 José M. Mestre1*
José M. Mestre1* Svenja Taubner2*†
Svenja Taubner2*† Catarina Pinheiro Mota3†
Catarina Pinheiro Mota3† Margarida Rangel Henriques4,5†
Margarida Rangel Henriques4,5† Andrea Saliba6†
Andrea Saliba6† Erkki Heinonen7,8†Sara Ramos1
Erkki Heinonen7,8†Sara Ramos1 Patricia Moreno-Peral9
Patricia Moreno-Peral9 Jana Volkert2,10Asta Adler11
Jana Volkert2,10Asta Adler11 Rasa Barkauskiene11
Rasa Barkauskiene11 Sonia Conejo-Cerón9
Sonia Conejo-Cerón9 Dina Di Giacomo12
Dina Di Giacomo12 Yianna Ioannou13
Yianna Ioannou13 Filipa Mucha Vieira4,5
Filipa Mucha Vieira4,5 Jan Ivar Røssberg14
Jan Ivar Røssberg14 Célia M. D. Sales4,5
Célia M. D. Sales4,5 Stefanie J. Schmidt15
Stefanie J. Schmidt15 Tjasa Stepisnik Perdih16
Tjasa Stepisnik Perdih16 Randi Ulberg14,17
Randi Ulberg14,17 Sonja Protić18*†
Sonja Protić18*†- 1Instituto para el Desarrollo Social y Sostenible (INDESS), Universidad de Cádiz, Cadiz, Spain
- 2Institute for Psychosocial Prevention, University of Heidelberg, Heidelberg, Germany
- 3Department of Education and Psychology, University of Trás-os-Montes and Alto Douro, Vila Real, Portugal
- 4Center for Psychology at University of Porto, Porto, Portugal
- 5Faculty of Psychology and Education Science, University of Porto, Porto, Portugal
- 6Department of Psychiatry, University of Malta and Mental Health Services Malta, Valletta, Malta
- 7National Institute for Health and Welfare, Helsinki, Finland
- 8Department of Psychology, University of Oslo, Oslo, Norway
- 9Instituto de Investigación Biomédica de Málaga, Maálaga, Spain
- 10Department of Psychology, MSB Medical School Berlin, Berlin, Germany
- 11Institute of Psychology, Vilnius University, Vilnius, Lithuania
- 12Department of Life, Health and Environmental Sciences, University of L'Aquila, L'Aquila, Italy
- 13Department of Social Sciences, University of Nicosia, Nicosia, Cyprus
- 14Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway
- 15Department of Clinical Psychology and Psychotherapy, University of Bern, Bern, Switzerland
- 16School of Advanced Social Studies, Nova Gorica, Slovenia
- 17Department of Psychiatry, Diakonhjemmet Hospital, Oslo, Norway
- 18Institute of Criminological and Sociological Research, Belgrade, Serbia
Background: Externalising behaviours are becoming a remarkably prevalent problem during adolescence, often precipitating both externalising and internalising disorders in later adulthood. Psychological treatments aim to increase the social functioning of adolescents in order for them to live a more balanced life and prevent these negative trajectories. However, little is known of the intervening variables and mediators involved in these treatments' change mechanisms. We conducted a systematic review, exploring the available evidence on mediators of psychological treatments for externalising behaviours and symptoms amongst adolescents (10 to 19 years old).
Methods: A systematic search was performed on Medline and PsycINFO databases, which identified studies from inception to February 23, 2020. Eligible studies included randomised controlled trials that enrolled adolescents with externalising symptoms and behaviours as, at least, one of the primary outcomes. A group of 20 reviewers from the COST-Action TREATme (CA16102) were divided into 10 pairs. Each pair independently screened studies for inclusion, extracted information from the included studies, and assessed the methodological quality of the included studies and the requirements for mediators, following Kazdin's criteria. Risk of bias of RCTs was assessed by the Mixed Methods Appraisal Tool. Extracted data from the included studies were reported using a narrative synthesis.
Results: Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA), after removing duplicates, 3,660 articles were screened. Disagreements were resolved by consensus. In a second stage, 965 full-text articles were assessed for eligibility. A total of 14 studies fulfilled all inclusion criteria. The majority were related to systemic psychological treatment approaches. Two types of mediators were identified as potentially being involved in the mechanisms of change for better social improvements of adolescents: to increase healthier parent–adolescent relationships and parental discipline. However, there were significant and non-significant results amongst the same mediators, which led to discussing the results tentatively.
Conclusions: Family variables were found to be the largest group of investigated mediators, followed by relational, behavioural, and emotional variables. No cognitive or treatment-specific mediators were identified. Both adequate behavioural control of adolescents' peer behaviour and a better positive balance in their relationships with their parents seemed to buffer the effects of externalising behaviours in adolescents. Several methodological limitations concerning mediation testing design, outcome measures, and mediator selection have been identified.
Ethics and Dissemination: Ethical approval was not required. PROSPERO registration number: CRD42021231835.
Introduction
During childhood and adolescence, externalising, or disruptive behavioural disorders become a significant risk factor for later juvenile delinquency, adult crime, aggressiveness, violence (1), and internalising disorders (2, 3). Both childhood externalising behaviours and juvenile delinquency are currently considered a serious public health concern (4). Consequently, youth violence prevention and intervention are considered one of our society's most pressing issues today (5–7). Identifying essential therapeutic change mechanisms and mediators of outcome in psychological interventions for externalising behaviours problems is of paramount importance as it would help in the treatment and prevention of externalising problems in adolescence and adulthood (8). Previous reviews on psychotherapy with adolescents (10–19 years old) for the treatment of externalising symptomatology have been published to identify potential mediators (6). However, there is still a lack of knowledge of the involved mechanisms of change.
The externalising symptomatology is a category of psychiatric social functioning disturbances (1) that have been categorised as externalising disorders (ED) (9). They can also be present in other specific disorders such as conduct disorder (CD), oppositional defiant disorder (ODD), attention deficit hyperactivity disorder (ADHD) (10), and substance abuse (11). Essentially, almost all ED are characterised by under-controlled (12), impulsive (13), or/and aggressive (14), or rule-breaking behaviours, which have been labelled as externalising behaviours (13) or externalising symptomatology (15).
Traditionally, Achenbach and colleagues introduced the construct of externalising vs. internalising disorders (ID). ED are oriented toward behavioural maladjustment, which affects social functioning. That is, externalising behaviours involve acting negatively on one's external environment. Conversely, ID are oriented toward explaining maladjustment in the child and adolescent's personal functioning (16, 17). However, ED and ID have a substantial overlap, as they share common aetiologies (18). For example, long-term externalising behaviours can lead to internalising symptoms later in life (19, 20) and vice versa (21) and are highly correlated (22). Despite the comorbidity of ED and ID, distinctive pathways have been described for externalising disorders from ODD via CD to anti-social-personality disorder in adulthood (22).
Some authors have pointed out a lack of consensus on including ADHD and drug abuse in the same category as oppositional defiant disorder and conduct disorder (23). ODD and CD are related more to disruptive behaviours, while ADHD is related to inattention, and alcohol abuse to dopaminergic problems of addiction (17). As stated in the DSM-5 (24), ODD co-occurs with ADHD in approximately half of the cases in the general population in children with a combined presentation (inattention and hyperactivity-impulsivity) and roughly a quarter of children and adolescents with a predominantly inattentive presentation. CD occurs in about one-quarter of children and adolescents with a combined display [e.g., ADHD, see (5)], depending on the age and setting (25). The impulsivity trait that typically manifests in children with ADHD confers considerable risk for the manifestation and development of externalising behaviours (26). Therefore, ADHD is highly comorbid with these disorders and predicts externalising behaviours but is not a disorder caused by the same distal (e.g., parenting style) or proximal (e.g., personality traits) causes (5, 27). Besides, from a neurological point of view, ADHD is considered a neurodevelopmental disorder linked with frontal lobe maturity (28) and substance abuse underlies neurobiochemical mechanisms (29). For the purpose of this review, we have decided to focus only on externalising behaviours and we therefore excluded those articles with a primary diagnosis of ADHD when externalising symptoms were not part of the primary outcomes.
Psychological treatments need to be tailored to the specific needs of individuals with ED, as most psychological interventions have been developed for ID and do not sufficiently address ED (6). Moreover, treatment response and motivation to change may be altered in individuals with ED in comparison to ID (22). Thus, there is a call for a deeper understanding of the mechanisms of change in ED treatment that could inform the development of more effective psychological therapies.
Meta-analyses have concluded that psychological treatments have a more substantial positive effect on externalising symptomatology than punishment-oriented or pedagogical interventions (30). Several psychological therapies have been designed for adolescents' externalising behaviours. The most effective programs include the family and/or peer systems such as multi-systemic (family) therapy, parent training, and multidimensional foster care (24, 26). Third-wave treatments have recently been modified for ED, such as dialectic behavioural treatment (31) and mentalisation-based treatment (32). However, different therapies are based on diverse change theories for addressing externalising symptoms and behaviours among adolescents. Hence, we are interested in reviewing therapies that may have different significant mediators related to externalising outcomes.
The following are the most commonly used psychological therapies for externalising symptoms and behaviours:
- Parent Management Training (PMT): Parent management training is based on behavioural and social learning principles (20, 21). PMT addresses problematic parent–child interactions, especially coercive family processes (33). According to Forehand et al. PMT's mechanisms of change focus on parents learning to replace these problematic interactions with more adaptive ones. Hence, parents are trained to improve positive contingencies to increase the child's desirable behaviours. Parents also receive instructions on applying effective parenting to reduce the child's undesirable behaviours (27). PMT has been recognised for its effectiveness in reducing externalising behaviours (34) and symptomology (35, 36).
- Multisystemic Therapy (MST): Von Sydow et al. described multisystemic therapy (MST) as follows: (1) perceives behavioural and mental symptoms within the context of the social systems in which people live; (2) focuses on interpersonal relationships and interactions, social constructions of realities, and causality between symptoms and interactions; (3) involves family members and significant others (e.g., teachers, friends, other professionals) directly or indirectly; and (4) uses clients' views of problems, resources, and preferred solutions (37). Von Sydow et al. (37) systematically reviewed 47 trials on the efficacy of different psychological treatments for ED in childhood and adolescence. They concluded that, primarily, systemic (family) therapy is effective for externalising behaviours and juvenile delinquency. Furthermore, they noted that systemic therapy effectively affects multiple functioning domains (primary and secondary mental health symptoms, family outcomes, problems with the judicial system, and school performance) (38). The family systems emphasise how family therapy perspectives locate the problem in the workings of the system rather than at the level of the individual (27, 33).
- Cognitive Behavioural Therapy: Cognitive behavioural therapy (CBT) interventions for children and adolescents with clinical symptoms of ED can be either youth-focused (mainly) or parent-focused. CBT aims to improve children and adolescents' coping skills in the face of life's challenges (39). CBT interventions have proven to help children learn to recognise and solve problems (40). When CBT was focused on parents, the primary goal was to improve parents' pedagogical skills, such as rule setting, consistent discipline, or positive reinforcement (41). Conversely, for adolescents and young adults, CBT is recommended when difficulties with socio-cognitive skills are identified in young people with antisocial behaviour problems (42–44). Young people with ED tend to have hostile attribution biases, misinterpret social cues, and have higher expectations of positive outcomes through aggression (34).
- Multidimensional Foster Care Treatment (MTFC): MTFC (45) treats ED children and adolescents with their families with low level of support due to high levels of abuse and neglect, severe mental health and behavioural problems, and juvenile delinquency issues (46). MTFC focuses on young people with severe and chronic delinquency problems. MTFC is a behavioural treatment alternative to residential placement for youth who have problems with chronic antisocial behaviour, emotional disturbance, and delinquency (46). This ED intervention establishes fair and consistent boundaries, supervision, predictable consequences for non-compliance, a supportive relationship with at least one adult mentor, and limited exposure and access to delinquent peers (47). Thus, the MTFC's primary goals are to decrease delinquent behaviour and increase participation in developmentally appropriate prosocial activities for these young people (25). Different MTFC programmes have been developed and validated for older children and adolescents involved in the juvenile justice system (46). MTFC is considered an evidence-based intervention. Several randomised clinical trial studies have shown satisfactory outcomes in treating ED symptoms (48).
All these therapies have highlighted the role of parenting styles as a mediating factor between treatments and outcomes compared to control groups to reduce externalising symptoms in adolescents (27, 35, 36). In summary, the different therapies address parenting styles to treat ED in adolescents. On the one hand, parental warmth, behavioural control, autonomy granting, and democratic parenting styles predict lower ED rates. On the other hand, strict control, authoritarian, permissive, and neglectful parenting styles are associated with more severe externalising problems, with stronger associations observed for stringent control and psychological control (49). However, there is a need to clarify how the theories of change and other mediators in therapies are involved in reducing ED in adolescents. Further research is needed to identify whether more pertinent mediators between treatments and outcomes with a comparator group exist. To our knowledge, there are no systematic reviews on general mediators (beyond parenting styles), both treatment-specific (e.g., psychotherapeutic intervention) and non-treatment specific (e.g., adolescents' capacities for affect regulation), which are involved in psychological treatments to reduce ED symptoms among adolescents. Even though the most common therapies originate from different therapeutic approaches, they overlap in addressing family factors, but they tended to neglect other potential mediators.
Rationale
This review aims to provide a systematic and comprehensive narrative synthesis of existing studies on mediators (treatment and non-treatment-specific) in psychotherapy with adolescents (10–19 years old) diagnosed with externalising behaviours (impulsivity, disruptive behaviours, aggression or violence, sexual offending, and delinquent behaviours). We aim to identify possible commonalities rather than differences in mediators and theories of change in the diverse interventions where efficacy was evaluated with at least one control group.
Method
Study Design
This article is based on work from COST Action 16102 European Network on Individualised Psychotherapy Treatment of Young People with Mental Disorders, supported by COST (European Cooperation in Science and Technology). TREATme was established in 2017 and composed of researchers from 30 countries. TREATme's main objective is to identify scientifically sound empirical research on therapeutic efficacy in young people. Several working groups have been set up to identify mechanisms of change, mediators, and moderators on the therapeutic efficacy, among other activities. This study is a result of work on mediators and theories of change in psychotherapy with adolescents with ED.
This systematic review of the literature follows Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (50). The PICO model defined the research question (patient/population, intervention, comparison, and outcomes); “In adolescents treated for externalising disorders (P), what were the mediators of psychological interventions (I) compared to the effect on the outcomes in other interventions or control groups (C) on ED (O) (51).
Eligibility Criteria
All full-text versions of potentially relevant studies were searched from inception on February 23, 2020, and were examined in detail for eligibility at the review team meetings. We considered published studies and grey literature from all geographical locations if written in English. Studies were included or excluded in this systematic review based on the following criteria:
Inclusion Criteria
The inclusion criteria used for the studies were as follows: (1) the study targeted an adolescent sample with a mean age between 10 and 19 years and standard deviation of 3 or lower; (2) the adolescents presented with EDs; (3) the study included a psychosocial intervention and/or psychotherapeutic intervention or treatment for adolescent's ED; (4) the study included a mediating analysis of the change of the intervention; and (5) the study was a randomised controlled trial or controlled study.
Exclusion Criteria
Articles were excluded if (1) the age of the participants was not given or if the age was below or above the target population; (2) the diagnosis of externalising symptoms was not one of the primary diagnosis; (3) a psychosocial, psychological/psychotherapeutic intervention was not included; (4) mediators were not investigated; or (5) the outcome of the study was not clearly defined or insufficient details were provided to determine whether the outcome was directly related to the intervention.
Search Strategies
The current study was conducted following the Cochrane Collaboration guidelines for systematic reviews and meta-analyses. The literature search included MEDLINE and PsycINFO databases. All searches were carried out on the same day (February 23, 2020) to control for daily updates. The entire search string is available on https://www.crd.york.ac.uk/PROSPEROFILES/248959_STRATEGY_20210414.pdf.
Study Selection Processes
Following the PRISMA guidelines (52), the flowchart presented in Figure 1 provides step-by-step details of our study selection process.
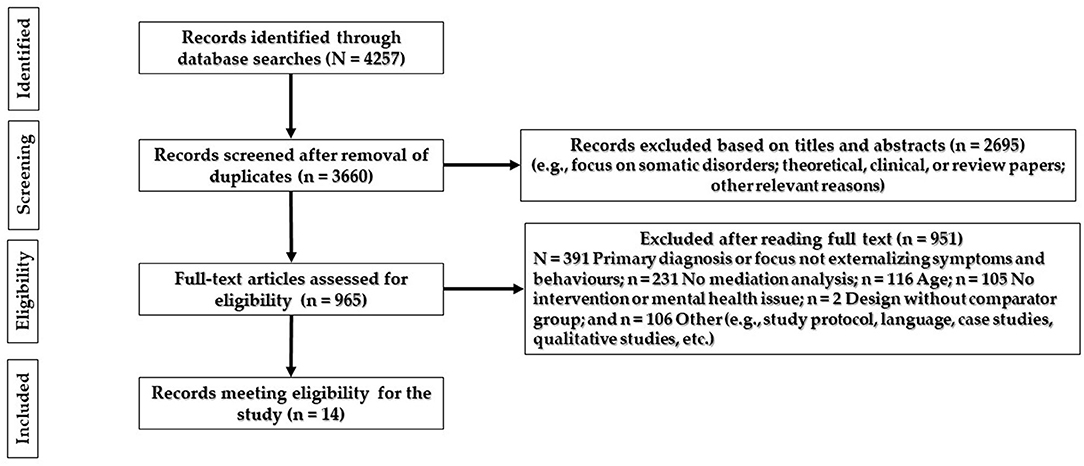
Figure 1. PRISMA flow diagram of the search.
Literature search based on the search strings revealed that 4,257 articles were identified through database searches when the search string was applied. Two experienced researchers carried out an initial sample of articles identified through database search and developed a data file with authors, year, titles, and abstracts. Duplicate studies were eliminated.
Twenty experienced researchers divided into 10 pairs used an excel database of 3,660 articles built for this purpose. In the first stage, the screening was carried out using the titles and the abstracts of the papers. Each member of each pair screened titles and abstracts and excluded studies that clearly did not meet the inclusion criteria. Each pair established consensus about which studies to exclude. A total of 2,695 articles were excluded based on titles and abstracts.
In the second stage of the screening process, the remaining 965 studies were divided among 10 pairs of researchers. Each member of each pair reviewed the full text and discussed disagreements, and when consensus could not be reached, a third reviewer was involved in the decision. The reasons for exclusion were registered. Next, the full-text versions of potentially relevant studies were retrieved and examined in detail for eligibility by part of the COST Action TREATme team. Differences regarding study selection were resolved by discussion in team meetings. In the end, an independent researcher performed a quality cheque by assessing every fifth paper that was excluded in order to assess for reliability between individual rater pairs. A total of 951 were excluded, with 14 original articles in the final review.
Data Extraction Processes
Two independent researchers extracted the data in pairs, and differences were discussed together. The categories for the extraction of data from the selected articles were as follows: specific symptoms, participants (age group, mean age, and standard deviation), setting of the intervention, design of the study, studied interventions, description of the comparator, times of assessment, follow-up(s) period(s), outcomes, results of each mediator in each outcome, and risk of bias.
Strategy for Data Synthesis
We performed a narrative review of the results from the included studies. After reading the results of the studies, we identified the different types of mediators by the 10 pairs of researchers. They came together to compare and discuss the differences in the synthesis. Then, mediators were classified into four categories: family, relational, behavioural, and emotional. A meta-analytical pooling was not feasible because of overlapping mediator constructs and a small number of studies per type mediator.
Risk of Bias and Quality Assessment
The 14 included studies were evaluated according to the quality of the evidence. Since no standard form for evaluating mediation studies has been established, methods of testing mediation effects were assessed according to the general criteria for identifying mediators of psychosocial interventions in research (53, 54). Namely, we considered (1) the sample size and study power, (2) validity and reliability of the measure used to assess the mediator, (3) temporality criteria and multiple assessments of the mediator, (4) comparison of theory-driven with non-specific mediators, and (5) whether there was manipulation of mediator dosages and their influence on the outcome. The Mixed Methods Appraisal Tool (55) was used for the risk of bias and the methodological quality assessment of randomised controlled trials.
Results
Study Characteristics
The PRISMA flow chart outlines the process of exclusion (see Figure 1) with the 14 studies, which met the eligibility criteria and were included in this systematic review.
A total of 12 of 14 experimental studies (56–67) examined samples with externalising behaviours as the primary diagnoses. In addition, there was one prevention study amongst 6th to 8th grade students (68) and one study that did not have a formal externalising diagnosis that was also related to a prevention study (69). Within these two studies (68, 69), externalising behaviours or symptoms were at least one of the primary outcomes.
Table 1 provides a detailed overview of extracted data and study characteristics. All articles came from Western-culture countries: 10 from the USA, 2 from the Netherlands, 1 from Canada, and the last 1 from Australia. American selected papers reported samples with high Hispanic adolescents (k > 60%); however, the rest of the studies did not report the ethnicity of the participants.
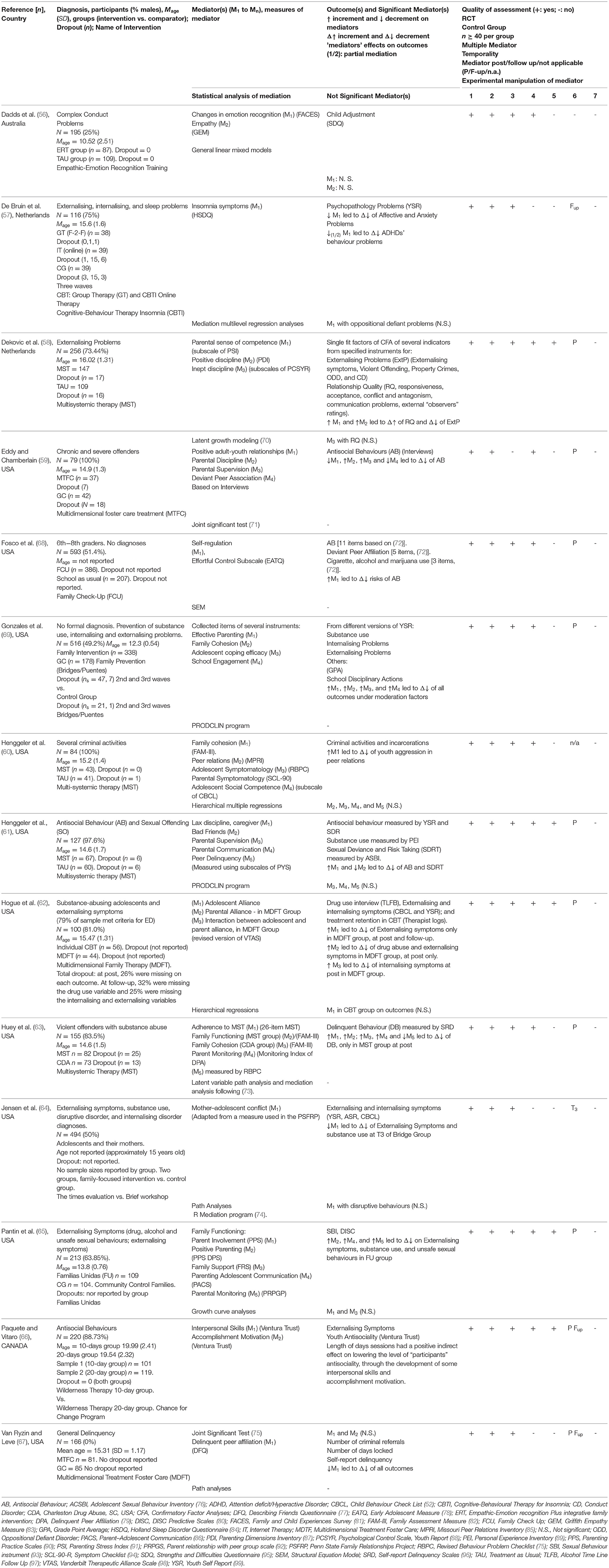
Table 1. Study characteristics.
With regards to gender, the majority of the studies reported males mainly, with an average percentage of 74.05% male individuals (ranged from 51.4 to 100%); except one with 100% of female participants (67), another with 25% of males (56), and another one (64) with a balanced gender distribution (50%); however, these studies were preventive interventions on externalising symptoms.
The average age of all participants was 14.85 years (SD = 1.39, and ranged from 6 to 30 years old). However, two studies did not accurately report the mean age of participants by group or total; they only reported the school grades that indicated an adolescent sample.
Table 2 reports the name of intervention, format, mode of delivery, and setting of the selected studies.
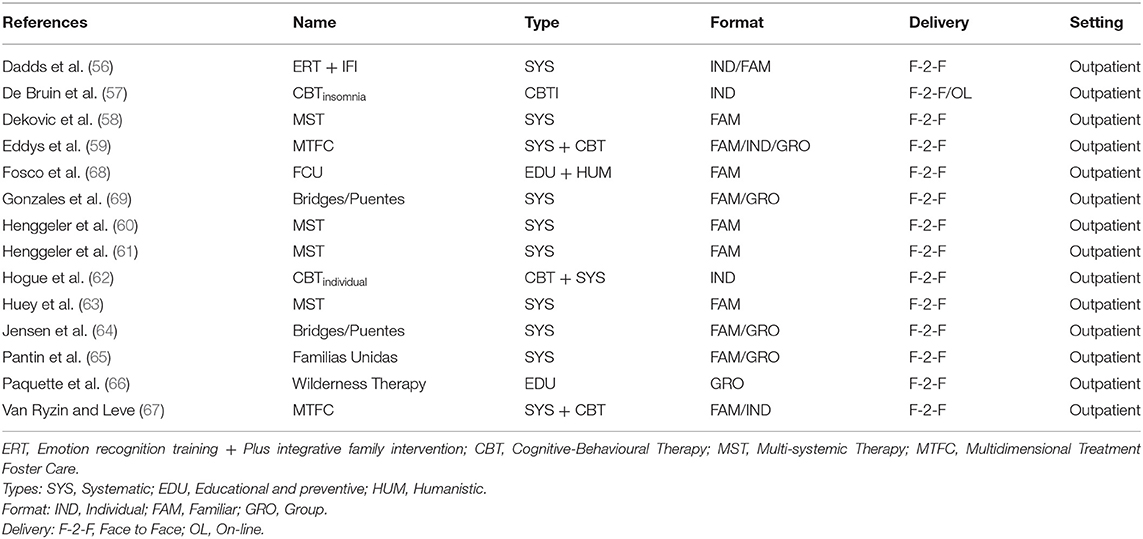
Table 2. Characteristics of the interventions in the selected articles.
Most psychological interventions were based on systemic approaches (k = 11), although three of them were blended with CBT (two with MTFC). Only one study was based on CBT only. Two studies used a psychoeducational approach, one in combination with a humanistic method. No other therapeutic modalities (e.g., psychodynamic or third wave therapies) were found to assess the change mechanisms and mediators matching our inclusion criteria.
With regards to the setting of the interventions, five of them included family members exclusively (58, 60, 61, 63, 68). Five others combined family and individual sessions (k = 5), two used individual sessions only (56, 66), two consisted of sessions in-group formats (64, 69), and one made use of all settings [group, individual, and family (59)]. Except for just one with an online group setting (56), the rest of the interventions were face-to-face. All studies were carried out with an outpatient population.
To assess ED, Achenbach and colleagues' YSR was used (57, 61, 66, 69) or CBCL (62) in most studies. However, different methods were used to determine externalising symptoms or behaviours, especially using items from other tools after implementing reliable confirmatory analyses (58, 68, 69). Most of the studies relied on ED outcomes using self-report measures. In contrast, some studies used interviews with parent and adolescents (59, 62) or derived ED directly from reports on delinquent activities and referrals (60, 67). There was a strong tendency to use confirmatory factor analyses to create a critical measure of ED through different items from different instruments, besides criminal or justice referrals (58, 61, 66, 68, 69).
The statistical analyses of mediation have changed in empirical research over time and thus varied in the reviewed studies. Most mediation analyses were based on different types of regressions analyses (57, 59, 61, 62, 66), two of them using the Baron and Kenny (71), and five studies included structural equations or path analyses to test mediational effects (61, 63, 64, 67, 68).
When it comes to Kazdin's criteria on quality of assessing mediation (see Table 1), only five studies met the temporality criteria, while none included the experimental manipulation of mediator. Although 11 out of 14 studies assessed multiple mediators, the vast majority of them compared mediators of the same kind (i.e., family or emotional mediators only).
Risk of Bias and Quality Assessment for Process Research
Table 3 reports the risk of bias and quality assessments of the 14 included RCT studies. Although quasi-experimental studies were included as including criterion, no one was finally selected. All of them positively established research questions and collected the data according to the research questions. Nonetheless, regarding the performance of the randomisation sample, two studies had an unclear performance of the randomisation (62, 68), while the rest were appropriately randomised. All the comparator groups were assessed at baseline except one, which was unclear (68). More difficulties were found regarding the accomplishment of outcome assessors being blinded to the intervention provided: unclear (58, 64, 65, 67) and just one not accomplished (68). Finally, all studies satisfactorily completed the question regarding the adherence of participants, although two of them were unclear (62, 68).
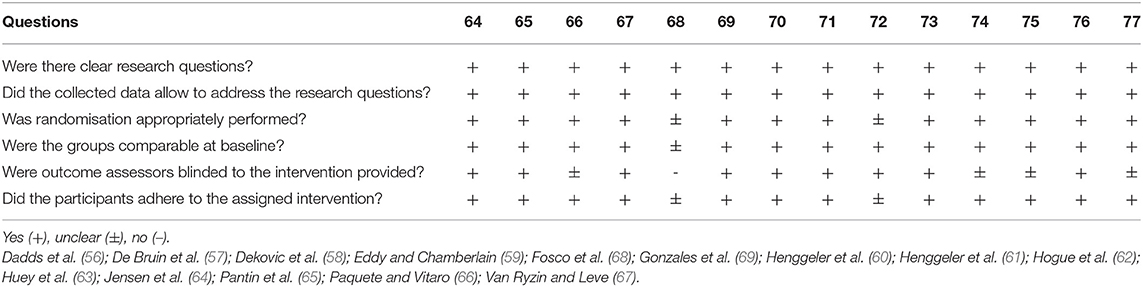
Table 3. Risk of bias and quality assessment for process research.
Mediators
Overall, 37 potential mediators were examined, of which the majority (m = 23; 62.16%) were significant. Intervening factors or mediators with a partial indirect effect on outcomes are represented as “1/2” in Table 1. We found different types of mediators in the studies; however, most of them were related to family process or parenting styles. The letter “m” represents the number of times that a particular mediator has been identified in the different selected studies.
Family Mediators
These types of mediators represented the largest group (m = 22; 61.11%). Both family and parenting mediators were shown to be significant−16 out of 22: Family cohesion (m = 3), parental monitoring (m = 2), positive youth–adult relationships (m = 1), parental discipline (m = 1), parenting sense of competence (m = 1), lax caregiver discipline (m = 1), mother–adolescent conflict (m = 1), positive discipline (m = 1), positive parenting (m = 1), parent alliance (m = 1), effective parenting (m = 1), and parent–adolescent communication (m = 1). The following family-related mediators were reported to be non-significant (all m = 1): parent involvement, inept discipline, family support, parental communication, and parent symptomatology. Results from parental supervision were inconclusive with one study reporting significance whereas the other did not (m = 2).
Relational Mediators
With regards to relational-functioning mediators (m = 8, 21.62%), three of eight mediators were identified as significant: deviant peer association (m = 1), delinquent peer affiliation (m = 2), and bad friends (m = 1). Non-significant relational mediators were interpersonal skills (m = 1), peer relations (m = 1), peer delinquency (m = 1), adolescence social competence (m = 1), and adolescent alliance (m = 1).
Behavioural Mediators
Findings of behavioural mediators (m = 4, 10.81%) that were significant were as follows: school engagement, insomnia symptoms, and self-regulation behaviours. Accomplishment motivation (m = 1) was not significantly related to outcomes.
Emotional Mediators
Three potential mediators (6.46%) related to relational emotion processes have been tested: coping efficacy (m = 1) proved to be significant, while the change in emotion regulation (m = 1) and empathy (m = 1) did not.
No cognitive mediators were investigated in the selected papers of this systematic review. Importantly, all investigated mediators were non-treatment-specific.
Discussion
To our knowledge, this is the first comprehensive systematic review that evaluated mediation studies in various forms of treatment of ED in adolescents. A total of 14 mediation studies with 3,314 participants were included, which investigated 37 different mediators in nine psychological interventions based on four theoretical foundations (systemic, CBT, educational, and humanistic).
A positive picture was gained regarding the risk of bias and study quality assessment. Although only eight studies met all the criteria for RCT, four additional faced only one problem—the absence of assessors' blindness. This result may suggest that the standards for performing RCTs are well-established and satisfyingly applied in the psychotherapy field. However, standards for mediation studies with respect to Kazdin's criteria (100) were low, which might be related to the fact that most studies were not designed as mechanism of change studies but efficacy studies in which mediation analyses were secondary research questions. Two main problems have been identified in the mediation designs: only one-third of studies included temporal precedence of the mediator, while none of studies performed experimental manipulation of mediator. The low quality of mediation testing questions the role of the proposed mediators in the respective mechanisms of change since causality could not be established and this means that changes in the putative mediators are mainly associated with the outcomes change. However, the temporal chain remains unclear (i.e., what changes first, outcome, or mediator).
With regards to outcome measures, the lack of a consensual criterion for assessing externalising behaviours was demonstrated. Namely, several studies (58, 60, 65, 66, 68) used various items from different self-report instruments to statistically develop an adjusted and reliable CFA to represent externalising behaviours. Others used objective, and hypothetically more robust measures of externalising behaviours such as interviews for testing antisocial behaviours (59, 62), criminal activities and incarcerations (60), and the number of criminal referrals and days locked up (67). The rest applied the externalising self-reports that are well-known and widely used in the literature. Thus, there was possible variance due to the evaluation method in outcomes (self-report vs. objective measures) that may have influenced the absence of significant results and would have required different statistical techniques, such as the multimethod–multitrait statistical approaches (53). Besides, some of the results might be compromised by the absence of clear clinical cutoff points in the instruments used for the assessment of externalising behaviours (50), while this was not the case for measuring depression with the Beck scale [see (13)].
The majority of psychological interventions were based on systemic principles (38). Hence, it appeared that systemic (family) psychological approaches were widely used in psychotherapy for treating externalising behaviours among adolescents (38) and are also focusing on establishing change mechanisms. Nonetheless, our systematic review points out that these interventions focused more on family-based treatment than on a theoretical systemic therapy orientation. Three randomised interventions were blended with CBT approaches (59, 62, 76), and eight used systemic theoretical mechanisms only (56, 58, 60, 61, 63–65, 69). They were presented in different formats: family (56, 58–61, 63–65, 67–69), group (59, 64–66, 69), and individual (59, 64–66, 69), and all systemic approaches were delivered face-to-face. Interestingly, no psychodynamic nor third-wave therapies were identified among these studies.
The review's main findings were related to the mediators that have been selected and proven to be significant. Family variables were found to be the largest group of investigated mediators (22 out of 37). The following groups are composed of a range of different relational (8 out of 37), behavioural (4 out of 37), and emotional (3 out of 37) mediators. No cognitive mediators were investigated. The lack of testing multiple mediators from different categories (e.g., family-related with emotional) was noted (see Table 1). Furthermore, none of the significant or non-significant mediators were treatment-specific and results in all these mediator categories showed both significant and non-significant results. We expect that some results are possibly coincidences (false-positive and false-negative) due to insufficient powering and not following Kazdin's recommendations.
With regards to the type of mediators, findings indicated that treatment approaches were mostly interested in evaluating mediators related to changes in the family system. Hence, family mediators were the largest group. Thus, they were closely related to the systemic therapeutic orientation and its findings (38). The commonalities observed with mediators showed how interventions improved family-based relationships (family cohesion, positive youth-adult relationships, lax caregiver discipline, mother-adolescent conflict, positive parenting, and parent-adolescent communication) and/or how-to-implement positive parenting (parental monitoring, parental discipline, parenting sense of competence, positive discipline, and effective parenting). These mediators were related to the presumed systemic mechanisms of change, which ranged from ineffective or negative parental styles to positive or more effective ones (58, 59, 62, 63, 65). Besides, studies also based on CBT approaches (59, 62, 67) included mechanisms of parental monitoring aimed at two primary purposes: to control/decrease risky peer relations (59–61, 63, 67) or/and to improve parental discipline (58, 59, 62, 64, 65). Both aim to help adolescents consider the consequences of their choices (especially with delinquent peers) before making decisions (1, 36, 57, 61, 88, 89, 95). These were followed by allowing adolescents to bear the consequences of poor decisions without bailing them out (5, 41, 60, 101, 102). Three studies (59, 61, 68) included family cohesion measures, i.e., strength of the emotional bonds between family members' mutual support under distressed environments and situations (103). Three studies demonstrated that increasing family cohesion might decrease ED (60, 63, 69). Therefore, it can be summarised that psychological ED treatments for adolescents often focused on these two mechanisms of change, i.e., increasing family relationships and improving effectiveness of parenting. Indeed, the majority of family-related mediators turned out to be significant in both domains of parenting and parent–adolescent relationship (16 out of 22). This points toward a putative change mechanism in the treatment of ED independent of the treatment approach.
Furthermore, our systematic review identified studies with relational mediators as the second largest group of mediators; however, only three out of eight proved to have significant effects. Significant relational mediators were related to the negative influence from peers adolescents with ED keep: deviant peer association, delinquent peer affiliation, and bad friends. Maintaining such relationships increases the likelihood of disruptive, delinquent or aggressive behaviour in adolescents with externalising symptoms (63, 67, 79). However, two studies investigating the influence of delinquent peers did not find a mediation effect on outcome. Furthermore, two studies reported on non-significant influences of social competences and also the therapeutic alliance.
Concerning behavioural mediators, two educational studies, which were oriented to decrease antisocial behaviours, were also reviewed (66, 68). One of them was a preventive study without a significant mediator (self-regulation) (68), and another had non-significant effects on lowering the level of participants' antisocial behaviour through the development of interpersonal skills and accomplishment motivation (66). Another rather unexpected significant mediator was reducing insomnia symptoms (CBT, individual and online settings), leading to lower internalising and externalising symptomatology (56).
Our review demonstrated a striking lack of studies on emotional mediators in research on treating externalising symptoms (100) as only three studies included mediators relating to emotional changes. Changes in empathy and emotion regulation turned out to be not significant in two studies, although increasing adolescents' emotional abilities is assumed to be a plausible mechanism that has been observed to improve the social (101, 104) and personality functioning (102, 103) of adolescents. The lack of emotional mediators as well as the absence of cognitive mediators may be a reflection of reductionist change theories in externalising disorders or the lack of effective treatments aside from family therapy that target at the system level more than on the adolescent him/herself.
There are some limitations to be considered when it comes to the methodology and findings of this systematic review. Firstly, we used general research terms and did not focus on externalising disorders in the systematic search—although it is expected that this kind of strategy would reveal any adolescent population in the psychotherapy process, more specific search terms would find at least, to some extent, different results. Second, the inclusion of only English literature could lead to some studies being excluded and some cultural biases. Thirdly, in order to obtain the most valid and reliable data, we excluded all the non-RCT studies that may limit or narrow the interpretability of available data. Hence, we found mainly US-based studies—and primarily systemic. Moreover, this review discussed the mediators that have been investigated so far, which turned out to be selective and biassed by the therapeutic school that was investigated. Finally, we aimed to give a narrative synthesis of the mediators. Due to their nature and variety, we were not able to conduct a meta-analysis and thus the theories of change specifically tested within the studies and related to specific therapies were not carried out.
Another issue to consider is the overlapping nature of mediators. In some ways, the types of mediators share characteristics. For example, family cohesion has both familial, relational, behavioural, and emotional connotations (104–106).
Conclusions
Due to a lack of methodological quality in mediation designs, as stated above, results should be interpreted tentatively.
After reviewing the existing studies that followed an RCT design, therapy-related biases and restrictions in the mediator selection process were found. Restrictions may also be related to a narrow clinical change theory of ED. As a result, emotional and cognitive mediators were strikingly neglected. Furthermore, some inconsistences regarding the mediators' significance were identified. Namely, several family and relational mediators were significant in some studies and not in others, which prevented us from developing an explanatory pattern with more strength. Therefore, with these caveats in mind, our conclusions are tentative pending further research on psychotherapeutic and mediator efficacy. In principle, it appeared that both adequate behavioural control of adolescents' peer behaviour and a better positive balance in their relationships with their parents seemed to buffer the effects of externalising behaviours in adolescents with ED.
We tried to derive three groups of recommendations for future research based on the open questions that emerged after the synthesis of findings. Firstly, future studies should extend the existing knowledge by investigating other plausible mediators (i.e., including other emotional mediators, cognitive mediators). Also, the statistical comparisons of explanatory power of different mediators and investigation of their (complex) relationship is needed. Furthermore, all psychotherapy schools still face the challenge to explain how they work since no data on treatment-specific mediators has been found. Moreover, some therapeutic schools, like psychodynamic or third-wave therapies, so far have not been engaged in examining potential mediators of their ED treatment. CBT treatments have not been studied with regard to cognitive mediators either. Furthermore, within systemic and family therapy approaches, it would be interesting to explore further mechanisms (for instance adolescent's emotional or cognitive capacities) that are built during the therapy process and that would be effective in preventing ED after the adolescent develops more autonomy and starts to live an independent and separate life from their family. Moreover, it would be important to examine which mediators are significant in adolescents with severe ED (e.g., those in correctional institutions) and whose families are not available or have no contact or influence on the adolescents' behaviour.
The second group of suggestions relates to research practises and is based on studies' methodological limitations that were recognised in this review. Namely, several design issues could be improved in order to have stricter and more rigorous testing of mediation according to established criteria. Also, a greater consensus on how to assess externalising behaviours that represents the common symptoms of the different mental disorders that belong to the ED would enable more reliable and valid conclusions. Looking into gender as a moderator of mediation effects could be another challenging question addressed in the future.
Finally, additional efforts could be made in order to understand the relationship between internalising and externalising symptoms. Similarly, the use of personality functioning as a construct consisting of self and interpersonal domains instead of externalising vs. internalising could be used to avoid stigmatisation during adolescence.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
JM, ST, MRH, CPM, AS, EH, SR, and SP drafted the first and second version of the manuscript. All co-authors provided a substantial contribution to the conception and design of the work by developing the research questions, the search string, and carrying out the stage 1 screening (SC-C, ST, EH, AS, SP, JV, AA, RB, DD, YI, JM, FM, CPM, MRH, JR, SS, TSP, RU, CS, and PM-P). The current manuscript was corrected and finally approved by the other authors (JV, AA, RB, DD, YI, SC-C, PM-P, FM, CPM, MRH, JR, SS, TSP, RU, and CS). RU coordinates the overall COST initiative. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This publication is based upon work from COST Action: CA16102, European Network on Individualised Psychotherapy Treatment of Young People with Mental disorders, supported by COST (European Cooperation in Science and Technology). https://www.cost.eu/actions/CA16102/. The publication fee was paid by Heidelberg University (Germany) and Universidad de Càdiz (Spain).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Liu J. Childhood externalizing behavior: theory and implications. J Child Adolesc Psychiatr Nurs. (2004) 17:93–103. doi: 10.1111/j.1744-6171.2004.tb00003.x
2. Kim-Cohen J, Caspi A, Moffitt TE, Harrington H, Milne BJ, Poulton R. Prior juvenile diagnoses in adults with mental disorder. Arch Gen Psychiatry. (2003) 60:709. doi: 10.1001/archpsyc.60.7.709
3. Fairchild G, Hawes DJ, Frick PJ, Copeland WE, Odgers CL, Franke B, et al. Conduct disorder. Nat Rev Dis Prim. (2019) 5:43. doi: 10.1038/s41572-019-0095-y
4. Sörberg Wallin A, Koupil I, Gustafsson J-E, Zammit S, Allebeck P, Falkstedt D. Academic performance, externalizing disorders and depression: 26,000 adolescents followed into adulthood. Soc Psychiatry Psychiatr Epidemiol. (2019) 54:977–86. doi: 10.1007/s00127-019-01668-z
5. Annett K. The Epidemiology of Child Psychopathology: Basic Principles and Research Data. In: Epidemiology Insights (InTech).
6. Riise EN, Wergeland GJH, Njardvik U, Öst LG. Cognitive behavior therapy for externalizing disorders in children and adolescents in routine clinical care: a systematic review and meta-analysis. Clin Psychol Rev. (2021) 83:101954. doi: 10.1016/j.cpr.2020.101954
7. Schwartz D, Mayeux L, Harper J. Bully/Victim Problems during Adolescence. In: Brown BB, Prinstein MJ, editors. Encyclopedia of Adolescence. New York, NY: Academic Press (2001). p. 25–34. doi: 10.1016/B978-0-12-373951-3.00045-4
8. Danielson ML, Bitsko RH, Holbrook JR, Charania SN, Claussen AH, McKeown RE, et al. Community-based prevalence of externalizing and internalizing disorders among school-aged children and adolescents in four geographically dispersed school districts in the United States. Child Psychiatry Hum Dev. (2020) 52:500–14. doi: 10.1007/s10578-020-01027-z
9. Achenbach TM, Edelbrock CS. Psychopathology of childhood. Annu Rev Psychol. (1984) 35:227–56. doi: 10.1146/annurev.ps.35.020184.001303
10. Levesque RJR. Externalizing and Internalizing Symptoms. In: Encyclopedia of Adolescence. Cham: Springer International Publishing (2018). p. 1274–7. doi: 10.1007/978-3-319-33228-4_539
11. Black JJ, Chung T. Mechanisms of change in adolescent substance use treatment: how does treatment work? Subst Abus. (2014) 35:344–51. doi: 10.1080/08897077.2014.925029
12. Samek DR, Hicks BM. Externalizing disorders and environmental risk: mechanisms of gene–environment interplay and strategies for intervention. Clin Pract. (2014) 11:537–47. doi: 10.2217/cpr.14.47
13. Tarver J, Daley D, Lockwood J, Sayal K. Are self-directed parenting interventions sufficient for externalising behaviour problems in childhood? A systematic review and meta-analysis. Eur Child Adolesc Psychiatry. (2014) 23:1123–37. doi: 10.1007/s00787-014-0556-5
14. Shortt JW, Stoolmiller M, Smith-Shine JN, Mark Eddy J, Sheeber L. Maternal emotion coaching, adolescent anger regulation, and siblings' externalizing symptoms. J Child Psychol Psychiatry. (2010) 51:799–808. doi: 10.1111/j.1469-7610.2009.02207.x
15. Van den Heuvel LL, Koning M, Nöthling J, Seedat S. Association of childhood maltreatment with internalising and externalising disorders in trauma-exposed adolescents. S Afr J Psychiatry. (2018) 24:a1266. doi: 10.4102/sajpsychiatry.v24i0.1266
16. Achenbach TM, Edelbrock CS. The classification of child psychopathology: a review and analysis of empirical efforts. Psychol Bull. (1978) 85:1275–301. doi: 10.1037/0033-2909.85.6.1275
17. Achenbach TM, Ivanova MY, Rescorla LA. Empirically based assessment and taxonomy of psychopathology for ages 1½−90+ years: developmental, multi-informant, and multicultural findings. Compr Psychiatry. (2017) 79:4–18. doi: 10.1016/j.comppsych.2017.03.006
18. van Wijk-Herbrink MF, Bernstein DP, Broers NJ, Roelofs J, Rijkeboer MM, Arntz A. Internalizing and externalizing behaviors share a common predictor: the effects of early maladaptive schemas are mediated by coping responses and schema modes. J Abnorm Child Psychol. (2018) 46:907–20. doi: 10.1007/s10802-017-0386-2
19. Lindstrom Johnson S, Elam K, Rogers AA, Hilley C. A meta-analysis of parenting practices and child psychosocial outcomes in trauma-informed parenting interventions after violence exposure. Prev Sci. (2018) 19:927–38. doi: 10.1007/s11121-018-0943-0
20. Vilela T, da Rocha MM, Figlie NB, Pillon SC, Diehl A, de Jesus Mari J. Domestic violence and risk of internalizing and externalizing problems in adolescents living with relatives displaying substance use disorders. J Bras Psiquiatr. (2020) 69:93–102. doi: 10.1590/0047-2085000000268
21. Ryan SM, Ollendick TH. The interaction between child behavioral inhibition and parenting behaviors: effects on internalizing and externalizing symptomology. Clin Child Fam Psychol Rev. (2018) 21:320–39. doi: 10.1007/s10567-018-0254-9
22. Willner CJ, Gatzke-Kopp LM, Bray BC. The dynamics of internalizing and externalizing comorbidity across the early school years. Dev Psychopathol. (2016) 28:1033–52. doi: 10.1017/S0954579416000687
23. Frick PJ, Matlasz TM. Disruptive, impulse-control, and conduct disorders. In: Developmental Pathways to Disruptive, Impulse-Control and Conduct Disorders. Cambridge, CA: Elsevier (2019). p. 3–20. doi: 10.1016/B978-0-12-811323-3.00001-8
24. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. American Psychiatric Association (2013). doi: 10.1176/appi.books.9780890425596
25. Fisher PA, Chamberlain P. Multidimensional treatment foster care. J Emot Behav Disord. (2000) 8:155–64. doi: 10.1177/106342660000800303
26. Beauchaine TP, McNulty T. Comorbidities and continuities as ontogenic processes: toward a developmental spectrum model of externalizing psychopathology. Dev Psychopathol. (2013) 25:1505–28. doi: 10.1017/S0954579413000746
27. Forehand R, Lafko N, Parent J, Burt KB. Is parenting the mediator of change in behavioral parent training for externalizing problems of youth? Clin Psychol Rev. (2014) 34:608–19. doi: 10.1016/j.cpr.2014.10.001
28. Berger I, Slobodin O, Aboud M, Melamed J, Cassuto H. Maturational delay in ADHD: evidence from CPT. Front Hum Neurosci. (2013) 7:691. doi: 10.3389/fnhum.2013.00691
29. Everitt BJ. Neural and psychological mechanisms underlying compulsive drug seeking habits and drug memories – indications for novel treatments of addiction. Eur J Neurosci. (2014) 40:2163–82. doi: 10.1111/ejn.12644
30. Cullen FT, Fisher BS, Applegate BK. Public opinion about punishment and corrections. Crime Justice. (2000) 27:1–79. doi: 10.1086/652198
31. Kersten L, Prätzlich M, Mannstadt S, Ackermann K, Kohls G, Oldenhof H, et al. START NOW - a comprehensive skills training programme for female adolescents with oppositional defiant and conduct disorders: study protocol for a cluster-randomised controlled trial. Trials. (2016) 17:568. doi: 10.1186/s13063-016-1705-6
32. Taubner S, Hauschild S. Conduct disorder – working with externalising behavioural problems in teens and their families. In: Mentalization-Based Treatment for Adolescents. Oxfordshire: Routledge (2021). p. 136–50. doi: 10.4324/9780429323928-9-13
33. Barlow DH, Patterson GR, Wells KC. A social learning approach, vol. 3: coercive family process. Behav Ther. (1984) 15:121–7. doi: 10.1016/S0005-7894(84)80046-5
34. McCart MR, Priester PE, Davies WH, Azen R. Differential effectiveness of behavioral parent-training and cognitive-behavioral therapy for antisocial youth: a meta-analysis. J Abnorm Child Psychol. (2006) 34:525–41. doi: 10.1007/s10802-006-9031-1
35. Weber L, Kamp-Becker I, Christiansen H, Mingebach T. Treatment of child externalizing behavior problems: a comprehensive review and meta–meta-analysis on effects of parent-based interventions on parental characteristics. Eur Child Adolesc Psychiatry. (2019) 28:1025–36. doi: 10.1007/s00787-018-1175-3
36. Webster-Stratton C. Randomized trial of two parent-training programs for families with conduct-disordered children. J Consult Clin Psychol. (1984) 52:666–78. doi: 10.1037/0022-006X.52.4.666
37. von Sydow K, Beher S, Schweitzer J, Retzlaff R. The efficacy of systemic therapy with adult patients: a meta-content analysis of 38 randomized controlled trials. Fam Process. (2010) 49:457–85. doi: 10.1111/j.1545-5300.2010.01334.x
38. von Sydow K, Retzlaff R, Beher S, Haun MW, Schweitzer J. The efficacy of systemic therapy for childhood and adolescent externalizing disorders: a systematic review of 47 RCT. Fam Process. (2013) 52:576–618. doi: 10.1111/famp.12047
39. Bosmans G. Cognitive behaviour therapy for children and adolescents: can attachment theory contribute to its efficacy? Clin Child Fam Psychol Rev. (2016) 19:310–28. doi: 10.1007/s10567-016-0212-3
40. Ugueto AM, Santucci LC, Krumholz LS, Weisz JR. Problem-Solving Skills Training. In: Evidence-Based CBT for Anxiety and Depression in Children and Adolescents. Chichester: John Wiley & Sons, Ltd. (2014). p. 247–59. doi: 10.1002/9781118500576.ch17
41. Dishion T, Forgatch M, Chamberlain P, Pelham WE. The oregon model of behavior family therapy: from intervention design to promoting large-scale system change. Behav Ther. (2016) 47:812–37. doi: 10.1016/j.beth.2016.02.002
42. Crick NR, Dodge KA. A review and reformulation of social information-processing mechanisms in children's social adjustment. Psychol Bull. (1994) 115:74–101. doi: 10.1037/0033-2909.115.1.74
43. de Castro BO, Veerman JW, Koops W, Bosch JD, Monshouwer HJ. Hostile attribution of intent and aggressive behavior: a meta-analysis. Child Dev. (2002) 73:916–34. doi: 10.1111/1467-8624.00447
44. Perry DG, Perry LC, Rasmussen P. Cognitive Social Learning Mediators of Aggression. Child Develop. (2016) 57:700–711. doi: 10.2307/1130347
45. Chamberlain P. The oregon multidimensional treatment foster care model: features, outcomes, and progress in dissemination. Cogn Behav Pract. (2003) 10:303–12. doi: 10.1016/S1077-7229(03)80048-2
46. Fisher PA, Gilliam KS. Multidimensional treatment foster care: an alternative to residential treatment for high risk children and adolescents. Psychosoc Interv. (2012) 21:195–203. doi: 10.5093/in2012a20
47. McKee L, Roland E, Coffelt N, Olson AL, Forehand R, Massari C, et al. Harsh discipline and child problem behaviors: the roles of positive parenting and gender. J Fam Violence. (2007) 22:187–96. doi: 10.1007/s10896-007-9070-6
48. Eyberg SM, Nelson MM, Boggs SR. Evidence-based psychosocial treatments for children and adolescents with disruptive behavior. J Clin Child Adolesc Psychol. (2008) 37:215–37. doi: 10.1080/15374410701820117
49. Pinquart M. Associations of parenting dimensions and styles with externalizing problems of children and adolescents: an updated meta-analysis. Dev Psychol. (2017) 53:873–932. doi: 10.1037/dev0000295
50. Yap MBH, Morgan AJ, Cairns K, Jorm AF, Hetrick SE, Merry S. Parents in prevention: a meta-analysis of randomized controlled trials of parenting interventions to prevent internalizing problems in children from birth to age 18. Clin Psychol Rev. (2016) 50:138–58. doi: 10.1016/j.cpr.2016.10.003
51. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
52. Cuijpers P. Meta-analyses in mental health research. A practical guide. Amsterdam: Uitgeverij. (2016) Available online at: https://indd.adobe.com/view/5fc8f9a0-bf1e-49d3-bf5f-a40bfe5409e0
53. Kazdin AE. Mediators and mechanisms of change in psychotherapy research. Annu Rev Clin Psychol. (2007) 3:1–27. doi: 10.1146/annurev.clinpsy.3.022806.091432
54. Lemmens LHJM, Müller VNLS, Arntz A, Huibers MJH, Shadish WR, Sweeney RB. Mediators and moderators in meta-analysis: theres reason we dont let dodo birds tell us which psychotherapies should have prizes. J Consult Clin Psychol. (2016) 59:883–93. doi: 10.1037/0022-006X.59.6.883
55. Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. (2018) 34:285–91. doi: 10.3233/EFI-180221
56. Dadds MR, Cauchi AJ, Wimalaweera S, Hawes DJ, Brennan J. Outcomes, moderators, and mediators of empathic-emotion recognition training for complex conduct problems in childhood. Psychiatry Res. (2012) 199:201–7. doi: 10.1016/j.psychres.2012.04.033
57. de Bruin EJ, Bögels SM, Oort FJ, Meijer AM. Improvements of adolescent psychopathology after insomnia treatment: results from a randomized controlled trial over 1 year. J Child Psychol Psychiatry. (2018) 59:509–22. doi: 10.1111/jcpp.12834
58. Deković M, Asscher JJ, Manders WA, Prins PJM, van der Laan P. Within-intervention change: Mediators of intervention effects during multisystemic therapy. J Consult Clin Psychol. (2012) 80:574–87. doi: 10.1037/a0028482
59. Eddy JM, Chamberlain P. Family management and deviant peer association as mediators of the impact of treatment condition on youth antisocial behavior. J Consult Clin Psychol. (2000) 68:857–63. doi: 10.1037/0022-006X.68.5.857
60. Henggeler SW, Melton GB, Smith LA. Family preservation using multisystemic therapy: an effective alternative t.: EBSCOhost. J Consult Clin Psychol. (1992) 60:953–961. Available online at: https://eds-b-ebscohost-com.ezp.waldenulibrary.org/eds/pdfviewer/pdfviewer?vid=4&sid=904576bc-14bc-48c1-99fe-c7d7a4103771%40pdc-v-sessmgr02%0Ahttp://web.bebscohost.com/ehost/detail/detail?vid=8&sid=ebae5ff4-bb97-4028-9384-83cca78fb86b%40sessionmgr101&bda
61. Henggeler SW, Letourneau EJ, Chapman JE, Borduin CM, Schewe PA, McCart MR. Mediators of change for multisystemic therapy with juvenile sexual offenders. J Consult Clin Psychol. (2009) 77:451–62. doi: 10.1037/a0013971
62. Hogue A, Dauber S, Stambaugh LF, Cecero JJ, Liddle HA. Early therapeutic alliance and treatment outcome in individual and family therapy for adolescent behavior problems. J Consult Clin Psychol. (2006) 74:121–9. doi: 10.1037/0022-006X.74.1.121
63. Huey SJ, Henggeler SW, Brondino MJ, Pickrel SG. Mechanisms of change in multisystemic therapy: Reducing delinquent behavior through therapist adherence and improved family and peer functioning. J Consult Clin Psychol. (2000) 68:451–67. doi: 10.1037/0022-006X.68.3.451
64. Jensen MR, Wong JJ, Gonzales NA, Dumka LE, Millsap R, Coxe S. Long-term effects of a universal family intervention: mediation through parent-adolescent conflict. J Clin Child Adolesc Psychol. (2014) 43:415–27. doi: 10.1080/15374416.2014.891228
65. Pantin H, Prado G, Lopez B, Huang S, Tapia MI, Schwartz SJ, et al. A randomized controlled trial of familias unidas for hispanic adolescents with behavior problems. Psychosom Med. (2009) 71:987–95. doi: 10.1097/PSY.0b013e3181bb2913
66. Paquette J, Vitaro F. Wilderness therapy, interpersonal skills and accomplishment motivation: impact analysis on antisocial behavior and socio-professional status. Resid Treat Child Youth. (2014) 31:230–52. doi: 10.1080/0886571X.2014.944024
67. Van Ryzin MJ, Leve LD. Affiliation with delinquent peers as a mediator of the effects of multidimensional treatment foster care for delinquent girls. J Consult Clin Psychol. (2012) 80:588–96. doi: 10.1037/a0027336
68. Fosco GM, Frank JL, Stormshak EA, Dishion TJ. Opening the “Black Box”: family check-up intervention effects on self-regulation that prevents growth in problem behavior and substance use. J Sch Psychol. (2013) 51:455–68. doi: 10.1016/j.jsp.2013.02.001
69. Gonzales NA, Dumka LE, Millsap RE, Gottschall A, McClain DB, Wong JJ, et al. Randomized trial of a broad preventive intervention for Mexican American adolescents. J Consult Clin Psychol. (2012) 80:1–16. doi: 10.1037/a0026063
70. Hess B. Assessing program impact using latent growth modeling: a primer for the evaluator. Eval Program Plann. (2000) 23:419–428. doi: 10.1016/S0149-7189(00)00032-X
71. Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. (1986) 51:1173–82. doi: 10.1037/0022-3514.51.6.1173
72. Van Ryzin MJ, Dishion TJ. The impact of a family-centered intervention on the ecology of adolescent antisocial behavior: Modeling developmental sequelae and trajectories during adolescence. Dev Psychopathol. (2012) 24:1139–1155. doi: 10.1017/S0954579412000582
73. Holmbeck GN. Toward terminological, conceptual, and statistical clarity in the study of mediators and moderators: Examples from the child-clinical and pediatric psychology literatures. J Consult Clin Psychol. (1997) 65:599–610. doi: 10.1037/0022-006X.65.4.599
74. Tofighi D, MacKinnon DP. RMediation: An R package for mediation analysis confidence intervals. Behav Res Methods. (2011) 43:692–700. doi: 10.3758/s13428-011-0076-x
75. Hogan AE, Quay HC, Vaughn S, Shapiro SK. Revised behavior problem checklist: stability, prevalence, and incidence of behavior problems in kindergarten and first-grade children. Psychol Assess A J Consult Clin Psychol. (1989) 1:103–11. doi: 10.1037/1040-3590.1.2.103
76. Friedrich WN, Lysne M, Sim L, Shamos S. Assessing sexual behavior in high-risk adolescents with the Adolescent Clinical Sexual Behavior Inventory (ACSBI). Child Maltreat. (2004) 9:239–50. doi: 10.1177/1077559504266907
78. Capaldi DA, Rothbart MK. Development and validation of an early adolescent measure. J Early Adolesc. (1992) 12:153–73. doi: 10.1177/0272431692012002002
79. Dishion TJ, Patterson GR, Stoolmiller M, Skinner ML. Family, school, and behavioral antecedents to early adolescent involvement with antisocial peers. Dev Psychol. (1991) 27:172–80. doi: 10.1037/0012-1649.27.1.172
80. Lucas CP, Zhang H, Fisher PW, Shaffer D, Regier DA, Narrow WE, et al. The DISC Predictive Scales (DPS): efficiently screening for diagnoses. J Am Acad Child Adolesc Psychiatry. (2001) 40:443–9. doi: 10.1097/00004583-200104000-00013
81. Dadds MR, Hawes D, Merz S. The UNSW Facial Emotion Task. Sidney, AU: University of New South Wales. (2004).
83. Dadds MR, Hunter K, Hawes DJ, Frost ADJ, Vassallo S, Bunn P, et al. Griffith Empathy Measure (GEM).[Database record]. APA Psyc Tests. (2008) doi: 10.1037/t64021-000
84. Kerkhof GA, Geuke ME, Brouwer A, Rijsman RM, Schimsheimer RJ, Van Kasteel V. Holland sleep disorders questionnaire: a new sleep disorders questionnaire based on the international classification of Sleep Disorders-2. J Sleep Res. (2013) 22:104–7. doi: 10.1111/j.1365-2869.2012.01041.x
85. Borduin CM, Blaske DM, Cone L, Mann BJ. Development and Validation of a Measure of Adolescent Peer Relations: The Missouri Peer Relations Inventory. Columbia, (1989). [Epub ahead of print].
86. Barnes HL, Olson DH. Parent-adolescent communication and the circumplex model. Child Dev. (1985) 56:438–47. doi: 10.2307/1129732
87. Slater MA, Power TG. “Multidimensional assessment of parenting in single-parent families,” in Advances in familily intervention, assessment, theory, ed. J. P. Vincent (Greenwich, CT: JAI Press), 197–228.
88. Barber BK. Parental psychological control: revisiting a neglected construct. Child Dev. (1996) 67:3296–319. doi: 10.2307/1131780
89. Winters KC, Henly GA. Personal Experience Scales (PES). Analyses of Treatment Research: NIDA Research Monograph (1989) 77:4–18. doi: 10.1037/t07539-000
90. Gorman-Smith D, Tolan PH, Zelli A, Huesmann LR. The relation of family functioning to violence among inner-city minority youths. J Fam Psychol. (1996) 10:115–29. doi: 10.1037/0893-3200.10.2.115
92. Prado G, Huang S, Maldonado-Molina M, Bandiera F, Schwartz SJ, de la Vega P, et al. An empirical test of ecodevelopmental theory in predicting HIV risk behaviors among hispanic youth. Heal Educ Behav. (2010) 37:97–114. doi: 10.1177/1090198109349218
93. Jemmott JB III, Sweet Jemmott L, Fong GT. Abstinence and safer sex HIV risk-reduction interventions for African American adolescents. JAMA. (1998) 279:1529. doi: 10.1001/jama.279.19.1529
94. Derogatis LR, Lazarus L. “SCL-90—R; Brief Symptom Inventory; matching clinical rating scales,” in The use of psychological testing for treatment planning outcome assessment, ed. M. E. Maruish (Lawrence Erlbaum Associates; Inc.), 217–248.
95. Goodman R. The strengths and difficulties questionnaire: a research note. J Child Psychol Psychiatry. (1997) 38:581–6. doi: 10.1111/j.1469-7610.1997.tb01545.x
96. Elliott DS, Ageton SS. Reconciling race and class differences in self-reported and official estimates of delinquency. Am Sociol Rev. (1980) 45:95–110. doi: 10.2307/2095245
97. Sobell LC, Brown J, Leo GI, Sobell MB. The reliability of the alcohol timeline followback when administered by telephone and by computer. Drug Alcohol Depend. (1996) 42:49–54. doi: 10.1016/0376-8716(96)01263-X
98. O'Malley SS, Suh CS, Strupp HH. The vanderbilt psychotherapy process scale: a report on the scale development and a process-outcome study. J Consult Clin Psychol. (1983) 51:581–6. doi: 10.1037/0022-006X.51.4.581
100. Mestre JM, Turanzas J, García-Gómez M, Guerra J, Cordon JR, De La Torre GG, et al. Do trait emotional intelligence and dispositional mindfulness have a complementary effect on the children's and adolescents' emotional states? Front Psychol. (2019) 10:2817. doi: 10.3389/fpsyg.2019.02817
101. Abrahamse ME, Niec LN, Junger M, Boer F, Lindauer RJL. Risk factors for attrition from an evidence-based parenting program: findings from the Netherlands. Child Youth Serv Rev. (2016) 64:42–50. doi: 10.1016/j.childyouth.2016.02.025
102. Ross JM, Granja K, Duperrouzel JC, Pacheco-Colón I, Lopez-Quintero C, Hawes SW, et al. Risky sexual behavior among adolescents: the role of decision-making, problems from cannabis use and externalizing disorder symptoms. J Clin Exp Neuropsychol. (2019) 41:300–11. doi: 10.1080/13803395.2018.1550192
103. Rivera FI, Guarnaccia PJ, Mulvaney-Day N, Lin JY, Torres M, Alegría M. Family cohesion and its relationship to psychological distress among Latino groups. Hisp J Behav Sci. (2008) 30:357–78. doi: 10.1177/0739986308318713
104. Tiernan K, Foster SL, Cunningham PB, Brennan P, Whitmore E. Predicting early positive change in multisystemic therapy with youth exhibiting antisocial behaviors. Psychotherapy (2015) 52:93–102. doi: 10.1037/a0035975
105. Blader JC. Which family factors predict children's externalizing behaviors following discharge from psychiatric inpatient treatment? J Child Psychol Psychiatry. (2006) 47:1133–42. doi: 10.1111/j.1469-7610.2006.01651.x
Keywords: externalising disorders, psychological-treatment effectiveness, externalising behaviours, therapeutic mediation, systematic review, adolescence, distal and proximal factors
Citation: Mestre JM, Taubner S, Mota CP, Rangel Henriques M, Saliba A, Heinonen E, Ramos S, Moreno-Peral P, Volkert J, Adler A, Barkauskiene R, Conejo-Cerón S, Di Giacomo D, Ioannou Y, Mucha Vieira F, Røssberg JI, Sales CMD, Schmidt SJ, Stepisnik Perdih T, Ulberg R and Protić S (2022) Theories of Change and Mediators of Psychotherapy Effectiveness in Adolescents With Externalising Behaviours: A Systematic Review. Front. Psychiatry 12:730921. doi: 10.3389/fpsyt.2021.730921
Received: 25 June 2021; Accepted: 05 November 2021;
Published: 14 January 2022.
Edited by:
Patrick W. L. Leung, The Chinese University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Say How Ong, Institute of Mental Health, SingaporeBenjamin Mugo Kagina, University of Cape Town, South Africa
Copyright © 2022 Mestre, Taubner, Mota, Rangel Henriques, Saliba, Heinonen, Ramos, Moreno-Peral, Volkert, Adler, Barkauskiene, Conejo-Cerón, Di Giacomo, Ioannou, Mucha Vieira, Røssberg, Sales, Schmidt, Stepisnik Perdih, Ulberg and Protić. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José M. Mestre, am9zZW1pLm1lc3RyZUB1Y2EuZXM=; Svenja Taubner, c3ZlbmphLnRhdWJuZXJAbWVkLnVuaS1oZWlkZWxiZXJnLmRl; Sonja Protić, c29uamEubWlsb2pldmljQGlrc2kuYWMucnM=
†These authors have contributed equally to this work