
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 05 November 2021
Sec. Public Mental Health
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.761555
This article is part of the Research Topic Causes, Effects and Treatment of Violence and Aggression in Mental Health and Social Care Settings View all 9 articles
 Mariá Romanio Bitencourt1*
Mariá Romanio Bitencourt1* Lincoln Luís Silva2
Lincoln Luís Silva2 Ana Carolina Jacinto Alarcão3Amanda de Carvalho Dutra1Marcos Rogério Bitencourt1Giovana Jorge Garcia4Luciano de Andrade1
Ana Carolina Jacinto Alarcão3Amanda de Carvalho Dutra1Marcos Rogério Bitencourt1Giovana Jorge Garcia4Luciano de Andrade1 João Ricardo Nickenig Vissoci5Sandra Marisa Pelloso1Maria Dalva de Barros Carvalho1
João Ricardo Nickenig Vissoci5Sandra Marisa Pelloso1Maria Dalva de Barros Carvalho1Introduction: The COVID-19 pandemic stressed the importance of healthcare personnel. However, there is evidence of an increase in violence against them, which brings consequences, such as anxiety. The aim of this study was to analyze the anxiety levels of health professionals who have or not suffered violence during the COVID-19 pandemic, and verify the variables associated with the risk of starting to take medication for anxiety.
Methods: We assessed the anxiety profile of health professionals in Brazil through an online questionnaire, using the Generalized Anxiety Disorder 7-item Scale (GAD-7), in relation to groups of participants who have or not suffered violence during the COVID-19 pandemic. We used Cronbach's alpha reliability coefficient to check the consistency of the responses, and the effect size using the r coefficient. Principal Component Analysis was used to verify the differences in anxiety scores between the two groups. Logistic regression analysis was also used to verify the variables associated with the risk of starting medication for anxiety and considered statistically significant when p < 0.05.
Results: A total of 1,166 health professionals participated in the study, in which 34.13% had a normal anxiety profile, 40.14% mild, 15.78% moderate, and 9.95% severe. The mean score of the sum of the GAD-7 was 7.03 (SD 5.20). The group that suffered violence had a higher mean (8.40; SD 5.42) compared to the group that did not (5.70; SD 4.60). In addition, the median between both groups was significantly different (7.0 vs. 5.0; p < 0.01). Approximately 18.70% of the participants reported having started taking medication to treat anxiety during the pandemic. The factors that increased the chances of these professionals starting medication for anxiety p < 0.05 were having suffered violence during the pandemic (OR 1.97; 95% CI 1.42–2.77), being nurses (OR 1.61; 95% CI 1.04–2.47) or other types of health professionals (OR 1.58; 95% CI 1.04–2.38), and having a mild (OR 2.11; 95% CI 1.37–3.34), moderate (OR 4.05; 95% CI 2.48–6.71) or severe (OR 9.08; 95% CI 5.39–15.6) anxiety level.
Conclusion: Brazilian healthcare professionals who have suffered violence during the pandemic have higher anxiety scores and higher risk to start taking anxiety medication.
The novel Coronavirus (COVID-19) pandemic has had a strong impact on the mental health of the population in general. Before the pandemic, the Brazilian prevalence of anxiety disorders was 9.3% (1). However, some studies have revealed an increasement of 7.4-fold during de COVID-19 pandemic in Brazil (2). According to a systematic review including articles from China, Spain, Italy, Iran, US, Turkey, Nepal and Denmark, rates ranged from 6.33 to 50.90% (3).
Healthcare professionals have been particularly impacted, with an increased occurrence of symptoms related to anxiety, depression, insomnia, stress, fear and frustration having been observed in several studies (4–6). The mental health of such professionals is vulnerable to the impacts of the pandemic due to the high number of cases and deaths of patients and coworkers, not to mention the fear of being infected and taking the virus to their homes (7). Other negative factors are precarious working conditions, long shifts and lack of personal protective equipment (PPE) (6, 8).
As of July 2021, Brazil has experienced more than 120 thousand cases of COVID-19 in health professionals, from a total of 20 million cases and 558 thousand deaths in the country (9, 10). Although those professionals in the frontline are seen as heroes by most people, not everyone acknowledges the importance of the role they play (11). There have been reports of attacks against health professionals not only in Brazil, but worldwide, which includes stopping them from entering public places or using public transportation, discrimination, physical violence and insults (12–16). Therefore, the strain on the mental health of these professionals may be further exacerbated as a result of violent verbal or physical outbursts from the general public or patients (8).
Several international studies have been carried out during the pandemic addressing discrimination and violence against healthcare personnel (8, 13, 14), and others on anxiety and mental health (5, 6, 8, 17). However, to date, no studies have been found in Brazil relating anxiety to the violence suffered by healthcare professionals during the COVID-19 pandemic. Therefore, the aim of this study was to analyze the anxiety levels of healthcare professionals who both have and have not personally experienced violence in and outside of the workplace during the COVID-19 pandemic in Brazil. This study also assessed what variables increased the likelihood that a healthcare professional would begin taking medication to manage symptoms of anxiety.
This is a cross-sectional study involving healthcare professionals in Brazil. They answered an online questionnaire containing questions about violence, anxiety and medication use during the COVID-19 pandemic. The questionnaire was available for completion for 15 days from October 1st, 2020.
People willing to participate were recruited using a snowball sampling method (17). No incentive was provided for the participants to complete the survey because the Ethical Committee does not allow any type of incentive.
The study participants were health professionals who work in Brazil. They were invited through social media to answer an online questionnaire available on Google Forms and share it with other healthcare professionals. Their participation was voluntary and anonymous, and the individuals signed an online consent form before completing the questionnaire.
The questionnaire consisted of 31 questions, of which eight refer to sociodemographic aspects, ten are related to profession and workplace, five are about violence and eight questions about anxiety. Regarding the eight anxiety-related questions, seven of them are the ones that compose the Generalized Anxiety Disorder 7-item Scale (GAD-7), and the last one was whether the participants started to use anxiety medications during the pandemic.
The GAD-7 is a self-report questionnaire that has been proven to be a reliable and valid measuring tool to assess the symptoms of generalized anxiety in different clinical contexts for the population in general (18, 19). It was created by Spitzer et al. (20) and validated by Kroenke et al. (21) in accordance with the criteria provided by the Diagnostic and Statistical Manual of Mental Disorders. Total scores range from 0 to 21, and the highest ones indicate higher levels of symptom severity. Regarding the severity classifications, we followed the recommendations of the original authors: none/normal (0–4), mild (5–9), moderate (10–14), and severe (more than 15) anxiety. Figure 1 shows the GAD-7 questions and scores.
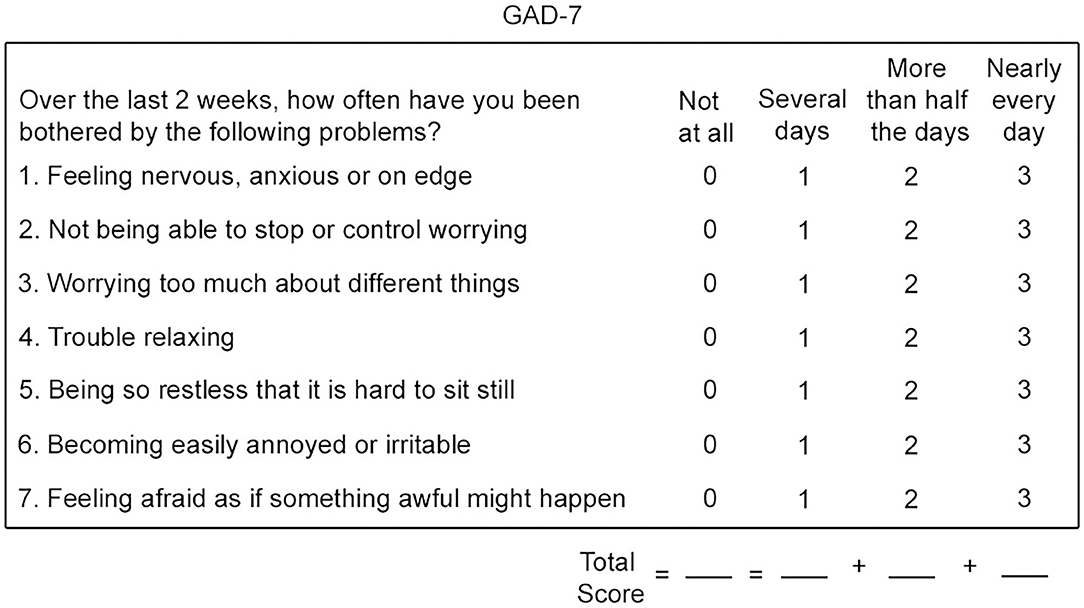
Figure 1. Generalized anxiety disorder 7-item scale (GAD-7).
The data obtained were organized on an Excel® spreadsheet (Microsoft Office, Microsoft Corporation, USA) and are available on an online repository on http://doi.org/10.6084/m9.figshare.c.5585541.
The sociodemographic characteristics of the studied population was published elsewhere in a previous paper (22).
The study population was divided into two groups: those who have suffered violence during the pandemic, and those who have not. We compared their anxiety levels and the variables associated with the risk of starting medication for anxiety. For the analysis of descriptive statistics, we used absolute and relative frequencies, means, and standard deviation.
The reliability coefficient (Cronbach's alpha) was used to verify the consistency of the participants' responses. Then, the effect size (r) of the average score item was analyzed to verify the difference comparing the answers provided by each group (23). The normality test was performed beforehand, as required for performing the Mann-Whitney test in order to verify whether the difference between groups exists.
Finally, principal component analysis (PCA) with two factors and varimax rotation was performed, since previous studies also detected two-dimensional structures to verify the most correlated GAD-7 variables (>0.6) with variability of scores for anxiety (24).
We performed a univariate logistic regression analysis of the study population using the following variables: sex, age range, race, education level, having children, having a partner, profession, length of service/experience availability of PPE at the workplace, if the PPE is considered adequate, weekly workload working hours, monthly income, having had COVID-19, being a frontline health professional, having suffered violence before the pandemic, having suffered violence during the pandemic, family members having suffered violence for being close to healthcare professionals, and, finally, the severity level within the anxiety scale.
Use of medication as a dependent variable was considered in order to estimate the risk of starting medication use for anxiety during the pandemic. Those variables with p=0.1 were selected to be analyzed together in the multivariate logistic regression analysis, and considered statistically significant when p < 0.05.
All statistical analyses were carried out with the software R Studio 1.1.456 using car, psych, corrplot and ggplot2 packages.
The study was approved by the Ethics Committee of the State University of Maringá, under registration number 37712820.4.0000.0104, in accordance with Normative Resolution 510/2016.
The reliability coefficient (Cronbach's alpha) of the GAD-7 for the study population was 0.91, which means that the answers provided by the participants were considered highly reliable. That enabled us to carry out the other analyses regarding the population.
The sociodemographic profile and anxiety level of the 1,166 participants are described in Table 1. As for the classification of their anxiety level, about 398 (34.13%) had a normal level, 468 (40.14%) mild, 184 (15.78%) moderate, and 116 (9.95%) severe.
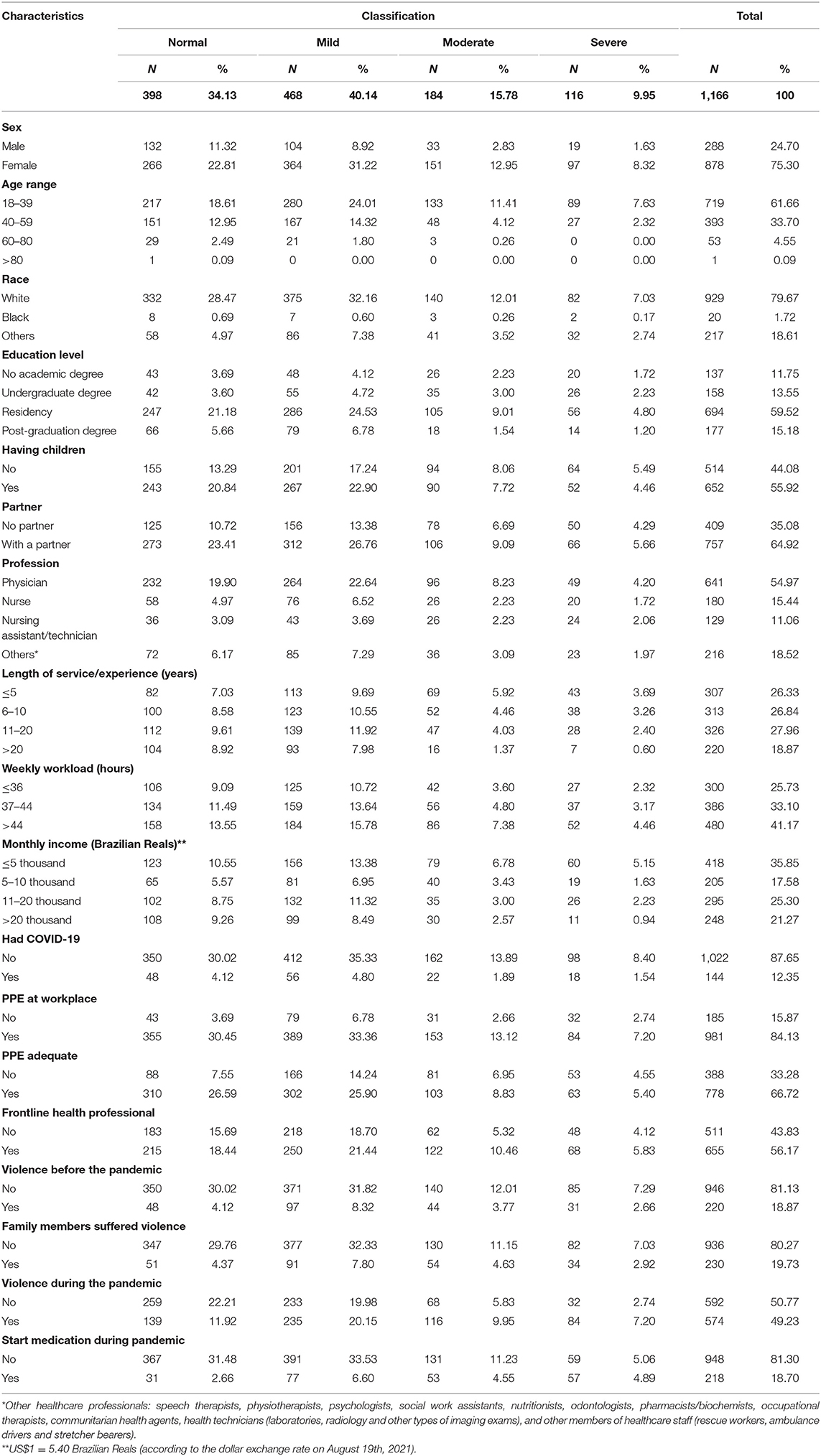
Table 1. Sociodemographic and professional characteristics of the participants according to their anxiety level.
The variables that have the greatest proportion comparing mild, moderate or severe anxiety levels to normal levels, were as follows: women (69.70%), aged 18–39 (69.81%), professionals who hold a graduate degree (73.41%), those who have no children (69.84%), those who do not have a partner (70.17%), nursing technicians or assistants (72.09%), those who had been working for <5 years in healthcare (73.28%), those who work over 44 h a week (67.08%), those whose income is inferior to 5 thousand Brazilian Reals (70.57%), those who had been diagnosed with COVID-19 (66.67%), those who had no access to PPE at their workplace (76.75%) or had access to inadequate PPE (77.31%), frontline healthcare professionals (67.17%), those who had suffered violence before (78.18%) and during the pandemic (75.18%) and, finally, those who started taking medication for anxiety during the pandemic (85.77%).
The study population was divided into 2 groups: (1) those who have suffered violence during the pandemic and (2) those who have not. We used the Mann-Whitney Test, which showed that the median of the score for those who were victims of violence is different from that of the group that suffered no violence (W = 118,187, p < 0.01) (7.0 vs. 5.0). Dispersion of the scores of both groups can be seen in Figure 2.
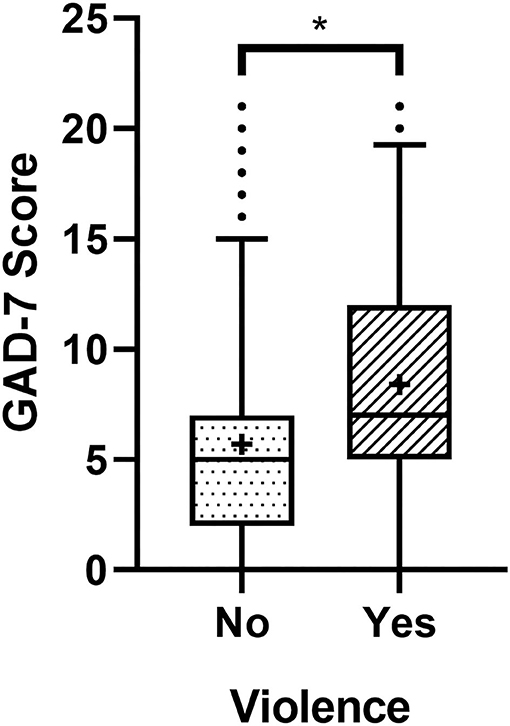
Figure 2. Boxplots showing the GAD-7 scores of the participants who have or not suffered violence during the pandemic. The dots above the superior limit represent the outliers. The crosses inside the boxplots indicate the score average of their respective group, and * indicates difference between the groups (p < 0.01).
Regarding the score of the GAD-7 items shown in Table 2, the mean score for the group that did not suffer violence ranged from 0.42 to 0.99, while the range of the group that suffered violence was between 0.75 and 1.42. Furthermore, the differences between both groups, expressed in terms of effect sizes, were found for items 1–6, which were those with the greatest divergences (r > 0.21). This means that items 1–6 had a slight increase in the average effect regarding the group that suffered violence.

Table 2. Mean, standard deviation, and r coefficient differences between groups.
In general, the means of the items were higher for the group that suffered violence. Considering the sum total of the group that suffered violence, the mean was 8.40, with a standard deviation (SD) of 5.42, while the group that did not suffer violence had an average of 5.70 and a SD of 4.60. As we can see, the descriptive parameters of the scores for anxiety are higher amongst the population that suffered violence.
The analysis of the main components of the population that did not suffer violence showed that two dimensions account for 75% of the data variance. The highest correlations in the first dimension (>0.6) were obtained between items 1- Nervous, anxious, on edge; 2- Not being able to stop or control worrying; 3- worrying too much about different things; 4- Trouble relaxing, and 6- Becoming easily annoyed or irritable. As for the second dimension, the items that stood out were 5- Being so restless that it is hard to sit still, and 7- Feeling afraid as if something awful might happen (Table 3).
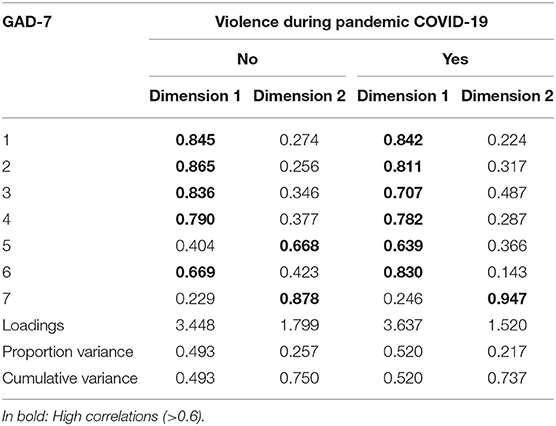
Table 3. Principal component analysis of each item in GAD-7 of the population study.
The population that suffered violence, on the other hand, also performed better within two dimensions that account for 73.7% of the data variance. The highest correlations (>0.6) in the first dimension refers to the following variables: 1–6 for the first dimension, and 7 as for the second dimension (Table 3).
This analysis showed that the items of the group that suffered violence have different information variability compared to the group that did not. In addition, item 5 had the most discrepant correlation between the two groups.
Figure 3 shows the dispersion of the scores of both groups in space. Each dot represents a participant's score. The first row contains the ellipses with the score distributions regarding the severity classification of the GAD-7 scale. The second row refers to medication use. Dots in the lower left quadrant of each figure represent the lowest scores, while the upper right quadrant shows the highest scores. The differences in color of the dots and ellipses represent the category that the dots and ellipses belong to. Dots outside the ellipses are considered outliers. Therefore, when looking at the first row, it is possible to see an ordered scale of score classification in the two groups regarding the anxiety level as normal (0), mild (1), moderate (2), and severe (3). In addition, the second row indicates that there are participants with similar scores among themselves. However, they belong to different groups when it comes to use of medication. Thus, it is suggested that, besides violence, there may be other factors involved in the use of medication by the participants to treat anxiety.
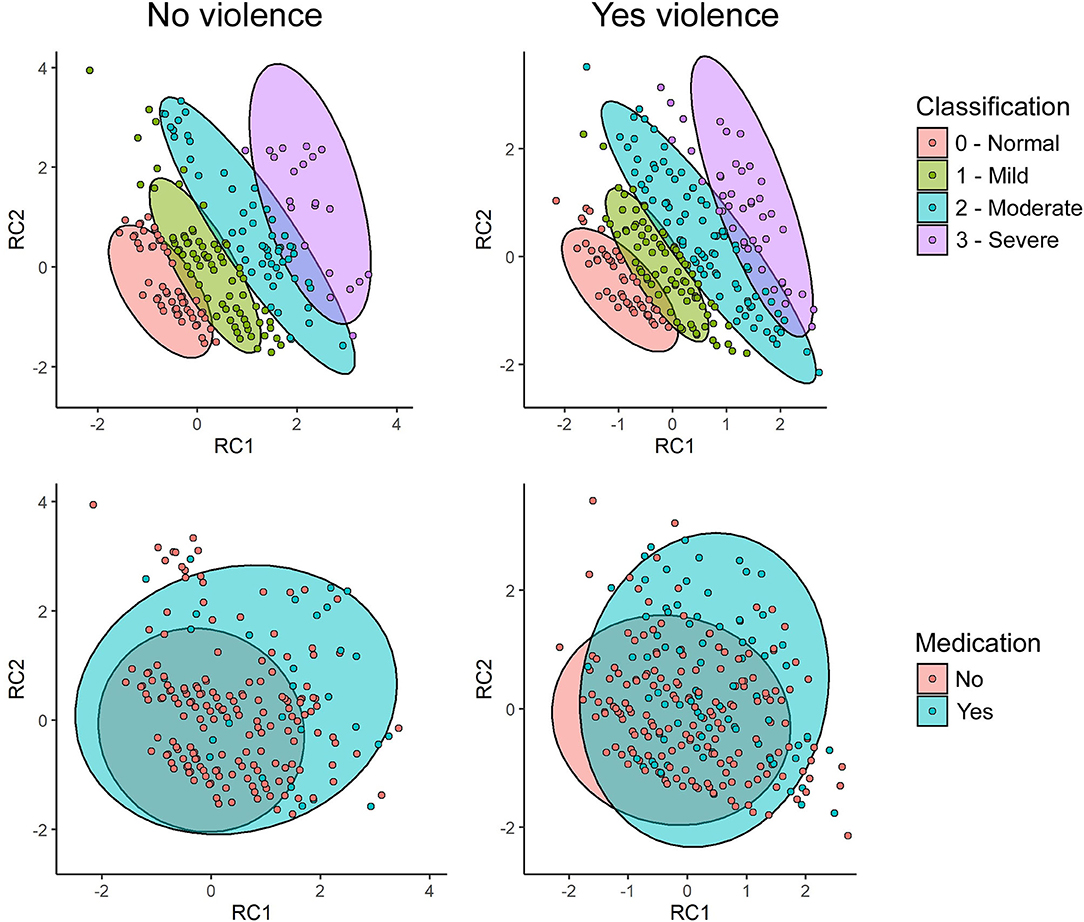
Figure 3. Distribution of the participants' anxiety scores, and grouping related to severity classification and use of medication between the group that suffered violence and the one that did not.
Considering the aforementioned variables, having suffered violence during the pandemic increases patients' chances of starting to use anxiety medication by 97%. Moreover, being a nurse, nursing assistant or technician, or having other healthcare-related jobs (not doctors) increase the chances by, 61%, 18%, and 58%, respectively. Finally, anxiety levels classified as mild, moderate, or severe increase the odds by 111%, 305%, and 808%, respectively (Table 4).

Table 4. Multivariate analysis of variables related to medication initiation during the pandemic.
In this work, healthcare professionals in Brazil who suffered any violence during the COVID-19 pandemic presented higher scores of anxiety in comparison to those who did not. Almost half of the participants (49.23%) reported having suffered some type of violence during the pandemic, and 30% of that group had not been victims of violence before the pandemic this reflects what has been observed in other studies. Corroborating our study, another one carried out with Chinese health professionals also showed that those who suffered violence in the workplace had a lower quality of life (25). In addition, a study in Saudi Arabia demonstrated the risk factors associated with higher levels of anxiety: being a nurse, having a previous history of anxiety, having a chronic disease and being a smoker (26).
Globally, many professionals were victims of violence in their workplace by family members of hospitalized patients who happened to be distressed by the uncertain results of effective therapies against COVID-19, risk of death and suspension of hospital visits (14, 25). Violence also occurs out of the professionals' workplace due to fear of being infected, since they work in direct contact with COVID patients (27). That leads people (even family and friends) to avoid or socially reject healthcare personnel (28).
Anxiety has been the most common mental health-related symptom presented by health professionals during the COVID-19 pandemic (17). According to the WHO, Brazil already was the country with the highest rate of people suffering from anxiety disorders in the world (1, 29). The data provided by the WHO informs that 9.3% of the Brazilian population have an anxiety disorder (1). There is no data informing the prevalence of anxiety disorder in Brazil during the pandemic to date. However, studies have shown a prevalence of anxiety among health professionals about 40% in others countries (19). Therefore, it is expected to verify an increased amount of people suffering from anxiety disorders in a near future in Brazil.
In this study, 75.3% of the participants were women and 52.4% were classified as having some level of anxiety. Data have showed that 70% of frontline professionals are women who, in addition to work, have to meet the demands of home, caring for children and other family members (30). This is in consonance with studies that linked anxiety, stress, burnout, and depression to being a female, at a young age, working as a nurse, and directly dealing with patients with COVID-19 (31). This overload and the pressure of having to fulfill all these roles can lead to feelings of frustration, anxiety and stress (8).
In fact, the overall prevalence of mental health diseases in women is higher, compared to men (32). However, men are far less likely to seek mental health treatment due to stigma (14, 32), according systematic review, in which showed that women have less stigma regarding seeking help for mental illness (33). Generally, social norms and cultural expectations enhance a powerful and dominant figure of men, making it difficult for them to express negative emotions and seek mental health care when necessary (32). The stigma related to mental illness can involve factors such as social, personal, professional, and cultural stigma. All these aspects act as barriers for the sick person and make it difficult to seek help.
Apart from women, nursing professionals are more likely than physicians to suffer from stress (8). Studies involving health professionals during the pandemic showed that the longer the time in contact with patients and their relatives, and the closer these professionals are to them, the greater is the number of mental health-related symptoms presented by nurses (26, 34). In this study, working as a nurse increased the chances of an individual starting to take anxiety medication by 61%. Nevertheless, reluctance in seek mental health treatment among physicians is common due to stigma. Physicians fear that if they disclose illness to their colleagues they will be judged as weak and less capable of doing their jobs, and maybe our findings could be due to this (35).
When asked about the use of medication to treat anxiety, 18.70% of the participants reported to have started taking it during the pandemic. Another study has shown that healthcare professionals with high levels of anxiety before the pandemic were more likely to seek help from mental health professionals (26). Yet, many of them do not admit that they need help, since their role as health professionals is to treat sick people. Thus, they are slow to seek help, or end up self-medicating (36). Self-medication among health professionals has been the target of other studies showing that many professionals start taking medication on their own since they have easy access to it, and because they can get prescriptions from co-workers (36, 37).
The COVID-19 pandemic had consequences that go beyond the disease and the number of deaths caused by it, for example: increasement of mental health disorders mostly anxiety and depression, financial problems for those who lost their jobs, feelings of guilt due to the loss of family members and social isolation (26, 38–42). Studies on public health crises emphasize that mental health care should be as paramount as primary care (42). Therefore, government officials must immediately pay attention to the effects of the pandemic in order to prevent further damage to the mental health of these professionals, whose work is crucial in the fight against COVID-19, but also because they need to be mentally well to play their roles in society.
The limitation faced by this research is the fact that the sampling was performed without a probabilistic sampling in Brazil, meaning that the number of participants is not a representative sample. In addition, snowball sampling can create an imbalanced number of participant classes, so participants from some groups may have far greater numbers than others. However, since Brazil is a continental-size country, this work counted on the participation of people from all regions, which allowed a broader view of the violence issue in the pandemic scenario.
The GAD-7 scale is a screening tool for anxiety, and the cross-sectional nature of this study does not allow for a proven diagnosis, which must be carried out by experts. Anyhow, the aim of this study was to verify the degree of anxiety based on the participants' responses.
In Brazil, health professionals who have suffered violence during the COVID-19 pandemic have higher anxiety scores in comparison to those who have not. Additionally, being nurses or other types of health professionals, and having a mild, moderate, or severe anxiety level have higher risk to start taking anxiety medication.
The datasets for this study can be found in the Figshare repository: http://doi.org/10.6084/m9.figshare.c.5585541.
The studies involving human participants were reviewed and approved by Comite de Ética Universidade Estadual de Maringá. The patients/participants provided their written informed consent to participate in this study.
MariB conceived the study, drafted the manuscript, and collected the data. LS and LA conducted the statistical analysis. AA designed the study. GG, AD, MarcB, JN, and SP helped to revise the manuscript. MC supervised the study. All authors have read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank all the healthcare professionals who participated in the research, as well as the Coordination for the Improvement of Higher Education Personnel (CAPES), the State University of Maringá and the Digital Technologies and Geoprocessing Research Group (GETS).
1. World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. Geneva: World Health Organization (2017).
2. Feter N, Caputo EL, Doring IR, Leite JS, Cassuriaga J, Reichert FF, et al. Sharp increase in depression and anxiety among Brazilian adults during the COVID-19 pandemic: findings from the PAMPA cohort. Public Health. (2021) 190:101–7. doi: 10.1016/j.puhe.2020.11.013
3. Xiong J, Lipsitz O, Nasri F, Lui LMW, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. (2020) 277:55–64. doi: 10.1016/j.jad.2020.08.001
4. Silva DFO, Cobucci RN, Soares-Rachetti VdP, Lima SCVC, Andrade FB de. Prevalence of anxiety among health professionals in times of COVID-19: a systematic review with meta-analysis. Cien Saude Colet. (2021) 26:693–710. doi: 10.1590/1413-81232021262.38732020
5. Liu S, Yang L, Zhang C, Xiang Y-T, Liu Z, Hu S, et al. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry. (2020) 7:e17–8. doi: 10.1016/S2215-0366(20)30077-8
6. Xiang Y-T, Yang Y, Li W, Zhang L, Zhang Q, Cheung T, et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry. (2020) 7:228–9. doi: 10.1016/S2215-0366(20)30046-8
7. Rajkumar RP. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatr. (2020) 52:102066. doi: 10.1016/j.ajp.2020.102066
8. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. (2020) 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
9. World Health Organization. The Coronavirus Disease (COVID-19) Dashboard – Brazil Situation. World Health Organization (2021). Available online at: https://covid19.who.int/region/amro/country/br (accessed July 2, 2021).
10. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Doença pelo Novo Coronavírus – COVID-19. Available online at: https://www.gov.br/saude/pt-br/media/pdf/2021/julho/23/boletim_epidemiologico_covid_72_final23jul21-c-1.pdf (Accessed June 13, 2021).
11. Cox CL. ‘Healthcare Heroes’: problems with media focus on heroism from healthcare workers during the COVID-19 pandemic. J Med Ethics. (2020) 46:510–3. doi: 10.1136/medethics-2020-106398
12. Gonçalo Jr T. Profissionais de saúde são hostilizados em trens: ‘Sai do vagão, seu doente’. Estadão. São Paulo (2020). Available online at: https://saude.estadao.com.br/noticias/geral,profissionais-de-saude-saohostilizados-em-trens-sai-do-vagaoseu-doente,70003246731 (accessed June 13, 2021).
13. Sheather J, Hartwell A, Norcliffe-Brown D. Serious violations of health workers' rights during pandemic. BMJ. (2020) 370:m2824. doi: 10.1136/bmj.m2824
14. Bagcchi S. Stigma during the COVID-19 pandemic. Lancet Infect Dis. (2020) 20:782. doi: 10.1016/S1473-3099(20)30498-9
15. Punzalan J. Ambulance driver hurt after getting shot over parking row in Quezon. ABS-CBN News. (2020). Available online at: https://news.abscbn.com/news/04/03/20/ambulancedriver-hurt-after-getting-shot-overparking-row-in-quezon (accessed May 3, 2021).
16. McKay D, Heisler M, Mishori R, Catton H, Kloiber O. Attacks against health-care personnel must stop, especially as the world fights COVID-19. Lancet. (2020) 395:1743–5. doi: 10.1016/S0140-6736(20)31191-0
17. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. (2020) 88:901–7. doi: 10.1016/j.bbi.2020.05.026
18. Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzog W, et al. Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Med Care. (2008) 46:266–74. doi: 10.1097/MLR.0b013e318160d093
19. Beard C, Björgvinsson T. Beyond generalized anxiety disorder: psychometric properties of the GAD-7 in a heterogeneous psychiatric sample. J Anxiety Disord. (2014) 28:547–52. doi: 10.1016/j.janxdis.2014.06.002
20. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
21. Kroenke K, Spitzer RL, Williams JBW, Monahan PO, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. (2007) 146:317–25. doi: 10.7326/0003-4819-146-5-200703060-00004
22. Bitencourt MR, Alarcão ACJ, Silva LL, Dutra A de C, Caruzzo NM, Roszkowski I, et al. Predictors of violence against health professionals during the COVID-19 pandemic in Brazil: a cross-sectional study. PLoS ONE. (2021) 16:e0253398. doi: 10.1371/journal.pone.0253398
23. Fritz CO, Morris PE, Richler JJ. Effect size estimates: current use, calculations, and interpretation. J Exp Psychol Gen. (2012) 141:2–18. doi: 10.1037/a0024338
24. Hinz A, Mehnert A, Kocalevent R-D, Brähler E, Forkmann T, Singer S, et al. Assessment of depression severity with the PHQ-9 in cancer patients and in the general population. BMC Psychiatry. (2016) 16:22. doi: 10.1186/s12888-016-0728-6
25. Xie X-M, Zhao Y-J, An F-R, Zhang Q-E, Yu H-Y, Yuan Z, et al. Workplace violence and its association with quality of life among mental health professionals in China during the COVID-19 pandemic. J Psychiatr Res. (2021) 135:289–93. doi: 10.1016/j.jpsychires.2021.01.023
26. Alenazi TH, BinDhim NF, Alenazi MH, Tamim H, Almagrabi RS, Aljohani SM, et al. Prevalence and predictors of anxiety among healthcare workers in Saudi Arabia during the COVID-19 pandemic. J Infect Public Health. (2020) 13:1645–51. doi: 10.1016/j.jiph.2020.09.001
27. Devi S. COVID-19 exacerbates violence against health workers. Lancet. (2020) 396:658. doi: 10.1016/S0140-6736(20)31858-4
28. Chen Q, Liang M, Li Y, Guo J, Fei D, Wang L, et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry. (2020) 7:e15–16. doi: 10.1016/S2215-0366(20)30078-X
29. de Souza IM, Machado-de-Sousa JP. Brazil: world leader in anxiety and depression rates. Braz J Psychiatry. (2017) 39:384. doi: 10.1590/1516-4446-2017-2300
30. Mehta S, Machado F, Kwizera A, Papazian L, Moss M, Azoulay É, et al. COVID-19: a heavy toll on health-care workers. Lancet Respir Med. (2021) 9:226–8. doi: 10.1016/S2213-2600(21)00068-0
31. Carmassi C, Foghi C, Dell'Oste V, Cordone A, Bertelloni CA, Bui E, et al. PTSD symptoms in healthcare workers facing the three coronavirus outbreaks: what can we expect after the COVID-19 pandemic. Psychiatry Res. (2020) 292:113312. doi: 10.1016/j.psychres.2020.113312
32. Chatmon BN. Males and mental health stigma. Am J Mens Health. (2020) 14:1557988320949322. doi: 10.1177/1557988320949322
33. Clement S, Schauman O, Graham T, Maggioni F, Evans-Lacko S, Bezborodovs N, et al. What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol Med. (2015) 45:11–27. doi: 10.1017/S0033291714000129
34. Shechter A, Diaz F, Moise N, Anstey DE, Ye S, Agarwal S, et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen Hosp Psychiatry. (2020) 66:1–8. doi: 10.1016/j.genhosppsych.2020.06.007
35. Brower KJ. Professional stigma of mental health issues: physicians are both the cause and solution. Acad Med. (2021) 96:635–40. doi: 10.1097/ACM.0000000000003998
36. Montgomery AJ, Bradley C, Rochfort A, Panagopoulou E. A review of self-medication in physicians and medical students. Occup Med. (2011) 61:490–7. doi: 10.1093/occmed/kqr098
37. Robinson J, Sareen J, Cox BJ, Bolton J. Self-medication of anxiety disorders with alcohol and drugs: results from a nationally representative sample. J Anxiety Disord. (2009) 23:38–45. doi: 10.1016/j.janxdis.2008.03.013
38. Clemente-Suárez VJ, Dalamitros AA, Beltran-Velasco AI, Mielgo-Ayuso J, Tornero-Aguilera JF. Social and psychophysiological consequences of the COVID-19 pandemic: an extensive literature review. Front Psychol. (2020) 11:580225. doi: 10.3389/fpsyg.2020.580225
39. Lima CKT, Carvalho PM de M, Lima I de AAS, Nunes JVA de O, Saraiva JS, de Souza RI, et al. The emotional impact of coronavirus 2019-nCoV (new coronavirus disease). Psychiatry Res. (2020) 287:112915. doi: 10.1016/j.psychres.2020.112915
40. Pancani L, Marinucci M, Aureli N, Riva P. Forced social isolation and mental health: a study on 1,006 Italians under COVID-19 lockdown. Front Psychol. (2021) 12:1540. doi: 10.3389/fpsyg.2021.663799
41. Duan L, Zhu G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry. (2020) 7:300–2. doi: 10.1016/S2215-0366(20)30073-0
Keywords: COVID-19, violence, healthcare personnel, psychological violence, occupational health, anxiety
Citation: Bitencourt MR, Silva LL, Alarcão ACJ, Dutra AdC, Bitencourt MR, Garcia GJ, de Andrade L, Nickenig Vissoci JR, Pelloso SM and Carvalho MDdB (2021) The Impact of Violence on the Anxiety Levels of Healthcare Personnel During the COVID-19 Pandemic. Front. Psychiatry 12:761555. doi: 10.3389/fpsyt.2021.761555
Received: 20 August 2021; Accepted: 05 October 2021;
Published: 05 November 2021.
Edited by:
Christos Theleritis, National and Kapodistrian University of Athens, GreeceReviewed by:
Jasmine M. Noble, Institute of Health Economics, CanadaCopyright © 2021 Bitencourt, Silva, Alarcão, Dutra, Bitencourt, Garcia, de Andrade, Nickenig Vissoci, Pelloso and Carvalho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariá Romanio Bitencourt, cm9tYW5pby5tYXJpYUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.