 Adrienn Rivnyák
Adrienn Rivnyák Bernadette Péley
Bernadette Péley András Láng
András Láng- Faculty of Humanities and Social Sciences, Institute of Psychology, University of Pécs, Pécs, Hungary
Growing evidence shows that diagnosing and treating borderline personality disorder (BPD) is of high relevance for affected youths. Although identity crisis is part of the normative developmental process, identity diffusion is a potential candidate for being an appropriate concept in further developing screening tools and interventions for BPD treatment in adolescence. We hypothesized that severity of borderline traits (as indicated by the strength of their associations with identity diffusion) would be negatively associated with non-clinical adolescents' endorsement of borderline features' presence. We also hypothesized that identity diffusion had a central role in the network of borderline personality traits and could be conceived of as a latent organizing principle of borderline personality disorder. In our study, 169 non-clinical adolescents (81 girls and 88 boys; Mage = 15.38; SDage = 1.52) filled out self-report measures of borderline personality features and identity diffusion. According to our results, having strong feelings and interpersonal sensitivity were the two most endorsed borderline personality features. Borderline personality features were positively correlated with identity diffusion. The more severe a borderline personality feature was, the less relevant it was for non-clinical adolescents. According to a network analysis, identity diffusion was the most central and least redundant element of the network of borderline personality traits. Results are discussed from a clinical point of view, further encouraging professionals to use identity diffusion screening tools to detect BPD in adolescence.
Introduction
This paper presents a study that investigated the role of identity diffusion in the organization of borderline personality features in adolescents. The dimensional approach to personality disorders in DSM-5 (1) allows us to make cautious inferences for clinical issues from non-clinical samples as the one in our study. We start by introducing concepts related to normative and pathological identity development in adolescence.
Identity Development in Adolescence
Both parents and clinicians face adolescence as a challenge. In today's society the developmental stage of adolescence has been prolonged or even to some degree blurred with what we call emerging adulthood (2). Nevertheless, this stage of life—from 10 to 24 years of age for adolescence (3) and from 18 to 25–30 years of age for emerging adulthood (2)—remains one with significant transformations ranging from biological to psychological and social. Although most of adolescents and their families report a trouble-free transition from childhood to adulthood, this period has been frequently described as one of “storm and stress” (4, 5). As part of the normative developmental processes, heightened emotionality—especially in relation to social cues—is a hallmark for adolescent transformation [for a psychopathology related summary see (6)]. Turbulences are also caused by a normative maladaptive shift in emotion regulation including rumination and aggression (7). Thus, normative changes in adolescence might seem to be similar to borderline traits (for a detailed elaboration of this issue see section Borderline personality disorder in adolescence).
The potential turbulences of this developmental stage are not surprising, given the several profound tasks that have to be solved in order to achieve psychologically balanced adult functioning; no matter whether at the end of adolescence or emerging adulthood [for a list of tasks see (8)]. These tasks can be summarized under the identity achievement vs. role confusion psychosocial developmental stage of Erikson (9, 10). Erikson [(11), p. 94] defines ego identity as “the accrued confidence that one's ability to maintain inner sameness and continuity. is matched by the sameness and continuity of one's meaning for others.” Relying on this definition and a review of social-cognitive and psychopathology oriented psychodynamic accounts of identity, Goth et al. (12) suggest two meaningful components of identity development: continuity and coherence. Both components are represented in three domains of psychosocial functioning: intrapersonal, interpersonal, and the level of mental representations.
On the one hand, continuity is the vital experience of subjective self-sameness with an inner stable timeline. Continuity is reflected in the three different domains of psychosocial functioning as goals, talents, commitments, roles, and relationships, and an ability to trust and rely on emotions. On the other hand, coherence is reflected as consistency in self-representations, autonomous psychological functioning with sufficient ego strength, and differentiated mental representations of self and others. By definition, coherence can be considered as the relatively contradiction-free and reflected content of self-representations.
For Erikson (9, 13), it was pivotal to make a distinction between normative identity crisis and identity diffusion. The source of normative identity crisis is development itself. By adolescence, childhood introjections and identifications lose their adaptive function, thereby forcing adolescents to revise them and integrate them into their ego identity at a more abstract level. Thus, identity crisis is a universal component of adolescent psychosocial development. Contrastingly, identity diffusion is the failure to solve the crisis successfully and falling short of achieving a continuous and coherent identity. For Kernberg (14, 15), identity diffusion results from the adolescent's inability to solve the ambivalence of newly achieved independence and attachment to parents and to integrate mental representations of self and others.
Borderline Personality Disorder in Adolescence
Borderline personality disorder (BPD) is a severe psychiatric disorder with chronic suicidality, unstable interpersonal relationships, and intense and fluctuating emotions (1). Being a very heterogeneous construct, there are 256 unique combinations of the nine diagnostic criteria for BPD. Moreover, factor analytic studies found multiple underlying latent factors explaining BPD criteria. Becker et al. (16) found four factors in a sample of adolescent inpatients. The four factor were (1) “suicidal threats or gestures” and “emptiness or boredom,” (2) “affective instability,” “uncontrolled anger,” and “identity disturbance,” (3) “unstable relationships” and “abandonment fears,” and (4) “impulsiveness” and “identity disturbance.” In a community-based sample, Chabrol et al. (17) found six factors: (1) dissociative/psychotic symptoms, (2) substance use, (3) interpersonal instability, (4) affectivity/identity disturbances, (5) narcissistic features, and (6) impulsivity. In a French-speaking international sample of adolescents diagnosed with BPD, Speranza et al. (18) found two factors accounting for 66.8% of variance in the nine criteria. The two factors were (1) internally oriented and (2) externally oriented criteria, composed of avoidance of abandonment, identity disturbance, chronic feeling of emptiness, and stress-related paranoid ideation for internally oriented criteria and unstable relationships, impulsivity, suicidal or self-mutilating behaviors, and inappropriate anger for externally oriented criteria. From these results we can conclude that albeit there is a single label for this disorder in taxonomy, BPD is a very heterogeneous construct.
Growing evidence shows that BPD is a valid, reliable, and clinically meaningful construct in adolescence (19, 20). The importance of emphasizing and promoting the BDP diagnosis for adolescents is twofold. First, BPD is highly prevalent (every fifth patient in the clinical setting is diagnosed with BPD) and highly dysfunctional (high comorbidity, increased risk for incarceration) mental disorder (21). Second, interventions in adolescence are or should be of high priority because of the malleability and flexibility of this developmental period (22). Successful interventions—even in case of subsyndromal BPD features—can serve as indicated prevention for adult BPD (22).
At the same time, professionals are still hesitant in many settings around the world to diagnose BPD in adolescents (23). The four main reasons for avoiding BPD diagnosis are: (1) invalidity of BPD diagnosis for adolescence, (2) the ongoing process of personality development, (3) difficulty to distinguish normative processes from BPD symptoms, and (4) strong stigmatization [Griffiths (24), Laurenssen et al. (25); for a general review on personality pathology in adolescence see (26)]. The first three of the above mentioned counter-arguments can be rejected based on empirical evidence. As for the validity of BPD diagnosis, prevalence and temporal stability of the diagnosis are very similar in adolescents and adult (27–29). Although personality development is an ongoing process and maturation during adolescence is evident [e.g., (30)], there is also substantial evidence for the stability in adolescence in personality traits (31). The difficulty to make a distinction between normative processes and BPD symptoms can be rejected using a dimensional approach to personality traits and personality disorder symptoms (32). Accordingly, we don't need qualitatively different traits to be present for sine morbo and personality disordered adolescents, a difference in frequency or intensity would suffice. Because stigmatization is highly dependent upon health care professionals' knowledge about BPD (33), progress in the three before mentioned domains could also decrease BPD-related stigmatization.
Borderline Personality Disorder and Identity Diffusion
Identity—a key process in normative adolescent development—plays an important role in the development and organization of BPD symptoms [e.g., (34, 35)]. The Alternative Model for Personality Disorders (Section III of DSM-5) (1) sees identity disturbance as a central construct in diagnosing personality disorders in general, and especially BPD. Moreover, impairments of identity affect other domains related to personality pathology. Identity diffusion interferes with pursuing goals (self-directedness), understanding others' perspectives (empathy), and establishing close relationships (intimacy) (34). Richtein et al. (35) showed in both clinical and non-clinical samples that together with affective instability, identity diffusion played a central role in the network of BPD symptoms. In a recent review, Kaufman and Meddaoui (36) called for a deeper empirical understanding of identity pathology. Identity diffusion could play a central role in building a unifying theory of BPD, because it is associated with constructs that form the core of BPD in different etiological models [impared mentalizing (37); distorted object relations (14, 15); invalidating environment (38); emotion dysregulation (39)]. Moreover, Wilkinson-Ryan and Westen (40) found that identity diffusion—especially painful incoherence—successfully distinguished patients with BPD from patients with other personality disorders and from individuals with no diagnosis.
Aims of the Study, Hypothesis
Based on the above presented theoretical background, the aim of the study was twofold. First, we wanted to further evidence that borderline personality features are not to be confused with signs of normative adolescent identity crisis. We hypothesized that severity of borderline traits [as indicated by the strengths of their correlations with identity diffusion—a sign of developmental breakdown (41)] is negatively associated with non-clinical adolescents' endorsement of borderline features' presence. Second, we wanted to test the relevance of identity diffusion in organizing borderline personality features. We hypothesized that identity diffusion had a central role in the network of borderline personality traits and could be conceived of as a latent organizing principle of borderline personality disorder.
Method
Sample and Procedure
Our participants were students from secondary schools in Pécs (South-Western Hungary). After parental informed consent 169 adolescents (81 girls and 88 boys) filled out the questionnaire package in paper–pencil format in groups of 20–30. Participants' age was between 12 and 18 with a mean age of 15.38 (SD = 1.52). The study was approved by the Hungarian United Ethical Review Committee for Research in Psychology (Ref. No.: 2017-110).
Measures
Identity diffusion was measured by Assessment of Identity Development in Adolescence [AIDA; Goth et al. (12); Rivnyák et al. (42) for the Hungarian version]. AIDA is a self-report measure of identity development to differentiate between normative adolescent identity crisis from the clinically relevant state of identity diffusion. The measure consists of 58 items that are evaluated on 5-point Likert-scales based on whether they describe the participant or not. Although AIDA measures different aspects of identity diffusion, we only used the total score in this study. Higher scores refer to more diffuse identity. AIDA proved to be a unidimensional measure of identity diffusion with high internal reliability (Cronbach's α = 0.94).
Borderline personality traits were measured with Borderline Personality Features Scale for Children-11 [BPFSC-11; (43)]. The scale was translated from English into Hungarian using the parallel back-translation procedure (44). The scale consists of 11 items tapping into the main characteristics of borderline personality disorder in the domains of emotional instability, emotional problems, and impaired interpersonal relations. Participants rate their agreement with the statements on 5-point Likert-scales. Higher scores refer to more prominent presence of borderline traits. A Cronbach's α value of 0.79 showed adequate internal reliability of BPFSC-11.
Statistical Analyses
To describe the variables means and standard deviations were computed. Skewness and kurtosis values were used to describe distribution. Internal reliability of the scales was indicated by Cronbach's α values. Pearson's correlations were used to test the association between variables. The above mentioned statistical analyses were run on IBM SPSS Statistics 22.
To investigate the network of the variables, we used network analysis with JASP 0.9.1.0. To achieve stable and easily interpretable networks, EBICglasso estimation was used. Based on Bayesian parameters and using the Graphical Least Absolute Shrinkage and Selection Operator (GLASSO), this estimation filters out weak correlations and false positive associations resulting from partial correlational analyses.
Networks can be described by several parameters (45–47). Node-related parameters can refer to the centrality of the node (i.e., variable) in the network. Betweenness refers to how many times a node is part of the shortest path between any pair of nodes. Closeness describes how many edges are needed to reach other nodes. Degree refers to how many and how strong edges depart from a node. Higher values refer to the more central role of the node in the network.
Local clustering coefficients quantify how close a node's neighbors are to being a complete graph. Thus, nodes with high local clustering coefficients are redundant in the network. Therefore, lower local clustering coefficients refer to the unique information attributed to a node (i.e., variable). There are several different methods to calculate local clustering coefficients. Costantini et al. (45) suggest to use the coefficient elaborated by Zhang and Horvath [2005 in Costantini et al. (45)] in the case of adaptive LASSO estimations. All centrality and local clustering coefficients reported in this study are standardized values. This means that the value zero refers to a mean value and values 1.0 and −1.0 refer to one standard deviation above and below mean, respectively.
Results
First, the descriptive characteristics of measured variables are presented. According to the kurtosis and skewness values (Table 1), all reported variables were considered to represent normal distributions (48).
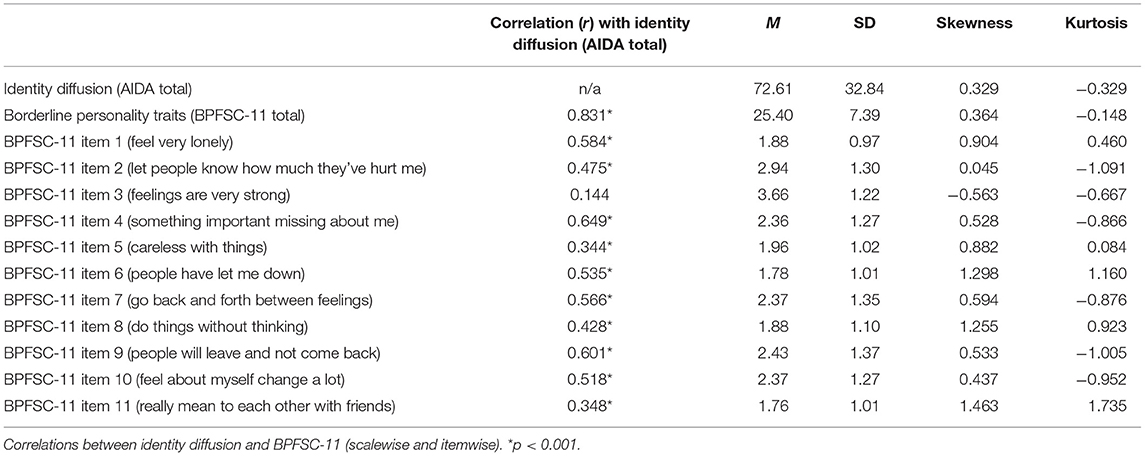
Table 1. Descriptive statistics for measured variables.
The associations between scales and single items were tested with Pearson's correlations. According to the results (Table 1), identity diffusion was strongly and positively related to borderline personality features in general. Identity diffusion also showed positive correlations with all specific borderline traits (i.e., items of BPFSC-11), except for item 3 (feelings are very strong). The strength of significant correlations ranged from moderate to strong. Identity diffusion was most strongly correlated with item 4 (something important missing about me) and item 9 (people will leave and not come back).
Next, we tested the association between the relative severity of specific borderline personality features and their relative relevance for non-clinical adolescents. To do so, we tested the linear correlation between the mean scores of BPFSC-11 items (as an indicator of the relative relevance of borderline features for non-clinical adolescents) and the strength of their correlations with identity diffusion (as an indicator of the relative severity of specific borderline features). With did this as an analog to computing similarity scores for measuring profile agreement (49). Although the correlation was not significant [r11 = −0.422; p = 0.196] because of the low sample size, there is a moderate negative correlation between relative severity (as indicated by each BPFSC-11 item's correlation with identity diffusion) and relative relevance (as indicated by the mean score of each BPFSC-11 item) of borderline personality traits. This means that non-clinical adolescents reported less agreement with borderline features as borderline features' association with identity diffusion increased.
To test the relative importance of identity diffusion in the organization of borderline personality features, we used network analysis. Both visual inspection of the network (Figure 1; see Table 1 for item content) and centrality and local clustering coefficients (Table 2) support the central role of the identity diffusion score in the network. All centrality parameters are the highest for identity diffusion score, while the local clustering coefficient is the lowest for AIDA Total. This means that most of the shortest paths going from a specific borderline trait to another specific borderline trait go through identity diffusion (betweenness), identity diffusion exerts the highest number of direct effects on specific borderline traits (closeness), and identity diffusion has the strongest effect on specific borderline traits (degree). Identity diffusion also has the less redundant (i.e., the most unique) information in the network (local clustering coefficient).
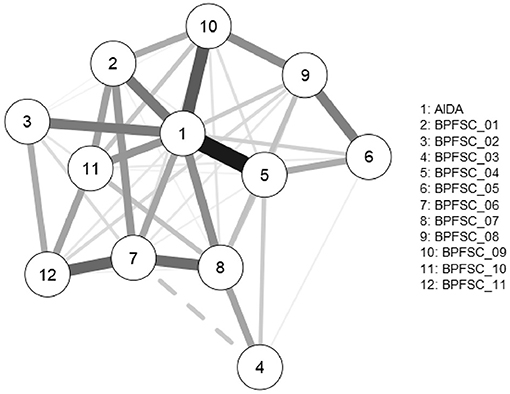
Figure 1. The network of identity diffusion and borderline personality features.
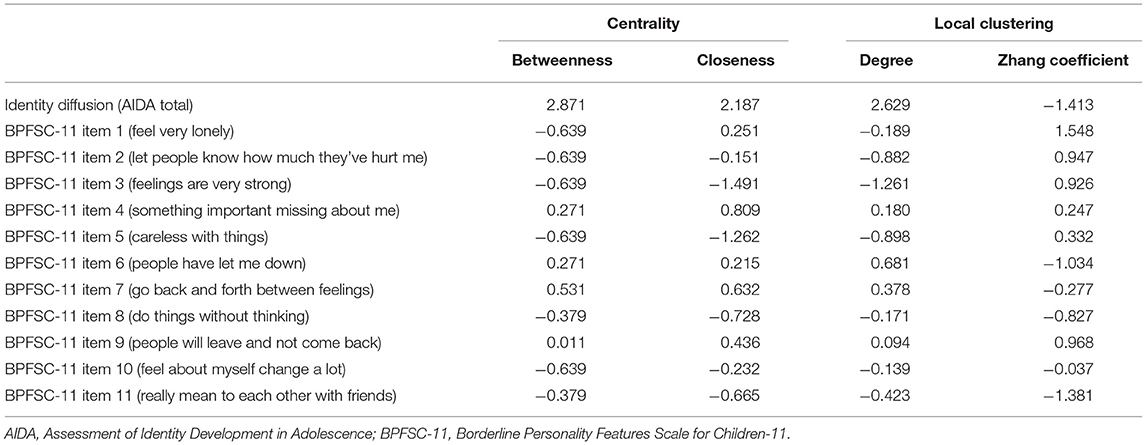
Table 2. Characteristic parameters of the network's nodes; centrality and local clustering coefficients (all coefficients are standardized values).
Discussion
With regard to the first aim of the study (i.e., to investigate the salience of specific borderline personality features in non-clinical adolescents in the conceptual framework of normative adolescent crisis), non-clinical adolescents reported less agreement with more severe borderline personality features (as indicated by the strength of their correlations with identity diffusion). Accordingly, professional concerns about confusing normative identity crisis with borderline personality features [e.g., (50, 51)] might be exaggerated. As adolescents' agreement with BPFSC-11 items increased, single items' strength of correlation with identity diffusion decreased. Thus, our results echo the conclusion of the developers of AIDA (12) and many who make a clear distinction between normative adolescent identity crisis and identity diffusion that is a risk factor for developing borderline personality disorder and personality disorders in general (52, 53).
With regard to the second aim of our study, results of the network analysis supported the hypothesis that identity diffusion could be a latent variable accounting for the interconnectedness of specific borderline personality traits. Although previous factor analytic studies revealed the multi-faceted nature of borderline personality in adolescents (16–18) and Paris (54) even argued that each feature of borderline personality disorder reflects different diatheses, our results showed that identity diffusion—as measured by AIDA (12)—played a central role in the network of borderline personality features in non-clinical adolescents. We suggest that the heterogeneous nature of borderline personality disorder (55) can become less perplexing if the diverse symptoms are conceptualized as stemming from a single source, namely identity diffusion. Nevertheless, we do not question the multiply determined nature of identity diffusion with etiological contributions from genetics to culture (56). In this sense, although distal etiological factor might be diverse, identity diffusion can be hypothesized as a single proximal etiological factor (57).
Limitations and Conclusions
Although our results are clear and extend previous research in a meaningful way, some limitations of our study should be mentioned. First, the sample size of our study is limited. In order to achieve even stronger conclusions, the sample size should be increased further. Second, although results are compelling, we should be very cautious in extrapolating our conclusions to clinical samples. Therefore, the study should be repeated with a clinical sample.
Our study is among the first to show the central role of identity diffusion as an organizing principle of borderline personality features with network analyses. From a methodological point of view, we join a group of colleagues (45–47) in advocating network analysis as a promising new method in the field of clinical and personality psychology. If clinical studies could replicate our results in the future, they proved identity diffusion to be a potentially useful intervention target in the treatment of adolescents with borderline personality disorder. This would further promote the importance and use of identity diffusion screening tools like AIDA (12).
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Hungarian United Ethical Review Committee for Research in Psychology (Ref. No.: 2017-110). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
AR: study design, data collection, and writing the first draft. MP: writing and revising the first draft. BP: revising the first draft. AL: statistical analysis, writing, and revising the first draft. All authors contributed to the article and approved the submitted version.
Funding
This project was supported by the European Union and co-financed by the European Social Fund (EFOP-3.6.1.-16-2016-00004—Comprehensive Development for Implementing Smart Specialization Strategies at the University of Pécs).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. American Psychiatric Association. (2013). DSM-5. Washington, DC: American Psychiatric Association Press.
2. Arnett JJ. Emerging adulthood: what is it, and what is it good for?. Child Dev Perspect. (2007) 1:68–73. doi: 10.1111/j.1750-8606.2007.00016.x
3. Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC. The age of adolescence. Lancet Child Adolescent Health. (2018) 2:223–8. doi: 10.1016/S2352-4642(18)30022-1
4. Gutgesell ME, Payne N. Issues of adolescent psychological development in the 21st century. Pediatr Rev. (2004) 25:79–85. doi: 10.1542/pir.25-3-79
5. Hazen E, Schlozman S, Beresin E. Adolescent psychological development: a review. Pediatr Rev. (2008) 29:161. doi: 10.1542/pir.29-5-161
6. Rapee RM, Oar EL, Johnco CJ, Forbes MK, Fardouly J, Magson NR, et al. Adolescent development and risk for the onset of social-emotional disorders: a review and conceptual model. Behav Res Ther. (2019) 123:103501. doi: 10.1016/j.brat.2019.103501
7. Cracco E, Goossens L, Braet C. Emotion regulation across childhood and adolescence: evidence for a maladaptive shift in adolescence. Eur Child Adolescent Psychiatry. (2017) 26:909–21. doi: 10.1007/s00787-017-0952-8
8. Seiffge-Krenke I, Gelhaar T. Does successful attainment of developmental tasks lead to happiness and success in later developmental tasks? A test of Havighurst's (1948) theses. J Adolesc. (2008) 31:33–52. doi: 10.1016/j.adolescence.2007.04.002
9. Erikson EH. The problem of ego identity. J Am Psychoanal Assoc. (1956) 4:56–121. doi: 10.1177/000306515600400104
12. Goth K, Foelsch P, Schlüter-Müller S, Birkhölzer M, Jung E, Pick O, et al. Assessment of identity development and identity diffusion in adolescence-Theoretical basis and psychometric properties of the self-report questionnaire AIDA. Child Adolesc Psychiatry Ment Health. (2012) 6:1–16. doi: 10.1186/1753-2000-6-27
14. Kernberg OF. The diagnosis of borderline conditions in adolescence. Adolescent Psy-chiatry. (1978) 6:298–319.
15. Kernberg OF. Identity diffusion in severe personality disorders. In: Strack S, editor. Handbook of Personology and Psychopathology. Hoboken, NJ: John Wiley and Sons Inc. (2005). p. 39–49.
16. Becker DF, McGlashan TH, Grilo CM. Exploratory factor analysis of borderline personality disorder criteria in hospitalized adolescents. Compr Psychiatry. (2006) 47:99–105. doi: 10.1016/j.comppsych.2005.07.003
17. Chabrol H, Montovany A, Ducong é E, Kallmeyer A, Mullet E, Leichsenring F. Factor structure of the borderline personality inventory in adolescents. Eur J Psychol Assess. (2004) 20:59–65. doi: 10.1027/1015-5759.20.1.59
18. Speranza M, Pham-Scottez A, Revah-Levy A, Barbe RP, Perez-Diaz F, Birmaher B, et al. Factor structure of borderline personality disorder symptomatology in adolescents. Can J Psychiatry. (2012) 57:230–7. doi: 10.1177/070674371205700406
19. Fonagy P, Speranza M, Luyten P, Kaess M, Hessels C, Bohus M. ESCAP Expert Article: Borderline personality disorder in adolescence: an expert research review with implications for clinical practice. Eur Child Adolescent Psychiatry. (2015) 24:1307–20. doi: 10.1007/s00787-015-0751-z
20. Fossati A. Diagnosing borderline personality disorder in adolescence: a review of the published literature. Scand J Child Adolescent Psychiatry Psychol. (2015) 3:5–21. doi: 10.21307/sjcapp-2015-002
21. Leichsenring F, Leibing E, Kruse J, New AS, Leweke F. Borderline personality disorder. Lancet. (2011) 377:74–84. doi: 10.1016/S0140-6736(10)61422-5
22. Chanen AM, McCutcheon L. Prevention and early intervention for borderline personality disorder: current status and recent evidence. Br J Psychiatry. (2013) 202:s24–s9. doi: 10.1192/bjp.bp.112.119180
23. Kaess M, Brunner R, Chanen A. Borderline personality disorder in adolescence. Pediatrics. (2014) 134:782–93. doi: 10.1542/peds.2013-3677
24. Griffiths M. Validity, utility and acceptability of borderline personality disorder diagnosis in childhood and adolescence: survey of psychiatrists. Psychiatrist. (2011) 35:19–22. doi: 10.1192/pb.bp.109.028779
25. Laurenssen EMP, Hutsebaut J, Feenstra DJ, Van Busschbach JJ, Luyten P. Diagnosis of personality disorders in adolescents: a study among psychologists. Child Adolesc Psychiatry Ment Health. (2013) 7:1–4. doi: 10.1186/1753-2000-7-3
26. Westen D, Chang C. Personality pathology in adolescence: a review. Adolesc Psychiatry. (2000) 25:61–100.
27. Chanen AM, Jackson HJ, McGorry PD, Allot KA, Clarkson V, Yuen HP. Two-year stability of personality disorder in older adolescent outpatients. J Pers Disord. (2004) 18:526–41. doi: 10.1521/pedi.18.6.526.54798
28. Coid J, Yang M, Tyrer P, Roberts A, Ullrich S. Prevalence and correlates of personality disorder in Great Britain. Br J Psychiatry. (2006) 188:423–31. doi: 10.1192/bjp.188.5.423
29. Johnson JG, Cohen P, Kasen S, Skodol AE, Oldham JM. Cumulative prevalence of personality disorders between adolescence and adulthood. Acta Psychiatr Scand. (2008) 118:410–3. doi: 10.1111/j.1600-0447.2008.01231.x
30. Klimstra TA, Hale WW III, Raaijmakers QA, Branje SJ, Meeus WH. Maturation of personality in adolescence. J Pers Soc Psychol. (2009) 96:898. doi: 10.1037/a0014746
31. Elkins RK, Kassenboehmer SC, Schurer S. The stability of personality traits in adolescence and young adulthood. J Econ Psychol. (2017) 60:37–52. doi: 10.1016/j.joep.2016.12.005
32. Hudziak JJ, Achenbach TM, Althoff RR, Pine DS. A dimensional approach to developmental psychopathology. Int J Methods Psychiatr Res. (2007) 16:S16–S23. doi: 10.1002/mpr.217
33. Ring D, Lawn S. Stigma perpetuation at the interface of mental health care: a review to compare patient and clinician perspectives of stigma and borderline personality disorder. J Mental Health. (2019) 1–21. doi: 10.1080/09638237.2019.1581337 [Epub ahead of print].
34. Benzi IMA, Madeddu F. Development of personality disorders: Identity as a key process. Int J Psychol Behav Anal. (2017) 3:124.
35. Richetin J, Preti E, Costantini G, De Panfilis C. The centrality of affective instability and identity in Borderline Personality Disorder: Evidence from network analysis. PLoS One. (2017) 12:e0186695.
36. Kaufman EA, Meddaoui B. Identity pathology and borderline personality disorder: an empirical overview. Curr Opin Psychol. (2021) 37:82–8. doi: 10.1016/j.copsyc.2020.08.015
37. Fonagy P, Gergely G, Jurist EL, Target M. Affect Regulation, Mentalization, and the Development of the Self. New York, NY: Other Press (2002).
38. Crowell SE, Beauchaine TP, Linehan MM. A biosocial developmental model of borderline personality: elaborating and extending linehan's theory. Psychol Bull. (2009) 135:495. doi: 10.1037/a0015616
39. Carpenter RW, Trull TJ. Components of emotion dysregulation in borderline personality disorder: a review. Curr Psychiatry Rep. (2013) 15:1–8. doi: 10.1007/s11920-012-0335-2
40. Wilkinson-Ryan T, Westen D. Identity disturbance in borderline personality disorder: an empirical investigation. Am J Psychiatry. (2000) 157:528–41. doi: 10.1176/appi.ajp.157.4.528
41. Laufer ME, Laufer M. Adolescence and Developmental Breakdown: A Psychoanalytic View. London: Routledge (2018).
42. Rivnyák A, Láng A, Péley B, Nagy G, Nagy E, Bóna A, et al. Az identitásfejlodés felmérése serdülokorban kérdoív magyar adaptációja (AIDA-Hungary) serdülok nem klinikai mintáján. Magyar Pszichol Szemle. (2020) 75:247–69. doi: 10.1556/0016.2020.00015
43. Sharp C, Steinberg L, Temple J, Newlin E. An 11-item measure to assess borderline traits in adolescents: Refinement of the BPFSC using IRT. Pers Disord Theory Res Treat. (2014) 5:70. doi: 10.1037/per0000057
44. Brislin RW. Back-translation for cross-cultural research. J Cross Cult Psychol. (1970) 1:185–216.
45. Costantini G, Epskamp S, Borsboom D, Perugini M, Mõttus R, Waldorp LJ, et al. State of the aRt personality research: a tutorial on network analysis of personality data in R. J Res Pers. (2015) 54:13–29. doi: 10.1016/j.jrp.2014.07.003
46. Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. (2018) 50:195–212. doi: 10.3758/s13428-017-0862-1
47. Fonseca-Pedrero E. Network analysis in psychology. Papeles del Psicólogo. (2018) 39:1–12. doi: 10.23923/pap.psicol2018.2852
48. George D, Mallery. P. SPSS for Windows Step by Step: A Simple Guide and Reference, 18.0 Update, 11th Edn. Boston, MA: Allyn and Bacon (2010).
49. McCrae RR. A note on some measures of profile agreement. J Pers Assess. (2008) 90:105–9. doi: 10.1080/00223890701845104
50. Garnet KE, Levy KN, Mattanah JJF, Edell WS, McGlashan TH. Borderline personality disorder in adolescents: ubiquitous or specific? Am J Psychiatry. (1994) 151:1380–2. doi: 10.1176/ajp.151.9.1380
51. Meijer M, Goedhart AW, Treffers PDA. The persistence of borderline personality disorder in adolescence. J Pers Disord. (1998) 12:13–22 doi: 10.1521/pedi.1998.12.1.13
52. Jung E, Pick O, Schlüter-Müller S, Schmeck K, Goth K. Identity development in adolescents with mental problems. Child Adolesc Psychiatry Ment Health. (2013) 7:1–8. doi: 10.1186/1753-2000-7-26
53. Westen D, Betan E, DeFife JA. Identity disturbance in adolescence: associations with borderline personality disorder. Dev Psychopathol. (2011) 23:305–13. doi: 10.1017/S0954579410000817
54. Paris J. The nature of borderline personality disorder: Multiple dimensions, multiple symptoms, but one category. J Pers Disord. (2007) 21:457–73. doi: 10.1521/pedi.2007.21.5.457
55. Trull TJ, Tomko RL, Brown WC, Scheiderer EM. Borderline personality disorder in 3-D: Dimensions, symptoms, measurement challenges. Soc Personal Psychol Compass. (2010) 4:1057–69. doi: 10.1111/j.1751-9004.2010.00312.x
56. Kernberg OF. Identity: Recent findings and clinical implications. Psychoanal Q. (2006) 75:969–1004. doi: 10.1002/j.2167-4086.2006.tb00065.x
Keywords: identity diffusion, borderline personality disorder, adolescence, network analysis, AIDA
Citation: Rivnyák A, Pohárnok M, Péley B and Láng A (2021) Identity Diffusion as the Organizing Principle of Borderline Personality Traits in Adolescents—A Non-clinical Study. Front. Psychiatry 12:683288. doi: 10.3389/fpsyt.2021.683288
Received: 20 March 2021; Accepted: 09 June 2021;
Published: 06 July 2021.
Edited by:
Hojka Gregoric Kumperscak, Maribor University Medical Centre, SloveniaReviewed by:
Carla Sharp, University of Houston, United StatesMario Speranza, Université de Versailles Saint-Quentin-en-Yvelines, France
Copyright © 2021 Rivnyák, Pohárnok, Péley and Láng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: András Láng, bGFuZy5hbmRyYXNAcHRlLmh1