, 1/8).
Conclusion: There is inconsistent evidence for MST-related adverse neurocognitive effects and preliminary evidence for the alleviation of psychotic symptoms in schizophrenia.
Schizophrenia is a severely disabling psychiatric disorder affecting ~1% of the population worldwide (1–3). The economic burden of schizophrenia amounted to $155.7 billion in the United States in 2013 (4). Despite advances in psychopharmacologic therapy, nearly 50% of schizophrenia patients do not respond to therapy with antipsychotics (5–7). Consequently, non-pharmacological therapies, such as augmentation strategies, have been widely used for schizophrenia in clinical practice, with neuromodulation techniques being particularly common (8), including electroconvulsive therapy (ECT) (9–11), repetitive transcranial magnetic stimulation (rTMS) (12), deep brain stimulation (DBS) (13, 14), non-convulsive electrotherapy (15, 16), transcranial direct current stimulation (tDCS) (17–19), and magnetic seizure therapy (MST) (20, 21).
ECT is the most effective treatment for individuals suffering from schizophrenia (22, 23) and mood disorders (24). For example, a recent randomized controlled trial (RCT) (22) and meta-analysis (23) found that the augmentation of clozapine with ECT is a highly effective therapy for clozapine-resistant schizophrenia (CRS). ECT is also an effective and safe method in treating elderly patients with treatment-resistant depression (TRD) (25). Interestingly, as reported by Osler et al.'s study (26), ECT was related to a decreased rate of dementia in patients aged 70 years and older. However, ECT-related adverse neurocognitive effects, including disorientation, amnesia, and executive dysfunction, prevent the use of ECT as a first-choice therapy for schizophrenia and mood disorders (27–29). Importantly, the damaging stigma surrounding ECT also potentially impedes widespread acceptance of this therapy among individuals suffering from schizophrenia (30).
MST is a novel neurotherapeutic intervention that induces therapeutic seizures based on high-frequency rTMS (31–34). MST appears to have a favorable clinical benefit on neurocognitive adverse effects and thus has been proposed as an alternative to ECT (21, 35). Accumulating evidence shows that MST is associated with relatively fewer neurocognitive adverse effects than ECT for major depressive disorder (MDD) (36, 37). In a recent meta-analysis, MST was associated with shorter recovery and reorientation times and lower cognitive impairment for MDD than ECT (38). However, inconsistent findings have been reported in two studies on patients with schizophrenia receiving MST treatments (20, 21).
To date, no systematic review on the efficacy and safety of adjunctive MST for schizophrenia has been published. Therefore, the target of the current study was to investigate the efficacy and safety of MST as an adjunctive therapy in schizophrenia.
This systematic review was conducted according to PRISMA guidelines (39). Studies were selected and screened for inclusion in line with the following PICOS criteria. Participants: adult subjects with a diagnosis of schizophrenia based on any standardized diagnostic instruments. Intervention vs. Comparison: treatment as usual (TAU) plus MST vs. TAU plus ECT (RCTs); MST added to TAU (open-label prospective trials). Outcomes: in this systematic review, the primary outcome was the improvement of psychotic symptoms, as measured by the Positive and Negative Syndrome Scale (PANSS) (40) or Brief Psychiatric Rating Scale (BPRS) (41). Key secondary outcomes were adverse neurocognitive effects, study defined response and remission, the rate of adverse drug reactions (ADRs), and discontinuation of treatment for any reason. Study: only published case series, open-label prospective trials or RCTs examining the efficacy and safety of adjunctive MST for individuals experiencing schizophrenia were eligible for inclusion. Meta-analyses and systematic reviews were excluded.
Two investigators (XYZ and XHY) independently searched English (PubMed, EMBASE, PsycINFO, and Cochrane Library) and Chinese (WanFang and Chinese Journal Net) databases from the date of inception until October 6, 2021 for studies on adjunctive MST for schizophrenia using the following search terms: (“magnetic seizure therapy”[Mesh] OR magnetic seizure therapy OR MST) AND (“schizophrenia”[Mesh] OR schizophrenic disorder OR disorder, schizophrenic OR schizophrenic disorders OR schizophrenia OR dementia praecox). Similarly, two independent investigators (XYZ and XHY) evaluated whether the potentially relevant studies fulfilled the inclusion criteria of this systematic review, and the senior author (WZ) was consulted in case of any differences of opinion.
Two investigators (XYZ and XHY) independently extracted data from each included study. Any discrepancies in data entry between the two investigators (XYZ and XHY) were discussed, and the senior author (WZ) was consulted as needed. We contacted the first and/or corresponding authors to acquire any missing information as necessary. The quality of each included RCT and open-label prospective trial was evaluated by two independent investigators (XYZ and XHY) using the Cochrane risk of bias (42) and the Newcastle-Ottawa Scale (NOS), respectively (43). A NOS score of 7 or above was considered high quality. The quality of evidence and strength of recommendations of this systematic review was evaluated using the grading of recommendations assessment, development, and evaluation (GRADE) system (44), ranging from “very low quality,” “low quality,” “moderate quality” to “high quality.
As shown in Figure 1, a total of 316 hits were identified from the aforementioned databases. Finally, two open-label self-controlled studies met the inclusion criteria of this systematic review (20, 21). It was not possible to conduct a meta-analysis because of the inconsistencies in study methodologies, parameters of MST, and antipsychotic dosages.
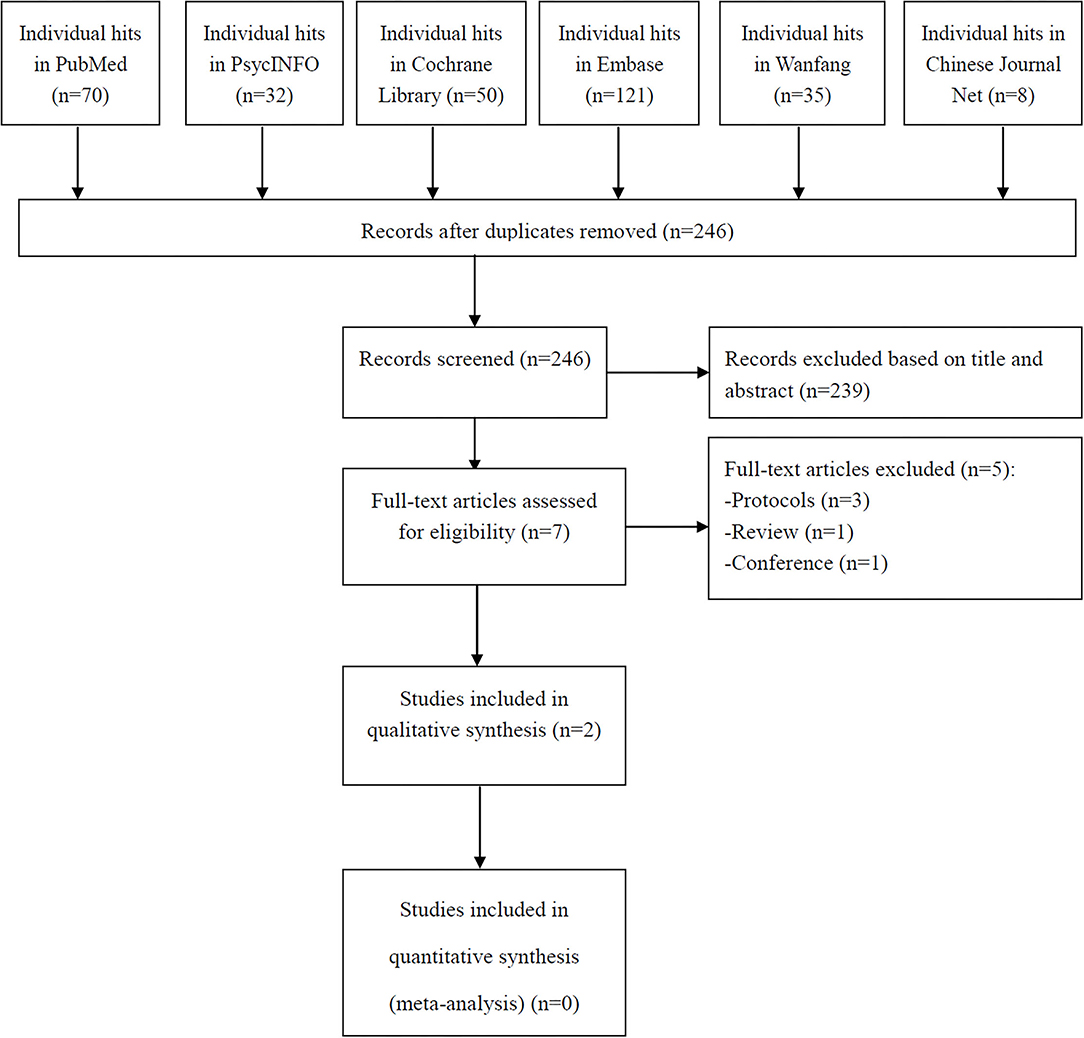
Figure 1. PRISMA flow diagram.
The characteristics of the two open-label self-controlled studies (n = 16) (20, 21) are summarized in Table 1. The included studies were published within the last 3 years, showing that adjunctive MST for schizophrenia is a new clinically important topic. One study was conducted in China (20), and the other was conducted in Canada (21). The studies differed in that the MST was administered using a stimulator machine at a fixed frequency of 25 Hz (100% output) in Jiang et al.'s study (20) and a flexible frequency of 25–100 Hz (100% output) in Tang et al.'s study (21).

Table 1. Summary of characteristics of included studies.
The Cochrane risk of bias was not used because no RCTs were included in this systematic review. The NOS scores of the two self-controlled studies (20, 21) were 7 points (high quality) (Table 1). Following the GRADE system, the quality of evidence for each outcome was considered as “low” (Supplementary Table 1).
As shown in Table 2, patients with schizophrenia experienced a significant improvement in psychotic symptoms post-MST, as measured by the PANSS scale (total scores and positive subscale scores) (20) and the BPRS scale (total scores) (21) (all Ps<0.05). In Jiang et al.'s study (20), 3 out of 8 patients (37.5%) responded to MST. In Tang et al.'s study (21), 37.5% (3/8) of the patients met the remission criteria, and 50% (4/8) of the patients met the response criteria.

Table 2. The improvement of psychotic symptoms after MST.
Table 3 summarizes the neurocognitive effects of adjunctive MST for schizophrenia. Jiang et al. found using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) that MST was associated with an improvement in immediate memory (66.7%, 2/3) but not in delayed memory (20). In the other study, MST was found to produce an significant decrease in neurocognitive performance, as measured by the Autobiographical Memory Inventory Short Form (AMI-SF) (P < 0.05), but no such decrease was found using the MATRICS Consensus Cognitive Battery (MCCB), Trail Making Test (TMT), Stroop Test or Verbal Fluency using the Controlled Oral Word Association Test (COWAT), and Montreal Cognitive Assessment (MoCA) (all Ps > 0.05) (21).
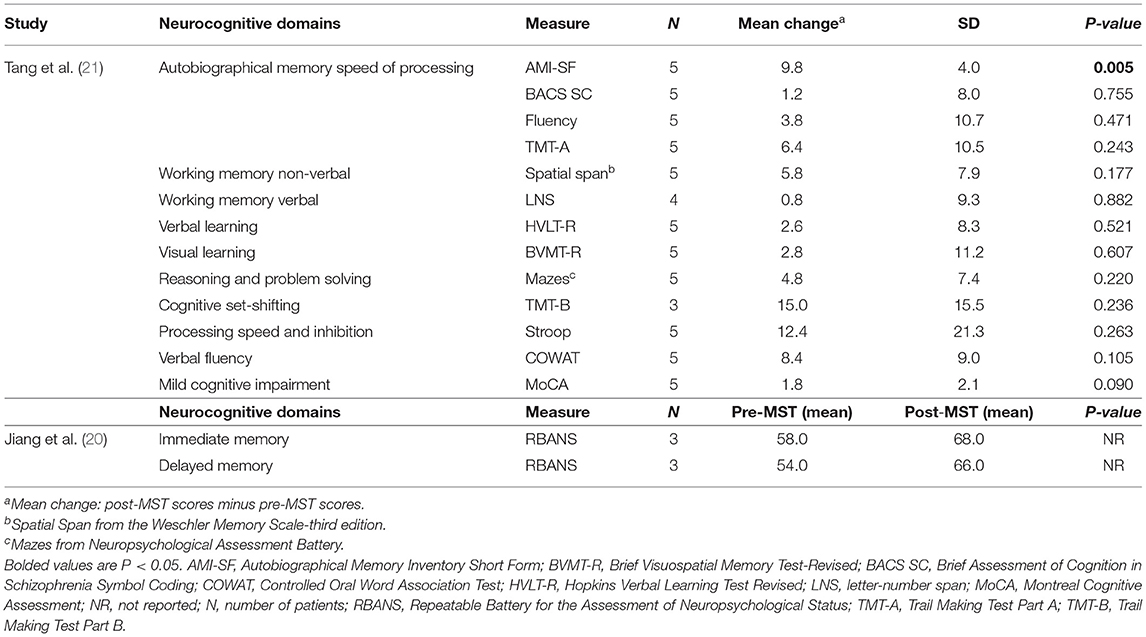
Table 3. Neurocognitive adverse events after MST.
In both studies, discontinuation of MST for any reason was reported for 50% (4/8) of the participants (20, 21). The patients' subjective experience of MST was only evaluated in one study, and the most common ADRs were found to be dizziness (25%, 2/8) and subjective memory loss (12.5%, 1/8) (20).
This article is the first systematic review on the efficacy and safety of MST as an adjunctive therapy for schizophrenia. Only two open-label self-controlled studies (20, 21) were included in this systematic review, corresponding to a total of 16 patients. The main findings were that adjunctive MST was efficacious for total psychopathology in schizophrenia, as measured by the PANSS and the BPRS, and did not have serious adverse neurocognitive effects. Both studies examined the neurocognitive effects of adjunctive MST for schizophrenia, but mixed findings were reported. A relatively high rate of discontinuation of MST for any reason was reported in both studies. The most common ADRs were evaluated in only one study and found to be dizziness and subjective memory loss (20). Although MST appears to be an interesting and potentially important adjunctive therapy for patients suffering from schizophrenia, these findings should be clearly verified in future studies with a randomized double-blind ECT-controlled design.
This systematic review shows there is preliminary evidence for the antipsychotic effects of MST in schizophrenia and negligible neurocognitive adverse effects. As reported in the two included studies (20, 21), the response rate of adjunctive MST for individuals experiencing schizophrenia ranged from 37.5 to 50%, which was far lower than the reported response rate to ECT of up to 74% (45). However, Kayser et al. reported that up to 69% of patients with TRD responded to MST (46). The latest meta-analysis (10 studies, 285 patients) found that MST produces a similar antidepressant effect to ECT (38). Furthermore, the optimal parameters of MST need to be determined.
As for other neurotherapeutic strategies, such as tDCS, DBS, or ECT, the main objective in investigating MST is to monitor the effects on neurocognition. The findings of this systematic review are that MST has little to no adverse neurocognitive effects, supporting the findings of an early study (47). However, the findings of the two included studies on the neurocognitive effects of MST were inconsistent (20, 21). Thus, more studies need to be performed to determine the neurocognitive effects of MST in schizophrenia. Interestingly, several clinical trials have shown non-convulsive electrotherapy to be effective for individuals suffering from schizophrenia (15) and TRD (48, 49) without associated adverse neurocognitive effects. However, no head-to-head studies have been published that compare the efficacy and safety of MST and non-convulsive electrotherapy in treating schizophrenia.
This systematic review is limited for the following reasons. First, only two open-label self-controlled studies (20, 21) with relatively small sample sizes were included. Second, a quantitative analysis could not be conducted because of the heterogeneity between the studies. Third, this systematic review has not been registered before the beginning of this systematic review. Finally, a high rate of discontinuation of MST for any reason was reported in both studies (20, 21), indicating the difficulty of treating individuals experiencing schizophrenia. In future clinical studies on adjunctive MST for schizophrenia, strategies need to be developed to address the problem of discontinuation.
There is inconsistent evidence for MST-related adverse neurocognitive effects and preliminary evidence for the alleviation of psychotic symptoms in schizophrenia. RCTs with an optimal sample size need to be performed on the use of adjunctive MST for schizophrenia to confirm and extend these findings.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
X-YZ and X-HY selected studies and extracted the data. WZ reviewed all the data and helped mediate disagreements. X-YZ, WZ, and D-BC wrote the first draft. All authors contributed to the interpretation of data and approved the final manuscript.
This study was funded by the National Natural Science Foundation of China (82101609), Scientific Research Project of Guangzhou Bureau of Education (202032762), Science and Technology Program Project of Guangzhou (202102020658), the Science and Technology Planning Project of Liwan District of Guangzhou (202004034), Guangzhou Health Science and Technology Project (20211A011045), Guangzhou science and Technology Project of traditional Chinese Medicine and integrated traditional Chinese and Western medicine (20212A011018), China International Medical Exchange Foundation (Z-2018-35-2002), Guangzhou Clinical Characteristic Technology Project (2019TS67), science and Technology Program Project of Guangzhou (202102020658), and Guangdong Hospital Association (2019ZD06). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.813590/full#supplementary-material
1. Mueser KT, McGurk SR. Schizophrenia. Lancet. (2004) 363:2063–72. doi: 10.1016/S0140-6736(04)16458-1
2. Richetto J, Meyer U. Epigenetic modifications in schizophrenia and related disorders: molecular scars of environmental exposures and source of phenotypic variability. Biol Psychiatry. (2021) 89:215–26. doi: 10.1016/j.biopsych.2020.03.008
3. McCutcheon RA, Reis Marques T, Howes OD. Schizophrenia-an overview. JAMA Psychiatry. (2020) 77:201–10. doi: 10.1001/jamapsychiatry.2019.3360
4. Cloutier M, Aigbogun MS, Guerin A, Nitulescu R, Ramanakumar AV, Kamat SA, et al. The economic burden of schizophrenia in the United States in 2013. J Clin Psychiatry. (2016) 77:764–71. doi: 10.4088/JCP.15m10278
5. Tiihonen J, Halonen P, Wahlbeck K, Repo-Tiihonen E, Hyvärinen S, Eronen M, et al. Topiramate add-on in treatment-resistant schizophrenia: a randomized, double-blind, placebo-controlled, crossover trial. J Clin Psychiatry. (2005) 66:1012–5. doi: 10.4088/JCP.v66n0808
6. Kane JM, Correll CU. Past and present progress in the pharmacologic treatment of schizophrenia. J Clin Psychiatry. (2010) 71:1115–24. doi: 10.4088/JCP.10r06264yel
7. Carbon M, Correll CU. Clinical predictors of therapeutic response to antipsychotics in schizophrenia. Dial Clin Neurosci. (2014) 16:505–24. doi: 10.31887/DCNS.2014.16.4/mcarbon
8. Siskind DJ, Lee M, Ravindran A, Zhang Q, Ma E, Motamarri B, et al. Augmentation strategies for clozapine refractory schizophrenia: a systematic review and meta-analysis. Australian New Zeal J Psychiatry. (2018) 52:751–67. doi: 10.1177/0004867418772351
9. Grover S, Sahoo S, Rabha A, Koirala R. ECT in schizophrenia: a review of the evidence. Acta Neuropsychiatr. (2019) 31:115–27. doi: 10.1017/neu.2018.32
10. Teodorczuk A, Emmerson B, Robinson G. Revisiting the role of electroconvulsive therapy in schizophrenia: where are we now? Australasian Psychiatry. (2019) 27:477–9. doi: 10.1177/1039856219860033
11. Sanghani SN, Petrides G, Kellner CH. Electroconvulsive therapy (ECT) in schizophrenia: a review of recent literature. Curr Opin Psychiatry. (2018) 31:213–22. doi: 10.1097/YCO.0000000000000418
12. Cole JC, Green Bernacki C, Helmer A, Pinninti N, O'Reardon JP. Efficacy of transcranial magnetic stimulation (TMS) in the treatment of schizophrenia: a review of the literature to date. Innov Clin Neurosci. (2015) 12:12–9.
13. Corripio I, Roldán A, Sarró S, McKenna PJ, Alonso-Solís A, Rabella M, et al. Deep brain stimulation in treatment resistant schizophrenia: a pilot randomized cross-over clinical trial. EBioMedicine. (2020) 51:102568. doi: 10.1016/j.ebiom.2019.11.029
14. Beszłej JA, Wieczorek T, Kobyłko A, Piotrowski P, Siwicki D, Weiser A, et al. Deep brain stimulation: new possibilities for the treatment of mental disorders. Psychiatria Polska. (2019) 53:789–806. doi: 10.12740/PP/OnlineFirst/103090
15. Li MZ, Chen LC, Rong H, Xu SX, Li Y, Yang QF, et al. Low-charge electrotherapy for patients with schizophrenia: a double-blind, randomised controlled pilot clinical trial. Psychiatry Res. (2019) 272:676–81. doi: 10.1016/j.psychres.2018.12.143
16. Miller DH, Clancy J, Cumming E. A comparison between unidirectional current nonconvulsive electrical stimulation given with Reiter's machine, standard alternating current electro-shock (Cerletti method), and pentothal in chronic schizophrenia. Am J Psychiatry. (1953) 109:617–20. doi: 10.1176/ajp.109.8.617
17. Valiengo L, Goerigk S, Gordon PC, Padberg F, Serpa MH, Koebe S, et al. Efficacy and safety of transcranial direct current stimulation for treating negative symptoms in schizophrenia: a randomized clinical trial. JAMA Psychiatry. (2020) 77:121–9. doi: 10.1001/jamapsychiatry.2019.3199
18. Brunoni AR, Shiozawa P, Truong D, Javitt DC, Elkis H, Fregni F, et al. Understanding tDCS effects in schizophrenia: a systematic review of clinical data and an integrated computation modeling analysis. Expert Review Med Devices. (2014) 11:383–94. doi: 10.1586/17434440.2014.911082
19. Sun CH, Jiang WL, Cai DB, Wang ZM, Sim K, Ungvari GS, et al. Adjunctive multi-session transcranial direct current stimulation for neurocognitive dysfunction in schizophrenia: a meta-analysis. Asian J Psychiatry. (2021) 66:102887. doi: 10.1016/j.ajp.2021.102887
20. Jiang JL, Li QW, Sheng JH, Yang FZ, Cao XY, Zhang TH, et al. 25 Hz magnetic seizure therapy is feasible but not optimal for Chinese patients with schizophrenia: a case series. Front Psychiatry. (2018) 9:224. doi: 10.3389/fpsyt.2018.00224
21. Tang VM, Blumberger DM, McClintock SM, Kaster TS, Rajji TK, Downar J, et al. Magnetic seizure therapy in treatment-resistant schizophrenia: a pilot study. Front Psychiatry. (2018) 8:310. doi: 10.3389/fpsyt.2017.00310
22. Petrides G, Malur C, Braga RJ, Bailine SH, Schooler NR, Malhotra AK, et al. Electroconvulsive therapy augmentation in clozapine-resistant schizophrenia: a prospective, randomized study. Am J Psychiatry. (2015) 172:52–8. doi: 10.1176/appi.ajp.2014.13060787
23. Wang G, Zheng W, Li XB, Wang SB, Cai DB, Yang XH, et al. ECT augmentation of clozapine for clozapine-resistant schizophrenia: a meta-analysis of randomized controlled trials. J Psychiatr Res. (2018) 105:23–32. doi: 10.1016/j.jpsychires.2018.08.002
24. Pagnin D, de Queiroz V, Pini S, Cassano GB. Efficacy of ECT in depression: a meta-analytic review. J ECT. (2004) 20:13–20. doi: 10.1097/00124509-200403000-00004
25. Jiang X, Xie Q, Liu LZ, Zhong BL, Si L, Fan F. Efficacy and safety of modified electroconvulsive therapy for the refractory depression in older patients. Asia-Pacific Psychiatry. (2020) 12:e12411. doi: 10.1111/appy.12411
26. Osler M, Rozing MP, Christensen GT, Andersen PK, Jørgensen MB. Electroconvulsive therapy and risk of dementia in patients with affective disorders: a cohort study. Lancet Psychiatry. (2018) 5:348–56. doi: 10.1016/S2215-0366(18)30056-7
27. Semkovska M, McLoughlin DM. Objective cognitive performance associated with electroconvulsive therapy for depression: a systematic review and meta-analysis. Biol Psychiatry. (2010) 68:568–77. doi: 10.1016/j.biopsych.2010.06.009
28. Lisanby SH. Electroconvulsive therapy for depression. N Engl J Med. (2007) 357:1939–45. doi: 10.1056/NEJMct075234
29. Gazdag G, Dragasek J, Takács R, Lõokene M, Sobow T, Olekseev A, et al. Use of electroconvulsive therapy in central-eastern european countries: an overview. Psychiatria Danubina. (2017) 29:136–40. doi: 10.24869/psyd.2017.136
30. Dowman J, Patel A, Rajput K. Electroconvulsive therapy: attitudes and misconceptions. J ECT. (2005) 21:84–7. doi: 10.1097/01.yct.0000161043.00911.45
31. Backhouse FA, Noda Y, Knyahnytska Y, Farzan F, Downar J, Rajji TK, et al. Characteristics of ictal EEG in Magnetic Seizure Therapy at various stimulation frequencies. Clin Neurophysiol. (2018) 129:1770–9. doi: 10.1016/j.clinph.2018.03.025
32. Lee WH, Lisanby SH, Laine AF, Peterchev AV. Comparison of electric field strength and spatial distribution of electroconvulsive therapy and magnetic seizure therapy in a realistic human head model. Eur Psychiatry. (2016) 36:55–64. doi: 10.1016/j.eurpsy.2016.03.003
33. Sun Y, Blumberger DM, Mulsant BH, Rajji TK, Fitzgerald PB, Barr MS, et al. Magnetic seizure therapy reduces suicidal ideation and produces neuroplasticity in treatment-resistant depression. Transl Psychiatry. (2018) 8:253. doi: 10.1038/s41398-018-0302-8
34. Sun Y, Farzan F, Mulsant BH, Rajji TK, Fitzgerald PB, Barr MS, et al. Indicators for remission of suicidal ideation following magnetic seizure therapy in patients with treatment-resistant depression. JAMA Psychiatry. (2016) 73:337–45. doi: 10.1001/jamapsychiatry.2015.3097
35. Tang VM, Blumberger DM, Throop A, McClintock SM, Voineskos D, Downar J, et al. Continuation magnetic seizure therapy for treatment-resistant unipolar or bipolar depression. J Clin Psychiatry. (2021) 82:20m13677. doi: 10.4088/JCP.20m13677
36. Lisanby SH, Luber B, Schlaepfer TE, Sackeim HA. Safety and feasibility of magnetic seizure therapy (MST) in major depression: randomized within-subject comparison with electroconvulsive therapy. Neuropsychopharmacology. (2003) 28:1852–65. doi: 10.1038/sj.npp.1300229
37. Daskalakis ZJ, Dimitrova J, McClintock SM, Sun Y, Voineskos D, Rajji TK, et al. Magnetic seizure therapy (MST) for major depressive disorder. Neuropsychopharmacology. (2020) 45:276–82. doi: 10.1038/s41386-019-0515-4
38. Chen M, Yang X, Liu C, Li J, Wang X, Yang C, et al. Comparative efficacy and cognitive function of magnetic seizure therapy vs. electroconvulsive therapy for major depressive disorder: a systematic review and meta-analysis. Transl Psychiatry. (2021) 11:437. doi: 10.1038/s41398-021-01560-y
39. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. (2009) 339:b2535. doi: 10.1136/bmj.b2535
40. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
41. Overall JE, Beller SA. The Brief Psychiatric Rating Scale (BPRS) in geropsychiatric research: I. Factor structure on an inpatient unit. J Gerontol. (1984) 39:187–93. doi: 10.1093/geronj/39.2.187
42. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The cochrane collaboration's tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
43. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25:603–5. doi: 10.1007/s10654-010-9491-z
44. Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. (2011) 64:401–6. doi: 10.1016/j.jclinepi.2010.07.015
45. Zhang ZJ, Chen YC, Wang HN, Wang HH, Xue YY, Feng SF, et al. Electroconvulsive therapy improves antipsychotic and somnographic responses in adolescents with first-episode psychosis–a case-control study. Schizophr Res. (2012) 137:97–103. doi: 10.1016/j.schres.2012.01.037
46. Kayser S, Bewernick BH, Matusch A, Hurlemann R, Soehle M, Schlaepfer TE. Magnetic seizure therapy in treatment-resistant depression: clinical, neuropsychological and metabolic effects. Psychol Med. (2015) 45:1073–92. doi: 10.1017/S0033291714002244
47. McClintock SM, Tirmizi O, Chansard M, Husain MM. A systematic review of the neurocognitive effects of magnetic seizure therapy. Int Rev Psychiatry. (2011) 23:413–23. doi: 10.3109/09540261.2011.623687
48. Zheng W, Jiang ML, He HB, Li RP, Li QL, Zhang CP, et al. A preliminary study of adjunctive nonconvulsive electrotherapy for treatment-refractory depression. Psychiatr Q. (2021) 92:311–20. doi: 10.1007/s11126-020-09798-3
Keywords: magnetic seizure therapy, schizophrenia, systematic review, neurocognitive function, response
Citation: Zhang XY, Chen HD, Liang WN, Yang XH, Cai DB, Huang X, Huang XB, Liu CY and Zheng W (2022) Adjunctive Magnetic Seizure Therapy for Schizophrenia: A Systematic Review. Front. Psychiatry 12:813590. doi: 10.3389/fpsyt.2021.813590
Received: 12 November 2021; Accepted: 10 December 2021;
Published: 10 January 2022.
Edited by:
Tianhong Zhang, Shanghai Jiao Tong University, ChinaReviewed by:
Yikang Zhu, Shanghai Jiao Tong University, ChinaCopyright © 2022 Zhang, Chen, Liang, Yang, Cai, Huang, Huang, Liu and Zheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wei Zheng, emhlbmd3ZWkwNzAyQDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.