 Gaia Sampogna1*
Gaia Sampogna1* Vincenzo Giallonardo1
Vincenzo Giallonardo1 Valeria Del Vecchio1
Valeria Del Vecchio1 Mario Luciano1
Mario Luciano1 Umberto Albert2,3
Umberto Albert2,3 Claudia Carmassi4
Claudia Carmassi4 Giuseppe Carrà5
Giuseppe Carrà5 Francesca Cirulli6
Francesca Cirulli6 Bernardo Dell'Osso7
Bernardo Dell'Osso7 Giulia Menculini8
Giulia Menculini8 Martino Belvederi Murri9
Martino Belvederi Murri9 Maurizio Pompili10
Maurizio Pompili10 Gabriele Sani11,12
Gabriele Sani11,12 Umberto Volpe13Valeria Bianchini14
Umberto Volpe13Valeria Bianchini14 Andrea Fiorillo1
Andrea Fiorillo1- 1Department of Psychiatry, University of Campania Luigi Vanvitelli, Naples, Italy
- 2Department of Medicine, Surgery and Health Sciences, University of Trieste, Trieste, Italy
- 3Department of Mental Health, Azienda Sanitaria Universitaria Giuliano Isontina—ASUGI, Trieste, Italy
- 4Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy
- 5Department of Medicine and Surgery, University of Milan Bicocca, Milan, Italy
- 6Center for Behavioral Sciences and Mental Health, National Institute of Health, Rome, Italy
- 7Department of Biomedical and Clinical Sciences, Luigi Sacco and Aldo Ravelli Center for Neurotechnology and Brain Therapeutic, University of Milan, Milan, Italy
- 8Department of Psychiatry, University of Perugia, Perugia, Italy
- 9Department of Biomedical and Specialty Surgical Sciences, Institute of Psychiatry, University of Ferrara, Ferrara, Italy
- 10Department of Neurosciences, Mental Health and Sensory Organs, Faculty of Medicine and Psychology, Sapienza University of Rome, Rome, Italy
- 11Department of Neuroscience, Section of Psychiatry, University Cattolica del Sacro Cuore, Rome, Italy
- 12Department of Psychiatry, Fondazione Policlinico Agostino Gemelli IRCCS, Rome, Italy
- 13Clinical Psychiatry Unit, Department of Clinical Neurosciences, Università Politecnica delle Marche, Ancona, Italy
- 14Department of Life, Health and Environmental Sciences, Psychiatric Unit: Trattamenti Riabilitativi Psicosociali, Interventi Precoci, TRIP, Psychosocial Rehabilitation Treatment, Early Interventions University Unit, University of L'Aquila, L'Aquila, Italy
The COVID-19 pandemic has affected the mental and physical health of the general population at any age, but it is expected to have a protracted and severe consequences for younger populations. The pandemic has had several consequences on mental health including anger and irritability, depressive symptoms and somatic complaints, insomnia, lack of motivation, and loneliness. In particular, loneliness and its related negative feelings are thought to be particularly pronounced during young adulthood because of the many social changes that young people deal with during this period of life. Therefore, it is essential to evaluate the type of impact of the pandemic on the mental health of young people and their levels of loneliness experienced during the first phase of the lockdown. Based on the largest Italian study on the effects of the COVID-19 pandemic on the mental health of general population, in this paper we aim to: (1) describe the levels of loneliness in a national sample of Italian young adults aged 18–34 years, during the first wave of lockdown in 2020; (2) evaluate the clinical and socio-demographic differences in young adults reporting low vs. high levels of loneliness; (3) assess the role of clinical symptomatology, coping strategies, levels of resilience, and duration of lockdown as possible predictors of loneliness. The final sample consists of 8,584 people, mainly female (72.6%), single, with a mean age of 26.4 (±4.4) years. The mean score at the UCLA was 47.5 (±13.6), with 27% (N = 2,311) of respondents exceeding the cut-off for high levels of loneliness. High levels of loneliness were predicted by the presence of avoidant coping strategies, such as self-distraction (Beta coefficient, B = 0.369, 95% Confidence Interval, CI = 0.328–0.411), venting (B = 0.245, 95% CI = 0.197–0.293), denial (B = 0.110, 95% CI = 0.061–0.159), and emotional disengagement (B = 0.133, 95% CI = 0.080–0.185). Weeks of exposure to the pandemic were significantly associated with worsening of loneliness (p < 0.000). There is currently considerable interest in trying to reduce loneliness, both within the context of COVID-19 and more generally. Our results highlight that young people are at a higher risk of developing loneliness and suggest that more interventions and practical guidelines are needed.
Introduction
The COVID-19 pandemic is a “new” form of trauma affecting different groups of individuals, communities, cities, regions at the same time, with no possibility to identify and limit the “enemy” (1–3). Although the pandemic has affected the mental and physical health of the general population at any age (4–6), it is expected that this global crisis can have protracted and severe consequences for younger populations (7). In fact, the pandemic is posing multiple challenges to young people, through the disruption of daily educational, academic, professional, social, and family life (8, 9).
Due to the rapid spread of the coronavirus, several preventive measures, including physical distance, face masks, home quarantine, and lockdown restrictions have been implemented in order to contain the transmission and the contagion of other people (10, 11).
On March 8, 2020, the Italian Prime Minister announced the “stay at home” order and entered the first national lockdown in response to the COVID-19 pandemic. Based on previous experience with infectious disease outbreaks, quarantine, lockdown, and physical distancing are unpleasant experiences, involving separation from loved ones, uncertainty, and unemployment (12), increased mental distress and post-traumatic symptoms (13–15), anger and irritability (11, 16), depressive symptoms and somatic complaints (17, 18), insomnia (19, 20), suicidal ideation (21, 22), lack of motivation and loneliness (11, 16, 23, 24). In the general population, the adoption of different coping styles (25), the levels of resilience (26) and familiarity with mental disorders (27) have been identified as the most relevant moderators of the impact of the pandemic on mental health (2).
Loneliness is defined as a negative emotion related with the discrepancy between desired and existing relations, and it can be either emotional and social (28, 29). Emotional loneliness is described as a subjective experience resulting from the absence of a close bonding with a person, whereas social loneliness reflects an objective lack of contacts and social networks (30, 31).
Loneliness represents a major public health concern, since it is associated with an increased risk of depressive disorders, anxiety disorders, and suicidal ideation (32), as well as of cardiovascular disease, stroke, coronary heart disease (33, 34), cognitive decline (35), and increased all-cause mortality risk (36–38).
Loneliness and its related negative feelings are thought to be particularly pronounced during adolescence and young adulthood (39) because of the many social and personal changes that young people deal with during this period of life (40–43). Loneliness itself has been referred to as an epidemic, and there have been heightened concerns about its effects during the COVID-19 pandemic (8, 44–46). Therefore, it is essential to evaluate the type of impact of the pandemic and the levels of loneliness experienced by young people (47). By disentangling such complex relationship between pandemic and loneliness, it would be possible to develop ad-hoc preventive strategies targeting the young people (48–50), which are expected to be the most severely hit by the long-term consequences of the pandemic (51–53).
Based on the largest Italian study on the effects of the COVID-19 pandemic on the mental health of general population (27), in this paper we aim to: (1) describe the levels of loneliness in a national sample of Italian young adults aged 18–34 years, during the first wave of lockdown in 2020; (2) evaluate the clinical and socio-demographic differences in young adults reporting low vs. high levels of loneliness; (3) assess the role of clinical symptomatology, coping strategies, levels of resilience, and duration of lockdown as possible predictors of loneliness.
Materials and Methods
The COvid Mental hEalth Trial (COMET) is a national trial coordinated by the University of Campania “Luigi Vanvitelli” (Naples) in collaboration with nine university sites: Università Politecnica delle Marche (Ancona), University of Ferrara, University of Milan Bicocca, University of Milan “Statale,” University of Perugia, University of Pisa, Sapienza University of Rome, “Catholic” University of Rome, University of Trieste. The Center for Behavioral Sciences and Mental Health of the National Institute of Health in Rome has been involved in the study by supporting the dissemination and implementation of the project according to the clinical guidelines produced by the National Institute of Health for managing the effects of the COVID-19 pandemic. The COMET was conceived as a cross-sectional observational design using a snowball sampling method for the recruitment of the Italian general population. The full study protocol is available elsewhere (54).
The main outcome measure of the study is the DASS-21, evaluating the general distress on a tripartite model of psychopathology (55, 56). It consists of 21 items grouped in three subscales: depression, anxiety and stress.
The levels of loneliness have been evaluated by the UCLA scale short version, which includes 10 items rated on a 4-level Likert scale (57). Higher values indicate higher levels of loneliness. As reported by Morahan-Martin and Schumacher (58), participants in the highest 20% of responses were classified as “Lonely,” compared with all other participants (“Non-lonely”).
Respondents' socio-demographic (e.g., gender, age, geographical region, working, and housing condition, etc.) and clinical information (e.g., having a previous physical or mental disorder, using illicit drugs or medications, etc.) have been collected through ad-hoc schedules. Other validated and reliable questionnaires included in the study are: the General Health Questionnaire-12 items version (GHQ) (59); the Obsessive-Compulsive Inventory—Revised version (OCI-R) (60), the Insomnia Severity Index (ISI) (61), the Suicidal Ideation Attributes Scale (SIDAS) (62), the Severity-of-Acute-Stress-Symptoms-Adult scale (SASS) (63), the Impact of Event Scale—short version (IES) (64), the Connor-Davidson resilience scale (65), the brief-COPE (66), the short form of Post-Traumatic Growth Inventory (PTGI) (67), the Multidimensional Scale of Perceived Social Support (MSPPS) (68), and (only for healthcare professionals) the Maslach Burnout Inventory (MBI) (69). The present paper is based on a sub-analysis of the sample of young people. A previous survey promoted by the International Labor Organization in the UK, entitled “Youth and COVID-19,” has selected participants aged 18–34 years and therefore the same age group has been considered in the present paper (70).
Ethics and Dissemination
This study is being conducted in accordance with globally accepted standards of good practice, in agreement with the Declaration of Helsinki and with local regulations.
The participants provided their written informed consent to participate in this study. The study has been approved by the Ethical Review Board of the University of Campania “L. Vanvitellii” (Protocol number:0007593/i).
Statistical Analysis
Descriptive statistics were performed in order to describe the socio-demographic and clinical characteristics of the sample. T-test for independent samples and Chi-square have been performed to test differences between “lonely” vs. “non-lonely” participants, as appropriate.
In order to identify possible predictors of the levels of loneliness, a multivariate linear regression model, weighted for the propensity score, was performed, including as independent variables: adaptive and maladaptive coping strategies, having been infected by the COVID-19, having a pre-existing mental disorder, being a healthcare professional. Furthermore, in order to evaluate the impact of the duration of lockdown and of other containment measures on the primary outcomes, the categorical variable “Week” was also entered in the regression models. The models were adjusted for the rate of new COVID-19 cases and of COVID-related mortality during the study period, as well as for several socio-demographic characteristics, such as gender, age, occupational status, having a physical comorbid condition, hours spent on Internet, health status, number of cohabiting people, satisfaction with one's own life, with cohabiting people, and with housing condition. All variables have been managed as reported in detail elsewhere (27).
Missing data have been handled using the multiple imputation approach. Statistical analyses were performed using the Statistical Package for Social Sciences (SPSS), version 17.0 and STATA, version 15. For all analyses, the level of statistical significance was set at p < 0.05.
Results
Global Sample
The final sample consists of 8,584 people, mainly female (72.6%, N = 6,232), single, with a mean age of 26.4 (±4.4). 58.2% of them (N = 5,000) have a university degree and 71.4% (N = 6,131) are single; 7.1% of respondents have lost their job or interrupted their studies during the pandemic.
The majority of participants reported to enjoy their living conditions (66.8%, N = 5,732) and to live with their co-habitants (70.5%, N = 6,055), while 24% of participants (N = 2,094) reported not to be satisfied with their own life. 5.4% (N = 461) participants reported to suffer from a mental disorder and 6.7% (N = 573) of a physical disorder.
The mean score at the UCLA was 47.5 (±13.6), with 27% (N = 2,311) of respondents exceeding the cut-off for high levels of loneliness (Table 1, Figure 1).
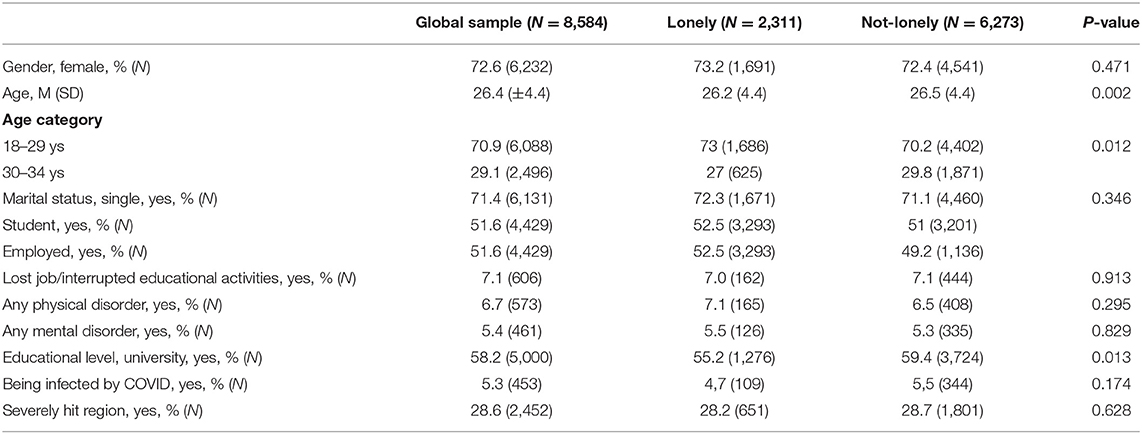
Table 1. Socio-demographic characteristics of the sample (N = 8,584).
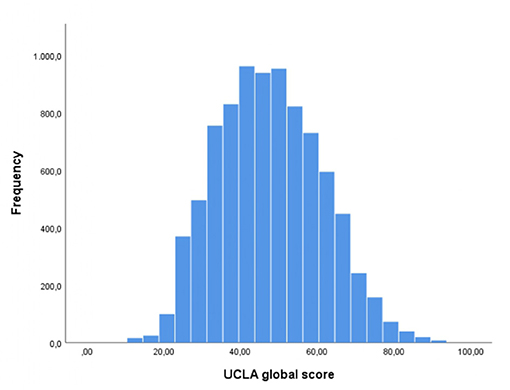
Figure 1. Distribution of the levels of loneliness.
Differences in “Lonely” vs. “Non-lonely” Respondents
Participants from the “lonely” group reported a higher severity of depressive, anxiety, and stress-related symptoms (DASS-Depression: 13.8 ± 6.8; DASS-anxiety: 8.7 ± 7.0; DASS-stress:17.2 ± 6.1), compared to the “non-lonely” sample (p < 0.0001) (Table 2).
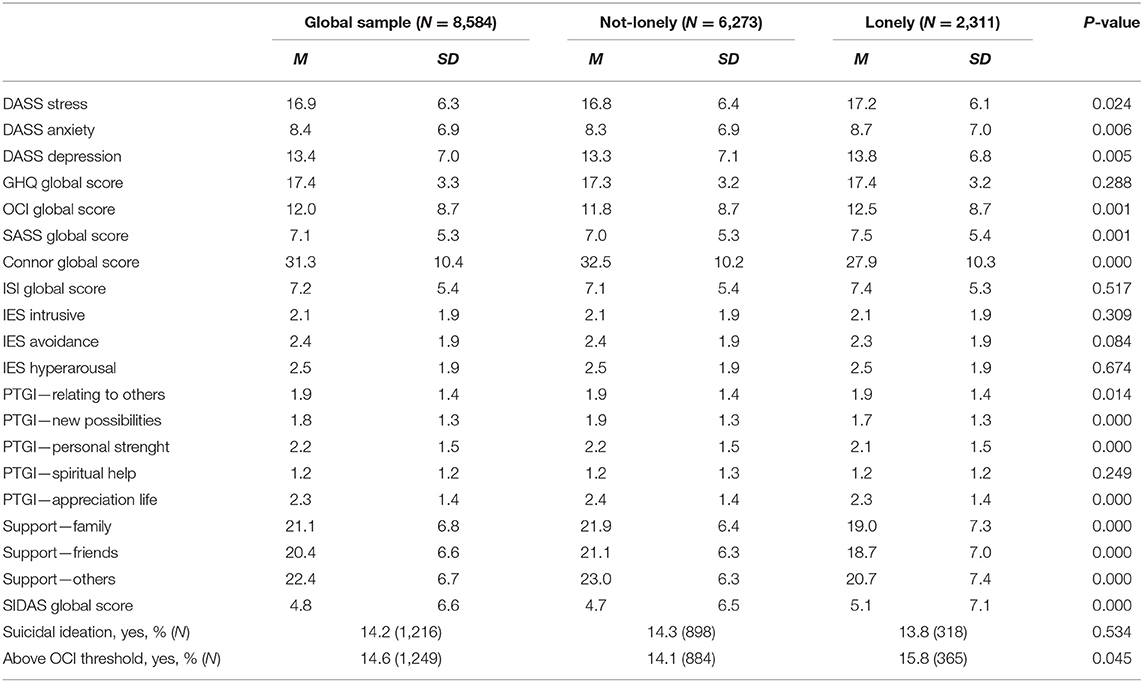
Table 2. Differences in clinical features between lonely and not-lonely participants.
Moreover, 15.8% (N = 365) of the “lonely” sample scored above the threshold for clinical relevance of obsessive-compulsive symptomatology, with a global severity of obsessive–compulsive symptoms of 12.5 ± 8.7 at OCI-R, significantly higher than the “non-lonely” group (p < 0.05). Suicidal ideation was reported by 13.8% (N =318) of the “lonely” group, with a mean score of 5.1 ± 7.1 at the SIDAS, compared to the 14.3% in the “not-lonely group” (4.7 ± 6.5).
The levels of resilience were significantly lower in participants from the “lonely” group, compared with the remaining sample (p < 0.0001).
People from the “lonely” group also reported to use maladaptive coping strategies very frequently. In particular, self-distraction was frequently used in 38% of cases (vs. 24% of cases in the “non-lonely” group, p < 0.0001), self-blame in 25% of cases (vs. 14.4%, p < 0.0001) and venting in 15.4% (vs. 8.4%, p < 0.0001). On the contrary, people from the “non-lonely” group more frequently used adaptive coping strategies, such as acceptance (47.7% of cases vs. 35.1%; p < 0.0001), planning (40.3 vs. 32%; p < 0.0001), and positive reframing (29% vs. 21.2%; p < 0.0001).
Predictors of Loneliness
According to the multivariate regression model, weighted for the propensity score, high levels of loneliness were predicted by the presence of avoidant coping strategies, such as self-distraction (Beta coefficient, B = 0.369, 95% Confidence Interval, 95% CI = 0.328–0.411), venting (B = 0.245, 95% CI = 0.197–0.293), denial (B = 0.110, 95% CI = 0.061–0.159), and emotional disengagement (B = 0.133, 95% CI = 0.080–0.185). Interestingly, the levels of loneliness were reduced by using adaptive coping strategies, such as search for information (B = −0.125, 95% CI = −0.184 to −0.066), planning (B = −0.106, 95% CI = −0.159 to −0.053) and positive reframing (B = −0.080, 95% CI= −0.127 to −0.034).
Weeks of exposure to the pandemic and to the related containment measures were significantly associated with worsening of loneliness, with Beta coefficient ranging from B = 0.4 (95% CI: 0.078–0.830) during the week April 16–22 to B = 0.323 (95% CI: 0.112–0.534) in the week April 30–May 4 (p < 0.000).
Being infected by COVID-19 and having a pre-existing mental or physical disorder did not impact on the levels of perceived loneliness, even after controlling for gender, age, living in the most severely affected areas, infection rate, and mortality rate for COVID-19 in Italy. We also found that the severity of depressive, anxiety or stress symptoms, of obsessive-compulsive symptoms, of insomnia, post-traumatic symptoms, and suicidal ideation did not have any influence on the levels of loneliness (Table 3).
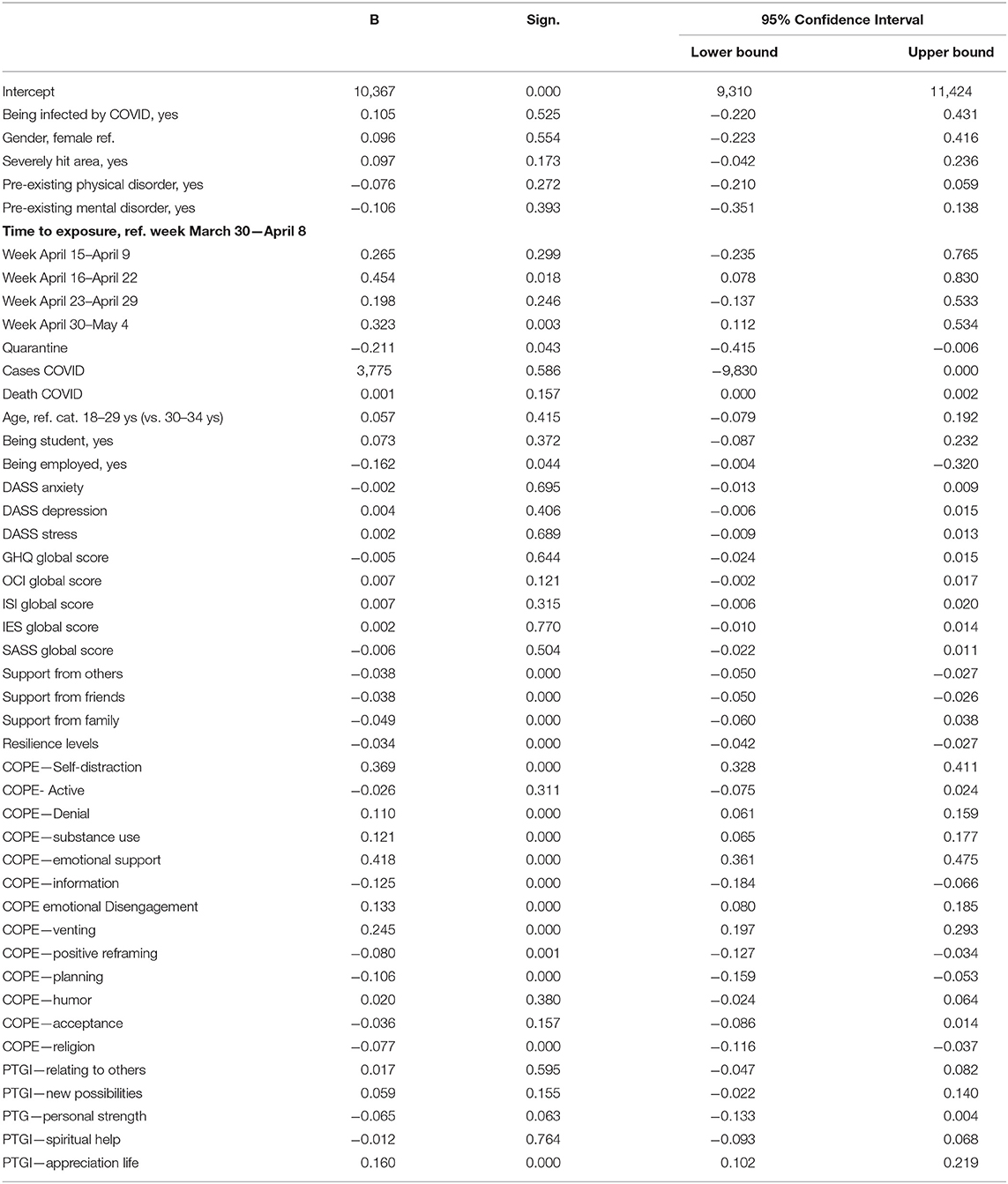
Table 3. Predictors of the levels of loneliness.
Finally, high levels of post-traumatic growth, such as appreciation for life (B = 0.160, 95% CI = 0.102–0.219) were a significant protective factor for levels of loneliness (Table 3).
Discussion
The COVID-19 pandemic represents an unprecedent traumatic event, which has completely disrupted the daily routine of the general population worldwide for more than a year now (71). The mental health of young adults has not been fully considered during the first weeks of the pandemic, although it was clear already from the beginning that young people would have been a group at higher risk of developing long-term physical, mental and social problems (72). In particular, the enforced physical isolation due to the public health containment measures can be associated with a subjective feeling of loneliness, which represent a specific dimension to be carefully monitored for the prevention of mental health problems (73). In many individuals, especially the younger ones, the lockdown and physical distancing can have increased the perception of social isolation. Although social isolation—defined as the absence of social interactions, contacts and relationships with others—is conceptually distinguished from loneliness—that is the feeling that one's social needs are not being met by the quantity or quality of one's social relationships, these two dimensions appear to be strongly interrelated, with physical and social isolation being a risk factor for becoming “lonely” (74).
During the ongoing health crisis, there have been calls to ascertain how the pandemic has affected loneliness to ensure that at-risk individuals receive all the necessary support. Therefore, in our study we decided to describe the levels of loneliness in a national sample of Italian adults, during the first wave of the lockdown in 2020, as one of the considered outcome measures.
In the sub-sample of young people aged 18–34 years, the levels of loneliness were quite high, being particularly severe in a third of cases. This is an expected finding, in line with those from other studies carried out in Europe, which highlighted that younger adults, women, people with low income, and those with mental health problems are more likely to be in the highest loneliness class relative to the lowest (75, 76). According to the COVID-19 Psychological Well-being study, people of younger age reported more severe levels of loneliness and were four to five times more likely to report loneliness, compared with older adults (77). In a sample of US young adults aged 18–35 years, the prevalence of loneliness was estimated at 43% (78). In this sample, results indicated a trend toward moderate levels of loneliness, with women reporting significantly more feelings of loneliness compared to men. In our sample, we did not find gender differences in the levels of loneliness, but this finding could be due to the overrepresentation of female population compared to male.
Furthermore, young people in the highest loneliness cluster reported a higher severity of depressive, anxiety and stress symptoms, of obsessive-compulsive symptomatology, and a high rate of suicidal ideation, even compared with the global COMET sample (27). As expected, people belonging to the group with highest rates of loneliness were those with more severe levels of psychiatric symptoms, confirming that loneliness is strongly associated with depression and other mental disorders both in old (79) and young adults (80, 81). Although loneliness has been traditionally linked with older adults (32, 82, 83), even young adults up to the age of 25 may experience high levels of loneliness (55, 84). These data confirm the hypothesis that loneliness can represent a useful dimension to be carefully monitored in routine clinical practice by healthcare professionals working with adolescents and young people (85, 86).
Another interesting finding is that adaptive coping strategies, such as planning and positive reframing, work as protective factors against loneliness. This is a relevant finding considering that coping strategies may easily change following specific psychosocial interventions, such as psychoeducation (87, 88) and problem-solving oriented interventions (89) or by improving the levels of resilience (25, 81, 90, 91).
Furthermore, we also found that the levels of loneliness tend to increase over time, being more severe in the last weeks of the lockdown, as confirmed in our regression models controlled for all respondents' socio-demographic characteristics. This finding confirms the hypothesis that the duration of containment measures significantly influences mental health and well-being of the general population (27, 92, 93). The same trend in the levels of self-reported loneliness was reported by Bu et al. (76), who described a U-shaped trajectory in the levels of loneliness in the period June-November 2020, corresponding to the limitations to social activities due to the lockdown policies (94). In fact, young people aged between 18 and 29 reported higher levels of loneliness, but with a decrease in loneliness in the first period of the pandemic, from March to May 2020 (76, 95–97).
In addition, being employed and being a student were associated with a lower risk of loneliness during the pandemic. This is consistent with Arnett's theory (98) that working and education status might potentially be signs of age-specific personal achievements (99). Moreover, school and workplace may also help young adults to increase their social network and to reduce social disconnection (100–102). Prolonged school closures, strict social isolation from peers, extended family, and community networks, economic shutdown, and the pandemic itself may have contributed to the mental health problems of many adolescents and young adults (103–105). Being confined to home leads to disturbances in sleep/wake cycles and physical exercise routines, and promotes the excessive use of technology (106–109). Further studies are needed in order to evaluate the long-term effects of these conditions on the development of full-blown mental health disorders (110, 111).
The present study has some limitations which are hereby acknowledged. First, the snowball sampling methodology could have led to a selection bias, with only those interested in the psychological consequences of the pandemic willing to participate (112). Second, the cross-sectional design of the survey prevents us to delineate any causal relationship between the selected variables. Third, several variables which could have had an impact on the levels of perceived loneliness, such number of contacts with peers (prior and during the pandemic), time spent with friends/peer, quality of social relationship, number of social activities in which they are usually involved, desire for social contact (113–115), the quality of family communication styles, and the individual acceptance and attitudes toward restrictive measures related to the pandemic, have not been collected in our study. Fourth, it is very difficult to disentangle the complex relationship between the exposure to COVID-19 pandemic and other contextual factors contributing to the levels of loneliness. In this study, the proxy measure selected is represented by the variable “weeks of lockdown,” but it should be acknowledged that many other variables could have had an influence on the loneliness levels.
Finally, our sample cannot be considered fully generalizable of all young people because we could recruit only people aged 18 years or more.
Among its strengths, we should consider that this is one largest surveys carried out in Italy on the effects of the COVID-19 pandemic on the mental health and well-being of the general population. Moreover, given the large sample size, we could analyze differences and similarities between young and old people, but also between males and females (116). Finally, the large battery of used tests allowed us to test the effects of loneliness on several mental health dimensions and symptoms.
Overall, our findings suggest that the levels of loneliness during the weeks of the first strict lockdown were high in young adults. People using maladaptive coping strategies, such as self-blame or self-distraction, were at higher risk for reporting highest levels of loneliness. However, certain social factors such as having close friends, having strong perceived social support, having high levels of resilience and using adaptive coping strategies were protective factors. There is currently considerable interest in trying to reduce loneliness within society, both within the context of COVID-19 pandemic and more generally (117–121). Our results highlight that young people are at a higher risk of developing loneliness and suggest that more interventions and practical guidelines are needed.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethical Committee of the University of Campania L. Vanvitelli. The participants provided their written informed consent to participate in this study.
Author Contributions
VG, GSam, and AF: conceptualization. ML and VV: methodology. GS: formal analysis. UA, CC, GSan, GC, MP, UV, BD, MBM, and FC: investigation. GS, VB, and GM: writing—original draft preparation. AF, UA, CC, GSan, MP, UV, BD, MBM, and FC: writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor declared a shared affiliation with one of the authors UV at the time of review.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Twenge JM, Joiner TE. Mental distress among U.S. adults during the COVID-19 pandemic. J Clin Psychol. (2020) 76:2170–82. doi: 10.1002/jclp.23064
2. Fiorillo A, Gorwood P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur Psychiatry. (2020) 63:e32. doi: 10.1192/j.eurpsy.2020.35
3. Marazziti D, Stahl SM. The relevance of COVID-19 pandemic to psychiatry. World Psychiatry. (2020) 19:261. doi: 10.1002/wps.20764
4. Unützer J, Kimmel RJ, Snowden M. Psychiatry in the age of COVID-19. World Psychiatry. (2020) 19:130–131. doi: 10.1002/wps.20766
5. Golberstein E, Wen H, Miller BF. Coronavirus disease 2019 (COVID-19) and mental health for children and adolescents. JAMA Pediatr. (2020) 174:819–20. doi: 10.1001/jamapediatrics.2020.1456
6. Adhanom Ghebreyesus T. Addressing mental health needs: an integral part of COVID-19 response. World Psychiatry. (2020) 19:129–30. doi: 10.1002/wps.20768
7. Abed R, Brüne M, Wilson DR. The role of the evolutionary approach in psychiatry. World Psychiatry. (2019) 18:370–1. doi: 10.1002/wps.20688
8. Silva Junior FJGD, Sales JCES, Monteiro CFS, Costa APC, Campos LRB, Miranda PIG, et al. Impact of COVID-19 pandemic on mental health of young people and adults: a systematic review protocol of observational studies. BMJ Open. (2020) 10:e039426. doi: 10.1136/bmjopen-2020-039426
9. D'Onofrio B, Emery R. Parental divorce or separation and children's mental health. World Psychiatry. (2019) 18:100–101. doi: 10.1002/wps.20590
10. Balanzá-Martínez V, Atienza-Carbonell B, Kapczinski F, Boni De, Lifestyle RB. behaviours during the COVID-19 - time to connect. Acta Psychiatr Scand. (2020) 141:399–400. doi: 10.1111/acps.13177
11. Chew NWS, Lee GKH, Tan BYQ, Jing M, Goh Y, Ngiam NJH, et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav Immun. (2020) 88:559–65. doi: 10.1016/j.bbi.2020.04.049
12. Pompili M, Innamorati M, Sampogna G, Albert U, Carmassi C, Carrà G, et al. The impact of Covid-19 on unemployment across Italy: consequences for those affected by psychiatric conditions. J Affect Disord. (2021) 296:59–66. doi: 10.1016/j.jad.2021.09.035
13. Bryant RA. Post-traumatic stress disorder: a state-of-the-art review of evidence and challenges. World Psychiatry. (2019) 18:259–69. doi: 10.1002/wps.20656
14. Morina N, Sterr TN. Lack of evidence for the efficacy of psychotherapies for PTSD and depression in child and adolescent refugees. World Psychiatry. (2019) 18:107–8. doi: 10.1002/wps.20596
15. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20.
16. Torales J, O'Higgins M, Castaldelli-Maia JM, Ventriglio A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int J Soc Psychiatry. (2020) 66:317–20. doi: 10.1177/0020764020915212
18. Li J, Yang Z, Qiu H, Wang Y, Jian L, Ji J, et al. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry. (2020) 19:249–50. doi: 10.1002/wps.20758
19. Krystal AD, Prather AA, Ashbrook LH. The assessment and management of insomnia: an update. World Psychiatry. (2019) 18:337–52. doi: 10.1002/wps.20674
20. Morin CM, Carrier J. The acute effects of the COVID-19 pandemic on insomnia and psychological symptoms. Sleep Med. (2020) 77:346–7. doi: 10.1016/j.sleep.2020.06.005
21. Wasserman D, Iosue M, Wuestefeld A, Carli V. Adaptation of evidence-based suicide prevention strategies during and after the COVID-19 pandemic. World Psychiatry. (2020) 19:294–306. doi: 10.1002/wps.20801
22. McIntyre RS, Lee Y. Preventing suicide in the context of the COVID-19 pandemic. World Psychiatry. (2020) 19:250–1. doi: 10.1002/wps.20767
23. Voitsidis P, Kerasidou MD, Nikopoulou AV, Tsalikidis P, Parlapani E, Holeva V, et al. A systematic review of questionnaires assessing the psychological impact of COVID-19. Psychiatry Res. (2021) 305:114183.
24. Kim MH, An JH, Lee HR, Jeong SH, Hwang SJ, Hong JP. Social isolation, loneliness and their relationships with mental health status in South Korea. Psychiatry Investig. (2021) 18:652–60.
25. Sampogna G, Del Vecchio V, Giallonardo V, Luciano M, Albert U, Carmassi C, et al. What Is the Role of Resilience and Coping Strategies on the Mental Health of the General Population during the COVID-19 Pandemic? Results from the Italian Multicentric COMET Study. Brain Sci. (2021) 11:1231.
26. Feldman R. What is resilience: an affiliative neuroscience approach. World Psychiatry. (2020) 19:132–50. doi: 10.1002/wps.20729
27. Fiorillo A, Sampogna G, Giallonardo V, Del Vecchio V, Luciano M, Albert U, et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: results from the COMET collaborative network. Eur Psychiatry. (2020) 63:e87. doi: 10.1192/j.eurpsy.2020.89
28. Weiss RS. Loneliness: The Experience of Emotional and Social Isolation. Cambridge, MA: The MIT Press (1973).
29. Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two population-based studies. Res Aging. (2004) 26:655–672. doi: 10.1177/0164027504268574
30. Jong Gierveld D, Van Tilburg T. A 6-item scale for overall, emotional, and social loneliness: confirmatory tests on survey data. Res Aging. (2006) 28:582–98. doi: 10.1177/0164027506289723
31. Green MF, Lee J, Wynn JK. Experimental approaches to social disconnection in the general community: can we learn from schizophrenia research? World Psychiatry. (2020) 19:177–8. doi: 10.1002/wps.20734
32. Beutel ME, Klein EM, Brähler E, Reiner I, Jünger C, Michal M, et al. Loneliness in the general population: prevalence, determinants and relations to mental health. BMC Psychiatr. (2017) 17:97. doi: 10.1186/s12888-017-1262-x
33. Steptoe A, Owen N, Kunz-Ebrecht SR, Brydon L. Loneliness and neuroendocrine, cardiovascular, and inflammatory stress responses in middle-aged men and women. Psychoneuroendocrinology. (2004) 29:593–611. doi: 10.1016/S0306-4530(03)00086-6
34. Williams RB. Loneliness and social isolation and increased risk of coronary heart disease and stroke: clinical implications. Heart. (2016) 102:2016. doi: 10.1136/heartjnl-2016-310073
35. Donovan NJ, Wu Q, Rentz DM, Sperling RA, Marshall GA, Glymour MM. Loneliness, depression and cognitive function in older US adults. Int J Geriatr Psychiatr. (2017) 32:564–73. doi: 10.1002/gps.4495
36. Lara E, Moreno-Agostino D, Martín-María N, Miret M, Rico-Uribe LA, Olaya B, et al. Exploring the effect of loneliness on all-cause mortality: are there differences between older adults and younger and middle-aged adults? Soc Sci Med. (2020) 258:113087. doi: 10.1016/j.socscimed.2020.113087
37. Rico-Uribe LA, Caballero FF, Martín-María N, Cabello M, Ayuso-Mateos JL, Miret M. Association of loneliness with all-cause mortality: a meta-analysis. PLoS ONE. (2018) 13:e0190033. doi: 10.1371/journal.pone.0190033
38. Hawkley LC, Cacioppo JT. Loneliness and pathways to disease. Brain Behav Immun. (2003) 17:98–05. doi: 10.1016/S0889-1591(02)00073-9
39. Brennan T. Loneliness at adoles-cence. In: Peplau LA, Perlman D, editors. Loneliness: A Sourcebook of Current Theory, Research, Therapy. New York, NY: Wiley Interscience (1982). p. 269–90.
40. Alegria M, Shrout PE, Canino G, Alvarez K, Wang Y, Bird H, et al. The effect of minority status and social context on the development of depression and anxiety: a longitudinal study of Puerto Rican descent youth. World Psychiatry. (2019) 18:298–307. doi: 10.1002/wps.20671
41. Widiger TA, Crego C. The Five Factor Model of personality structure: an update. World Psychiatry. (2019) 18:271–2. doi: 10.1002/wps.20658
42. Squeglia LM. Alcohol and the developing adolescent brain. World Psychiatry. (2020) 19:393–4. doi: 10.1002/wps.20786
43. Goossens L. Emotion, affect, and loneliness in adolescence. In: Jackson S, Goossens L, editors. Handbook of Adolescent Development. Psychology Press (2006). p. 51–70.
44. Hards E, Loades ME, Higson-Sweeney N, Shafran R, Serafimova T, Brigden A, et al. Loneliness and mental health in children and adolescents with pre-existing mental health problems: a rapid systematic review. Br J Clin Psychol. (2020). doi: 10.1111/bjc.12331. [Epub ahead of print].
45. Cielo F, Ulberg R, Di Giacomo D. Psychological Impact of the COVID-19 outbreak on mental health outcomes among youth: a rapid narrative review. Int J Environ Res Public Health. (2021) 18:6067. doi: 10.3390/ijerph18116067
46. Forte A, Orri M, Brandizzi M, Iannaco C, Venturini P, Liberato D, et al. “My Life during the Lockdown”: emotional experiences of European adolescents during the COVID-19 Crisis. Int J Environ Res Public Health. (2021) 18:7638. doi: 10.3390/ijerph18147638
47. Rosen ML, Rodman AM, Kasparek SW, Mayes M, Freeman MM, Lengua LJ, et al. Promoting youth mental health during the COVID-19 pandemic: A longitudinal study. PLoS One. (2021) 16:e0255294. doi: 10.1371/journal.pone.0255294
48. Stewart DE, Appelbaum PS. COVID-19 and psychiatrists' responsibilities: a WPA position paper. World Psychiatry. (2020) 19:406–407. doi: 10.1002/wps.20803
49. Masi CH, Chen CH, Hawkley LC. A meta-analysis of interventions to reduce loneliness. Personal Soc Psychol Rev. (2011) 15:219–66. doi: 10.1177/1088868310377394
50. Mann F, Bone JK, Lloyd-Evans B, Frerichs J, Pinfold V, Ma R, et al. A life less lonely: the state of the art in interventions to reduce loneliness in people with mental health problems. Soc Psychiatry Psychiatr Epidemiol. (2017) 52:627–38. doi: 10.1007/s00127-017-1392-y
51. Pai N, Vella SL. COVID-19 and loneliness: a rapid systematic review. Aust N Z J Psychiatry. (2021) 13:48674211031489. doi: 10.1177/00048674211031489
52. Rooksby M, Furuhashi T, McLeod HJ. Hikikomori: a hidden mental health need following the COVID-19 pandemic. World Psychiatry. (2020) 19:399–400. doi: 10.1002/wps.20804
53. Kato TA, Kanba S, Teo AR. Defining pathological social withdrawal: proposed diagnostic criteria for hikikomori. World Psychiatry. (2020) 19:116–7. doi: 10.1002/wps.20705
54. Giallonardo V, Sampogna G, Del Vecchio V, Luciano M, Albert U, Carmassi C, et al. The impact of quarantine and physical distancing following COVID-19 on mental health: study protocol of a multicentric Italian population trial. Front Psychiatry. (2020) 11:533. doi: 10.3389/fpsyt.2020.00533
55. Lim MH, Holt-Lunstad J, Badcock JC. Loneliness: contemporary insights into causes, correlates, and consequences. Soc Psychiatry Psychiatr Epidemiol. (2020) 55:789–91. doi: 10.1007/s00127-020-01891-z
56. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety & Stress Scales. 2nd ed. Sydney, NSW: Psychology Foundation (1995).
57. Hays RD, Di Matteo MR. A short-form measure of loneliness. J Pers Assess. (1987) 51:69–81. doi: 10.1207/s15327752jpa5101_6
58. Morahan-Martin J, Schumacher P. Loneliness and social uses of the Internet. Comput Hum Behav. (2003) 196:659–71. doi: 10.1016/S0747-5632(03)00040-2
59. Goldberg DP, Gater R, Sartorius N, Ustun TB, Piccinelli M, Gureje O, et al. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol Med. (1997) 27:191–7. doi: 10.1017/S0033291796004242
60. Foa EB, Huppert JD, Leiberg S, Langner R, Kichic R, Hajcak G, et al. The Obsessive-Compulsive Inventory: development and validation of a short version. Psychol Assess. (2002) 14:485–96. doi: 10.1037/1040-3590.14.4.485
61. Morin CM, Belleville G, Bélanger L, Ivers H. The Insomnia Severity Index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. (2011) 34:601–8. doi: 10.1093/sleep/34.5.601
62. van Spijker BA, Batterham PJ, Calear AL, Farrer L, Christensen H, Reynolds J, et al. The suicidal ideation attributes scale (SIDAS): community-based validation study of a new scale for the measurement of suicidal ideation. Suicide Life Threat Behav. (2014) 44:408–19. doi: 10.1111/sltb.12084
63. Kilpatrick DG, Resnick HS, Friedman MJ. Severity of Acute Stress Symptoms-Adult (National Stressful Events Survey Acute Stress Disorder Short Scale [NSESSS]). Washington, DC: American Psychiatric Association (2013).
64. Thoresen S, Tambs K, Hussain A, Heir T, Johansen VA, Bisson JI. Brief measure of posttraumatic stress reactions: Impact of Event Scale-6. Soc Psychiatry Psychiatr Epidemiol. (2010) 45:405–12.
65. Connor KM, Davidson JRT. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC) Depress. Anxiety. (2003) 18:71–82.
67. Cann A, Calhoun LG, Tedeschi RG, Taku K, Vishnevsky T, Triplett KN, et al. A short form of the posttraumatic growth inventory. Anxiety Stress Coping. (2010) 23:127–37.
68. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Personal Assess. (1988) 1:30–41. doi: 10.1207/s15327752jpa5201_2
69. Maslach C, Jackson SE. MBI: Maslach Burnout Inventory. Palo Alto, CA: Consulting Psychologists Press (1981).
70. International Labour Organization. Youth and COVID-19: Impacts on Jobs, Education, Rights and Mental Well-Being. Geneva (2020).
71. Gorwood P, Fiorillo A. One year after the COVID-19: what have we learnt, what shall we do next? Eur Psychiatry. (2021) 64:e15. doi: 10.1192/j.eurpsy.2021.9
72. Binagwaho A. We need compassionate leadership management based on evidence to defeat COVID-19. Int J Health Policy Manag. (2020) 9:413–4. doi: 10.34172/ijhpm.2020.73
73. Reinhardt GY, Vidovic D, Hammerton C. Understanding loneliness: a systematic review of the impact of social prescribing initiatives on loneliness. Perspect Public Health. (2021) 141:204–13. doi: 10.1177/1757913920967040
74. Holt-Lunstad J. A pandemic of social isolation? World Psychiatry. (2021) 20:55–6. doi: 10.1002/wps.20839
75. Hu Y, Gutman LM. The trajectory of loneliness in UK young adults during the summer to winter months of COVID-19. Psychiatry Res. (2021) 303:114064. doi: 10.1016/j.psychres.2021.114064
76. Bu F, Steptoe A, Fancourt D. Loneliness during a strict lockdown: trajectories and predictors during the COVID-19 pandemic in 38,217 United Kingdom adults. Soc Sci Med. (2020) 265:113521. doi: 10.1016/j.socscimed.2020.113521
77. Groarke JM, McGlinchey E, McKenna-Plumley PE, Berry E, Graham-Wisener L, Armour C. Examining temporal interactions between loneliness and depressive symptoms and the mediating role of emotion regulation difficulties among UK residents during the COVID-19 lockdown: longitudinal results from the COVID-19 psychological wellbeing study. J Affect Disord. (2021) 285:1–9. doi: 10.1016/j.jad.2021.02.033
78. Killgore WDS, Cloonan SA, Taylor EC, Miller MA, Dailey NS. Three months of loneliness during the COVID-19 lockdown. Psychiatry Res. (2020) 293:113392. doi: 10.1016/j.psychres.2020.113392
79. Domènech-Abella J, Mundó J, Haro JM, Rubio-Valera M. Anxiety, depression, loneliness and social network in the elderly: longitudinal associations from The Irish Longitudinal Study on Ageing (TILDA). J Affect Disord. (2019) 246:82–8. doi: 10.1016/j.jad.2018.12.043
80. Richard A, Rohrmann S, Vandeleur CL, Schmid M, Barth J, Eichholzer M. Loneliness is adversely associated with physical and mental health and lifestyle factors: results from a Swiss national survey. PLoS One. (2017) 12:e0181442. doi: 10.1371/journal.pone.0181442
81. Reynolds CF. Optimizing personalized management of depression: the importance of real-world contexts and the need for a new convergence paradigm in mental health. World Psychiatry. (2020) 19:266–268. doi: 10.1002/wps.20770
82. Dykstra PA. Older adult loneliness: myths and realities. Eur J Ageing. (2009) 6:91–100. doi: 10.1007/s10433-009-0110-3
83. Boss L, Kang D.- H, Branson S. Loneliness and cognitive function in the older adult: a systematic review. Int Psychogeriatr. (2015) 27:541. doi: 10.1017/S1041610214002749
84. Child ST, Lawton L. Loneliness and social isolation among young and late middle-age adults: associations with personal networks and social participation. Aging Ment Health. (2019) 23:196–204. doi: 10.1080/13607863.2017.1399345
85. Maj M, Stein DJ, Parker G, Zimmerman M, Fava GA, Hert D, et al. The clinical characterization of the adult patient with depression aimed at personalization of management. World Psychiatry. (2020) 19:269–93. doi: 10.1002/wps.20771
86. Cooper K, Hards E, Moltrecht B, Reynolds S, Shum A, McElroy E, Loades M. Loneliness, social relationships, and mental health in adolescents during the COVID-19 pandemic. J Affect Disord. (2021) 289:98–104. doi: 10.1016/j.jad.2021.04.016
87. Sampogna G, Luciano M, Del Vecchio V, Malangone C, De Rosa C, Giallonardo V, et al. The effects of psychoeducational family intervention on coping strategies of relatives of patients with bipolar I disorder: results from a controlled, real-world, multicentric study. Neuropsychiatr Dis Treat. (2018) 14:977–89. doi: 10.2147/NDT.S159277
88. Gabrielli S, Rizzi S, Bassi G, Carbone S, Maimone R, Marchesoni M, et al. Engagement and effectiveness of a healthy-coping intervention via chatbot for university students during the COVID-19 pandemic: mixed methods proof-of-concept study. JMIR Mhealth Uhealth. (2021) 9:e27965. doi: 10.2196/27965
89. Hentati A, Forsell E, Ljótsson B, Kraepelien M. Practical and emotional problems reported by the general public during the COVID-19 pandemic when using a self-guided digital problem-solving intervention: a content analysis. JMIR Form Res. (2021) 5:e31722. doi: 10.2196/31722
90. Masten AS. Resilience from a developmental systems perspective. World Psychiatry. (2019) 18:101–2. doi: 10.1002/wps.20591
91. Golemis A, Voitsidis P, Parlapani E, Nikopoulou VA, Tsipropoulou V, Karamouzi P, et al. Young adults' coping strategies against loneliness during the COVID-19-related quarantine in Greece. Health Promot Int. (2021) daab053. doi: 10.1093/heapro/daab053
92. Sibley CG, Greaves LM, Satherley N, Wilson MS, Overall NC, Lee CHJ, et al. Effects of the COVID-19 pandemic and nationwide lockdown on trust, attitudes toward government, and well-being. Am Psychol. (2020) 75:618–30. doi: 10.1037/amp0000662
93. Gross JJ, Uusberg H, Uusberg A. Mental illness and well-being: an affect regulation perspective. World Psychiatry. (2019) 18:130–9. doi: 10.1002/wps.20618
94. Wang J, Mann F, Lloyd-Evans B, Ma R, Johnson S. Associations between loneliness and perceived social support and outcomes of mental health problems: a systematic review. BMC Psychiatr. (2018) 18:156. doi: 10.1186/s12888-018-1736-5
95. Bu F, Steptoe A, Fancourt D. Who is lonely in lockdown? Cross-cohort analyses of predictors of loneliness before and during the COVID-19 pandemic. Public Health. (2020) 186:31–4. doi: 10.1016/j.puhe.2020.06.036
96. O'Connor RC, Wetherall K, Cleare S, McClelland H, Melson AJ, Niedzwiedz CL, et al. Mental health and well-being during the COVID-19 pandemic: longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br J Psychiatry. (2020) 21:1–8. doi: 10.31234/osf.io/r8cdw
97. Li LZ, Wang S. Prevalence and predictors of general psychiatric disorders and loneliness during COVID-19 in the United Kingdom. Psychiatry Res. (2020) 291:113267. doi: 10.1016/j.psychres.2020.113267
98. Arnett JJ. Emerging adulthood: a theory of development from the late teens through the twenties. Am Psychol. (2000) 55:469–80.
99. Luhmann M, Hawkley LC. Age differences in loneliness from late adolescence to oldest old age. Dev Psychol. (2016) 52:943–59. doi: 10.1037/dev0000117
100. Qualter P, Vanhalst J, Harris R, Van Roekel E, Lodder G, Bangee M, et al. Loneliness across the life span. Perspect Psychol Sci. (2015) 10:250–64. doi: 10.1177/1745691615568999
101. Kutcher S, Wei Y. School mental health: a necessary component of youth mental health policy and plans. World Psychiatry. (2020) 19:174–5. doi: 10.1002/wps.20732
102. Ormel J, Cuijpers P, Jorm AF, Schoevers R. Prevention of depression will only succeed when it is structurally embedded and targets big determinants. World Psychiatry. (2019) 18:111–2. doi: 10.1002/wps.20580
103. Sinha M, Collins P, Herrman H. Collective action for young people's mental health: the citiesRISE experience. World Psychiatry. (2019) 18:114–5. doi: 10.1002/wps.20615
104. Tan BYQ, Chew NWS, Lee GKH, Jing M, Goh Y, Yeo LLL, et al. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann Intern Med. (2020) 173:317–20. doi: 10.7326/M20-1083
105. Pedrosa AL, Bitencourt L, Fróes ACF, Cazumbá MLB, Campos RGB, de Brito SBCS, et al. Emotional, Behavioral, and Psychological Impact of the COVID-19 Pandemic. Front Psychol. (2020) 11:566212.
106. Xie X, Xue Q, Zhou Y, Zhu K, Liu Q, Zhang J, et al. Mental health status among children in home confinement during the coronavirus disease 2019 outbreak in Hubei Province, China. JAMA Pediatr. (2020) 174:898–900. doi: 10.1001/jamapediatrics.2020.1619
107. Racine N, Cooke JE, Eirich R, Korczak DJ, McArthur B, Madigan S. Child and adolescent mental illness during COVID-19: a rapid review. Psychiatry Res. (2020) 292:113307. doi: 10.1016/j.psychres.2020.113307
108. Tyagi A, Prasad AK, Bhatia D. Effects of excessive use of mobile phone technology in India on human health during COVID-19 lockdown. Technol Soc. (2021) 67:101762. doi: 10.1016/j.techsoc.2021.101762
109. Morin CM, Carrier J, Bastien C, Godbout R. Canadian sleep and circadian network. sleep and circadian rhythm in response to the COVID-19 pandemic. Can J Public Health. (2020) 111:654–7. doi: 10.17269/s41997-020-00382-7
110. McGorry P, Trethowan J, Rickwood D. Creating headspace for integrated youth mental health care. World Psychiatry. (2019) 18:140–1. doi: 10.1002/wps.20619
111. Shah JL, Scott J, McGorry PD, Cross SPM, Keshavan MS, Nelson B, et al. Transdiagnostic clinical staging in youth mental health: a first international consensus statement. World Psychiatry. (2020) 19:233–42. doi: 10.1002/wps.20745
112. Baltar F, Brunet I. Social research 2.0: virtual snowball sampling method using facebook. Internet Res. (2012) 22:57–74.
113. Bonsang E, Van Soest A. Satisfaction with social contacts of older Europeans. Soc Indic Res. (2012) 105:273–92. doi: 10.1007/s11205-011-9886-6
114. Delmelle EC, Haslauer E, Prinz T. Social satisfaction, commuting and neighborhoods. J Transp Geogr. (2013) 30:110–6. doi: 10.1016/j.jtrangeo.2013.03.006
115. Wrzus C, Hänel M, Wagner J, Neyer FJ. Social network changes and life events across the life span: a meta-analysis. Psychol Bull. (2013) 139:53–80. doi: 10.1037/a0028601
116. Solomou I, Constantinidou F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: age and sex matter. Int J Environ Res Public Health. (2020) 17:4924. doi: 10.3390/ijerph17144924
117. Jorm AF, Kitchener BA, Reavley NJ. Mental Health First Aid training: lessons learned from the global spread of a community education program. World Psychiatry. (2019) 18:142–3. doi: 10.1002/wps.20621
118. Dawson KS, Watts S, Carswell K, Shehadeh MH, Jordans MJD, Bryant RA, et al. Improving access to evidence-based interventions for young adolescents: Early Adolescent Skills for Emotions (EASE). World Psychiatry. (2019) 18:105–7. doi: 10.1002/wps.20594
119. Whitley R, Shepherd G, Slade M. Recovery colleges as a mental health innovation. World Psychiatry. (2019) 18:141–2. doi: 10.1002/wps.20620
120. Reynolds CF III. Building resilience through psychotherapy. World Psychiatry. (2019) 18:289–91. doi: 10.1002/wps.20663
Keywords: loneliness, trauma, pandemic, mental disorders, youth
Citation: Sampogna G, Giallonardo V, Del Vecchio V, Luciano M, Albert U, Carmassi C, Carrà G, Cirulli F, Dell'Osso B, Menculini G, Belvederi Murri M, Pompili M, Sani G, Volpe U, Bianchini V and Fiorillo A (2021) Loneliness in Young Adults During the First Wave of COVID-19 Lockdown: Results From the Multicentric COMET Study. Front. Psychiatry 12:788139. doi: 10.3389/fpsyt.2021.788139
Received: 01 October 2021; Accepted: 11 November 2021;
Published: 10 December 2021.
Edited by:
Laura Orsolini, Marche Polytechnic University, ItalyReviewed by:
Luca Steardo, University Magna Graecia of Catanzaro, ItalyAnna Szczegielniak, Medical University of Silesia, Poland
Copyright © 2021 Sampogna, Giallonardo, Del Vecchio, Luciano, Albert, Carmassi, Carrà, Cirulli, Dell'Osso, Menculini, Belvederi Murri, Pompili, Sani, Volpe, Bianchini and Fiorillo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gaia Sampogna, Z2FpYS5zYW1wb2duYUBnbWFpbC5jb20=