 Caroline Meyer1*†
Caroline Meyer1*† Rayan El-Haj-Mohamad1,2†
Rayan El-Haj-Mohamad1,2† Nadine Stammel1,2
Nadine Stammel1,2 Annett Lotzin3
Annett Lotzin3 Ingo Schäfer3
Ingo Schäfer3 Christine Knaevelsrud1
Christine Knaevelsrud1 Maria Böttche1,2
Maria Böttche1,2- 1Department of Clinical Psychological Intervention, Freie Universität Berlin, Berlin, Germany
- 2Research Department, Center ÜBERLEBEN, Berlin, Germany
- 3Department of Psychiatry and Psychotherapy, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Background: The COVID-19 pandemic has led to a wide range of stressors related to depressive symptoms. Prevention measures like physical distancing have burdened the general population, especially in highly urbanized areas. However, little is known about the associations between pandemic-related stressors, coping strategies, and depressive symptoms in highly urbanized vs. less urbanized environments.
Methods: Participants were recruited in a cross-sectional online survey in Germany. Propensity score matching yielded a matched sample of city (n = 453) and town (n = 453) inhabitants. Depressive symptoms, COVID-19-related stressors, and coping strategies were compared between cities and towns. Multiple regression analysis was performed to determine associations between pandemic-related stressors and depressive symptoms for the two groups separately.
Results: City inhabitants showed significantly higher depression scores than town inhabitants (t = 2.11, df = 897.95, p = 0.035). Seven coping strategies were more often used by the city sample. Depressive symptoms were associated with “restricted physical social contact” and “difficult housing conditions” (adjusted R2= 0.19, F[9,443] = 12.52, p < 0.001) in city inhabitants, and with “fear of infection” and “difficult housing conditions” (adjusted R2= 0.20, F[9,443] = 13.50, p < 0.001) in town inhabitants.
Limitations: The data were collected at the end of the first wave and represent a snapshot without causal inferences. Pandemic-related stressors were measured with a newly developed scale.
Conclusion: Depressive symptoms, perceived stressors, and approach/avoidance coping strategies differed between city vs. town inhabitants. These differences should be considered in policy-making and mental health care.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has affected the lives of hundreds of millions of people worldwide, changing their ways of living, working, and interacting with others. According to the latest figures provided by the World Health Organization (1), over 218 million people across the world have been infected and over 4.5 million people have died (1). To contain the spread of COVID-19, governments around the world have taken various non-pharmaceutical measures, including those that restrict physical social contact and movement. During the first wave of COVID-19 in Germany (02/2020 to 05/2020), these measures included contact restrictions (e.g., restricted personal contact), work-related restrictions (e.g., closure of shops and restaurants, working from home), restrictions in daily activity (e.g., reduced leisure activities), closure of educational institutions (e.g., schools, universities, and kindergartens), and border closures (2). These preventive measures have resulted in massive disruptions in economic systems and in people's personal lives, leading, among other problems, to job loss or reduced income (3). As a result of the variety of stressors caused by the pandemic and by preventive measures to contain the spread of infection, people have been confronted with a wide range of known risk factors for mental health problems, thus amplifying major mental health problems, and specifically depressive symptoms, worldwide (4–7). An increase in depressive and anxiety symptoms, as well as distress due to the pandemic, has also been reported in Germany (8, 9). As the virus spreads primarily through direct contact or airborne via droplets and aerosols, it spreads more easily in urbanized areas with a high population density (10). In general, people living in highly urbanized areas of high-income countries are more vulnerable to mental health problems than those living in less urbanized areas (11). Accordingly, the pandemic's impact on mental health has been found to be greater in highly urbanized and thus densely populated areas (12, 13). In a representative sample in Germany, a higher degree of urbanization was strongly associated with higher rates of mood disorders (14, 15). Moreover, studies have found that high population density, noise pollution, and light pollution in areas with a high degree of urbanization are responsible for higher levels of stress and consequently higher levels of affective disorders (16, 17). However, recent research has identified social stress, and specifically social isolation, as the most important risk factor for inhabitants of highly urbanized areas (18). During the pandemic, the long-term reduction of physical social contact, i.e., the social isolation, seems to have been associated with feelings of loneliness and disconnect from daily routine, leading to an increase in depressive and anxiety symptoms (19, 20). On the other hand, living in highly urbanized areas is not only a risk factor for inhabitant's mental health but also offers several advantages that can mitigate stressors due to the higher degree of urbanization. For instance, cities can provide better educational and professional opportunities, infrastructure, cultural opportunities, and health care (17, 21). However, many of these advantages and protective factors are no longer applicable due to the COVID-19 restrictions. In particular, measures to counteract social isolation were strongly restricted during lockdown, including cultural activities, social meeting points, public spaces and parks, restaurants or cafés, and other areas that enable and encourage social encounters (21).
Since many of the protective factors of life in cities are not present during the ongoing pandemic, it is additionally important to assess situational coping strategies that might buffer the pandemic-related stressors and might have an impact in terms of exacerbating or mitigating mental health problems [e.g. association between coping strategies and depression in older adults, (22)]. The most widely used measure to assess situational coping strategies is the Brief COPE (23, 24). According to a recent review (25), the most frequently used two-factor model classifies coping strategies into approach-related coping strategies, in which the individual actively approaches the stressor (e.g., active coping, acceptance), and avoidance-related coping strategies, in which the individual attempts to ignore the stressor or avoid its impacts (e.g., self-distraction, self-blame). Several studies have demonstrated an association between coping strategies and depressive symptoms during the pandemic. For instance, it was shown that approach-related coping strategies like positive reframing or active coping tend to be associated with lower levels of depressive symptoms (26–28). By contrast, avoidance-related coping strategies, such as self-distraction, behavioral disengagement, and self-blame, seem to be significantly associated with a higher degree of depressive symptoms (26–28). During the pandemic, the most frequently employed coping strategy is that of “acceptance” (27–29). Overall, the non-pharmaceutical measures that were implemented to control the number of infections during the first wave in Germany amplified the risk factors for depressive symptoms that are especially relevant in highly urbanized populations, such as social isolation, while simultaneously limiting the utilization of protective factors. Given the higher psychological burden in more urbanized areas and the restricted protective factors during the pandemic, a better understanding of pandemic-related stressors and protective factors such as coping strategies is needed. To develop adequate mental health response plans, it is crucial to understand the psychological consequences in areas with different population density and respective beneficial coping strategies. Therefore, the aim of this study was to compare the association of COVID-19-related stressors with depressive symptoms and coping mechanisms in relation to the level of urbanization in a German sample. In Germany, the majority of people (85%) live in urbanized areas such as towns (more than 5,000 inhabitants) or cities (more than 100,000 inhabitants). Due to Germany's high overall level of urbanization, living and working conditions in rural and suburban areas are strongly dependent on the infrastructure of the surrounding towns or cities, and the actual level of urbanization is therefore difficult to determine in suburbs and in rural areas. To minimize this heterogeneity, the present study focuses only on urban populations, with a town's population representing a moderate level of urbanization and population density and a city's population representing a high level of urbanization and population density.
In accordance with previous findings in the literature, the hypotheses of the study were threefold. First, we expected to find higher levels of depressive symptoms in the highly urbanized areas (city sample) compared to the moderately urbanized areas (town sample) during the COVID-19 pandemic. Second, we expected pandemic-related stressors (e.g., restricted physical social contact, problems with childcare, restricted access to resources) to show a differential association with depressive symptoms between the two samples. Third, we expected coping strategies to differ between the city and the town sample as a possible result of different levels of depressive symptoms.
Methods
Design and Sample
The cross-sectional study was part of a pan-European longitudinal study on psychopathology, pandemic-related stressors, and coping during the COVID-19 pandemic [30, study registry: https://doi.org/10.17605/OSF.IO/8XHYG]. An online survey was used to collect data from the general population in Germany between June and September 2020. Ethical approval was obtained from the Local Psychological Ethics Committee at the Center for Psychosocial Medicine (LPEK) at the University Medical Center Hamburg-Eppendorf (LPEK-0149).
Eligibility criteria included (1) minimum age of 18 years and (2) ability to understand and write in German. Prior to participation, all participants were informed about the aim of the study and provided informed consent. The link for the survey was sent via various networks to increase variability of the sample (e.g., social media, professional organizations, leisure and sports clubs). Participants received no compensation.
Measures
In addition to the primary and secondary outcome measures, sociodemographic variables were assessed, including propensity characteristics (i.e., age, gender, COVID-19 infection, migration background, refugee background, general health status, partnership, number of children, household income, education) as well as the main variable for matching, i.e., self-reported residential area (city, suburb, town, rural area).
Depressive Symptoms
The Brief Patient Health Questionnaire (PHQ-9) assesses depressive symptoms during the last two weeks with nine items (30) rated on a 4-point Likert scale (0 = “not at all” to 3 = “nearly every day”). The overall score ranges from 0 to 27, with higher scores indicating more depressive symptoms. The measure has been validated in several populations (31, 32) and has shown excellent reliability (α = 0.86 to 0.91). The German version of the PHQ-9 is likewise well validated (32).
Pandemic Stressor Scale
The Pandemic Stressor Scale (33) assesses the perceived burden of COVID-19-related stressors during the last month with 30 items. Each item is rated on a 4-point Likert scale (0 = not at all burdened to 3 = strongly burdened), with an additional category “does not apply to me.”
The items are based on recently published research examining the burden of the COVID-19 pandemic. An exploratory factor analysis of a German sample yielded a nine-factor solution, which was cross-validated by a confirmatory factor analysis using the data of an Austrian sample of the ADJUST study (33).
Overall, nine COVID-19-related stressors, each containing up to five items, were identified: “Restricted physical social contact,” “Problems with childcare,” “Work-related problems,” “Fear of infection,” “Burden of infection,” “Restricted activity,” “Crisis management and communication,” “Restricted access to resources,” and “Difficult housing conditions.” Subscale scores were computed by calculating the average of the scores of the respective items. Before calculating the subscores, the category “Does not apply to me” was recoded into 0 (“Not at all burdened”). For details, see Appendix A.
Coping
The Brief COPE Inventory (23) is the short version of the COPE scale (34) and measures coping strategies on 14 two-item scales, with items rated on a 4-point Likert scale (1 = I haven't been doing this at all to 4 = I've been doing this a lot). The Brief COPE assesses situational coping responses to a specific stressor. In the current study, the COVID-19 pandemic was named as the specific stressor. According to Solberg et al. (25), the subscales of the Brief COPE are mostly categorized into two types of coping: approach coping styles (Use of emotional support, Use of instrumental support, Positive reframing, Acceptance, Active coping, Planning) and avoidance coping styles (Self-distraction, Denial, Substance use, Behavioral disengagement, Venting, Self-blame). The subscales humor and religion are not integrated in this dichotomy.
Statistical Analyses
First, propensity score matching was performed to reduce the risk of selection bias due to different group sizes, but mainly to control for various confounding variables arising from the convenience sampling (i.e., non-randomized assignment of the two groups). The potential confounding variables used in the propensity score matching included age, gender, previous COVID-19 infection, migration status (own or parental migration), refugee status, subjective physical health status, partnership, having children, household income, and level of education. For propensity score matching on the groups of towns and cities, we used 1:1 matching on propensity scores with nearest neighbor matching without replacement, which is the most common form of matching (35, 36). To evaluate the balance of covariates, standardized mean differences (SMD) and level of significance were assessed before and after matching using t-tests for metric variables and X2 or Fisher's exact tests for categorical variables. An SMD of 0.1 or less indicates a negligible difference between two groups (37). A t-test was used to examine whether the groups differed with respect to the primary outcome of depressive symptoms.
Multiple regression analysis was performed separately for the city sample and the town sample to determine associations between pandemic-related stressors and depressive symptoms in each group. Finally, t-test analyses were conducted to determine whether the groups used different coping strategies.
Complete case analysis was used, as recommended for propensity score matching when data is missing at random (38). This method excludes all cases with missing data in the primary outcome or at least one of the covariates. All statistical analyses were performed using R4.0.2.
Results
Baseline Characteristics Before and After Matching
In total, N = 2,782 participants from all 16 Federal states of Germany participated in the cross-sectional online survey. We excluded participants who were not living in Germany at the time of the study (n = 30) or did not complete the Patient Health Questionnaire-9 (PHQ-9, n = 502), as this was the main outcome for the study. Given the aim of the present study, we excluded an additional n = 452 participants who lived in suburbs (n = 263) or rural areas (n = 189). The final sample before propensity score matching consisted of N = 1,798 participants, 1,319 of whom lived in a city (73.4%). Baseline characteristics before and after matching are shown in Table 1. Before matching, there were significant differences between city and town participants in terms of age (participants in towns were older), being in a partnership (more people in towns were living in a partnership), having children (more people in towns reported having children), and educational level (higher educational level in cities). The standardized mean difference of potential covariates ranged from−0.201 to 0.385.
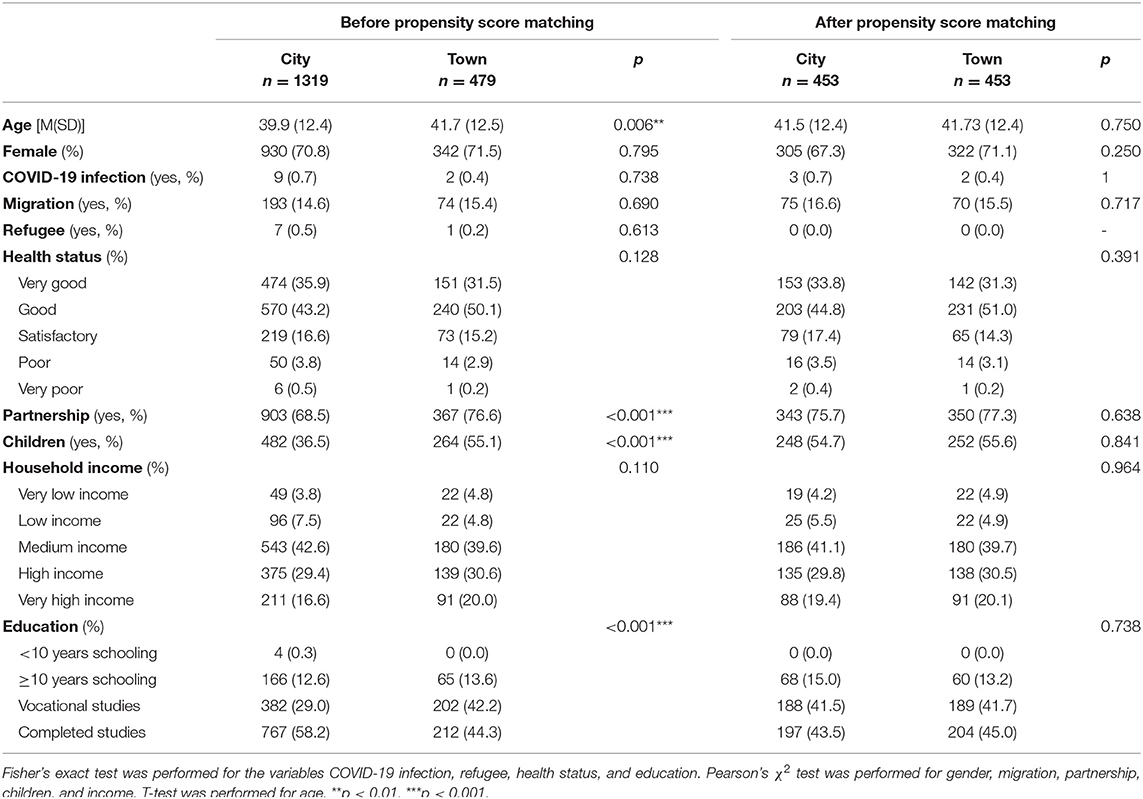
Table 1. Covariates before and after propensity score matching.
To evaluate the quality of our matched sample, we used both the p-value and the standardized mean difference as criteria. After propensity score matching, city and town samples did not differ substantially in all reported covariates (all p > 0.05, Table 1), and the standardized mean difference was within 0.1 (Figure 1). The matching process resulted in a total sample of n = 906 participants, with n = 453 in each group. In the matched sample, the age ranged from 18 to 78 years (M = 41.6, SD = 12.4) and the majority of participants were female (n = 627, 69.2%).
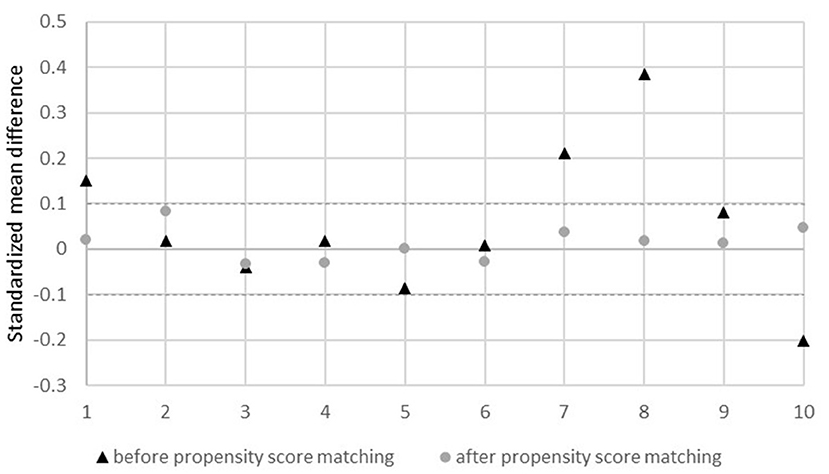
Figure 1. Standardized mean difference before and after propensity score matching. 1, age; 2, sex; 3, infection yes/no; 4, migration yes/no; 5, refugee yes/no; 6, health status; 7, partner yes/no; 8, children yes/no; 9, income; 10, educational level.
Depressive Symptoms and COVID-19-Related Stressors in Cities and Towns
For all subsequent analyses, only the matched sample was considered. The city sample reported significantly higher levels of depressive symptoms compared to the town sample (t = 2.11, df = 897.95, p = 0.03, Table 2).
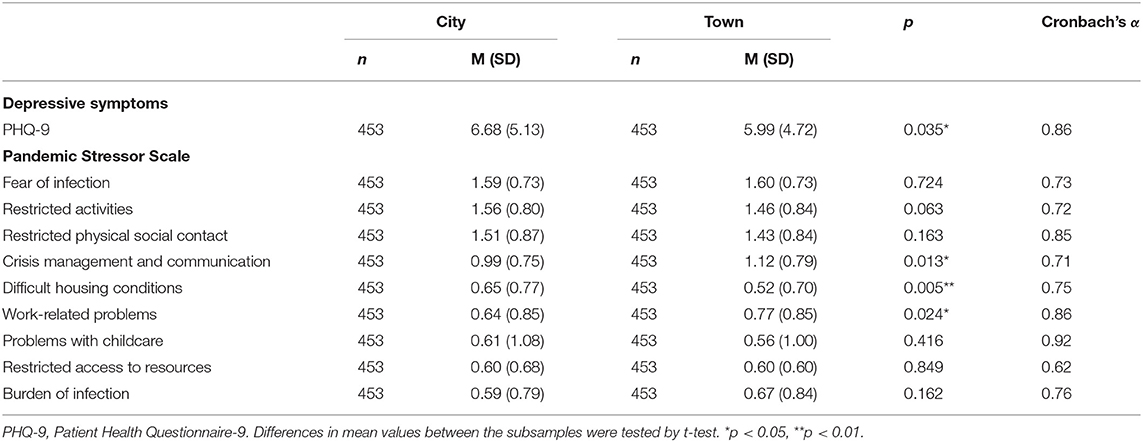
Table 2. Depressive symptoms measured by the PHQ-9 and stressors measured by the Pandemic Stressor Scale after propensity score matching.
Overall, people from cities and towns perceived similar COVID-19-related stressors. In total, the perceived stressors exerted low or moderate levels of burden in both samples (lowest burden M = 0.59, “burden of infection” in cities; highest burden M = 1.60, “fear of infection” in towns; range from 0 to 3). The following stressors were perceived to be the most stressful in both samples: problems with fear of infection (M = 1.59 in cities, M = 1.60 in towns), restricted activities (M = 1.56 in cities, M = 1.46 in towns), and restricted physical contact (M = 1.51 in cities, M = 1.43 in towns). Nevertheless, there were three significant differences between the town and city inhabitants: Participants in towns were more stressed because of work-related problems and “crisis management and communication” compared to those in cities. At the same time, participants living in cities were significantly more stressed due to the “difficult housing conditions” (Table 2).
Associations Between COVID-19-Related Stressors and Depressive Symptoms in Cities and Towns
We conducted correlation analysis (Appendices B,C) and multiple regression analyses (Table 3) to examine the relationship between depressive symptoms and the pandemic stressor subscales for each sample separately. Correlates of depressive symptoms differed between the city and town samples (Table 3).
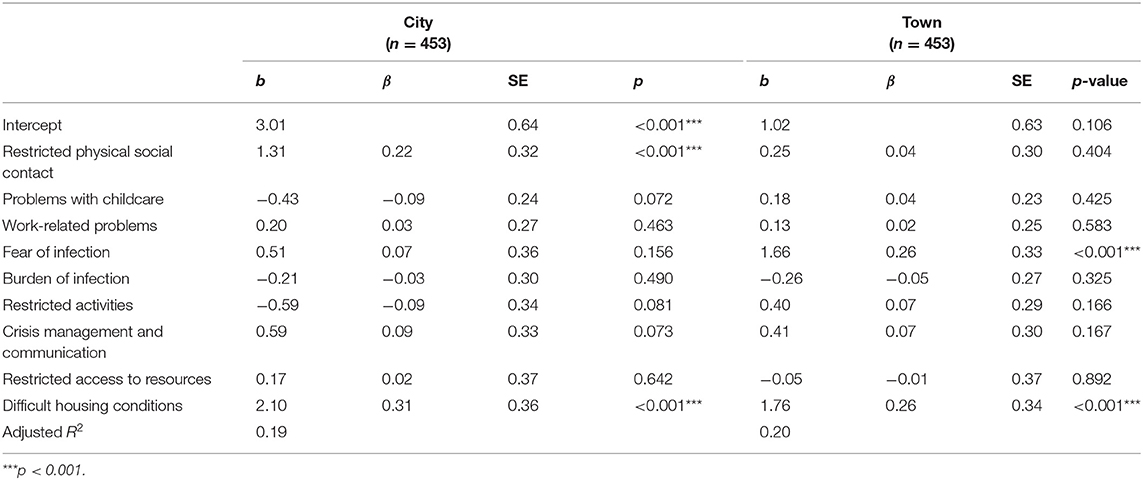
Table 3. Regression analysis of stressor subscales on depressive symptoms for city sample and town sample after propensity score matching.
For the city sample, depressive symptoms were associated with “restricted physical social contact” and “difficult housing conditions” (adjusted R2= 0.19, F[9,443] = 12.52, p < 0.001). For the town sample, depressive symptoms were associated with “fear of infection” and “difficult housing conditions” (adjusted R2 = 0.20, F[9,443] = 13.50, p < 0.001).
Coping Strategies in Cities and Towns
When comparing coping strategies between the two samples, the city inhabitants reported a higher use of seven out of fourteen coping strategies compared to those from towns. Participants living in cities reported significantly higher values on approach coping strategies (active coping, instrumental support, acceptance, emotional support) but also on avoidance coping strategies (venting, substance use) as well as the strategy “humor.” The most frequently used coping strategies in both samples were acceptance, self-distraction, and positive reframing (Table 4).

Table 4. Coping strategies by subsamples after propensity score matching and results of group comparison between city sample and town sample.
Discussion
The current study examined differences and similarities in depressive symptoms, COVID-19-related stressors, and coping strategies in city and town inhabitants in Germany. Through the use of propensity score matching, we were able to control for systematic differences between the two groups that may have resulted from convenience sampling. This allowed us to estimate, for the first time, a more precise representation of city and town inhabitants regarding the above-mentioned variables and shows the importance of the matched factors, as they varied significantly before matching. We found higher levels depressive symptoms in the city sample compared to the town sample in the matched samples, confirming previous results while controlling for several confounding factors. The relationship between pandemic related stressors and depressive symptoms differed between city and town inhabitants. Furthermore, city inhabitants reported a more frequent use of several coping strategies.
We found significantly higher levels of depressive symptoms in participants from cities compared to those from towns. Our results are in line with previous studies describing generally higher depressive symptoms in urban areas (11, 14). Moreover, they also correspond to recent studies that investigated populations in high-income countries during the pandemic and found a link between higher levels of urbanization and higher levels of mental distress (39, 40). This seems to reflect the effect of the non-pharmaceutical lockdown measures that were implemented to control the number of infections during the first wave of COVID-19 in Germany, which focused on contact restrictions and especially restricted time spent in public places both outdoors and indoors (2). These measures therefore amplified social isolation, being one of the main risk factors for depressive symptoms in city inhabitants (18). In accordance with this, the stressor “restricted physical social contact” was perceived as one of the most burdensome pandemic-related stressors by the city inhabitants. It was also strongly associated with depressive symptoms in the city sample but not in the town sample, indicating a potentially stronger impact of contact restrictions on depressive symptoms in more densely populated areas, though our cross-sectional design does not allow for causal inferences. At the same time, most of the benefits of living in cities (e.g., cultural activities, social meeting points) were eliminated due to the pandemic-specific restrictions. In contrast, access to outdoor spaces and a view of nature were found to be protective factors during the pandemic and are related to reduced levels of depressive and anxiety symptoms, especially under strict lockdown conditions (41). Both of these natural “buffers” are less available in cities.
Our study also aimed at a more differentiated understanding of possible factors influencing depressive symptoms in both cities and towns. Concerning stressors and coping strategies, we found both similarities and substantial differences. The findings on pandemic-specific stressors illustrate the extent to which the inhabitants of cities and towns felt stressed in various areas of everyday life and leisure during the pandemic. In the present study, only three significant differences emerged (“work-related problems” and “crisis management and communication” were higher in towns, “difficulties in housing conditions” were higher in cities), while the majority of pandemic-related stressors were perceived as equally burdensome in cities and towns. For both groups, the stressors perceived as the most burdensome were “fear of infection,” “restricted activities,” and “restricted physical social contact.” Studies have shown that infection-related stressors, i.e., fear of infecting others and loved ones, are perceived as highly stressful during the pandemic (42) due to the fact that the virus is life-threatening for people in high-risk groups [e.g., elderly, people with lung or heart diseases, (43)]. Furthermore, fear can also be explained by a lack of knowledge and by the unfamiliar and unpredictable new reality (44). The higher perceived stress with regard to restrictions of activities and physical social contacts appears to be self-evident due to the overall reported benefits of physical activity and social contacts (45).
“Work-related problems” as well as “crisis management and communication” were perceived as significantly more burdensome in towns. It is possible that people in cities can adapt more easily to crises due to a better infrastructure. This might, for example, include digitalization, better job opportunities in the case of job loss, better health care, and more services that offer support (46). These infrastructure advantages in cities could therefore mitigate the association between the aforementioned stressors and depressive symptoms. Previous research has already indicated an impact of media coverage on fears relating to COVID-19 (42). Garfin et al. (47) recommend using trustworthy and informative media and avoiding repetitive exposure to media with little new information. Especially in times of lack of knowledge, this is of high importance and could buffer the stressor “crisis management and communication.” In cities, “difficult housing conditions” were perceived as significantly more stressful. One explanation could be that the limited options in cities (e.g., small apartments, fewer social alternatives to seeing friends or family members, limited public spaces) were perceived as more burdensome.
The relationship between pandemic-related stressors and the severity of depressive symptoms illustrates that “difficult housing conditions” are associated with depressive symptoms in both samples. This is in line with previous findings suggesting that poor housing conditions, and especially limited space, are related to higher levels of depressive symptoms (48). In cities, the “restricted physical social contacts” were also significantly related to depressive symptoms. COVID-19 measures resulted in limited to no social contact over several months. As mentioned above, it can be assumed that these measures, especially in cities, aggravated a trend that has been found in previous studies. As previous findings show, people have begun to feel lonely during the pandemic, which is strongly correlated with depressive symptoms (19, 20). In towns, “fear of infection” was significantly related to severity of depressive symptoms. Due to a lesser social anonymity in towns, a potential fear of stigmatization as a result of an infection could explain this additional significant finding (49).
With regard to coping strategies, it was found that city inhabitants use seven of the examined 14 coping strategies significantly more often compared to town inhabitants (approach-related strategies i.e., active coping, acceptance, emotional and instrumental support; avoidance-related coping strategies, i.e., venting, substance use as well as the coping strategy “humor”). There were no significant differences in the other seven strategies. Recent studies have shown that “active coping,” “venting,” and “substance use” in particular are associated with depressive symptoms due to the pandemic (27). One explanation for why city inhabitants, on average, use more often strategies to cope with the pandemic could lie in the fact that depressive symptoms are higher in cities than in the towns, meaning that there is a greater need to use these strategies. However, research has shown that more frequent use of positive coping strategies might not be predictive of better positive adjustment over time (50). At this point, it is also important to mention that the rank order of the frequency of coping strategies used is the same in cities and towns. In both samples, “acceptance,” “positive reframing,” and “self-distraction” are used most frequently. This is in line with previous studies that also found “acceptance” and “self-distraction” to be among the most frequently used strategies during the pandemic (27–29). In a recent study, the coping strategy of “positive reframing” was the most beneficial in coping with depressive symptoms (27).
In our study, we found significant relationships between situational stressors and depressive symptoms even at an early stage of the pandemic. Presumably, these effects have intensified further over the course of the pandemic. The ongoing dilemma of lockdown and reopening has several implications, and the present findings emphasize that the level of urbanization has an impact on depressive symptoms as well as perceived COVID-19-related stressors.
Limitations
The study findings should be interpreted in the light of several limitations. First, the data were collected in the period of June 2020 to September 2020. This period was at the end of the first wave of the pandemic, when infection rates were low and relatively few restrictions were in place in Germany. Second, as the data were cross-sectional, they represent a momentary snapshot of the situation without providing any information about the time course. Also, no statements can be made about representativeness as the sample was circumstantial and purposeful and the rate of return is unknown. However, different recruitment strategies were applied to increase the variability of the sample (e.g., social media, interest groups, companies). Third, pandemic-specific restrictions were measured using a newly developed instrument (33). Fourth, some of the subscales of the Brief COPE showed questionable or poor reliability scores in our study (Cronbach's Alpha: 0.53–0.92). This has also been reported in other studies (51, 52) and seems to be a general problem of the questionnaire, which is also reflected in the inconsistent factor structure of the Brief COPE (53). Fifth, although the propensity score matching has several advantages for examining the hypotheses and ensured comparability of our samples, the current dataset does not contain all participants and the representativeness of the two subsamples may have been altered especially in the city sample.
Conclusion
Characteristics regarding depressive symptoms and coping strategies as well as the impact of pandemic-related stressors in cities and towns should be considered when addressing psychosocial support for vulnerable groups during and after the pandemic. Policy makers need to be aware of the special risks and needs in urban populations and should carefully evaluate the COVID-19-related measures taken in view of mental health costs and benefits. It seems to be important to investigate implications for different life circumstances and also to detect specific characteristics due to the level of urbanization. Future studies should therefore apply standardized measures of urbanization, e.g., by including population figures or other objective measures. Specifically, it becomes clear that restricted activities and physical social contact as well as housing conditions seem to be most burdensome in urban inhabitants. These stressors should receive special attention, both to better identify vulnerable people and to make future restrictions less stressful.
Long-term effects of the restrictions on mental health must be closely monitored, and mental health care offers need to be adapted to increased needs as early as possible.
This could be addressed in an easy and cost-effective manner by implementing low-threshold (online) interventions with instructions for self-help and self-care. In addition, longitudinal studies will be needed to differentiate between functional and dysfunctional coping strategies during and after the pandemic and to determine their effect on depressive symptoms. It is important to learn from this exceptional situation, to be able to give advice to vulnerable populations for the current situation and for potentially similar situations in the future.
Data Availability Statement
The detailed sociodemographic information of the dataset does not fully protect the anonymity of the respondents. For this reason, the entire dataset cannot be made publicly available. However, excerpts of the data on a higher aggregation level can be provided upon justified request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Center for Psychosocial Medicine (LPEK) at the University Medical Center Hamburg-Eppendorf (LPEK-0149). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AL designed the study in cooperation with the project steering committee formed by the representatives of the ESTSS countries [see (54)]. AL, MB, and RE-H-M were responsible for the data collection in Germany. CM, RE-H-M, and MB carried out the statistical analyses and drafted the manuscript. AL, IS, NS, and CK carefully revised the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the team of the coordinating site at University of Hamburg, in particular Laura Kenntemich, Laura Gutewort and Lennart Schwierzke. In addition, we would like to thank Dr. Sven Buth and Eike Neumann-Runde for the technical support. We acknowledge support by the Open Access Publication Initiative of Freie Universität Berlin.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.791312/full#supplementary-material
References
1. World Health Organization. WHO Coronavirus (COVID-19) Dashboard. (2021). Available online at: https://covid19.who.int/ (accesssed September 6, 2021).
2. Aravindakshan A, Boehnke J, Gholami E, Nayak A. Preparing for a future COVID-19 wave: insights and limitations from a data-driven evaluation of non-pharmaceutical interventions in Germany. Sci Rep. (2020) 10:1–14. doi: 10.1038/s41598-020-76244-6
3. Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socio-economic implications of the coronavirus and COVID-19 pandemic: a review. Int J Surg. (2020) 78:185–93. doi: 10.1016/j.ijsu.2020.04.018
4. Bueno-Notivol J, Gracia-García P, Olaya B, Lasheras I, López-Antón R, Santabárbara J. Prevalence of depression during the COVID-19 outbreak: a meta-analysis of community-based studies. Int J Clin Health Psychol. (2021) 21:100196. doi: 10.1016/j.ijchp.2020.07.007
5. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. (2020) 288:112954. doi: 10.1016/j.psychres.2020.112954
6. Shah SMA, Mohammad D, Qureshi MFH, Abbas MZ, Aleem S. Prevalence, Psychological Responses and associated correlates of depression, anxiety and stress in a global population, during the coronavirus disease (COVID-19) pandemic. Community Ment Health J. (2021) 57:101–10. doi: 10.1007/s10597-020-00728-y
7. Wu T, Jia X, Shi H, Niu J, Yin X, Xie J, et al. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J Affect Disord. (2020) 281:91–8. doi: 10.1016/j.jad.2020.11.117
8. Bauer LL, Seiffer B, Deinhart C, Atrott B, Sudeck G, Hautzinger M, et al. Associations of exercise and social support with mental health during quarantine and social-distancing measures during the COVID-19 pandemic: a cross-sectional survey in Germany. MedRxiv. (2020). doi: 10.1101/2020.07.01.20144105
9. Bäuerle A, Steinbach J, Schweda A, Beckord J, Hetkamp M, Weismüller B, et al. Mental health burden of the CoViD-19 outbreak in germany: predictors of mental health impairment. J Prim Care Community Health. (2020) 11:2150132720953682. doi: 10.1177/2150132720953682
10. Taylor S. The Psychology Of Pandemics: Preparing For The Next Global Outbreak Of Infectious Disease. Newcastle upon Tyne: Cambridge Scholars Publishing (2019).
11. Peen J, Dekker J, Schoevers RA, Ten Have M, de Graaf R, Beekman AT. Is the prevalence of psychiatric disorders associated with urbanization? Soc Psychiatry Psychiatr Epidemiol. (2007) 42:984–9. doi: 10.1007/s00127-007-0256-2
12. Chen Y, Jin Y, Zhu L, Fang Z, Wu N, Du M, et al. The network investigation on knowledge, attitude and practice about COVID-19 of the residents in Anhui Province. Zhonghua Yu Fang Yi Xue Za Zhi. (2020) 54:367–73. doi: 10.3760/cma.j.cn112150-20200205-00069
13. Özdin S, Bayrak Özdin S. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: the importance of gender. Int J Soc Psychiatry. (2020) 66:504–11. doi: 10.1177/0020764020927051
14. Dekker J, Peen J, Koelen J, Smit F, Schoevers R. Psychiatric disorders and urbanization in Germany. BMC Public Health. (2008) 8:1–9. doi: 10.1186/1471-2458-8-17
15. Jacobi F, Höfler M, Siegert J, Mack S, Gerschler A, Scholl L, et al. Twelve-month prevalence, comorbidity and correlates of mental disorders in Germany: the mental health module of the german health interview and examination survey for adults (DEGS1-MH). Int J Methods Psychiatr Res. (2014) 23:304–19. doi: 10.1002/mpr.1439
16. Cho Y, Ryu S-H, Lee BR, Kim KH, Lee E, Choi J. Effects of artificial light at night on human health: a literature review of observational and experimental studies applied to exposure assessment. Chronobiol Int. (2015) 32:1294–310. doi: 10.3109/07420528.2015.1073158
17. Gruebner O, Rapp MA, Adli M, Kluge U, Galea S, Heinz A. Cities and mental health. Dtsch Ärztebl Int. (2017) 114:121. doi: 10.3238/arztebl.2017.0121
18. Adli M, Schöndorf J. Macht uns die Stadt krank? Wirkung von Stadtstress auf Emotionen, Verhalten und psychische Gesundheit. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz. (2020) 63:1–8. doi: 10.1007/s00103-020-03185-w
19. Meyer J, McDowell C, Lansing J, Brower C, Smith L, Tully M, et al. Changes in physical activity and sedentary behavior in response to COVID-19 and their associations with mental health in 3052 US adults. Int J Environ Res Public Health. (2020) 17:6469. doi: 10.3390/ijerph17186469
20. Santini ZI, Jose PE, Cornwell EY, Koyanagi A, Nielsen L, Hinrichsen C, et al. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): a longitudinal mediation analysis. Lancet Public Health. (2020) 5:e62–70. doi: 10.1016/S2468-2667(19)30230-0
21. Behr S, Schöndorf J, Berger M, Adli M. Psychische Gesundheit in der Stadt. Stadtsoziologie und Stadtentwicklung. (2020) 379–90. doi: 10.5771/9783845276779
22. Bjørkløf GH, Engedal K, Selbæk G, Kouwenhoven SE, Helvik A-S. Coping and depression in old age: a literature review. Dement Geriatr Cogn Disord. (2013) 35:121–54. doi: 10.1159/000346633
23. Carver CS. You want to measure coping but your protocol's too long: Consider the Brief COPE. Int J Behav Med. (1997) 4:92–100. doi: 10.1207/s15327558ijbm0401_6
24. Kato T. Frequently used coping scales: a meta-analysis. Stress Health. (2015) 31:315–23. doi: 10.1002/smi.2557
25. Solberg MA, Gridley MK, Peters RM. The factor structure of the brief cope: a systematic review. West J Nurs Res. (2021) 01939459211012044. doi: 10.1177/01939459211012044
26. Gurvich C, Thomas N, Thomas EH, Hudaib A-R, Sood L, Fabiatos K, et al. Coping styles and mental health in response to societal changes during the COVID-19 pandemic. Int J Soc Psychiatry. (2020) 67:540–9. doi: 10.1177/0020764020961790
27. Shamblaw AL, Rumas RL, Best MW. Coping during the COVID-19 pandemic: Relations with mental health and quality of life. Can Psychol. (2021) 62:92–100. doi: 10.1037/cap0000263
28. Skapinakis P, Bellos S, Oikonomou A, Dimitriadis G, Gkikas P, Perdikari E, et al. Depression and its relationship with coping strategies and illness perceptions during the COVID-19 lockdown in Greece: a cross-sectional survey of the population. Depress Res Treat. (2020) 2020:3158954. doi: 10.1155/2020/3158954
29. Rettie H, Daniels J. Coping and tolerance of uncertainty: predictors and mediators of mental health during the COVID-19 pandemic. Am psychol. (2020) 76:427–37. doi: 10.1037/amp0000710
30. Spitzer RL, Kroenke K, Williams JB, Group PHQPCS, Group PHQPCS. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. JAMA. (1999) 282:1737–44. doi: 10.1001/jama.282.18.1737
31. Kroenke K, Spitzer RL, Williams JB, Löwe B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry. (2010) 32:345–59. doi: 10.1016/j.genhosppsych.2010.03.006
32. Reich H, Rief W, Brähler E, Mewes R. Cross-cultural validation of the German and Turkish versions of the PHQ-9: an IRT approach. BMC psychol. (2018) 6:1–13. doi: 10.1186/s40359-018-0238-z
33. Lotzin A, Ketelsen R, Buth S, Zrnic I, Lueger-Schuster B, Böttche M, et al. The Pandemic Stressor Scale - Factorial validity and reliability of a measure of stressors during a pandemic [Manuscript in preparation.]. Department of Psychiatry and Psychotherapy, University Medical Center Hamburg-Eppendorf, Hamburg, Germany. (2021). doi: 10.21203/rs.3.rs-555631/v1
34. Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: a theoretically based approach. J Pers Soc Psychol. (1989) 56:267. doi: 10.1037/0022-3514.56.2.267
35. Thoemmes FJ, Kim ES. A systematic review of propensity score methods in the social sciences. Multivariate Behav Res. (2011) 46:90–118. doi: 10.1080/00273171.2011.540475
36. Zakrison T, Austin P, McCredie V. A systematic review of propensity score methods in the acute care surgery literature: avoiding the pitfalls and proposing a set of reporting guidelines. Eur J Trauma Emerg Surg. (2018) 44:385–95. doi: 10.1007/s00068-017-0786-6
37. Steiner PM, Cook TD, Shadish WR, Clark MH. The importance of covariate selection in controlling for selection bias in observational studies. Psychol Methods. (2010) 15:250. doi: 10.1037/a0018719
38. Malla L, Perera-Salazar R, McFadden E, Ogero M, Stepniewska K, English M. Handling missing data in propensity score estimation in comparative effectiveness evaluations: a systematic review. J Comp Eff Res. (2018) 7:271–9. doi: 10.2217/cer-2017-0071
39. Hubbard G, Daas Cd, Johnston M, Murchie P, Thompson CW, et al. Are rurality, area deprivation, access to outside space, and green space associated with mental health during the COVID-19 pandemic? a cross sectional study (CHARIS-E). Int J Environ Res Public Health. (2021) 18:3869. doi: 10.3390/ijerph18083869
40. Okubo R, Yoshioka T, Nakaya T, Hanibuchi T, Okano H, Ikezawa S, et al. Urbanization level and neighborhood deprivation, not COVID-19 case numbers by residence area, are associated with severe psychological distress and new-onset suicidal ideation during the COVID-19 pandemic. J Affect Disord. (2021) 287:89–95. doi: 10.1016/j.jad.2021.03.028
41. Pouso S, Borja Á, Fleming LE, Gómez-Baggethun E, White MP, Uyarra MC. Contact with blue-green spaces during the COVID-19 pandemic lockdown beneficial for mental health. Sci Total Environ. (2021) 756:143984. doi: 10.1016/j.scitotenv.2020.143984
42. Mertens G, Gerritsen L, Duijndam S, Salemink E, Engelhard IM. Fear of the coronavirus (COVID-19): predictors in an online study conducted in March 2020. J Anxiety Disord. (2020) 74:102258. doi: 10.1016/j.janxdis.2020.102258
43. World Health Organization. COVID-19: Vulnerable And High Risk Groups (2020). Available online at: https://www.who.int/westernpacific/emergencies/covid-19/information/high-risk-groups (accessed July 8, 2021).
44. Arora A, Jha AK, Alat P, Das SS. Understanding coronaphobia. Asian J Psychiatr. (2020) 54:102384. doi: 10.1016/j.ajp.2020.102384
45. Schuch FB, Vancampfort D, Firth J, Rosenbaum S, Ward PB, Silva ES, et al. Physical activity and incident depression: a meta-analysis of prospective cohort studies. Am J Psychiatry. (2018) 175:631–48. doi: 10.1176/appi.ajp.2018.17111194
46. Meyer WB. The Environmental Advantages Of Cities: Countering Commonsense Antiurbanism. MIT Press (2013). doi: 10.7551/mitpress/9513.001.0001
47. Garfin DR, Silver RC, Holman EA. The novel coronavirus (COVID-2019) outbreak: Amplification of public health consequences by media exposure. Health psychol. (2020) 39:355. doi: 10.1037/hea0000875
48. Amerio A, Brambilla A, Morganti A, Aguglia A, Bianchi D, Santi F, et al. COVID-19 lockdown: housing built environment's effects on mental health. Int J Environ Res Public Health. (2020) 17:5973. doi: 10.3390/ijerph17165973
49. Person B, Sy F, Holton K, Govert B, Liang A. Fear and stigma: the epidemic within the SARS outbreak. Emerg Infect Dis. (2004) 10:358. doi: 10.3201/eid1002.030750
50. Heffer T, Willoughby T. A count of coping strategies: a longitudinal study investigating an alternative method to understanding coping and adjustment. PLoS ONE. (2017) 12:e0186057. doi: 10.1371/journal.pone.0186057
51. Matsumoto S, Yamaoka K, Nguyen HDT, Nguyen DT, Nagai M, Tanuma J, et al. Validation of the brief coping orientation to problem experienced (Brief COPE) inventory in people living with HIV/AIDS in Vietnam. Global Health Med. (2020) 2:374–83. doi: 10.35772/ghm.2020.01064
52. Umucu E, Lee B. Examining the impact of COVID-19 on stress and coping strategies in individuals with disabilities and chronic conditions. Rehabil Psychol. (2020) 65:193. doi: 10.1037/rep0000328
53. Rahman HA, Issa WB, Naing L. Psychometric properties of brief-COPE inventory among nurses. BMC Nurs. (2021) 20:73. doi: 10.1186/s12912-021-00592-5
54. Lotzin A, Acquarini E, Ajdukovic D, Ardino V, Böttche M, Bondjers K, et al. Stressors, coping and symptoms of adjustment disorder in the course of the COVID-19 pandemic–study protocol of the European society for traumatic stress studies (ESTSS) pan-European study. Eur J Psychotraumatol. (2020) 11:1780832. doi: 10.1080/20008198.2020.1780832
Keywords: coronavirus, depression, restrictions, level of urbanization, pandemic stressors, mental health
Citation: Meyer C, El-Haj-Mohamad R, Stammel N, Lotzin A, Schäfer I, Knaevelsrud C and Böttche M (2022) Associations of Depressive Symptoms, COVID-19-Related Stressors, and Coping Strategies. A Comparison Between Cities and Towns in Germany. Front. Psychiatry 12:791312. doi: 10.3389/fpsyt.2021.791312
Received: 08 October 2021; Accepted: 27 December 2021;
Published: 27 January 2022.
Edited by:
Daria Smirnova, Samara State Medical University, RussiaReviewed by:
Piotr Długosz, Pedagogical University of Kraków, PolandAnca Livia Panfil, Spitalul Clinic Județean de Urgență “Pius Brînzeu” Timișoara, Romania
Copyright © 2022 Meyer, El-Haj-Mohamad, Stammel, Lotzin, Schäfer, Knaevelsrud and Böttche. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Caroline Meyer, Y2Fyb2xpbmUubWV5ZXJAZnUtYmVybGluLmRl
†These authors have contributed equally to this work and share first authorship