 María Paz García-Portilla1,2,3,4,5
María Paz García-Portilla1,2,3,4,5 Leticia García-Álvarez2,3,4,5,6
Leticia García-Álvarez2,3,4,5,6 Leticia González-Blanco1,2,3,4,5*
Leticia González-Blanco1,2,3,4,5* Francesco Dal Santo1,2,4,5
Francesco Dal Santo1,2,4,5 Teresa Bobes-Bascarán1,3,4,5,6
Teresa Bobes-Bascarán1,3,4,5,6 Clara Martínez-Cao2,4,5
Clara Martínez-Cao2,4,5 Ainoa García-Fernández2,4,5
Ainoa García-Fernández2,4,5 Pilar A. Sáiz1,2,3,4,5
Pilar A. Sáiz1,2,3,4,5 Julio Bobes1,2,3,4,5
Julio Bobes1,2,3,4,5- 1Servicio de Salud del Principado de Asturias (SESPA), Oviedo, Spain
- 2Department of Psychiatry, Universidad de Oviedo, Oviedo, Spain
- 3Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Madrid, Spain
- 4Instituto de Investigación Sanitaria del Principado de Asturias (ISPA), Oviedo, Spain
- 5Instituto Universitario de Neurociencias del Principado de Asturias (INEUROPA), Oviedo, Spain
- 6Department of Psychology, Universidad de Oviedo, Oviedo, Spain
Introduction: Interest in the idea of recovery for certain patients with schizophrenia has been growing over the last decade. Improving symptomatology and functioning is crucial for achieving this. Our study aims to identify those factors that substantially contribute to real-world functioning in these patients.
Methods: We carried out a cross-sectional study in stable outpatients with schizophrenia on maintenance antipsychotic monotherapy. Patients: We studied 144 outpatients with schizophrenia (DSM-IV-TR criteria) meeting the following criteria: (1) 18–65 years of age; (2) being clinically stable for at least the previous three months; (3) on maintenance antipsychotic monotherapy (prescriptions ≤ 10 mg olanzapine, ≤200 mg quetiapine, or ≤100 mg levomepromazine as hypnotics were also allowed); and (4) written informed consent. Assessment: We collected information on demographic and clinical variables by using an ad hoc questionnaire. For psychopathology, we employed the Spanish versions of the following psychometric instruments: the Positive and Negative Syndrome Scale (PANSS), the Brief Negative Symptom Scale (BNSS-Sp), and the Calgary Depression Scale (CDS). In addition, cognitive domains were assessed using the Verbal Fluency Test (VFT), the Digit Symbol Substitution Test (DSST), and the Trail Making Test, parts A and B (TMT-A and TMT-B). Finally, we employed the Spanish versions of the University of California San Diego Performance-based Skills Assessment (Sp-UPSA) and the Personal and Social Performance (PSP) for assessing functional capacity and real-world functioning, respectively. Statistical analysis: A forward stepwise regression was conducted by entering those variables significantly associated with PSP total score into the univariate analyses (Student's t-test, ANOVA with Duncan's post-hoc test, or bivariate Pearson correlation).
Results: A total of 144 patients; mean age 40 years, 64% males, mean length of illness 12.4 years, PSP total score 54.3. The final model was a significant predictor of real-world functioning [F(7, 131) = 36.371, p < 0.001] and explained 66.0% of the variance. Variables retained in the model: BNSS-Sp abulia, asociality, and blunted affect, PANSS general psychopathology, Sp-UPSA transportation, TMT-B, and heart rate.
Conclusion: Our model will contribute to a more efficient and personalized daily clinical practice by assigning specific interventions to each patient based on specific impaired factors in order to improve functioning.
Introduction
Although schizophrenia has traditionally been linked to severe functional deficits, interest in the idea of recovery as a possibility for particular patients has been growing in recent years. This concept of recovery is relatively new and still under construction in schizophrenia. It is complex, encompasses multiple aspects of the patient's life, and can be operationalized in two domains that are distinct, but to some extent interdependent, i.e., the objective or clinical and the subjective or personal (1–3).
The objective clinical recovery domain includes symptomatology and functioning, and it is well known that there is no direct relationship between the two (4). Furthermore, numerous studies have focused on functioning predictors, but their results are rarely replicated. Among the most consistently reported predictors are negative symptoms and cognitive performance (2, 5–15). Recently, a systematic review and evidence synthesis on the relationship between functional capacity, as measured by the University of California San Diego Performance-based Skills Assessment (UPSA), and different measurements of real-world functioning reported a connection between these two constructs that merits further investigation (16). In this sense, Menendez-Miranda et al. (9) quantified the relationship between the UPSA and the Personal and Social Performance scale (PSP), one of the most widely used real-world functioning measures, reporting that each one explained 17% of the variance of the other. Depressive symptoms have also been associated with worse functioning (10, 17), although the strength of this relationship was very weak (17). Gonzalez-Blanco et al. (15) found IL-2, a peripheral inflammatory biomarker, to be associated with worse functioning and negative and general psychopathology symptoms. Other predictors of functional remission or recovery in patients with schizophrenia identified by Vita and Barlati (3) in their review were education level, employment status, family economic status, age at onset, hospitalizations, relapses, adherence to treatment, and disorganization symptoms. Except for age at onset, all of these were reported by a single study.
Concerning treatment, Tandon et al. (18) concluded that side effects associated with second-generation antipsychotics substantially impact patient functioning and quality of life. However, they acknowledged that this is a convoluted, under-researched area. To better understand the relationship between different treatment options and outcomes measures, we need studies in naïve patients, but the difficulty enrolling them severely hampers the research (19).
With the above in mind, it can be hypothesized that different factors would have a small but significant effect on the real-world functioning of patients with schizophrenia. Therefore, identifying this plethora of factors would help to manage this disorder with greater precision and reduce its associated functional impairments through specific interventions aimed at their modification. Thus, this study aims to model the relationship between the real-world functioning of patients with schizophrenia on maintenance antipsychotic monotherapy and an extensive range of independent variables. We hypothesize that, in addition to negative symptoms and cognitive performance, depressive symptoms, somatic comorbidities, and functional capacity will be found to substantially contribute to patient functioning.
Methods
Design
This is a naturalistic, cross-sectional study carried out in outpatients with schizophrenia consecutively seen at either of the two mental health centers participating in the study. Both centers are in Oviedo, Northern Spain, and each has a catchment area population of about 80,000 inhabitants.
The study was conducted according to the Declaration of Helsinki (20). The Clinical Research Ethics Committee of Hospital Universitario Central de Asturias in Oviedo approved the study protocol (Ref. 127/15), and written informed consent was obtained from all participants before enrolment.
Patients
A total of 144 outpatients with schizophrenia (DSM-IV-TR criteria) were included in the study. Inclusion criteria were: (1) 18–65 years of age; (2) being clinically stable for at least the previous 3 months (without hospitalizations, symptom exacerbation, or any significant change in the type/dose of antipsychotic treatment); (3) on maintenance antipsychotic monotherapy (prescriptions ≤ 10 mg olanzapine, ≤ 200 mg quetiapine, or ≤ 100 mg levomepromazine as hypnotics were also allowed); and (4) written informed consent. Having an intellectual disability disorder or acquired brain injury was the sole exclusion criteria.
The sample was collected between July 2017 and December 2019. Therefore, we consecutively offered the study to the patients meeting all the inclusion criteria and none of the exclusion criteria at the clinic.
Assessment
Information on sociodemographic and clinical characteristics, including weight, heart rate, and blood pressure, was collected using an ad hoc questionnaire. To evaluate different psychopathological domains, we used the Spanish versions of the following psychometric instruments: Positive and Negative Syndrome Scale (PANSS) (21), Brief Negative Symptoms Scale (BNSS-Sp) (22), and Calgary Depression Scale for Schizophrenia (CDSS) (23). In all cases, higher scores indicate greater severity of the symptomatology.
Cognition was evaluated using phonemic (F-A-S) and semantic (animals) Verbal Fluency (VF) tests (24, 25), Digit Symbol Substitution Test (DSST) (26), and Trail Making Test parts A and B (TMT-A and TMT-B) (27). These tests measure the following cognitive domains:
• VF tests: attention, memory, verbal fluency, and executive functions (28)
• DSST: motor speed, attention, and visuoperceptual functions, but probably also associative learning and working memory (29) and
• TMT: Part A measures psychomotor speed, attention, and spatial organization, while Part B measures attention switching, mental flexibility, and recall (30).
For VF and DSST, lower scores indicate lower cognitive performance, while for TMT-A and -B, higher scores reflect lower cognitive performance.
We employed the Spanish version of the University of California San Diego Performance-based Skills Assessment (Sp-UPSA) to measure functional capacity (31). It assesses everyday adaptive skills, including finance management, communication, planning recreational activities, and transportation, under optimal conditions. The Sp-UPSA provides four domain scores (from 0 to 25 points) and a total score, potentially ranging from 0 to 100 points. In all cases, higher scores indicate better functional capacity.
Finally, real-world functioning was assessed using the Personal and Social Performance scale (PSP) (32). The PSP is a clinician-rated instrument that evaluates patient functioning in four areas of their lives: self-care, socially useful activities including work and study, personal and social relationships, and disturbing and aggressive behaviors. It provides scores in each of the four areas ranging from 0 to 6, where higher scores indicate worse functioning. It also provides a single total score ranging from 0 to 100, where higher scores reflect better personal and social functioning.
Statistical Analysis
To estimate the proportion of patients with a PSP total score ≥70, starting from a population size of 250 patients on maintenance antipsychotic monotherapy at our clinics, a sample of 144 subjects is required. This sample size was determined for a 95% confidence interval, with a precision of ±5%, and taking into account that the true estimated proportion will be 33%.
The statistical analysis was performed using IBM SPSS Statistics for Windows, Version 24.0. For all tests, the significance level was set at p < 0.05. To explore the potential relationships between PSP total score and sociodemographic, clinical, and psychometric variables, we used Student's t-test, ANOVA with Duncan's post-hoc test, or bivariate Pearson correlation. Finally, to model the relationship between the PSP total score and all variables found to be significantly associated with it in the univariate analysis, we performed a multiple linear regression (forward stepwise regression). To avoid collinearity, for those psychometric instruments that provide subscale scores (i.e., PANSS total score, UPSA total score), we do not include the total score in the analysis, nor do we include redundant measures (i.e., PANSS negative subscale or Marder negative factor).
Results
Sociodemographic and Clinical Characteristics
Patient mean age was 39.67 (11.93), 63.6% were males, and 58.3% had a secondary school degree. Most of the patients were never married (72.2%), were living with their family of origin (64.6%), and were not working (70.1%), and almost half were receiving a mental disability benefit (43.8%).
Their mean length of illness was 12.36 (10.91) years. Most had had at least one previous hospitalization (70.8%), and 19.4% had a history of suicide attempts. In addition, 45.8% had psychiatric comorbidities (substance use disorders, especially tobacco), and 63.9% had physical comorbidities (see Table 1).
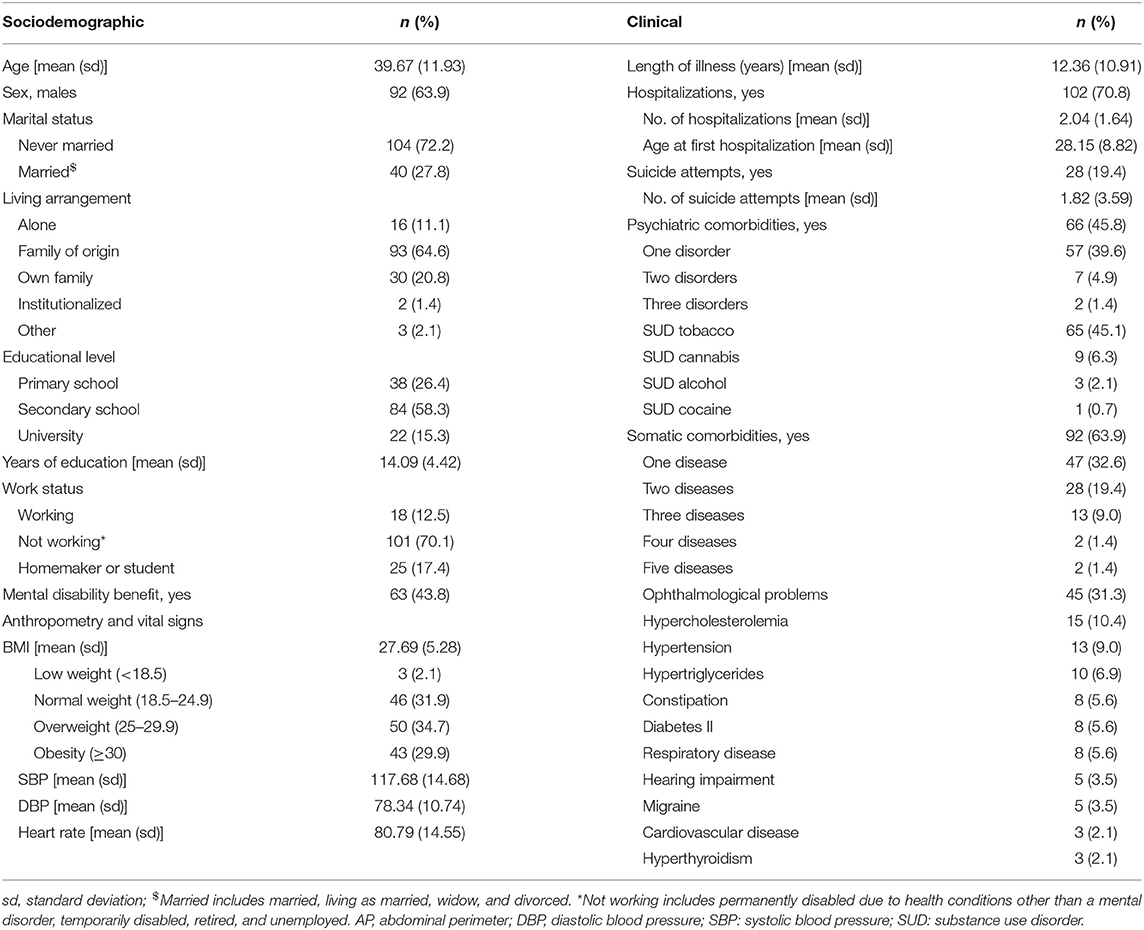
Table 1. Sociodemographic and clinical characteristics of the sample.
Concerning psychopharmacotherapy, all patients were on maintenance antipsychotic monotherapy (paliperidone 46.5%, aripiprazole 19.5%, olanzapine 13.9%, clozapine 4.9%, and only 3.5% of patients received typical antipsychotics). Almost half were on long-acting intramuscular antipsychotics (paliperidone LAI-3 months 20.1%, paliperidone LAI-1 month 13.9%, aripiprazole LAI 1-month 6.3%, fluphenazine decanoate 2.1%, and Risperdal Consta LAI 1.4%). Furthermore, 15% of patients were taking low doses of olanzapine (7.6%) or quetiapine (7.6%) as hypnotics, 19.4% were taking antidepressants and 43.8% at least one benzodiazepine (see Table 2).
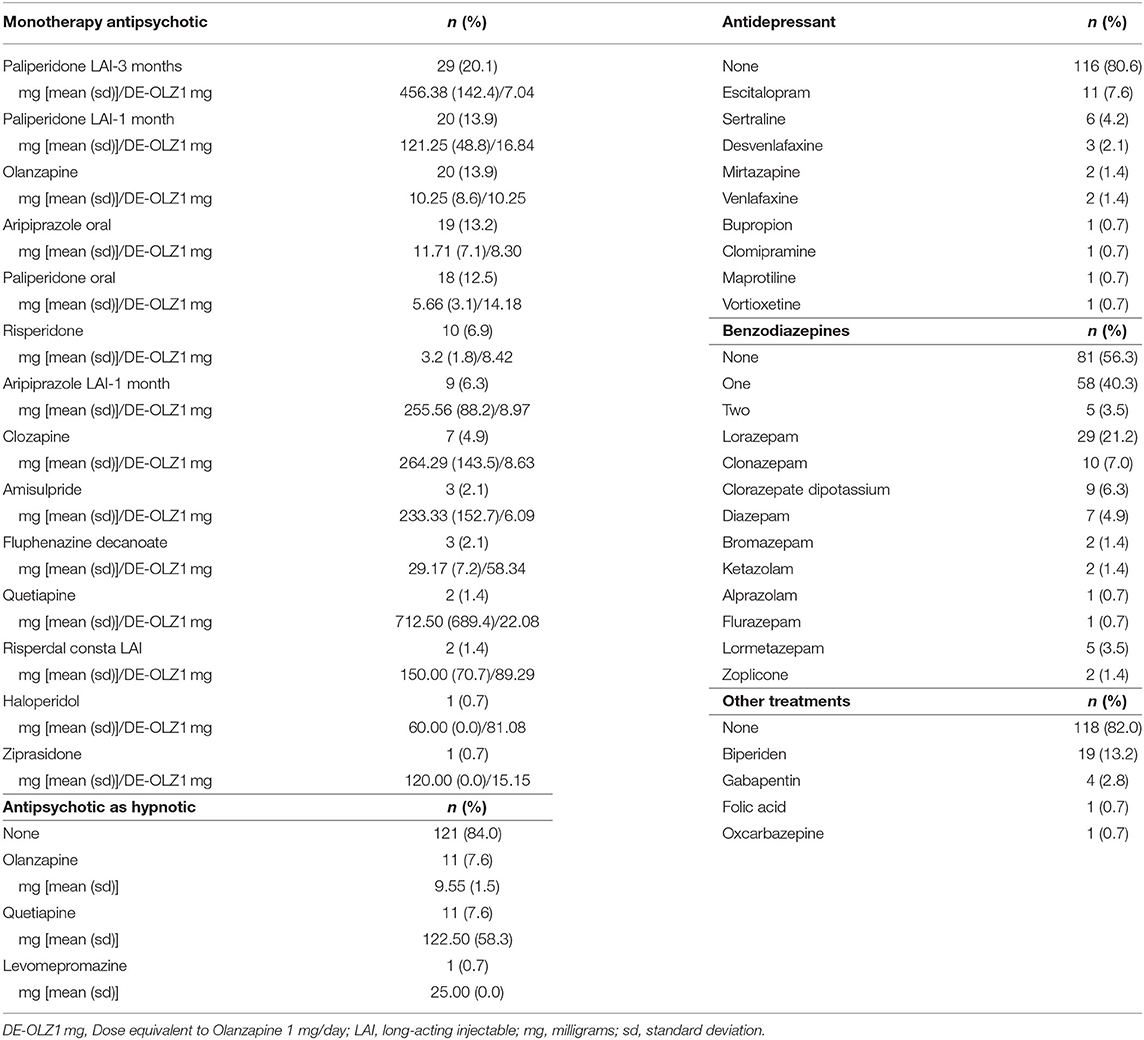
Table 2. Prescribed pharmacological treatment in descending order of frequency.
On the whole, patients included in the study had predominantly negative symptoms [PANSS Negative = 18.68 (5.57), PANSS Positive = 12.31 (5.30)], almost no depressive symptomatology [CDSS = 2.96 (3.62)] and performed relatively poorly on the cognitive tests [Verbal Fluency phonemic total = 26.03 (10.18), semantic animals = 16.70 (5.33), Digit Symbol Substitution = 41.73 (17.02), and TMT-A = 50.02 (25.89) and -B = 124.96 (67.19)]. Their functional capacity was mildly impaired [Sp-UPSA total score = 70.90 (14.56)], with communication being the domain most impaired [15.87 (4.75)] while transportation was the least [18.87 (4.72); see Table 1].
Real-World Functioning and Its Predictors
Patients showed manifest impairment in real-world functioning [PSP total score = 54.33 (18.43)], and only 18.1% of the patients showed a reasonable level of functioning (PSP total score > 70). Useful activities and relationships were the areas most impaired [2.32 (1.29) and 2.31 (1.29), respectively].
As shown in Tables 3, 4, several independent variables were significantly associated with patient real-world functioning. All variables involving negative symptoms showed the strongest correlations, followed by general psychopathology and functional capacity. On the contrary, the cognitive domains showed the weakest correlation with functioning, with attention switching, mental flexibility, and recall being the most strongly related. Also, being female, having some higher education, working or a homemaker/student, not receiving a mental disability benefit, having no history of suicide attempts, and no alcohol or benzodiazepine use were associated with better real-world functioning.
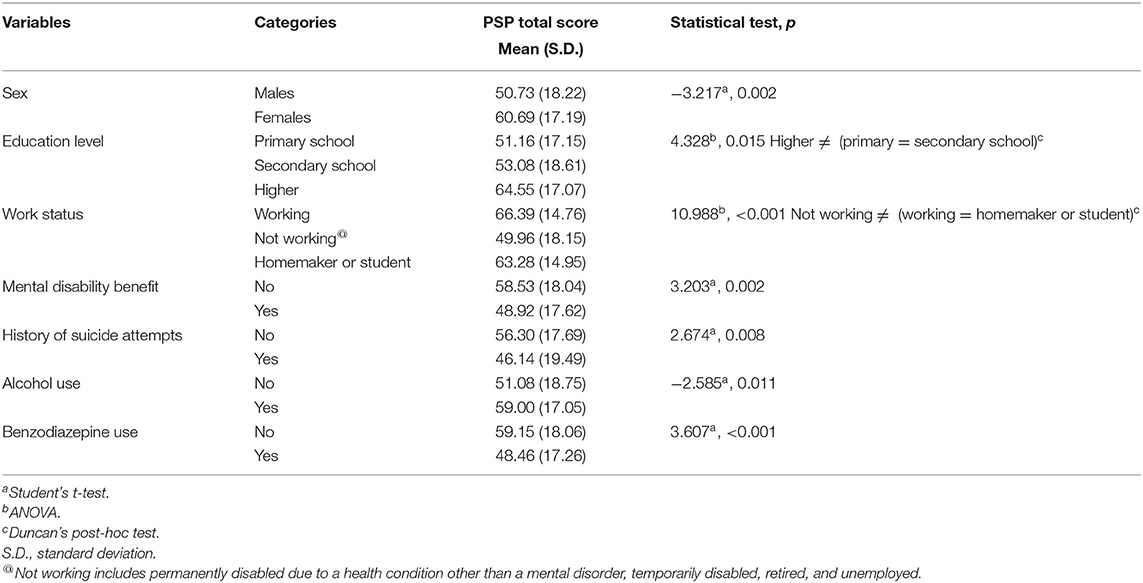
Table 3. Statistically significant associations between PSP total score and independent (categorical) variables.
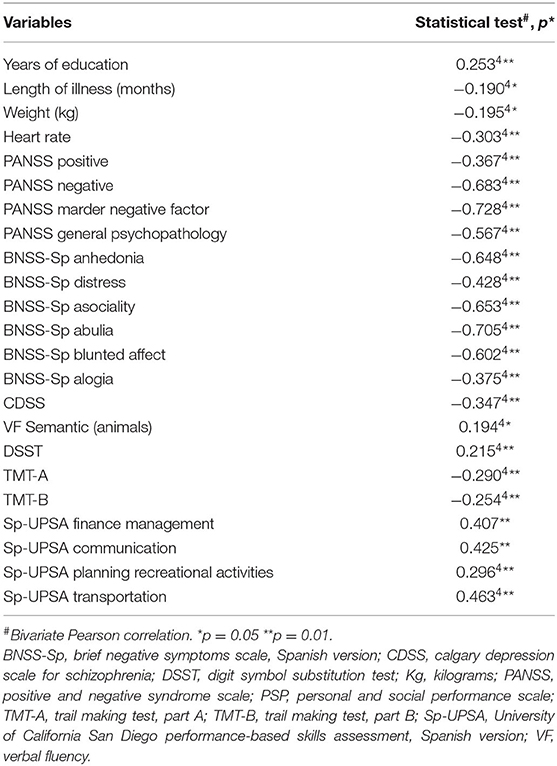
Table 4. Statistically significant associations between PSP total score and independent (continuous) variables.
Results of the multiple linear regression are shown in Table 5. The final model explained 66.0% of the variance (R2 = 0.660, standard error of the estimate = 10.928), and the model was a significant predictor of real-world functioning [F(7, 131) = 36.371, p < 0.001]. As shown in Table 2, the seven variables retained in the model contributed significantly to it. The final predictive model was:
Abulia and asociality were the independent variables that had the highest multicollinearity with other variables, but their variance inflation factor (VIF) values were very far from 5 (2.410 and 2.166, respectively, see Table 2).
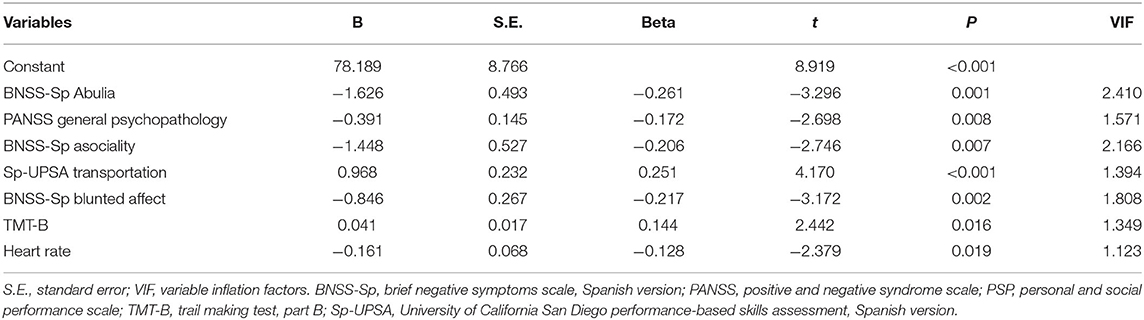
Table 5. Multiple linear regression model predicting real-world functioning (PSP total score).
Discussion
In line with our objective, we were able to model the relationship between the real-world functioning of patients with schizophrenia on maintenance antipsychotic monotherapy and several independent variables. Our hypothesis identified seven factors with a small but significant effect on patient real-world functioning. Negative symptomatology (BNSS abulia, asociality, and blunted affect subscales), general psychopathology (PANSS subscale), functional capacity (UPSA transportation domain), cognitive performance (Trail Making Test, part B), and heart rate were found to significantly contribute to predicting real-world functioning.
Unsurprisingly, negative symptomatology was found to be the most robust predictor of real-world functioning, as reported by other authors (8, 9, 11–15, 33). It is worth highlighting the advantage of using the BNSS over the PANSS negative subscale or the Marder negative factor. It allowed us to determine the relationships between these two domains more accurately. We found that three out of the five dimensions that constitute the negative syndrome (34)—abulia, asociality, and blunted affect—were retained in the model. In this respect, we previously found identical results in patients during their first 10 years of the disorder (mean age 31.7, mean length of illness 4.6 years) (15), although other authors (11, 13, 35) did not find any relationship between the so-called expressive dimension of the negative symptomatology (blunted affect and alogia) and functioning. However, as early as 2000; Jablensky et al. (36) had linked the deficit in language and communication with difficulties in daily life, interpersonal relationships, and social functioning. We find our result regarding the relevance of affective expression to real-world functioning of great interest since non-verbal language constitutes more than 90% of the oral communication between human beings, and communication is a crucial ability for appropriate functioning in our society. Thus, psychosocial interventions intended to improve language and communication difficulties in these patients could also help enhance their psychosocial functioning.
Although Szabo et al. (16), in their systematic review and evidence synthesis, did not find a significant impact of functional capacity, measured using the UPSA, on different measurements of real-world functioning [Specific Level of Functioning (SLOF), Global Assessment of Functioning (GAF), and Multidimensional Scale of Independent Functioning (MSIF)] some studies have demonstrated the opposite. For example, Menendez-Miranda et al. (9) and Galderisi et al. (11) reported a positive and significant influence of functional capacity on real-world functioning (PSP and SLOF, respectively), as we did in this study. Specifically, we found that out of the four domains included in the functional capacity construct, the use of public transportation was retained in the model. Like the other tasks included in the UPSA, this specific task reflects general abilities essential to independent living, such as planning and organizing (37), and would mediate the potential functional impact of cognitive performance (11, 38).
The impact of cognitive performance on functioning was also demonstrated in patients with schizophrenia (5–7, 11), but the majority of the studies proving their relationship were carried out more than 10 years ago. Recently, Galderisi et al. (11) reported an indirect neurocognitive effect on patient work skills and interpersonal relationships. Social cognition was the mediator in both areas of real-world functioning, while functional capacity acted as a mediator only for work skills. However, Gonzalez-Blanco et al. (15) did not find any effect. These contradictory results could be explained by the fact that in the first study, the performance in the different neurocognitive areas was considered a single factor, while in the second, each cognitive domain was considered separately. Our study found that attention switching, mental flexibility, and recall were the only cognitive domains retained in the model. But, to further cloud the issue they were associated with functioning in the unexpected direction (partial correlation coefficient = 0.041); that is, if the rest of the variables in the equation remain constant, an increase of 1 second in performing the TMT-B will result in an increase of 0.041 points in the PSP total score. The magnitude of the coefficient is indeed minimal, but its contribution to the model is significant. This unexpected result could have been due to multicollinearity between TMT-B and other independent variables in the model, but this is not the case, as shown in Table 2. The TMT-B is a multifactorial test that measures processing speed, complex attention, cognitive flexibility, inhibitory control, and for some authors working memory as well. It is known that it is influenced by several factors such as age, motor speed (related to the former), and years of education, among others. Although neither age nor educational level was included in the model, both significantly affected the results of the univariate analysis in the expected direction (results not shown).
Furthermore, some prospective studies reported the effect of cognition on functioning to be mediated by negative and general symptomatology (39, 40), and Gonzalez-Blanco et al. (15) also found a significant effect of general psychopathology on PSP total score, as we did. Thus, further research is required to elucidate the real contribution of the TMT-B on real-world functioning. Unfortunately, there are no TMT-B normative data for Spanish patients with schizophrenia, and our sample size does not allow us to conduct the analysis stratifying for these factors.
Increased heart rate has been described in patients with schizophrenia since Kraepelin and also demonstrated in untreated first-episode patients and healthy first-degree relatives (41). This autonomic dysfunction has been related to the excess cardiovascular and metabolic morbidity and mortality seen in these patients (41, 42), as well as those with positive symptomatology (43, 44) and impairment in psychosocial functioning (45), even in first-episode patients (46). Our results add more support to the negative impact of autonomic dysfunction on real-world functioning, providing a specific line of intervention to improve it. This relationship may be mediated by the cognitive impairment often present in these patients. In this sense, a recent meta-analysis confirmed a significant association between the presence of several cardiovascular risk factors and cognitive impairment in patients with schizophrenia (47); thus, cognitive impairment is a plausible mediating factor between autonomic dysfunction and poor real-world functioning.
Contrary to our hypothesis, our model did not include depressive symptoms. However, in the bivariate analysis, total score on the CDSS was significantly related to PSP total score. Therefore, we think our result is mainly connected to the sample characteristics and their effect on the statistical analyses. On the one hand, our patients had almost no depressive symptomatology when they were evaluated. On the other, negative symptomatology, which showed the most robust relationship to patient functioning, displaced depressive symptoms in the multivariate analysis.
It is beyond the scope of this study to detect differences in the level of functioning according to the pharmacological treatment patients were prescribed. Still, we would like to highlight that only benzodiazepine use was related to real-world functioning in the univariate analysis. Although this is highly speculative, the lack of relationship to the antipsychotic treatment could be associated with the inclusion criterion of a monotherapy regimen.
The main limitation of our study is its cross-sectional design. Long-term longitudinal studies could describe changes in real-world functioning and search for predictor variables of these changes. It would also be of great interest to conduct this research in first-episode schizophrenia patients before starting pharmacological treatment. Thus, we could more accurately delineate the influence of the different factors from the beginning of the disorder and design phase-specific interventions to modify their impact. As for our study's strengths, the extensive range of variables and domains included and the use of the BNSS to assess the negative syndrome of schizophrenia instead of the PANSS negative subscale are the two main ones. Finally, the condition of being on antipsychotic monotherapy is a novelty in this field.
In conclusion, we have provided clinicians with a simple formula that identifies the factors most substantially associated with patient real-world functioning. This formula will contribute to a more efficient and personalized daily clinical practice by assigning specific interventions to each patient based on specific impaired factors to improve functioning.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Clinical Research Ethics Committee of Hospital Universitario Central de Asturias in Oviedo (Ref. 127/15). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MG-P, PS, and JB designed the study and wrote the protocol. LG-Á, LG-B, and FD managed the literature searches and analyses. LG-Á undertook the statistical analysis. MG-P wrote the first draft of the manuscript. All authors contributed to and have approved the final manuscript.
Funding
This work was partly supported by the Instituto de Salud Carlos III (grant ref. PI16/01761), the Government of the Principality of Asturias PCTI-2018-2022 IDI/2018/235, and Fondos Europeos de Desarrollo Regional (FEDER). This study received funding from an unrestrictive grant from Janssen (ref. CIB-APS-2015-01). This funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of Interest
MG-P has been a consultant to and/or has received honoraria/grants from Angelini, Alianza OtsukaLundbeck, Instituto de Salud Carlos III, Janssen-Cilag, Lundbeck, Otsuka, and Pfizer. LG-Á has received honoraria from the 7th Framework Program European Union. LG-B has received honoraria/grants from the Spanish Foundation of Psychiatry and Mental Health, European Psychiatric Association, Otsuka, Lundbeck, Angelini, Janssen-Cilag and Pfizer. FS has received grants from the Spanish Foundation of Psychiatry and Mental Health. PS has been a consultant to and/or has received honoraria or grants from Adamed, CIBERSAM, European Comission, GlaxoSmithKline, Instituto de Salud Carlos III, Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Plan Nacional Sobre Drogas and Servier. JB has received research grants and served as consultant, advisor, or speaker within the last 5 years for: AB-Biotics, Acadia Pharmaceuticals, Angelini, Casen Recordati, D&A Pharma, Exeltis, Gilead, GSK, Ferrer, Indivior, Janssen-Cilag, Lundbeck, Mundipharma, Otsuka, Pfizer, Reckitt-Benckiser, Roche, Sage Therapeutics, Servier, Shire, Schwabe Farma Ibérica, research funding from the Spanish Ministry of Economy and Competiveness–Centro de Investigación Biomedica en Red area de Salud Mental (CIBERSAM) and Instituto de Salud Carlos III-, Spanish Ministry of Health, Social Services and Equality—Plan Nacional sobre Drogas—and the 7th Framework Program of the European Union.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors wish to thank Sharon Grevet for her English assistance.
References
1. Van Eck RM, Burger TJ, Velling A, Schirmbeck F, de Haan L. The relationship between clinical and personal recovery patients with schizophrenia spectrum disorders: a systematic review and meta-analysis. Schizophr Bull. (2018) 44:631–42. doi: 10.1093/schbul/sbx088
2. Lahera G, Gálvez JL, Sánchez P, Martínez-Roig M, Pérez-Fuster JV, García-Portilla P, et al. Functional recovery in patients with schizophrenia: recommendations from a panel of experts. BMC Psychiatry. (2018) 18:176. doi: 10.1186/s12888-018-1755-2
3. Vita A, Barlati S. Recovery from schizophrenia: is it possible? Curr Opin Psychiatry. (2018) 32:246–55. doi: 10.1097/YCO.0000000000000407
4. Bobes J, Ciudad A, Alvarez E, San L, Polavieja P, Gilaberte I. Recovery from schizophrenia: results from 1-year follow-up observational study of patients in symptomatic remission. Schizophr Res. (2009) 115:58–66. doi: 10.1016/j.schres.2009.07.003
5. Bowie CR, Harvey PD. Cognitive deficits and functional outcome in schizophrenia. Neuropsychiatr Dis Treat. (2006) 2:531–6. doi: 10.2147/nedt.2006.2.4.531
6. Green MF. Cognitive impairment and functional outcome in schizophrenia and bipolar disorder. J Clin Psychiatry. (2006) 67:3–8. doi: 10.4088/JCP.1006e12
7. Bowie CR, Leung WW, Reichenberg A, McClure MM, Patterson TL, Heaton RK, et al. Predicting schizophrenia patients' real-world behavior with specific neuropsychological and functional capacity measures. Biol Psychiatry. (2008) 63:505–11. doi: 10.1016/j.biopsych.2007.05.022
8. Harvey PD. Disability in schizophrenia: contributing factors and validated assessments. J Clin Psychiatry. (2014) 75:15–20. doi: 10.4088/JCP.13049su1c.03
9. Menendez-Miranda I, Garcia-Portilla MP, Garcia-Alvarez L, Arrojo M, Sanchez P, Sarramea F, et al. Predictive factors of functional capacity and real-world functioning in patients with schizophrenia. Eur Psychiatry. (2015) 30:622–7. doi: 10.1016/j.eurpsy.2014.12.011
10. Strassnig MT, Raykov T, O'Gorman C, Bowie CR, Sabbag S, Durand D, et al. Determinants of different aspects of everyday outcome in schizophrenia: the roles of negative symptoms, cognition, and functional capacity. Schizophr Res. (2015) 165:76–82. doi: 10.1016/j.schres.2015.03.033
11. Galderisi S, Rossi A, Rocca P, Bertolino A, Mucci A, Bucci P, et al. Italian network for research on psychoses. Pathways to functional outcome in subjects with schizophrenia living in the community and their unaffected first-degree relatives. Schizophr Res. (2016) 175:154–60. doi: 10.1016/j.schres.2016.04.043
12. Immonen J, Jääskeläinen E, Korpela H, Miettunen J. Age at onset and the outcomes of schizophrenia: a systematic review and meta-analysis. Early Interv Psychiatry. (2017) 11:453–60. doi: 10.1111/eip.12412
13. Bucci P, Galderisi S, Mucci A, Rossi A, Rocca P, Bertolino A, et al. Italian network for research on psychoses. Premorbid academic and social functioning in patients with schizophrenia and its association with negative symptoms and cognition. Acta Psychiatr Scand. (2018) 138:253–66. doi: 10.1111/acps.12938
14. Strassnig M, Bowie C, Pinkham AE, Penn D, Twamley EW, Patterson TL, et al. Which levels of cognitive impairments and negative symptoms are related to functional deficits in schizophrenia? J. Psychiatr Res. (2008) 104:124–9. doi: 10.1016/j.jpsychires.2018.06.018
15. Gonzalez-Blanco L, Garcia-Portilla MP, Dal Santo F, Garcia-Alvarez L, de la Fuente-Tomas L, Menendez-Miranda I, et al. Predicting real-world functioning in outpatients with schizophrenia: role of inflammation and psychopathology. Psychiatry Res. (2019) 280:112509. doi: 10.1016/j.psychres.2019.112509
16. Szabo S, Merikle E, Lozano-Ortega G, Powell L, Macek T, Cline S. Assessing the relationship between performance on the University of California performance skills assessment (UPSA) and outcomes in schizophrenia: a systematic review and evidence synthesis. Schizophr Res Treat. (2018) 2018:9075174. doi: 10.1155/2018/9075174
17. Galderisi S, Rossi A, Rocca P, Bertolino A, Mucci A, Bucci P, et al. Italian network for research on psychoses. The influence of illness-related variables, personal resources and context-related factors on real-life functioning of people with schizophrenia. World Psychiatry. (2014) 13:275–87. doi: 10.1002/wps.20167
18. Tandon R, Lenderking WR, Weiss C, Shalhoub H, Barbosa CD, Chen J, et al. The impact on functioning of second-generation antipsychotic medication side effects for patients with schizophrenia: a worldwide, cross-sectional, web-based survey. Ann Gen Psychiatry. (2020) 19:42. doi: 10.1186/s12991-020-00292-5
19. Martinuzzi E, Barbosa S, Daoudlarian D, Bel Haj Ali W, Gilet C, Fillatre L, et al. Stratification and prediction of remission in first-episode psychosis patients: the OPTiMiSE cohort study. Transl Psychiatry. (2019) 9:20. doi: 10.1038/s41398-018-0366-5
20. World Medical Association General Assembly. Declaration of Helsinki, Ethical Principles for Medical Research Involving Human Subjects. Fortaleza: World Medical Association (2013).
21. Peralta V, Cuesta MJ. Validación de la Escala de los Síndromes Positivo y Negativo (PANSS) en una muestra de esquizofrénicos españoles. Actas Luso-Esp Neurol Psiquiatr. (1994) 4:44–50.
22. Mané A, García-Rizo C, Garcia-Portilla MP, Bergé D, Sugranyes G, Garcia-Alvarez L, et al. Spanish adaptation and validation of the brief negative symptoms scale. Compr Psychiatry. (2014). 55:1726–9. doi: 10.1016/j.comppsych.2014.05.024
23. Sarró S, Dueñas RM, Ramírez N, Arranz B, Martínez R, Sánchez JM, et al. Cross-cultural adaptation and validation of the Spanish version of the calgary depression scale for schizophrenia. Schizophr Res. (2004) 68:349–56. doi: 10.1016/S0920-9964(02)00490-5
24. Benton AL, Hamsher K. Multilingual Aphasia Examination Manual - Revised. Iowa City, IA: University of Iowa (1978).
25. Spreen O, Strauss E. A Compendium of Neuropsychological Tests. Administration, Norms, and Commentary. New York, NY: Oxford University Press (1998).
26. Wechsler D. Wechsler Adult Intelligence Scale-Third Edition (WAIS-III). San Antonio, TX: The Psychological Corporation (1997). doi: 10.1037/t49755-000
27. Reitan RM. Trail Making Test: Manual for Administration and Scoring. Tucson, AZ: Reitan Neuropsychology Laboratory (1992).
28. Crowe SF. Decrease in performance on the verbal fluency test as a function of time: evaluation in a young healthy sample. J Clin Exp Neuropsychol. (1998) 20:391–401. doi: 10.1076/jcen.20.3.391.810
29. Jaeger J. Digit symbol substitution test. The case for sensitivity over specificity in neuropsychological testing. J Clin Psychopharmacol. (2018) 38:513–9. doi: 10.1097/JCP.0000000000000941
30. Corrigan JD, Hinkeldey NS. Relationships between parts A and B of the trail making test. J Clin Psychol. (1987) 43:402–9. doi: 10.1002/1097-4679(198707)43:4<402::AID-JCLP2270430411>3.0.CO;2-E
31. Garcia-Portilla MP, Gomar JJ, Bobes-Bascaran MT, Menendez-Miranda I, Saiz PA, Muñiz J, et al. Validation of a European Spanish-version of the University of California performance Skills Assessment (Sp-UPSA) in patients with schizophrenia and bipolar disorder. Schizophr Res. (2013) 150:421–6. doi: 10.1016/j.schres.2013.07.049
32. Garcia-Portilla MP, Saiz PA, Bousoño M, Bascaran MT, Guzmán-Quilo C, Bobes J, et al. Validation of the Spanish Personal and Social Performance scale (PSP) in outpatients with stable and unstable schizophrenia. Rev Psiquiatr Salud Ment. (2011) 4:9–18. doi: 10.1016/S2173-5050(11)70003-6
33. Lahera G, Ruiz A, Brañas A, Vicens M, Orozco A. Reaction time, processing speed and sustained attention in schizophrenia: impact on social functioning. Rev Psiquiatr Salud Ment. (2017) 10:197–205. doi: 10.1016/j.rpsm.2017.04.001
34. Ahmed AO, Kirkpatrick B, Galderisi S, Mucci A, Rossi A, Bertolino A, et al. Cross-cultural validation of the 5-Factor structure of negative symptoms in schizophrenia. Schizophr Bull. (2019) 45:305–14. doi: 10.1093/schbul/sby050
35. Rocca P, Montemagni C, Zappia S, Piterà R, Sigaudo M, Bogetto F. Negative symptoms and everyday functioning in schizophrenia: a cross-sectional study in a real world-setting. Psychiatry Res. (2014) 218:284–9. doi: 10.1016/j.psychres.2014.04.018
36. Jablensky A, McGrath J, Herrman H, Castle D, Gureje O, Evans M, et al. Psychotic disorders in urban areas: an overview of the study on low prevalence disorders. Aust NZ J Psychiatry. (2000) 34:221–36. doi: 10.1080/j.1440-1614.2000.00728.x
37. Patterson TL, Goldman S, McKibbin CL, Hughs T, Jeste DV. UCSD performance-based skills assessment: development of a new measure of everyday functioning for severely mentally ill adults. Schizophr Bull. (2001) 27:235–45. doi: 10.1093/oxfordjournals.schbul.a006870
38. Green MF, Nuechterlein KH, Kern RS, Baade LE, Fenton WS, Gold JM, et al. Functional co-primary measures for clinical trials in schizophrenia: results from the MATRICS Psychometric and Standardization Study. Am J Psychiatry. (2008) 165:221–8. doi: 10.1176/appi.ajp.2007.07010089
39. Simons CJ, Bartels-Velthuis AA, Pijnenborg GH, Genetic Risk and Outcome of Psychosis (GROUP) Investigators. Cognitive performance and long-term social functioning in psychotic disorder: a three-year follow-up study. PLoS ONE. (2016) 11:e0151299. doi: 10.1371/journal.pone.0151299
40. Lee EHM, Hui CLM, Chan KPK, Chan PY, Law EYL, Chong CSY, et al. The role of symptoms and insight in mediating cognition and functioning in first-episode psychosis. Schizophr Res. (2019) 206:251–6. doi: 10.1016/j.schres.2018.11.009
41. Bär KJ. Cardiac autonomic dysfunction in patients with schizophrenia and their healthy relatives - a small review. Front Neurol. (2015) 24:139. doi: 10.3389/fneur.2015.00139
42. De Hert M, Correll CU, Bobes J, Cetkovich-Bakmas M, Cohen D, Asai I, et al. Physical illness in patients with severe mental disorders. I Prevalence, impact of medications and disparities in health care. World Psychiatry. (2011) 10:52–77. doi: 10.1002/j.2051-5545.2011.tb00014.x
43. Bär KJ, Letzsch A, Jochum T, Wagner G, Greiner W, Sauer HJ. Loss of efferent vagal activity in acute schizophrenia. Psychiatr Res. (2005) 39:519–27. doi: 10.1016/j.jpsychires.2004.12.007
44. Bär KJ, Boettger MK, Koschke M, Schulz S, Chokka P, Yeragani VK, et al. Non-linear complexity measures of heart rate variability in acute schizophrenia. Clin Neurophysiol. (2007) 118:2009–15. doi: 10.1016/j.clinph.2007.06.012
45. Fujibayashi M, Matsumoto T, Kishida I, Kimura T, Ishii C, Ishii N, et al. Autonomic nervous system activity and psychiatric severity in schizophrenia. Psychiatry Clin Neurosci. (2009) 63:538–45. doi: 10.1111/j.1440-1819.2009.01983.x
46. Reed AC, Lee J, Green MF, Hamilton HK, Miller GA, Subotnik KL, et al. Associations between physiological responses to social-evaluative stress and daily functioning in first-episode schizophrenia. Schizophr Res. (2020) 218:233–9. doi: 10.1016/j.schres.2019.12.040
Keywords: functioning, recovery, schizophrenia, monotherapy, antipsychotic
Citation: García-Portilla MP, García-Álvarez L, González-Blanco L, Dal Santo F, Bobes-Bascarán T, Martínez-Cao C, García-Fernández A, Sáiz PA and Bobes J (2021) Real-World Functioning in Patients With Schizophrenia: Beyond Negative and Cognitive Symptoms. Front. Psychiatry 12:700747. doi: 10.3389/fpsyt.2021.700747
Received: 26 April 2021; Accepted: 15 July 2021;
Published: 09 August 2021.
Edited by:
Armida Mucci, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Janusz K. Rybakowski, Poznan University of Medical Sciences, PolandKrzysztof Krysta, Medical University of Silesia, Poland
Cristiana Montemagni, University of Turin, Italy
Copyright © 2021 García-Portilla, García-Álvarez, González-Blanco, Dal Santo, Bobes-Bascarán, Martínez-Cao, García-Fernández, Sáiz and Bobes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Leticia González-Blanco, bGV0aWNpYWdvbnphbGV6YmxhbmNvQGdtYWlsLmNvbQ==