 Yu Jin1†
Yu Jin1† Yue Li2†Xiu-Ya Li3†Yan-Jie Zhao4,5,6†
Yue Li2†Xiu-Ya Li3†Yan-Jie Zhao4,5,6† Teris Cheung7Gabor S. Ungvari8,9Michael Li10Feng-Rong An11*
Teris Cheung7Gabor S. Ungvari8,9Michael Li10Feng-Rong An11* Yu-Tao Xiang4,5,6
Yu-Tao Xiang4,5,6- 1College of Education for the Future, Beijing Normal University, Beijing, China
- 2Department of Nursing, Beijing Tongren Hospital, Capital Medical University, Beijing, China
- 3Department of Otorhinolaryngology, Beijing Tongren Hospital, Capital Medical University, Beijing, China
- 4Unit of Psychiatry, Department of Public Health and Medicinal Administration, Institute of Translational Medicine, Faculty of Health Sciences, University of Macau, Macao, China
- 5Centre for Cognitive and Brain Sciences, University of Macau, Macao, China
- 6Institute of Advanced Studies in Humanities and Social Sciences, University of Macau, Macao, China
- 7School of Nursing, Hong Kong Polytechnic University, Hong Kong, China
- 8Division of Psychiatry, School of Medicine, University of Western Australia/Graylands Hospital, Perth, WA, Australia
- 9University of Notre Dame Australia, Fremantle, WA, Australia
- 10The Hong Kong Academy for Performing Arts, Hong Kong, China
- 11The National Clinical Research Center for Mental Disorders, Beijing Key Laboratory of Mental Disorders Beijing Anding Hospital, Advanced Innovation Center for Human Brain Protection, School of Mental Health, Capital Medical University, Beijing, China
Background: The coronavirus disease 2019 (COVID-19) pandemic has caused psychological distress and heavy burden in medical professionals. This study examined the prevalence of fatigue and its association with quality of life (QOL) in clinicians working in ophthalmology and otolaryngology departments during the COVID-19 pandemic in China.
Methods: This was a cross-sectional national online survey conducted between March 15 and March 20, 2020 in China. The severity of fatigue, depression and QOL were measured using the Numeric Rating Scale (NRS), the 9-item Patient Health Questionnaire (PHQ-9), and the World Health Organization Quality of Life Questionnaire-Brief Version (WHOQOL-BREF), respectively.
Results: In total, 3,912 clinicians completed the survey (2,155 in ophthalmology department, and 1,757 in otolaryngology department); 2,049 [52.4%; 95% confidence interval (CI) = 50.8–53.9%] reported fatigue (NRS score ≥ 4). Multiple logistic regression analysis revealed that junior clinicians [Odds ratio (OR) = 0.82, 95% CI = 0.68–1.00, P = 0.045] had lower risk of fatigue; while clinicians working in tertiary hospitals (OR = 1.23, 95% CI = 1.02–1.49, P = 0.029), and the presence of more severe depressive symptoms (PHQ-9 total score ≥ 5; OR = 7.40, 95% CI = 6.29–8.70, P < 0.001) were independently associated with higher risk of fatigue. After controlling for covariates, clinicians with fatigue had significantly lower QOL compared with those without [F(1, 3, 911) = 283.75, P < 0.001].
Conclusion: Fatigue was common in clinicians working in ophthalmology and otolaryngology departments during the COVID-19 pandemic. Considering the negative impact of fatigue on clinicians' QOL, health authorities and policymakers should conduct regular screening for fatigue and develop preventive strategies for frontline clinicians working under excessive stress.
Introduction
The coronavirus disease 2019 (COVID-19) was first reported in China in December 2019 and then it emerged in more than 200 countries and territories (1, 2). COVID-19 is more infectious than Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) (3). Hence, the World Health Organization (WHO) declared COVID-19 as a public health emergency of international concern on the January 30, 2020 (1). As of the middle of May 2021, there have been more than 167 million confirmed cases worldwide (4).
The COVID-19 outbreak imposed a heavy burden on health professionals (5) due to long working hours, inadequate personal protective equipment, suboptimal training, shift duty and high-risk of infection (6). Physical and mental health problems were always common in health professionals during outbreaks of infectious diseases. For instance, a systematic review found that 75.9% [95% confidence interval (CI) = 65.9–83.7%] of health professionals during the SARS/MERS/COVID-19 outbreaks reported fever, 41.2% (95% CI = 18.2–33.2%) reported fatigue, 29.0% (95% CI = 14.2–50.3%) reported anxiety and 26.3% (95% CI = 12.5–47.1%) reported depressive symptoms (7). Recent studies on mental health of Chinese health professionals exposed to COVID-19 found that depression (19.8–50.4%), anxiety (35.6–57.3%) insomnia (18.4–55.7%) and general distress (41.5–71.5%) were common (8–13).
Physical and mental health problems such as depression, anxiety, distress and post-traumatic stress symptoms in frontline health professionals during the COVID-19 pandemic have been frequently reported (8, 9, 13). Fatigue has been underestimated, despite it was also common in health professionals during the SARS/MERS outbreaks (7, 14). Fatigue affects the whole organism, including subjective feelings of exhaustion and deterioration of mental and physical activities (15, 16), which leads to a range of negative health outcomes such as poor morale, absenteeism, apathy, irritability, increased tendency for depression, and poor motivation at work. In addition, fatigue may also result in non-specific physical complaints such as headache, dizziness, palpitations, rapid breathing, loss of appetite, indigestion, or insomnia (17, 18).
By nature of the clinical specialty, clinicians working in ophthalmology and otolaryngology departments have a higher likelihood to be infected due to close proximity to COVID-19 patients and asymptomatic carriers compared with their counterparts in other clinical specialties. Due to the heavy workload and high risk of infection, clinicians in ophthalmology and otolaryngology departments are more likely to report physical and mental ailments including fatigue that influences quality of patient care and increase the risk of conflicts with patients. In order to reduce the occurrence of fatigue and its negative consequences, it is important to understand its patterns and associated factors in clinicians working in different specialties, particularly those working in high risk clinical settings during the COVID-19 pandemic.
This study examined the prevalence of fatigue and its association with quality of life (QOL) in clinicians working in ophthalmology or otolaryngology departments during the COVID-19 pandemic in China. The main hypothesis of the study was that fatigue would be common in these clinicians and it would be associated with lower QOL during the COVID-19 epidemic in China.
Methods
Setting and Sample
This cross-sectional, national online survey was conducted between March 15 and March 20, 2020. Due to the high risk of contagion, face-to-face interviews were not performed during the COVID-19 pandemic. Similar to other studies (10), snowball sampling and the WeChat-based QuestionnaireStar program were used to collect data. WeChat is a widely used social communication application with more than 1 billion Chinese users (6). With the help of the Panels of Ophthalmology and Otolaryngology of the Chinese Nursing Association, the Quick Response code (QR code) linked to the invitation to participate in the study and the assessment instruments were delivered to all panel members in each province of China by WeChat. Panel members in each province then distributed the QR Code to all hospitals in their respective areas. Clinicians in these hospitals/units participated in this study on a voluntary basis. The inclusion criteria were: (1) adults aged 18 years or above; (2) frontline clinicians (including doctors, nurses, and nurse assistants) working in ophthalmology or otolaryngology departments during the outbreak of COVID-19; and (3) ability to understand the content of assessment and provide written informed consent. Ethical approval was obtained from the Ethics Committee of Beijing Anding Hospital, China.
Instruments
Participants' basic demographic data, including gender, age, marital status, education level, living circumstances, current smoking, type of hospital (primary/tertiary), department (ophthalmology/otolaryngology), rank [junior (nursing assistants, residents, and senior medical officers)/senior (vice consultant, consultant, and head nurses)], site of work (inpatient/outpatient), shift duty requirement (yes/no) and work experience during the 2003 SARS outbreak (yes/no), were collected. Three additional standard questions were asked: (1) whether they provided direct care to COVID-19 patients; (2) whether they had any family members, friends, or colleagues infected with COVID-19; and (3) whether there have been 500 or more local COVID-19 patients in the province where they lived/worked.
Severity of fatigue was assessed by the Numeric Rating Scale (NRS) scoring from “0”-“10,” with “0” indicating “no fatigue” and “10” indicating “unbearable fatigue” (19, 20). A total score of ≥ 4 indicated “clinically relevant fatigue (fatigue hereafter),” and ≥7 indicated “severe fatigue” (21).
Depressive symptoms were measured with the Chinese version of the Patient Health Questionnaire-9 (PHQ-9) (22, 23). The total score of PHQ-9 ranges from 0 to 27, with higher scores indicating more severe depressive symptoms (24). Global quality of life (QOL) was measured with the first two items of the World Health Organization Quality of Life Questionnaire-brief version (WHOQOL-BREF) (25, 26). Higher total scores indicate higher QOL. The Chinese version of the scale has been validated in Chinese populations with good sensitivity and specificity (27, 28).
Data Analysis
Data were analyzed using SPSS, Version 24.0 (IBM SPSS, IBM Crop., Armonk, NY, USA). Chi-square-tests, Mann-Whitney U-tests, and independent samples t-tests compared socio-demographic and clinical characteristics between clinicians with and without fatigue, as appropriate. Multiple logistic regression analyses using the “enter” method (i.e., all independent variables were included at the same time) was conducted to examine the independent demographic and clinical correlates of fatigue. Fatigue was the dependent variable, while the variables with a P-value of < 0.05 in the univariate analyses were entered as independent variables. Analysis of covariance (ANCOVA) was performed to compare overall QOL between the fatigue and no fatigue groups after controlling for variables that significantly differed between the two groups in univariate analyses. The level of significance was set at P < 0.05 (two-sided).
Results
In total, 3,912 clinicians met the study criteria and completed the assessments (2,155 in ophthalmology department, and 1,757 in otolaryngology department); 2,049 (52.4%; 95% CI = 50.8–53.9%) reported fatigue (NRS score ≥ 4) including 579 (14.8%; 95% CI: 13.7–15.9%) with severe fatigue (NRS score ≥ 7) during the COVID-19 outbreak. The mean NRS total score was 4.15 (SD = 2.20) in the whole sample. Table 1 shows the participants' socio-demographic and clinical characteristics.
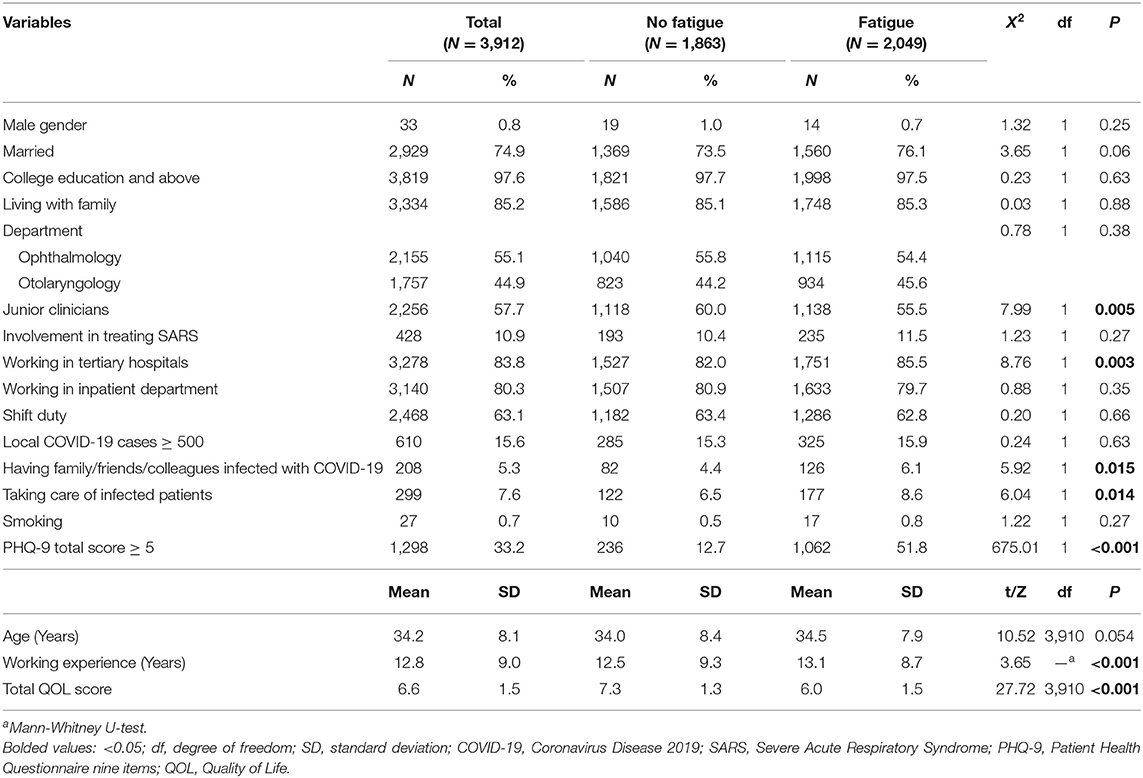
Table 1. Demographic characteristics of clinicians in ophthalmology and otolaryngology departments.
Univariate analyses found that fatigue was significantly associated with the clinicians' ranking, working in tertiary hospitals, having family/friends/colleagues infected with COVID-19, taking care of infected patients and PHQ-9 total score ≥ 5 (all P-values < 0.05). After controlling for covariates, clinicians with fatigue had significantly lower QOL compared with those without fatigue [F(1, 3, 911) = 283.75, P < 0.001].
Multiple logistic regression analysis revealed that junior clinicians [Odds ratio (OR) = 0.82, 95% CI = 0.68–1.00, P = 0.045] had lower risk of fatigue, while working in tertiary hospitals (OR = 1.23, 95% CI = 1.02–1.49, P = 0.029), and presenting with more severe depressive symptoms (PHQ-9 total score ≥ 5; OR = 7.40, 95% CI = 6.29–8.70, P < 0.001) were factors independently associated with higher risk of fatigue (Table 2).

Table 2. Independent correlates of fatigue by multiple logistic regression analysis.
Discussion
To the best of our knowledge, this was the first study that examined the epidemiology and correlates of fatigue in clinicians in ophthalmology and otolaryngology departments during the COVID-19 pandemic. More than half (52.4%; 95% CI = 50.8–53.9%) of these clinicians suffered from fatigue (NRS score ≥ 4), and 14.8% (95% CI = 13.7–15.9%) even experienced severe fatigue (NRS score ≥ 7).
These figures (52.4%; 95% CI = 50.8–53.9%) are higher than those reported in similar studies. In a systematic review fatigue in healthcare workers during SARS/MERS/COVID-19 outbreaks was 41.2% (95% CI = 18.2–68.8%), with 80.0% (95% CI = 73.8–85.1%) during the SARS outbreak, 25.6% (95% CI = 15.5–39.3%) during the MERS outbreak and 38% (95% CI = 15.3–67.4%) during the COVID-19 epidemic (7). A survey on 140 intensive care unit nurses who volunteered to work in Wuhan from Jiangsu province (i.e., the epicenter of the COVID-19 epidemic in China) found that 15.0% reported fatigue during the COVID-19 pandemic (29). The discrepancy concerning the rate of fatigue between studies could be explained by the following reasons. First, apart from heavy clinical duties, clinicians from many ophthalmology and otolaryngology departments often had to undertake additional workload such as looking after COVID-19 patients and suspected cases during the pandemic. This led to longer shifts, less sleep, and increased psychological pressure, all of which increased the risk of fatigue (14, 30). Second, asymptomatic COVID-19 patients were more frequently encountered in hospitals than those with typical symptoms, which put clinicians at increased likelihood of being infected (31). Many clinicians stayed in hospitals, rather than returning home after work to reduce the risk of spreading virus to their family members and the wider community. This self-isolation could have further worsened their fatigue (32). In addition, during the pandemic, after looking after or contacting infected/suspected cases and patients with fever, clinicians needed to spend at least 2 weeks in quarantine, which could also lead to fatigue (9, 12, 33, 34). Fourth, various self-administered or interviewer-rating instruments on fatigue were used in studies, which could also contribute to the diversity in the findings.
Senior clinicians who were working in tertiary hospitals reported more severe depressive symptoms and were associated with higher risk of fatigue. Compare to junior clinicians, apart from clinical duties, senior clinicians, particularly those in tertiary hospitals had more administrative, teaching and academic responsibilities and pressure (13). For example, many senior clinicians were required to join the emergency response teams in their affiliated hospitals during the COVID-19 outbreak. Additionally, senior clinicians were usually older than junior colleagues, which means they might have more family responsibilities and greater financial burdens, all of which could increase the risk of fatigue. In China, clinicians working in tertiary hospitals had heavier workload and more severe burnout symptoms than those working in primary and secondary hospitals (16, 35, 36). Since January 2020, all provinces, municipalities, and autonomous regions in China have launched the first-level responses to combating the novel coronavirus disease (37). Most tertiary hospitals set up designated emergency isolation hospitals/units to provide clinical services for local infected cases (8). Many clinicians in tertiary hospitals including those working in ophthalmology and otolaryngology departments were assigned to these newly established hospitals/units, which could contribute to higher rates of fatigue.
Frontline clinicians with depressive symptoms were more likely to report fatigue in this study. The relationship between depression and fatigue was bidirectional. On one hand, clinicians who suffered from fatigue and related problems such as loss of energy, impaired concentration, irritability and reduced productivity, face a higher risk of depression (38, 39). On the other hand, fatigue is one of the common symptoms of depression (40, 41), thus there is an overlap of presentations between fatigue and depression.
The concept of QOL comprises a person's physical condition, psychological state, level of independence, social relationships, environment, and spirituality (42). Clinicians suffering from a higher level of psychological stress and burnout were at increased risk of substance abuse and suicide, particularly when they were facing huge demands at work, illness, death, interpersonal conflicts and lack of knowledge or support during a public health crisis such as the SARS/COVID-19 outbreaks (43, 44). Considering the negative impact of fatigue on the quality of clinical practice and fatigue-related negative health outcomes such as low energy, decreased physical endurance, poor cognition, and mental distress (45), it is reasonable to assume that clinicians with fatigue are more likely to have lower QOL than clinicians without it as confirmed in this study. Similar findings were also reported prior to the COVID-19 pandemic (8, 10, 13).
The strengths of this study include the large sample size, and the use of standardized instruments on fatigue and QOL. However, there were several limitations that need to be acknowledged. First, potentially important variables associated with fatigue, such as physical comorbidities, lifestyle factors (e.g., regular physical exercise and sleeping habits) and social support, were not examined due to logistical reasons. Second, the causality between fatigue and other variables could not be established because of the cross-sectional study design. Third, due to the risk of cross-infection, random sampling could not be used when recruiting frontline health professionals during the COVID-19 outbreak. Fourth, more than 95% of the participants were female clinicians, which makes the sample subject to selection bias. Finally, COVID-19 information was collected by self-report questions, thus the information obtained is likely to be affected by demographic factors, such as education level.
In conclusion, fatigue was common in ophthalmology and otolaryngology departments clinicians during COVID-19 pandemic in China. Considering the negative impact of fatigue on QOL, health authorities and policymakers should develop preventive strategies and conduct effective interventions targeting this population exposed to excessive demands in clinical practice.
Data Availability Statement
The Ethics Committee of Beijing Anding Hospital that approved the study prohibits the authors from making the research data set publicly available. Readers and all interested researchers may contact Dr. Feng-Rong An (Email address: YWZyeWxtQHNpbmEuY29t) for details. Dr. An could apply to the Ethics Committee of Beijing Anding Hospital for the release of the data.
Ethics Statement
The studies involving human participants were reviewed and approved by The Ethics Committee of Beijing Anding Hospital. The patients/participants provided electronic written informed consent to participate in this study. Electronic written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
YJ, F-RA, and Y-TX: conception and design. YL and Y-TX: administrative support. X-YL and YL: provision of study materials or patients. X-YL, YL, and Y-JZ: collection and assembly of data. YJ, TC, and GU: data analysis and interpretation. YJ, Y-TX, GU, and ML: manuscript writing and revision. All authors: final approval of manuscript.
Funding
This study was supported by the National Science and Technology Major Project for investigational new drug (2018ZX09201-014), the Beijing Municipal Science and Technology Commission (No. Z181100001518005), and the University of Macau (MYRG2019-00066-FHS).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Sohrabi C, Alsafi Z, O'Neill N, Khan M, Kerwan A, Al-Jabir A, et al. World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int J Surg. (2020) 76:71–6. doi: 10.1016/j.ijsu.2020.02.034
2. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the chinese center for disease control and prevention. JAMA. (2020) 323:1239–42. doi: 10.1001/jama.2020.2648
3. Harapan H, Itoh N, Yufika A, Winardi W, Keam S, Te H, et al. Coronavirus disease 2019 (COVID-19): a literature review. J Infect Public Health. (2020) 13:667–73. doi: 10.1016/j.jiph.2020.03.019
4. World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Geneva: World Health Organization (2021).
5. Xiang YT, Zhao YJ, Liu ZH, Li XH, Zhao N, Cheung T, et al. The COVID-19 outbreak and psychiatric hospitals in China: managing challenges through mental health service reform. Int J Biol Sci. (2020) 16:1741–4. doi: 10.7150/ijbs.45072
6. Xin M, Luo S, She R, Yu Y, Li L, Wang S, et al. Negative cognitive and psychological correlates of mandatory quarantine during the initial COVID-19 outbreak in China. Am Psychol. (2020) 75:607–17. doi: 10.1037/amp0000692
7. Salazar de Pablo G, Vaquerizo-Serrano J, Catalan A, Arango C, Moreno C, Ferre F, et al. Impact of coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. J Affect Disord. (2020) 275:48–57. doi: 10.1016/j.jad.2020.06.022
8. An Y, Yang Y, Wang A, Li Y, Zhang Q, Cheung T, et al. Prevalence of depression and its impact on quality of life among frontline nurses in emergency departments during the COVID-19 outbreak. J Affect Disord. (2020) 276:312–5. doi: 10.1016/j.jad.2020.06.047
9. Du J, Dong L, Wang T, Yuan C, Fu R, Zhang L, et al. Psychological symptoms among frontline healthcare workers during COVID-19 outbreak in Wuhan. Gen Hosp Psychiatry. (2020) 67:144–5. doi: 10.1016/j.genhosppsych.2020.03.011
10. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. (2020) 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
11. Tuna O, Enez Darcin A, Tarakcioglu MC, Aksoy UM. COVID-19 positive psychiatry inpatient unit: a unique experience. Asia Pac Psychiatry. (2020) 12:e12410. doi: 10.1111/appy.12410
12. Xia L, Chen C, Liu Z, Luo X, Guo C, Liu Z, et al. Prevalence of sleep disturbances and sleep quality in Chinese healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Front Psychiatry. (2021) 12:646342. doi: 10.3389/fpsyt.2021.646342
13. Zhou Y, Yang Y, Shi T, Song Y, Zhou Y, Zhang Z, et al. Prevalence and demographic correlates of poor sleep quality among frontline health professionals in Liaoning Province, China during the COVID-19 outbreak. Front Psychiatry. (2020) 11:520. doi: 10.3389/fpsyt.2020.00520
14. Ofner-Agostini M, Gravel D, McDonald LC, Lem M, Sarwal S, McGeer A, et al. Cluster of cases of severe acute respiratory syndrome among Toronto healthcare workers after implementation of infection control precautions: a case series. Infect Control Hosp Epidemiol. (2006) 27:473–8. doi: 10.1086/504363
16. Tang C, Liu C, Fang P, Xiang Y, Min R. Work-related accumulated fatigue among doctors in tertiary hospitals: a cross-sectional survey in six provinces of China. Int J Environ Res Public Health. (2019) 16:3049. doi: 10.3390/ijerph16173049
17. Gaba DM, Howard SK. Fatigue among clinicians and the safety of patients. N Engl J Med. (2002) 347:1249–55. doi: 10.1056/NEJMsa020846
18. Torres-Harding S, Jason LA. What is fatigue? History and epidemiology. In: In J. DeLuca editors. Fatigue as a Window to the Brain. Cambridge, MA: MIT Press (2005). p. 3–17.
19. Berger AM, Abernethy AP, Atkinson A, Barsevick AM, Breitbart WS, Cella D, et al. NCCN clinical practice guidelines cancer-related fatigue. J Natl Compr Canc Netw. (2010) 8:904–31. doi: 10.6004/jnccn.2010.0067
20. Radbruch L, Strasser F, Elsner F, Gonçalves JF, Løge J, Kaasa S, et al. Fatigue in palliative care patients – an EAPC approach. Palliat Med. (2008) 22:13–32. doi: 10.1177/0269216307085183
21. Oldenmenger WH, de Raaf PJ, de Klerk C, van der Rijt CC. Cut points on 0-10 numeric rating scales for symptoms included in the Edmonton Symptom Assessment Scale in cancer patients: a systematic review. J Pain Symptom Manage. (2013) 45:1083–93. doi: 10.1016/j.jpainsymman.2012.06.007
22. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
23. Wang W, Bian Q, Zhao Y, Li X, Wang W, Du J, et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. (2014) 36:539–44. doi: 10.1016/j.genhosppsych.2014.05.021
24. Moriarty AS, Gilbody S, McMillan D, Manea L. Screening and case finding for major depressive disorder using the Patient Health Questionnaire (PHQ-9): a meta-analysis. Gen Hosp Psychiatry. (2015) 37:567–76. doi: 10.1016/j.genhosppsych.2015.06.012
25. The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. (1998) 28:551–8. doi: 10.1017/S0033291798006667
26. Skevington SM, Lotfy M, O'Connell KA. The World Health Organization's WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. (2004) 13:299–310. doi: 10.1023/B:QURE.0000018486.91360.00
27. Xia P, Li N, Hau KT, Liu C, Lu Y. Quality of life of Chinese urban community residents: a psychometric study of the mainland Chinese version of the WHOQOL-BREF. BMC Med Res Methodol. (2012) 12:37. doi: 10.1186/1471-2288-12-37
28. Yang SC, Kuo PW, Wang JD, Lin MI, Su S. Development and psychometric properties of the dialysis module of the WHOQOL-BREF Taiwan version. J Formos Med Assoc. (2006) 105:299–309. doi: 10.1016/S0929-6646(09)60121-2
29. Yifan T, Ying L, Chunhong G, Jing S, Rong W, Zhenyu L, et al. Symptom cluster of ICU nurses treating COVID-19 pneumonia patients in Wuhan, China. J Pain Symptom Manage. (2020) 60:e48–53. doi: 10.1016/j.jpainsymman.2020.03.039
30. Lu W, Wang H, Lin Y, Li L. Psychological status of medical workforce during the COVID-19 pandemic: a cross-sectional study. Psychiatry Res. (2020) 288:112936. doi: 10.1016/j.psychres.2020.112936
31. Liu CY, Yang YZ, Zhang XM, Xu X, Dou QL, Zhang WW, et al. The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: a cross-sectional survey. Epidemiol Infect. (2020) 148:e98. doi: 10.1017/S0950268820001107
32. Li R, Pei S, Chen B, Song Y, Zhang T, Yang W, et al. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science. (2020) 368:489–93. doi: 10.1126/science.abb3221
33. Evans NG. Covid-19: the ethics of clinical research in quarantine. BMJ. (2020) 369:m2060. doi: 10.1136/bmj.m2060
34. Zhang M, Zhou M, Tang F, Wang Y, Nie H, Zhang L, et al. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J Hosp Infect. (2020) 105:183–7. doi: 10.1016/j.jhin.2020.04.012
35. Bianchi R, Schonfeld IS, Laurent E. Burnout symptoms: depressive manifestations under psychosocial labels? Asia Pac Psychiatry. (2017) 9:e12280. doi: 10.1111/appy.12280
36. Wen J, Cheng Y, Hu X, Yuan P, Hao T, Shi Y. Workload, burnout, and medical mistakes among physicians in China: a cross-sectional study. Biosci Trends. (2016) 10:27–33. doi: 10.5582/bst.2015.01175
37. Xiang YT, Zhao N, Zhao YJ, Liu Z, Zhang Q, Feng Y, et al. An overview of the expert consensus on the mental health treatment and services for major psychiatric disorders during COVID-19 outbreak: China's experiences. Int J Biol Sci. (2020) 16:2265–70. doi: 10.7150/ijbs.47419
38. Barker LM, Nussbaum MA. Fatigue, performance and the work environment: a survey of registered nurses. J Adv Nurs. (2011) 67:1370–82. doi: 10.1111/j.1365-2648.2010.05597.x
39. Geiger-Brown J, Rogers VE, Trinkoff AM, Kane RL, Bausell RB, Scharf SM. Sleep, sleepiness, fatigue, and performance of 12-hour-shift nurses. Chronobiol Int. (2012) 29:211–9. doi: 10.3109/07420528.2011.645752
40. Demyttenaere K, De Fruyt J, Stahl SM. The many faces of fatigue in major depressive disorder. Int J Neuropsychopharmacol. (2005) 8:93–105. doi: 10.1017/S1461145704004729
41. Targum SD, Fava M. Fatigue as a residual symptom of depression. Innov Clin Neurosci. (2011) 8:40–3.
42. Bonomi AE, Patrick DL, Bushnell DM, Martin M. Validation of the United States' version of the World Health Organization Quality of Life (WHOQOL) instrument. J Clin Epidemiol. (2000) 53:1–12. doi: 10.1016/S0895-4356(99)00123-7
43. Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, job dissatisfaction. JAMA. (2002) 288:1987–93. doi: 10.1001/jama.288.16.1987
44. Su JA, Weng HH, Tsang HY, Wu JL. Mental health and quality of life among doctors, nurses and other hospital staff. Stress Health J Int Soc Investig Stress. (2009) 25:423–30. doi: 10.1002/smi.1261
Keywords: COVID-19, fatigue, ophthalmology, otolaryngology, clinicians, quality of life
Citation: Jin Y, Li Y, Li X-Y, Zhao Y-J, Cheung T, Ungvari GS, Li M, An F-R and Xiang Y-T (2021) Prevalence of Fatigue and Its Association With Quality of Life Among Frontline Clinicians in Ophthalmology and Otolaryngology Departments During the COVID-19 Pandemic. Front. Psychiatry 12:678917. doi: 10.3389/fpsyt.2021.678917
Received: 10 March 2021; Accepted: 02 June 2021;
Published: 09 July 2021.
Edited by:
Charlotte R. Blease, Beth Israel Deaconess Medical Center and Harvard Medical School, United StatesReviewed by:
Siddharth Sarkar, All India Institute of Medical Sciences, IndiaChun Yang, Nanjing Medical University, China
Copyright © 2021 Jin, Li, Li, Zhao, Cheung, Ungvari, Li, An and Xiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Feng-Rong An, YWZyeWxtQHNpbmEuY29t
†These authors have contributed equally to this work