
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 19 November 2021
Sec. Public Mental Health
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.690291
This article is part of the Research TopicPrison health is Public Health: The Right to Equitable HealthcareView all 7 articles
 Félix Pageau1*
Félix Pageau1* Corinne Devaud Cornaz2
Corinne Devaud Cornaz2 Isabelle Gothuey2
Isabelle Gothuey2 Helene Seaward1
Helene Seaward1 Tenzin Wangmo1
Tenzin Wangmo1 Bernice S. Elger1,2
Bernice S. Elger1,2Background: Mental healthcare and lifestyle habits in prison, especially for older individuals, has been shown to be suboptimal. Most psychiatric conditions left untreated worsen food choices, physical inactivity, and substance abuse. In turn, bad habits lead to poorer mental health.
Methods: To comprehensively illustrate this downward spiraling, we completed a thorough analysis of data obtained through semi-structured qualitative interviews. There were 50 interviews of aging incarcerated people included in this article. They were analyzed following a classical six-stepped thematic analysis.
Results: According to our participants, sports are not well-adapted to aging individuals, nor to people with medical conditions. Prison is even more unadapted for those who both are aging and have medical conditions. Also, food served is less than optimal. According to our interviews, the older imprisoned individual often does not have access to food adapted to his or her medical conditions. Sport is maladapted for older incarcerated individuals and mostly tailored for younger ones. Finally, boredom and lack of responsibility hinder change toward a better lifestyle for older adults in prison.
Conclusion: Our paper shows why prison environmental modifications are needed to help older adults with their lifestyle habits. It also exposes an original way to see the relationship between mental health and lifestyle habits.
An increasing number of imprisoned persons will reach 50 years in Western societies in the upcoming years (1, 2), and they continue to remain a neglected sub-group among the prison population (3). Incarcerated older individuals often require special care for they are more ill than their younger counterparts (4, 5). The harsh carceral environment makes the incarcerated age more rapidly and hinders their uptake of good life habits. For example, some older adults in prison lack mobility leading to exclusion from sports and leisure facilities when compared to the younger individuals (5, 6). Likewise, no specific incentives exist for older incarcerated person's participation in sports. Furthermore, older persons often do not take actions toward improvement despite their harmful lifestyle habits in prisons (7). In medicine, lifestyle habits comprise physical activities, nutrition, and consumption of drugs, alcohol, and tobacco.
Individual and systemic factors play a role in these unhealthy dynamics. Indeed, there is no specific program for lifestyle changes in prison for older individuals, even if they suffer from several health conditions such as hypertension, arthritis, chronic back pain, COPD, cardiovascular diseases, diabetes, asthma, and liver diseases (8, 9). Depending on reporting methods, 11–46% of incarcerated individuals also have at least one mental health diagnosis (4, 8, 10, 11). However, these somatic and mental health problems could be ameliorated if specific lifestyle modification programs were implemented.
In Western detention centers, imprisoned persons often gain weight due to unhealthy diet and lack of physical activity. Countries with longer duration and increased frequency of incarceration experience a rise in health problems related to unhealthy lifestyle. This is particularly present in countries with aging incarcerated individuals, and this is recognized as an important public health issue. Arnold (12) predicted an increased incidence and related consequences of non-communicable disease with the rise of aging detained individuals.
Also, a systematic analysis of body mass index and diet revealed that even young female incarcerated persons were more likely to be obese (13). These study participants had a sodium intake two to three times higher than recommended norms (13). Other authors already wrote articles on the topic in relation to physical health (14, 15).
There is a dearth of literature on mental health in prison, and even less pertaining to older incarcerated adults (16, 17). Our research is therefore explorative, since the topic has not been examined sufficiently yet, and they derive from a larger project, which aimed at understanding the older incarcerated adult's general experience on aging and mental health care in prison. This article addresses more precisely these participants' view on unhealthy lifestyle caused by imprisonment, its effect on mental health, and suggestions to make lifestyle habits better behind the bar. We follow the “Journal article reporting guidelines (JARS)” for qualitative research (18), which considered multiple qualitative guidelines when it was developed, including COREQ (19). We obtained ethics approval from our leading regional commission named Northwestern and Central Swiss Ethics Committee (translated from its German name: Ethikkommission Nordwest-und Zentralschweiz) as well as the Ethics Committee of Bern (in German: Kantonale Ethikkkommission Bern), the Cantonal Ethics Committee of Vaud on Human Research (in French: Commission cantonale d'éthique de la recherche sur l'être humain CER-VD), and Zurich Ethics Committee (in German: Ethikkommission Zürich).
From Switzerland, a total of 15 prisons and forensic-psychiatric units were included in the study. The inclusion criteria are abridged in Table 1.
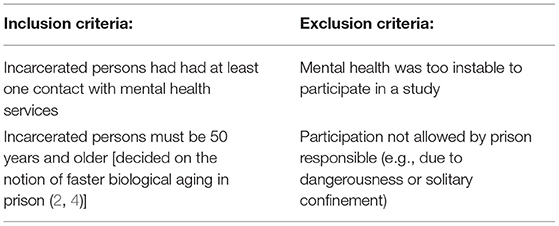
Table 1. Criteria for our study participants.
A prison contact person supported the research team with the recruitment. Our sampling methodology was purposive, that is, the contact person was informed about our study criteria and he or she distributed our study information accordingly and proceeded with providing the informed consent documents to the potential participants. This person also scheduled the interviews once the prospective participant indicated his or her willingness to talk with the researchers. Once again, on the day of the interview, the interviewer informed the participant again about the objectives of the study, reassured and stated confidentiality. Refusal to participate was still possible at this point and all time during the interview process. Thereafter, written informed consent was obtained. There was no compensation for this study participation. Interviews were held in French, Germain, Swiss-Germain, or English according to the participant preference.
In total, 57 older incarcerated individuals were interviewed for our main project. One interview was carried out for each interviewee. Interviews were held between December 2017 and December 2018. The data saturation principle led our final decisions on the total number of participants (20). Meaning that no new information was attained with the latest data (20). To follow saturation, we did data analysis while collecting our data, allowing us to decide when this point was reached. Seven interviews were excluded because of their poor quality. Hence, data from 50 older incarcerated individuals are included in this article. Table 2 recapitulates participant characteristics.
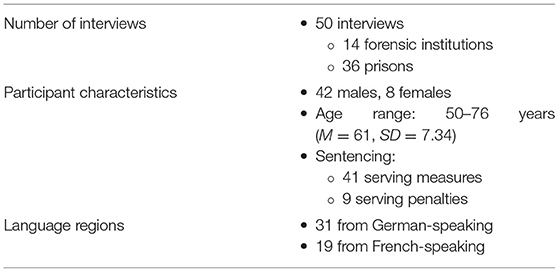
Table 2. Study participant characteristics.
Interviews were done in person, in a separate room within the facility walls. We were able to assure privacy and allow the participants to speak freely during the process. Interviewers and interviewees had not met before this project. Two research assistants conducted the interviews. They were both trained in qualitative interview techniques. They were working as PhD students at the time of interviews. The discussions took 16–120 min (M = 69, SD = 26.19). Table 3 summarizes the semi-structured interview guide.
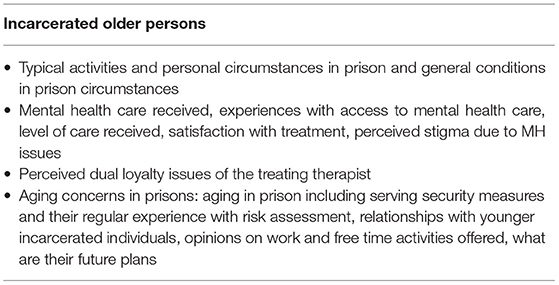
Table 3. Interview guide content.
Our team transcribed verbatim all interviews in the language used by participants. Swiss German interviews were written in Standard German, which is the norm for Swiss studies. Quality and accuracy of the transcriptions were then assessed by another of our team members. Anonymization was carried out during the process of transcription. Participants did not receive the interviews for verification upon completion.
We used a thematic analysis approach during the entire process (21) following six phases: (1) acknowledging the data, (2) creating original codes, (3) finding themes, (4) reassessing the preceding themes, (5) designating and describing themes, and (6) producing results. First, eight interview transcripts were read and used for coding. Second, memos and codes were named by team members resulting in a code tree. Third, three of our team members coded the rest of the transcripts by themselves. The same people discussed important topics and themes for subsequent papers following steps (3–5). No disagreements emerged from these discussions in relation to this paper. Hence, there has been no need for an external expert to resolve disagreement. Moreover, they examined the overall findings from the project using results of all participants and comparing them for step (5). The first author of this paper completed the analysis for this article more in depth (step 5 and 6) pertaining to bad habits and mental health. All authors supported the interpretation and writing of this article and agreed to the results presented in this paper.
Both studied settings (prisons and forensic-psychiatric units) showed similar results with regard to the following topics.
Not every incarcerated individual observes a healthy training routine. This may come from the lack of adapted sports in prison or the fear of hurting oneself. The importance of a professional guidance to encourage participation in age-appropriate physical activities transpired in our interviews. Older incarcerated individuals understood well the need for good habits. See Table 4, PQ1.
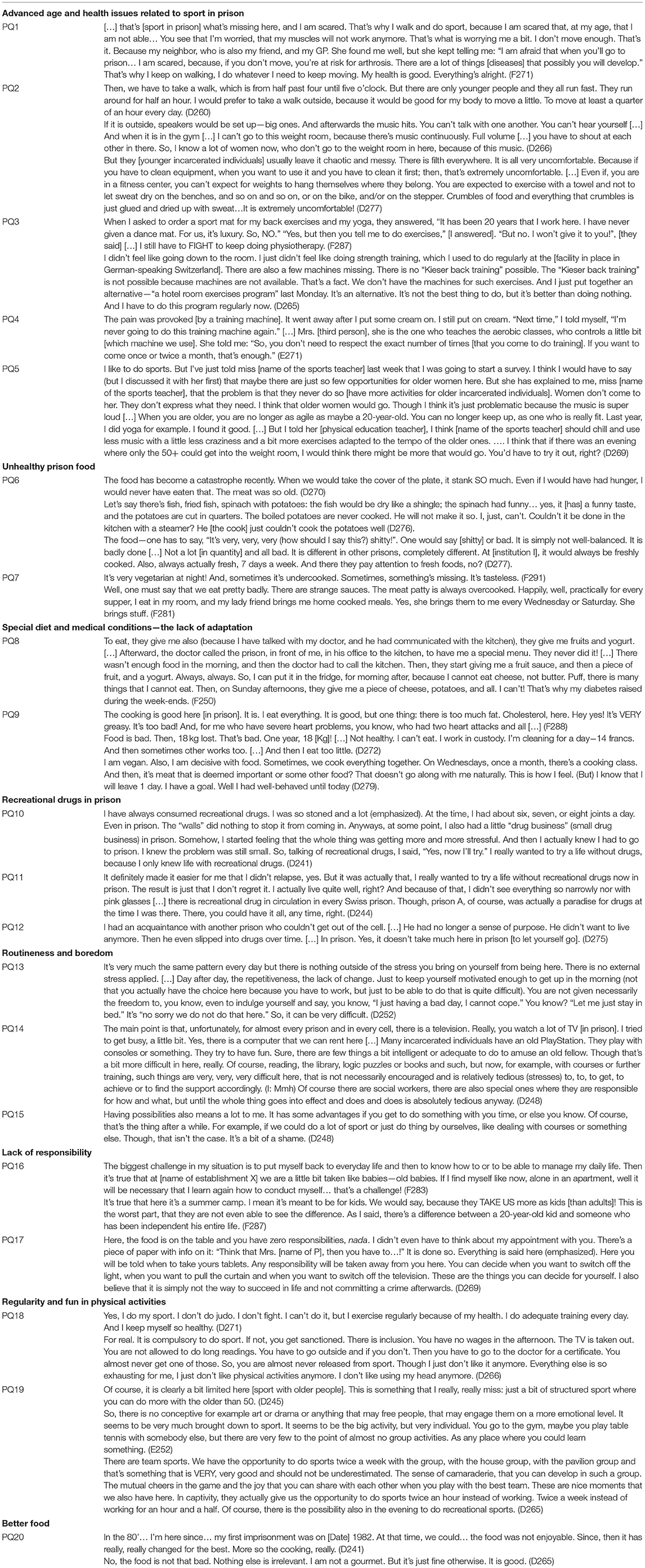
Table 4. Participants' quotes (PQ).
There is a frequently expressed discomfort from older incarcerated individuals when it comes to doing sport with younger ones. Older imprisoned individuals reported their different needs when completing physical activity than their younger counterparts. These included their need for more time to complete a less strenuous activity, the noise levels that become unbearable for them, and the inacceptable habits of younger persons in observing general rules related to the use of training equipment. These maladaptations of prison services causes a reduction of participation in sport for elders in prison. Also, they recognize the lack thereof. See Table 4, PQ2.
Even though the lack of cleanliness and loud music affect all individuals in prison, this seems to affect older ones more specifically, according to our interviews when older interviewees talked about their younger counterparts. Asked-for equipment also seemed not to be given to incarcerated individuals. One highly motivated gentleman was able to adapt his routine to prison even when needed equipment was not available. Nevertheless, not every imprisoned individual has the knowledge and motivation to do so. Especially if there is no support and even obstacles existing in the penitentiary. See Table 4, PQ3.
As incarcerated individuals get older, they experience health problems reducing their ability to participate in physical training. One incarcerated woman expressed her problem with her knees (D266). Another imprisoned individual talked about back problems (D265). Pain may be a major factor for not doing fitness training which could be adapted in certain circumstances. See Table 4, PQ4.
Adapted sport for the elderly seems to be lacking in prison as prison is also recognized as bad for health in general. Their medical conditions should lead to a better training plan and special measures for the elderly. It seems to be known by some health professionals that prison is bad for health. See Table 4, PQ5.
According to most interviewees, food is not as nutritious as expected by participants and often is mediocre in taste. “The cook cannot cook!” (D276), said one of the participants. Participants also complained about the poor quality of the meals that they received. See Table 4, PQ6.
All the above were German-speaking incarcerated individuals. French-speaking imprisoned individuals also complained about the food quality and quantity. One participant said that a friend brings him food. He is lucky that he could count on the help of a friend. Though, not everyone has this chance. So, cultural aspects related to Swiss linguistic regions did not play a major role when one talked about food. See Table 4, PQ7.
Health problems are not taken into consideration when adapting an incarcerated individual's diet. That means that special regimens are not followed. A medical prescription is demanded to obtain healthier food for some, but this is not always fulfilled accordingly. See Table 4, PQ8.
Participants reported that fatty ingredients are also exceedingly present in an incarcerated individual's diet even though this can potentially worsen health conditions. Moreover, incarcerated individuals stated that an unhealthy diet in prison is responsible for them developing health problems. See Table 4, PQ9.
Since good behaviors are a prerequisite for incarcerated individuals, an interviewee could not really tell authorities that he does not eat meat. As food is customary, everyone must eat meat and get along with it despite some of them being vegan or vegetarian.
According to some interviewees, prison appears not to be a good time to stop recreational drugs. This partakes in the negative aspects of prison on life habits. See Table 4, PQ10.
It is uncertain if the previous succeed in stopping recreational drugs. It is unclear if it got more difficult to have recreational drugs in prison, but this incarcerated individual sees imprisonment as an opportunity to stop taking those drugs. See Table 4, PQ11.
Recreational drugs are easily available and frequently used in the penitentiary. Depending on the incarcerated individual's will to stop consuming, this may lead to worsening mental health as part of bad life habits. See Table 4, PQ12.
Routineness and invariability are omnipresent in detention and was reported by many participants. See Table 4, PQ13.
This shows how prison routines may lead to a lack of spur even for people who used to be very motivated. Boredom is seen as continuous by some (D270 and See Table 4, PQ14).
Lack of activities is noticeable. “There is nothing for individuals, no group activities” (F285), one said. This results in boredom in prison. See Table 4, PQ15.
Also, we noted that responsibilities were taken away from incarcerated individuals. This, in turn, could worsen the lack of motivation to implement a healthy lifestyle. Imprisoned individuals are being treated like “children.” “We [incarcerated individuals] are infantilized! They [prison staff] make us IDIOT. They make us voluntarily stupid! I can't stand this!”, (F285) a participant said. They find that their autonomy is not promoted to the fullest. See Table 4, PQ16.
Incarcerated individuals have no or very little responsibility in their view. Subsequently, lack of impetus and responsibility to get through their daily routine is reflecting on incarcerated individuals' hindrance for changes in bad habits. See Table 4, PQ17.
As many incarcerated individuals complained about bad living conditions in prison pertaining to sport, food, and routineness, few expressed a different perspective. Their experience could help set the example for other facilities.
Regularity in physical activities integrated more easily to a daily routine renders it easy. It can be an individual choice. Although, making it a mandatory activity for all may help also to enhance sport in prison from a structural perspective. See Table 4, PQ18.
We should be careful in forcing sport on older incarcerated adults as the latter expressed his discontent. Hence, adaptations could be made for more strenuous physical activities. Walking appeared to be very popular as many imprisoned individuals explained that it is their main physical activity. “Walks maintain good health. It's well-known,” one incarcerated individual mentioned (F282). They do promenades in the courtyard which is obligatory for some (F288). As it is done more regularly, sport appears to be easily integrated in one's routine. Other positive aspects of sport could also be great motivations, apart from obligation, and routine. Incarcerated individuals suggest that sport could be an enjoyable moment between imprisoned persons, especially for older ones, if it was to be adapted to them. The spirit of communion is important in doing sport. It appeared to be an important motivation for most. Team spirit and camaraderie are reported as being very important. See Table 4, PQ19.
While many incarcerated individuals voiced their aversion to prison food, others mentioned how well they eat behind bars. See Table 4, PQ20.
So very low expectations or previous experiences in prison seem to help incarcerated individuals appreciate food when in detention centers. Nevertheless, the quality and quantity have been considered very low for most of the interviewees.
We delineate six major aspects of unhealthy lifestyle in prison. First, unadapt sport for elders prevail behind the bars. This has already been demonstrated in several articles (5, 14, 22, 23). Second, exercise equipment is either lacking or in bad condition due to poor maintenance. These two previous aspects might lead to more inactive lifestyle on the part of older incarcerated individuals, leading to health decline (5, 14). As already mentioned, thus far, neither the prison infrastructures nor the organization of activities has been designed for elderly people, neither in Switzerland nor in other countries. Third, many incarcerated individuals complained about the food quality and quantity. Food is starchy or fatty in prison according to interviewees. Furthermore, the adjustment of diets for specific medical condition is lacking (5, 16). Incarcerated individuals experience worsening of their health condition because of the preceding and might be related to earlier aging (2, 4). Forth, it is unclear if prison exacerbates drug consumption according to our participants. However, a Swiss study reported that older incarcerated individuals usually consume less drugs but more alcohol according to literature on the topic (16). Fifth, boredom and routineness do not help incarcerated individuals to make changes in their unhealthy lifestyles. Last, our results show that lack of responsibilities also hinder change for imprisoned persons. Motivation is essential to promote a change toward a better lifestyle. The monotony and lack of challenges may affect one's perspective on life changes. This may cause an unwillingness to adhere to a better lifestyle. Therefore, the penitentiary is a burden for change and contributes to a downward spiraling of bad habits. Since an unhealthy lifestyle leads to poorer mental health (15, 24) and in turn poor mental health to an unhealthy lifestyle (25), this creates a downward spiraling of unhealthy lifestyle and poor mental health (Figure 1).
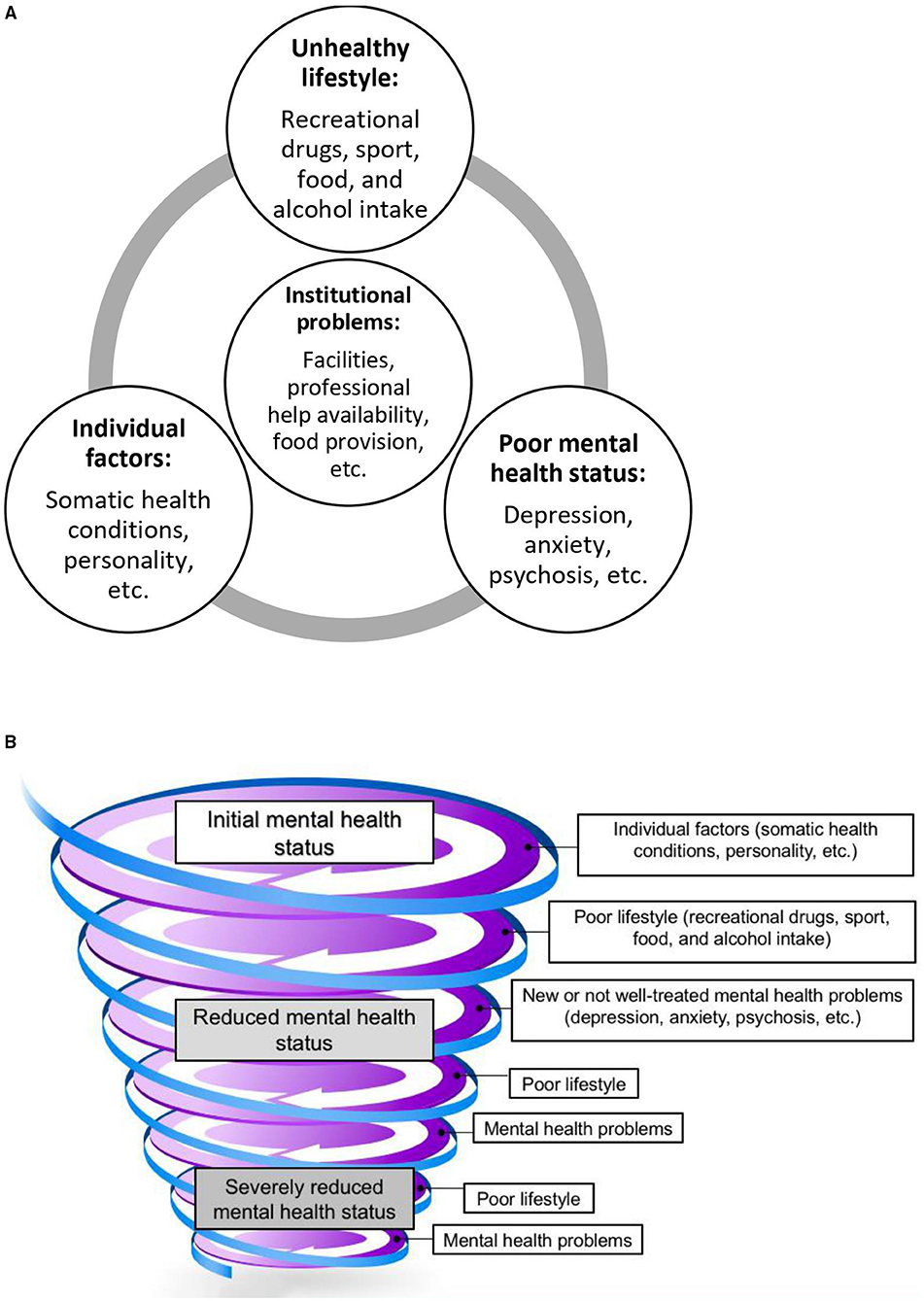
Figure 1. Downward spiraling of unhealthy lifestyle and poor mental health. (A) Interactions between factors pertaining to mental health. (B) Downward spiraling.
We need to address this pressing issue of bad habits and mental health of older adults in prison. We use a downward spiraling framework to organize our ideas as it presents a useful approach to connect different factors with one another. This framework was conceived by our team following knowledge of the recent literature on these topics, independently from our data, as a skeleton with which our data was conceptually organized. Similar to our proposed framework, another interesting model is that of Fredrickson and colleagues, who reported that the upward spirals of positive emotions counter downward spirals of negativity (26). Although it is not prison specific, it shows how psychosocial components interfere with positive and negative emotions. It also shows how a downward spiraling model can theorize psychological and psychiatric problems. Nevertheless, it lacks a few components of the spiraling model that we put forth, such as lifestyle habits and institutional factors.
Our framework (Figures 1A,B) therefore presents a useful approach to illustrate the connectedness of different factors which could consequently be investigated by future research. The pathological relationship between mental health problems and poor lifestyle is well-known (27). Sleep disorders, loss or gain in appetite, fatigue, and lack of motivation can be symptoms of mental illnesses. These can lead to a worsening lifestyle because of the lack of motivation to eat well, do sport, and be sober. The lack of adapted physical and mental activity, as well as a healthy diet in prison worsen these further. In turn, bad habits negatively impact mental health (24, 28). Worsening of mental health then leads to a decline in lifestyle habits, thus creating a downward spiraling (Figures 1A,B). Our proposed descriptive framework may allow policy makers and prison personnel to seek to address these varying concerns as a whole and not target the pieces. Taking a piecemeal approach does not produce much needed improvement in health and well-being of the prisoners, and thereby cost-efficient prison administration.
In prison, as shown by our interviewees, the environment is deleterious. It contributes to downward spiraling and hinders a lifestyle change. Poor mental health should be treated with psychotherapy in an integrative approach (29) to gain access to a healthy lifestyle modification if needed. Prison offers a unique opportunity for change. It can be health-arming or health-promoting (30). Nowadays, many mental health professionals are promoting an integrative approach to treat psychiatric conditions (27, 29, 31). These experts campaigned for the prevention and treatment of mental health conditions through healthy lifestyle such as regular physical activity, wholesome food, and sobriety. Hence, individual and institutional aspects need to be addressed to better treat mental health conditions. Indeed, the WHO report on mental illness mentioned that the mental health determinants are not only individual factors, but also environmental and socials factors (32). Consequently, poor mental health is at the interface of many determinants such as physical health, physical inactivity (24, 33), discrimination, disrespect of human rights, and many others. These factors are particularly significant and manifest in prison because the environmental factors are predominantly influential.
Even though prisons can be deleterious for the elders incarcerated there, the penitentiary has shown to have some positive aspects. In some prisons, food and exercise are well-balanced according to a few of our interviewees. One participant (D271) has shown resilience and maintained regular physical activity despite being detained, although he was the only interviewee showing such an attitude toward sport. Those examples show that change is possible, since good conditions existed in some prisons. Thus, we need to address the problem of detention institutions which are not health-promoting. Our findings are important because they present the aging imprisoned individual's perspective. Although our results are similar to what is known with similar studies on younger imprisoned individuals about psychotropic medication (34), racial disparities, and prison experience of care (35, 36), it fills in part of the well-known (by clinicians and researchers) lack of literature on the older incarcerated persons (16, 17). In doing so, we further substantiate the poor conditions of the prison infrastructure and add to the calls to improve the care given to prisoners in order to halt the downward spiraling of bad habits in prisons. Doing so will not only be beneficial for the health and well-being of the individual prisoner but also the prison system as a whole.
Although we sought to reduce our result biases diligently through various methods, they might still be inherent to our study and study design. First, social acceptability is a common limitation to qualitative studies. That is, participants might not say what they think but rather what they think investigators want to hear or what is socially right. To account for this bias, we assured anonymity and confidentiality to limit its impact. Second, volunteering bias might limit the strength of our results. We accounted for this through saturation. We were able to observe variation and multiple themes. Third, interviews were done in the participant language of choice and translated to English for this article. Some elements might have been lost due to translation. Our international team who encompasses French, German, Swiss-German, and English speakers reviewed translations to reduce biases due to translation. Fourth, our study included only older persons deprived of liberty with mental health problems. However, we could assume that similar factors affect everyone who is incarcerated. As our study sample is unique, it could be argued that they have more problems. If this is the case, it is important to help affected individuals even though they might be a minority. Finally, the sample is not representative of all older prisoners in Switzerland because generalization is not a goal of a qualitative methodology. Instead, purposive sampling in qualitative studies aims at collecting a high variability of opinions and different situations.
Many studies on incarcerated adults and psychiatric patients have come to the same conclusion (34–36). However, there is a scarcity of research when it comes to the older imprisoned adult with mental health problems (16, 17), which our study findings address. Thus, our project gave voice to older imprisoned adults, and we have incorporated our results within this topic of bad habits in a downward spiraling framework. Prisons hinder change and worsen poor lifestyle; thus, contributing to the downward spiraling of mental health and bad habits. Because a healthy lifestyle is key for mental health care, we hope for a change of mentalities in prison. Our research outlined the problems related to lifestyle in prison. Food, sport equipment, and opportunity for change are desperately lacking behind the bars according to our participants. This would help imprisoned individuals to break out of the downward spiraling of bad mental health and unhealthy lifestyle. To paraphrase Victor's writing: the force of a democracy can be measured by the way it treats his child, his older and his incarcerated individuals (37). We hope for a change pertaining to lifestyle and mental health in prisons for the older incarcerated persons, as more and more mental health professionals are promoting a more integrative approach for the treatment of mental illnesses (27, 29, 31).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Northwestern and Central Swiss Ethics Committee (translated from its German name: Ethikkommission Nordwest-und Zentralschweiz) as well as the Ethics Committee of Bern (in German: Kantonale Ethikkkommission Bern), the Cantonal Ethics Committee of Vaud on Human Research (in French: Commission cantonale d'éthique de la recherche sur l'être humain CER-VD), and Zurich Ethics Committee (in German: Ethikkommission Zürich). The patients/participants provided their written informed consent to participate in this study.
BE and TW designed the project. HS contributed to data collection. HS, TW, and FP analyzed data of the project. Specific analysis was carried out by FP and validated by all co-authors. FP wrote the manuscript. All co-authors read draft versions of it, provided critical and useful suggestions to improve the quality and precision of our data analysis, and thus the quality of the overall manuscript. All authors approved the final version submitted for publication and take responsibility for its content.
This work was part of the larger research project Agequake in prisons—second part: Mental health care and forensic evaluation of aging prisoners and persons serving security measures in Switzerland and was supported by the Swiss National Science Foundation (Grant Number: 166043).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all our participants who shared their time and experiences with us. We thank Sophie Haesen and Arnaud Imber who contributed to data collection. We thank our team of research assistants who transcribed the interviews and corrected the transcribed documents: Antonina Brunner, Chiara Andenmatten, Déborah Schorno, Emely Schweizer, Flavienne Bieri, Laryssa Grosjean, Laudelina Taboas Hidalgo, Leila Meyer, Luisa Waschkowski, Sabrina Wenger, Sasa Pospisilova, Sophie Dieffenbacher, Valentina Memma, Vivianne Götz, Bianca Ballaman, Ziad Kassem, and Yael Becker.
1. Hayes AJ. Ageing inside: older adults in prison. In: Elger B, Ritter C, Stöver H, editors. Emerging Issues in Prison Health. Dordretch: Springer (2012). p. 1–12.
2. Merkt H, Haesen S, Meyer L, Kressig R, Elger BS, Wangmo T. Defining an age cut-off for older offenders: a systematic review of literature. Int J Prison Health. (2020) 16:95–116. doi: 10.1108/IJPH-11-2019-0060
3. Frazer L. Ageing Inside. School for Policy Studies Working Paper Series Paper Number 1. Bristol: University of Bristol (2003).
4. Hayes A, Burns A, Turnbull P, Shaw J. The health and social needs of older male prisoners. Int J Geriatr Psychiatry. (2012) 27:1155–62. doi: 10.1002/gps.3761
5. Wangmo T, Handtke V, Bretschneider W, Elger BS. Improving the health of older prisoners: nutrition and exercise in correctional institutions. J Correctional Health Care. (2018) 24:352–64. doi: 10.1177/1078345818793121
6. Her Majesty's Inspectorate of Prisons (HMIP London). ‘No Problem- Old and Quiet’: Older Prisoners in England and Wales. A Thematic Review. London: HMIP (2004).
7. Hayes AJ, Shaw J. Practice into policy: the need of elderly prisoners in England and Wales. Prison Service J. (2011) 143:38–45.
8. Baillargeon J, Black S, Pulvino J, Dunn K. The disease profile of Texas prison inmates. Ann Epidemiol. (2000) 10:74–80. doi: 10.1016/S1047-2797(99)00033-2
9. Hornung CA, Greifinger RB, Gadre S. A projection Model of Selected Chronic Diseases in the Inmate Population. In: National Commission on Correctional Health Care, editor. The Health Status of Soon-To-Be-Released Inmates: A Report to Congress, Vol. 2. Report. Document Number No.: 189736. Award No.: 97-IJ-CX-K018. Sponsored by the U.S. Department of Justice. Chicago, IL: NCCHC (2004). p. 39–56.
10. Brown GP, Brozowski K. Golden years? The incarceration of older offender. Geriatric Today. (2003) 6:32–5.
11. Caverley SJ. Older mentally ill inmates: a descriptive study. J Correctionnal Health Care. (2006) 12:262–8. doi: 10.1177/1078345806295546
12. Arnold FW. Non-communicable diseases in prisons. Lancet. (2012) 379:1931–3. doi: 10.1016/S0140-6736(12)60471-1
13. Herbert K, Plugge E, Foster C, Doll H. Prevalence of risk factors for non-communicable diseases in prison populations worldwide: a systematic review. Lancet. (2012) 379:1975–82. doi: 10.1016/S0140-6736(12)60319-5
14. Elger BS. Prison life: television, sports, work, stress and insomnia in a remand prison. Int J Law Psychiatr. (2009) 32:74–83. doi: 10.1016/j.ijlp.2009.01.001
15. Collin C, Assmann KE, Andreeva VA, Lemogne C, Hercberg S, Galan P, et al. Adherence to dietary guidelines as a protective factor against chronic or recurrent depressive symptoms in the French SU.VI.MAX cohort. Prev Med. (2016) 91:335–43. doi: 10.1016/j.ypmed.2016.09.001
16. Moschetti K, Stadelmann P, Wangmo T, Holly A, Bodenmann P, Wasserfallen JB, et al. Disease profiles of detainees in the Canton of Vaud in Switzerland: gender and age differences in substance abuse, mental health and chronic health conditions. BMC Public Health. (2015) 15:872. doi: 10.1186/s12889-015-2211-6
17. Haesen S, Merkt H, Imber A, Elger BS, Wangmo T. Substance use and other mental health disorders among older prisoners. Int J Law Psychiatr. (2019) 62:20–31. doi: 10.1016/j.ijlp.2018.10.004
18. Levitt H, Bamberg M, Creswell JW, Frost D, Josselson R, Suarez-Orozco C. Journal article reporting standards for qualitative primary, qualitative meta-analytic, and mixed methods research in psychology. APA Publ Commun Board Task. (2018) 73:26–46. doi: 10.1037/amp0000151
19. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health C. (2007) 19:349–57. doi: 10.1093/intqhc/mzm042
20. Fusch P, Ness L. Are we there yet? Data saturation in qualitative research. Qual Rep. (2015) 20:1408–16. doi: 10.46743/2160-3715/2015.2281
21. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
22. Bretschneider W, Elger BS. Expert perspectives on Western European Prison Health services: do ageing prisoners receive equivalent care? Bioethical Inquiry. (2014) 11:3. doi: 10.1007/s11673-014-9547-y
23. Elger BS. A balanced diet – from facts to solutions. In: Elger BS, Critter C, Stöver H, editors. Emerging Issues in Prison Health. Heidelberg: Springer (2017). p. 107–21.
24. Schuch F, Vancampfort D, Firth J, Rosenbaum S, Ward P, Reichert T, et al. Physical activity and sedentary behavior in people with major depressive disorder: a systematic review and meta-analysis. J Affect Disord. (2016) 210:139–50. doi: 10.1016/j.jad.2016.10.050
25. Wirnick E, Meneton P, Empana J-P, Siemiatycki J, Hoertel N, Vulser H, et al. Cardiovascular risk goes up as your mood goes down: interaction of depression and socioeconomic status in determination of cardiovascular risk in the COSTANCES cohort. Int J Cardiol. (2018) 262:99–105. doi: 10.1016/j.ijcard.2018.02.033
26. Garland EL, Fredrickson B, Kring AM, Johnson DP, Meyer PS, Penn DL. Upward spirals of positive emotions counter downward spirals of negativity: insights from the broaden-and-build theory and affective neuroscience on the treatment of emotion dysfunctions and deficits in psychopathology. Clin Psychol. (2010) 30:849–64. doi: 10.1016/j.cpr.2010.03.002
27. Bochicchio L, Stefancic A, Gurdak K, Swarbrick M, Cabassa LJ. “We're all in this together”: peer-specialist contributions to a healthy lifestyle intervention for people with serious mental illness. Adm Policy Ment Health. (2019) 46:298–310. doi: 10.1007/s10488-018-0914-6
28. Li Y, Lv MR, Wei YJ, Sun L, Zhang HG, Li B. Dietary patterns and depression risks: a meta-analysis. Psychiatry Res. (2017) 253:373–82. doi: 10.1016/j.psychres.2017.04.020
29. Lopresti AL. It is time to investigate integrative approaches to enhance treatment outcomes for depression? Med Hypotheses. (2019) 126:82–94. doi: 10.1016/j.mehy.2019.03.008
30. Prost SG, Archuleta AJ, Golder S. Older adults incarcerated in state prison: health and quality of life disparities between age cohorts. Ageing Mental Health. (2021) 25:260–8. doi: 10.1080/13607863.2019.1693976
31. Sayer J, Panjagua D, Ballentine S, Sheehan L, Carson M, Nieweglowski K, et al. Perspectives on diet and physical activity among urban african americans with serious mental illness. Social Work Health Care. (2019) 58:509–25. doi: 10.1080/00981389.2019.1587662
32. World Health Organization (WHO). Mental Health-Action Plan 2013-2020. WHO (2013). Available online at: https://apps.who.int/iris/bitstream/handle/10665/89966/9789241506021_eng.pdf;jsessionid=EE3B62E05104A793EBC40684C239E55B?sequence=1 (accessed March 10, 2021).
33. Zhai L, Zhang Y, Zhang D. Sedentary behavior and the risk of depression: a meta-analysis. Br J Sports Med. (2015) 49:705–9. doi: 10.1136/bjsports-2014-093613
34. Bowen RA, Rogers A, Shaw J. Medication management and practices in prison for people with mental health problems: a qualitative study. Int J Mental Health Syst. (2009) 3:24. doi: 10.1186/1752-4458-3-24
35. Binswanger IA, Redmond N, Steiner JF, Hicks LS. Health disparities and the criminal justice system: an agenda for further research and action. J Urban Health. (2011) 89:98–107. doi: 10.1007/s11524-011-9614-1
Keywords: lifestyle-related disease, mental health care, prison, physical activity, food
Citation: Pageau F, Cornaz CD, Gothuey I, Seaward H, Wangmo T and Elger BS (2021) Prison Unhealthy Lifestyle and Poor Mental Health of Older Persons—A Qualitative Study. Front. Psychiatry 12:690291. doi: 10.3389/fpsyt.2021.690291
Received: 02 April 2021; Accepted: 22 October 2021;
Published: 19 November 2021.
Edited by:
Heino Johann Stöver, Frankfurt University of Applied Sciences, GermanyReviewed by:
Ronald Burian, Evangelische Krankenhaus Königin Elisabeth Herzberge (KEH), GermanyCopyright © 2021 Pageau, Cornaz, Gothuey, Seaward, Wangmo and Elger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Félix Pageau, ZmVsaXgucGFnZWF1QHVuaWJhcy5jaA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.