 Lijiao Jiang
Lijiao Jiang Dandan Yang3†
Dandan Yang3† Jiajin Yuan
Jiajin Yuan
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry , 18 November 2021
Sec. Child and Adolescent Psychiatry
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.786386
This article is part of the Research Topic Mental Health of Adolescents during the Pandemic: Consequences of Social Isolation View all 11 articles
The current study examined the influence of pubertal development stage on depression and its psychosocial mechanisms in a non-clinical population of 502 adolescents (244 boys and 258 girls) in China, graded 5 to 8. Results indicated that (1) pubertal development was positively correlated with depression, negative physical self and interpersonal stress. (2) There is a significant gender by pubertal development interaction on the measure of academic self-concept, which is accounted for by decreased academic self in boys but not in girls as a function of pubertal development. (3) Mediation analyses show that increased depression in late compared to pre- puberty is partly mediated by the enhancement of negative physical self and interpersonal stress. These findings suggest that the late stage of puberty is coupled by a higher risk of depression in adolescents partly through increased negative physical self and interpersonal stress.
Adolescent depression is a common neuropsychiatric disorder. Epidemiological studies have shown that the onset of depression peaks in adolescence (1–3), and lifelong depression usually begins at puberty (4). Early studies of adolescent health showed that the incidence of depressive symptoms increases significantly after the age of 12 (5), and levels of depressive disorders were significantly higher in mid adolescence than in childhood (6, 7). Adolescent depression can affect normal growth, cause serious educational barriers, and impair social relationships with peers and families (8–12). In addition, adolescent depression is closely associated with adult depression, suicide ideation and behavior (12, 13). There are also gender differences in adolescent depression. Studies have shown that pre-pubertal boys have a higher proportion of depressive symptoms than counterpart girls (14), however, with the development of puberty, the depression level of girls gradually increases with their developmental stage, especially by ages 12 to 13 or in the middle of puberty (15). In brief, previous researches have suggested that compared with childhood, the risk of adolescent depression increases, with greater prevalence in girls than in boys.
Prior studies have proposed several explanations for this phenomenon (16–18), First, physiological changes associated with adolescent development may have an impact on adolescent depression. Adolescents need to face sudden physical changes in the onset of puberty. Rapid changes in hormone levels and other physiological characteristics bring emotional stress to adolescents and even result in adaptive disorders (e.g., depression, binge drinking) (2, 18, 19). This adaptive stress may vary at different pubertal stages. For example, depression in pre-pubertal children is less common than that in adolescents (6, 7, 20), while the rate of depression increased significantly in the mid-puberty (16). Girls have a higher rate of depression after Tanner III and boys have a higher rate of depression before that (14).
Secondly, adolescent development is also linked with multiple psychosocial stressors, such as physical self-dissatisfaction, interpersonal stress and academic stress (17, 21–23). Several studies have shown that negative physical self (17, 24–26), interpersonal stress (27, 28), and academic self-stress (29) all contribute to the increase in adolescent depression.
In more detail, studies have indicated that body image dissatisfaction can be especially harmful to adolescents who undergo dramatic physical changes (24). In addition, the quality of parent-child relationship declines temporarily and the conflict increases with adolescent development (30). Indirect peer stress (e.g., the emergence of school and class norms) increases from early to middle adolescence (27). Academic stress also increases with adolescent ages, as academic pressure is indicated to be one of the most common sources of stress for teenagers (29, 31). In summary, adolescence development is associated with adaptive stresses that are considered to contribute to depressive disorders.
However, pubertal development is the key event during adolescence (32). Epidemiological evidence has shown that the risk of psychosocial disorders starts to rise with pubertal transition, including depression and behavioral disorders like substance misuse (3). Nonetheless, most studies of adolescent development used age or grade as the criteria to define the timing of adolescence (33–35), with the impacts of puberty on depression and psychosocial stresses less studied. As we know, age and grade are not necessarily indicative of levels of physical maturation, which, by contrast, is embodied by pubertal developmental stage.
In this regard, despite current knowledge of the relation between adolescent development and adaptive stress or depression, it is necessary to determine how puberty, the land marking event of adolescence, influences depression in teenagers. As analyzed above, it is possible that psychosocial stressors, from body image concern, interpersonal stress to academic stress, may mediate the association between puberty and depression. However, the roles of these psychosocial variables in the association between pubertal development and depression need to directly illustrated.
In addition, prior studies have indicated sex difference in the prevalence of depression and certain psychosocial stress (e.g., interpersonal stress) during adolescence (16, 36, 37). Also, there is evidence that the pattern of sex difference in emotion processing varies as a function of pubertal stage (38). Therefore, this study first examined sex differences in the impact of pubertal development on depression and perceived psychosocial stress. Then, according to the result, we further explored psychosocial factors that may mediate the relationship between pubertal development and adolescent depression, taking sex as a moderator. The mediation effect of each single stressor as well as the comprehensive effects of multiple stressors were examined, respectively.
Five hundred and two (N = 502) teenagers from grade 5 to grade 8 in Chengjiang Primary School and Chongqing 23 th high school in China were recruited by random sampling. Among them (244 boys and 258 girls), 60 (Mage = 11.23, SD = 0.93) were classified as in the pre-pubertal, 145 (Mage = 11.57, SD = 0.94) in the early pubertal, 159 (Mage = 12.0, SD = 1.15) in the mid pubertal, and 138 (Mage = 12.52, SD = 0.98) in the late pubertal stage according to their scores in the Pubertal Developmental Scale [PDS, (39, 40)]. Written informed consent was obtained from every participant and their parents prior to the experiment, and the study was approved by the Human Ethics Committee of Southwest University and Sichuan Normal University.
The pubertal developmental stages were assessed via the self-reports in the Pubertal Development Scale (PDS). The PDS is a 4-point and 5-item self-report scale that is divided into two subscales for puberty assessment in boys and girls, respectively (39, 41). The two subscales have three common items for assessing growth spurt, body hair development and skin changes in both sexes. Additionally, boys are asked to report facial hair growth and voice change, while girls report breast development and menarche [coded as 1 (not yet) or 4 (yes)]. And the internal-consistency reliability (Cronbach's alpha) of the PDS was 0.722 based on the current sample statistics (N = 502).
The degree of depressive symptoms was measured using the Beck Depression Inventory [BDI (42)]. BDI is a self-report questionnaire with 21 items to evaluate the presence and severity of depression in adolescents. The higher the score of the scale, the higher the degree of depression (43, 44). The highest total score was 63, which had a high convergence validity with the interviewer's score of depression severity. In this study, the Cronbach's alpha of the BDI was 0.933.
In this study, we measured adolescents' negative physical self, interpersonal stress, and academic self-stress.
We used the Negative Physical Self Scale [NPSS (45)] to measure adolescents' negative physical self-concept. It has 48 questions divided into five dimensions, namely overall dissatisfaction, appearance, thin, short and fat, using a five-point rating scale with 0 indicating totally disagree, and 4 denoting fully agree. The average score of each dimension was obtained by averaging the total scores across all the items for each subject. The higher score denotes more dissatisfied with one's physical self. The Cronbach's alpha of each subscale based on the current sample is: αtotal = 0.929, αoverall dissatisfaction = 0.701, αfat = 0.914, αthin = 0.817, αappearance = 0.915, αshort = 0.904.
We used the Adolescent Interpersonal Stress Scale (AISS) to measure adolescents' interpersonal stress. The AISS has 23 items and uses a 5-point scale ranging from 0 to 4, with higher score indicating greater stress. The AISS consists of four subscales: teacher stress, peer stress, family environment stress and parental discipline stress. The scores in each subscale and the total AISS scores were computed, respectively, for each subject. The Cronbach's alpha of the AISS is: αtotal = 0.889, αteacher = 0.847, αpeer = 0.780, αfamily environment = 0.542, αparental discipline = 0.637.
Academic self was measured using the Adolescent Student's General Academic Self-Concept Scale (46). It has 20 items divided into four subscales: ability perception, behavioral inhibition, emotional experience and achievement value. The scale uses a 5-point scale, ranging from 1 (the description is completely unfit for me) to 5 (completely fit for me). The higher scores indicate better feeling in each specific area. The Cronbach's alpha of the scale is: αtotal = 0.940, αability perception = 0.833, αemotional experience = 0.881, αbehavioral inhibition = 0.867, αachievement value = 0.827.
First, according to the predicted development level, students of grade 4–8 were randomly selected and tested with the Pubertal Development Scale (PDS). Then, the students were classified into different pubertal developmental stages according to the PDS scores. Furthermore, students of different stages and genders were asked to fill in the stress questionnaires, the Beck Depression Inventory and the Spielberger State-Trait Anxiety Inventory (STAI), with necessary guidance if needed. Finally, all the questionnaires were collected and souvenirs were distributed to the participants. Unusable questionnaires with random answers and unfinished questionnaires were deleted. A total of 502 students were randomly sampled from grade 4 to grade 8.
SPSS23.0 was used for data preprocessing, analysis of variance, and calculation of correlation among various variables. Mplus7.3 was used to test each structural equation model. According to the two-step sequence of Anderson and Gerbing (47), the measurement model needs to be checked before modeling. Firstly, the measurement models of the four latent variables were tested to evaluate the goodness of fit represented by their indicators. The confirmatory factor analysis and the maximum likelihood estimation method were used to test the model fitting for the datasets, and the bias-corrected bootstrap confidence intervals were used to test the mediating effects.
The multi-item inflation measurement error of latent variables was controlled according to the packaging strategy of Wu and Wen (48). In more detail, the one-dimensional scale was packaged into three indicators by the factor balance method, and the multidimensional scale was packaged into corresponding indicators according to the number of dimensions. The mean scores of corresponding items were calculated to represent the measurement scores of the index. Since the pubertal development stage is a categorical variable, dummy coding is used for this variable in the mediation test model (49).
The following four indices were utilized to evaluate the goodness of fit of the model: (a) chi-square statistic (χ2), χ2/df, (b) the standardized root mean square residual (SRMR), (c) the root mean square error of approximation (RMSEA), and (d) the comparative fit index [CFI, (50, 51)]. According to Wen and Marsh (2004), when χ2/df < 5, CFI, TLI > 0.90, RMSEA < 0.08, and SRMR < 0.08, the model is considered to be well-fitted (52).
Correlation analysis showed that, variables were significantly correlated with one another (Table 1).

Table 1. Descriptive data and zero-order correlations across variables.
Then, the multivariate analysis of variance used gender and pubertal stage as independent variables, while depression, negative physical self, interpersonal stress and academic self as dependent variables. The results showed that the main effects of gender (F(1,494) = 5.910, p < 0.05) and pubertal stage (F(3,494) = 2.636, p < 0.05), as well as the gender by pubertal stage interaction (F(3,494) = 3.956, p < 0.01) were significant on the academic self. The subsequent analyses showed a significant pubertal stage effect in boys (p < 0.01) and girls (p < 0.02). Boys in middle and late stages had lower academic self than in pre-pubertal stage (p < 0.05). For girls, the only significant comparison is the reduced academic self in late compared to the middle stage (p < 0.05) (Figure 1A). In another direction, boys showed lower academic self than girls in middle (p < 0.01) and late stage (p < 0.05) but not in the pre-and early stage (p > 0.1) (Figure 1B).
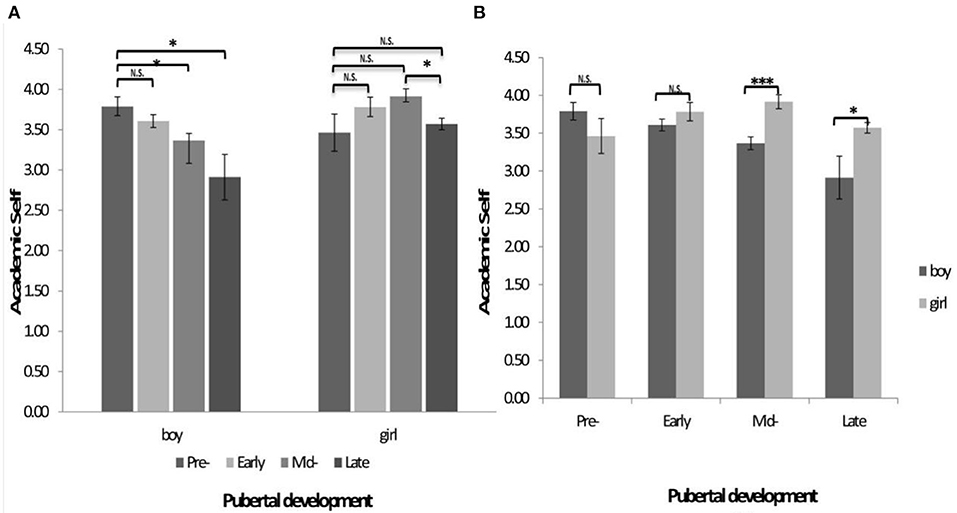
Figure 1. (A,B) The interaction of gender and pubertal development on the rating score of academic self. *p < 0.05, **p < 0.01, ***p < 0.001; N.S., not significant.
In addition, there was a significant main effect of pubertal stage on depression F(3,494) =4.288, p < 0.01. Post hoc comparisons showed that the depression level in late stage was significantly higher than that in pre- (p < 0.01), early- (p < 0.01), and mid-stages (p < 0.01), while no significant differences were observed amongst pre-, early and mid-stages (p > 0.1). There were no other significant main or interaction effects.
Confirmatory factor analysis was used to test whether the measurement model could adequately fit the sample data. The full measurement model included four latent constructs (depression, interpersonal stress, academic self and negative physical self), which altogether generated sixteen observed variables. The results showed that the measurement model can fit the sample data well (χ2 = 330.093, df = 98, χ2/df = 3.368, CFI = 0.942, TLI = 0.929, RMSEA = 0.069, SRMR = 0.068). However, among the five indicators of negative physical self, the factor loading coefficients of the overall dissatisfaction and thin were lower than 0.45 (0.281 and 0.399, respectively), so these two indicators were deleted (52) to improve the model fitting (χ2 = 170.894, df = 71, χ2/df = 2.410, CFI = 0.973, TLI = 0.966, RMSEA = 0.053, SRMR = 0.046). Then, the standardized factor loadings of all the observed variables on the corresponding latent constructs were statistically significant (p < 0.001), indicating that the structural equation model can be used in the next step of analysis.
Using Harman single factor test, we analyzed the principal component factors of all the items in the questionnaire without rotation. The results showed that the variance of the maximum factor interpretation was 15.91% (<40%), which indicated that the common method bias of this study was not significant (53).
In the first step, as mentioned above, the direct effect of the predictor (pubertal stage) on the dependent variable (depression) without mediators was significant (F(3,498) =4.288, p < 0.01). The level of depression tended to increase as a function of pubertal stage (pre: 0.384 ± 0.469, early: 0.425 ± 0.506, mid: 0.436 ± 0.507, late: 0.684 ± 0.581), and depression was significantly higher in the late compared to other pubertal stages. Therefore, the pre puberty was used as the reference baseline, and three dummy variables of early, middle and late puberty were set as independent variables. Then, Model 1 and Model 2 were established with negative physical self (M1) or interpersonal stress (M2) as mediators. Model 3 was established with academic self as mediator and gender as moderator, given observation of a gender & puberty interaction effect on academic self. The results of the mediation model showed a satisfactory fitting of Model 1, Model 2 (Model 1: χ2 = 60.195, df = 20, χ2/df = 3.010, CFI = 0.977, TLI = 0.962, RMSEA = 0.063, SRMR = 0.033, Model 2: χ2 = 42.004, df = 28, χ2/df = 1.500, CFI = 0.993, TLI = 0.989, RMSEA = 0.032, SRMR = 0.023).
The bias-corrected bootstrap method was used to test the mediating effect (sampling = 1000). The results showed that the mediating effects of Model 1 and Model 2 were not significant in the early and mid-stage, while the mediating effects of negative physical self (Model 1) and interpersonal stress (Model 2) were significant in the late stage (Figures 2A,B). The mediating effect of academic self (Model 3) was not significant (Figure 2C). Monte Carlo power analyses were used to calculate the statistical power of Model 1 and Model 2. Results showed that Model 1 (negative physical self) had a statistical power of 0.99, while Model 2 (interpersonal stress) had a statistical power of 0.74.
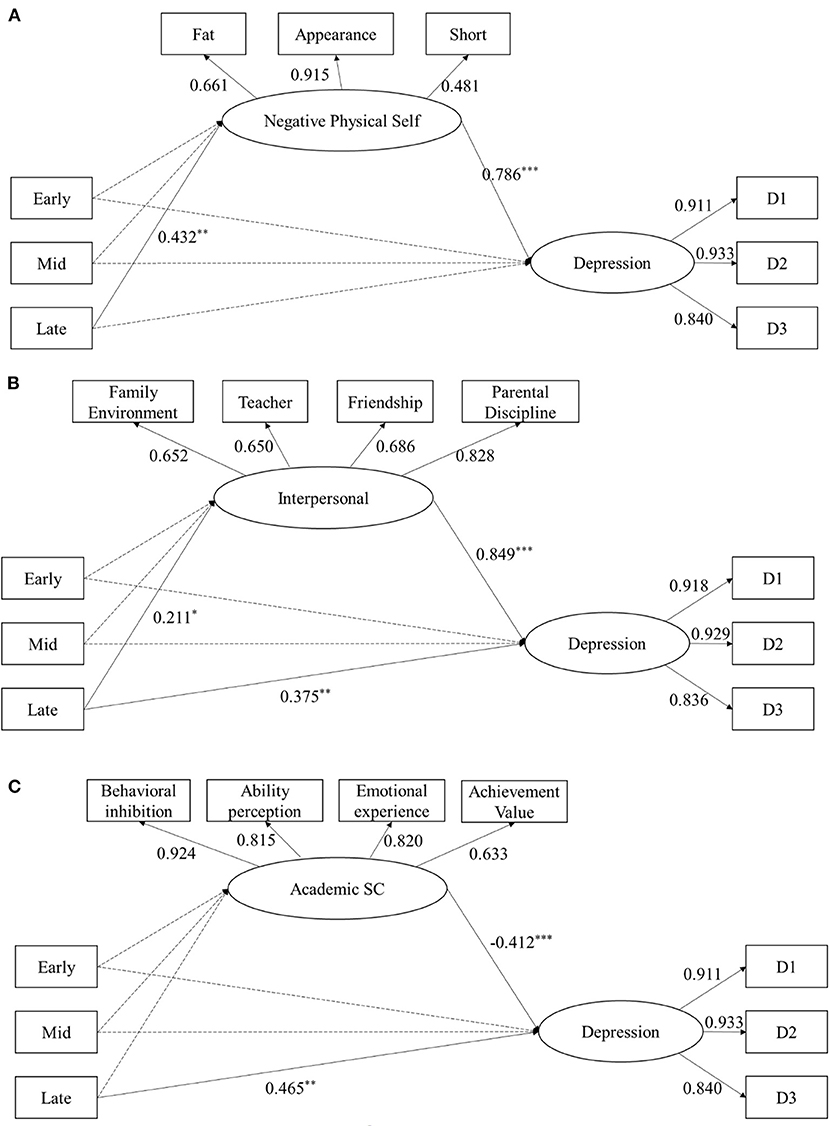
Figure 2. Single factor mediation Model 1, Model 2 and Model 3 were established with negative physical self (A) or interpersonal stress (B) as mediator, respectively. Model 3 was established with academic self (C) as mediator and gender as moderator. Path coefficient was standardized. *p < 0.05, **p < 0.01, ***p < 0.001, Early, Early puberty; Mid, Mid puberty; Late, Late puberty.
According to the results of the single factor mediation model, the multiple mediation model was established with negative physical self and interpersonal stress as mediators (Model 4). The model fitting is satisfactory, χ2 = 210.420, df = 54, χ2/df = 3.896, CFI = 0.939, TLI = 0.915, RMSEA = 0.076, SRMR = 0.092. In Model 4, the mediating effect of interpersonal stress was not significant in the early and mid-puberty. The mediating effects of interpersonal stress [95% CI: (0.002, 0.283)] and negative physical self [95% CI: (0.134, 0.431)] were significant in the late pubertal stage (Figure 3).
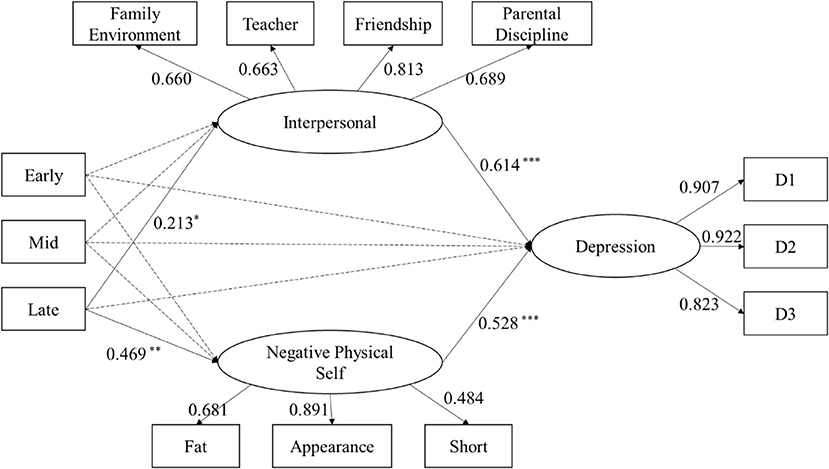
Figure 3. Multiple mediation Model 4 between the pubertal stage and depression through interpersonal stress and negative physical self. Path coefficient was standardized. *P < 0.05, **P < 0.01, ***P < 0.001; Early, Early puberty; Mid, mid puberty; Late, late puberty.
This research yielded three main results. First, through correlation analysis, we found that pubertal development is associated with an increase in the levels of depression and psychosocial stresses in adolescents. Specifically, the level of depression, psychosocial stresses such as negative physical self, interpersonal stress and perceived academic stress all increased with pubertal development. In addition, multiple psychosocial stressors were positively correlated with the level of depression, which implies that the stresses coupled by puberty development may contribute to the generation of depression. Second, concerning the gender differences in depression and stressors across pubertal stages, we only observed a significant pubertal stage and gender interaction effect on the ratings of academic self. Boys, instead of girls, faced higher academic stress with pubertal development, while the analysis of other stressors (interpersonal stress and negative physical self) did not show this pattern of effect. Moreover, our correlation analyses showed greater stresses in the measures of academic self, negative physical self and interpersonal stress with pubertal development. Third and most important, single factor mediation analysis showed that negative physical self and interpersonal stress mediates the increased depression in late compared to pre pubertal stages, respectively. The significant mediators of interpersonal stress and negative physical self are further replicated in the multiple-factor mediation model.
Our finding of higher academic stress in boys but not in girls with pubertal development is consistent with a couple of prior observations. For example, there was evidence showing an advantage of girls over boys in the four dimensions of the academic self (54–56). First of all, research has shown that girls' academic performance is generally better than boys around the senior grades of primary school or early high school (56). Also, early study has shown that girls are more inclined than boys to internally attribute improved academic performance to their own efforts and abilities through positive perception (55). In addition, girls outperform boys in behavioral self-control (57). On the other hand, boys have more academic procrastination than girls, like delayed implementation and delayed remediation (54), and boys experience more negative academic emotions than girls.
The results suggest that the effects of pubertal development on negative physical self, interpersonal stress, and depression were consistent across boys and girls. One explanation for the lack of gender differences in these measures may be related to the range of ages of the subjects (10–14 years). Early studies have shown that there is no gender difference in depressive mood for adolescents at 12–14 years old (58), while gender differences appear from 14 to 15 years (14, 59). This coincided with our finding of rising depression in late compared to pre, early and mid-pubertal stages, while the latter three stages showed similarly low levels of depression across genders.
Previous studies have shown that body dissatisfaction was a major predictor of low self-esteem, depression, and eating disorders in adolescents (60–62). In addition, the concept of “thinness as beauty for girls and strong as beauty for boys” usually prevails, leading to teenager's irrational expectations for figure, weight and increased physical self-dissatisfaction since entry into puberty. For example, it has been reported that stress from peers, parents and social media predisposes teenagers to be easily dissatisfied with body image, thus promoting the risk of depression (27, 63).
On the other hand, adolescents have excessive comfort seeking and greater emotional dependence on their friends compared to people in other periods (64), which suggests that adolescents are more susceptible to interpersonal stress (e.g., relationship breakdown) than other age groups, which also increases the risk of depressive symptoms (64). Recent studies have shown that multiple physiological indicators (e.g., salivary alpha amylase, systolic blood pressure) of adolescents are significantly higher than those of children during peer rejection or social exclusion (64–66). In addition, parent-child conflict constitutes an important part of interpersonal stress at adolescence, since seeking affective and behavioral independence from parents is one of the key motivations in this period (30, 67).
In summary, the current study identified negative physical self as a key mediator underpinning the predictive role of puberty in adolescent depression. This shows that negative physical self is a major stressor that contributes to adolescent depression during late pubertal period. However, the current cross-sectional design measured depression, pubertal stage and psychosocial stressors at the same phase. In this regard, though we observed reliable mediation effects of negative physical self and interpersonal stress on the association between puberty and depression, the causal relationship between adolescent depression, pubertal stage and psychosocial variables cannot be firmly inferred. Therefore, future studies need to administer a longitudinal design to a large sample of subjects across different pubertal stages, to determine the influence of puberty on affective health and its related psychosocial mechanisms.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by Ethics committee of human research at Southwest University and Sichuan Normal University. Written informed consent to participate in this study was provided by the participant's legal guardian/next of kin.
JY: conceptualized the study and research design. JY and DY: paper writing. LJ: data analysis and presentation. DY and YL: data connection. All authors contributed to the article and approved the submitted version.
This study was supported by the National Natural Science Foundation of China (NSFC31971018; 31871103).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Altemus M, Sarvaiya N, Neill Epperson C. Sex differences in anxiety and depression clinical perspectives. Front Neuroendocrinol. (2014) 35:320–30. doi: 10.1016/j.yfrne.2014.05.004
2. Forbes EE, Ryan ND, Phillips ML, Manuck SB, Worthman CM, Moyles DL, et al. Healthy adolescents' neural response to reward: associations with puberty, positive affect, and depressive symptoms. J Am Acad Child Adolesc Psychiatry. (2010) 49:162–72. doi: 10.1016/j.jaac.2009.11.006
3. Patton GC, Viner R. Pubertal transitions in health. Lancet. (2007) 369:1130–9. doi: 10.1016/S0140-6736(07)60366-3
4. Hankin BL. Adolescent depression: description, causes, and interventions. Epilepsy Behav. (2006) 8:102–14. doi: 10.1016/j.yebeh.2005.10.012
5. Bertha EA, Balßzs J. Subthreshold depression in adolescence: a systematic review. Eur Child Adolesc Psychiatry. (2013) 22:589–603. doi: 10.1007/s00787-013-0411-0
6. Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, et al. The epidemiology of major depressive disorder: results from the national comorbidity survey replication (ncs-r). JAMA. (2003) 289:3095. doi: 10.1001/jama.289.23.3095
7. Pedrelli P, Shapero B, Archibald A, Dale C. Alcohol use and depression during adolescence and young adulthood: a summary and interpretation of mixed findings. Current Addiction Reports. (2016) 3:91–7. doi: 10.1007/s40429-016-0084-0
8. Dunn V, Goodyer L. Longitudinal investigation into childhood- and adolescence-onset depression: psychiatric outcome in early adulthood. Br J Psychiatry. (2006) 188:216–22. doi: 10.1192/bjp.188.3.216
9. Fletcher JM. Adolescent depression and educational attainment: results using sibling fixed effects. Health Econ. (2010) 19:855–71. doi: 10.1002/hec.1526
10. Lewinsohn PM, Rohde P, Seeley JR. Major depressive disorder in older adolescents: prevalence, risk factors, and clinical implications. Clin Psychol Rev. (1998) 18:765–94. doi: 10.1016/S0272-7358(98)00010-5
11. Tuisku V, Kiviruusu O, Pelkonen M, Karlsson L, Strandholm T, Marttunen M. Depressed adolescents as young adults – predictors of suicide attempt and non-suicidal self-injury during an 8-year follow-up. J Affect Disord. (2014) 152–154:313–9. doi: 10.1016/j.jad.2013.09.031
12. Weersing VR, Jeffreys M, Do MCT, Schwartz K, Bolano C. Evidence base update of psychosocial treatments for child and adolescent depression. J Clin Child Adolesc Psychol. (2016) 46:1−33. doi: 10.1080/15374416.2016.1220310
13. Zhang B, Yan X, Zhao F, Yuan F. The relationship between perceived stress and adolescent depression: the roles of social support and gender. Soc Indic Res. (2015) 123: 501–18. doi: 10.1007/s11205-014-0739-y
14. Angold A, Costello EJ, Worthman CM. Puberty and depression: the roles of age, pubertal status and pubertal timing. Psychol Med. (1998) 28:51–61. doi: 10.1017/S003329179700593X
15. Maughan B, Collishaw S, Stringaris A. Depression in childhood and adolescence. J Can Acad Child Adolesc Psychiatry. (2013) 22:35–40.
16. Hankin BL, Abramson LY. Development of gender differences in depression: an elaborated cognitive vulnerabilitytransactional stress theory. Psychol Bull. (2001) 127:773–96. doi: 10.1037/0033-2909.127.6.773
17. Cruz-Sáez S, Pascual A, Wlodarczyk A, Echeburúa E. The effect of body dissatisfaction on disordered eating: The mediating role of self-esteem and negative affect in male and female adolescents. J Health Psychol. (2020) 25:1098–108.
18. Wetherill RR, Squeglia LM, Yang TT, Tapert SF. A longitudinal examination of adolescent response inhibition: neural differences before and after the initiation of heavy drinking. Psychopharmacology. (2013) 230:663–71. doi: 10.1007/s00213-013-3198-2
19. Ramirez JM. Hormones and aggression in childhood and adolescence. Aggress Violent Behav. (2003) 8:621–44. doi: 10.1016/S1359-1789(02)00102-7
20. Harrington R. Adolescent depression: same or different? Arch Gen Psychiatry. (2001) 58:21. doi: 10.1001/archpsyc.58.1.21
21. Flynn M, Kecmanovic J, Alloy LB. An examination of integrated cognitive-interpersonal vulnerability to depression: the role of rumination, perceived social support, and interpersonal stress generation. Cognit Ther Res. (2010) 34:456. doi: 10.1007/s10608-010-9300-8
22. Flynn M, Rudolph KD. Stress generation and adolescent depression: contribution of interpersonal stress responses. J Abnorm Child Psychol. (2011) 39:1187–98. doi: 10.1007/s10802-011-9527-1
23. Quach AS, Epstein NB, Riley PJ, Falconier MK, Fang X. Effects of parental warmth and academic pressure on anxiety and depression symptoms in chinese adolescents. J Child Fam Stud. (2013) 24:106–16. doi: 10.1007/s10826-013-9818-y
24. Choi E, Choi I. The associations between body dissatisfaction, body figure, self-esteem, and depressed mood in adolescents in the United States and Korea: a moderated mediation analysis. J Adolesc. (2016) 53:249–59. doi: 10.1016/j.adolescence.2016.10.007
25. Hyde JS, Mezulis AH, Abramson LY. The ABCs of depression: integrating affective, biological, and cognitive models to explain the emergence of the gender difference in depression. Psychol Rev. (2008) 115:291–313. doi: 10.1037/0033-295X.115.2.291
26. You S, Shin K, Kim AY. Body Image, Self-esteem, and depression in Korean adolescents. Child Indic Res. (2017) 10:231–45. doi: 10.1007/s12187-016-9385-z
27. Helfert S, Warschburger P. The face of appearance-related social pressure: gender, age and body mass variations in peer and parental pressure during adolescence. Chin Med. (2013) 7:16. doi: 10.1186/1753-2000-7-16
28. Hu J, Ai H. Self-esteem mediates the effect of the parent-adolescent relationship on depression. J Health Psychol. (2014) 1359105314541315. doi: 10.1177/1359105314541315
29. Fuentes MC, García-Ros R, Pérez-González F, Sancerni D. Effects of parenting styles on self-regulated learning and academic stress in Spanish adolescents. Int J Environ Res Public Health. (2019) 16:2778. doi: 10.3390/ijerph16152778
30. Branje S. Development of parent–adolescent relationships: conflict interactions as a mechanism of change. Child Dev Perspect. (2018) 12. doi: 10.1111/cdep.12278
31. Kouzma NM, Kennedy GA. Self-reported sources of stress in senior high school students. Psychol Rep. (2004) 94:314. doi: 10.2466/pr0.94.1.314-316
32. Blakemore SJ, Burnett S, Dahl RE. The role of puberty in the developing adolescent brain. Hum Brain Mapp. (2010) 31. doi: 10.1002/hbm.21052
33. Fergusson DM, Horwood LJ, Ridder EM, Beautrais AL. Subthreshold depression in adolescence and mental health outcomes in adulthood. Arch Gen Psychiatry. (2005) 62:66. doi: 10.1001/archpsyc.62.1.66
34. Hankin BL, Young JF, Abela J, Smolen A, Jenness JL, Gulley LD, et al. Depression from childhood into late adolescence: influence of gender, development, genetic susceptibility, and peer stress. J Abnorm Psychol. (2015) 124:803. doi: 10.1037/abn0000089
35. Steiger AE, Allemand M, Robins RW, Fend HA. Low and decreasing self-esteem during adolescence predict adult depression two decades later. J Pers Soc Psychol. (2014) 106:325–38. doi: 10.1037/a0035133
36. Naninck EFG, Lucassen PJ, Bakker J. Sex differences in adolescent depression: do sex hormones determine vulnerability?. J Neuroendocrinol. (2011) 23:383–92. doi: 10.1111/j.1365-2826.2011.02125.x
37. Hankin BL, Mermelstein R, Roesch L. Sex differences in adolescent depression: stress exposure and reactivity models. Child Dev. (2007) 78:279–95. doi: 10.1111/j.1467-8624.2007.00997.x
38. Yang J, Zhang S, Lou Y, Long Q, Liang Y, Xie S, et al. The increased sex differences in susceptibility to emotional stimuli during adolescence: an event-related potential study. Front Hum Neurosci. (2018) 11:660. doi: 10.3389/fnhum.2017.00660
39. Petersen AC, Crockett L, Richards M, Boxer A. A self-report measure of pubertal status: reliability, validity, and initial norms. J Youth Adolesc. (1988) 17:117–33. doi: 10.1007/BF01537962
40. Earls G, Buka SL. Project on human development in chicago neighborhoods. Bur Justice Stat. (1997) 1–123. doi: 10.1037/e520172006-001
41. Earls F, Brooksgunn J, Raudenbush SW, Sampson R. Project on human development in Chicago neighborhoods (PHDCN): young adult self report, wave 2, 1997-2000. FEMS Microbiol Lett. (2005) 73:351–9. doi: 10.3886/ICPSR13666
42. BECK AT. An inventory for measuring depression. Arch Gen Psychiatry. (1961) 4:561–71. doi: 10.1001/archpsyc.1961.01710120031004
43. Erica R, Racz S, Augenstein TM, Keeley L. A multi-informant approach to measuring depressive symptoms in clinical assessments of adolescent social anxiety using the beck depression inventory-ii: convergent, incremental, and criterion-related validity. Child Youth Care Forum. (2017) 46:661–83. doi: 10.1007/s10566-017-9403-4
44. Kim MH, Mazenga AC, Devandra A, Ahmed S, Kazembe PN, Yu X, et al. Prevalence of depression and validation of the beck depression inventory-ii and the children's depression inventory-short amongst hiv-positive adolescents in malawi. J Int AIDS Soc. (2014) 17:18965. doi: 10.7448/IAS.17.1.18965
45. Chen H, Jackson T, Huang X. The negative physical self scale: initial development and validation in samples of Chinese adolescents and young adults. Body Image. (2006) 3:401–12. doi: 10.1016/j.bodyim.2006.07.005
46. Guo C, He X, Zhang D. A review of academic self-concept and its relationship with academic achievement. Psychol Sci. (in Chinese). (2006). 29:133
47. Anderson J, Gerbing C, Gerbing DW. Structural equation modeling in practice: a review and recommended two-step approach. Psychol Bull. (1988) 103:411. doi: 10.1037/0033-2909.103.3.411
48. Yan WU, Wen ZL. Item parceling strategies in structural equation modeling. Adv Psychol Sci. (2011) 19:1859–67.
49. Fang J, Wen ZL, Zhang M. Mediation analysis of categorical variables. J Psychol Sci. (2017) 2:217–23.
50. Hu L-t, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Structural Equation Modeling. (1999) 6:1–55. doi: 10.1080/10705519909540118
51. Kline R, Kline RB, Kline R. Principles And Practice Of Structural Equation Modeling. New York, NY: Journal of the American Statistical Association (2011). 101(12).
52. Wen ZL, Hau KT, Marsh HW. Structural equation model testing: cutoff criteria for goodness of fit indices and chi-square test. Acta Psychologica Sinica. (2004) 36:186–94.
53. Xiong HX, Zhang J, Ye BJ, Zheng X, Sun PZ. Common method variance effects and the models of statistical approaches for controlling it. Adv Psychol ence. (2012) 20:757–69. doi: 10.3724/SP.J.1042.2012.00757
54. Balkis M, Erdinç D. Gender differences in the relationship between academic procrastination, satifaction with academic life and academic performance. Elect J Res Edu Psychol. (2017) 15:105–25.
55. LaNoue JB, Curtis RC. Improving women's performance in mixed-sex situations by effort attributions. Psychol Women Q. (1985) 9:337–56. doi: 10.1111/j.1471-6402.1985.tb00885.x
56. Zhang J, Tian LM, Zhang WX, Psychology SO, University SN. Relations between peer rejection and early adolescents' academic achievement: the moderating effects of peer acceptance and friendship support. Psychol Dev Edu. (2013) 29:353–60.
57. Yuan J, He Y, Qinglin Z, Chen A, Li H. Gender differences in behavioral inhibitory control: ERP evidence from a two-choice oddball task. Psychophysiology. (2008) 45:986–93. doi: 10.1111/j.1469-8986.2008.00693.x
58. Wichstrom Lars. The emergence of gender difference in depressed mood during adolescence: the role of intensified gender socialization. Dev Psychol. (1999) 35:232–45. doi: 10.1037/0012-1649.35.1.232
59. Joinson C, Heron J, Araya R, Paus T, Lewis G. Association between pubertal development and depressive symptoms in girls from a UK cohort. Psychol Med. (2012) 42:1–11. doi: 10.1017/S003329171200061X
60. Jessica F, Frazier LD. Body dissatisfaction in early adolescence: the coactive roles of cognitive and sociocultural factors. J Youth Adoles. (2016) 46:1–16. doi: 10.1007/s10964-016-0559-2
61. Jones DC. Body image among adolescent girls and boys: a longitudinal study. Dev Psychol. (2004) 40:823–35. doi: 10.1037/0012-1649.40.5.823
62. Smolak L. Body image in children and adolescents: where do we go from here? Body Image. (2004) 1:15–28. doi: 10.1016/S1740-1445(03)00008-1
63. Justine R, Dana V, Christy G. Weight status and body image perceptions in adolescents: current perspectives. Adolesc Health Med Ther. (2015) 6:149–58. doi: 10.2147/AHMT.S68344
64. Hamilton JL, Potter CM, Olino TM, Abramson LY, Heimberg RG, Alloy LB. The temporal sequence of social anxiety and depressive symptoms following interpersonal stressors during adolescence. J Abnorm Child Psychol. (2016) 44:495–509. doi: 10.1007/s10802-015-0049-0
65. Spear LP. Heightened stress responsivity and emotional reactivity during pubertal maturation: implications for psychopathology. Dev Psychopathol. (2009) 21:87–97. doi: 10.1017/S0954579409000066
66. Stroud LR, Foster E, Papandonatos GD, Handwerger K, Granger DA, Kivlighan KT, et al. Stress response and the adolescent transition: performance versus peer rejection stressors. Dev Psychopathol. (2009) 21:47–68. doi: 10.1017/S0954579409000042
Keywords: adolescent development, depression, negative physical self, interpersonal stress, academic self
Citation: Jiang L, Yang D, Li Y and Yuan J (2021) The Influence of Pubertal Development on Adolescent Depression: The Mediating Effects of Negative Physical Self and Interpersonal Stress. Front. Psychiatry 12:786386. doi: 10.3389/fpsyt.2021.786386
Received: 30 September 2021; Accepted: 27 October 2021;
Published: 18 November 2021.
Edited by:
Miao Qu, Capital Medical University, ChinaReviewed by:
Siman Liu, Chinese Academy of Sciences (CAS), ChinaCopyright © 2021 Jiang, Yang, Li and Yuan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiajin Yuan, eXVhbmppYWppbjE2OEAxMjYuY29t; eXVhbmppYWppbjE2OEBzaWNudS5lZHUuY24=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.