 Filippo Cantù1
Filippo Cantù1 Giandomenico Schiena2
Giandomenico Schiena2 Domenico Sciortino1Lorena Di Consoli2Giuseppe Delvecchio2
Domenico Sciortino1Lorena Di Consoli2Giuseppe Delvecchio2 Eleonora Maggioni2*
Eleonora Maggioni2* Paolo Brambilla1,2
Paolo Brambilla1,2- 1Department of Pathophysiology and Transplantation, University of Milan, Milan, Italy
- 2Department of Neurosciences and Mental Health, Fondazione Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) Ca' Granda Ospedale Maggiore Policlinico, Milan, Italy
Background: Depressive episodes, especially when resistant to pharmacotherapy, are a hard challenge to face for clinicians and a leading cause of disability worldwide. Neuromodulation has emerged as a potential therapeutic option for treatment-resistant depression (TRD), in particular transcranial magnetic stimulation (TMS). In this article, we present a case series of six patients who received TMS with an accelerated intermittent theta-burst stimulation (iTBS) protocol in a public healthcare setting.
Methods: We enrolled a total number of six participants, affected by a treatment-resistant depressive episode, in either Major Depressive Disorder (MDD) or Bipolar Disorder (BD). Patients underwent an accelerated iTBS protocol, targeted to the left dorsolateral prefrontal cortex (DLPFC), 3-week-long, with a total of 6 days of overall stimulation. On each stimulation day, the participants received 3 iTBS sessions, with a 15-min pause between them. Patients were assessed by the Hamilton Rating Scale for Depression (HAM-D), the Montgomery-Asberg Depression Rating Scale (MADRS), the Hamilton Rating Scale for Anxiety (HAM-A), and the Mania Rating Scale (MRS). At baseline (T0), at the end of the second week (T1), and at the end of the cycle of stimulation (T2).
Results: The rANOVA (repeated Analysis of Variance) statistics showed no significant effect of time on the rating scale scores, with a slight decrease in MADRS scores and a very slight increase in HAM-A and HAM-D scores. No manic symptoms emerged during the entire protocol.
Conclusions: Although accelerated iTBS might be considered a less time-consuming strategy for TMS administration, useful in a public healthcare setting, our results in a real-word six-patient population with TRD did not show a significant effect. Further studies on wider samples are needed to fully elucidate the potential of accelerated iTBS protocols in treatment-resistant depression.
Introduction
Depressive episodes, either in Major Depressive Disorder (MDD) or in Bipolar Disorder (BD), are recognized as leading causes of disability worldwide (1, 2), having a significant economic and social burden (3). Although numerous therapeutic approaches are currently available for depressive episodes, it is estimated that more than 30% of patients affected by MDD fail to respond to pharmacological therapy (4–6), and up to 40% of patients with bipolar depression are classified as non-responders (7, 8).
Clinicians are frequently forced to manage treatment-resistant depression (TRD), which is usually defined as the failure to respond to at least two pharmacological trials at an adequate dose for at least 6 weeks (5, 9). When a depressive episode appears in the context of a Bipolar Disorder, resistance is defined as the failure to respond to at least two separate monotherapeutic trials at an adequate dose for at least 8 weeks, or one monotherapy with one combination treatment (8).
In this scenario, neuromodulation has emerged as a potential therapeutic option. Among neuromodulation techniques, repetitive Transcranial Magnetic Stimulation (rTMS) is the most commonly employed. It induces an electrical current in a targeted region of the brain through a magnetic field generated by a coil, positioned on the scalp (10). rTMS delivers trains of stimuli at high frequencies (i.e., more than 5 Hz) or low frequencies (i.e., <5 Hz), which are thought to exert excitatory or inhibitory effects on the underlying cortex, respectively (11).
A specific way of delivering rTMS is Theta Burst Stimulation (TBS), which uses triplets of pulses (i.e., bursts) at high frequency (in the 30–50 Hz range), with an inter-burst interval of 200 ms (5 Hz). TBS can be performed using continuous (cTBS) protocols, which reduce the excitability of the underlying cerebral cortex, or with intermittent protocols (iTBS), which have enhancing properties (10, 12). Theta rhythms facilitate long-term potentiation (13–16), thus TBS protocols are thought to induce more rapid and long-lasting effects on synaptic plasticity than conventional rTMS (17). Recently, the non-inferiority of iTBS compared to excitatory rTMS has been demonstrated in treating depressive episodes in MDD (18). Moreover, TBS protocols last 3 min, conventional 10 Hz rTMS sessions 37.5 min (19). Therefore, TBS seems to be more advantageous in terms of cost-utility (18) and appears of particular interest in public healthcare settings, where these issues are crucial.
Accelerated TMS (aTMS) is another strategy to improve the conventional TMS protocols. It consists of delivering multiple sessions on the same day, to condense the overall stimulation time and accelerate the clinical response (20). To date, aTMS has shown encouraging results, as reported by a recent meta-analysis (21).
Combining the two abovementioned strategies, the use of TBS in an accelerated protocol might be an option in order to further optimize the cost-utility of rTMS (4, 22). Indeed, a recent accelerated iTBS protocol, improved by the use of neuronavigation, has shown promising results in TRD (23).
In this case-series, we presented and discussed the effectiveness of an accelerated iTBS protocol employed in a group of six real-world patients with TRD recruited in public service.
Materials and Methods
Participants
We enrolled a total number of six participants, affected by a depressive episode, either in MDD or in BD, diagnosed according to the Diagnostic and Statistical Manual fifth edition (DSM-5) criteria. Each patient was evaluated by a psychiatrist, who collected a detailed medical history and performed a Structured Clinical Interview for DSM, clinical version (SCID-CV) before enrolment. The patients were recruited in the outpatient services of the Psychiatry Unit of the Department of Neurosciences and Mental Health at Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Milan, Italy. Participants before their enrolment signed a written informed consent.
Inclusion and Exclusion Criteria
The inclusion criteria were: (a) age: between 21 and 70 years; (b) right-handedness; (c) current depressive episode according to DSM-5 criteria, either in MDD or in BD; (d) no pharmacological change in the last 4 weeks before the beginning of the stimulation cycle; (e) pharmacological resistance (i.e., at least two adequate trials of antidepressants in MDD); (f) at least two separate monotherapeutic trials, or one monotherapy with one combination treatment, in BD.
The exclusion criteria were: (a) diagnosis of schizophrenia or other psychotic disorders; (b) diagnosis of neurological disorders; (c) diagnosis of substance use disorder in the last 6 months, according to DSM-5 criteria; (d) contraindications to TMS according to the Consensus Recommendations for the safe and effective application of rTMS (24).
Protocol
The study started in October 2019 and ended in October 2020. TMS stimulation was delivered using an STM9000 Magnetic Stimulator (ATES Medical Device, Italy) with a 70 mm butterfly cooled coil.
Accelerated iTBS was delivered to the left dorsolateral prefrontal cortex (DLPFC), in a 3-week protocol, with 3 days of stimulation during the first week, 2 days of stimulation during the second week, and 1 day of stimulation in the last one, for a total of 6 days of stimulation. A total of 18 stimulation sessions were performed. On each stimulation day, the participants received 3 iTBS sessions, with a 15-min pause between them. This procedure was similar to an accelerated rTMS protocol demonstrated to be as effective as the standard rTMS protocol in a recent study (20).
The site of stimulation was found 5 cm anterior to the site of motor threshold (MT) determination, in a parasagittal plane. We delivered, at 80% of the motor threshold (MT), triplet 30 Hz bursts, repeated at 5 Hz; 2 s on and 12.3 s off; 600 pulses per session, 1,800 pulses per day of stimulation. All these parameters were set according to international safety guidelines (25).
The protocol was approved by the local Ethics Committee.
Rating Scales
Clinical evaluation was performed by means of the following scales: (a) Hamilton Rating Scale for Depression [HAM-D; (26)]; (b) Montgomery-Asberg Depression Rating Scale [MADRS; (27)]; (c) Hamilton Rating Scale for Anxiety [HAM-A; (28)]; (d) Mania Rating Scale [MRS; (29)].
The rating scales were administered at baseline (T0), at the end of the second week (T1), and at the end of the cycle of stimulation (T2). The MRS was mainly used as a clinical tool to monitor possible switches to manic or hypomanic episodes.
In order to avoid interfering factors, pharmacotherapy was implemented and maintained during the whole treatment.
Data Analysis
The iTBS protocol effectiveness was assessed (i) at the subject level, by qualitatively comparing the rating scale scores over time, (ii) at the group-level, by quantitatively comparing the rating scale scores at different time points. In (ii), for each rating scale, a model with time as within-subject factor and the intercept as between-subject factor was fitted to the multiple scale measurements per subject (response variables). The model was interrogated through a repeated-measures analysis of variance (rANOVA). In the event of significant effects of time on the rating scale scores (p < 0.05), post-hoc pairwise time comparisons were performed.
Results
The sample demographic and longitudinal clinical characteristics are reported in Table 1. Our group of patients was composed of four women and two men. Four patients were affected by MDD, two by BD II, with a mean age of 58.3 years and a standard deviation of 10.06 years. Two patients were taking mood stabilizing drugs (lithium or lamotrigine), five patients an atypical antipsychotic (quetiapine), two patients a second antidepressant, and two patients benzodiazepines.
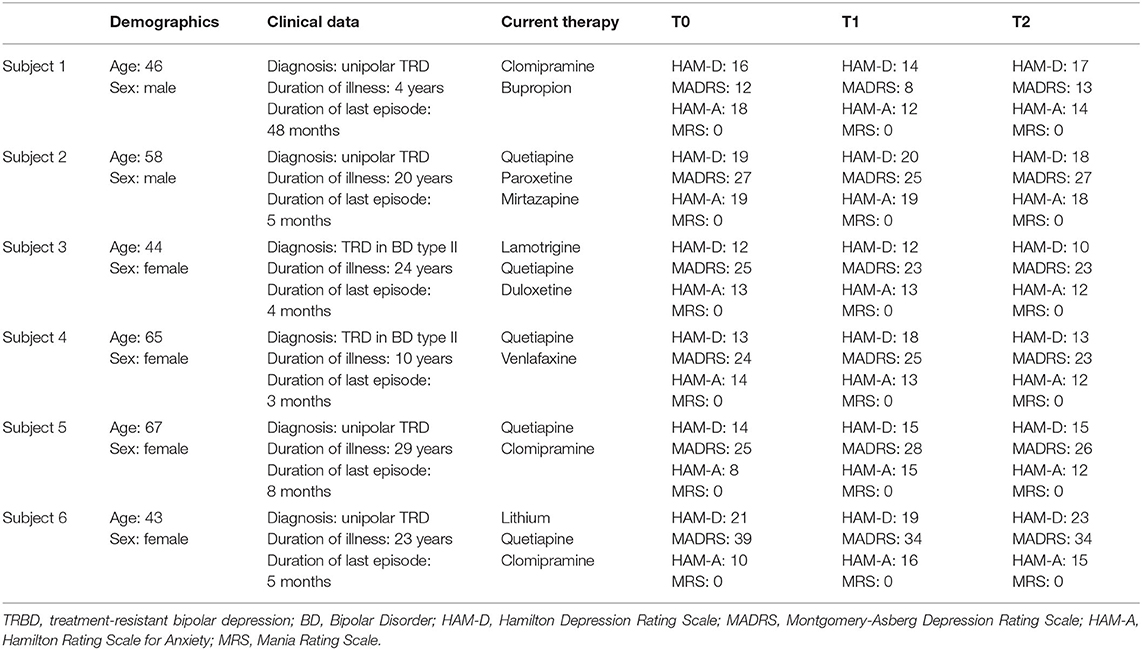
Table 1. Demographic, clinical, and pharmacological variables of each subject.
The subject-level HAM-D, HAM-A, and MADRS scores from baseline to follow-up are shown in the bar diagrams of Figure 1. The group-level score distributions, shown in Figure 2, indicate a large inter-individual variability of the effects of accelerated iTBS on depressive and anxiety symptoms over time. The rANOVA statistics showed no significant effects of the time factor on the rating scale scores (HAM-D: F = 0.115, p = 0.749, HAM-A: F = 0.270, p = 0.626, MADRS: F = 0.981, p = 0.367), therefore no post-hoc pairwise comparisons (T0 vs. T1, T0 vs. T2, etc.) were performed. From T0 to T2, a slight decrease in MADRS scores was observed, accompanied by very slight increases in HAM-A and HAM-D scores. No manic symptoms appeared during the entire protocol.
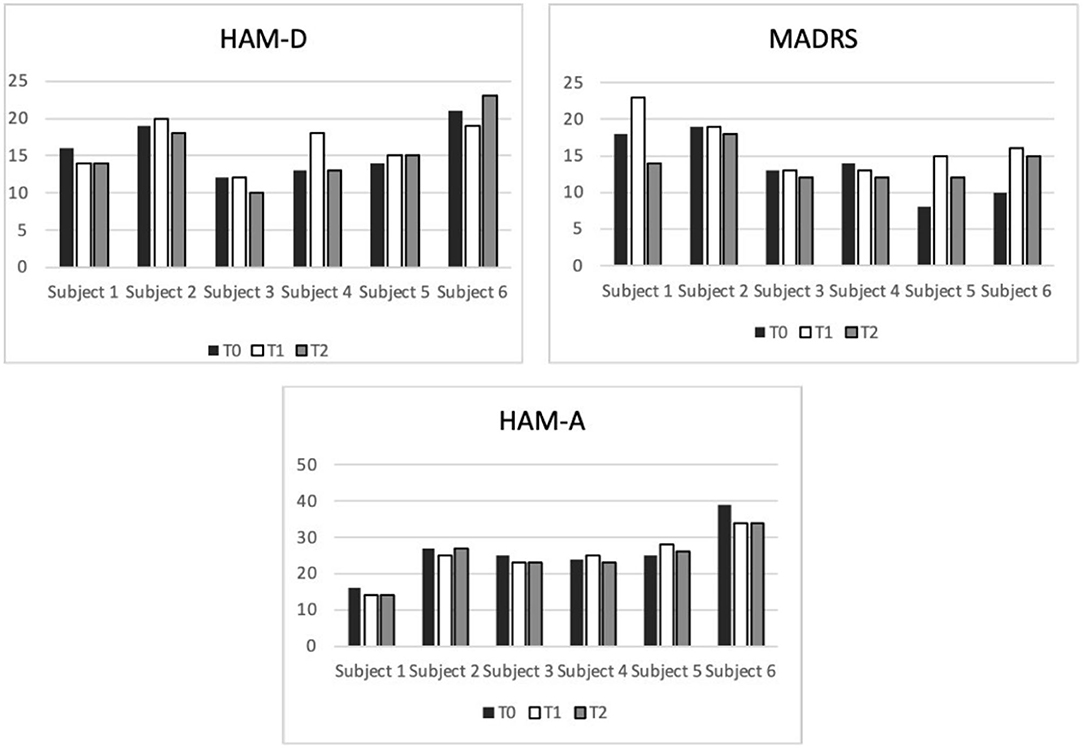
Figure 1. Bar diagrams showing subject-level depression and anxiety symptom scores before, during, and after iTBS protocol administration. On the X axis are displayed the subjects, on the Y the total scores. HAM-D, Hamilton Depressive Rating Scale; HAM-A, Hamilton Anxiety Rating Scale; MADRS, Montgomery-Asberg Depressive Rating Scale.
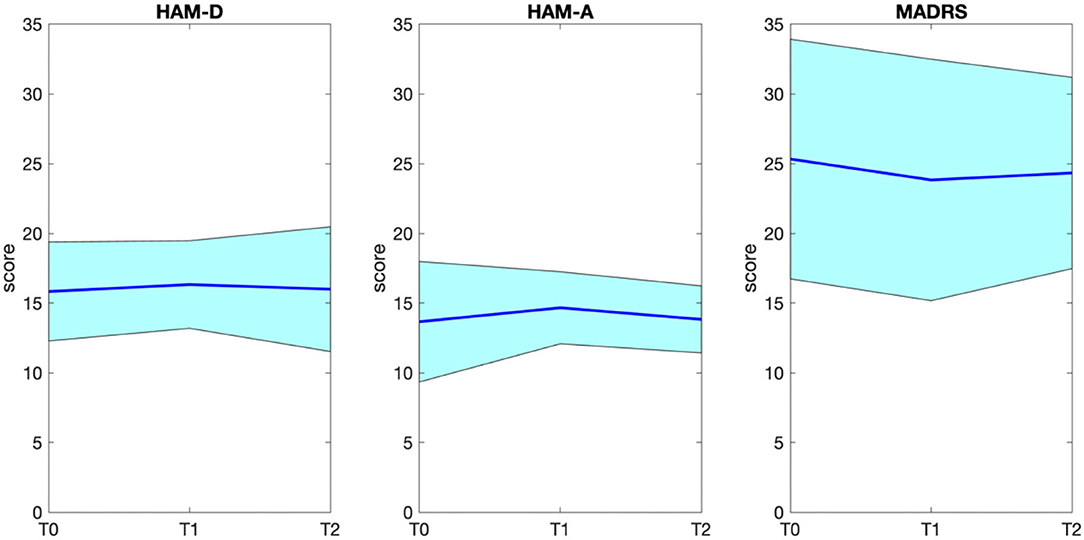
Figure 2. Group distribution (average ± standard deviation) of HAM-D, HAM-A, and MADRS scores before (T0), during (T1), and after (T2) iTBS protocol administration. HAM-D, Hamilton Depressive Rating Scale; HAM-A, Hamilton Anxiety Rating Scale; MADRS, Montgomery-Asberg Depressive Rating Scale.
The MRS, as expected, was consistent with a total score of 0 from T0 to T2 in each patient.
Discussion
In this preliminary case series, we explored the effect of accelerated iTBS in six patients affected by drug-resistant MDD or BD. A robust pattern of improvement in terms of depressive symptoms did not emerge. The small sample size could have hampered the detection of the putative antidepressant effects of our protocol. Besides, three “technical” reasons could be highlighted.
First, a parameter that might have negatively impacted is the burst frequency of iTBS protocol, which was set to 30 Hz due to technical limitations of our equipment. Although 30-Hz iTBS frequency has been previously reported to be effective in reducing depressive symptoms (30–33), it is possible that a frequency closer to 50 Hz might have enhanced the iTBS efficacy. However, to date, a direct comparison between different iTBS frequencies has not been performed yet; future studies are warranted to further elucidate this issue.
A second parameter that might have influenced our results is the duration of the interval between sessions (15 min in our protocol). Indeed, contrasting results are present in the literature. On one hand, it has been found that in an accelerated protocol with 15-min intervals, the cortical excitability significantly increased up to 60 min post-stimulation (34). On the other hand, it has been reported that time intervals longer than 15 min are necessary to induce long term potentiation (LTP) in low-threshold synapses (35). This is consistent with a previous study showing that intervals from 40 to 50 min are required for the process of protein synthesis underlying the LTP effects (36). Therefore, the 15-min pause between stimulation sessions we used, which was similar to an accelerated rTMS protocol demonstrated to be as effective as the standard rTMS protocol in a recent study (20), could have been suboptimal.
Third, the heterogeneity in treatment regimens across our patients might have also limited the identification of significant effects of accelerated iTBS on clinical symptomatology. However, after enrolment in the study protocol, the doses of this variety of pharmacological treatments were not modified, thus reducing their possible confounding effects.
In conclusion, although accelerated iTBS is a less time-consuming approach for TMS administration useful in a public healthcare setting where time and personnel resources are often limited, our preliminary results in a real-world population affected by TRD did not show significant benefits on patients' symptomatology. Further studies on wider samples and exploring the effects of different accelerated iTBS parameters are needed to make definite conclusions on such a new and unexplored topic.
Limitations
Our paper shows limitations which must be taken into account when reading our preliminary research. First, the reduced number of patients, even if producing significant data, might have produced limited amount of information. Another important aspect which might have impacted on our results is the absence of neuronavigation, which usually provides a more accurate administration of TMS. Further studies are necessary to implement our protocol with a more wide sample size.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
FC, GS, and PB contributed equally to the manuscript ideation. DS in ideation and in the recruitment of patients, while LC helped in writing minor corrections and in minor recruitment details. EM and GD gave important theatrical support for the manuscript writing and for statistical data. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We acknowledge the funding to EM, who was supported by the Italian Ministry of Health (GR-2018-12367789).
References
1. Salagre E, Solé B, Tomioka Y, Fernandes BS, Hidalgo-Mazzei D, Garriga M, et al. Treatment of neurocognitive symptoms in unipolar depression: a systematic review and future perspectives. J Affect Disord. (2017) 221:205–21. doi: 10.1016/j.jad.2017.06.034
2. Merikangas KR, Jin R, He JP, Kessler RC, Lee S, Sampson NA, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry. (2011) 68:241–51. doi: 10.1001/archgenpsychiatry.2011.12
3. Miller S, Dell'Osso B, Ketter TA. The prevalence and burden of bipolar depression. J Affect Disord. (2014) 169:S3–11. doi: 10.1016/S0165-0327(14)70003-5
4. Fitzgerald PB, Chen L, Richardson K, Daskalakis ZJ, Hoy KE. A pilot investigation of an intensive theta burst stimulation protocol for patients with treatment resistant depression. Brain Stimul. (2020) 13:137–44. doi: 10.1016/j.brs.2019.08.013
5. McConnell VL, Carter SL, Patterson K. Major depressive disorder: treatment-resistant depression and augmentation of other medication classes. Medsurg Nursing. (2019) 28:251–6. doi: 10.2147/ndt.s3369
6. Fava M. Diagnosis and definition of treatment-resistant depression. Biol Psychiatry. (2003) 53:649–59. doi: 10.1016/S0006-3223(03)00231-2
7. Sienaert P, Lambrichts L, Dols A, De Fruyt J. Evidence-based treatment strategies for treatment-resistant bipolar depression: a systematic review. Bipolar Disord. (2013) 15:61–9. doi: 10.1111/bdi.12026
8. Hidalgo-Mazzei D, Berk M, Cipriani A, Cleare AJ, Florio AD, Dietch D, et al. Treatment-resistant and multi-therapy-resistant criteria for bipolar depression: consensus definition. Br J Psychiatry. (2019) 214:27–35. doi: 10.1192/bjp.2018.257
9. Anderson IM. We all know what we mean by treatment-resistant depression–don't we? Br J Psychiatry. (2018) 212:259–61. doi: 10.1192/bjp.2018.56
10. Valero-Cabré A, Amenguala JL, Stengela C, Pascual-Leone A, Coubard OA. Transcranial magnetic stimulation in basic and clinical neuroscience: a comprehensive review of fundamental principles and novel insights. Neurosci Biobehav Rev. (2017) 83:381–404. doi: 10.1016/j.neubiorev.2017.10.006
11. Hallett M. Transcranial magnetic stimulation: a primer. Neuron. (2007) 55:187–99. doi: 10.1016/j.neuron.2007.06.026
12. Oberman L, Edwards D, Eldaief M, Pascual-Leone A. Safety of theta burst transcranial magnetic stimulation: a systematic review of the literature. J Clin Neurophysiol. (2011) 28:67–74. doi: 10.1097/WNP.0b013e318205135f
13. Hill AJ. First occurrence of hippocampal spatial firing in a new environment. Exp Neurol. (1978) 62:282–97. doi: 10.1016/0014-4886(78)90058-4
14. Larson J, Wong D, Lynch G. Patterned stimulation at the theta frequency is optimal for the induction of hippocampal long-term potentiation. Brain Res. (1986) 368:347–50. doi: 10.1016/0006-8993(86)90579-2
15. Staubli U, Lynch G. Stable hippocampal long-term potentiation elicited by ‘theta'pattern stimulation. Brain Res. (1987) 435:227–34. doi: 10.1016/0006-8993(87)91605-2
16. Klimesch W, Doppelmayr M. Theta band power in the human scalp EEG and the encoding of new information. Neuroreport. (1996) 7:1235–40. doi: 10.1097/00001756-199605170-00002
17. Rachid F. Repetitive transcranial magnetic stimulation and treatment-emergent mania and hypomania: a review of the literature. J Psychiatr Pract. (2017) 23:150–9. doi: 10.1097/PRA.0000000000000219
18. Blumberger DM, Vila-Rodriguez F, Thorpe KE, Feffer K, Noda Y, Giacobbe P, et al. Effectiveness of theta burst versus high-frequency repetitive transcranial magnetic stimulation in patients with depression (THREE-D): a randomised non-inferiority trial. Lancet. (2018) 391:1683–92. doi: 10.1016/S0140-6736(18)30295-2
19. O'Reardon JP, Solvason HB, Janicak PG, Sampson S, Isenberg KE, Nahas Z, et al. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial. Biol Psychiatry. (2007) 62:1208–16. doi: 10.1016/j.biopsych.2007.01.018
20. Fitzgerald PB, Hoy KE, Elliot D, McQueen RS, Wambeek LE, Daskalakis ZJ. Accelerated repetitive transcranial magnetic stimulation in the treatment of depression. Neuropsychopharmacology. (2018) 43:1565–72. doi: 10.1038/s41386-018-0009-9
21. Sonmez AI, Camsari DD, Nandakumar AL, Voort JLV, Kung S, Lewis CP, et al. Accelerated TMS for depression: a systematic review and meta-analysis. Psychiatry Res. (2019) 273:770–81. doi: 10.1016/j.psychres.2018.12.041
22. Chung SW, Hoy KE, Fitzgerald PB. Theta-burst stimulation: a new form of TMS treatment for depression? Depress Anxiety. (2015) 32:182–92. doi: 10.1002/da.22335
23. Cole EJ, Stimpson KH, Bentzley BS, Gulser M, Cherian K, Tischler C, et al. Stanford accelerated intelligent neuromodulation therapy for treatment-resistant depression. Am J Psychiatry. (2020) 177:716–26. doi: 10.1176/appi.ajp.2019.19070720
24. McClintock SM, Reti IM, Carpenter LL, McDonald WM, Dubin M, Taylor SF. Consensus recommendations for the clinical application of repetitive transcranial magnetic stimulation (rTMS) in the treatment of depression. J Clin Psychiatry. (2018) 79:16cs10905. doi: 10.4088/JCP.16cs10905
25. Rossi S, Hallett M, Rossini PM, Pascual-Leone A, Safety Safety of TMS Consensus Group. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin Neurophysiol. (2009) 120:2008–39. doi: 10.1016/j.clinph.2009.08.016
26. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. (1960) 23:56–62. doi: 10.1136/jnnp.23.1.56
27. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. (1979) 134:382–9. doi: 10.1192/bjp.134.4.382
28. Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. (1959) 32:50–5. doi: 10.1111/j.2044-8341.1959.tb00467.x
29. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
30. Nyffeler T, Wurtz P, Luscher HR, Hess CW, Senn W, Pflugshaupt T, et al. Repetitive TMS over the human oculomotor cortex: comparison of 1-Hz and theta burst stimulation. Neurosci Lett. (2006) 409:57–60. doi: 10.1016/j.neulet.2006.09.011
31. Nyffeler T, Cazzoli D, Wurtz P, Luthi M, von Wartburg R, Chaves S, et al. Neglect-like visual exploration behaviour after theta burst transcranial magnetic stimulation of the right posterior parietal cortex. Eur J Neurosci. (2008) 27:1809–13.
32. Pedapati EV, Gilbert DL, Horn PS, Huddleston DA, Laue CS, Shahana N, et al. Effect of 30 Hz theta burst transcranial magnetic stimulation on the primary motor cortex in children and adolescents. Front Hum Neurosci. (2015) 9:91. doi: 10.3389/fnhum.2015.00091
33. Wu SW, Shahana N, Huddleston DA, Gilbert DL. Effects of 30Hz θ burst transcranial magnetic stimulation on the primary motor cortex. J Neurosci Methods. (2012) 208:161–4. doi: 10.1016/j.jneumeth.2012.05.014
34. Tse NY, Goldsworthy MR, Ridding MC, Coxon JP, Fitzgerald PB, Fornito A, et al. The effect of stimulation interval on plasticity following repeated blocks of intermittent theta burst stimulation. Sci Rep. (2018) 8:8526. doi: 10.1038/s41598-018-26791-w
35. Thomson AC, Kenis G, Tielens S, de Graaf TA, Schuhmann T, Rutten BPF, et al. Transcranial magnetic stimulation-induced plasticity mechanisms: TMS-related gene expression and morphology changes in a human neuron-like cell model. Front Mol Neurosci. (2020) 13:528396. doi: 10.3389/fnmol.2020.528396
Keywords: iTBS, accelerated, TMS, TRD, depression, Bipolar Disorder
Citation: Cantù F, Schiena G, Sciortino D, Di Consoli L, Delvecchio G, Maggioni E and Brambilla P (2022) Use of 30-Hz Accelerated iTBS in Drug-Resistant Unipolar and Bipolar Depression in a Public Healthcare Setting: A Case Series. Front. Psychiatry 12:798847. doi: 10.3389/fpsyt.2021.798847
Received: 20 October 2021; Accepted: 20 December 2021;
Published: 12 January 2022.
Edited by:
Ali Saffet Gonul, Ege University, TurkeyReviewed by:
Hayriye Elbi, Ege University, TurkeyAlessio Simonetti, Baylor College of Medicine, United States
Copyright © 2022 Cantù, Schiena, Sciortino, Di Consoli, Delvecchio, Maggioni and Brambilla. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eleonora Maggioni, ZWxlb25vcmEubWFnZ2lvbmkmI3gwMDA0MDtwb2xpY2xpbmljby5taS5pdA==