
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 10 September 2021
Sec. Mood Disorders
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.699682
This article is part of the Research TopicBio-Psycho-Social Indicators of Suicide RiskView all 18 articles
 Balpreet Panesar1
Balpreet Panesar1 Tea Rosic2,3Myanca Rodrigues3
Tea Rosic2,3Myanca Rodrigues3 Nitika Sanger4
Nitika Sanger4 Natasha Baptist-Mohseni5Alannah Hillmer1Caroul Chawar2Alessia D'Elia1
Natasha Baptist-Mohseni5Alannah Hillmer1Caroul Chawar2Alessia D'Elia1 Luciano Minuzzi2
Luciano Minuzzi2 Lehana Thabane6,7
Lehana Thabane6,7 Zainab Samaan2,6,7*
Zainab Samaan2,6,7*Background: Suicide is a serious public health concern for which there have been well-established protective and risk factors reported in literature. There is a lack of evidence on the indirect effects of other variables on these factors. Specifically, the association between stressful life events and suicidal behavior may be affected by perceived social support, but its role in this association is largely uninvestigated.
Objectives: Thus, this paper aims to explore the role of perceived social support in the association between stressful life events and suicidal behavior. Perceived social support will be explored as a mediator and as a moderator in this association.
Methods: Data were obtained from the Determinants of Suicidal Behavior Conventional and Emergent Risk (DISCOVER), a study conducted to identify risk factors of suicidal behavior. The study participants are individuals with suicide attempts admitted to hospital. Participants (n = 343) were recruited from hospital setting. Suicidal behavior was measured using two outcomes (1) the occurrence of a suicide attempt (2) level of suicide intent as measured by the Pierce Suicide Intent Scale. Perceived social support was measured using the Sarason Social Support Questionnaire.
Results: Stressful life events were significantly associated with suicide attempts (OR 1.440, 95% CI 1.440, 1.682, p < 0.001) and perceived social support (B −0.785, 95% CI −1.501, −0.068, p = 0.032). There was no significant mediation effect by perceived social support in the association between stressful life events and suicide attempts (Sobel's test statistic 1.64, p = 0.100). Perceived social support did not moderate the relationship between stressful life events and suicide attempts [(OR 1.007, 95% CI 0.987, 1.027, p = 0.514] or the relationship between stressful life events and level of suicidal intent (B −0.043, 95% CI −0.132, 0.046, p = 0.343).
Conclusion: Stressful life events are associated with increased risk of suicide attempts. The study also identified an inverse relationship between stressful life events and perceived social support. These associations were independent of perceived social support. This study highlights the effects of stressful life events on suicide risk is not affected by perceived social support, requiring further investigation into measures to reduce the impact of social stressors on people with risk of suicide.
Suicide and suicidal behavior are serious social and health concerns. Every year, about 800,000 people worldwide die by suicide, and it is one of the leading causes of death for 15–29 years old (1). Researchers have identified a multitude of risk and protective factors for suicide in recent years. Factors such as depression (2–6), family history of suicide (7–9), and stressful life events (10–14) have been found to have direct relationships with suicidal behavior. It is important to elaborate on these well-established direct effects to uncover and clarify causal links through which these effects may occur, and to ultimately inform suicide prevention and intervention efforts with specific, defined pathways rather than broad associations. As such, a growing area of research interest is the examination of the indirect effects of such factors on suicidal behavior, and interactions between different risk or protective factors (15, 16). Recently, studies have attempted to clarify indirect effects of well-established risk factors for suicide; for example, studies looking at depression and suicide that suggest the inclusion of variables such as life satisfaction and psychiatric status to induce the causal pathway between depression and suicide (17, 18). The recent evidence for the influence of different factors on the well-established association between depression and suicide presents reason to clarify the links between other known associations relating to suicidal behavior. One such established association is between stressful life events and suicidal behavior, for which a direct pathway has been consistently reported (10–14).
Stressful life events are defined as unexpected and undesired life events that often have the capacity to influence health and well-being (19). The association between stressful life events and suicidal behavior has been extensively studied, but there is limited evidence on indirect factors that moderate or mediate the relationship between the two variables. Perceived social support is defined as the individual's subjective understanding of the level of social support that can be provided by members of their social network (20). Current literature has shown moderating effects of perceived social support in the association between stressful life events and depression (21, 22), stressful life events and hopelessness (23, 24), and stressful life events and subjective well-being (25). There is also evidence for perceived social support as a moderator in the association between stressful life events (i.e., traumatic events, discrimination, medical diagnosis) and suicidal behavior in specific populations such as South African adolescents and transgender samples (26–28). There is limited evidence for perceived social support as a mediator (29) in the association between stressful life events and suicidal behavior but there is reason to suggest that perceived social support and stressful life events are correlated. Specifically, there are studies that show there is deterioration of perceived social support after the occurrence of a stressful life event (30, 31), and there has been a recent study in adolescents that established perceived social support as a mediator in the association between stressful life events and suicidal ideation and suicide attempts (32). Furthermore, a study looking at relationship between stress and health suggests that the stress-health connection is influenced by perceived social support, and can only be appropriately understood after the consideration of moderating and mediating factors (19). Thus, although there is limited evidence of perceived social support as either a moderator or mediator in the association between stressful life events and suicide, there are indications in literature that perceived social support is involved in the association between stressful life events and suicidal behavior. Furthermore, stressful life events are risk factors that are difficult to address with suicide prevention strategies as they can be unpredictable events (33, 34). In contrast, social support is a modifiable factor that is likely able to be influenced by suicide related prevention and intervention strategies, and as such, more investigation is needed to determine how perceived social support fits into the association between stressful life events and suicidal behavior.
This study will expand on current literature by investigating the role of perceived social support in the association between stressful life events and suicidal behavior in patients with suicide attempts admitted to psychiatric hospital. The limited evidence on the role of perceived social support in the association, combined with the established direct associations between stressful life events and suicidal behavior (10–14), perceived social support and suicidal behavior (35–37), and adequate evidence for stressful life events and perceived social support (30–32) provide further reason to clarify the associations between these three variables. Thus, this study will explore the role of perceived social support in the association between stressful life events and suicidal behavior by assessing its role as a mediator or moderator. The findings from this study will add to current literature that is defining the indirect effects of variables on well-established relationships between protective and risk factors for suicide and suicidal behavior. The goal of this research is to identify an actionable modifiable factor such as social support to reduce the risk of suicide.
The objectives of this study are to explore the role of perceived social support in the association between stressful life events and suicidal behavior by investigating if:
1 the association between stressful life events, reported within the last year, and the occurrence of suicide attempts is mediated by the self-reported level of perceived social support,
2 the association between stressful life events, reported within the last year, and the occurrence of suicide attempts is moderated by the self-reported level of perceived social support,
3 the association between stressful life events, reported within the last year, and level of suicide intent is mediated by the self-reported level of perceived social support,
4 the association between stressful life events, reported within the last year, and level of suicide intent is moderated by the self-reported level of perceived social support.
The study is reporting according to the Strengthening of the Reporting of Observational Studies in Epidemiology (STROBE) statement for cross-sectional studies (38).
The data from this study were obtained from the case-control study titled Determinants of Suicidal Behavior Conventional and Emergent Risk (DISCOVER), which was conducted to identify risk factors of suicidal behavior (39, 40). The study was approved by the Hamilton Health Sciences (#10-661) and St. Joseph's Healthcare (#11-3479) Research Ethics Boards. The study design for this paper is cross-sectional as data were taken from questionnaires administered at one time point. Study recruitment was completed from two city hospitals including Hamilton General Hospital, and St. Joseph's Healthcare, Hamilton where psychiatric inpatient services provided.
The inclusion criteria for the cases (individuals with suicide attempt) in this study were adult (18 years or older) participants that were admitted to hospital (the psychiatric or general hospitals), had a recent or past suicide attempt. The inclusion criteria for the controls in this study were psychiatric inpatients admitted at the same time as the cases with no history of suicide attempts and non-psychiatric inpatients without a history of suicide attempts. All study participants provided written informed consent and were interviewed face-to-face to conduct study related procedures. Participants were recruited from February 2011 to December 2014.
The socio-demographic characteristics included in this study were age, sex, ethnicity, marital status, current employment, and satisfaction with social support. Marital status was operationalized as those with a partner (currently married, common law, living with a partner) and those without a partner (never married, widowed, separated, divorced). Satisfaction with social support was measured using the Sarason Social Support Questionnaire (SSQ) short form, which asks participants how satisfied they were with the social support they were receiving on a six-point rating scale ranging from “very dissatisfied” to “very satisfied.” (41). It asks participants to list up to 10 people who they can count on to be dependable, who can help them relax when under pressure, who accept their worst and best points, who really care about them, who can help them feel better, and who can console them. A social support score is generated by means of the number of people the participant has listed for each of the 6 items that were asked. The higher the number of the satisfaction with social support score, the greater the satisfaction of the participant. The satisfaction with social support score is generated by the means of the satisfaction ratings for all 6 items included in the SSQ (41). The Cronbach alpha for inter-reliability for this questionnaire is 0.97 (41).
Information about any stressful life events the participants experienced in the last year was also collected. Stressful life events included the dichotomous variables of marital separation, loss of job/retirement, loss of crop/business failure, violence, major intra-family conflict, major personal injury or illness, death/major illness of a close family member, death of a spouse, and other. These dichotomous variables were coded, where no occurrence of the stressful life event was coded as zero and the occurrence of a stressful life event was coded as one. These coded variables were then added to create a continuous stressful life events score.
Suicidal behavior was assessed using the occurrence of a suicide attempt and the level of suicidal intent. The occurrence of a suicide attempt was determined by self-reported suicide history data, which was then confirmed through access to medical records (39). The questionnaire used in the DISCOVER study to evaluate the level of suicidal intent was the Pierce Suicide Intent Scale (42). The Pierce Suicide Intent Scale is comprised of 12 questions that generate an output score of 0–22. A score of 0–3 on the questionnaire indicates low intent, 4–10 indicates medium intent, and 10+ indicates high intent (42). The Cronbach alpha value for the Pierce Suicide Intent Scale is 0.77 (43).
Version 26 of SPSS (44) was used to conduct all descriptive, mediation, moderation, and interaction analyses. Descriptive statistics were used to summarize the demographic data of the study population. Continuous variables are presented as means with standard deviations, while dichotomous variables are summarized using percentages.
Our first objective was to explore whether the association between stressful life events and suicide attempts is mediated by level of perceived social support. Our mediation analysis was conducted in three steps, as follows:
1 First, we assessed the association between stressful life events score (independent variable) and suicide attempt (dependent variable) using a logistic regression model with age and sex included as covariates.
2 Second, we assessed the association between stressful life events score (independent variable) and social support score (mediator) using a linear regression model with age and sex included as covariates.
3 Third, we constructed a final logistic regression model with suicide attempt included as the dependent variable, and both social support score and stressful life events score as independent variables, adjusting also for age and sex. If social support exerted a mediation effect, the association between stressful life events and suicide attempt would diminish as compared to that detected in step one of our analysis. We then applied Sobel's test to assess the statistical significance of the mediation effect using an online calculator (45).
Our second objective was to explore whether the association between stressful life events and suicide attempts is moderated by level of perceived social support. Our moderation analysis was conducted as follows: we created a continuous interaction term using the product of the stressful life events score and the social support score and tested this interaction in a logistic regression model using suicide attempt as the dependent variable. Our model was adjusted for age and sex, as well as the social support score, and the stressful life events score.
Our third objective was to explore whether the association between stressful life events and level of suicide intent is mediated by level of perceived social support. This mediation analysis was conducted using the same steps as described earlier:
1 First, we assessed the association between stressful life events score (independent variable) and level of suicide intent (dependent variable) using a linear regression model with age and sex included as covariates.
2 Second, we assessed the association between stressful life events score (independent variable) and social support score (mediator) using a linear regression model with age and sex included as covariates.
3 Third, we constructed a final linear regression model with level of suicide intent included as the dependent variable, and both social support score and stressful life events score as independent variables, adjusting for age and sex. If social support exerted a mediation effect, the association between stressful life events and level of suicide would diminish as compared that detected in to step one of our analysis. Sobel's test was used to assess the statistical significance of the mediation effect (45).
Our fourth objective was to explore whether the association between stressful life events and level of suicide intent is moderated by the self-reported level of perceived social support. We created a continuous interaction term using the product of the stressful life events score and the social support score and tested this interaction in a linear regression model using level of suicidal intent as the dependent variable. Our model was adjusted for age and sex, as well as the social support score, and the stressful life events score.
For logistic regression analyses, we report odds ratios (OR) with 95% confidence interval (CI), and p-values. For linear regressions, we report unstandardized Beta-coefficients (B) with 95% CI, and p-values. For all analyses the alpha level of significance was set to a = 0.05. We assessed for multicollinearity using the variance inflation factor (VIF), where a VIF less than two was considered to be an acceptable cut-off.
Altogether, 343 individuals included in this study, 146 of whom were cases with a past or recent suicide attempt, and 197 of whom were controls (Figure 1). There were more women than men (women cases 55.5%, women control 49.7%) in the cases compared to the controls, and the cases were more likely to be without a partner (cases without partner 73.1%, controls without partner 59.4%). There was a larger proportion of individuals with European ethnicity seen in the cases group (92.5%) compared to the control group (72.8%). The mean social support score was 9.11 SD 8.88) compared to controls (12.5 SD 10.8), in contrast to the stressful life events score which was higher in cases (11.4 SD 1.53) compared to controls (10.5 SD 1.52). One of the highest reported stressful life events was “other stressful life event” where 44.6% of cases reported having other and 32.6% of controls reported having other stressors. Examples of these “other” stressors are “inability to find work,” “financial stress,” “having a baby,” and “housing issues.” The study participants' characteristics are provided in Table 1.
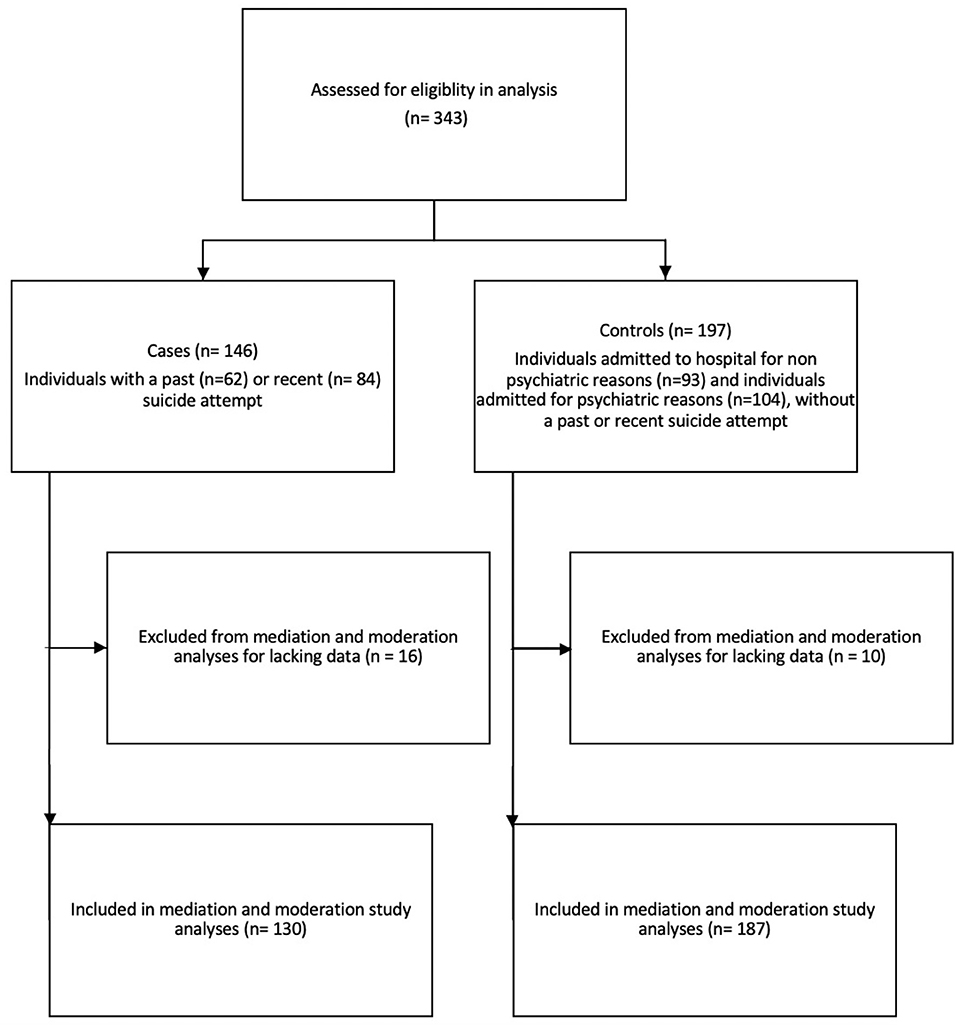
Figure 1. Study flow diagram.
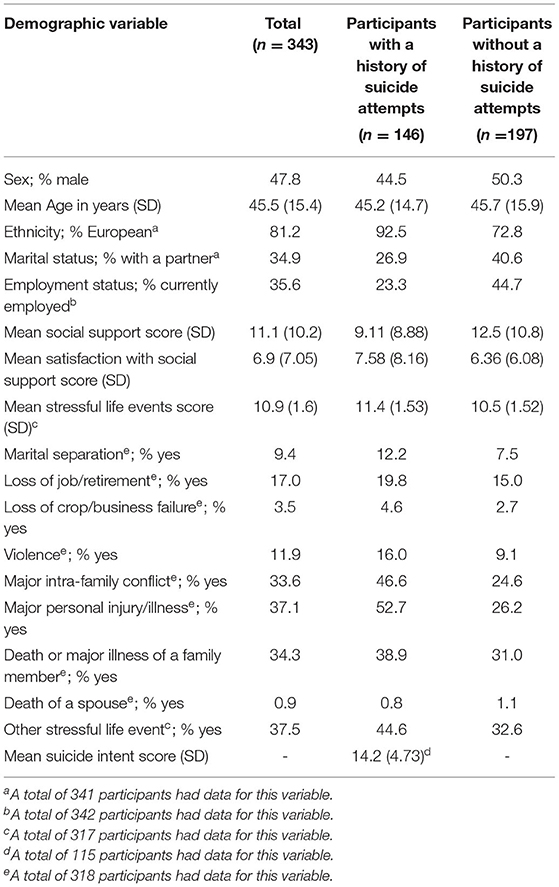
Table 1. Demographic characteristics of participants with and without a history of suicide attempts.
We found a significant association between stressful life events and suicide attempts, such that for each additional stressful life event, the odds of having a suicide attempt were 1.440 times greater (OR 1.440, 95% CI 1.440, 1.682, p < 0.001; Table 2). We also found a significant association between stressful life events and social support; each additional stressful life event was associated with a decrease in social support score (B −0.785, 95% CI −1.501, −0.068, p = 0.032). Our mediation analysis, which included both perceived social support and stressful life events as independent variables, revealed significant associations between both stressful life events (OR 1.414, 95% CI 1.209, 1.655, p = 0.001) and perceived social support (OR 0.967, 95% CI 0.942, 0.993, p = 0.013) and suicide attempt. The OR for stressful life events decreased from 1.440 in the first analysis to 1.414 in the mediation analysis, however, this effect did not reach the threshold of statistical significance when the Sobel's test was conducted (test statistic 1.64, p = 0.100). Details on the models used to conduct mediation analyses can be found in Table 2.
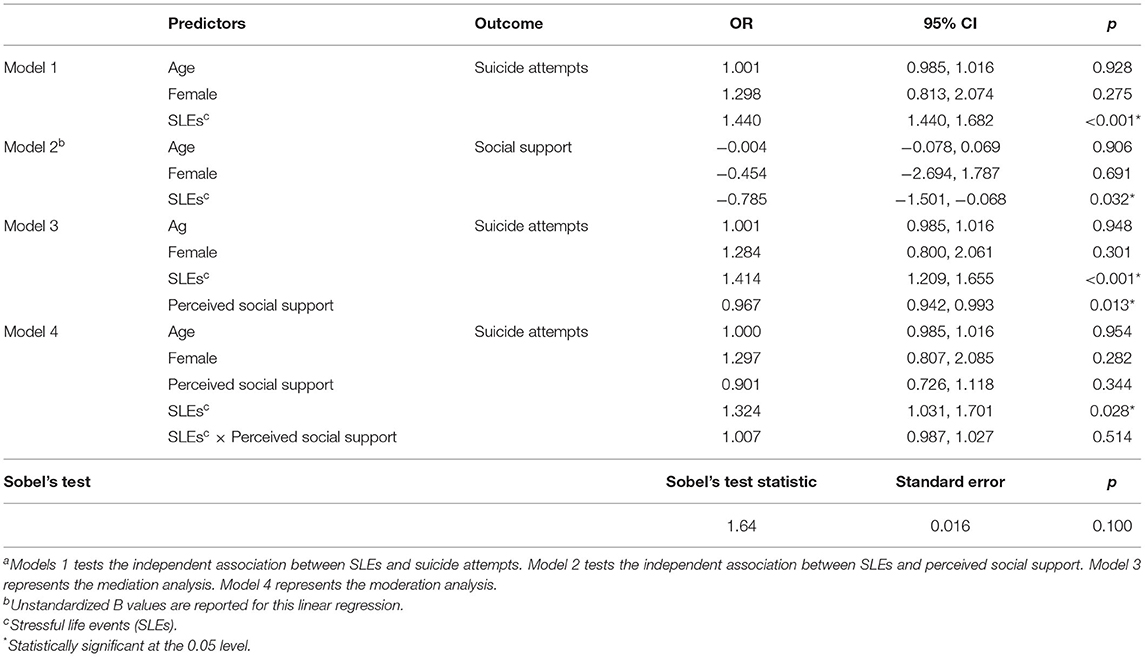
Table 2. Logistic and linear regression results from mediation and moderation analyses with suicide attempts as the outcomea.
Perceived social support was not a moderator of the association between stressful life events and suicide attempt, as evidenced by a non-significant interaction effect between perceived social support and stressful life events (OR 1.007, 95% CI 0.987, 1.027, p = 0.514; Table 2).
We did not find a significant association between stressful life events and level of suicidal intent reported by participants (B 0.040, 95% CI −0.571, 0.652, p = 0.896; Table 3). No mediation effect of perceived social support could be detected (Table 3).
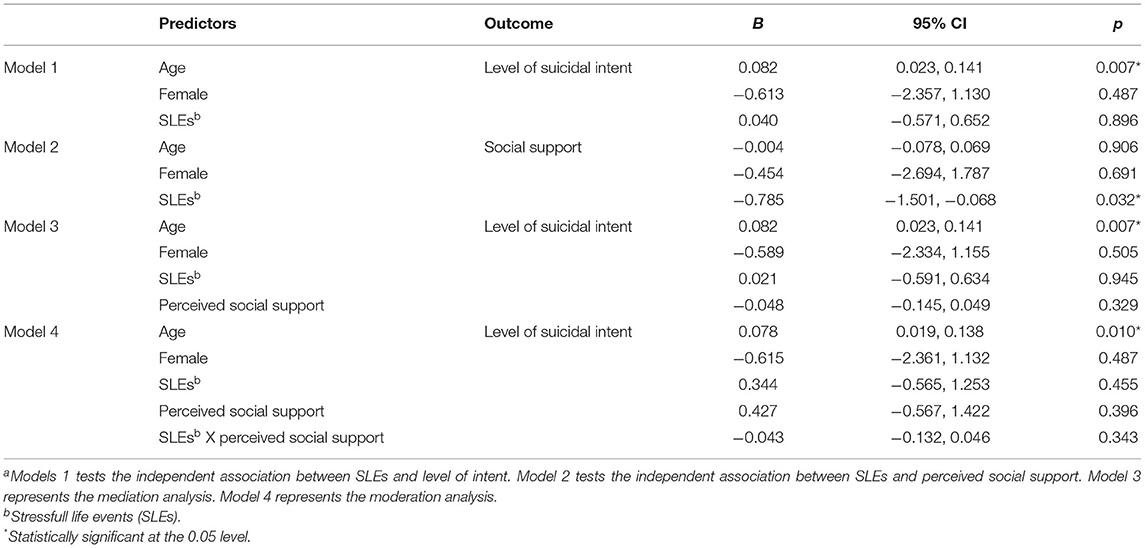
Table 3. Linear regression results from mediation and moderation analyses with level of suicide intent as the outcomea.
Perceived social support was not a moderator of the association between stressful life events and level of suicidal intent, as evidenced by a non-significant interaction effect between perceived social support and stressful life events (B −0.043, 95% CI −0.132, 0.046, p = 0.343; Table 3).
In this study, we explored the role of perceived social support as a mediator and as a moderator in the relationship between stressful life events and suicidal behavior. We identified that stressful life events were associated with increased risk of suicide attempts and social supported reduced the risk of suicide attempts, however social support did not mitigate the risk of suicide attempts when considered as an effect modifier between stressful events and suicide attempt. We used two outcome variables, the occurrence of suicide attempts and level of suicidal intent, to define suicidal behavior measures, and we did not detect any statistically significant mediation or moderation effects of perceived social support in the association between stressful life events and either of these outcome variables. Our findings are in contrast to a recent study by Yildiz et al. (32) that found perceived social support to mediate the relationship between stressful life events and suicide attempts in a sample of adolescents (32). Our contrasting finding suggests that mediation by perceived social support may not apply to this study sample of adults with suicide attempts admitted to psychiatric hospital, as the cited study was based on a general population sample with mean age of 15 years using different methods of assessing the exposure and outcome measures (32). Alternatively, Yildiz et al. included psychological distress as a partial mediator in the regression model used to assess the role of perceived social support, and the authors state that all variables in the model were imperative to the significance of the mediation (32), which presents the possibility that there may be reason to include a measure of psychological distress in the regression model to adequately assess the mediation effects of perceived social support.
Although there is evidence for moderation by perceived social support (27, 28, 46), and indication in literature that the effect of stress on suicide differs according to differing perceived social support, this was not seen in our study. The studies looking at the moderation effects of perceived social support in the investigated association often included specific populations such as transgender youth (28), women with breast cancer (33), African children diagnosed with HIV (27), and as such, the moderating effect by perceived social support may not be present in our population of psychiatric inpatients with a history of suicidal behavior. Studies conducted in different populations used alternative measures to define perceived social support. For instance, the study on transgender youth used a perceived social support scale that limited responses to friends, significant others, and family (28), whereas the perceived social support measures used in our study do not limit the participant's responses to the type of individual providing the support. Thus, it may be important to evaluate perceived social support from different support figures within the psychiatric population and re-examine their moderating effects.
Despite not detecting mediating or moderating effects of perceived social support, we did find significant associations independently between stressful life events and suicide attempts, and stressful life events and perceived social support. The significance of the independent associations between stressful life events and suicide attempts (12–14), and stressful life events and perceived social support (30, 31), is consistent with what is seen in literature. Our findings lend further support for considering these factors both in statistical models and in clinical practice.
We did not find an association between stressful life events and level of suicidal intent, despite finding an association between stressful life events and suicide attempt. Although a high level of suicide intent is highly predictive of suicidal behavior as seen in literature (47), there is limited literature on the role of perceived social support in the association of stressful life events and level of suicidal intent specifically, which may provide reason as to why an independent relationship between stressful life events and suicidal intent was not established. Furthermore, there is more evidence for the association between stressful life events and severe forms of suicidal behavior such as suicide attempts, as evidenced by a review looking at the association between stressful life events and suicidal behavior in 95 independent studies (29). Thus, when investigating the role of perceived social support in this association, it may be necessary to define the outcome using specific definition of suicidal behavior such as suicide attempt.
This is a cross sectional study limiting the inferences of the associations between stressors and suicide attempts. Furthermore, the stressful life events were reliant on self-report and subject to recall bias. Another limitation of this study is that the perception of social support is relative to the time of recruitment, whereas the participant's suicide attempt predates the time of recruitment and completion of the questionnaires. As such the reported perception of social support at the time of recruitment may have a different relevance on a suicide attempt that has occurred previously. Future directions may consider completing such assessments closer to the time of the suicidal behavior when feasible. An additional limitation regarding the stressful life events is that the scale used for data collection did not have objective weightings associated with the listed events. Thus, it may be important for future research to explore these analyses while also giving weightings to the stressful life events as different life events may have varying levels of impact predates the time of recruitment and completion of the questionnaires relevance Previously. may consider completing such assessments closer to the time of the suicidal behavior when feasible additional not withstanding these limitations, the study provides further data into the role of stressful life events and perceived social support in the association with suicidal behavior in a high-risk group of patients with psychiatric disorders and suicide attempts admitted to psychiatric hospital.
This study explored the role of perceived social support in the association between stressful life events and suicidal behavior. We found that perceived social support did not act as a mediator or moderator in the investigated association, but there were significant independent relationships between stressful life events and perceived social support and stressful life events and suicide attempts. There is limited evidence on the association between stressful life events and perceived social support, and as such, our study adds to literature by providing evidence for this association in a psychiatric population. The results from this study also reinforce the importance of screening for variables such as stressful events and low perceived social support in the psychiatric population, in order to adequately assess risk for suicidal behavior. Future directions should include the investigation of the role of perceived social support as a mitigating factor in reducing the risk of suicide. Further investigations into the role of perceived social support in outcomes with different aspects of suicidal behavior will also provide clarification on the role of perceived social support in reducing suicidal behavior.
The raw data and related information supporting the conclusions of this article can be made available upon request.
The studies involving human participants were reviewed and approved by the study was approved by the Hamilton Health Sciences (#10-661) and St. Joseph's Healthcare (#11-3479) Research Ethics Boards. The patients/participants provided their written informed consent to participate in this study.
ZS conceived the study and outlined study design and implementation. BP wrote the study manuscript, including the introduction, methods, results, and discussion. TR and MR contributed to the methods section and helped draft the methods and results sections of the manuscript. NS, NB-M, AH, CC, AD'E, LM, LT, and ZS provided feedback and edits for the manuscript. All authors have read and approved this manuscript.
This study from which this article has drawn data from was supported by a Brain and Behavior Research Foundation Young Investigator Grant (#19058) awarded to ZS (39). The Brain Behaviour and Research Foundation does not have any role in study design, analysis or reporting of results.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. WHO|Suicide Data. (2018). Available online at: http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/ (accessed January 18, 2019).
2. Jeon HJ. Depression and suicide. J Korean Med Assoc. (2011) 54:370. doi: 10.5124/jkma.2011.54.4.370
3. Goldman ML, Shah RN, Bernstein CA. Depression and suicide among physician trainees: recommendations for a National response. JAMA Psychiatry. (2015) 72:411–2. doi: 10.1001/jamapsychiatry.2014.3050
4. Takahashi Y. Depression and suicide. Jpn Med Assoc J. (2001) 44:359–63. https://www.med.or.jp/english/pdf/2001_08/359_363.pdf
5. Wålinder J, Rutz W. Male depression and suicide. Int Clin Psychopharmacol. (2001) 16:S21. doi: 10.1097/00004850-200103002-00004
6. Wetzel RD, Margulies T, Davis R, Karam E. Hopelessness, depression, and suicide intent. J Clin Psychiatry. (1980) 41:159–60.
7. Qin P, Agerbo E, Mortensen PB. Suicide risk in relation to family history of completed suicide and psychiatric disorders: a nested case-control study based on longitudinal registers. Lancet. (2002) 360:1126–30. doi: 10.1016/S0140-6736(02)11197-4
8. Roy A. Family history of suicide. Arch General Psychiatry. (1983) 40:971–4. doi: 10.1001/archpsyc.1983.01790080053007
9. Runeson B, Åsberg M. Family history of suicide among suicide victims. AJP. (2003) 160:1525–6. doi: 10.1176/appi.ajp.160.8.1525
10. Bagge CL, Glenn CR, Lee H-J. Quantifying the impact of recent negative life events on suicide attempts. J Abnormal Psychol. (2013) 122:359–68. doi: 10.1037/a0030371
11. Paykel ES, Prusoff BA, Myers JK. Suicide attempts and recent life events: a controlled comparison. Arch General Psychiatry. (1975) 32:327–33. doi: 10.1001/archpsyc.1975.01760210061003
12. McFeeters D, Boyda D, O‘Neill S. Patterns of stressful life events: distinguishing suicide ideators from suicide attempters. J Affect Disord. (2015) 175:192–8. doi: 10.1016/j.jad.2014.12.034
13. Jaiswal S, Faye A, Gore S, Shah H, Kamath R. Stressful life events, hopelessness, and suicidal intent in patients admitted with attempted suicide in a tertiary care general hospital. J Postgrad Med. (2016) 62:102–4. doi: 10.4103/0022-3859.180556
14. Guillén AI, Panadero S, Rivas E, Vázquez JJ. Suicide attempts and stressful life events among female victims of intimate partner violence living in poverty in Nicaragua. Scand J Psychol. (2015) 56:349–56. doi: 10.1111/sjop.12207
15. Rosoff DB, Kaminsky ZA, McIntosh AM, Davey Smith G, Lohoff FW. Educational attainment reduces the risk of suicide attempt among individuals with and without psychiatric disorders independent of cognition: a bidirectional and multivariable Mendelian randomization study with more than 815,000 participants. Transl Psychiatry. (2020) 10:1–15. doi: 10.1038/s41398-020-01047-2
16. Nock MK. Future directions for the study of suicide and self-injury. J Clin Child Adolescent Psychol. (2012) 41:255–9. doi: 10.1080/15374416.2012.652001
17. Kamali M, Reilly-Harrington NA, Chang WC, McInnis M, McElroy SL, Ketter TA, et al. Bipolar depression and suicidal ideation: moderators and mediators of a complex relationship. J Affect Disord. (2019) 259:164–72. doi: 10.1016/j.jad.2019.08.032
18. Kwok SYCL, Gu M. Childhood neglect and adolescent suicidal ideation: a moderated mediation model of hope and depression. Prev Sci. (2019) 20:632–42. doi: 10.1007/s11121-018-0962-x
19. Schwarzer R, Schulz U. Stressful life events. J Nervous Mental Disease. (2003) 178:1–38. doi: 10.1002/0471264385.wei0902
20. Cohen S, McKay G. Social support, stress, and the buffering hypothesis: A theoretical analysis. In: Baum A, Taylor SE, Singer JE, editors. Handbook of Psychology and Health, 4th Edn. Oxfordshire: Routledge (1984). p. 253–67. doi: 10.1201/9781003044307-10
21. Chou K-L, Chi I. Stressful life events and depressive symptoms: social support and sense of control as mediators or moderators? Int J Aging Hum Dev. (2001) 52:155–71. doi: 10.2190/9C97-LCA5-EWB7-XK2W
22. Brailovskaia J, Teismann T, Margraf J. Positive mental health, stressful life events, and suicide ideation. Crisis. (2020) 41:383–8. doi: 10.1027/0227-5910/a000652
23. Tham S-G, Ibrahim S, Hunt IM, Kapur N, Gooding P. Examining the mechanisms by which adverse life events affect having a history of self-harm, and the protective effect of social support. J Affect Disord. (2020) 263:621–8. doi: 10.1016/j.jad.2019.11.037
24. Odafe MO, Salami TK, Walker RL. Race-related stress and hopelessness in community-based African American adults: moderating role of social support. Cultural Diversity Ethnic Minority Psychol. (2017) 23:561–9. doi: 10.1037/cdp0000167
25. Ouyang M, Gui D, Cai X, Yin Y, Mao X, Huang S, et al. Stressful life events and subjective well-being in vocational school female adolescents: the mediating role of depression and the moderating role of perceived social support. Front Psychol. (2021) 11:603511. doi: 10.3389/fpsyg.2020.603511
26. Panagioti M, Gooding PA, Taylor PJ, Tarrier N. Perceived social support buffers the impact of PTSD symptoms on suicidal behavior: implications into suicide resilience research. Comprehensive Psychiatry. (2014) 55:104–12. doi: 10.1016/j.comppsych.2013.06.004
27. Casale M, Boyes M, Pantelic M, Toska E, Cluver L. Suicidal thoughts and behaviour among South African adolescents living with HIV: can social support buffer the impact of stigma? J Affect Disord. (2019) 245:82–90. doi: 10.1016/j.jad.2018.10.102
28. Trujillo MA, Perrin PB, Sutter M, Tabaac A, Benotsch EG. The buffering role of social support on the associations among discrimination, mental health, and suicidality in a transgender sample. Int J Transgenderism. (2017) 18:39–52. doi: 10.1080/15532739.2016.1247405
29. Liu RT, Miller I. Life events and suicidal ideation and behavior: a systematic review. Clin Psychol Rev. (2014) 34:181–92. doi: 10.1016/j.cpr.2014.01.006
30. Kaniasty K, Norris F. A test of the social support deterioration model in the context of natural disaster. J Personal Soc Psychol. (1993) 64:395–408. doi: 10.1037/0022-3514.64.3.395
31. Norris FH, Kaniasty K. Received and perceived social support in times of stress: a test of the social support deterioration deterrence model. J Personal Soc Psychol. (1996) 71:498–511. doi: 10.1037/0022-3514.71.3.498
32. Yildiz M. Stressful life events and adolescent suicidality: an investigation of the mediating mechanisms. J Adolesc. (2020) 82:32–40. doi: 10.1016/j.adolescence.2020.05.006
33. Mineka S, Kihlstrom JF. Unpredictable and uncontrollable events: a new perspective on experimental neurosis. J Abnorm Psychol. (1978) 87:256–271. doi: 10.1037/0021-843X.87.2.256
34. Bp D. The role of adversity and stress in psychopathology: some evidence and its implications for theory and research. J Health Soc Behav. (2000) 41:1–19. doi: 10.2307/2676357
35. Moller CI, Cotton SM, Badcock PB, Hetrick SE, Berk M, Dean OM, et al. Relationships between different dimensions of social support and suicidal ideation in young people with major depressive disorder. J Affect Disord. (2021) 281:714–20. doi: 10.1016/j.jad.2020.11.085
36. Rowe JL, Conwell Y, Schulberg HC, Bruce ML. Social support and suicidal ideation in older adults using home healthcare services. Am J Geriatr Psychiatry. (2006) 14:758–66. doi: 10.1097/01.JGP.0000218324.78202.25
37. Miller AB, Esposito-Smythers C, Leichtweis RN. Role of social support in adolescent suicidal ideation and suicide attempts. J Adolesc Health. (2015) 56:286–92. doi: 10.1016/j.jadohealth.2014.10.265
38. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. (2007) 370:1453–7. doi: 10.1016/S0140-6736(07)61602-X
39. Samaan Z, Bawor M, Dennis BB, El-Sheikh W, DeJesus J, Rangarajan S, et al. Exploring the determinants of suicidal behavior: conventional and emergent risk (DISCOVER): a feasibility study. Pilot Feasibility Stud. (2015) 1:17. doi: 10.1186/s40814-015-0012-4
40. Eisen RB, Perera S, Bawor M, Dennis BB, Bhatt M, Zielinski L, et al. Sex differences in social risk factors for suicidal behaviour. Mental Health Prevent. (2017) 8:1–6. doi: 10.1016/j.mhp.2017.08.003
41. Sarason IG, Levine HM, Basham RB, Sarason BR. Assessing social support: the social support questionnaire. J Personal Soc Psychol. (1983) 44:127–39. doi: 10.1037/0022-3514.44.1.127
42. Pierce DW. Suicidal intent in self-injury. Br J Psychiatry. (1977) 130:377–85. doi: 10.1192/bjp.130.4.377
43. Sisask M, Kõlves K, Värnik A. Severity of attempted suicide as measured by the pierce suicidal intent scale. Crisis. (2009) 30:136–43. doi: 10.1027/0227-5910.30.3.136
45. Interactive Mediation Tests. Available online at: http://quantpsy.org/sobel/sobel.htm (accessed March 29, 2021).
46. Tang GX, Yan PP, Yan CL, Fu B, Zhu SJ, Zhou LQ, et al. Determinants of suicidal ideation in gynecological cancer patients. Psychooncology. (2016) 25:97–103. doi: 10.1002/pon.3880
Keywords: suicide, mediation, moderation, stressful life events, social support
Citation: Panesar B, Rosic T, Rodrigues M, Sanger N, Baptist-Mohseni N, Hillmer A, Chawar C, D'Elia A, Minuzzi L, Thabane L and Samaan Z (2021) The Role of Perceived Social Support in the Association Between Stressful Life Events and Suicidal Behavior. Front. Psychiatry 12:699682. doi: 10.3389/fpsyt.2021.699682
Received: 23 April 2021; Accepted: 17 August 2021;
Published: 10 September 2021.
Edited by:
Gianluca Serafini, San Martino Hospital (IRCCS), ItalyReviewed by:
Eleonora Gattoni, University of Eastern Piedmont, ItalyCopyright © 2021 Panesar, Rosic, Rodrigues, Sanger, Baptist-Mohseni, Hillmer, Chawar, D'Elia, Minuzzi, Thabane and Samaan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zainab Samaan, c2FtYWFuekBtY21hc3Rlci5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.