
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 11 October 2021
Sec. Public Mental Health
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.741328
 Kamrun Nahar Koly1*
Kamrun Nahar Koly1* Cleo Baskin2
Cleo Baskin2 Ivylata Khanam1Mala Rao2Sabrina Rasheed1Graham R. Law3Farhana Sarker4Shamini Gnani2
Ivylata Khanam1Mala Rao2Sabrina Rasheed1Graham R. Law3Farhana Sarker4Shamini Gnani2Background: To bridge significant mental health treatment gaps, it is essential that the healthcare workforce is able to detect and manage mental health conditions. We aim to synthesise evidence of effective educational and training interventions aimed at healthcare workers to increase their ability to detect and manage mental health conditions in South and South-East Asia.
Methods: Systematic review of six electronic academic databases from January 2000 to August 2020 was performed. All primary research studies were eligible if conducted among healthcare workers in South and South-East Asia and reported education and training interventions to improve detection and management of mental health conditions. Quality of studies were assessed using Modified Cochrane Collaboration, ROBINS-I, and Mixed Methods Appraisal Tools and data synthesised by narrative synthesis. Results are reported according to Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines. A review protocol was registered with the PROSPERO database (CRD42020203955).
Findings: We included 48 of 3,654 screened articles. Thirty-six reported improvements in knowledge and skills in the detection and management of mental health conditions. Training was predominantly delivered to community and primary care health workers to identify and manage common mental health disorders. Commonly used training included the World Health Organization's mhGAP guidelines (n = 9) and Cognitive Behavioural Therapy (n = 8) and were successfully tailored and delivered to healthcare workers. Digitally delivered training was found to be acceptable and effective. Only one study analysed cost effectiveness. Few targeted severe mental illnesses and upskilling mental health specialists or offered long-term follow-up or supervision. We found 21 studies were appraised as low/moderate and 19 as high/critical risk of bias.
Interpretation: In low resource country settings, upskilling and capacity building of primary care and community healthcare workers can lead to better detection and management of people with mental health disorders and help reduce the treatment gap.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42020203955.
South and South-East Asian countries comprise one-quarter of the world's population and approximately 150–200 million people have a diagnosed psychiatric disorder and limited access to mental health (1, 2). This has significant health and socio-economic implications; the estimated global loss by 2030 is 12 billion working days and $16 trillion to the economy (3). Despite this huge burden, <1% of national budgets in the South and South-East Asian regions are allocated to mental health (4).
International effort has focussed on reducing the mental health treatment gap in low-middle income countries (LMIC) (5). Acute shortages of qualified mental healthcare workers all levels of the health system significantly contribute to the treatment gap, which is compounded by the centralisation of mental health specialists in urban secondary and tertiary care hospitals (6–10). Although the World Health Organisation (WHO) strongly recommends integrating mental health services into primary care delivery (11), only 30% of South and South-East Asian countries have trained primary care doctors in mental health and only 50% have trained nurses (12).
To address this many LMICs have adopted a task-distribution approach whereby community health workers, with fewer qualifications and a small amount of training, deliver mental health services. However, it still remains necessary to increase the number of highly qualified mental health specialists, namely psychiatrists, psychiatric nurses, psychologists, and clinical psychologists, to manage sicker patients and deliver training, support and supervision to non-specialists.
Education and training of the healthcare workforce is key to reducing the mental health treatment gap and achieving universal health coverage. Our review aimed to describe the various types of educational and training interventions targeted at healthcare workers in South and South-East Asia to improve detection and management of people mental health conditions, their cost- effectiveness, and the enabling factors and barriers that influence the effectiveness of these interventions.
This review was registered in PROSPERO (registration number CRD42020203955) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-SR) guidelines (13). Ethical approval was not sought for this study as it was an evidence synthesis of existing published research. A detailed research protocol has been previously published (14). Further, there was no deviation from the protocol.
• What type of educational and training interventions have been used to improve the knowledge, skills, and attitudes of healthcare workers in South and Southeast Asian countries in the early detection and management of people with mental health conditions?
• What type of interventions are effective and for whom are they effective?
• What factors, enabling and barriers, influence how effective these interventions are?
• What type of educational and training interventions are cost-effective?
We included studies that focussed on healthcare workers including doctors, nurses, primary healthcare workers, community workers, and lay health counsellors, who are part of the formal health system (Table 1). While there are various permutations and combinations of what constitutes a “formal health workforce,” we have used a widely accepted definition to be individuals employed by the health system to provide direct patient care, in this case mental healthcare, and excluded studies involving volunteers and medical, nursing, or therapy students. We acknowledge that volunteers and students, whilst not a formal part of the healthcare sector, can play a key role (15).
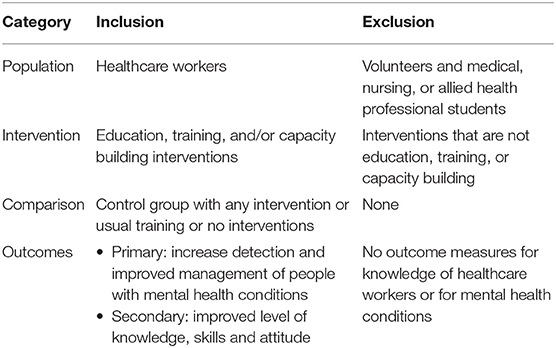
Table 1. Eligibility criteria.
We included studies conducted in countries that are part of South Asia and South-East Asia regions. We used the World Bank's regional definition for South Asian countries (Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, and Sri Lanka). We used World Health Organisation's definition for South-East region as they overlap (Afghanistan, Bangladesh, Bhutan, Democratic People's Republic of Korea India, Indonesia, Maldives, Myanmar, Nepal, Pakistan, Sri Lanka, Thailand, and Timor-Leste). We excluded other countries as we sought to reflect cultural and religious similarities in populations.
Interventions had to involve an activity associated with the education, training, or capacity building of healthcare workers to detect and manage mental health conditions. We included all mental health disorders, as defined by the World Health Organization's International Classification of Diseases (ICD)10 (16) and ICD-11 (17) or American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM) IV (18) and DSM-V (19). We included all primary research studies published in English. Abstracts, posters, book chapters, editorials, letters, and secondary research were excluded. Studies published before 2000 were excluded to ensure findings were relevant to current mental health systems.
We searched six electronic databases on 3 August 2020: Medline, Embase, PsycINFO, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane, and Global health.
The search strategy (Supplementary Table 1) was created using the PICO (population; intervention; comparison; outcomes) framework adapted for each electronic database. We included all primary research studies regardless of the presence of a comparison group to optimise the number of articles identified. To further identify relevant studies, we searched the reference list of all studies selected for inclusion, using forward and backward citation techniques, along with manual searching of journals. We repeated the literature search before data analysis to ensure no recent publications were missed.
Using Covidence systematic review software, two independent reviewers (KNK and CB) screened non-duplicate titles and abstracts and conducted full text review. All conflicts at abstract and full-text stage (32% of articles) were resolved by a third reviewer (SG).
Two reviewers (CB, MIK) extracted data independently in Excel and included: country; study design; study setting; study period; sample size; age range; gender distribution; socio-demographic and cultural background; intervention characteristics checklist (Template for Intervention Description and Replication) (20); details of control conditions; outcomes; theory of change; factors influencing implementation of intervention.
The risk of bias of each study was critically assessed by two independent reviewers (BC, MK) and disagreements were resolved by review team discussion. We used the Cochrane Collaboration Tool (21) to assess RCT studies and report an overall assessment of bias as “low,” “high,” or “unclear.” The ROBINS-I (Risk of Bias in Non-randomised Studies-of Interventions) tool (22) was used to assess the risk of bias for non-randomised trials and categorise each of the seven domains as “low,” “moderate,” “serious,” “critical,” or “no information.” MMAT (Mixed Method Appraisal Tool) version-8 (23) was used to appraise the quality of qualitative and mixed methods studies; each of the five domains were categorised as “yes,” “no,” or “can't tell.”
We screened 3,654 abstracts and 147 full text studies and identified 48 studies that met our eligibility criteria (PRISMA flow diagram, Figure 1).
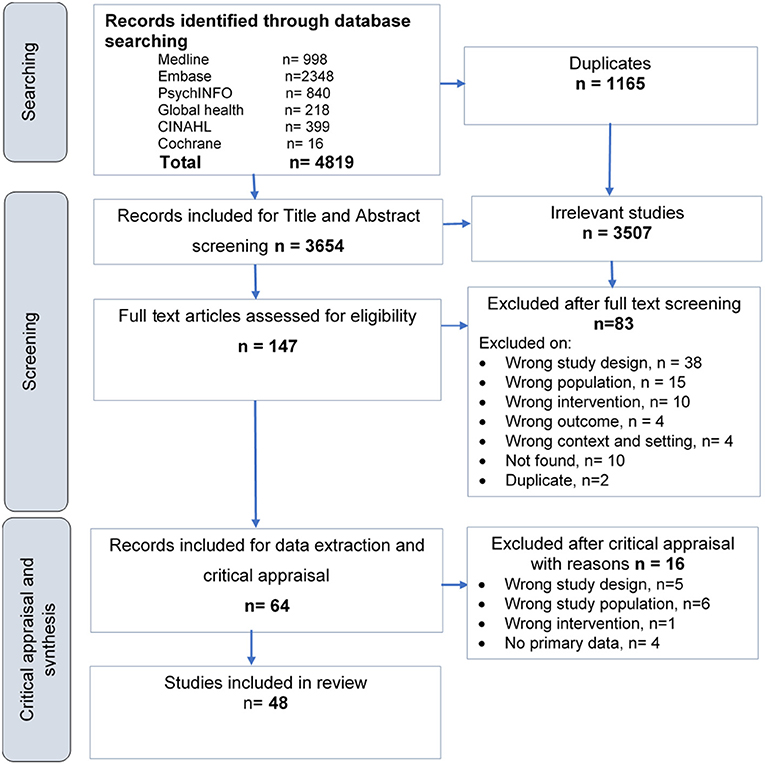
Figure 1. PRISMA flow diagram of included studies.
Of the 48 studies conducted in South and South-East Asia, most studies were undertaken in India (n = 17) followed by Nepal (n = 10), Pakistan (n = 5), Sri Lanka (n = 3), Indonesia (n = 2), Afghanistan (n = 1), and Bangladesh (n = 1) (Table 2). No studies were conducted in Bhutan, Democratic People's Republic of Korea, Maldives, Myanmar, Thailand, or Timor-Leste. Nine studies described an intervention with no primary data (Table 3) and were undertaken in India (n = 6), Afghanistan (n = 1), Bangladesh (n = 1), and Sri Lanka (n = 1).

Table 2. Summary of review studies (N = 39).
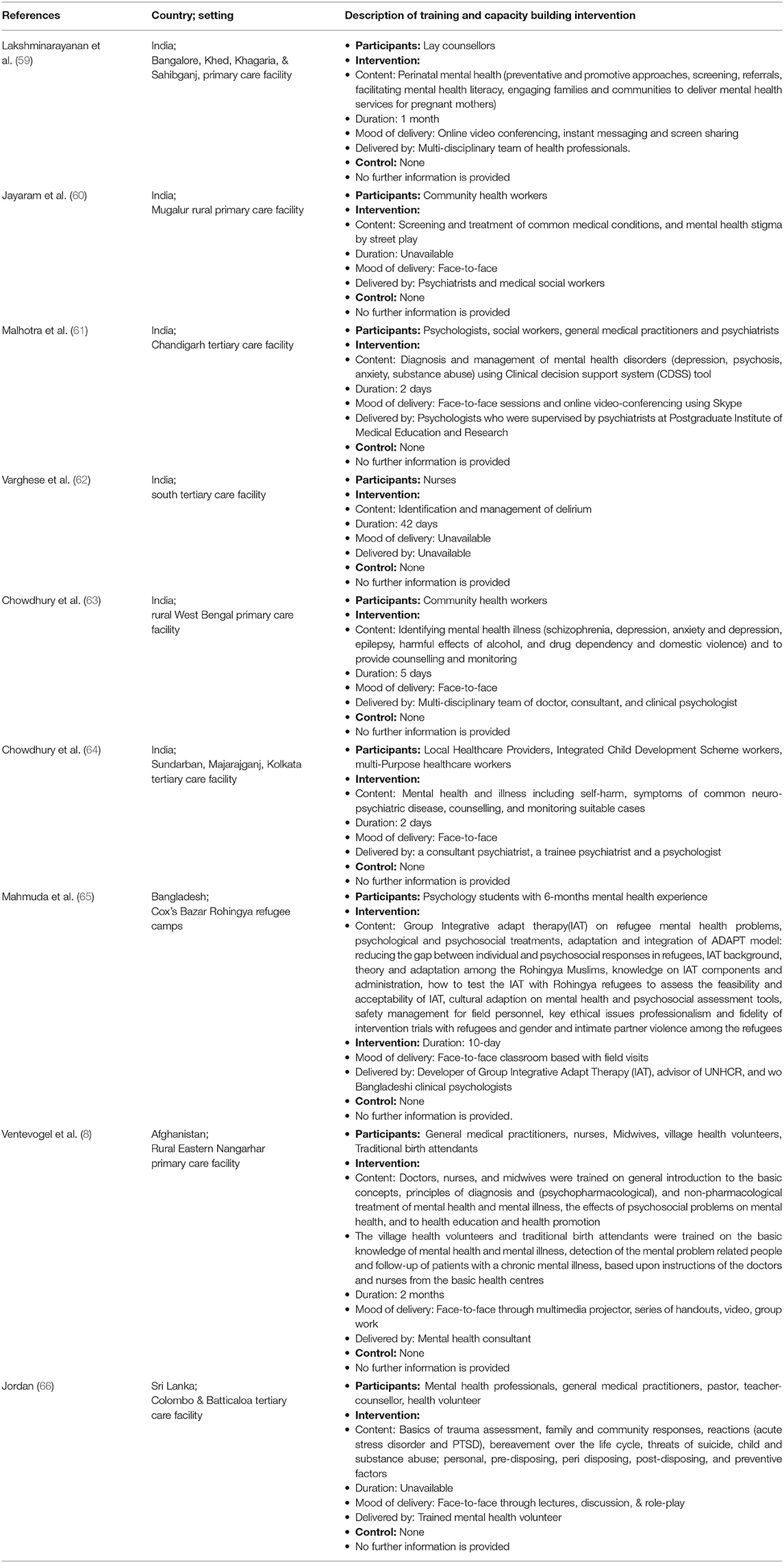
Table 3. Summary of articles with description of intervention only (N = 9).
Most studies were conducted in rural primary care settings (n = 36) followed by tertiary care (n = 9), and other settings (n = 3). There were 31 quantitative studies (21 pre-post-studies, seven RCTs, two quasi-experimental design, and one case-control study). Five studies were qualitative and three mixed methods.
Six of the seven RCT studies were assessed as low-risk and one as high-risk. Among the non-randomised RCTs (n = 23), using the Robins-I tool, four studies were categorised as critical, 10 as serious risk, eight as moderate risk, and one as low risk of bias. We used MMAT to assess risk of bias for eight studies; four were categorised as low-risk, three as high-risk and one as critical risk of bias.
Tirmizi's et al. (24) quasi-experimental study reported results of training on depression delivered to primary healthcare workers in four districts in Afghanistan. The intervention group (n = 62) received recorded lectures and video training via smartphones and face-to-face lectures over 1 month with weekly Skype question and answer sessions. Details of the control group (n = 32) were not provided. There was a significant improvement post-test in the intervention group compared to the control (mean knowledge score = 16.06 vs. 6.80, p = 0.009).
The WHO mhGAP-HIG (Humanitarian Intervention Guide) tool was evaluated by Tarannum et al. (25). Primary health care workers (n = 62) in Rohingya refugee camps were trained over 6-days to identify and manage people with mental, neurological, and substance use conditions. After seven months of training and supervision, researchers reported improvements in knowledge and skills (pre-post-test: 55 vs. 75%) and increased consultation rates from <40 to 160 per month.
Ashok Malla et al. (26) assessed in his part II paper, the effectiveness of mental health specialists training community health workers (n = 40) to provide basic mental health services for severe mental illnesses in an area of conflict. At 14 months, trained lay health workers diagnosed 262 new cases of severe mental disorders. Patients reported significant improvements in symptoms and functioning [F (df , 3.449) = 104.729, p < 0.001] and in all domains of quality of life including psychological health [F (df , 1.845) = 55.490, p < 0.001].
James et al. (27) evaluated the change in attitude of community health workers (Accredited Social Health Activists–ASHAs) toward people with mental illness after their involvement in a community-based rehabilitation program for people with severe mental illness. Community Attitudes to Mental Illness scale was administered at baseline and after 18 months of training and the study reported significant improvement in three of the four domains (p < 0.001).
Two studies by Maulik et al. (28, 67) evaluated the Systematic Medical Appraisal Referral and Treatment (SMART) Mental Health programme. The intervention comprised (1) an anti-stigma campaign, (2) training of ASHAs to screen for common mental disorders using Android tablets and to refer high-risk individuals to a primary care centre, (3) training of primary care doctors in WHO mhGAP-IG and to implement management guidelines using point-of-care decision support also using Android tablets, and (4) a system for ASHAs and doctors to follow-up patients. The 2017 study (67) evaluated a 10-day training delivered across 30 primary healthcare facilities in 15 villages with two primary care doctors and 21 ASHAs. ASHAs identified and referred 238 individuals with common mental disorders. Use of mental health services increased from 0.8% (n = 238) to 12.6% (n = 30) following the intervention. There was also a significant reduction in depression mean score (3.6, p < 0.0001) and anxiety mean score (1.3, p = 0.004). These results were built on in 2020 (28) among 40 ASHAs and five primary care doctors. Results showed increased mental health service use by patients from 3.3 to 81.2% (odds ratio 133.3, 95% CI 89.0–199.7; P < 0.001) and a significant reduction in mean depression and anxiety scores, from 13.4 to 3.1 (P < 0.001) and from 12.9 to 1.9 (P < 0.001) respectively.
Mehrotra's et al. (30) study examined Project ECHO; a hub and spoke tele-mentoring model that used video technology to connect mental health and addiction care specialists and healthcare providers in rural areas. Healthcare workers (n = 12) from rural hospitals received reading materials and participated in 12 fortnightly video conferences to discuss patients. Results showed improved knowledge (t-test: 3.71, p ≤ 0–01), self-confidence and efficacy (pre- vs. post-test: mean score: 58.16, SD = 12.23 vs. 70.83, SD = 11.06).
Another study by Muke et al. (29) studied the acceptability and feasibility of digital technology (mobiles, laptops, and tablets) to train ASHA workers (n = 32) on depression. They found it useful and convenient but recommended more interactive content, simple language, and greater use of images to increase engagement.
Two Indian studies focussed on older peoples' mental health. A qualitative study by Michael et al. (31) examined a geriatric mental health training program delivered to primary healthcare workers (n = 5). They found knowledge on depression, dementia, anxiety, substance abuse disorders, and use of medical and psychosocial interventions increased. Shaji et al. (40) evaluated dementia training undertaken by academic psychiatrists among 19 community health workers in Kerala using case vignettes. Community health workers identified 1,979 60-year-olds with suspected dementia. Health workers who received additional training identified a further 51 suspected cases; 33 confirmed dementia (positive predictive value of screening was 64.7%).
Shidhaye et al. (33) evaluated a 2-day training programme based on WHO mhGAP-IG training material and conducted under the Programme for Improving Mental health care (PRIME) district-level mental health care plan in rural India. The PRIME team carried out a separate 2-day training programme for 20 front-line workers and 15 paramedical staff on how to detect mental health within the community, where to refer, and how to provide mental health first aid. This was followed by weekly meetings between medical officers and the PRIME team. At 1-month follow-up, five patients were detected as depressed and three were referred to hospital. No pharmacological treatment was provided.
Patel et al. (38) assessed MANAS (MANAshanti Sudhar), a stepped-care intervention in Goa, involving a lay health counsellor, primary care physician, and visiting psychiatrist for individuals with depression and anxiety. Lay health counsellors received a 2-month structured training course to case manage patients, deliver non-drug treatments, and refer patients who do not get better to primary care physicians. Primary care physicians received half a day of training and a manual. Referral to a visiting psychiatrist was reserved for high-risk individuals or those who were unresponsive to earlier treatment. Adults who screened positive for a common mental disorder at primary care facilities (12 public, 12 private) were randomised to receive the MANAS intervention or “enhanced usual care” (n = 2,796) that consisted of primary care physicians who received only a tailored treatment manual. At public facilities, the MANAS intervention was consistently associated with strong beneficial effects over 12 months across all outcomes according to ICD-10 diagnoses: prevalence of common mental disorders (risk ratio = 0.70, 95% CI 0.53–0.92); depression (RR = 0.76, 95% CI 0.59–0.98); and suicide attempts and plans (RR = 0.64, 95% CI 0.42–0.98). In contrast, private facilities showed little evidence of impact.
Nimgaonkar's et al. (34) pre-post-test study evaluated a task-shifting programme in a rural tribal community. Health workers (n = 106) were trained to provide community education and identify and refer individuals with psychiatric problems to a community hospital. Psychiatric patients were followed up to improve treatment adherence. Results showed significant improvements in knowledge and attitude among participants (pre-post-test: 35 vs. 94%) and improvements in daily functioning among treated patients (pre-post-test: mean: 2.38 vs. 2.56; p = 0.01; No CI or SE) and self-referrals rates (27 vs. 57%) over 3 years. The cost of the program was USD 1.6 per person per annum.
Paudel et al. (35) examined the impact of depression and anxiety training delivered to community health workers (n = 26) by social workers. Focus group discussions found participants were able to identify symptoms of depression, suggest management options, and that they were more supportive and empathetic toward patients.
We found two studies that evaluated the effectiveness of Cognitive Behavioural Therapy (CBT) training in rural India. Beck et al. (36) evaluated a 5-day training programme for non-medical health professionals (n = 14) delivered by a clinical psychologist. Results on knowledge and clinical application of CBT were compared with UK participants of the same course; 9.2 vs. 9 and 18.7 vs. 16.3, respectively. Gupta and Aman (68) also evaluated change in knowledge among 20 psychologists, general medical practitioners, consultants, and medical students who received 3-day face-to-face training thorough role play and online supervision by psychiatrists. They found significant improvements in pre- and post- training knowledge among participants, t(13) = −6.899, (p ≤ 0.001, r = 0.886).
Armstrong's et al. (69) study investigated a 4-day mental health training program implemented among 66 community health workers. They were trained by two local healthcare professionals on mental health diagnosis, referrals, mental health first aid, and mental health promotion and were followed up after 3 months. Results showed an improved diagnostic capability in depression (pre-test: 22.7%, 95% CI = 13.3–24.7, p = 0.002) vs. post-test: 50.0%, 95% CI = 37.4–62.7, p = 0.002) and psychosis (pre-test: 9.1%, 95% CI = 3.4–18.7, p = 0.001) vs. post-test 27.3%, 95% CI = 10–39.6, p = 0.001) and a reduction in stigmatising attitudes among patients with mental illness (pre-test: 84.8% vs. post-test: 62.1%).
A study examining a training delivered by booklet to nurses (n = 35) at an Indian tertiary care hospital (37) on suicide prevention. They found improved knowledge (pre- and post-test: Z = 5.183, p ≤ 0.001) and attitude toward suicide attempted patients (pre- and post-test: Z = −4.380, p ≤ 0.001).
Thara et al. (39) conducted a retrospective study to determine the nature, quality and frequency of psychosocial support training delivered to community health workers after the 2004 tsunami in Tamilnadu. Participants (n = 127) were identified from government databases and included both government and NGO-employed community health workers and members of local women's voluntary groups. The majority reported to have benefited greatly from training, however, a lack of coordination led to overlap. Community members were generally happy with the interventions provided and were felt to be necessary for minimum 6 months.
In 2004, Indonesia integrated clinical psychologists into primary care and in 2015, an adapted WHO-mhGAP was incorporated as an add-on training to selected primary care doctors and nurses. Anjara's et al. (70) pragmatic two-arm cluster RCT investigated outcomes in patients who either received mental health care from doctors at primary care clinics who received WHO mhGAP training (n= 14 clinics) or co-located clinical psychologists (n = 14 clinics). Outcomes of doctor care (n = 153 patients) were proven to be statistically not inferior to clinical psychologists (n = 141 patients) in reducing symptoms of social and physical impairment, reducing disability, and improving health-related quality of life at 6 months. Economic analyses indicate lower costs and better outcomes in the co-located clinical psychologist arm.
Citraningtyas et al. (41) conducted a mixed method evaluation of a 5-day Capacity Building for Child and Adolescent Mental Health in Disaster Areas (CAMHD) training-of-trainers in Jakarta. Participants (n = 16) were non-specialist resident doctors, psychiatrists, psychologists, and social workers. Pre-post-test results showed a significant improvement of knowledge (mean = 2.75; 13.75%; p < 0.001) among participants. In qualitative interviews, participants identified the benefits of learning using case studies and role play.
Acharya's et al. (50) evaluated a WHO mhGAP-based training delivered digitally and on-site. Clinicians (n = 27) at a rural Nepali primary care centre viewed five video lectures followed by on-site skills-building and clinical coaching to help use new knowledge in clinical practise. Pre-post-tests indicated a significant increase in median scores on knowledge questionnaires for acute stress (median increase: 20, p = 0.03), grief (40, p < 0.01), psychosis (22, p = 0.01), and post-traumatic stress disorder (PTSD) (20, p= 0.01) but not for depression (11, p = 0.12).
Two RCT studies evaluated the effect of training community health workers to deliver psychosocial interventions (47, 48). Markkula et al. (48) evaluated a 5-day training programme in psychosocial counselling, basic therapeutic skills, CBT, problem-solving, exposure therapy, yoga, and meditation. The control group received 5-day training on detecting and treating mental health disorders with a 3-day refresher course (enhanced usual care). A total of 287 participants (n = 141 intervention; n = 146 control arm), predominantly socially disadvantaged women, were randomised to each arm. The researchers found a significant reduction in depression measured by Beck Depression Inventory (BDI) scale [mean difference −7.43 (95% CI −9.71 to −5.14)] and anxiety (mean difference −5.42, 95% CI −7.59 to −3.27) at 6 months in the intervention compared to the control group suggesting lay psychosocial counselling is effective in treating depression and anxiety.
Sangraula et al. (47) evaluated the training of psychosocial health workers by an NGO to deliver Problem Management Plus (PM+), a five-session intervention designed for individuals with psychological distress living in communities affected by adversity. People diagnosed with depression were randomly allocated to receive PM+ (n = 61) or enhanced usual care (n = 60) which consisted of family meetings, psychosocial support, and information on local mental health services. Patients with mental illness who received PM+ showed a significantly greater reduction in depression (mean score = −3.5), common psychological problems (mean score = −1.0), PTSD (mean score = −2.7) and an increase in perceived social support (mean score = 0.9) compared to the control group.
We found six studies that focussed on examining the impact of the PRIME district mental health plan, an intervention to scale up treatment for alcohol use disorder, depression, epilepsy, and psychosis in primary care in Chitwan, Nepal. As part of PRIME, primary care workers were trained in the WHO mhGAP. Kohrt et al. (49) conducted an evaluation of 44 primary care workers who took part in the training. They found improved mean scores for knowledge (10.37, p < 0.001, d = 1.75) and competencies (7.87, p < 0.001, d = 1.44) on mental health and reduced stigma toward people with mental illness (−3.25, p = 0.003, d = −0.55).
As part of PRIME, community health workers were trained to use the Community Informant Detection Tool (CIDT) tool to identify and refer individuals with mental illness to primary care centres. Jordans et al. conducted two studies (44, 51) to evaluate this training. In their pragmatic RCT, community health workers at 24 health facilities were randomly assigned to receive “standard and CIDT training” (intervention) or “standard” training alone (control). All participants were trained on mental health, stigma, mental health services in primary care, and self-referral. The CIDT group received additional training in proactive community referrals consisting of vignettes and pictures designed for low literacy populations. The authors compared the number of patients registered at health facilities before and 6 months post training; 309 patients were registered at health facilities in the CIDT group compared with 182 patients in the control group (median = 24 vs. 16, p = 0.04, r = 0.42).
Aldridge et al. (42) evaluated the indirect impact of PRIME on suicidal ideation among individuals diagnosed with depression (n = 137 treatment; n = 75 control) and alcohol use disorder (AUD) (n = 175 treatment; n = 57 comparison). Participants in the treatment group received psychotropic medication, psychosocial support, and psychoeducation according to mhGAP-IG clinical decision algorithm. The control group received standard primary care with no mental health treatment provided. Patients with depression in the treatment group had a greater reduction in ideation compared to the control group at 12 months (OR = 0.31, 95% CI: 0.08–1.12; p = 0.07), with a significant treatment over time effect (p = 0.02). Among the AUD group, there was no significant difference in suicidal ideation between treatment and control group at 12 months (OR = 0.46, 95% CI: 0.06–3.27; p = 0.44), and no treatment over time effect (p = 0.72).
Kohrt et al. (45), conducted a mixed-method evaluation of integrating anti-stigma modules (entitled RESHAPE) into the PRIME mental health care program. The adapted training curriculum was delivered in two sessions to 41 primary healthcare providers. In qualitative interviews, primary healthcare providers described positive changes in their views that individuals with mental illness are violent and their ability to treat mental illness effectively. At 16 months, their willingness to interact with individuals with a mental illness increased from 54% pre-training to 81% and observed clinical competency increased from 49 to 93%.
Luitel et al. (46), conducted a process evaluation of the implementation of PRIME in Chitwan. They reported challenges due to low levels of mental health literacy, heavy workload among primary care workers, frequent transfer of trained staff, stigma, inadequate physical facilities, lack of private consultation rooms, complex and lengthy drug procurement and distribution processes, and poor mental health supervision in primary care. They found primary care workers were motivated to learn about mental healthcare, and that mentoring and supervision provided by psychiatrists, support from the Ministry of Health and the District Public Health Office, and procurement of new psychotropic medicines helped overcome implementation challenges.
Three studies evaluated the “Thinking Healthy Program” (THP), a CBT-based training delivered to community health workers to treat perinatal depression that has been integrated into the heath system in Pakistan. Rahman et al. (71) evaluated a digital adaptation of THP. The Technology-Assisted Cascaded Training and Supervision (TACTS) system facilitated the training of community health workers using an Android tablet through a cascade training/supervision model. The cascade model began with a specialist THP master trainer (n = 1) training a non-specialist THP trainer (n = 1; psychology graduate) in a 5-day workshop and a Skype supervision session. These non-specialist trainers then delivered a 5-day technology-assisted training to four community health workers trained as supervisors and continued to supervise them via monthly Skype sessions. These supervisors then cascaded the 5-day training to 40 community health workers. Eighty community health workers were randomly assigned to either TACTS or conventional face-to-face training and supervision by a specialist. Results indicated no significant differences between health workers trained using TACTS and supervised from distance vs. those trained and supervised by a specialist face-to-face (mean ENACT score 24.97 vs. 27.27, p = 0.079, 95% CI 4.87–0.27) and at 3 months follow-up assessment (44.48 vs. M = 43.63, p = 0.53, CI −1.88–3.59).
Zafar et al. (54) qualitative study evaluated THP training for 40 community health workers within a combined nutrition and early child development program was found to be useful and effective. THP training was conducted in the first 2 days of a 5-day training program, and skills learned were repeatedly practised throughout the five days. Study participants were able to apply these skills effectively and the approach was found to be useful by community health workers, mothers, and their families.
Rahman's et al. (52) RCT examined the THP training which was delivered to community health workers using a manual, which could be kept for reference. Mothers in the intervention clusters (n = 463) received the THP training from 20 specially trained community health workers. Mothers in the control clusters (n = 440) received the same number of visits to those in the intervention group but by routinely trained community health workers (n = 20). At 6 months, 23 and 53% mothers in the intervention and control groups, respectively, met the criteria for major depression [adjusted odds ratio (OR) 0.22, 95% CI 0.14–0.36, p < 0.0001]. These effects were sustained at 12 months (27 vs. 59%, adjusted OR 0.23, 95% CI 0.15–0.36, p < 0.0001).
Humayun et al. (53) evaluated a mhGAP training delivered to 56 physicians and psychosocial staff in a conflict-affected district in Pakistan. The 2-day training was delivered by psychiatrists and focused on diagnosis, treatment, follow-up, and referral of mental, neurological and substance use disorders. Participant mean pre- and post-test scores were 15.43, 62% (p = 0.000, S.D. 4.05) and 19.48, 78% (p =0.000, S.D. 3.13), respectively, which showed significant improvement.
Taj et al. (55) conducted a 5-day face-to-face multi-method teaching program for 50 mental health professional on practical skills to manage depression, anxiety, substance abuse, and other common problems through role plays and video and slide presentations by mental health professionals. Result showed an improved knowledge score (pre- vs. post-test: 65 vs. 74%).
We found two studies evaluating training that used WHO mhGAP guidelines to integrate mental health into primary care in Sri Lanka. Siriwardhana et al. (56) found knowledge scores improved after a 3-day training delivered to primary care practitioners (n = 12) serving post-conflict populations (pre- vs. post-test: 72.8%, SD: 11.4 vs. 77.2%, SD: 11.8). Jenkins et al. (58) evaluated the training of 260 primary care staff in five areas in Sri Lanka and found improved knowledge in pre- vs. post-test scores in all.
Blignault et al. (57) conducted a two phased collaborative capacity-building training program adopting a train-the trainer model. In phase I, 14-day face-to-face training course took place in Sydney, Australia for eight senior clinicians to improve their identification and management of mood disorders. After 3 months, they received 5-day follow-up training and went on to train 48 medical officers of mental health and 42 psychiatric support workers and general counsellors over 5 days (phase II). Results demonstrated the improved mental health knowledge (pre- vs. post-test: 4.5 ± 2.5 vs. 6.2 ± 2.0, CI = 0.86–2.71, p = 0.0002) and attitude toward people with mental illness (pre- vs. post-test: 36.9 ± 6.9 vs. 32.4 ± 7.2, CI = 2.82–6.15, p = 0.0000) among participants.
Among 48 reviewed articles, training was provided and evaluated in 39 studies (81%) (24–31, 33–58, 67–71) (Table 2) and another nine studies (19%) (42–51) (Table 3) only described the intervention or training module and did not report any results.
Of the 39 studies, the majority focused training to general medical practitioners (n = 13, 33%) (24, 28, 34, 38, 41, 50, 53, 56–58, 67, 68, 70) followed by nurses (n = 5, 13%) (25, 34, 37, 45, 70), psychologists (n = 4, 10%) (25, 30, 41, 68), psychiatrists (n = 2, 5%) (41, 58) and other non-clinical professionals such as community healthcare workers (n = 29, 74%) (24, 26–31, 33–35, 38–54, 57, 67), health or medical assistants (n = 4, 10%) (25, 45, 50, 69), health educators (n = 2, 5%) (25, 71) and paramedics (n = 1, 3%) (33). Thirty-two studies (82%) were conducted in primary healthcare facilities (24, 26–31, 33–36, 38, 39, 41–44, 46–48, 50, 52–58, 67, 69–71) followed by five studies (13%) in tertiary care settings (37, 40, 45, 49, 51), and two studies (5%) in refugee camps or other (25, 68).
Twenty-three (59%) studies provided interventions that addressed common mental disorders (CMD) (24, 25, 29, 34–36, 38, 39, 41–43, 47–49, 52, 54, 55, 57, 67–71), five (13%) addressed severe mental illness (26, 27, 30, 37, 40), and 10 studies (26%) addressed both common and severe illnesses (28, 31, 33, 44, 45, 49, 50, 53, 56, 58). Thirty-six studies (92%) provided training to participants face-to-face (24–28, 31, 33–58, 67–70) and eight (21%) used digital technology and web-based training (24, 28–30, 50, 67, 68, 71). Training programmes were delivered in a variety of formats, such as lectures and slide presentations, role play, case discussions, audio-visual material, question and answer sessions, team review sessions, and workshops. Most of the training sessions were discrete and they ranged from one to 30 days.
Training interventions were commonly delivered by multi-disciplinary teams (n = 12, 31%) comprising of psychiatrists, psychologists, counsellors, and social workers (25, 26, 28, 30, 33, 37, 41, 49, 56, 67, 69, 70). Six studies (15%) were delivered by a psychiatrist (27, 32, 34, 40, 50, 53), two (5%) by a psychologist (36, 71), and one (3%) by a social worker (35). Eighteen studies did not provide any information regarding trainers. The content of interventions were highly heterogenous. Twelve (31%) studies adapted WHO mhGAP guidelines (24, 25, 28, 33, 42, 44–46, 49, 53, 56, 70) of which six studies (15%) were conducted under the auspices of the PRIME program (33, 42, 44–46, 49) and one integrated the RESHAPE module (3%) (45). Three studies (5%) conducted the THP training (52, 54, 71), two studies (5%) delivered the SMART module (28, 67). There was one study conducted for PM+ training (3%) (47), the MANAS trial (3%) (38) and the SPRING program (3%) (54).
Thirteen (33%) studies trained participants to deliver basics of mental health treatment including eight (21%) studies trained healthcare workers to deliver psychotherapy like CBT (36, 39, 40, 48, 52, 54, 68, 71), psychoeducation, psycho-social counselling, pharmacotherapy, behavioural activation therapy, meditation, and yoga (27, 29, 35, 43, 69).
Twenty-three studies (59%) evaluated the knowledge, skills and attitude of healthcare workers (24, 25, 29–31, 33, 35–37, 41, 43, 45, 46, 49, 50, 53–58, 68, 69), 18 studies (46%) assessed diagnostic capabilities and competencies (26, 27, 29, 30, 33–35, 40–43, 45–47, 51, 54, 69, 71) three (8%) studies assessed referral ability (35, 43, 51), four (10%) measured stigma among healthcare workers (26, 46, 49, 69) and three (8%) assessed patient's well-being status (43, 47, 51).
The mental health status of individuals who received care from trained healthcare workers was measured using a range of scales, including WHODAS (WHO Disability Assessment Schedule), GHQ-12 (General Health Questionnaire-12), PHQ-9 (Patient Health Questionnaire-9), GAD-7 (Generalised Anxiety Disorder), MICA (Mental Illness: Clinicians' Attitudes), and ENACT (Enhancing Assessment of Common Therapeutic factors).
We found digital technology was an effective enabling factor in implementing training among healthcare workers in primary and community settings. Large-scale interventions found it was important to have early and sustained involvement of key stakeholders, including traditional healers and religious leaders. Training that involved a higher number of sessions, a multidisciplinary team, and where there was longer term supervision and mentoring, typically had sustained effects. Other enabling factors included using simple language, synonyms for difficult words, contextually specific images, and interactive content. Interventions that were of low cost and did not require a large time commitment had good participation rates.
Barriers to implementation included the lack of physical space to deliver the training program, as well as implementing the training itself, for example a separate room to offer psychosocial counselling. Other studies reported practical issues such as transport for healthcare workers to attend, inadequate numbers of trainers, and a lack of collaboration between different training providers to adhere to time constraints of the program. Several studies mentioned the quality of training arrangements, such as smaller numbers of sessions and difficulty in understanding guidelines as critical barriers for healthcare workers. Additionally, issues of stigma and inadequate mental health knowledge affected participation rates. Two studies mentioned healthcare workers were re-assigned or retired and lost to follow up.
A few studies described how patients themselves were unwilling to receive treatment due to issues of stigma or as a result of low mental health literacy. A lack of essential psychotropic medications and adequate transport to the healthcare facility were further barriers for patients seeking mental health care.
Only one study conducted a cost-effectiveness analysis (71). In this study, two types of interventions such as technology-assisted cascaded training and supervision (TACTS) and conventional face-to-face training were provided to 40 community healthcare workers. Results showed that costing of a TACTS training program was equally effective and 30% less expensive than the conventional methods of training and supervision.
We examined the risk of bias in 39 of the 48 studies. Thirty-one were quantitative study designs, five qualitative and three mixed methods. Twenty-one quantitative studies had a pre-post-design, of which 10 were appraised with high risk of bias (25, 43, 49, 51, 55–57, 67–69), followed by moderate (n = 6) (26, 27, 30, 34, 40, 53), critical (n = 4) (36, 37, 50, 58) and low risk (n = 1) (45). Two quasi-experimental studies (24, 28) and one case-control studies (42) were assessed as moderate risk of bias.
We assessed seven RCT studies using Cochrane Collaboration tool; six were low risk of bias (n = 6) (38, 44, 47, 48, 52, 71) and only one study was assessed high risk (70). Qualitative studies were appraised using MMAT; three were assessed as low risk of bias (29, 35, 39), one high (54) and one critical risk (31). Among three mixed method studies two studies were low risk (41) and two were high risk of bias (33, 46).
Additional analysis such as meta-analysis was not conducted due to the extreme heterogeneities in terms of population, intervention contents, modalities, measurement scales, and outcome of those studies.
We identified 48 studies since 2000 that focussed on mental health training and upskilling health care workers from South and South-East Asia. Most studies were concentrated in India or Nepal and two studies were conducted in South-East Asia. It is unclear why so few were conducted in South-East Asia, as both regions face a similar mental health burden, experience insufficient levels of investment, and a paucity of mental health policies.
Most of the focus of mental health training was directed toward improving primary healthcare workers' ability to identify, manage, and refer people with mental illness. This finding is consistent with studies in other developing countries (72–75) as well as research from high income countries with stronger health care systems that report intervening in primary care is effective (76, 77). Primary healthcare facilities in countries such as Bangladesh, Pakistan and India can serve between 6,000 and 30,000 people (78–80). Therefore, sensitising primary level health workers about mental health is an efficient use of scarce resources (81, 82). Each country had varied types of primary healthcare workers with differing knowledge and skill gaps; this should be acknowledged when designing interventions (74, 75).
Our review findings are consistent with task sharing research published in other LMICs (83–86) that suggest that community health workers, who have limited or no prior training in the mental health, can effectively deliver psychological interventions. Scaling up these training programmes has potential to strengthen the wider health system as effective, yet the least resource intensive treatment, can be delivered to patients first; only “stepping up” to intensive/specialist services as clinically required (38, 87, 88).
While there was high heterogeneity on the content of interventions, many utilised established mental health modules such as the WHO mhGAP guidelines. Overall, these modules were successful in increasing mental health knowledge and improving the treatment and management of people with mental ill-health (89). Training programmes such as the THP and PM+ demonstrated the broader role of the mhGAP-IG in encouraging the development and evaluation of acceptable, feasible and scalable talking therapies in the South and South-East Asian region. Further evidence on the process of how interventions are being tailored would benefit future efforts to scale established mental health training modules (90, 91).
Many successful interventions were provided by multidisciplinary teams that consisted of both specialists (such as psychiatrists and psychologists) and non-specialists (such as community health workers). Existing research suggests this is an essential tool for constructing an effective and patient-centred healthcare delivery system (92, 93) as it can break down the hierarchy and power of individuals, give more leverage to workers, and produce a higher level of work and job satisfaction (92, 94, 95).
Most interventions were delivered face-to-face, and participants valued content delivered in an interactive manner, for example through role play, case discussion, and question and answer sessions. More recent studies were successful in leveraging digital technology to deliver training and provide ongoing virtual supervision to rural and remote areas and areas with scarce resources. This is consistent with research supporting the benefits of online education and training to overcome geographical, human resource and cost barriers without sacrificing on knowledge outcomes (96, 97). However, it is important to select appropriate digital devices and applications for delivering the intended content, and that these interventions can function offline or within network connectivity constraints of the target setting.
We found only a few studies (26, 28, 34, 38, 42, 47, 48, 51, 52, 67, 69, 70) that evaluated the impact of training in terms of patient outcome. Most studies focused on the initial three stages (reaction, learning, and behaviour) developed by Kirkpatrick and Kirkpatrick (98) in evaluating impact of training. Future studies need to evaluate the effect of training on patient outcome as well as participants.
In many LMICs, volunteers trained by NGOs can play a critical role in the provision of mental healthcare. However, they are excluded in this review as their role in the healthcare workforce is not a sustainable solution for health systems to achieve universal health coverage. Mainstream health services require capacity for basic provision of mental healthcare. We only included studies published in English and may have missed valuable evidence published in the native language to the country where the study was conducted. A broad range of countries were included with diverse health systems and differential need, and this may limit how we generalise our findings to the whole region.
We found few studies that offered supervision and support post-training. Training programmes should ensure that there is continued opportunities for refresher training and/or supervision of healthcare workers as a critical component to ensuring quality of care. Future research should assess long term outcomes in patients to determine if application of newly acquired knowledge and skills in everyday practise is sustained.
Most interventions were designed to detect and manage common mental disorders with severe mental illnesses, such as schizophrenia, severe depression and bipolar affective disorder, less frequently targeted. It is important that healthcare workers can identify and manage individuals with severe mental illnesses, particularly in light of the high burden in the region. Additionally, few studies targeted the upskilling of existing mental health specialists. Even if task-shifting to community health workers is implemented extensively, the need for mental health specialists will continue as they play an essential role in delivery of services and in training, supervision, and mentoring of non-specialist workers (99).
We found only one study that assessed cost effectiveness of intervention (71). Less than 1% of national budgets in the South and South-East Asian region is allocated to mental health, and so the mobilisation of financial resources to develop the healthcare workforce is a major challenge to strengthening mental health systems. It is therefore critical that rigorous cost-effectiveness studies are conducted to inform the design and scaling-up of training interventions.
Training primary and community health workers in the identification and treatment of mental health disorders can lead to significant improvements in knowledge and to the effective delivery of mental health care, through community-based programmes and task-shifting approaches. Future research in the field should focus on severe mental illnesses, upskilling healthcare workers along the entire care pathway, and examining the sustainability of knowledge and skills gained and the role of ongoing supervision.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
KK, CB, IK, and SG developed the study protocol with the contributions from MR, GL, and SR and registered in PROSPERO. KK, CB, IK, and SG developed the search strategy and searched the articles with the help of librarian. Titles, abstracts and full texts of the retrieved articles were screened separately by KK and CB. SG resolved any conflicts as a third reviewer. KK, CB, and IK conducted the data extraction and narrative synthesis with the guidance of SG. KK, CB, IK, and SG developed the manuscript. All authors contributed, critically provided feedback and approved the final version of the manuscript for submission.
This project was funded and supported by the United Kingdom Research and Innovation (UKRI) Global Challenges Research Fund (GCRF) (Grant Reference Number WPPA-G24119).
The views expressed are those of the author(s) and not necessarily those of the UKRI.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the medical librarian at Imperial College London for assistance in developing the search strategy and helping to retrieve articles. The team at Imperial College London and the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) are grateful to the governments of Bangladesh, Canada, Sweden and the UK for providing unrestricted support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.741328/full#supplementary-material
1. Naveed S, Waqas A, Chaudhary AMD, Kumar S, Abbas N, Amin R, et al. Prevalence of common mental disorders in South Asia: a systematic review and meta-regression analysis. Front Psychiatry. (2020) 11:899. doi: 10.3389/fpsyt.2020.602062
2. Thara R, Padmavati R. Community mental health care in South Asia. World Psychiatry. (2013) 12:176. doi: 10.1002/wps.20042
3. Canady V. Mental illness will cost the world $16 trillion (USD) by 2030. Ment Health Wkly. (2018) 28:1–8. doi: 10.1002/mhw.31630
4. Saxena S, Sharan P, Saraceno B. Budget and financing of mental health services: baseline information on 89 countries from WHO's project atlas. J Ment Health Policy Econ. (2003) 6:135–43.
5. Bruckner TA, Scheffler RM, Shen G, Yoon J, Chisholm D, Morris J, et al. The mental health workforce gap in low-and middle-income countries: a needs-based approach. Bull World Health Organ. (2011) 89:184–94. doi: 10.2471/BLT.10.082784
6. WHO. Mental Health Atlas 2017. WHO (2017). Available online at: https://www.who.int/mental_health/evidence/atlas/mental_health_atlas_2017/en/
7. Hossain MD, Ahmed HU, Chowdhury WA, Niessen LW, Alam DS. Mental disorders in Bangladesh: a systematic review. BMC Psychiatry. (2014) 14:216. doi: 10.1186/s12888-014-0216-9
8. Ventevogel P. Integration of mental health into primary healthcare in low-income countries: avoiding medicalization. Int Rev Psychiatry. (2014) 26:669–79. doi: 10.3109/09540261.2014.966067
9. Thara R, Patel V. Role of non-governmental organizations in mental health in India. Indian J Psychiatry. (2010) 52:S389–95. doi: 10.4103/0019-5545.69276
10. Saraceno B, van Ommeren M, Batniji R, Cohen A, Gureje O, Mahoney J, et al. Barriers to improvement of mental health services in low-income and middle-income countries. Lancet. (2007) 370:1164–74. doi: 10.1016/S0140-6736(07)61263-X
11. World Health Organization WH. Mental Health in Primary Care: Illusion or Inclusion? World Health Organization (2018).
12. Sharan P, Sagar R, Kumar S. Mental health policies in South-East Asia and the public health role of screening instruments for depression. WHO South East Asia J Public Health. (2017) 6:5–11. doi: 10.4103/2224-3151.206165
13. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
14. Koly KN, Baskin C, Lata I, Rao M, Rasheed S, Law G, et al. Educational and training interventions aimed at healthcare workers in the detection and management of people with mental health conditions in South and Southeast Asia: systematic review protocol. BMJ Open. (2021) 11:e045615. doi: 10.1136/bmjopen-2020-045615
15. World Health Organization WH. The World Health Report 2006: Working Together for Health. World Health Organization (2006).
16. World Health Organization. The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. Wkly Epidemiol Rec. (1992) 67:227.
17. Almeida MSC, Sousa Filho LF, Rabello PM, Santiago BM. International classification of diseases−11th revision: from design to implementation. Rev Saúde Públic. (2020) 54:104. doi: 10.11606/s1518-8787.2020054002120
18. American Psychiatric Association. DSM-IV: Diagnostic and Statistical Manual of Mental Disorders. American Psychiatric Association (1980).
19. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). American Psychiatric Association (2013).
20. Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. (2014) 348:g1687. doi: 10.1136/bmj.g1687
21. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The cochrane collaboration's tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
22. Jüni P, Loke Y, Pigott T, Ramsay C, Regidor D, Rothstein H, et al. Risk of bias in non-randomized studies of interventions (ROBINS-I): detailed guidance. Br Med J. (2016).
23. Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed Methods Appraisal Tool (MMAT), Version 2018 (2018).
24. Tirmizi SN, Khoja S, Patten S, Yousafzai AW, Scott RE, Durrani H, et al. Mobile-based blended learning for capacity building of health providers in rural Afghanistan. Mhealth. (2017) 3:14. doi: 10.21037/mhealth.2017.04.01
25. Tarannum S, Elshazly M, Harlass S, Ventevogel P. Integrating mental health into primary health care in Rohingya refugee settings in Bangladesh: experiences of UNHCR. Intervention. (2019) 17:130–9. doi: 10.4103/INTV.INTV_34_19
26. Malla A, Margoob M, Iyer S, Majid A, Lal S, Joober R, et al. Testing the effectiveness of implementing a model of mental healthcare involving trained lay health workers in treating major mental disorders among youth in a conflict-ridden, low-middle income environment: part II results. Can J Psychiatry. (2019) 64:630–7. doi: 10.1177/0706743719839314
27. James JW, Sivakumar T, Kumar CN, Thirthalli J. Change in attitude of ASHAs towards persons with mental illnesses following participation in community based rehabilitation project. Asian J Psychiatry. (2019) 46:51–3. doi: 10.1016/j.ajp.2019.09.031
28. Maulik PK, Devarapalli S, Kallakuri S, Bhattacharya A, Peiris D, Patel A. The systematic medical appraisal referral and treatment mental health project: Quasi-experimental study to evaluate a technology-enabled mental health services delivery model implemented in rural India. J Med Internet Res. (2020) 22:e15553. doi: 10.2196/15553
29. Muke SS, Shrivastava RD, Mitchell L, Khan A, Murhar V, Tugnawat D, et al. Acceptability and feasibility of digital technology for training community health workers to deliver brief psychological treatment for depression in rural India. Asian J Psychiatry. (2019) 45:99–106. doi: 10.1016/j.ajp.2019.09.006
30. Mehrotra K, Chand P, Bandawar M, Sagi MR, Kaur S, Aurobind G, et al. Effectiveness of NIMHANS ECHO blended tele-mentoring model on integrated mental health and addiction for counsellors in rural and underserved districts of Chhattisgarh, India. Asian J Psychiatry. (2018) 36:123–7. doi: 10.1016/j.ajp.2018.07.010
31. Michael A, Thirumoorthy A, Girish N, Sivakumar P. Training community health workers in geriatric mental health: process of manual development and pilot testing findings. Asian J Psychiatry. (2018) 38:12–5. doi: 10.1016/j.ajp.2018.10.017
32. Maulik PK, Tewari A, Devarapalli S, Kallakuri S, Patel A. The systematic medical appraisal, referral and treatment (SMART) mental health project: development and testing of electronic decision support system and formative research to understand perceptions about mental health in rural India. PLoS ONE. (2016) 11:e0164404. doi: 10.1371/journal.pone.0164404
33. Shidhaye R, Shrivastava S, Murhar V, Samudre S, Ahuja S, Ramaswamy R, et al. Development and piloting of a plan for integrating mental health in primary care in Sehore district, Madhya Pradesh, India. Br J Psychiatry. (2016) 208:s13–20. doi: 10.1192/bjp.bp.114.153700
34. Nimgaonkar AU, Menon SD. A task shifting mental health program for an impoverished rural Indian community. Asian J Psychiatry. (2015) 16:41–7. doi: 10.1016/j.ajp.2015.05.044
35. Paudel S, Gilles N, Hahn S, Hexom B, Premkumar R, Arole S, et al. Impact of mental health training on village health workers regarding clinical depression in rural India. Community Ment Health J. (2014) 50:480–6. doi: 10.1007/s10597-013-9630-6
36. Beck A, Virudhagirinathan B, Santosham S, Begum FJ. Developing cognitive behaviour therapy training in India: using the kolb learning cycle to address challenges in applying transcultural models of mental health and mental health training. Int Rev Psychiatry. (2014) 26:572–8. doi: 10.3109/09540261.2014.918024
37. Jincy J, Linu S, Binil V. Effectiveness of an informational booklet on care of attempted suicide patients. Int J Nurs Educ. (2011) 3(1):71–73.
38. Patel V, Weiss HA, Chowdhary N, Naik S, Pednekar S, Chatterjee S, et al. Lay health worker led intervention for depressive and anxiety disorders in India: impact on clinical and disability outcomes over 12 months. Br J Psychiatry. (2011) 199:459–66. doi: 10.1192/bjp.bp.111.092155
39. Thara R, Rao K, John S. An assessment of post-tsunami psychosocial training programmes in Tamilnadu, India. Int J Soc Psychiatry. (2008) 54:197–205. doi: 10.1177/0020764008090421
40. Shaji K, Arun Kishore N, Lal KP, Prince M. Revealing a hidden problem. An evaluation of a community dementia case-finding program from the Indian 10/66 dementia research network. Int J Geriatr Psychiatry. (2002) 17:222–5. doi: 10.1002/gps.553
41. Citraningtyas T, Wiwie M, Amir N, Diatri H, Wiguna T. Capacity building for child and adolescent mental health in disaster areas: Learning from the experiences of mental health care workers in Indonesia. Australas J Disaster Trauma Stud. (2017) 21:57–64.
42. Aldridge LR, Garman EC, Luitel NP, Jordans MJ. Impact of a district mental health care plan on suicidality among patients with depression and alcohol use disorder in Nepal. PLoS ONE. (2020) 15:e0231158. doi: 10.1371/journal.pone.0231158
43. Gupta PP, Jyotsana P, Larrison C, Rodrigues S, Lam C, Dowrick C. Effectiveness of mental health community training on depression and anxiety to the health care profession working in rural centers of eastern Nepal. J Fam Med Prim Care. (2020) 9:2416–9. doi: 10.4103/jfmpc.jfmpc_6_20
44. Jordans MJ, Luitel NP, Lund C, Kohrt BA. Evaluation of proactive community case detection to increase help seeking for mental health care: a pragmatic randomized controlled trial. Psychiatr Serv. (2020) 71:810–5. doi: 10.1176/appi.ps.201900377
45. Kohrt BA, Turner EL, Rai S, Bhardwaj A, Sikkema KJ, Adelekun A, et al. Reducing mental illness stigma in healthcare settings: proof of concept for a social contact intervention to address what matters most for primary care providers. Soc Sci Med. (2020) 250:112852. doi: 10.1016/j.socscimed.2020.112852
46. Luitel NP, Breuer E, Adhikari A, Kohrt BA, Lund C, Komproe IH, et al. Process evaluation of a district mental healthcare plan in Nepal: a mixed-methods case study. BJPsych open. (2020) 6:1–7. doi: 10.1192/bjo.2020.60
47. Sangraula M, Turner E, Luitel N, van‘t Hof E, Shrestha P, Ghimire R, et al. Feasibility of group problem management plus (PM+) to improve mental health and functioning of adults in earthquake-affected communities in Nepal. Epidemiol Psychiatr Sci. (2020) 29:e130. doi: 10.1017/S2045796020000414
48. Markkula N, Lehti V, Adhikari P, Peña S, Heliste J, Mikkonen E, et al. Effectiveness of non-medical health worker-led counselling on psychological distress: a randomized controlled trial in rural Nepal. Glob Ment Health. (2019) 6:e15. doi: 10.1017/gmh.2019.15
49. Kohrt BA, Mutamba BB, Luitel NP, Gwaikolo W, Onyango Mangen P, Nakku J, et al. How competent are non-specialists trained to integrate mental health services in primary care? Global health perspectives from Uganda, Liberia, and Nepal. Int Rev Psychiatry. (2018) 30:182–98. doi: 10.1080/09540261.2019.1566116
50. Acharya B, Tenpa J, Basnet M, Hirachan S, Rimal P, Choudhury N, et al. Developing a scalable training model in global mental health: pilot study of a video-assisted training program for generalist clinicians in rural Nepal. Glob Ment Health. (2017) 4:e8. doi: 10.1017/gmh.2017.4
51. Jordans MJ, Kohrt BA, Luitel NP, Lund C, Komproe IH. Proactive community case-finding to facilitate treatment seeking for mental disorders, Nepal. Bull World Health Organ. (2017) 95:531–6. doi: 10.2471/BLT.16.189282
52. Rahman A, Malik A, Sikander S, Roberts C, Creed F. Cognitive behaviour therapy-based intervention by community health workers for mothers with depression and their infants in rural Pakistan: a cluster-randomised controlled trial. Lancet. (2008) 372:902–9. doi: 10.1016/S0140-6736(08)61400-2
53. Humayun A, Haq I, Khan F, Azad N, Khan M, Weissbecker I. Implementing mhGAP training to strengthen existing services for an internally displaced population in Pakistan. Glob Ment Health. (2017) 4:e6. doi: 10.1017/gmh.2017.1
54. Zafar S, Sikander S, Haq Z, Hill Z, Lingam R, Skordis-Worrall J, et al. Integrating maternal psychosocial well-being into a child-development intervention: the five-pillars approach. Ann N Y Acad Sci. (2014) 1308:107–17. doi: 10.1111/nyas.12339
55. Taj R, Khan AM, Jenkins R. Integrating mental health into primary care in remote rural areas of Pakistan. Asian J Psychiatry. (2011) 4:66.
56. Siriwardhana C, Adikari A, Jayaweera K, Abeyrathna B, Sumathipala A. Integrating mental health into primary care for post-conflict populations: a pilot study. Int J Ment Health Syst. (2016) 10:12. doi: 10.1186/s13033-016-0046-x
57. Blignault I, Manicavasagar V, Parker G, Wijeratne C, Sumathipala A. Building capacity in identification and management of mood disorders: an Australia–Sri Lanka collaboration. Australas Psychiatry. (2012) 20:53–6. doi: 10.1177/1039856211432481
58. Jenkins R, Mendis J, Cooray S, Cooray M. Integration of mental health into primary care in Sri Lanka. Ment Health Fam Med. (2012) 9:15.
59. Lakshminarayanan M, Kathuria N, Mehra S. Delivery of perinatal mental health services by training lay counselors using digital platforms. Asian J Psychiatry. (2020) 54:102277. doi: 10.1016/j.ajp.2020.102277
60. Jayaram G, Goud R, Chandran S, Pradeep J. MAANASI-A Sustained, Innovative, Integrated Mental Healthcare Model in South India. Disabil CBR Incl Dev. (2019) 30:104–13. doi: 10.5463/dcid.v30i2.851
61. Malhotra S, Chakrabarti S, Shah R. A model for digital mental healthcare: Its usefulness and potential for service delivery in low-and middle-income countries. Indian J Psychiatry. (2019) 61:27.
62. Varghese NC, Macaden L, Premkumar B, Mathews P, Kumar S. Delirium in older people in hospital: an education programme. Brit J Nurs. (2014) 23:704–9. doi: 10.12968/bjon.2014.23.13.704
63. Chowdhury AN, Brahma A, Banerjee S, Biswas MK. Community mental health service by IRMC model involving Multi-Purpose Health Workers in Sundarban, India. Int Med J. (2006) 13:185–90.
64. Chowdhury AN, Brahma A, Banerjee S. How to Operationalise Community Mental Health Service at the Primary Care? : Experience of IRMC Model from Sundarban, India. Int Med J. (2004) 11:105–10.
65. Mahmuda M, Miah MA, Elshazly M, Khan S, Tay AK, Ventevogel P. Contextual adaptation and piloting of Group Integrative Adapt Therapy (IAT-G) amongst Rohingya refugees living in Bangladesh. Intervention. (2019) 17:149. doi: 10.4103/INTV.INTV_48_19
66. Jordan K. A case study: How a disaster mental health volunteer provided spiritually, culturally, and historically sensitive trauma training to teacher-counselors and other mental health professionals in Sri Lanka, 4 weeks after the tsunami. Br Treat Crisis Intervent. (2006) 6:316. doi: 10.1093/brief-treatment/mhl012
67. Maulik PK, Kallakuri S, Devarapalli S, Vadlamani VK, Jha V, Patel A. Increasing use of mental health services in remote areas using mobile technology: a pre–post evaluation of the SMART mental health project in rural India. J Glob Health. (2017) 7:010408. doi: 10.7189/jogh.07.010408
68. Gupta A, Aman H. an evaluation of training in brief cognitive–behavioural therapy in a non-english-speaking region: experience from India. Int Psychiatry. (2012) 9:69–71. doi: 10.1017/S174936760000326X
69. Armstrong G, Kermode M, Raja S, Suja S, Chandra P, Jorm AF. A mental health training program for community health workers in India: impact on knowledge and attitudes. Int J Ment Health Syst. (2011) 5:17. doi: 10.1186/1752-4458-5-17
70. Anjara SG, Bonetto C, Ganguli P, Setiyawati D, Mahendradhata Y, Yoga BH, et al. Can general practitioners manage mental disorders in primary care? A partially randomised, pragmatic, cluster trial. PLoS ONE. (2019) 14:e0224724. doi: 10.1371/journal.pone.0224724
71. Rahman A, Akhtar P, Hamdani SU, Atif N, Nazir H, Uddin I, et al. Using technology to scale-up training and supervision of community health workers in the psychosocial management of perinatal depression: a non-inferiority, randomized controlled trial. Glob Ment Health. (2019) 6:e8. doi: 10.1017/gmh.2019.7
73. Chibanda D, Mesu P, Kajawu L, Cowan F, Araya R, Abas MA. Problem-solving therapy for depression and common mental disorders in Zimbabwe: piloting a task-shifting primary mental health care intervention in a population with a high prevalence of people living with HIV. BMC Public Health. (2011) 11:828. doi: 10.1186/1471-2458-11-828
74. Mendenhall E, De Silva MJ, Hanlon C, Petersen I, Shidhaye R, Jordans M, et al. Acceptability and feasibility of using non-specialist health workers to deliver mental health care: stakeholder perceptions from the PRIME district sites in Ethiopia, India, Nepal, South Africa, and Uganda. Soc Sci Med. (2014) 118:33–42. doi: 10.1016/j.socscimed.2014.07.057
75. Murray LK, Dorsey S, Bolton P, Jordans MJ, Rahman A, Bass J, et al. Building capacity in mental health interventions in low resource countries: an apprenticeship model for training local providers. Int J Ment Health Syst. (2011) 5:30. doi: 10.1186/1752-4458-5-30
76. Scott EM, Hermens DF, Glozier N, Naismith SL, Guastella AJ, Hickie IB. Targeted primary care-based mental health services for young Australians. Med J Austra. (2012) 196:136–40. doi: 10.5694/mja11.10481
77. Lu J, Jamani S, Benjamen J, Agbata E, Magwood O, Pottie K. Global mental health and services for migrants in primary care settings in high-income countries: a scoping review. Int J Environ Res Public Health. (2020) 17:8627. doi: 10.3390/ijerph17228627
78. Chokshi M, Patil B, Khanna R, Neogi SB, Sharma J, Paul V, et al. Health systems in India. J Perinatol. (2016) 36:S9–12. doi: 10.1038/jp.2016.184
79. Din MAU, Vardag ABS, Anwer F. Thromboprophylaxis–A neglected front in hospitalised patients with COVID-19 in Pakistan. Euro Oncol Haematol. (2020) 16:14–5. doi: 10.17925/EOH.2020.16.1.14
80. Mercer A, Khan MH, Daulatuzzaman M, Reid J. Effectiveness of an NGO primary health care programme in rural Bangladesh: evidence from the management information system. Health Policy Plan. (2004) 19:187–98. doi: 10.1093/heapol/czh024
81. Perry H, Crigler L. Developing and strengthening community health worker programs at scale. In: A Reference Guide and Case Studies for Program Managers and Policymakers. MCHIP, USAID Jhpiego Corporation (2013).
83. Goncalves DA, Fortes S, Campos M, Ballester D, Portugal FB, Tófoli LF, et al. Evaluation of a mental health training intervention for multidisciplinary teams in primary care in Brazil: a pre-and posttest study. Gen Hosp Psychiatry. (2013) 35:304–8. doi: 10.1016/j.genhosppsych.2013.01.003
84. Mutiso V, Pike K, Musyimi C, Rebello T, Tele A, Gitonga I, et al. Changing patterns of mental health knowledge in rural Kenya after intervention using the WHO mhGAP-intervention guide. Psychol Med. (2019) 49:2227–36. doi: 10.1017/S0033291718003112
85. Are A, Olisah V, Bella-Awusah T, Ani C. Controlled clinical trial of teacher-delivered cognitive behavioural therapy (CBT) for adolescents with clinically diagnosed depressive disorder in Nigeria. Int J Ment Health. (2021) 22:1–20. doi: 10.1080/00207411.2021.1891361
86. Sibeko G, Milligan PD, Roelofse M, Molefe L, Jonker D, Ipser J, et al. Piloting a mental health training programme for community health workers in South Africa: an exploration of changes in knowledge, confidence and attitudes. BMC psychiatry. (2018) 18:191. doi: 10.1186/s12888-018-1772-1
87. Dodd R, Palagyi A, Jan S, Abdel-All M, Nambiar D, Madhira P, et al. Organisation of primary health care systems in low-and middle-income countries: review of evidence on what works and why in the Asia-Pacific region. BMJ Glob Health. (2019) 4 (Suppl. 8):e001487. doi: 10.1136/bmjgh-2019-001487
88. Abayneh S, Lempp H, Alem A, Alemayehu D, Eshetu T, Lund C, et al. Service user involvement in mental health system strengthening in a rural African setting: qualitative study. BMC Psychiatry. (2017) 17:187. doi: 10.1186/s12888-017-1352-9
89. Keynejad R, Spagnolo J, Thornicroft G. WHO mental health gap action programme (mhGAP) intervention guide: updated systematic review on evidence and impact. Evid Based Ment Health. (2021) 24:124–30. doi: 10.1136/ebmental-2021-300254
90. Heim E, Kohrt BA. Cultural adaptation of scalable psychological interventions. Clin Psychol Europe. (2019) 1:e37679. doi: 10.32872/cpe.v1i4.37679
91. Metzger I, Cooper SM, Zarrett N, Flory K. Culturally sensitive risk behavior prevention programs for African American adolescents: a systematic analysis. Clin Child Fam Psychol Rev. (2013) 16:187–212. doi: 10.1007/s10567-013-0133-3
92. Rosen MA, DiazGranados D, Dietz AS, Benishek LE, Thompson D, Pronovost PJ, et al. Teamwork in healthcare: key discoveries enabling safer, high-quality care. Am Psychol. (2018) 73:433–50. doi: 10.1037/amp0000298
93. Saint-Pierre C, Herskovic V, Sepúlveda M. Multidisciplinary collaboration in primary care: a systematic review. Fam Pract. (2018) 35:132–41. doi: 10.1093/fampra/cmx085
94. Woodham NS, Taneepanichskul S, Somrongthong R, Kitsanapun A, Sompakdee B. Effectiveness of a multidisciplinary approach intervention to improve blood pressure control among elderly hypertensive patients in rural Thailand: a quasi-experimental study. J Multidiscipl Healthc. (2020) 13:571–80. doi: 10.2147/JMDH.S254286
95. Wicklein RC, Schell JW. Case studies of multidisciplinary approaches to integrating mathematics, science, & technology education. J Technol Educ. (1995) 6(2). doi: 10.21061/jte.v6i2.a.5
96. Banna S. Face-to-Face Training is Still the Better Choice Over Digital Lessons. Association for Talent Development (2014).
98. Kurt S, Kirkpatrick J. Evaluating training programs: The four levels. Berrett-Koehler Publishers (2006).
Keywords: health system, mental health, education and training, capacity building, healthcare workers, interventions
Citation: Koly KN, Baskin C, Khanam I, Rao M, Rasheed S, Law GR, Sarker F and Gnani S (2021) Educational and Training Interventions Aimed at Healthcare Workers in the Detection and Management of People With Mental Health Conditions in South and South-East Asia: A Systematic Review. Front. Psychiatry 12:741328. doi: 10.3389/fpsyt.2021.741328
Received: 14 July 2021; Accepted: 07 September 2021;
Published: 11 October 2021.
Edited by:
Daniel Bressington, Charles Darwin University, AustraliaReviewed by:
Kuda Muyambi, University of South Australia, AustraliaCopyright © 2021 Koly, Baskin, Khanam, Rao, Rasheed, Law, Sarker and Gnani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kamrun Nahar Koly, a29seUBpY2RkcmIub3Jn; YWt1bXJ1bkB5YWhvby5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.