 Yumeng Xie
Yumeng Xie Gaohua Wang
Gaohua Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry, 05 November 2021
Sec. Mood Disorders
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.705559
This article is part of the Research TopicFundamentals of 21st Century NeuroscienceView all 32 articles
Background: It is necessary to seek alternative therapies for depression, because side effects of medications lead to poor adherence and some patients do not achieve a clinical treatment effect. Recently the role of exercise as a low-cost and easy-to-use treatment for depression has gained attention with a number of studies showing that exercise is effective at reducing depressive symptoms and improving body functions such as cardiorespiratory system and cognitive function. Because of the heterogeneity of exercise therapy programs, there is no standardized and unified program. Few studies have summarized the specific properties of exercise programs (type, intensity, duration, and frequency) and clinical prescriptions for exercise are not mentioned in most articles.
Aims: This study aimed to investigate the feasibility and efficacy of exercise therapy for patients with depression, in order to appraise the evidence and outline accepted guidelines to direct individualized treatment plans for patients with depression based on their individual situations.
Methods: A systematic review of English language literature including papers published from 2010 to present in PubMed was performed. Given the feasibility of prescribing exercise therapy for patients with depression, nearly 3 years of clinical studies on the treatments of depressive symptoms with exercise were first reviewed, comparing the exercise programs utilized.
Conclusions: Exercise has therapeutic effects on depression in all age groups (mostly 18–65 years old), as a single therapy, an adjuvant therapy, or a combination therapy, and the benefits of exercise therapy are comparable to traditional treatments for depression. Moderate intensity exercise is enough to reduce depressive symptoms, but higher-dose exercise is better for overall functioning. Exercise therapy has become more widely used because of its benefits to the cardiovascular system, emotional state, and systemic functions.
Recommendations: Aerobic exercise/mind-body exercise (3–5 sessions per week with moderate intensity lasting for 4–16 weeks) is recommended. Individualized protocols in the form of group exercise with supervision are effective at increasing adherence to treatment.
Depression is characterized by low mood, anhedonia, and loss of interest. It has a relatively high incidence affecting both mental and physical health and places a heavy burden on individuals, families, and society. The World Health Organization once showed that ~350 million people were currently suffering from depression, and the disease may last for years (1). The Global Burden of Disease project revealed that depression was now the most serious disease burden of non-fatal neuropsychiatric diseases, and was projected to be in the top three of all disease burdens by 2030 (2). The financial toll of depression is enormous. The annual cost of days lost to depression and anxiety worldwide is estimated at $1.15 trillion, and is projected to triple by 2030 (3). The treatment and prevention of depression is a hot and widely studied research topic.
At present, depression therapies mainly include pharmacotherapy, psychotherapy, biological interventions [electric convulsive therapy (ECT), transcranial direct current stimulation, and transcranial magnetic stimulation], and naturopathic interventions. Antidepressants play a significant role in the treatment of depression, but there are disadvantages to their use, including the possibility of more and longer lasting side effects, poor adherence to antidepressant medications, increased risk of cardiovascular disease, low remission rate, and high recurrence rate (4–6). Only half of patients taking antidepressants achieve a clinical treatment effect, a decrease of 50% or more in depressive symptoms (7). In addition, dropout rates of drug therapy ranged from 15 to 132% higher than placebo (6). Concerns about antidepressant efficacy and tolerability in patients have led to interest in non-pharmacological treatments for depression (5). Compared with medication therapy, patients who are particularly averse to drugs and worry about side effects prefer non-medication therapy (5). In Steffi et al.'s interview of patients with depression (8), among the treatment options of psychotherapy, natural remedies, acupuncture, relaxation, psychotropic drugs, meditation/yoga, and ECT, psychotherapy was identified as the most favored treatment in cases of depression, with half of the interviewees identifying it as their first choice, while psychotropic drug treatment was ranked fourth. Non-pharmacological interventions may have a beneficial effect on relapse rates following treatment (9) and lower adverse effects (5). Therefore, exercise therapy, as an emerging non-pharmacological treatment, is a new feasible choice in the treatment of depression. It is simple to perform (10). Additionally, such therapy has a low cost (10, 11) and has almost no side effects (10, 11). It can prevent recurrence (12), has a positive role in overall body function (11), and has no stigma. A growing body of research has shown that exercise can relieve symptoms of depression, and that it can be used as an adjunct or individual treatment.
A systematic review of English language literature published from 2010 to present in PubMed was performed, with 822 studies searched. Terms included in the cross-searches were: depression, exercise, physical activity, swimming, aerobic exercise, non-pharmacological treatment, and exercise therapy. Randomized controlled studies, case-control studies, reviews, and animal experiments were included in our work. Inclusion criteria were: (1) treatment with an exercise program; (2) patients with depression or depressive symptoms estimated by depression scales such as the Hamilton Depression Scale, Beck Depression Inventory and the Diagnostic and Statistical Manual of Mental Disorders; and (3) the outcome measures included primary depression outcomes (cognition, mood state, and psychometric outcomes), or associated health outcomes (quality of life, anxiety, cardiorespiratory system, physiological outcomes, etc.). The literature screening process excluded articles that did not address depressive illness or depressive symptoms, and that did not include depressive symptoms and related improvement in the primary measures. Studies on prevention of depression were not included.
In the last 10 years of the literature, heterogeneity in exercise therapy programs has been found. There is no standardized and unified program. Moreover, few studies summarize the specific properties of exercise programs (type, intensity, duration, and frequency), and clinical prescriptions for exercise are not mentioned in most articles. This paper reviews observational and interventional studies incorporating both preclinical and clinical studies on the relationship between exercise and depression, including the selection and comparison of exercise programs, the effects of exercise on depression treatment and the related mechanisms, and the role of exercise in comorbid diseases with depression, its clinical application, and prospects. This paper aims to investigate the feasibility and efficacy of exercise therapy for patients with depression to appraise the evidence and outline accepted guidelines to direct individualized treatment plans for patients with depression based on their individual situations.
Exercise programs are generally heterogeneous, with different types, intensities, durations, and frequencies. The types of exercise include aerobic, non-aerobic, and mind-body exercise. In clinical research, exercise types include walking (13–18), various types of bicycle use (bicycle, stationary bicycle, ergometric bicycle, and recumbent bicycle) (4, 19–30), swimming (29), jogging or treadmill use (20, 23, 24, 27, 28, 31), cross-training (22), jumping rope (22), use of “transport” machines (23), step aerobics and cardio-kickboxing (15), resistance exercises using TheraBand, dumbbells, Swiss Balls, etc. (29), stretching exercises (19, 32–34), free weight training (35), traditional Chinese exercises such as Taijiquan and Qigong (36–39), yoga (15, 32–34, 40), and Pilates (15, 41). Aerobic exercise was the most selected intervention in the experiments. To improve participants' compliance, several types of exercises were provided for participants to choose from (20). Various forms of exercise, including yoga, resistance, and aerobic exercise, have shown beneficial effects on the mental health of young people (42). Similarly, mind-body exercise, aerobic exercise, and resistance exercise are effective treatments for depressive symptoms in elderly patients (43).
In clinical trials, the most common way to determine exercise intensity is to set the amount of time each week or each day. Other studies have also utilized metabolic equivalent (MET) (44), heart rate (HR) or maximal heart rate (HRmax) (4, 14, 20, 21, 24, 44–46), maximal oxygen uptake (VO2 max) (4, 44, 47, 48), maximum power output (Wmax) (49), Borg Scale (16, 28), kilocalories burned per kilogram of body weight per week (KKW) (20, 24, 47), and ratings of perceived exertion (RPE) (4, 14, 24, 27, 48–50). Moderate-intensity exercise is the most popular choice in previous studies, but the standard for moderate exercise remains equivocal. In addition, high-intensity exercise programs and low-intensity exercise programs may also produce positive results. Low-intensity exercises include yoga, stretching exercises, mechanical exercises, and combined exercises, which are sometimes utilized in control groups in experiments. Moderate- and high-intensity exercise programs are often considered to have a greater antidepressant effect, but a higher intensity program often has lower compliance and a higher dropout rate (51). Hence, various factors, such as the intensity, longevity, and sustainability of exercise, need to be taken into consideration (52). There is no standardized exercise therapy program at present, and individualized treatment programs may play a role in the efficacy of exercise therapy.
In addition to a single-type exercise program, several studies (19, 53) combine different types of high-intensity and low-intensity exercises to form a systematic and structured exercise program. Similarly, one experiment (22) chose an exercise program that had both high-intensity (16–17 on the Borg Scale) and low-intensity (13–14 on the Borg Scale) exercises, resulting in improvements in the Montgomery-Asberg Depression Rating Scale (MADRS) score (mean change=-10.3, 95% confidence interval (CI) [−13.5 to −7.1], p = 0.038) and cardiovascular fitness (mean change = 2.4 ml oxygen/kg/min, 95% CI [1.5–3.3], p = 0.017) in the exercise group. The duration of the exercise program ranges from 4 to 24 weeks, with most experiments choosing 12 weeks. Another publication chose a single exercise session (17), but only showed a transient regulation effect. Only a handful of studies had follow ups at 6-month or 1-year periods to examine long-term effects, and in one 16-month work (54), patients with MDD (major depressive disorder) were followed for up to a year after 4 months of aerobic training. The results showed that regular exercise during the follow-up period seems to enhance the beneficial effects of short-term exercise and augment the efficacy of antidepressants. In a 12-month follow-up in another study (34), no increase was found in the severity of depression among patients with mild to moderate depression, suggesting that the beneficial effects of exercise on depression were not temporary. However, few studies are followed up, and more evidence is consequently needed. The frequency of exercise was based on the number of days or sessions per week, and most of the trials adapted exercise protocols with 3–5 days/sessions per week.
It is controversial whether the intensity and dose of exercise improves depressive symptoms differently. Hanssen et al. (4) demonstrated that both high-intensity low volume (HILV) (25 repetitions of 30 s high-intensity intervals at 80% VO2 max) and moderate continuous aerobic training (MCT) (20 min at a constant pace of 60% VO2 max) exercise regimens (three times a week for a period of 4 weeks) significantly reduced the depression severity index, with the former being superior. Similarly, one work has found that a higher dose (intensity, duration, and frequency) according to public health guidelines improved depressive symptoms more greatly than a lower dose of exercise (33). Compared to moderate exercise intensities, higher intensities are able to increase circulating brain-derived neurotrophic factor (BDNF) (55), a neurotrophin that is decreased significantly in depression patients. Commonly, moderate and vigorous exercise both improve the level of depression in patients with moderate depression, but very low-intensity exercise has no effect (46). A meta-analysis (56) concluded that moderate exercises, aerobic exercises, and interventions supervised by exercise professionals were more effective in MDD patients, and the benefits of exercise may have been underestimated in previous meta-analyses due to publication bias. However, other studies (33, 48) have suggested that the effect of exercise on depression is independent of the dose, intensity, or other natures of exercise. Exercise intensity may not be the main factor affecting depressive relief, as light exercise is sufficient to improve the outcome of late-life depression (25). Additionally, low-intensity mind-body exercise (such as yoga) has a significant effect as a treatment for depression (43). One probable explanation for why light exercise is more beneficial than moderate exercise is that the former is easier to perform and patients gain a greater sense of self-esteem and control (33).
This paper suggest that aerobic exercise was the most selected intervention in the experiments and moderate intensity was chosen the most though the standard for moderate exercise remains equivocal. The duration of the exercise program ranges from 4 to 24 weeks, with most experiments choosing 12 weeks. Most of the trials adapted exercise protocols with 3–5 days/sessions per week. Consequently, there is no standardized exercise therapy program at present, and individualized treatment program may play a role in the efficacy of exercise therapy. This article provides a summary table of clinical studies of exercise therapy for depression or depressive symptoms in recent years, listed in Table 1. Many of the latest studies (18, 30, 37, 38, 41, 66–69) are included.
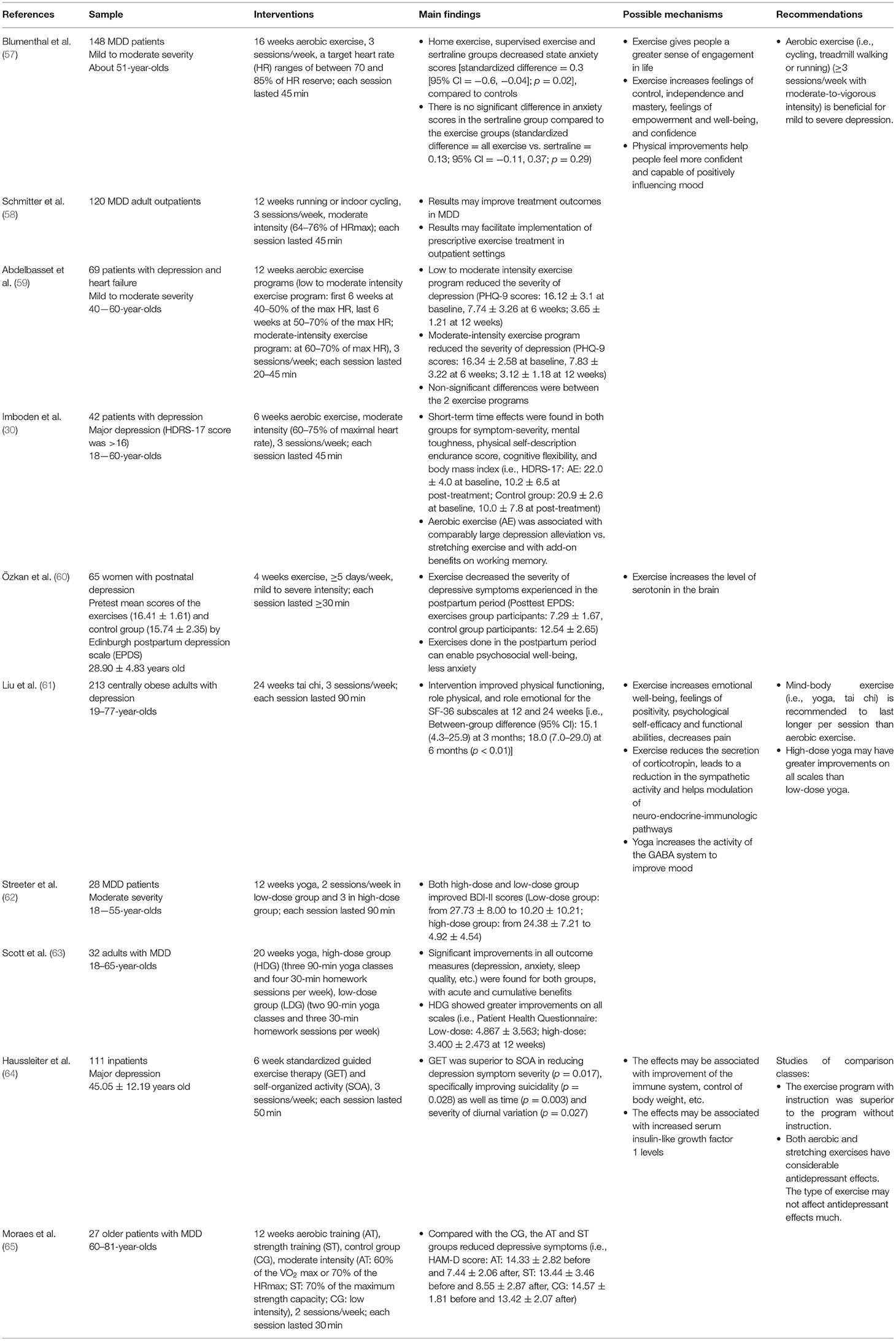
Table 1. The effects of recent exercise interventions in patients with diagnosed depression.
It is widely known that exercise has beneficial effects on depressive symptoms and body functions. However, more research is needed into the mechanisms underlying the antidepressant effects of exercise. Most studies on the mechanisms of the antidepressant effect of exercise are rodent studies, and some clinical studies are involved as well. Therefore, we have synthesized rodent research and human studies to summarize the mechanisms of the antidepressant effect of exercise.
The mechanisms of exercise therapy for depression are related to psychological mechanisms and physiological mechanisms. The former includes psychosocial and cognitive factors; the latter includes anti-inflammatory effects, neuroplasticity mechanisms, etc. The biochemical factors involved include β-endorphin (20), vascular endothelial growth factor (VEGF) (70), brain-derived neurotrophic factor (BDNF) (20, 49, 71), 5-hydroxytryptamine (5-HT) (20, 70), insulin-like growth factor 1 (IGF-1) (70, 72), histone methyltransferase G9a (73), neuropeptide oxytocin (OXT) (73), arginine vasopressin (AVP) (73), and several others (74–77), which will be introduced in detail below.
Person-centered physical therapy approaches (person-centered aerobic exercise using intervals with higher perceived intensity for 10 weeks) (22), in which investigators explored the patient's perceived needs and beliefs based on humanism, typically have a better outcome in treating depression. This finding, as well as the significant effects of mind-body exercise on depression mentioned above, suggested the role of psychological factors in the improvement of depressive symptoms through exercise, at least to some extent.
Combining the results of previous studies, exercise can enhance self-worth and self-esteem after receiving positive feedback (78), and may augment self-efficacy, self-confidence, sleep quality, and life satisfaction (20, 26, 79, 80). Physical therapist-guided aerobic exercise enhanced the feeling of being alive and made them feel that they were doing something good for themselves (79). A review (81) that conducted non-systematic searches to identify mechanisms of the antidepressant effect of exercise provided evidence that exercise can promote self-esteem, self-perception, and self-efficacy and can enhance social support to create a buffer against depressive symptoms. For cognitive function, a 12-week, multimodal exercise program of 70–90% HRmax may play a role in transferring negative thoughts of youth with MDD (53). Some studies (80, 82) also suggested that during exercise interventions, patients may seek social support, which reduces loneliness. Based on the psychological and social benefits, group exercise is generally considered to be more effective than individual exercise, but no studies have compared their efficacies to each other (individual compared to group exercise). In addition, exercise may also be related to mechanisms involved in behavioral activation (53).
Neuroinflammation is well-known to play a key role in the pathogenesis of depression. In the central nervous system (CNS), microglia are best known as the key immune cells of the brain (83). Findings have shown that activation of microglia under pathological conditions leads to a decrease in neurogenesis (84) and the release of a large number of inflammatory factors, including interleukin-18 (IL-18), interleukin-1β (IL-1β), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α), which exerted neurotoxic effects and cause depression and anxiety (85). A large number of studies have confirmed that stress can cause the activation of microglia and the release of proinflammatory factors (85, 86). Caspase-1 is the effector protein of the nucleotide-binding and oligomerization domain (NOD)-like receptor (NLR) protein 3 (NLRP3) inflammasome, a member of the NLR family of cytosolic pattern recognition receptors (87). The inflammasome is known to consist of the NLR family member NLRP3, the apoptosis-associated speck-like protein containing a caspase recruitment domain (ASC) adaptor protein and the effector protein caspase-1. It has been revealed that after exposure to stressors, assembly of the NLRP3 inflammasome increases, leading to an increase in the protein levels of ASC and cleaved caspase 1 (88). NLRP3 continuously cleaves IL-1β and IL-18 precursors into mature IL-1β and IL-18 through activated caspase-1, thereby producing a large number of downstream inflammatory mediators (89). After caspase-1 is activated, cleaved caspase-1 is released from the inflammasome (90). Thus, we proposed that exercise alleviates depressive symptoms through antidepressant effects, although the mechanism of exercise therapy for depression has not been fully elucidated.
The anti-inflammatory effect of exercise has been mentioned in articles (12, 53, 72, 74, 75). Sixteen-week exercise (dose recommendations based on the Ainsworth Compendium of Physical Activities) with at least four 40-min homework exercise sessions per week, consisting of at least moderate physical activity, increases the production of the anti-inflammatory cytokine IL-10 and reduces the production of proinflammatory cytokines, proinflammatory markers, and cytokines such as C-reactive protein (CRP) and IL-6 in MDD, which may be the mechanism of its antidepressant effect of depression (75). A clinical investigation by Ventura et al. (76) showed that aerobic exercise programs, of which in-clinic training consisting of a combination of moderate intensity aerobic exercises (1-min intervals) and moderate to high intensity strength and calisthenic conditioning (1-min intervals) for 45 min twice a week over a period of 6 months, can reduce IL-6 levels in patients with schizophrenia, and that the reduction of pro-inflammatory IL-6 level was significantly associated with reduced depressive symptoms, suggesting that exercise plays an important role in the anti-inflammatory mechanism in the treatment of depression. More research is needed to illustrate the anti-inflammatory effect of exercise.
Oxidative stress (OS)-related endothelial damage is associated with the occurrence and development of a variety of diseases, such as vascular depression and late-life depression (91). Moderate aerobic exercise reduces OS and inflammation, reduces endothelial damage, improves endogenous antioxidant defense systems, and promotes the expression of superoxide dismutase, glutathione peroxidase, and glutathione reductase. It also reduces the concentration of several inflammatory biomarkers, such as IL-6, homocysteine, and tumor necrosis factor-α (TNF-α), and restrains the activity of NADH oxidase (74, 91). Brocardo et al. (92) illustrated that voluntary wheel running alleviated depression-like symptoms in male rats from prenatal ethanol exposure and that the positive effects of exercise were linked to increased levels of antioxidants such as glutathione. Moreover, an animal study (93) has demonstrated that exercise increased the endothelial nitric oxide synthase (eNOS) expression and activation both in the vascular wall and in the perivascular adipose tissue, which was associated with lowering ROS in the vascular wall, leading to the improvement of the vascular function. In addition, the inhibition of hippocampal DNA oxidation (11) was also mentioned. In clinical studies, 12-week aquatic exercise in depressed elderly individuals (n = 92) was shown to reduce depression and anxiety, and decreases oxidative stress (94).
The antidepressant effects of exercise are associated with enhanced neurogenesis in the adult hippocampus, increased synaptic growth, and synaptic plasticity (47, 74, 95, 96), which effectively stimulate neurogenesis in the hippocampal dentate gyrus (DG) and promote hippocampal growth (12, 97). Within the signaling pathways, two related growth factors are VEGF and IGF-1 (70). Research by Tang et al. (98) indicated that exercise increases the expression of oligodendrocyte-related proteins and the number of oligodendrocytes in the hippocampus of rats with depression. In previous studies, growth-associated protein 43 (GAP-43) and synaptophysin (SYN) were involved in the alterations of hippocampal plasticity in mice, and SIRT1/microRNA, CREB/BDNF, and AKT/GSK-3β signaling pathways may be related to the regulation (77). Exercise also promotes neural differentiation, enhances the plasticity of new neurons by increasing the complexity of dendrites and the short-term synaptic plasticity of some nerves, and has pro-neurogenic action of progenitor cells of the hippocampus (95). Ma et al. (96) examined the roles of physical exercise in inducing hippocampal neurogenesis in humans and rodents to determine its effectiveness in the prevention or decline of cognition, confirming that physical exercise induces neurogenesis including proliferation, differentiation, survival, maturation, and function.
BDNF is associated with neuronal survival and synaptic plasticity (17), and a growing body of research suggests that BDNF may mediate exercise to improve depressive-like behavior. Szuhany and Otto's studies of outpatients with MDD and persistent depression (99) demonstrated that both acute and regular exercise caused an increase in BDNF. Several additional studies (49, 71) have also linked BDNF to neurogenesis and plasticity. A study of elderly women with major depression showed that a single exercise session significantly increased serum BDNF levels; however, it showed a significant secondary decrease in BDNF serum levels after 30 min of rest (17), suggesting that acute exercise might be beneficial for MD treatment and further studies including the effects of long-term exercise on BDNF serum levels are needed. However, to date there are no reports of sustained augmentation of BDNF after acute exercise (74). Differences between studies suggest that more longitudinal studies are needed to demonstrate the relationship between exercise and BDNF.
In addition, exercise causes an increase in neurotransmitters associated with increased activity of dopamine, 5-hydroxytryptamine, and noradrenaline in the central nervous system (CNS) (28, 74, 100). The volume and structural integrity of the hippocampus, anterior cingulate cortex (ACC), prefrontal cortex, and corpus callosum and alteration of the responsivity of the ventral striatum are also related to the neural mechanism of exercise therapy for depression (100, 101). A more recent study (102) also confirmed that moderate-intensity (which was defined as 50–70% of maximum heart rate) aerobic exercise, consisting of 30 min running, 4 days per week for 3 months, can induce structural changes in the rostral ACC in adolescents with subthreshold mood syndromes.
The relationship between exercise and the hypothalamic pituitary adrenal (HPA) axis is complex and is influenced by the different natures of exercise and stress and the characteristics of the research population (74). There is experimental evidence that short-term running stimulates neurogenesis in rats, while long-term exercise may be turned into a stressor by the activation of the HPA axis, which reduces the rate of cell proliferation (97).
Swimming can alleviate the depression-like behavior of rat offspring, which is associated with mitochondrial movement related to O-GlcNAc transferase (OGT), which includes the PINK1/Parkin and AKT/GSK3 signaling pathways. Another study (103) has also shown that this effect was related to the improvement of mitochondrial morphology and function, which illustrated that hippocampal ATP production and mitochondrial membrane potential of rats in the exercise group increased significantly, while the production of mitochondrial superoxide decreased significantly; also, the high HPA activity in rats with depression was reversed. Endurance exercise has also been shown to stimulate mitochondrial biogenesis in a wide range of tissues (74).
The neuroimmune mechanisms of exercise include an increase in the number of macrophages entering the CNS in cellular immunity, the upregulation of CXCL1, CXCL12, MKP-1, and IGF-1 in humoral immunity, and the activation of anti-inflammation and antioxidation, as detailed in Harris Eyre's review (104). The downstream changes were as follows: (1) HPA axis: glucocorticoids (GCs) were downregulated, and glucocorticoid receptor (GR) receptor activity and density increased. (2) Neurodegenerative changes: neuronal proliferation increased, metabolism decreased, BDNF was upregulated, and caspase activation decreased. (3) Monoamine metabolism: 5-HT and NA were upregulated, and indoleamine-2,3-dioxygenase (IDO) and quinolinic acid (Quin) were downregulated.
The antidepressant effects are related to hormonal responses. The mechanisms involved include increased testosterone levels (11) and endorphins release (46) as well. Resistance exercise has been shown to elicit a significant acute hormonal response, involving hormones including testosterone, growth hormones (GH), cortisol, insulin-like growth factors (IGFs), insulin, catecholamine, and other hormones, as detailed in Kraemer's review (105).
It is also believed that exercise regulates the metabolism of kynurenine, which enhances antidepressant ability (106–108).
The beneficial effects of exercise on depression and depressive symptoms have been demonstrated in the last decade, with a large body of research supporting the effect of physical exercise on reducing depressive symptoms in patients (26, 95). For instance, a study (30) aimed at patients with depression (aged 18–60) revealed regardless of aerobic exercise or stretching exercise, there was a significant short-term time effect for symptom severity [Hamilton Depression Rating Scale 17 (HDRS17): p < 0.001, η2 = 0.70; BDI: p < 0.001, η2 = 0.51], mental toughness (p < 0.001, η2 = 0.32), physical self-description endurance score (p = 0.013, η2 = 0.16), cognitive flexibility (p = 0.013, η2 = 0.14), and body mass index (BMI) (p = 0.006, η2 = 0.19). A meta-analytical review (109) that included 1,452 clinically depressed adults revealed that large effects in favor of exercise were found, irrespective of the exercise mode and study quality, compared to the control condition.
A summary of clinical studies over the past 3 years on the exercise effects on depression is provided in Table 1. Aerobic exercises (i.e., stride walking, treadmills, cycling, cross trainers) for people with other conditions (schizophrenia, dementia, chronic stroke, at high risk of depression, etc.) (18, 66, 72, 107, 110–124) and mind-body exercises (i.e., yoga, tai chi, Qigong, Ba-Duan-Jin, Pilates) for people with other conditions (healthy state, menopause, aging, scleroderma, Parkinson's disease, fibromyalgia, HIV, etc.) (37, 39–41, 120, 125–136) were proven to improve depression, anxiety, cognitive function, and overall functions such as sleep quality, psychological well-being, sexual function, and cardiorespiratory fitness as well. Although aerobic exercise and mind-body exercise are the most studied types of exercise with significant results, resistance exercise, stretching exercise, endurance exercise, and other types of exercise have also proven to be effective treatment options for depression (67, 72, 107, 110, 137–140). Structured/combined exercise (including resistance, aerobic, strength, balance, relaxation, and endurance exercise) is recommended (53, 69, 141–151); however, there have been no studies comparing structured exercise with a single exercise program.
Existing studies have almost covered patients with depression in a wide range of characteristics. Most of the research subjects were adults (18–65 years old), and a few subjects were teenagers and elderly people. Exercise benefits young people in terms of improving their mental health, and there is a bidirectional relationship between physical activity and adolescent mental health (42). Nasstasia et al. (53) used a structured multimodal exercise program combined with motivational interviewing (MI) as adjunctive therapy in patients aged 15–25 with major depression (MDD), resulting in a significant difference in the revised Beck Depression Inventory II (BDI-II) cognitive and affective subscales of the intervention group after treatment and improved somatic health and behavioral activation. Several studies of patients with late-life (older than 65) depression (152) have also confirmed that exercise reduced depressive symptoms.
There are a number of trials (29, 153–155) that have failed to prove the efficacy of exercise in treating depressive symptoms. For instance, clinical research in 2012 has shown that the provision of tailored advice and encouragement for physical activity did not improve depression outcomes or antidepressant use in adults with depression when compared with usual care (156). In Table 1, there are two experiments that failed to reveal the antidepressant effect of exercise. One study (157) reported that a sedentary program may be more beneficial to boys' moods than exercise. Another study (158) reported that 1-week high cadence cycling failed to improve depression symptoms. Methodological weaknesses, excessively severe depressive symptoms in participants, discrepancies in the mean age of the sample, imperfect exercise programs, and bias would affect the results.
Exercise can be used as a single treatment for depression (47). As a single therapy, one clinical trial (24) reported that depressive symptoms were significantly reduced in MDD patients (58%) after 8 weeks of moderate aerobic exercise, compared with 22% in the placebo group.
As a therapy to treat depression, exercise is an intervention with moderate and significant effects that can be used as an independent approach and as an adjuvant to antidepressant therapy (159). Aerobic exercise has been performed as an independent intervention and as an adjunct intervention to medication and psychotherapy (160). For patients with major depression who are resistant to medication, moderate intensity exercise as an adjunct intervention can ameliorate depressive and functional parameters (13). For MDD patients, the addition of exercise therapy to sertraline therapy was associated with a higher rate of depression relief and a significant improvement in symptoms than the sertraline-only group, with improvements observed from the end of the 4th week of exercise (161, 162). As adjunct treatments to pharmacotherapy for major depressive disorder (MDD) in older persons, the aerobic training and strength training groups showed significant reductions in depressive symptoms (treatment response = 50% decrease in the pre to post intervention assessment) through the Hamilton Depression Rating Scale and Beck Depression Inventory, compared with the control group (65). In a clinical publication (4) aiming to investigate the effects of different exercise modalities on the depression severity index and arterial stiffness, the results confirmed the positive effects of aerobic exercise as adjuvant treatment for patients with depression. In addition, the combination of exercise and sertraline treatment has a positive effect on cardiac autonomic control, reducing cardiovascular risk (163). A recent review (95) suggests that fluoxetine and running may have similar but not completely overlapping ranges of antidepressant effects and may therefore effectively complement each other to relieve depression- and anxiety-like symptoms. These findings further support the effectiveness of exercise as an adjunct to antidepressant therapy.
Cognitive behavior therapy (CBT) is one of the three major schools in the field of psychotherapy. The combination of exercise and CBT has a greater improvement for mild to moderate depression, suicidal ideation, and activities of daily living than CBT alone (16), and an exploratory randomized controlled trial reported that the combination of CBT and exercise had an anti-inflammatory effect by increasing IL-10 and reducing CRP in patients with major depression (75). The initial phase of cognitive activation allows patients to find the benefits of exercise on a psychological level and thus increase their motivation to exercise, which in turn benefits patients with depression more, making this is a benign combination. In addition, there is preliminary evidence (160) that suggests the feasibility of combining repetitive transcranial magnetic stimulation (rTMS) with aerobic exercise.
Evidence suggests that exercise programs can improve depressive symptoms and overall functioning as an adjunct to traditional therapies such as medication or psychotherapy.
Exercise therapy is believed to be equivalent to psychotherapy and medication therapy (32). A meta-analysis (159) showed that when compared with established psychotherapy (cognitive behavioral therapy, interpersonal psychotherapy, and cognitive therapy) or antidepressant treatment, there was no difference in the therapeutic effect of exercise. Another meta-analysis (164) specifically compared exercise therapy and selective serotonin reuptake inhibitor (SSRI) antidepressant treatment and found no difference in efficacy. Chronotherapy is the application of temporal pharmacology to improve efficacy and reduce adverse reactions. Exercise therapy is less effective than chronotherapy in patients with major depression (165), but both therapies are viable treatments, with depressive symptoms continuing to be improved and remitted during long-term follow-up. In addition to the comparisons between exercise therapy and traditional treatment methods such as medication and psychotherapy, there are some studies comparing exercise methods with different doses or different programs (4, 63–65, 166–173). The following information can be obtained from existing studies: The benefits of exercise therapy are comparable to traditional treatments for depression (168–170). In general, moderate intensity exercise is enough to reduce depressive symptoms, but higher doses are better for overall functioning (4, 63, 166). Mind-body exercise or aerobic exercise under supervision are recommended, and they are superior to stretching exercise and breathing exercise (30, 64, 171, 172).
Currently, an increasing number of people focus on combined depression because the prognosis of the patient is generally worse when disease is combined with depression. As a treatment for these patients, exercise has a considerable beneficial effect (174). For example, exercise reduced the depressive symptoms of cancer patients with primary lung cancer, chemotherapy cancer, and gastroesophageal junction cancer (14, 19, 107). While reducing the depressive symptoms of diabetes and other chronic diseases, exercise can also reduce cardiovascular risk factors and improve psychological status and the quality of life (36, 175). For clinical heart failure patients, exercise has obvious benefits for depressive symptoms, and the beneficial effects are consistent regardless of age, intervention duration, exercise settings, and test quality (78). In addition, exercise has a certain degree of curative effect on depressive symptoms and the overall function of patients with schizophrenia, Alzheimer's disease, Parkinson's disease, hemodialysis, arthritis, and other rheumatisms, heart transplantation, multiple sclerosis, etc. (10, 95, 140, 176–179). In prenatal and postpartum depression, exercise is an effective treatment method, which has been confirmed by several studies (82, 180). Consequently, exercise therapy has become more widely used because of its benefits to the cardiovascular system, emotional state and systemic functions. The advantages of exercise therapy are reflected when the body has contraindications to drugs.
Exercise as an optional treatment for depression can not only improve depression symptoms and reduce their severity, but also has a positive effect on the overall function of the body, cardiorespiratory fitness (45, 181), and cognitive function (24, 26). As mentioned earlier, the combination of structural physical exercise and sertraline treatment may be beneficial to the autonomous cardiac control of elderly MDD patients (163). Another large sample study (44) showed that the combination of exercise and sertraline can also improve the risk factors for coronary heart disease in patients with MDD and reduce the risk of atherosclerotic cardiovascular disease (ASCVD). In addition, exercise improves arterial stiffness (4).
Many depressed patients have persistent symptoms after taking antidepressants, such as cognitive impairment. One investigation (182) explored the effects of different doses of exercise on the cognitive function of MDD patients and concluded that the cognitive function of participants in the high-dose group [16 kcal per kg per week (KKW)] was significantly improved compared to that of the low-dose group (4 KKW). In both groups, depressive symptoms and cognitive functions in multiple areas, such as psychomotor speed, visuospatial memory, and executive function, were improved. On the other hand, a systematic meta-analysis by Sun et al. (183) reported that exercise failed to show significant effects on the overall cognitive function and individual cognitive domains of MDD patients. However, interventions that combine physical exercise with cognitive activities can significantly enhance overall cognitive function. Low-intensity exercises show a more positive effect than high-intensity exercises, which may be related to better compliance with low-intensity exercises. There is direct evidence that exercise can improve the performance of cognitive tasks such as spatial memory, pattern separation, situational fear adjustment, and new object recognition (95). The multiple beneficial effects of exercise therapy make its clinical application more valuable.
One of the first ideas that suggested exercise as a preventative and therapeutic approach to depression was proposed by Brown (184), but there were no clinical studies of exercise therapy in depression at that time. Since the 1990s, there has been a growing awareness of the link between exercise and mental health. There is also a growing body of research on the effects of exercise on physical and mental illnesses such as depression and anxiety. In 1992, an investigation confirmed that high-intensity aerobic exercise had positive effects on well-being in an adolescent population (185).
Currently, the relevance of the exercise to prevent or treat depression is well-established. However, limitations still need to be solved. Due to the heterogeneity of exercise programs and methods for evaluating curative effects selected in different studies, more high-quality studies are needed to explore standard exercise programs, the comparison of therapies, and the efficacy of combined use. Longer follow-ups are also required to determine the long-term efficacy of exercise. The mechanism of exercise treatment for depression also needs further research and exploration. A relatively large number of patients are not willing to participate in the exercise treatment because they lack motivation, and the feasibility of regular exercise training at home under less supervision has not been clarified at this time (4). The use of behavioral activation (186), mobile app support (4), and a short duration of physical activity (187) are promising tools to increase motivation and adherence to regular exercise. Group and supervised exercise patterns were more likely to increase motivation (113). Severe depression may be better treated with antidepressants as an initial therapy (5).
The World Health Organization (WHO) and the UK National Institute for Health and Clinical Excellence (NICE) guidelines recommend physical exercise as the standard complementary treatment option for depression (109). Among previous depression treatment guidelines, the suggestion proposed by NICE in 2009 recommended physical exercise as the initial treatment for mild to moderate depression (154). In Rethorst's review of the antidepressive effects of exercise, it was suggested that exercise be conducted three times a week for 45–59 min per session, lasting for 10–16 weeks (188).
Currently, clinical exercise prescriptions have not yet been widely used. The reasons why doctors do not generally prescribe exercise include lack of infrastructure (58%), belief that exercise prescriptions are not effective (50%), that patients do not follow the prescription due to habit (50%), and that patients are in poor physical condition (33%) [see questionnaires of Zanetidou et al. (25)]. After participating in the study, most doctors changed their views, with 80% of them prescribing medications for elderly patients to treat their depressive symptoms. In addition to the aforementioned questionnaire results, Murri et al. (189) also concluded the following common views: exercise has a positive effect on the body (“from the neck down”), but its effectiveness in treating the core features of depression (“from the neck up”) is not fully understood. It is believed that only strenuous exercise is effective and that exercise is harmful to the elderly. Therefore, some stereotypes hinder the large-scale application of exercise prescriptions. Currently, the beneficial effects of exercise are increasingly recognized, and more exercise is prescribed.
At present, people pay more attention to lifestyle, as a healthy lifestyle improves many disease symptoms. Exercise is expected to be popular in the clinical treatment of depression in the future, and the following points should be considered when prescribing exercises in clinical practice: on the one hand, the individual exercise program should be customized based on the patient's age, gender, exercise ability, financial ability, and value synergistically. On the other hand, the patient's personal preference should be foremost. Additionally, the exercise plan should be supervised or instructed by professionals such as physical therapists, personal trainers, and other health professionals providing regular guidance or special support.
Exercise has therapeutic effects on depression in all age groups (mostly 18–65 years old), as a single therapy, an adjuvant therapy, or combination therapy, and the benefits of exercise therapy are comparable to traditional treatments for depression. Moderate intensity exercise is enough to reduce depressive symptoms, but higher-dose exercise is better for overall functioning. Exercise therapy has become more widely used because of its benefits to the cardiovascular system, emotional state and systemic functions. Aerobic exercise/mind-body exercise (3–5 sessions per week with moderate intensity lasting for 4–16 weeks) is recommended. Individualized protocols in the form of group exercise with supervision are effective at increasing adherence to treatment.
YX, ZW, and GW participated in the design of the study, carried out the data collection, and drafted the manuscript. LS and LZ helped with the analysis. LX and HW advised on the article ideas and helped to draft the manuscript. YX and GW edited the manuscript. All authors read, edited, and approved the final manuscript.
This study was supported by the National Natural Science Foundation of China (Nos. 81871072 and 82071523) and the Medical Science Advancement Program of Wuhan University (No. TFLC2018001). Design of this study was supported by the Key research and development program of Hubei Province (2020BCA064).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
2. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. (2006) 3:e442. doi: 10.1371/journal.pmed.0030442
3. Chisholm D, Sweeny K, Sheehan P, Rasmussen B, Smit F, Cuijpers P, et al. Scaling-up treatment of depression and anxiety: a global return on investment analysis. Lancet Psychiatry. (2016) 3:415–24. doi: 10.1016/S2215-0366(16)30024-4
4. Hanssen H, Minghetti A, Faude O, Schmidt-Trucksäss A, Zahner L, Beck J, et al. Effects of endurance exercise modalities on arterial stiffness in patients suffering from unipolar depression: a randomized controlled trial. Front Psychiatry. (2017) 8:311. doi: 10.3389/fpsyt.2017.00311
5. Farah WH, Alsawas M, Mainou M, Alahdab F, Farah MH, Ahmed AT, et al. Non-pharmacological treatment of depression: a systematic review and evidence map. Evid Based Med. (2016) 21:214–21. doi: 10.1136/ebmed-2016-110522
6. Cipriani A, Furukawa TA, Salanti G, Chaimani A, Atkinson LZ, Ogawa Y, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. (2018) 391:1357–66. doi: 10.1016/S0140-6736(17)32802-7
7. Pigott HE. The STAR*D trial: it is time to reexamine the clinical beliefs that guide the treatment of major depression. Can J Psychiatry. (2015) 60:9–13. doi: 10.1177/070674371506000104
8. Riedel-Heller SG, Matschinger H, Angermeyer MC. Mental disorders–who and what might help? Help-seeking and treatment preferences of the lay public. Soc Psychiatry Psychiatr Epidemiol. (2005) 40:167–74. doi: 10.1007/s00127-005-0863-8
9. Clarke K, Mayo-Wilson E, Kenny J, Pilling S. Can non-pharmacological interventions prevent relapse in adults who have recovered from depression? a systematic review and meta-analysis of randomised controlled trials. Clin Psychol Rev. (2015) 39:58–70. doi: 10.1016/j.cpr.2015.04.002
10. Song YY, Hu RJ, Diao YS, Chen L, Jiang XL. Effects of exercise training on restless legs syndrome, depression, sleep quality, and fatigue among hemodialysis patients: a systematic review and meta-analysis. J Pain Symptom Manage. (2018) 55:1184–95. doi: 10.1016/j.jpainsymman.2017.12.472
11. Sigwalt AR, Budde H, Helmich I, Glaser V, Ghisoni K, Lanza S, et al. Molecular aspects involved in swimming exercise training reducing anhedonia in a rat model of depression. Neuroscience. (2011) 192:661–74. doi: 10.1016/j.neuroscience.2011.05.075
12. Blake H. Physical activity and exercise in the treatment of depression. Front Psychiatry. (2012) 3:106. doi: 10.3389/fpsyt.2012.00106
13. Mota-Pereira J, Silverio J, Carvalho S, Ribeiro JC, Fonte D, Ramos J. Moderate exercise improves depression parameters in treatment-resistant patients with major depressive disorder. J Psychiatr Res. (2011) 45:1005–11. doi: 10.1016/j.jpsychires.2011.02.005
14. Chen HM, Tsai CM, Wu YC, Lin KC, Lin CC. Randomised controlled trial on the effectiveness of home-based walking exercise on anxiety, depression and cancer-related symptoms in patients with lung cancer. Br J Cancer. (2015) 112:438–45. doi: 10.1038/bjc.2014.612
15. Schneider KL, Panza E, Handschin B, Ma Y, Busch AM, Waring ME, et al. Feasibility of pairing behavioral activation with exercise for women with type 2 diabetes and depression: the Get It study pilot randomized controlled trial. Behav Ther. (2016) 47:198–212. doi: 10.1016/j.beth.2015.10.005
16. Abdollahi A, LeBouthillier DM, Najafi M, Asmundson GJG, Hosseinian S, Shahidi S, et al. Effect of exercise augmentation of cognitive behavioural therapy for the treatment of suicidal ideation and depression. J Affect Disord. (2017) 219:58–63. doi: 10.1016/j.jad.2017.05.012
17. Laske C, Banschbach S, Stransky E, Bosch S, Straten G, Machann J, et al. Exercise-induced normalization of decreased BDNF serum concentration in elderly women with remitted major depression. Int J Neuropsychopharmacol. (2010) 13:595–602. doi: 10.1017/S1461145709991234
18. Liu YH, Chang CF, Hung HM, Chen CH. Outcomes of a walking exercise intervention in postpartum women with disordered sleep. J Obstet Gynaecol Res. (2021) 47:1380–7. doi: 10.1111/jog.14672
19. Midtgaard J, Stage M, Møller T, Andersen C, Quist M, Rørth M, et al. Exercise may reduce depression but not anxiety in self-referred cancer patients undergoing chemotherapy. Post-hoc analysis of data from the 'Body & Cancer' trial. Acta Oncol. (2011) 50:660–9. doi: 10.3109/0284186X.2010.543145
20. Schuch FB, Vasconcelos-Moreno MP, Borowsky C, Fleck MP. Exercise and severe depression: preliminary results of an add-on study. J Affect Disord. (2011) 133:615–8. doi: 10.1016/j.jad.2011.04.030
21. Krogh J, Rostrup E, Thomsen C, Elfving B, Videbech P, Nordentoft M. The effect of exercise on hippocampal volume and neurotrophines in patients with major depression–a randomized clinical trial. J Affect Disord. (2014) 165:24–30. doi: 10.1016/j.jad.2014.04.041
22. Danielsson L, Papoulias I, Petersson EL, Carlsson J, Waern M. Exercise or basic body awareness therapy as add-on treatment for major depression: a controlled study. J Affect Disord. (2014) 168:98–106. doi: 10.1016/j.jad.2014.06.049
23. Schuch FB, Vasconcelos-Moreno MP, Borowsky C, Zimmermann AB, Rocha NS, Fleck MP. Exercise and severe major depression: effect on symptom severity and quality of life at discharge in an inpatient cohort. J Psychiatr Res. (2015) 61:25–32. doi: 10.1016/j.jpsychires.2014.11.005
24. Olson RL, Brush CJ, Ehmann PJ, Alderman BL. A randomized trial of aerobic exercise on cognitive control in major depression. Clin Neurophysiol. (2017) 128:903–913. doi: 10.1016/j.clinph.2017.01.023
25. Zanetidou S, Murri MB, Menchetti M, Toni G, Asioli F, Bagnoli L, et al. Physical exercise for late-life depression: customizing an intervention for primary care. J Am Geriatr Soc. (2017) 65:348–55. doi: 10.1111/jgs.14525
26. Imboden C, Gerber M, Beck J, Eckert A, Pühse U, Holsboer-Trachsler E, et al. Effects of aerobic exercise as add-on treatment for inpatients with moderate to severe depression on depression severity, sleep, cognition, psychological well-being, and biomarkers: study protocol, description of study population, manipulation check. Front Psychiatry. (2019) 10:262. doi: 10.3389/fpsyt.2019.00262
27. Gujral S, Aizenstein H, Reynolds CF 3rd, Butters MA, Grove G, Karp JF, et al. Exercise for depression: a feasibility trial exploring neural mechanisms. Am J Geriatr Psychiatry. (2019) 27:611–6. doi: 10.1016/j.jagp.2019.01.012
28. Shivakumar G, Brandon AR, Snell PG, Santiago-Muñoz P, Johnson NL, Trivedi MH, et al. Antenatal depression: a rationale for studying exercise. Depress Anxiety. (2011) 28:234–42. doi: 10.1002/da.20777
29. Pfaff JJ, Alfonso H, Newton RU, Sim M, Flicker L, Almeida OP. ACTIVEDEP: a randomised, controlled trial of a home-based exercise intervention to alleviate depression in middle-aged and older adults. Br J Sports Med. (2014) 48:226–32. doi: 10.1136/bjsports-2013-092510
30. Imboden C, Gerber M, Beck J, Holsboer-Trachsler E, Pühse U, Hatzinger M. Aerobic exercise or stretching as add-on to inpatient treatment of depression: similar antidepressant effects on depressive symptoms and larger effects on working memory for aerobic exercise alone. J Affect Disord. (2020) 276:866–76. doi: 10.1016/j.jad.2020.07.052
31. Toups M, Carmody T, Greer T, Rethorst C, Grannemann B, Trivedi MH. Exercise is an effective treatment for positive valence symptoms in major depression. J Affect Disord. (2017) 209:188–94. doi: 10.1016/j.jad.2016.08.058
32. Hallgren M, Kraepelien M, Öjehagen A, Lindefors N, Zeebari Z, Kaldo V, et al. Physical exercise and internet-based cognitive-behavioural therapy in the treatment of depression: randomised controlled trial. Br J Psychiatry. (2015) 207:227–34. doi: 10.1192/bjp.bp.114.160101
33. Helgadóttir B, Hallgren M, Ekblom Ö, Forsell Y. Training fast or slow? Exercise for depression: a randomized controlled trial. Prev Med. (2016) 91:123–31. doi: 10.1016/j.ypmed.2016.08.011
34. Helgadóttir B, Forsell Y, Hallgren M, Möller J, Ekblom Ö. Long-term effects of exercise at different intensity levels on depression: a randomized controlled trial. Prev Med. (2017) 105:37–46. doi: 10.1016/j.ypmed.2017.08.008
35. Stanton R, Reaburn P. Exercise and the treatment of depression: a review of the exercise program variables. J Sci Med Sport. (2014) 17:177–82. doi: 10.1016/j.jsams.2013.03.010
36. Wang X, Pi Y, Chen B, Chen P, Liu Y, Wang R, et al. Effect of traditional Chinese exercise on the quality of life and depression for chronic diseases: a meta-analysis of randomised trials. Sci Rep. (2015) 5:15913. doi: 10.1038/srep15913
37. Zhu M, Zhang Y, Pan J, Fu C, Wang Y. Effect of simplified Tai Chi exercise on relieving symptoms of patients with mild to moderate Parkinson's disease. J Sports Med Phys Fitness. (2020) 60:282–8. doi: 10.23736/S0022-4707.19.10104-1
38. Cheung DST, Chau PH, Yeung WF, Deng W, Hong AWL, Tiwari AFY. Assessing the effect of a mind-body exercise, qigong Baduanjin, on sleep disturbance among women experiencing intimate partner violence and possible mediating factors: a randomized-controlled trial. J Clin Sleep Med. (2021) 17:993–1003. doi: 10.5664/jcsm.9102
39. Redwine LS, Pung MA, Wilson K, Bangen KJ, Delano-Wood L, Hurwitz B. An exploratory randomized sub-study of light-to-moderate intensity exercise on cognitive function, depression symptoms and inflammation in older adults with heart failure. J Psychosom Res. (2020) 128:109883. doi: 10.1016/j.jpsychores.2019.109883
40. Lu X, Liu L, Yuan R. Effect of the information support method combined with yoga exercise on the depression, anxiety, and sleep quality of menopausal women. Psychiatr Danub. (2020) 32:380–8. doi: 10.24869/psyd.2020.380
41. Ravari A, Mirzaei T, Bahremand R, Raeisi M, Kamiab Z. The effect of Pilates exercise on the happiness and depression of elderly women: a clinical trial study. J Sports Med Phys Fitness. (2021) 61:131–9. doi: 10.23736/S0022-4707.20.10730-8
42. Pascoe MC, Parker AG. Physical activity and exercise as a universal depression prevention in young people: a narrative review. Early Interv Psychiatry. (2019) 13:733–9. doi: 10.1111/eip.12737
43. Miller KJ, Gonçalves-Bradley DC, Areerob P, Hennessy D, Mesagno C, Grace F. Comparative effectiveness of three exercise types to treat clinical depression in older adults: a systematic review and network meta-analysis of randomised controlled trials. Ageing Res Rev. (2020) 58:100999. doi: 10.1016/j.arr.2019.100999
44. Sherwood A, Blumenthal JA, Smith PJ, Watkins LL, Hoffman BM, Hinderliter AL. Effects of exercise and sertraline on measures of coronary heart disease risk in patients with major depression: results from the SMILE-II randomized clinical trial. Psychosom Med. (2016) 78:602–9. doi: 10.1097/PSY.0000000000000301
45. Kerling A, Tegtbur U, Gützlaff E, Kück M, Borchert L, Ates Z, et al. Effects of adjunctive exercise on physiological and psychological parameters in depression: a randomized pilot trial. J Affect Disord. (2015) 177:1–6. doi: 10.1016/j.jad.2015.01.006
46. Balchin R, Linde J, Blackhurst D, Rauch HL, Schönbächler G. Sweating away depression? The impact of intensive exercise on depression. J Affect Disord. (2016) 200:218–21. doi: 10.1016/j.jad.2016.04.030
47. Toups MSP, Greer TL, Kurian BT, Grannemann BD, Carmody TJ, Huebinger R, et al. Effects of serum brain derived neurotrophic factor on exercise augmentation treatment of depression. J Psychiatr Res. (2011) 45:1301–6. doi: 10.1016/j.jpsychires.2011.05.002
48. Meyer JD, Koltyn KF, Stegner AJ, Kim JS, Cook DB. Influence of exercise intensity for improving depressed mood in depression: a dose-response study. Behavior Therapy. (2016) 47:527–7. doi: 10.1016/j.beth.2016.04.003
49. Heyman E, Gamelin FX, Goekint M, Piscitelli F, Roelands B, Leclair E, et al. Intense exercise increases circulating endocannabinoid and BDNF levels in humans–possible implications for reward and depression. Psychoneuroendocrinology. (2012) 37:844–51. doi: 10.1016/j.psyneuen.2011.09.017
50. Alderman BL, Olson RL, Brush CJ, Shors TJ. MAP training: combining meditation and aerobic exercise reduces depression and rumination while enhancing synchronized brain activity. Transl Psychiatry. (2016) 6:e726. doi: 10.1038/tp.2015.225
51. Stubbs B, Vancampfort D, Rosenbaum S, Ward PB, Richards J, Soundy A, et al. Dropout from exercise randomized controlled trials among people with depression: a meta-analysis and meta regression. J Affect Disord. (2016) 190:457–66. doi: 10.1016/j.jad.2015.10.019
52. Schuch FB, Deslandes AC, Stubbs B, Gosmann NP, Silva C, Fleck MPA. Factors that influence the neurobiological effects of exercise likely extend beyond age and intensity in people with major depression. Neurosci Biobehav Rev. (2017) 77:301–2. doi: 10.1016/j.neubiorev.2017.04.004
53. Nasstasia Y, Baker AL, Lewin TJ, Halpin SA, Hides L, Kelly BJ, et al. Differential treatment effects of an integrated motivational interviewing and exercise intervention on depressive symptom profiles and associated factors: a randomised controlled cross-over trial among youth with major depression. J Affect Disord. (2019) 259:413–23. doi: 10.1016/j.jad.2019.08.035
54. Hoffman BM, Babyak MA, Craighead WE, Sherwood A, Doraiswamy PM, Coons MJ, et al. Exercise and pharmacotherapy in patients with major depression: one-year follow-up of the SMILE study. Psychosom Med. (2011) 73:127–33. doi: 10.1097/PSY.0b013e31820433a5
55. Gustafsson G, Lira CM, Johansson J, Wisén A, Wohlfart B, Ekman R, et al. The acute response of plasma brain-derived neurotrophic factor as a result of exercise in major depressive disorder. Psychiatry Res. (2009) 169:244–8. doi: 10.1016/j.psychres.2008.06.030
56. Schuch FB, Vancampfort D, Richards J, Rosenbaum S, Ward PB, Stubbs B. Exercise as a treatment for depression: a meta-analysis adjusting for publication bias. J Psychiatr Res. (2016) 77:42–51. doi: 10.1016/j.jpsychires.2016.02.023
57. Blumenthal JA, Babyak MA, Craighead WE, Davidson J, Hinderliter A, Hoffman B, et al. The role of comorbid anxiety in exercise and depression trials: secondary analysis of the SMILE-II randomized clinical trial. Depress Anxiety. (2021) 38:124–33. doi: 10.1002/da.23088
58. Schmitter M, Spijker J, Smit F, Tendolkar I, Derksen AM, Oostelbos P, et al. Exercise enhances: study protocol of a randomized controlled trial on aerobic exercise as depression treatment augmentation. BMC Psychiatry. (2020) 20:585. doi: 10.1186/s12888-020-02989-z
59. Abdelbasset WK, Alqahtani BA, Alrawaili SM, Ahmed AS, Elnegamy TE, Ibrahim AA, et al. Similar effects of low to moderate-intensity exercise program vs moderate-intensity continuous exercise program on depressive disorder in heart failure patients: a 12-week randomized controlled trial. Medicine. (2019) 98:e16820. doi: 10.1097/MD.0000000000016820
60. Özkan SA, Kücükkelepce DS, Korkmaz B, Yilmaz G, Bozkurt MA. The effectiveness of an exercise intervention in reducing the severity of postpartum depression: a randomized controlled trial. Perspect Psychiatr Care. (2020) 56:844–50. doi: 10.1111/ppc.12500
61. Liu X, Williams G, Kostner K, Brown WJ. The effect of Tai Chi on quality of life in centrally obese adults with depression. J Altern Complement Med. (2019) 25:1005–8. doi: 10.1089/acm.2019.0050
62. Streeter CC, Gerbarg PL, Brown RP, Scott TM, Nielsen GH, Owen L, et al. Thalamic gamma aminobutyric acid level changes in major depressive disorder after a 12-week iyengar yoga and coherent breathing intervention. J Altern Complement Med. (2020) 26:190–7. doi: 10.1089/acm.2019.0234
63. Scott TM, Gerbarg PL, Silveri MM, Nielsen GH, Owen L, Nyer M, et al. Psychological function, iyengar yoga, and coherent breathing: a randomized controlled dosing study. J Psychiatr Pract. (2019) 25:437–50. doi: 10.1097/PRA.0000000000000435
64. Haussleiter IS, Bolsinger B, Assion HJ, Juckel G. Adjuvant guided exercise therapy versus self-organized activity in patients with major depression. J Nerv Ment Dis. (2020) 208:982–8. doi: 10.1097/NMD.0000000000001240
65. Moraes HS, Silveira HS, Oliveira NA, Matta Mello Portugal E, Araújo NB, Vasques PE, et al. Is strength training as effective as aerobic training for depression in older adults? a randomized controlled trial. Neuropsychobiology. (2020) 79:141–9. doi: 10.1159/000503750
66. Zeibig JM, Seiffer B, Sudeck G, Rösel I, Hautzinger M, Wolf S. Transdiagnostic efficacy of a group exercise intervention for outpatients with heterogenous psychiatric disorders: a randomized controlled trial. BMC Psychiatry. (2021) 21:313. doi: 10.1186/s12888-021-03307-x
67. Gökşin I, Aşiret GD. The effect of progressive muscle relaxation on the adaptation of elderly women to depression and old age: a randomised clinical trial. Psychogeriatrics. (2021) 21:333–41. doi: 10.1111/psyg.12673
68. Tang Y, Jiang J, Shen P, Li M, You H, Liu C, et al. Liuzijue is a promising exercise option for rehabilitating discharged COVID-19 patients. Medicine. (2021) 100:e24564. doi: 10.1097/MD.0000000000024564
69. Izquierdo-Alventosa R, Inglés M, Cortés-Amador S, Gimeno-Mallench L, Chirivella-Garrido J, Kropotov J, et al. Low-intensity physical exercise improves pain catastrophizing and other psychological and physical aspects in women with fibromyalgia: a randomized controlled trial. Int J Environ Res Public Health. (2020) 17:3634. doi: 10.3390/ijerph17103634
70. Kiuchi T, Lee H, Mikami T. Regular exercise cures depression-like behavior via VEGF-Flk-1 signaling in chronically stressed mice. Neuroscience. (2012) 207:208–17. doi: 10.1016/j.neuroscience.2012.01.023
71. Erickson KI, Miller DL, Roecklein KA. The aging hippocampus: interactions between exercise, depression, and BDNF. Neuroscientist. (2012) 18:82–97. doi: 10.1177/1073858410397054
72. Liu IT, Lee WJ, Lin SY, Chang ST, Kao CL, Cheng YY. Therapeutic effects of exercise training on elderly patients with dementia: a randomized controlled trial. Arch Phys Med Rehabil. (2020) 101:762–9. doi: 10.1016/j.apmr.2020.01.012
73. Kim TK, Lee JE, Kim JE, Park JY, Choi J, Kim H, et al. G9a-mediated regulation of OXT and AVP expression in the basolateral amygdala mediates stress-Induced lasting behavioral depression and its reversal by exercise. Mol Neurobiol. (2016) 53:2843–56. doi: 10.1007/s12035-015-9160-z
74. Lopresti AL, Hood SD, Drummond PD. A review of lifestyle factors that contribute to important pathways associated with major depression: diet, sleep and exercise. J Affect Disord. (2013) 148:12–27. doi: 10.1016/j.jad.2013.01.014
75. Euteneuer F, Dannehl K, Del Rey A, Engler H, Schedlowski M, Rief W. Immunological effects of behavioral activation with exercise in major depression: an exploratory randomized controlled trial. Transl Psychiatry. (2017) 7:e1132. doi: 10.1038/tp.2017.76
76. Ventura J, McEwen S, Subotnik KL, Hellemann GS, Ghadiali M, Rahimdel A, et al. Changes in inflammation are related to depression and amount of aerobic exercise in first episode schizophrenia. Early Interv Psychiatry. (2020) 15:213–16. doi: 10.1111/eip.12946
77. Liu W, Xue X, Xia J, Liu J, Qi Z. Swimming exercise reverses CUMS-induced changes in depression-like behaviors and hippocampal plasticity-related proteins. J Affect Disord. (2018) 227:126–35. doi: 10.1016/j.jad.2017.10.019
78. Tu RH, Zeng ZY, Zhong GQ, Wu WF, Lu YJ, Bo ZD, et al. Effects of exercise training on depression in patients with heart failure: a systematic review and meta-analysis of randomized controlled trials. Eur J Heart Fail. (2014) 16:749–57. doi: 10.1002/ejhf.101
79. Danielsson L, Kihlbom B, Rosberg S. “Crawling out of the cocoon”: patients' experiences of a physical therapy exercise intervention in the treatment of major depression. Phys Ther. (2016) 96:1241–50. doi: 10.2522/ptj.20150076
80. Schuch FB, Dunn AL, Kanitz AC, Delevatti RS, Fleck MP. Moderators of response in exercise treatment for depression: a systematic review. J Affect Disorders. (2016) 195:40–9. doi: 10.1016/j.jad.2016.01.014
81. Kandola A, Ashdown-Franks G, Hendrikse J, Sabiston CM, Stubbs B. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev. (2019) 107:525–39. doi: 10.1016/j.neubiorev.2019.09.040
82. Daley AJ, Blamey RV, Jolly K, Roalfe AK, Turner KM, Coleman S, et al. A pragmatic randomized controlled trial to evaluate the effectiveness of a facilitated exercise intervention as a treatment for postnatal depression: the PAM-PeRS trial. Psychol Med. (2015) 45:2413–25. doi: 10.1017/S0033291715000409
83. Yirmiya R, Rimmerman N, Reshef R. Depression as a microglial disease. Trends Neurosci. (2015) 38:637–58. doi: 10.1016/j.tins.2015.08.001
84. Bassett B, Subramaniyam S, Fan Y, Varney S, Pan H, Carneiro AMD, et al. Minocycline alleviates depression-like symptoms by rescuing decrease in neurogenesis in dorsal hippocampus via blocking microglia activation/phagocytosis. Brain Behav Immun. (2021) 91:519–30. doi: 10.1016/j.bbi.2020.11.009
85. Stein DJ, Vasconcelos MF, Albrechet-Souza L, Ceresér KMM, de Almeida RMM. Microglial over-activation by social defeat stress contributes to anxiety- and depressive-like behaviors. Front Behav Neurosci. (2017) 11:207. doi: 10.3389/fnbeh.2017.00207
86. Kim TK, Kim JE, Choi J, Park JY, Lee JE, Lee EH, et al. Local Interleukin-18 system in the basolateral amygdala regulates susceptibility to chronic stress. Mol Neurobiol. (2017) 54:5347–58. doi: 10.1007/s12035-016-0052-7
87. Jin C, Flavell RA. Molecular mechanism of NLRP3 inflammasome activation. J Clin Immunol. (2010) 30:628–31. doi: 10.1007/s10875-010-9440-3
88. Yue N, Huang H, Zhu X, Han Q, Wang Y, Li B, et al. Activation of P2X7 receptor and NLRP3 inflammasome assembly in hippocampal glial cells mediates chronic stress-induced depressive-like behaviors. J Neuroinflammation. (2017) 14:102. doi: 10.1186/s12974-017-0865-y
89. Reddy VS, Harskamp RE, van Ginkel MW, Calhoon J, Baisden CE, Kim IS. Interleukin-18 stimulates fibronectin expression in primary human cardiac fibroblasts via PI3K-Akt-dependent NF-kappaB activation. J Cell Physiol. (2008) 215:697–707. doi: 10.1002/jcp.21348
90. Boucher D, Monteleone M, Coll RC, Chen KW, Ross CM, Teo JL, et al. Caspase-1 self-cleavage is an intrinsic mechanism to terminate inflammasome activity. J Exp Med. (2018) 215:827–40. doi: 10.1084/jem.20172222
91. Luca M, Luca A. Oxidative stress-related endothelial damage in vascular depression and vascular cognitive impairment: beneficial effects of aerobic physical exercise. Oxidative Med Cell Longevity. (2019) 2019:1–6. doi: 10.1155/2019/8067045
92. Brocardo PS, Boehme F, Patten A, Cox A, Gil-Mohapel J, Christie BR. Anxiety- and depression-like behaviors are accompanied by an increase in oxidative stress in a rat model of fetal alcohol spectrum disorders: protective effects of voluntary physical exercise. Neuropharmacology. (2012) 62:1607–18. doi: 10.1016/j.neuropharm.2011.10.006
93. Meziat C, Boulghobra D, Strock E, Battault S, Bornard I, Walther G, et al. Exercise training restores eNOS activation in the perivascular adipose tissue of obese rats: impact on vascular function. Nitric Oxide. (2019) 86:63–7. doi: 10.1016/j.niox.2019.02.009
94. Silva LAD, Tortelli L, Motta J, Menguer L, Mariano S, Tasca G, et al. Effects of aquatic exercise on mental health, functional autonomy and oxidative stress in depressed elderly individuals: a randomized clinical trial. Clinics. (2019) 74:e322. doi: 10.6061/clinics/2019/e322
95. Micheli L, Ceccarelli M, D'Andrea G, Tirone F. Depression and adult neurogenesis: positive effects of the antidepressant fluoxetine and of physical exercise. Brain Res Bull. (2018) 143:181–93. doi: 10.1016/j.brainresbull.2018.09.002
96. Ma CL, Ma XT, Wang JJ, Liu H, Chen YF, Yang Y. Physical exercise induces hippocampal neurogenesis and prevents cognitive decline. Behav Brain Res. (2017) 317:332–9. doi: 10.1016/j.bbr.2016.09.067
97. Lucassen PJ, Meerlo P, Naylor AS, van Dam AM, Dayer AG, Fuchs E, et al. Regulation of adult neurogenesis by stress, sleep disruption, exercise and inflammation: implications for depression and antidepressant action. Neuropsychopharmacology. (2010) 20:1–17. doi: 10.1016/j.euroneuro.2009.08.003
98. Tang J, Liang X, Zhang Y, Chen L, Wang F, Tan C, et al. The effects of running exercise on oligodendrocytes in the hippocampus of rats with depression induced by chronic unpredictable stress. Brain Rese Bull. (2019) 149:1–10. doi: 10.1016/j.brainresbull.2019.04.001
99. Szuhany KL, Otto MW. Assessing BDNF as a mediator of the effects of exercise on depression. J Psychiatr Res. (2020) 123:114–8. doi: 10.1016/j.jpsychires.2020.02.003
100. Sacheli MA, Neva JL, Lakhani B, Murray DK, Vafai N, Shahinfard E, et al. Exercise increases caudate dopamine release and ventral striatal activation in Parkinson's disease. Mov Disord. (2019) 34:1891–900. doi: 10.1002/mds.27865
101. Gujral S, Aizenstein H, Reynolds CF 3rd, Butters MA, Erickson KI. Exercise effects on depression: possible neural mechanisms. Gen Hosp Psychiatry. (2017) 49:2–10. doi: 10.1016/j.genhosppsych.2017.04.012
102. Lin K, Stubbs B, Zou W, Zheng W, Lu W, Gao Y, et al. Aerobic exercise impacts the anterior cingulate cortex in adolescents with subthreshold mood syndromes: a randomized controlled trial study. Transl Psychiatry. (2020) 10:155. doi: 10.1038/s41398-020-0840-8
103. Wu T, Huang Y, Gong Y, Xu Y, Lu J, Sheng H, et al. Treadmill exercise ameliorates depression-like behavior in the rats with prenatal dexamethasone exposure: the role of hippocampal mitochondria. Front Neurosci. (2019) 13:264. doi: 10.3389/fnins.2019.00264
104. Eyre H, Baune BT. Neuroimmunological effects of physical exercise in depression. Brain Behav Immun. (2012) 26:251–66. doi: 10.1016/j.bbi.2011.09.015
105. Kraemer WJ, Ratamess NA. Hormonal responses and adaptations to resistance exercise and training. Sports Med. (2005) 35:339–61. doi: 10.2165/00007256-200535040-00004
106. Notarangelo FM, Pocivavsek A, Schwarcz R. Exercise your kynurenines to fight depression. Trends Neurosci. (2018) 41:491–3. doi: 10.1016/j.tins.2018.05.010
107. Herrstedt A, Bay ML, Simonsen C, Sundberg A, Egeland C, Thorsen-Streit S, et al. Exercise-mediated improvement of depression in patients with gastro-esophageal junction cancer is linked to kynurenine metabolism. Acta Oncol. (2019) 58:579–87. doi: 10.1080/0284186X.2018.1558371
108. Allison DJ, Nederveen JP, Snijders T, Bell KE, Kumbhare D, Phillips SM, et al. Exercise training impacts skeletal muscle gene expression related to the kynurenine pathway. Am J Physiol Cell Physiol. (2019) 316:C444–8. doi: 10.1152/ajpcell.00448.2018
109. Nebiker L, Lichtenstein E, Minghetti A, Zahner L, Gerber M, Faude O, et al. Moderating effects of exercise duration and intensity in neuromuscular vs. endurance exercise interventions for the treatment of depression: a meta-analytical review. Front Psychiatry. (2018) 9:305. doi: 10.3389/fpsyt.2018.00305
110. Broberg L, Tabor A, Rosthøj S, Backhausen M, Frokjaer VG, Damm P, et al. Effect of supervised group exercise on psychological well-being among pregnant women with or at high risk of depression (the EWE Study): a randomized controlled trial. Acta Obstet Gynecol Scand. (2021) 100:129–38. doi: 10.1111/aogs.13982
111. Aguiar LT, Nadeau S, Britto RR, Teixeira-Salmela LF, Martins JC, Samora GAR, et al. Effects of aerobic training on physical activity in people with stroke: a randomized controlled trial. NeuroRehabilitation. (2020) 46:391–401. doi: 10.3233/NRE-193013
112. McIntyre KM, Puterman E, Scodes JM, Choo TH, Choi CJ, Pavlicova M, et al. The effects of aerobic training on subclinical negative affect: a randomized controlled trial. Health Psychol. (2020) 39:255–64. doi: 10.1037/hea0000836
113. Ryu J, Jung JH, Kim J, Kim CH, Lee HB, Kim DH, et al. Outdoor cycling improves clinical symptoms, cognition and objectively measured physical activity in patients with schizophrenia: a randomized controlled trial. J Psychiatr Res. (2020) 120:144–53. doi: 10.1016/j.jpsychires.2019.10.015
114. Norouzi E, Hosseini F, Vaezmosavi M, Gerber M, Pühse U, Brand S. Zumba dancing and aerobic exercise can improve working memory, motor function, and depressive symptoms in female patients with Fibromyalgia. Eur J Sport Sci. (2020) 20:981–91. doi: 10.1080/17461391.2019.1683610
115. Lederman O, Ward PB, Rosenbaum S, Maloney C, Watkins A, Teasdale S, et al. Stepping up early treatment for help-seeking youth with at-risk mental states: feasibility and acceptability of a real-world exercise program. Early Interv Psychiatry. (2020) 14:450–62. doi: 10.1111/eip.12871
116. Kogure GS, Lopes IP, Ribeiro VB, Mendes MC, Kodato S, Furtado CLM, et al. The effects of aerobic physical exercises on body image among women with polycystic ovary syndrome. J Affect Disord. (2020) 262:350–8. doi: 10.1016/j.jad.2019.11.025
117. Lin FL, Yeh ML, Lai YH, Lin KC, Yu CJ, Chang JS. Two-month breathing-based walking improves anxiety, depression, dyspnoea and quality of life in chronic obstructive pulmonary disease: a randomised controlled study. J Clin Nurs. (2019) 28:3632–40. doi: 10.1111/jocn.14960
118. Abdelbasset WK, Alqahtani BA, Elshehawy AA, Tantawy SA, Elnegamy TE, Kamel DM. Examining the impacts of 12 weeks of low to moderate-intensity aerobic exercise on depression status in patients with systolic congestive heart failure - a randomized controlled study. Clinics. (2019) 74:e1017. doi: 10.6061/clinics/2019/e1017
119. Al-Sharman A, Khalil H, El-Salem K, Aldughmi M, Aburub A. The effects of aerobic exercise on sleep quality measures and sleep-related biomarkers in individuals with multiple sclerosis: a pilot randomised controlled trial. NeuroRehabilitation. (2019) 45:107–15. doi: 10.3233/NRE-192748
120. Kong Z, Sze TM, Yu JJ, Loprinzi PD, Xiao T, Yeung AS, et al. Tai Chi as an alternative exercise to improve physical fitness for children and adolescents with intellectual disability. Int J Environ Res Public Health. (2019) 16:1152. doi: 10.3390/ijerph16071152
121. Kucharski D, Lange E, Ross AB, Svedlund S, Feldthusen C, Önnheim K, et al. Moderate-to-high intensity exercise with person-centered guidance influences fatigue in older adults with rheumatoid arthritis. Rheumatol Int. (2019) 39:1585–94. doi: 10.1007/s00296-019-04384-8
122. Huang HP, Wen FH, Yang TY, Lin YC, Tsai JC, Shun SC, et al. The effect of a 12-week home-based walking program on reducing fatigue in women with breast cancer undergoing chemotherapy: a randomized controlled study. Int J Nurs Stud. (2019) 99:103376. doi: 10.1016/j.ijnurstu.2019.06.007
123. Murawski B, Plotnikoff RC, Rayward AT, Oldmeadow C, Vandelanotte C, Brown WJ, et al. Efficacy of an m-health physical activity and sleep health intervention for adults: a randomized waitlist-controlled trial. Am J Prev Med. (2019) 57:503–14. doi: 10.1016/j.amepre.2019.05.009
124. Tollár J, Nagy F, Moizs M, Tóth BE, Sanders LMJ, Hortobágyi T. Diverse exercises similarly reduce older adults' mobility limitations. Med Sci Sports Exerc. (2019) 51:1809–16. doi: 10.1249/MSS.0000000000002001
125. Saltan A, Ankarali H. Does pilates effect on depression status, pain, functionality, and quality of life in university students? A randomized controlled study. Perspect Psychiatr Care. (2021) 57:198–205. doi: 10.1111/ppc.12547
126. Huberty J, Sullivan M, Green J, Kurka J, Leiferman J, Gold K, et al. Online yoga to reduce post traumatic stress in women who have experienced stillbirth: a randomized control feasibility trial. BMC Complement Med Ther. (2020) 20:173. doi: 10.1186/s12906-020-02926-3
127. Huberty J, Eckert R, Dueck A, Kosiorek H, Larkey L, Gowin K, et al. Online yoga in myeloproliferative neoplasm patients: results of a randomized pilot trial to inform future research. BMC Complement Altern Med. (2019) 19:121. doi: 10.1186/s12906-019-2530-8
128. Cetin SY, Calik BB, Ayan A. Investigation of the effectiveness of Tai Chi exercise program in patients with scleroderma: a randomized controlled study. Complement Ther Clin Pract. (2020) 40:101181. doi: 10.1016/j.ctcp.2020.101181
129. Moon S, Sarmento CVM, Steinbacher M, Smirnova IV, Colgrove Y, Lai SM, et al. Can Qigong improve non-motor symptoms in people with Parkinson's disease - a pilot randomized controlled trial? Complement Ther Clin Pract. (2020) 39:101169. doi: 10.1016/j.ctcp.2020.101169
130. Quigley A, Brouillette MJ, Gahagan J, O'Brien KK, MacKay-Lyons M. Feasibility and impact of a yoga intervention on cognition, physical function, physical activity, and affective outcomes among people living with hiv: a randomized controlled pilot trial. J Int Assoc Provid AIDS Care. (2020) 19:2325958220935698. doi: 10.1177/2325958220935698
131. Jiao J, Russell IJ, Wang W, Wang J, Zhao YY, Jiang Q. Ba-Duan-Jin alleviates pain and fibromyalgia-related symptoms in patients with fibromyalgia: results of a randomised controlled trial. Clin Exp Rheumatol. (2019) 37:953–962.
132. Sharma KNS, Pailoor S, Choudhary NR, Bhat P, Shrestha S. Integrated yoga practice in cardiac rehabilitation program: a randomized control trial. J Altern Complement Med. (2020) 26:918–27. doi: 10.1089/acm.2019.0250
133. Lundt A, Jentschke E. Long-term changes of symptoms of anxiety, depression, and fatigue in cancer patients 6 months after the end of yoga therapy. Integr Cancer Ther. (2019) 18:1534735418822096. doi: 10.1177/1534735418822096
134. Aibar-Almazán A, Hita-Contreras F, Cruz-Díaz D, de la Torre-Cruz M, Jiménez-García JD, Martínez-Amat A. Effects of pilates training on sleep quality, anxiety, depression and fatigue in postmenopausal women: a randomized controlled trial. Maturitas. (2019) 124:62–7. doi: 10.1016/j.maturitas.2019.03.019
135. Papp ME, Nygren-Bonnier M, Gullstrand L, Wändell PE, Lindfors P. A randomized controlled pilot study of the effects of 6-week high intensity hatha yoga protocol on health-related outcomes among students. J Bodyw Mov Ther. (2019) 23:766–72. doi: 10.1016/j.jbmt.2019.05.013
136. Chen CH, Hung KS, Chung YC, Yeh ML. Mind-body interactive qigong improves physical and mental aspects of quality of life in inpatients with stroke: a randomized control study. Eur J Cardiovasc Nurs. (2019) 18:658–66. doi: 10.1177/1474515119860232
137. Whitworth JW, Nosrat S, SantaBarbara NJ, Ciccolo JT. Feasibility of resistance exercise for posttraumatic stress and anxiety symptoms: a randomized controlled pilot study. J Trauma Stress. (2019) 32:977–84. doi: 10.1002/jts.22464
138. de Lima TA, Ferreira-Moraes R, Alves W, Alves TGG, Pimentel CP, Sousa EC, et al. Resistance training reduces depressive symptoms in elderly people with Parkinson disease: a controlled randomized study. Scand J Med Sci Sports. (2019) 29:1957–67. doi: 10.1111/sms.13528
139. Sadeghi Bahmani D, Razazian N, Farnia V, Alikhani M, Tatari F, Brand S. Compared to an active control condition, in persons with multiple sclerosis two different types of exercise training improved sleep and depression, but not fatigue, paresthesia, and intolerance of uncertainty. Mult Scler Relat Disord. (2019) 36:101356. doi: 10.1016/j.msard.2019.07.032
140. Sadeghi Bahmani D, Kesselring J, Papadimitriou M, Bansi J, Pühse U, Gerber M, et al. In Patients with multiple sclerosis, both objective and subjective sleep, depression, fatigue, and paresthesia improved after 3 weeks of regular exercise. Front Psychiatry. (2019) 10:265. doi: 10.3389/fpsyt.2019.00265
141. Campo G, Tonet E, Chiaranda G, Sella G, Maietti E, Bugani G, et al. Exercise intervention improves quality of life in older adults after myocardial infarction: randomised clinical trial. Heart. (2020) 106:1658–64. doi: 10.1136/heartjnl-2019-316349
142. Quist M, Langer SW, Lillelund C, Winther L, Laursen JH, Christensen KB, et al. Effects of an exercise intervention for patients with advanced inoperable lung cancer undergoing chemotherapy: a randomized clinical trial. Lung Cancer. (2020) 145:76–82. doi: 10.1016/j.lungcan.2020.05.003
143. Ozkul C, Guclu-Gunduz A, Eldemir K, Apaydin Y, Yazici G, Irkec C. Combined exercise training improves cognitive functions in multiple sclerosis patients with cognitive impairment: a single-blinded randomized controlled trial. Mult Scler Relat Disord. (2020) 45:102419. doi: 10.1016/j.msard.2020.102419
144. Oliveira VHF, Rosa FT, Santos JC, Wiechmann SL, Narciso AMS, Franzoi de Moraes SM, et al. Effects of a combined exercise training program on health indicators and quality of life of people living with hiv: a randomized clinical trial. AIDS Behav. (2020) 24:1531–41. doi: 10.1007/s10461-019-02678-3
145. Hall KS, Morey MC, Bosworth HB, Beckham JC, Pebole MM, Sloane R, et al. Pilot randomized controlled trial of exercise training for older veterans with PTSD. J Behav Med. (2020) 43:648–59. doi: 10.1007/s10865-019-00073-w
146. Rhee SY, Song JK, Hong SC, Choi JW, Jeon HJ, Shin DH, et al. Intradialytic exercise improves physical function and reduces intradialytic hypotension and depression in hemodialysis patients. Korean J Intern Med. (2019) 34:588–98. doi: 10.3904/kjim.2017.020
147. Soriano-Maldonado A, Carrera-Ruiz Á, Díez-Fernández DM, Esteban-Simón A, Maldonado-Quesada M, Moreno-Poza N, et al. Effects of a 12-week resistance and aerobic exercise program on muscular strength and quality of life in breast cancer survivors: study protocol for the EFICAN randomized controlled trial. Medicine. (2019) 98:e17625. doi: 10.1097/MD.0000000000017625
148. Samuel SR, Maiya AG, Fernandes DJ, Guddattu V, Saxena PUP, Kurian JR, et al. Effectiveness of exercise-based rehabilitation on functional capacity and quality of life in head and neck cancer patients receiving chemo-radiotherapy. Support Care Cancer. (2019) 27:3913–20. doi: 10.1007/s00520-019-04750-z
149. Penttinen H, Utriainen M, Kellokumpu-Lehtinen PL, Raitanen J, Sievänen H, Nikander R, et al. Effectiveness of a 12-month exercise intervention on physical activity and quality of life of breast cancer survivors; five-year results of the BREX-study. In Vivo. (2019) 33:881–8. doi: 10.21873/invivo.11554
150. Yildiz Kabak V, Cetinkaya DU, Kuskonmaz B, Cetin N, Duger T. Effects of multimodal exercise on clinical status and patient-reported outcomes in children undergoing hematopoietic stem cell transplantation. Pediatr Hematol Oncol. (2019) 36:410–21. doi: 10.1080/08880018.2019.1648619
151. Apóstolo J, Dixe MDA, Bobrowicz-Campos E, Areosa T, Santos-Rocha R, Braúna M, et al. Effectiveness of a combined intervention on psychological and physical capacities of frail older adults: a cluster randomized controlled trial. Int J Environ Res Public Health. (2019) 16:3125. doi: 10.3390/ijerph16173125
152. Klil-Drori S, Klil-Drori AJ, Pira S, Rej S. Exercise intervention for late-life depression: a meta-analysis. J Clin Psychiatry. (2020) 81:19r12877. doi: 10.4088/JCP.19r12877
153. Underwood M, Lamb SE, Eldridge S, Sheehan B, Slowther AM, Spencer A, et al. Exercise for depression in elderly residents of care homes: a cluster-randomised controlled trial. Lancet. (2013) 382:41–9. doi: 10.1016/S0140-6736(13)60649-2
154. Brondino N, Rocchetti M, Fusar-Poli L, Codrons E, Correale L, Vandoni M, et al. A systematic review of cognitive effects of exercise in depression. Acta Psychiatr Scand. (2017) 135:285–95. doi: 10.1111/acps.12690
155. Matthews J, Torres SJ, Milte CM, Hopkins I, Kukuljan S, Nowson CA, et al. Effects of a multicomponent exercise program combined with calcium-vitamin D(3)-enriched milk on health-related quality of life and depressive symptoms in older men: secondary analysis of a randomized controlled trial. Eur J Nutr. (2020) 59:1081–91. doi: 10.1007/s00394-019-01969-8
156. Chalder M, Wiles NJ, Campbell J, Hollinghurst SP, Haase AM, Taylor AH, et al. Facilitated physical activity as a treatment for depressed adults: randomised controlled trial. BMJ. (2012) 344:e2758. doi: 10.1136/bmj.e2758
157. Williams CF, Bustamante EE, Waller JL, Davis CL. Exercise effects on quality of life, mood, and self-worth in overweight children: the SMART randomized controlled trial. Transl Behav Med. (2019) 9:451–9. doi: 10.1093/tbm/ibz015
158. Harper SA, Dowdell BT, Kim JH, Pollock BS, Ridgel AL. Non-motor symptoms after one week of high cadence cycling in parkinson's disease. Int J Environ Res Public Health. (2019) 16: 2104. doi: 10.3390/ijerph16122104
159. Kvam S, Kleppe CL, Nordhus IH, Hovland A. Exercise as a treatment for depression: a meta-analysis. J Affect Disord. (2016) 202:67–86. doi: 10.1016/j.jad.2016.03.063
160. Ross RE, VanDerwerker CJ, Newton JH, George MS, Short EB, Sahlem GL, et al. Simultaneous aerobic exercise and rTMS: feasibility of combining therapeutic modalities to treat depression. Brain Stimul. (2018) 11:245–6. doi: 10.1016/j.brs.2017.10.019
161. Murri MB, Amore M, Menchetti M, Toni G, Neviani F, Cerri M, et al. Physical exercise for late-life major depression. Br J Psychiatry. (2015) 207:235–42. doi: 10.1192/bjp.bp.114.150516
162. Murri MB, Ekkekakis P, Menchetti M, Neviani F, Trevisani F, Tedeschi S, et al. Physical exercise for late-life depression: effects on symptom dimensions and time course. J Affect Disord. (2018) 230:65–70. doi: 10.1016/j.jad.2018.01.004
163. Toni G, Murri MB, Piepoli M, Zanetidou S, Cabassi A, Squatrito S, et al. Physical exercise for late-Life depression: effects on heart rate variability. Am J Geriatr Psychiatry. (2016) 24:989–97. doi: 10.1016/j.jagp.2016.08.005
164. Samartzis L, Dimopoulos S, Tziongourou M, Koroboki E, Kyprianou T, Nanas S. SSRIs versus exercise training for depression in chronic heart failure: a meta-analysis of randomized controlled trials. Int J Cardiol. (2013) 168:4956–8. doi: 10.1016/j.ijcard.2013.07.143
165. Martiny K, Refsgaard E, Lund V, Lunde M, Thougaard B, Lindberg L, et al. Maintained superiority of chronotherapeutics vs. exercise in a 20-week randomized follow-up trial in major depression. Acta Psychiatr Scand. (2015) 131:446–57. doi: 10.1111/acps.12402
166. Plag J, Schmidt-Hellinger P, Klippstein T, Mumm JLM, Wolfarth B, Petzold MB, et al. Working out the worries: a randomized controlled trial of high intensity interval training in generalized anxiety disorder. J Anxiety Disord. (2020) 76:102311. doi: 10.1016/j.janxdis.2020.102311
167. Rolid K, Andreassen AK, Yardley M, Gude E, Bjørkelund E, Authen AR, et al. High-intensity interval training and health-related quality of life in de novo heart transplant recipients - results from a randomized controlled trial. Health Qual Life Outcomes. (2020) 18:283. doi: 10.1186/s12955-020-01536-4
168. Otones P, García E, Sanz T, Pedraz A. A physical activity program versus usual care in the management of quality of life for pre-frail older adults with chronic pain: randomized controlled trial. BMC Geriatr. (2020) 20:396. doi: 10.1186/s12877-020-01805-3
169. Hallgren M, Helgadóttir B, Herring MP, Zeebari Z, Lindefors N, Kaldo V, et al. Exercise and internet-based cognitive-behavioural therapy for depression: multicentre randomised controlled trial with 12-month follow-up. Br J Psychiatry. (2016) 209:414–20. doi: 10.1192/bjp.bp.115.177576
170. Redwine LS, Wilson K, Pung MA, Chinh K, Rutledge T, Mills PJ, et al. A randomized study examining the effects of mild-to-moderate group exercises on cardiovascular, physical, and psychological well-being in patients with heart failure. J Cardiopulm Rehabil Prev. (2019) 39:403–8. doi: 10.1097/HCR.0000000000000430
171. Kwok JYY, Kwan JCY, Auyeung M, Mok VCT, Lau CKY, Choi KC, et al. Effects of mindfulness yoga vs stretching and resistance training exercises on anxiety and depression for people with parkinson disease: a randomized clinical trial. JAMA Neurol. (2019) 76:755–63. doi: 10.1001/jamaneurol.2019.0534
172. Evaristo KB, Mendes FAR, Saccomani MG, Cukier A, Carvalho-Pinto RM, Rodrigues MR, et al. Effects of aerobic training versus breathing exercises on asthma control: a randomized trial. J Allergy Clin Immunol Pract. (2020) 8:2989–96.e4. doi: 10.1016/j.jaip.2020.06.042
173. Schönfelder M, Oberreiter H, Egger A, Tschentscher M, Droese S, Niebauer J. Effect of different endurance training protocols during cardiac rehabilitation on quality of life. Am J Med. (2021) 134:805–11. doi: 10.1016/j.amjmed.2020.10.048
174. Rozanski A. Exercise as medical treatment for depression. J Am Coll Cardiol. (2012) 60:1064–6. doi: 10.1016/j.jacc.2012.05.015
175. de Groot M, Doyle T, Kushnick M, Shubrook J, Merrill J, Rabideau E, et al. Can lifestyle interventions do more than reduce diabetes risk? Treating depression in adults with type 2 diabetes with exercise and cognitive behavioral therapy. Curr Diab Rep. (2012) 12:157–66. doi: 10.1007/s11892-012-0261-z
176. Kelley GA, Kelley KS, Hootman JM. Effects of exercise on depression in adults with arthritis: a systematic review with meta-analysis of randomized controlled trials. Arthritis Res Ther. (2015) 17:21. doi: 10.1186/s13075-015-0533-5
177. Christensen SB, Dall CH, Prescott E, Pedersen SS, Gustafsson F. A high-intensity exercise program improves exercise capacity, self-perceived health, anxiety and depression in heart transplant recipients: a randomized, controlled trial. J Heart Lung Transplant. (2012) 31:106–7. doi: 10.1016/j.healun.2011.10.014
178. Dauwan M, Begemann MJ, Heringa SM, Sommer IE. Exercise improves clinical symptoms, quality of life, global functioning, and depression in schizophrenia: a systematic review and meta-analysis. Schizophr Bull. (2016) 42:588–99. doi: 10.1093/schbul/sbv164
179. Roeh A, Kirchner SK, Malchow B, Maurus I, Schmitt A, Falkai P, et al. Depression in somatic disorders: is there a beneficial effect of exercise? Front Psychiatry. (2019) 10:141. doi: 10.3389/fpsyt.2019.00141
180. Daley AJ, Foster L, Long G, Palmer C, Robinson O, Walmsley H, et al. The effectiveness of exercise for the prevention and treatment of antenatal depression: systematic review with meta-analysis. BJOG. (2015) 122:57–62. doi: 10.1111/1471-0528.12909
181. Stubbs B, Rosenbaum S, Vancampfort D, Ward PB, Schuch FB. Exercise improves cardiorespiratory fitness in people with depression: a meta-analysis of randomized control trials. J Affect Disord. (2016) 190:249–53. doi: 10.1016/j.jad.2015.10.010
182. Greer TL, Grannemann BD, Chansard M, Karim AI, Trivedi MH. Dose-dependent changes in cognitive function with exercise augmentation for major depression: results from the TREAD study. Eur Neuropsychopharmacol. (2015) 25:248–56. doi: 10.1016/j.euroneuro.2014.10.001
183. Sun M, Lanctot K, Herrmann N, Gallagher D. Exercise for cognitive symptoms in depression: a systematic review of interventional studies. Can J Psychiatry. (2018) 63:115–28. doi: 10.1177/0706743717738493
184. Briazgounov IP. The role of physical activity in the prevention and treatment of noncommunicable diseases. World Health Stat Q. (1988) 41:242–50.
185. Norris R, Carroll D, Cochrane R. The effects of physical activity and exercise training on psychological stress and well-being in an adolescent population. J Psychosom Res. (1992) 36:55–65. doi: 10.1016/0022-3999(92)90114-H
186. Szuhany KL, Otto MW. Efficacy evaluation of exercise as an augmentation strategy to brief behavioral activation treatment for depression: a randomized pilot trial. Cogn Behav Ther. (2020) 49:228–41. doi: 10.1080/16506073.2019.1641145
187. Boolani A, Sur S, Yang D, Avolio A, Goodwin A, Mondal S, et al. Six minutes of physical activity improves mood in older adults: a pilot study. J Geriatr Phys Ther. (2021) 44:18–24. doi: 10.1519/JPT.0000000000000233
188. Rethorst CD, Wipfli BM, Landers DM. The antidepressive effects of exercise: a meta-analysis of randomized trials. Sports Med. (2009) 39:491–511. doi: 10.2165/00007256-200939060-00004
Keywords: depression, exercise, neuroinflammation, neuroplasticity, therapeutic mechanism
Citation: Xie Y, Wu Z, Sun L, Zhou L, Wang G, Xiao L and Wang H (2021) The Effects and Mechanisms of Exercise on the Treatment of Depression. Front. Psychiatry 12:705559. doi: 10.3389/fpsyt.2021.705559
Received: 05 May 2021; Accepted: 05 October 2021;
Published: 05 November 2021.
Edited by:
Nilesh Bhailalbhai Patel, University of Nairobi, KenyaReviewed by:
Mario Bernardo-Filho, Rio de Janeiro State University, BrazilCopyright © 2021 Xie, Wu, Sun, Zhou, Wang, Xiao and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gaohua Wang, d2doNjQwMkAxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.