 Heinz Grunze
Heinz Grunze Réka Csehi
Réka Csehi Christoph Born
Christoph Born Ágota Barabássy
Ágota Barabássy- 1Psychiatrie Schwäbisch Hall, Schwäbisch Hall, Germany
- 2Paracelsus Medical University, Nuremberg, Germany
- 3Gedeon Richter Plc, Medical Division, Budapest, Hungary
The dopaminergic system plays a central and decisive role in substance use disorder (SUD), bipolar disorder (BD), and possibly in a subgroup of patients with refractory depression. Common genetic markers and underlying cellular processes, such as kindling, support the close link between these disorders, which is also expressed by the high rate of comorbidity. Although partial dopamine agonists/antagonists acting on D2 and D3 receptors have an established role in treating BD, their usefulness in SUD is less clear. However, dopamine D3 receptors were shown to play a central role in SUD and BD, making D2/D3 partial agonists/antagonists a potential target for both disorders. This narrative review examines whether these substances bear the promise of a future therapeutic approach especially in patients with comorbid BD and SUD.
Introduction
Bipolar disorder (BD) is a complex and serious psychiatric disorder characterized by recurrent mood episodes. Its prevalence is estimated to be at least around 1% in the general population, and it is associated with premature death with a loss of 10–20 years of life attributable to both physical and psychiatric comorbidities (1). Its co-occurrence with other mental illnesses is the norm rather than the exception, especially with substance use disorder (SUD) (2).
Prevalence
The prevalence of SUD in BD population was extensively explored by Hunt et al. (3, 4) who gathered data from clinical settings and national surveys conducted between 1990 and 2015. The prevalence of SUD was found to be more than 30% in community-, and more than 40% in clinical settings. Alcohol use disorder (AUD) was the most prevalent SUD with 20–30% prevalence rates in both community and clinical settings. Among illicit drugs, cannabis was the most commonly abused drug (around 20%), followed by cocaine (around 10%). The findings of these meta-analyses are in line with those of other studies with cannabis use ranking second after AUD (2, 5, 6).
Significance and Consequences of Comorbidity
Both BD and SUD have been associated with detrimental consequences on their own, but the co-occurrence of SUD further complicates the already heterogenous clinical presentation of BD, often masking BD diagnosis and predicting an even worse prognostic outcome for patients (3, 7). Such patients experience more frequent and severe mood destabilizations, increased hospital admissions, accentuated depressive symptoms, an increased likelihood of suicidal behavior and suicide attempts as well as interference with the efficacy of therapeutic medications—either by lowering their mood stabilizing effects or requiring higher doses of the medication to achieve the therapeutic dose (3, 8, 9). Furthermore, earlier mean age of onset was observed for comorbid SUD in BD patients (20.7 years), compared to BD individuals without a lifetime prevalence of SUD (24.0 years), reflecting a significant difference in age of onset in these groups (3). Earlier onset of BD was found to result in a more severe course of illness (10).
Shared Underlying Mechanisms and the Role of the Dopaminergic System and the D3 Receptors
As patients with comorbid SUD and BD present with accentuated severity of symptoms and have worse prognostic outcomes, shared underlying physiological mechanisms of these disorders are implied and several hypotheses were proposed in support of this notion (11).
One mechanism proposed to underlie SUD and BD comorbidity involves “kindling” which refers to the concept that neurons become increasingly sensitized due to repeated disruptions—and increased sensitization makes them more susceptible to interruption (12). Sensitization is observable in both SUD, where individuals progress from occasional to frequent substance use, and BD, where mood becomes increasingly unstable, depressive, and manic episodes alternate with greater frequency and intensity and periods of remission become briefer (13). Thus, the notion of kindling holds that some individuals might be more vulnerable to neuron sensitization, increasing their risk for developing both SUD and BD.
Furthermore, genetic risk factors are known to play a role in the development of both SUD and BD. Individuals with SUD have a greater chance of having a family member with mood disorder than individuals without such family members—and vice versa—suggesting that SUD and BD might share common gene variants that increase the risk for developing both disorders (12).
The “disorder fostering disorder” concept suggests that the pathological effects of BD and SUD might increase the risk for developing the other (12). Patients with BD might look to self-medicate in order to alleviate their symptoms by taking drugs or consuming alcohol. This view implies that having BD increases the risk for developing SUD. However, the reverse is also true, as substance use exacerbates pathophysiological changes in the already dysfunctional neurotransmitter systems or signaling pathways (14).
The concept of allostasis (the process of maintaining homeostasis through the adaptive change of the organism's internal environment) may provide further insights in the understanding of the pathogenetic mechanisms underlying the comorbidity of BD and SUD (15): if BD is assumed to be a disease involving the cumulative build-up of allostatic states, which as a progressive dysregulation of reward circuits is expressed as negative affective states, it may leave BD patients more vulnerable to drug addiction (16). Furthermore, functional neuroimaging studies identified abnormalities of brain networks—the Default Mode Network—in BD and SUD that are possibly involved in the pathophysiology of both disorders and therefore provide evidence for the shared underlying mechanisms (15).
Yet another mechanism proposed to underlie SUD and BD comorbidity concerns the role of the dopaminergic system, which was recognized a long time ago in both BD and SUD. In BD, bipolar depression is characterized by increased striatal dopamine transporter levels, resulting in attenuated dopaminergic function (17). In contrast, increased D2/D3 receptor availability as well as hyper-responsive reward system in the ventral striatum is observed in bipolar mania, leading to heightened dopaminergic neurotransmission (17). In SUD, nearly all neurochemical systems in the brain are involved in the pathophysiology, including the dopaminergic system which has been extensively examined due to its involvement in reward and reinforcement (18). Particularly the D3 receptor system and its significance in addiction sparked interest: firstly, due to its anatomical localization, as D3 receptors are highly expressed in limbic areas that form the “reward” circuitry, therefore implying that they mediate motivation, emotions, and by extension, may be involved in addiction (19). The other pivotal feature of D3 receptors is that they have the highest overall affinity to endogenous dopamine (Ki = 30 nM) among the five dopamine-subtypes (20, 21). Thus, they are the most sensitive to basal concentration (19), indicating greater occupancy of D3 receptors after dopamine-elevating drug administration (most drugs of abuse) in comparison with D1 or D2 receptors (estimated to be 96% vs. 25–27%) (22).
Human positron emission tomography (PET) studies have contributed greatly to bringing light to the dopaminergic abnormalities in addictions, especially related to the D2-like dopamine receptors (D2 and D3), by allowing measurement of receptor occupancy (18). Reduced striatal D2 receptor availability was found in individuals with SUD [including cocaine (23), alcohol (24), and methamphetamine (25)] compared to healthy controls (18). These abnormalities have been linked to behavioral traits relevant to addiction, such as emotional and behavioral impulsivity (26)—which is also a common feature in BD—, but also in response inhibition (27) and relapse after clinical intervention (28). PET studies further discovered blunted dopamine release at D2 receptors in subjects with addiction [including cocaine (29), alcohol (24), and methamphetamine (25)], assumed to be associated with hypoactive dopaminergic state that bolsters drug-seeking behavior (18).
Recent findings, however, have found that unlike D2 receptors, D3 receptors have actually shown an upregulation in human post-mortem (30) and animal studies (18, 31). Despite these in vitro findings, the examination of D3 receptors in humans in vivo was restricted due to the lack of a selective PET ligand. The relatively recent introduction of [11C]-(+)-PHNO—a D3 preferring PET radioligand—has, however, enabled the investigation of D3 receptors in addiction in the human brain in vivo (19, 32). Indeed, PET studies using [11C]-(+)-PHNO confirmed the findings of in vitro studies: D3 receptor availability is heightened in individuals with SUD, and they were shown to be associated with impulsivity (23), drug craving (33), cognitive dysfunction (34), and symptom severity (18).
Thus, evidence suggests that both SUD and BD share similar dopaminergic dysfunctions especially at the D2 and D3 receptors, which shifts the attention toward dopamine modulating agents such as partial agonists acting at the D2/D3 dopamine receptors.
Treatment of BD and SUD
Traditionally, comorbid SUD in BD or other psychiatric illnesses have usually been treated either in parallel, i.e., patients were receiving concurrent treatment for both disorders, but in different programs, or in sequence, i.e., SUD first, BD second (9). Despite extensive evidence highlighting the frequency of the occurrence of SUD in BD, as well as its detrimental impact on the prognosis and treatment outcomes of BD, only a few studies aimed at exploring appropriate treatment options for this subgroup of BD patients, especially in terms of pharmacotherapies (9). Instead, BD has been traditionally treated with mood stabilizers and anticonvulsant agents, or with second-generation antipsychotics (35). For SUD, the need for pharmacological therapy has long been acknowledged, yet adequate therapeutic options are lacking (36). Current medications include (depending on the substance of abuse) buprenorphine, naltrexone, topiramate, varenicline, bupropion, clonidine, and methadone (37). Given antipsychotics' dopamine-stabilizing effects, they were anticipated to reduce craving in SUD, leading researchers to investigate this notion (2). According to a meta-analysis, the antipsychotics investigated in the study (amisulpride, aripiprazole, olanzapine, and quetiapine) did not produce significant reductions in alcohol craving or drinking behavior in patients with primary AUD without comorbidities (38). Aripiprazole, however, was significantly associated with a decrease in the number of drinks as well as heavy drinking days (39). Furthermore, a study involved patients with comorbid BD/schizoaffective disorder and SUD who were switched to aripiprazole (40). Patients with comorbid AUD showed reduced alcohol craving and spent less dollars on alcohol, while patients with cocaine use disorder showed a decrease in cocaine craving, but not cocaine use (40). Quetiapine, an atypical antipsychotic with a very low affinity for D2/3 receptors (41), was further investigated whether it relieves alcohol craving similarly to aripiprazole (42). Results, however, did not demonstrate efficacy in a randomized controlled trial for alcohol use measures in patients with comorbid BD and AUD (42).
In light of the shared underlying mechanisms, integrated treatment options—addressing both disorders by the same team at the same time—need to be established for this patient population (9), and the most likely drug candidates to treat with seem to be partial agonists acting at D2/D3 dopamine receptors.
Dopamine D2/D3 Partial Agonists in the Treatment of BD and SUD
The currently known and markedly available dopamine D2/D3 partial agonists are aripiprazole, cariprazine, and brexpiprazole (43). Some older compounds (such as bifeprunox), as well as some newer compounds in development (e.g., OSU-6162) also exist and provide valuable information to the understanding of the efficacy of partial agonists in BD and SUD (44, 45).
The efficacy of D2/D3 partial agonists in SUD is not well-examined and much of the data comes from animal studies. As such, one animal model has investigated the anti-abuse effects of cariprazine, aripiprazole, and bifeprunox in cocaine addiction in rats (44). All compounds succeeded at reducing the rewarding effects of cocaine—as indicated by enhanced self-administration of the drug—as well as prevented relapse to cocaine seeking following a period of complete withdrawal from cocaine and its related cues (44). Equipotent effects of cariprazine and bifeprunox were observed, 20 times more potent than that of aripiprazole (44). The beneficial effects of partial agonists in animal studies were also observed in alcohol abuse: the compound OSU-6162 effectively reduced self-administration, withdrawal and reinstatement in rats (45), and aripiprazole lessened the acute stimulant effects of alcohol in mice (46, 47). Furthermore, one study investigated the effect of a D3 partial agonist, CJB090, in methamphetamine addiction in rats, where the investigational drug yielded reductions in methamphetamine self-administration (fixed ratio schedule) and its excessive intake in a group of rats with extended access to methamphetamine (48). Human data in SUD is scarce, and little information is available.
The efficacy of D2/D3 partial agonists in BD has been well-examined for the currently available compounds with different findings. While cariprazine proved to be efficacious in both bipolar mania and bipolar depression (49) [3–6 mg in bipolar mania (50) and 1.5–3 mg in bipolar depression (51)], studies of aripiprazole confirmed efficacy in bipolar mania only (52). Brexpiprazole studies in bipolar mania were unsuccessful (53), and, following a positive pilot trial (54), a RCT in bipolar depression is ongoing (55). Human PET studies with cariprazine (56, 57), aripiprazole (58), and brexpiprazole (58) have pointed to the difference potentially explaining these findings: while all three compounds were able to occupy the D2 receptors in the brain, only cariprazine was able to sufficiently occupy the D3 receptors as well [(59); Figure 1]. Additionally, a clinical trial has been initiated to further study the dopamine D3 receptor occupancy of cariprazine (1.5 vs. 3 mg/day) in patients with unmedicated bipolar depression (60).
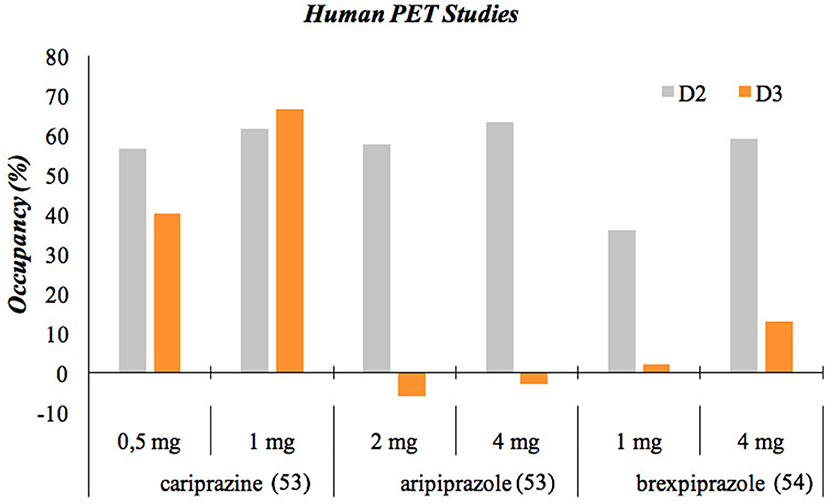
Figure 1. Occupancy of D2 and D3 receptors of antipsychotics. The cariprazine and aripiprazole data come from a PET study involving healthy volunteers that aimed to assess the D3 receptor occupancy of cariprazine and aripiprazole at doses that attain similar D2 receptor occupancy by both drugs. This was assessed using two different methods, and the data presented here is the average of the outcome of these methods. The brexpiprazole data comes from a PET study involving schizophrenia patients.
Cariprazine has in fact a preferential binding to D3 receptors, and its binding is stronger than that of any other antipsychotics and even dopamine itself (61). Given dopamine's very high affinity for the D3 receptors, the low affinities of antipsychotics, with the exception of cariprazine, make them unable to block the D3 receptors in the presence of dopamine in the living brain (62). This means that only cariprazine is able to exhibit the effects usually associated with D3 partial agonism, which are improvements in negative, cognitive and depressive symptoms as well as in motivation and reward (49). Given the increasingly acknowledged role of D3 in SUD along with BD, cariprazine's high affinity for D3 receptors makes it an appropriate candidate for the treatment of comorbid BD with SUD.
Two clinical trials have been initiated to investigate cariprazine's efficacy in SUD, although results are not available yet. An investigator-initiated trial aims to explore cariprazine's effects on the brain and behavior in cocaine use disorder in a phase II, randomized, single-blind, placebo-controlled study using fMRI (1.5 vs. 3 mg/day) (63). Furthermore, a phase IIa, randomized, placebo-controlled pilot study was designed to explore how low-dose cariprazine (1.5 mg/day) affects cocaine use in medically stable patients with comorbid opioid use disorder who have already been taking buprenorphine/naloxone at a stable dose (64). Additionally, scarce data is available from case reports as summarised in Table 1. Evidence for the effects of several partial agonists in SUD, BD, and BD or related psychotic disorders and comorbid SUD is depicted in the Supplementary Table 1, which also includes two additional recent case reports on cariprazine treatment in major psychiatric disorders with comorbid SUD (67).
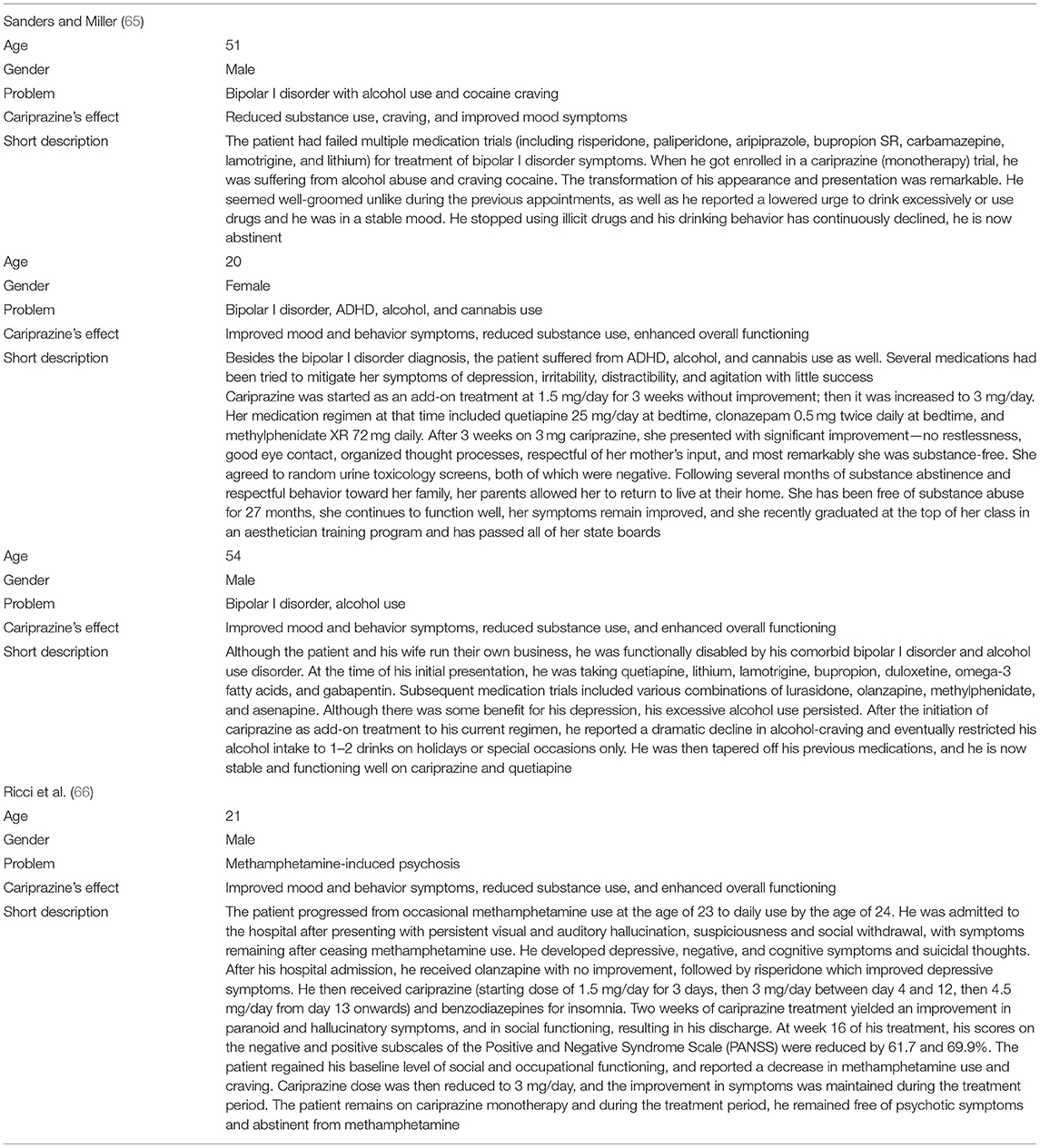
Table 1. Cariprazine case reports.
Conclusion
So far, pharmacological treatment concepts hardly considered the joint treatment of SUD and BD, which seem to share a common action on dopamine D2 and D3 receptors. An ideal integrated pharmacological treatment would therefore address both disorders through the D2 and D3 receptors, in addition to other therapeutic interventions, such as psychotherapy. Since cariprazine has shown to exert effects on both D2 and D3 receptors (partial agonist effect) next to serotonin receptors, as well as has well-established efficacy in bipolar I disorder, it is believed to be a potential treatment option for this patient population. Data for this assumption comes from animal studies and case reports, however, further studies are needed to validate this rationale-based assumption.
Author Contributions
HG, RC, CB, and ÁB contributed to developing the concept of the manuscript. RC wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
Gedeon Richter provided funds for the open access publication fees.
Conflict of Interest
RC and ÁB are employees of Gedeon Richter Plc.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.803208/full#supplementary-material
References
1. McIntyre RS, Berk M, Brietzke E, Goldstein BI, López-Jaramillo C, Kessing LV, et al. Bipolar disorders. Lancet. (2020) 396:1841–56. doi: 10.1016/s0140-6736(20)31544-0
2. Grunze H, Schaefer M, Scherk H, Born C, Preuss UW. Comorbid bipolar and alcohol use disorder—a therapeutic challenge. Front Psychiatry. (2021) 12:660432. doi: 10.3389/fpsyt.2021.660432
3. Hunt GE, Malhi GS, Cleary M, Lai HM, Sitharthan T. Prevalence of comorbid bipolar and substance use disorders in clinical settings, 1990-2015: systematic review and meta-analysis. J Affect Disord. (2016) 206:331–49. doi: 10.1016/j.jad.2016.07.011
4. Hunt GE, Malhi GS, Cleary M, Lai HM, Sitharthan T. Comorbidity of bipolar and substance use disorders in national surveys of general populations, 1990-2015: systematic review and meta-analysis. J Affect Disord. (2016) 206:321–30. doi: 10.1016/j.jad.2016.06.051
5. Pinto JV, Medeiros LS, Santana da Rosa G, Santana de Oliveira CE, Crippa JAS, Passos IC, et al. The prevalence and clinical correlates of cannabis use and cannabis use disorder among patients with bipolar disorder: a systematic review with meta-analysis and meta-regression. Neurosci Biobehav Rev. (2019) 101:78–84. doi: 10.1016/j.neubiorev.2019.04.004
6. Lucatch AM, Coles AS, Hill KP, George TP. Cannabis and mood disorders. Curr Addict Rep. (2018) 5:336–45. doi: 10.1007/s40429-018-0214-y
7. Frye MA, Altshuler LL, McElroy SL, Suppes T, Keck PE, Denicoff K, et al. Gender differences in prevalence, risk, and clinical correlates of alcoholism comorbidity in bipolar disorder. Am J Psychiatry. (2003) 160:883–9. doi: 10.1176/appi.ajp.160.5.883
8. Salloum IM, Thase ME. Impact of substance abuse on the course and treatment of bipolar disorder. Bipolar Disord. (2000) 2(3 Pt 2):269–80. doi: 10.1034/j.1399-5618.2000.20308.x
9. Levin FR, Hennessy G. Bipolar disorder and substance abuse. Biol Psychiatry. (2004) 56:738–48. doi: 10.1016/j.biopsych.2004.05.008
10. Post RM, Leverich GS, Kupka RW, Keck PE Jr., McElroy SL, Altshuler LL, et al. Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood. J Clin Psychiatry. (2010) 71:864–72. doi: 10.4088/JCP.08m04994yel
11. Swann AC. The strong relationship between bipolar and substance-use disorder. Ann N Y Acad Sci. (2010) 1187:276–93. doi: 10.1111/j.1749-6632.2009.05146.x
12. Quello SB, Brady KT, Sonne SC. Mood disorders and substance use disorder: a complex comorbidity. Sci Pract Perspect. (2005) 3:13–21. doi: 10.1151/spp053113
13. Post RM, Rubinow DR, Ballenger JC. Conditioning and sensitisation in the longitudinal course of affective illness. Br J Psychiatry. (1986) 149:191–201. doi: 10.1192/bjp.149.2.191
14. Markou A, Kosten TR, Koob GF. Neurobiological similarities in depression and drug dependence: a self-medication hypothesis. Neuropsychopharmacology. (1998) 18:135–74. doi: 10.1016/s0893-133x(97)00113-9
15. Di Nicola M, Pepe M, Modica M, Lanzotti P, Panaccione I, Moccia L, et al. Mixed states in patients with substance and behavioral addictions. Psychiatr Clin North Am. (2020) 43:127–37. doi: 10.1016/j.psc.2019.10.012
16. Pettorruso M, De Risio L, Di Nicola M, Martinotti G, Conte G, Janiri L. Allostasis as a conceptual framework linking bipolar disorder and addiction. Front Psychiatry. (2014) 5:173. doi: 10.3389/fpsyt.2014.00173
17. Ashok AH, Marques TR, Jauhar S, Nour MM, Goodwin GM, Young AH, et al. The dopamine hypothesis of bipolar affective disorder: the state of the art and implications for treatment. Mol Psychiatry. (2017) 22:666–79. doi: 10.1038/mp.2017.16
18. Boileau I, Nakajima S, Payer D. Imaging the D3 dopamine receptor across behavioral and drug addictions: positron emission tomography studies with [(11)C]-(+)-PHNO. Eur Neuropsychopharmacol. (2015) 25:1410–20. doi: 10.1016/j.euroneuro.2015.06.002
19. Payer D, Balasubramaniam G, Boileau I. What is the role of the D3 receptor in addiction? A mini review of PET studies with [(11)C]-(+)-PHNO. Prog Neuropsychopharmacol Biol Psychiatry. (2014) 52:4–8. doi: 10.1016/j.pnpbp.2013.08.012
20. Lévesque D, Diaz J, Pilon C, Martres MP, Giros B, Souil E, et al. Identification, characterization, and localization of the dopamine D3 receptor in rat brain using 7-[3H]hydroxy-N,N-di-n-propyl-2-aminotetralin. Proc Natl Acad Sci USA. (1992) 89:8155–9. doi: 10.1073/pnas.89.17.8155
21. Sokoloff P, Giros B, Martres MP, Andrieux M, Besancon R, Pilon C, et al. Localization and function of the D3 dopamine receptor. Arzneimittelforschung. (1992) 42:224–30.
22. Richtand NM. Behavioral sensitization, alternative splicing, and d3 dopamine receptor-mediated inhibitory function. Neuropsychopharmacology. (2006) 31:2368–75. doi: 10.1038/sj.npp.1301163
23. Payer DE, Behzadi A, Kish SJ, Houle S, Wilson AA, Rusjan PM, et al. Heightened D3 dopamine receptor levels in cocaine dependence and contributions to the addiction behavioral phenotype: a positron emission tomography study with [11C]-+-PHNO. Neuropsychopharmacology. (2014) 39:311–8. doi: 10.1038/npp.2013.192
24. Martinez D, Gil R, Slifstein M, Hwang DR, Huang Y, Perez A, et al. Alcohol dependence is associated with blunted dopamine transmission in the ventral striatum. Biol Psychiatry. (2005) 58:779–86. doi: 10.1016/j.biopsych.2005.04.044
25. Volkow ND, Chang L, Wang GJ, Fowler JS, Ding YS, Sedler M, et al. Low level of brain dopamine D2 receptors in methamphetamine abusers: association with metabolism in the orbitofrontal cortex. Am J Psychiatry. (2001) 158:2015–21. doi: 10.1176/appi.ajp.158.12.2015
26. Lee B, London ED, Poldrack RA, Farahi J, Nacca A, Monterosso JR, et al. Striatal dopamine d2/d3 receptor availability is reduced in methamphetamine dependence and is linked to impulsivity. J Neurosci. (2009) 29:14734–40. doi: 10.1523/jneurosci.3765-09.2009
27. Ghahremani DG, Tabibnia G, Monterosso J, Hellemann G, Poldrack RA, London ED. Effect of modafinil on learning and task-related brain activity in methamphetamine-dependent and healthy individuals. Neuropsychopharmacology. (2011) 36:950–9. doi: 10.1038/npp.2010.233
28. Wang GJ, Smith L, Volkow ND, Telang F, Logan J, Tomasi D, et al. Decreased dopamine activity predicts relapse in methamphetamine abusers. Mol Psychiatry. (2012) 17:918–25. doi: 10.1038/mp.2011.86
29. Martinez D, Broft A, Foltin RW, Slifstein M, Hwang DR, Huang Y, et al. Cocaine dependence and d2 receptor availability in the functional subdivisions of the striatum: relationship with cocaine-seeking behavior. Neuropsychopharmacology. (2004) 29:1190–202. doi: 10.1038/sj.npp.1300420
30. Staley JK, Mash DC. Adaptive increase in D3 dopamine receptors in the brain reward circuits of human cocaine fatalities. J Neurosci. (1996) 16:6100–6. doi: 10.1523/jneurosci.16-19-06100.1996
31. Neisewander JL, Fuchs RA, Tran-Nguyen LT, Weber SM, Coffey GP, Joyce JN. Increases in dopamine D3 receptor binding in rats receiving a cocaine challenge at various time points after cocaine self-administration: implications for cocaine-seeking behavior. Neuropsychopharmacology. (2004) 29:1479–87. doi: 10.1038/sj.npp.1300456
32. Wilson AA, McCormick P, Kapur S, Willeit M, Garcia A, Hussey D, et al. Radiosynthesis and evaluation of [11C]-(+)-4-propyl-3,4,4a,5,6,10b-hexahydro-2H-naphtho[1,2-b][1,4]oxazin-9-ol as a potential radiotracer for in vivo imaging of the dopamine D2 high-affinity state with positron emission tomography. J Med Chem. (2005) 48:4153–60. doi: 10.1021/jm050155n
33. Boileau I, Payer D, Houle S, Behzadi A, Rusjan PM, Tong J, et al. Higher binding of the dopamine D3 receptor-preferring ligand [11C]-(+)-propyl-hexahydro-naphtho-oxazin in methamphetamine polydrug users: a positron emission tomography study. J Neurosci. (2012) 32:1353–9. doi: 10.1523/jneurosci.4371-11.2012
34. Nakajima S, Gerretsen P, Takeuchi H, Caravaggio F, Chow T, Le Foll B, et al. The potential role of dopamine D3 receptor neurotransmission in cognition. Eur Neuropsychopharmacol. (2013) 23:799–813. doi: 10.1016/j.euroneuro.2013.05.006
35. Rhee TG, Olfson M, Nierenberg AA, Wilkinson ST. 20-year trends in the pharmacologic treatment of bipolar disorder by psychiatrists in outpatient care settings. Am J Psychiatry. (2020) 177:706–15. doi: 10.1176/appi.ajp.2020.19091000
36. Forray A, Sofuoglu M. Future pharmacological treatments for substance use disorders. Br J Clin Pharmacol. (2014) 77:382–400. doi: 10.1111/j.1365-2125.2012.04474.x
37. Elias D, Kleber HD. Minding the brain: the role of pharmacotherapy in substance-use disorder treatment. Dialogues Clin Neurosci. (2017) 19:289–97. doi: 10.31887/DCNS.2017.19.3/hkleber
38. Kishi T, Sevy S, Chekuri R, Correll CU. Antipsychotics for primary alcohol dependence: a systematic review and meta-analysis of placebo-controlled trials. J Clin Psychiatry. (2013) 74:e642–54. doi: 10.4088/JCP.12r08178
39. Anton RF, Kranzler H, Breder C, Marcus RN, Carson WH, Han J. A randomized, multicenter, double-blind, placebo-controlled study of the efficacy and safety of aripiprazole for the treatment of alcohol dependence. J Clin Psychopharmacol. (2008) 28:5–12. doi: 10.1097/jcp.0b013e3181602fd4
40. Brown ES, Jeffress J, Liggin JD, Garza M, Beard L. Switching outpatients with bipolar or schizoaffective disorders and substance abuse from their current antipsychotic to aripiprazole. J Clin Psychiatry. (2005) 66:756–60. doi: 10.4088/jcp.v66n0613
41. Vernaleken I, Janouschek H, Raptis M, Hellmann S, Veselinovic T, Bröcheler A, et al. Dopamine D2/3 receptor occupancy by quetiapine in striatal and extrastriatal areas. Int J Neuropsychopharmacol. (2010) 13:951–60. doi: 10.1017/s1461145710000374
42. Brown ES, Garza M, Carmody TJ. A randomized, double-blind, placebo-controlled add-on trial of quetiapine in outpatients with bipolar disorder and alcohol use disorders. J Clin Psychiatry. (2008) 69:701–5. doi: 10.4088/jcp.v69n0502
43. Citrome L. The ABC's of dopamine receptor partial agonists - aripiprazole, brexpiprazole and cariprazine: the 15-min challenge to sort these agents out. Int J Clin Pract. (2015) 69:1211–20. doi: 10.1111/ijcp.12752
44. Román V, Gyertyán I, Sághy K, Kiss B, Szombathelyi Z. Cariprazine (RGH-188), a D3-preferring dopamine D3/D2 receptor partial agonist antipsychotic candidate demonstrates anti-abuse potential in rats. Psychopharmacology. (2013) 226:285–93. doi: 10.1007/s00213-012-2906-7
45. Steensland P, Fredriksson I, Holst S, Feltmann K, Franck J, Schilström B, et al. The monoamine stabilizer (-)-OSU6162 attenuates voluntary ethanol intake and ethanol-induced dopamine output in nucleus accumbens. Biol Psychiatry. (2012) 72:823–31. doi: 10.1016/j.biopsych.2012.06.018
46. Jerlhag E. The antipsychotic aripiprazole antagonizes the ethanol- and amphetamine-induced locomotor stimulation in mice. Alcohol. (2008) 42:123–7. doi: 10.1016/j.alcohol.2007.11.004
47. Moreira FA, Dalley JW. Dopamine receptor partial agonists and addiction. Eur J Pharmacol. (2015) 752:112–5. doi: 10.1016/j.ejphar.2015.02.025
48. Orio L, Wee S, Newman AH, Pulvirenti L, Koob GF. The dopamine D3 receptor partial agonist CJB090 and antagonist PG01037 decrease progressive ratio responding for methamphetamine in rats with extended-access. Addict Biol. (2010) 15:312–23. doi: 10.1111/j.1369-1600.2010.00211.x
49. Stahl SM, Laredo S, Morrissette DA. Cariprazine as a treatment across the bipolar I spectrum from depression to mania: mechanism of action and review of clinical data. Ther Adv Psychopharmacol. (2020) 10:2045125320905752. doi: 10.1177/2045125320905752
50. Ketter TA, Sachs GS, Durgam S, Lu K, Starace A, Laszlovszky I, et al. The safety and tolerability of cariprazine in patients with manic or mixed episodes associated with bipolar I disorder: A 16-week open-label study. J Affect Disord. (2018) 225:350–6. doi: 10.1016/j.jad.2017.08.040
51. McIntyre RS, Suppes T, Earley W, Patel M, Stahl SM. Cariprazine efficacy in bipolar I depression with and without concurrent manic symptoms: post hoc analysis of 3 randomized, placebo-controlled studies. CNS Spectr. (2020) 25:502–10. doi: 10.1017/s1092852919001287
52. Li DJ, Tseng PT, Stubbs B, Chu CS, Chang HY, Vieta E, et al. Efficacy, safety and tolerability of aripiprazole in bipolar disorder: an updated systematic review and meta-analysis of randomized controlled trials. Prog Neuropsychopharmacol Biol Psychiatry. (2017) 79(Pt B):289–301. doi: 10.1016/j.pnpbp.2017.06.023
53. Vieta E, Sachs G, Chang D, Hellsten J, Brewer C, Peters-Strickland T, et al. Two randomized, double-blind, placebo-controlled trials and one open-label, long-term trial of brexpiprazole for the acute treatment of bipolar mania. J Psychopharmacol. (2021) 35:971–82. doi: 10.1177/0269881120985102
54. Brown ES, Khaleghi N, Van Enkevort E, Ivleva E, Nakamura A, Holmes T, et al. A pilot study of brexpiprazole for bipolar depression. J Affect Disord. (2019) 249:315–8. doi: 10.1016/j.jad.2019.02.056
55. NCT04569448. Brexpiprazole Treatment for Bipolar I Depression. (2020). Available online at: https://clinicaltrials.gov/ct2/show/NCT04569448 (accessed October 15, 2020).
56. Girgis RR, Slifstein M, D'Souza D, Lee Y, Periclou A, Ghahramani P, et al. Preferential binding to dopamine D3 over D2 receptors by cariprazine in patients with schizophrenia using PET with the D3/D2 receptor ligand [(11)C]-(+)-PHNO. Psychopharmacology. (2016) 233:3503–12. doi: 10.1007/s00213-016-4382-y
57. Girgis RR, Abi-Dargham A, Slifstein M, Chen L, Periclou A, Adham N, et al. In vivo dopamine D3 and D2 receptor occupancy profile of cariprazine versus aripiprazole: a PET study. Neuropsychopharmacology. (2017) 42:S595.
58. Girgis RR, Forbes A, Abi-Dargham A, Slifstein M. A positron emission tomography occupancy study of brexpiprazole at dopamine D(2) and D(3) and serotonin 5-HT(1A) and 5-HT(2A) receptors, and serotonin reuptake transporters in subjects with schizophrenia. Neuropsychopharmacology. (2020) 45:786–92. doi: 10.1038/s41386-019-0590-6
59. Laszlovszky I, Barabássy Á, Németh G. Cariprazine, a broad-spectrum antipsychotic for the treatment of schizophrenia: pharmacology, efficacy, and safety. Adv Ther. (2021) 38:3652–73. doi: 10.1007/s12325-021-01797-5
60. NCT05060549. Dopamine D3 Receptor Occupancy in Bipolar Depression. (2021). Available online at: https://clinicaltrials.gov/ct2/show/NCT05060549 (accessed October 15, 2021).
61. Kiss B, Horváth A, Némethy Z, Schmidt E, Laszlovszky I, Bugovics G, et al. Cariprazine (RGH-188), a dopamine D(3) receptor-preferring, D(3)/D(2) dopamine receptor antagonist-partial agonist antipsychotic candidate: in vitro and neurochemical profile. J Pharmacol Exp Ther. (2010) 333:328–40. doi: 10.1124/jpet.109.160432
62. Stahl SM. Mechanism of action of cariprazine. CNS Spectr. (2016) 21:123–7. doi: 10.1017/s1092852916000043
63. NCT03430544. Cariprazine Effects on Brain and Behavior in Cocaine Use Disorder. (2018). Available online at: https://clinicaltrials.gov/ct2/show/NCT03430544 (accessed October 15, 2021).
64. NCT05063201. Cariprazine for Comorbid Cocaine and Opioid Use Disorder. (2021). Available online at: https://clinicaltrials.gov/ct2/show/NCT05063201 (accessed October 15, 2021).
65. Sanders LO, Miller JJ. Cariprazine may decrease substance abuse in patients with bipolar I disorder. Psychiatr Times. (2019) 36:10–3.
66. Ricci V, Di Salvo G, Maina G. Remission of persistent methamphetamine-induced psychosis after cariprazine therapy: presentation of a case report. J Addict Dis. (2021). doi: 10.1080/10550887.2021.1945398. [Epub ahead of print].
Keywords: substance use disorder (SUD), cariprazine, psychopharmacotherapy, partial agonist, antipsychotic, bipolar disorder
Citation: Grunze H, Csehi R, Born C and Barabássy Á (2021) Reducing Addiction in Bipolar Disorder via Hacking the Dopaminergic System. Front. Psychiatry 12:803208. doi: 10.3389/fpsyt.2021.803208
Received: 27 October 2021; Accepted: 23 November 2021;
Published: 14 December 2021.
Edited by:
Agata Szulc, Medical University of Warsaw, PolandReviewed by:
Marco Di Nicola, Catholic University of the Sacred Heart, ItalyCopyright © 2021 Grunze, Csehi, Born and Barabássy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Réka Csehi, Y3NlaGlyQHJpY2h0ZXIuaHU=