
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 20 May 2021
Sec. Public Mental Health
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.676256
This article is part of the Research TopicImproving Disaster Health Outcomes and Resilience through Rapid Research: Implications for Public Health Policy and PracticeView all 17 articles
 Matthew R. G. Brown1,2
Matthew R. G. Brown1,2 Hannah Pazderka2
Hannah Pazderka2 Vincent I. O. Agyapong2
Vincent I. O. Agyapong2 Andrew J. Greenshaw2
Andrew J. Greenshaw2 Ivor Cribben3
Ivor Cribben3 Pamela Brett-MacLean2
Pamela Brett-MacLean2 Julie Drolet4
Julie Drolet4 Caroline B. McDonald-Harker5
Caroline B. McDonald-Harker5 Joy Omeje2
Joy Omeje2 Bonnie Lee6Monica Mankowsi7Shannon Noble8
Bonnie Lee6Monica Mankowsi7Shannon Noble8 Deborah T. Kitching7
Deborah T. Kitching7 Peter H. Silverstone2*
Peter H. Silverstone2*In Fort McMurray, Alberta, Canada, the wildfire of May 2016 forced the population of 88,000 to rapidly evacuate in a traumatic and chaotic manner. Ten percentage of the homes in the city were destroyed, and many more structures were damaged. Since youth are particularly vulnerable to negative effects of natural disasters, we examined possible long-term psychological impacts. To assess this, we partnered with Fort McMurray Public and Catholic Schools, who surveyed Grade 7–12 students (aged 11–19) in November 2017, 2018, and 2019—i.e., at 1.5, 2.5, and 3.5 years after the wildfire. The survey included validated measurement scales for post-traumatic stress disorder (PTSD), depression, anxiety, drug use, alcohol use, tobacco use, quality of life, self-esteem, and resilience. Data analysis was done on large-scale anonymous surveys including 3,070 samples in 2017; 3,265 samples in 2018; and 3,041 samples in 2019. The results were unexpected and showed that all mental health symptoms increased from 2017 to 2019, with the exception of tobacco use. Consistent with this pattern, self-esteem and quality of life scores decreased. Resilience scores did not change significantly. Thus, mental health measures worsened, in contrast to our initial hypothesis that they would improve over time. Of note, we observed higher levels of mental health distress among older students, in females compared to male students, and in individuals with a minority gender identity, including transgender and gender-non-conforming individuals. These findings demonstrate that deleterious mental health effects can persist in youth for years following a wildfire disaster. This highlights the need for multi-year mental health support programs for youth in post-disaster situations. The indication that multi-year, post-disaster support is warranted is relatively novel, although not unknown. There is a need to systematically investigate factors associated with youth recovery following a wildfire disaster, as well as efficacy of psychosocial strategies during later phases of disaster recovery relative to early post-disaster interventions.
In May 2016, a large wildfire affected Fort McMurray, Alberta, Canada and the surrounding area. Called “The Beast” in the popular media (1), the wildfire necessitated the evacuation of the entire city on May 3, 2016, and over 88,000 residents were displaced for several weeks. In addition to damaging community structures and infrastructure, the fire destroyed 10% of the homes in Fort McMurray, leaving many individuals homeless. The fire burned 590,000 hectares of land before it was brought under control on July 4, 2016. Insurance costs for the damages were estimated at $3.6 billion by the Insurance Bureau of Canada, which made the Fort McMurray wildfire the most expensive insured catastrophe in Canadian history (2). Many individuals were left jobless due to damage and closure of local businesses. Social, emotional, and psychological difficulties also affected the community, as is typical after severe disasters (3, 4).
Disasters tend to impact children and youth in particular (5–10) given developmental vulnerabilities (cognitive, emotional, social, and physiological) associated with childhood and adolescence, including the need to rely on others for support (11). Our group has previously examined Fort McMurray school mental health surveys completed by Grade 7–12 students in November 2017 (12, 13). Brown et al. (12) reported elevated mental health symptoms for PTSD and depression compared to a control population from the same province which had not experienced a natural disaster. As reported in (13), individuals who were more personally impacted by the 2016 wildfire, such as having their home destroyed, exhibited greater symptoms of PTSD, depression, anxiety, and alcohol and/or substance misuse. These findings were consistent with previous findings of altered mental health in youth following natural disasters (9, 14).
Previous studies have also reported links between wildfires and adverse mental health effects in adults and children, including increased symptoms of PTSD (15–24), increased symptoms of depression and anxiety (17, 19, 23–28), mental health difficulties (18, 29, 30), reduction in health and well-being (31), increased consumption of anxiolytics-hypnotics (32), and decreased capacity to cope with adversity (33). The combined adverse impacts of wildfire disasters on individuals' mental health and coping abilities, particularly in youth, are important because coping plays a major role in post-disaster recovery, and lack thereof can be detrimental to long-term mental health outcomes [also see (34)]. More generally, non-wildfire disasters, including floods, earthquakes, and tsunamis, have also been linked to adverse effects on mental health in adults and children in the form of increased symptoms or incidences of PTSD, major depressive disorder, suicidality, generalised anxiety disorder, and substance use disorder [see (8, 9, 35–39)]. Displacement caused by natural disasters (e.g., short- and long-term evacuation, homelessness) imposes additional physical, emotional, and psychosocial stress on families, which may then adversely affect longer-term development of children and youth (40).
Longitudinal studies, most of which have focused on adults, have reported long-term negative impacts on mental health from natural disasters (17, 25, 41–46). The pattern of long-term effects can be complex, with individuals exhibiting better recovery from some symptoms, such as depression or anxiety, but lesser recovery for others such as PTSD symptoms (47). Relatively few longitudinal studies have focused on mental health outcomes among youth following natural disaster, although studies of children and youth following Hurricane Katrina have shown long term impacts on mental health (48), with varying recovery trajectories for different groups (49, 50). We are aware of only three population studies that examined wildfire impacts on youth mental health, including one study focusing on PTSD and depression (19) and our previous Fort McMurray studies (12, 13).
In the present study, our hypothesis was that mental health symptoms among Fort McMurray youth would improve with time following the November 2017 survey. This hypothesis was based on theoretical work on trauma recovery, which consistently emphasises the role of time in the recovery process (4, 51, 52). To test this hypothesis, we examined mental health survey data collected by Fort McMurray school boards in Grades 7–12 in November across three consecutive years, including 2017, 2018, and 2019. This repeated testing was conducted 1.5, 2.5, and 3.5 years after the 2016 wildfire (All data were collected prior to the COVID-19 pandemic). We hypothesised specifically that symptoms of PTSD, depression, anxiety, and alcohol/substance use would steadily improve from 2017 to 2018 to 2019.
Information collected from students included questions on demographics, mental health, resilience, and personal exposure to and direct impacts of the wildfire. Measurement instruments were selected by the school systems, informed by the relevant literature and advice from the University of Alberta research team. Written letters were sent to parents and guardians to inform them of the survey 2 weeks prior. Parents and guardians could have their child(ren) not participate in the survey, and students also independently had the option to participate or not in the survey as explained at the start of each survey session (see details below and Appendix A: Survey Description Script in the Supplementary Material). Survey data collection was intentionally anonymous, and participants were not asked for their names nor any other identifying information. The study design was approved by the University of Alberta's Health Research Ethics Board (ethics protocol number Pro00072669 approved June 26, 2017). This paper reports on findings from the anonymous survey data collected from both school boards.
Mental health surveys were conducted by the two school boards in Fort McMurray—Fort McMurray Public Schools and Fort McMurray Catholic Schools (henceforth, “Schools”). They asked all students in Grades 7–12 to complete the surveys in November 2017 (18 months after the 2016 wildfire), November 2018 (30 months post-wildfire), and November 2019 (42 months post-wildfire) (All data were collected before the COVID-19 pandemic). The survey was administered during regular class time as part of the standard curriculum to evaluate the support programs the Schools had put in place following the wildfire (see Appendix B: Mental Health Support Programs, in the Supplementary Material). The Schools determined that surveys would be done in November 2017, 2018, and 2019 as the month of November worked best given various logistical and staff capacity considerations.
Fort McMurray Public Schools and Fort McMurray Catholic Schools (“Schools”) administered all aspects of survey data collection, including participant consent, in accordance with their standard procedures and policies. The Schools asked researchers from the University of Alberta for assistance in designing the survey and analysing the anonymous dataset.
The survey included 10 questionnaires (see Table 1 for additional details):
1. Demographics Questionnaire (Demographics, 7 questions)—a custom-designed questionnaire assessing age, gender, and the student's grade and school.
2. Impact of Fire Questionnaire (IOF, 6 questions)—a custom-designed questionnaire to assess the impact of the 2016 wildfire on the student.
3. Child PTSD Symptom Scale (CPSS, 19 questions)—used to assess symptoms of post-traumatic stress disorder (PTSD) (53); total CPSS score ranges from 0 to 51.
4. Patient Health Questionnaire, Adolescent version (PHQ-A, 11 questions)—used to assess symptoms of depression and suicidality (54, 55); total PHQ-A score ranges from 0 to 27.
5. Hospital Anxiety and Depression Scale (HADS, 7 questions, anxiety-related questions only)—used to assess symptoms of anxiety (56); total HADS score ranges from 0 to 21.
6. CRAFFT Questionnaire (CRAFFT, 9 questions)—used to assess symptoms of alcohol and substance misuse (57, 58); total CRAFFT scores ranges from 0 to 6.
7. Tobacco Use Questionnaire (2 questions) – two questions on tobacco use: “During the past month, did you smoke tobacco products?” and “During the past month, did you use smokeless tobacco products?”
8. Rosenberg Self-Esteem Scale (Rosenberg, 10 questions)—used to assess self-esteem (59); total score ranges from 0 to 30 with higher scores indicating higher self-esteem.
9. Kidscreen Questionnaire (Kidscreen-10, 11 questions)—used to assess quality of life (60); total Kidscreen-10 score ranges from 0 to 44 with higher scores indicating better quality of life.
10. Child and Youth Resilience Measure (CYRM-12, 12 questions)—used to assess resilience to adverse experience or trauma (61); total CYRM-12 score ranges from 12 to 60.
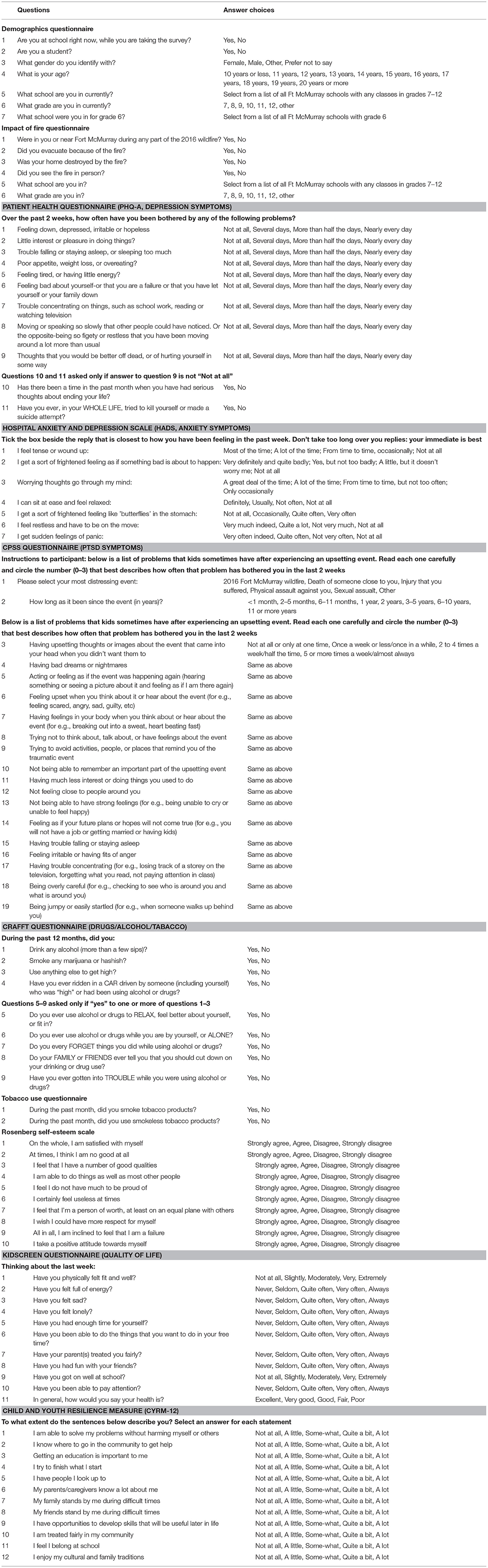
Table 1. Questionnaire details [table reproduced with permission from our previously-published paper Brown et al. (13)].
The vast majority (>98%) of students who completed the survey did so during regular school hours. A few students citing special circumstances completed the survey from home on their own computers. Depending on their school, students either completed the survey using a desktop computer in a computer laboratory or used laptops brought to their classroom. The survey website was based on an HTML/CSS front end and a back end server written in the Clojure programming language (http://clojure.org). A survey description script was read to each class at the beginning of the survey session (reproduced in the Supplementary Material). The script explained the purpose of the survey and provided instructions for completing the survey. It also explained that the survey was anonymous (participants were not asked for their names nor date of birth) and that participation was voluntary. Students had an opportunity to ask questions before participating. The survey battery included 96 questions in total. Participation required <20 min for most students, but a small number of students took up to 50 min. Participants were able to skip questions, but the survey description script and the survey website did encourage them to answer all questions.
The first mental health survey of Fort McMurray Grade 7–12 students was completed in November 2017 and was then repeated in November 2018 and November 2019. Many students were present for the survey across all 3 years. Other students were present for only 1 or 2 years. For example, students entering Grade 7 in September 2018 or September 2019 were not surveyed in earlier years (i.e., November 2017 and November 2018, respectively). Similarly, students graduating from Grade 12 in June 2018 or June 2019 were not re-surveyed the following November. Some students also moved to, or away from, Fort McMurray between 2017 and 2019. In summary, some of the surveys collected in 2017, 2018, and 2019 were completed by unique students (i.e., no repetition), although the majority were completed by the same students (i.e., repeated measures over 2 or 3 years). Because survey responses were anonymous, we were unable to link surveys completed by specific students from 1 year to the next. We therefore employed a between-subject analysis (treating all survey samples as independent) rather than using a repeated-measures, within-subject analysis over successive years. It is important to note that adopting a between-subject approach is statistically conservative as there is an expectation of increased overall error variance compared to the likely advantage of within-subject analysis.
Probable diagnoses of four different psychiatric conditions were established by thresholding each participant's scores on specific scales. Threshold values for probable diagnoses were derived from the relevant literature for each scale, as described below. Specific probable diagnoses included PTSD (based on the CPSS scale), depression (from the PHQ-A), anxiety (from the HADS), and alcohol/substance use disorder (based on the CRAFFT).
The term “probable diagnosis” is used here, as opposed to “clinical diagnosis,” because the scores were based on self-report scales rather than psychiatric clinical interviews. The literature reports good agreement between psychiatric clinical diagnoses of PTSD, depression, anxiety, and alcohol/substance use disorder with probable diagnoses derived from widely-published threshold scores for the above four questionnaires (57, 58, 62–65), and we have previously used this approach (66).
Probable PTSD was determined based on a CPSS score of 15 or more (65, 67). Probable depression was determined based on a PHQ-A score of 11 or more (63). Probable moderately severe depression was determined based on a PHQ-A score of 15 or more (62). Suicidal thinking was determined from responses to two questions from the PHQ-A: question 9 “Over the past 2 weeks, how often have you been bothered by any of the following problems: Thoughts that you would be better off dead, or of hurting yourself in some way?” and question 10 “Has there been a time in the past month when you have had serious thoughts about ending your life?” Participants were assessed as exhibiting suicidal thinking if they answered “Several days,” “More than half the days,” or “Nearly every day” to PHQ-A question 9 and “Yes” to question 10. Participants answering “Not at all” to question 9 skipped (were not shown) question 10, and they were assessed as not exhibiting suicidal thinking. In addition, participants answering “Several days,” “More than half the days,” or “Nearly every day” to PHQ-A question 9 and “No” to question 10 were assessed as not exhibiting suicidal thinking (as distinct from thinking about self-harm) (PHQ-A question 11 was not considered in the definition of suicidal thinking). Probable anxiety was determined based on a HADS score of 11 or more (64). Probable alcohol/substance use disorder was determined based on a CRAFFT score of 2 or more (57, 58). Tobacco use was determined as answering “yes” to either of the two questions on the Tobacco Use Questionnaire. Finally, an “Any of 4 probable diagnoses” criterion was defined as being positive for one or more of the four probable diagnoses: PTSD, depression, anxiety, or alcohol/substance use disorder.
We examined the following 15 dependent measures: (1) CPSS PTSD score, (2) PHQ-A depression score, (3) HADS anxiety score, (4) CRAFFT alcohol/substance use score, (5) Rosenberg self-esteem score, (6) Kidscreen quality of life score, (7) CYRM-12 resilience score, (8) percent probable PTSD, (9) percent probable depression, (10) percent probable moderately severe depression, (11) percent suicidal thinking, (12) percent probable anxiety, (13) percent probable alcohol/substance use disorder, (14) percent tobacco use, and (15) percent any of four probable diagnoses (See “Cut-off Scores and Probable Diagnoses” section above for details of scoring cut-offs used to determine probable diagnoses). In analysing data for a given measure (e.g., mean CPSS) or probable diagnosis (e.g., probable PTSD), we included only those participants who provided answers for all questions in the relevant questionnaire.
For each of the 15 dependent measures, we tested five statistical effects: (1) linear effect of time (2017 vs. 2018 vs. 2019), (2) linear effect of age (11 to 19 years old), (3) effect of female vs. male gender identity, (4) effect of other vs. female/male gender identity, and (5) effect of preferred not to say vs. female/male gender identity.
Participant age was determined by Demographics Questionnaire question 4 “What is your age?,” with answer choices “10 years or less,” “11 years,” “12 years,” “13 years,” “14 years,” “15 years,” “16 years,” “17 years,” “18 years,” “19 years,” and “20 years or more.” Note that participants answering “10 years or less” or “20 years or more” were excluded to enable modelling of age as a linear variable (see “Data Exclusion” section in the Results).
Participant gender identity was determined based on Demographics Questionnaire question 3 “What gender do you identify with?,” with answer choices “female,” “male,” “other,” and “prefer not to say.” Statistical test 3 (female vs. male) compared participants answering “female” vs. those answering “male.” Test 4 (other vs. female/male) compared participants answering “other” vs. those answering either “female” or “male.” Test 5 (preferred not to say vs. female/male) compared participants answering “prefer not to say” vs. those answering either “female” or “male.” Each test of a gender effect included only those participants with the relevant gender identities (test 3: female and male; test 4: female, male, and other; test 5: female, male, and preferred not to say).
All statistical comparisons were done using permutation testing on the slope parameter from a fitted linear model, with a null hypothesis of zero slope. The linear model included a slope parameter for the effect variable (time, age, female vs. male, other vs. female/male, preferred not to say vs. female/male) as well as parameters for “nuisance variables” as described below. Mathematical details of the linear modelling procedure are included in the “Details of Linear Modelling” section below.
Permutation testing is a non-parametric method and was chosen for its robustness against non-normality. The number of iterations was 105 for all permutation tests. All tests were two-tailed (That is, to compute the p-value for a given test, the absolute value of the slope parameter fitted to the real data was compared against the absolute values of the 105 simulated slope parameters fitted to permuted data).
In total, our analysis of the five statistical effects for each of 15 dependent variables included 75 individual statistical tests. We addressed multiple comparisons using the Benjamini-Hochberg method for false discovery rate (FDR) correction. This method computed a threshold of p = 0.025 for FDR correction across all 75 tests.
Distributions of gender identities and ages were similar across time, and the distribution of gender identities was similar across different ages (see “Demographics” in the Results section). Nonetheless, to address the possibility that results for one effect might have been driven in part by some small difference in one or more of the other effect variables, we included “nuisance variables” in the linear models to which permutation testing was applied. To test effects of time (2017 vs. 2018 vs. 2019), we used a linear model with a term for time as well as nuisance variables including a covariate for age and four indicator variables for gender identity: female, male, other, and preferred not to say. For analyses on the effects of time, only the fitted slope parameter for time was used to generate p-values. Including the other nuisance variables allowed the model to separate out effects of age and gender from effects of time. Similarly, analyses of age used five nuisance variables, including a time covariate and four indicator variables for gender identities. Analyses of gender effects (female vs. male, other vs. female/male, preferred not to say vs. female/male) included time and age as nuisance variables.
As expected from a sample of students in Grade 7–12, there were substantially fewer participants who were 11 or 18–19 years old, compared to those who were 12–17 years old, at the time of data collection (see “Demographics” in the Results section). To address the possibility that results for effects of age might be driven by leverage effects from smaller sample numbers in the extremes (aged 11 or 18–19 years old), we ran a follow-up analysis which included only participants aged 12–17.
We performed all analyses using in-house computer code written in the Clojure programming language (http://clojure.org). The code for statistical testing and FDR correction is available at http://github.com/mbrown/mrgbstats.
For a given analysis, we defined an effect variable xi and a dependent variable yi, as well as J covariate nuisance variables vj, i and K indicator nuisance variables wk, i, where i∈[1, N] with N being the number of surveys used in the analysis.
For analyses on effects of time or effects of age, the effect variable xi was mean-centred to make it “independent” (orthogonal) to the intercept (i.e., constant offset). For analyses on effects of gender (female vs. male, other vs. female/male, preferred not to say vs. female/male), the effect variable was categorical and therefore not mean-centred. Covariate nuisance variables vj, i were mean-centred, and indicator nuisance variables wk, i were not mean-centred.
For analyses on effects of time or effects of age, we did not include an intercept term in the model (i.e., a constant offset column containing all ones in the model matrix). Because analyses of time and age included four nuisance indicator variables for gender identities, an intercept column would have been a linear combination of those four indicator variables, rendering the model matrix degenerate. The effect variable for time or for age was mean-centred and therefore orthogonal to the constant offset, in any case. For analyses of effects of gender, which did not have the four nuisance variables for gender, we did include a constant offset term.
For each analysis, we created a model matrix X from the effect variable xi, J covariate nuisance variables vj, i, and K indicator nuisance variables wk, i, as well as a constant offset term for analyses of gender effects. Each survey i contributed one effect variable value, one dependent variable value, and one value for each of (J + K) nuisance variables. For example, for analyses on effects of time, xi was time; v1, i was age; w1, i, w2, i, w3, i, and w4, i were indicator variables for gender identity, including female, male, other, and preferred not to say; and there was no constant offset column. To take a second example, for analyses of other vs. female/male gender identity, xi was 0 for participants identifying as female or male and 1 for those with other gender identity; v1, i and v2, i were time and age, respectively; there were no indicator nuisance variables; and there was a constant offset column. We created a model matrix X with size N by (1 + J + K) or else N by (2 + J + K), for analyses without and with a constant offset column, respectively. The first column of X consisted of the effect variable values xi. If a constant offset column was included, it was the second column. The next J columns were comprised of the mean-centred covariate nuisance variables vj, i, and the last K columns were comprised of the indicator nuisance variables wk, i. We defined the vector where was the vector of dependent variable values yi. The slope parameter used for permutation testing was , the first element of , representing the fitted scaling parameter for the effect variable.
The survey was administered to all Grade 7–12 students in Fort McMurray, Alberta, Canada who were attending either the Public or Catholic schools on the days the survey was conducted during the month of November in 2017, 2018, and 2019. Five Public schools and two Catholic schools participated in the survey. In total, 9,920 surveys were collected during the period of 2017 to 2019. Forty five percentage were collected from Public schools and 55% from Catholic schools. As all surveys were anonymous, there was no way to identify which students did or did not repeat the survey over successive years.
Data from 544 surveys were excluded based the following exclusion criteria:
1. Participant answered “10 years or less” to the age question (Demographics Questionnaire question 4).
2. Participant answered “20 years or more” to the age question (Demographics Questionnaire question 4).
3. Participant gave inconsistent answers for positive and negative questions included in the Rosenberg questionnaire (for details, see Appendix C: Exclusion Criteria in the Supplementary Material).
4. Participant gave inconsistent answers for positive questions from the Rosenberg questionnaire and positive questions from the Kidscreen questionnaire (see Appendix C: Exclusion Criteria the Supplementary Material, for details).
5. Participant gave inconsistent answers among the non-reversed and reversed questions from the HADS questionnaire (For two of the HADS questions, the answer order is reversed to test for consistency; see details in Supplementary Material).
Criteria 1 and 2 above excluded participants with ambiguous age. The remaining participants had non-ambiguous ages in the range 11–19 years, allowing us to model effects of age as a linear variable. Criteria 3 to 5 above excluded participants who gave inconsistent answers, possibly because they were not paying attention to the survey or did not understand the questions. After exclusions, the final dataset included 9,376 surveys.
Demographics for the 9,376 surveys were as follows. Self-reported gender identity was 47.3% female, 48.6% male, 1.7% other, and 2.4% preferred not to say. Age ranged from 11 to 19, and the mean age of participants was 14.3 years ± 1.8 (standard deviation). For additional demographic details, see Table 2. Distributions of gender identities and ages were similar across the 3 years of data collection (Table 2). The distribution of gender identities was similar across different ages as well (Table 2).
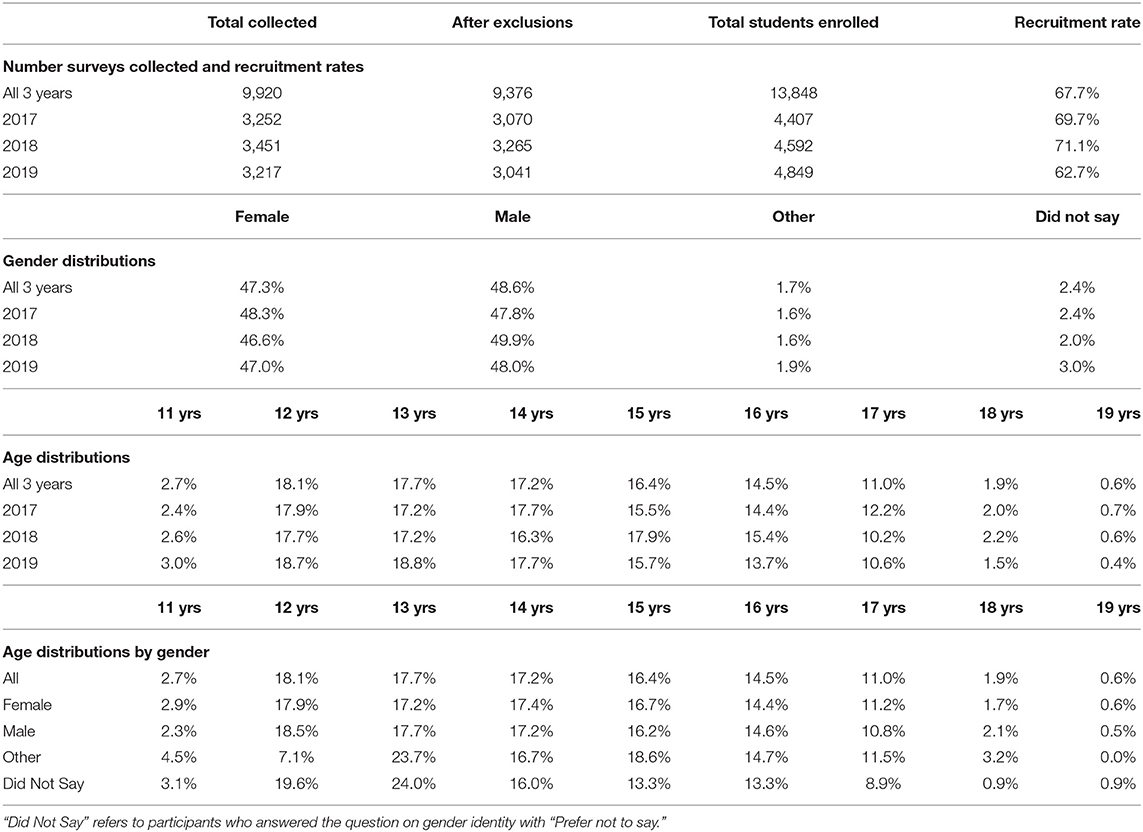
Table 2. Demographics.
Table 3 shows results for analysis of changes over time. Permutation testing of the linear effect of time, with age and gender partialled out, indicated that 13 of the 15 dependent measures changed over time during the period from 2017 to 2019, with statistical significance surviving FDR multiple comparison correction. Scores for PTSD (CPSS), depression (PHQ-A), anxiety (HADS), and alcohol/substance use (CRAFFT) increased from 2017 to 2019. Self-esteem (Rosenberg) and quality of life (Kidscreen) scores decreased. Resilience (CYRM-12) scores did not change significantly. Rates of probable diagnoses of PTSD, depression, moderately severe depression, suicidal thinking, anxiety, alcohol/substance use disorder, and the “Any of 4 probable diagnoses” category all increased. Rates of tobacco use did not change significantly.
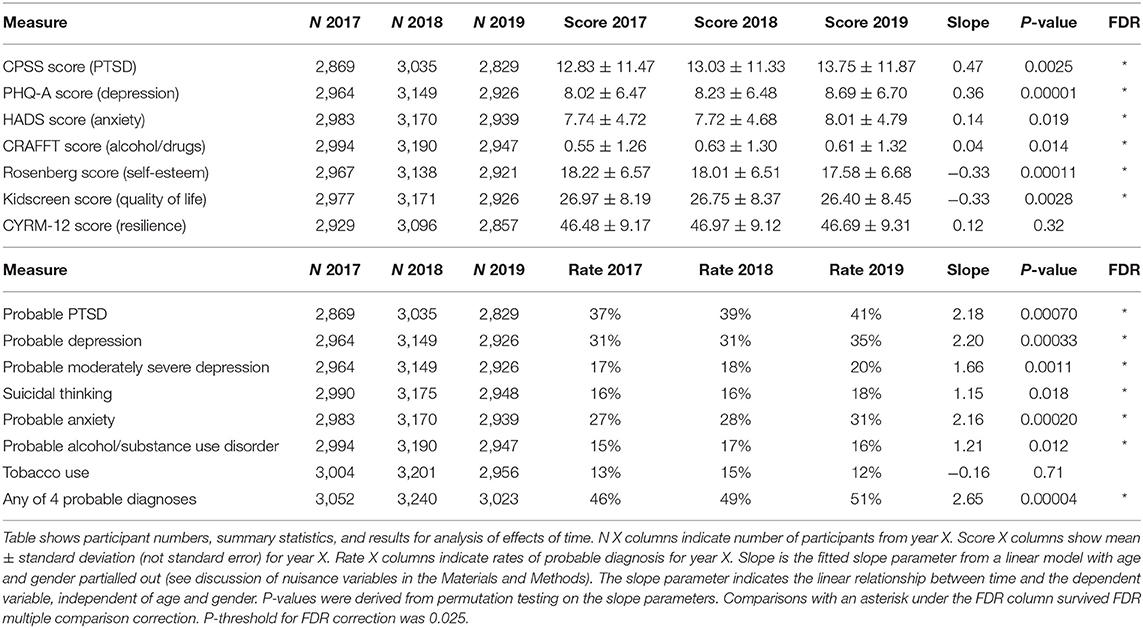
Table 3. Changes over time (2017, 2018, 2019).
Table 4 shows results for the analysis of age effects. Permutation testing of the linear effect of age over the range 11–19 years old, with time and gender partialled out, revealed that all 15 dependent measures changed with age, with statistical significance surviving FDR multiple comparison correction. Scores for PTSD (CPSS), depression (PHQ-A), anxiety (HADS), and alcohol/substance use (CRAFFT) increased with age. Self-esteem (Rosenberg), quality of life (Kidscreen), and resilience (CYRM-12) scores decreased with age. Rates of probable diagnoses of PTSD, depression, moderately severe depression, suicidal thinking, anxiety, alcohol/substance use disorder, tobacco use, and the “Any of 4 probable diagnoses” category all increased with age.
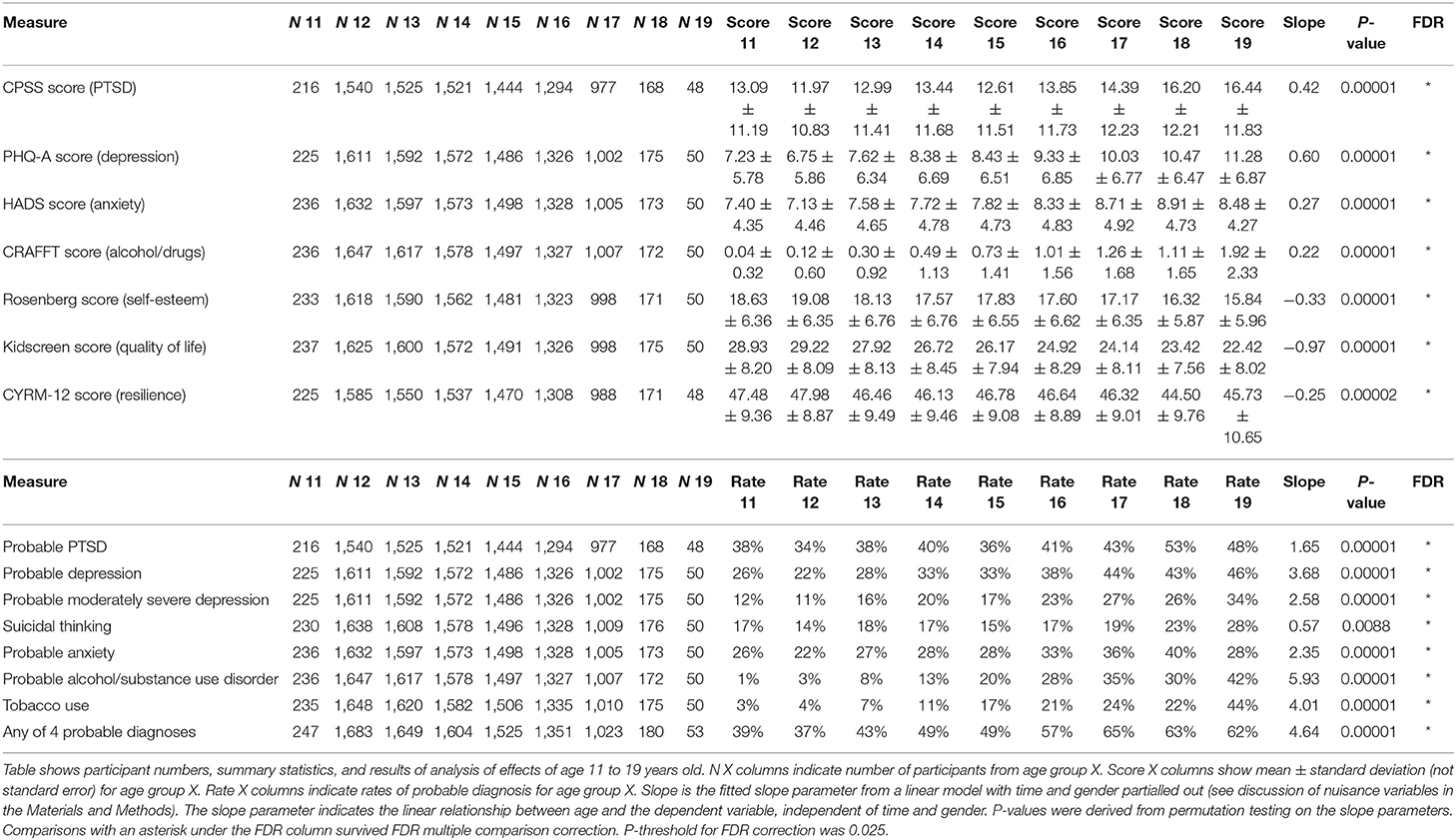
Table 4. Effects of age (11–19 years old).
We did follow-up analyses of age restricted to participants aged 12–17 years old, with time and gender partialled out. Suicidal thinking did not change significantly over time with participants aged 12–17 years (p = 0.11), in contrast to analysis of age 11–19 years, which found a statistically significant increase in the rate of suicidal thinking with age (p = 0.0088). The other 14 dependent measures exhibited the same pattern of statistically significant changes in analyses with age 12–17 years (CYRM-12 p = 0.00038, CPSS p = 0.00002, all other tests p = 0.00001) as compared to analyses with age 11–19 years.
Tables 5–7 present results of three analyses of gender identity. Gender identity was determined based on Demographics Questionnaire question 3 “What gender do you identify with?,” with answer choices “female,” “male,” “other,” and “prefer not to say.” Analyses of gender identity compared female vs. male (Table 5), other vs. female/male (Table 6), and preferred not to say vs. female/male (Table 7) (See “Dependent Variables and Statistical Effects Tested” in the Materials and Methods section for additional details). Analyses of gender effects were done using permutation testing, with time and age partialled. All 15 dependent measures showed significant differences for all three gender identity comparisons, with statistical significance surviving FDR multiple comparison correction for all tests. Scores for PTSD (CPSS), depression (PHQ-A), anxiety (HADS), and alcohol/substance use (CRAFFT) were higher in females vs. males, in those with other gender identity vs. females/males, and in those who preferred not to say vs. females/males. Self-esteem (Rosenberg), quality of life (Kidscreen), and resilience (CYRM-12) scores were lower in females, in participants with other gender identity, and in participants who preferred not to say. Rates of probable diagnoses of PTSD, depression, moderately severe depression, suicidal thinking, anxiety, alcohol/ substance use disorder, tobacco use, and the “Any of 4 probable diagnoses” category were higher in females, in those with other gender identity, and in those who preferred not to say.
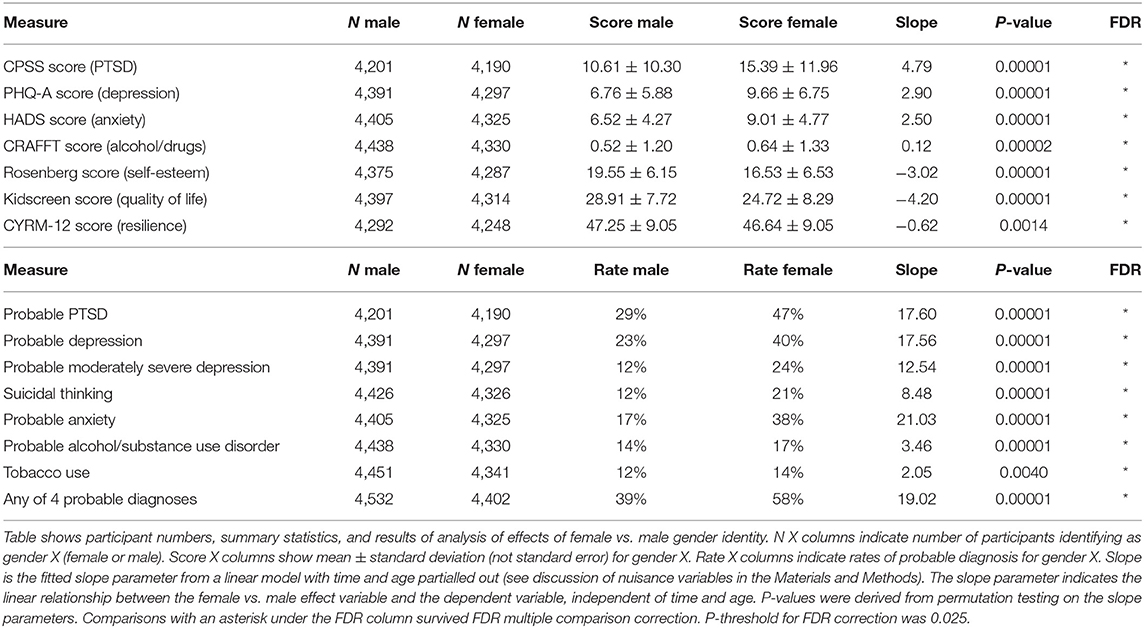
Table 5. Effects female vs. male gender identity.
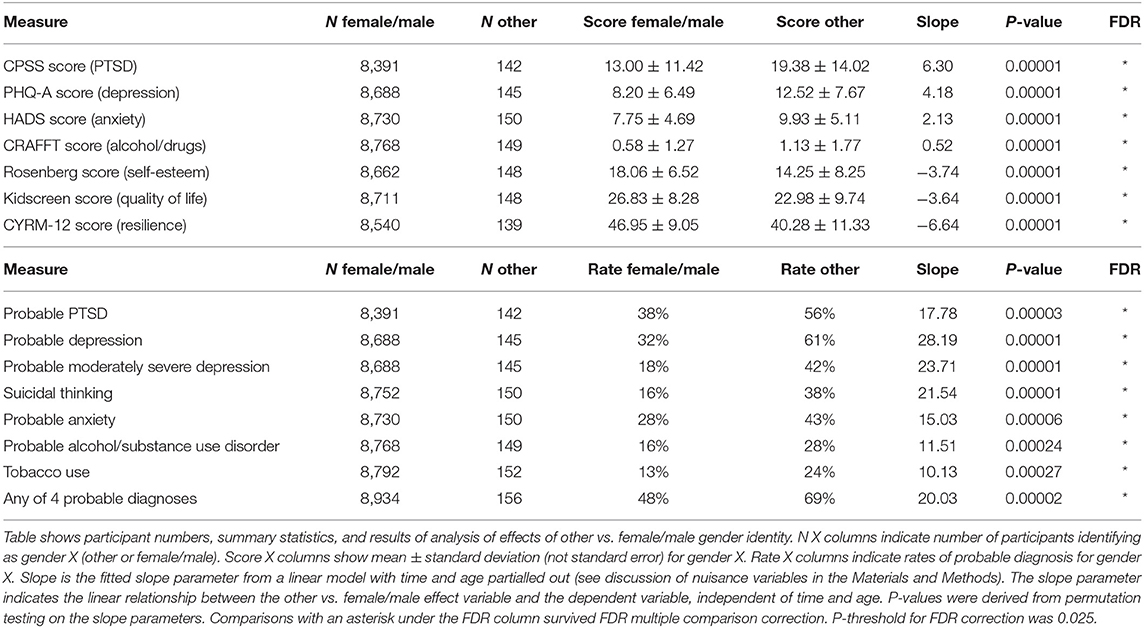
Table 6. Effects of other vs. female/male gender identity.
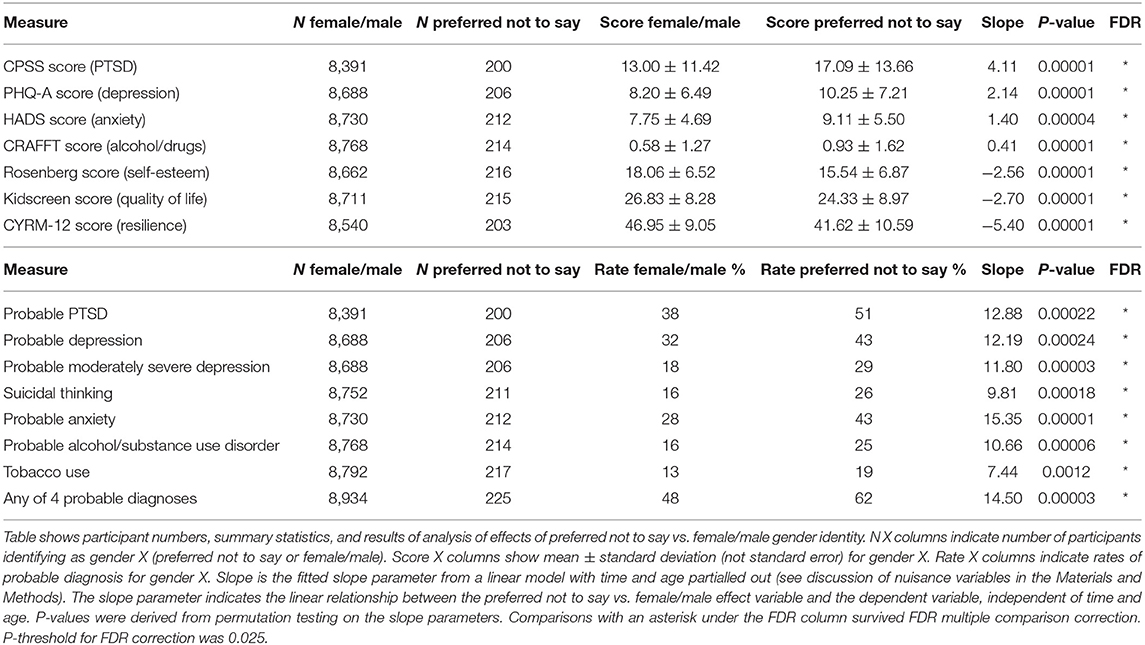
Table 7. Effects of “prefer not to say” vs. female/male gender identity.
This study investigated the multi-year impacts of wildfires on youth mental health. We examined 9,376 mental health survey samples from students in Grades 7–12 in Fort McMurray, Alberta. Surveys were conducted in 2017, 2018, and 2019, in the aftermath of the 2016 Fort McMurray wildfire.
As we have previously reported, the Fort McMurray student population exhibited elevated rates of probable depression, suicidal thinking, and tobacco use; elevated symptoms of anxiety; and reduced scores for quality of life and self-esteem 18 months after the 2016 wildfire, as compared to a control population that had not recently experienced a natural disaster (12). At that time, we observed similar mental health patterns for youth who were not actually present in Fort McMurray during the 2016 wildfire, although youth with greater personal exposure to impacts of the fire (e.g., home destroyed) exhibited worse symptoms of PTSD, depression, anxiety, and alcohol/substance use and lower scores for self-esteem and quality of life (13). The current study provides evidence of ongoing long-term mental health impacts on youth 3.5 years (42 months) post-wildfire.
The results from the present study indicate a slow but statistically significant trend of worsening mental health from 2017 to 2019, including increased symptom scores and increased rates of probable diagnoses of PTSD, depression, anxiety, drug use, and alcohol use. Quality of life and self-esteem scores also decreased from 2017 to 2019. Tobacco use and resilience scores did not change significantly. These findings are consistent with other studies reporting long-term negative impacts on mental health from natural disasters (41–45), although these studies are not directly comparable because they focused on mental health in adulthood and/or used different outcome measures.
Our results do not support our hypothesis that mental health would improve with time following the 2016 wildfire. One possibility is that 3.5 years may not be sufficient time for this population to recover from the adverse mental health effects of the wildfire, though that possibility seems unlikely in light of reports that many individuals affected by disaster do recover within 1–2 years (4). Theories of recovery from trauma identify various factors important to the recovery process including a sense of safety and stability, self- and community efficacy, hope, support from family and friends, social support, and social connectedness (4, 51, 52). It is possible that one or more factors important to recovery may be at issue. For example, Fort McMurray has experienced an economic downturn related to the reduction in oil prices starting in 2014, and this may negatively affect the community's sense of stability and hope. Future studies would be needed to test this suggestion.
It is noteworthy that CYRM-12 resilience measures did not change significantly with time (p = 0.27), indicating that the above-discussed changes in mental health measures may not be attributable to a change in resilience.
There was a statistically significant increase in suicidal thinking with age in the analysis of participants aged 11–19 (p = 0.0088) but not in the analysis of participants aged 12–17 (p = 0.11). The difference in results seems to be driven by the larger proportion of students aged 18 and 19 exhibiting suicidal thinking (18 years: 23%, 19 years: 28%) compared to younger students (14–19%) (see Table 4).
We observed worse average scores on all 15 dependent measures in older vs. younger students. Specifically, older students exhibited higher mental health symptom scores, higher rates of probable diagnoses, and lower scores for self-esteem, quality of life, and resilience. These results are consistent with previous reports of increased mental health impairment among older youth compared to younger youth post-disaster (68), as well as higher rates of mental health symptoms in older adolescents more generally (69). As has been suggested by others (68), one possible interpretation of this finding, that would bear future exploration, is that greater awareness among older youth regarding challenges facing their families and the larger community (rebuilding, economic implications, etc.), as well as concerns they may have regarding their future, may negatively influence their well-being compared to younger youth. That older students also exhibited higher mental health symptom scores and lower resilience scores is consistent previous research showing an association between lesser resilience and worse mental health outcomes following disaster (28, 35, 70, 71) and with theoretical conceptions of resilience and its role in buffering the individual's mental health from harm due to adverse experiences (72–74). Reduced resilience may have played a role in making older students more vulnerable to developing negative mental health symptoms.
Our analyses revealed worse average scores on all 15 dependent measures in students identifying as female vs. male, in students with other gender identity vs. females/males, and students who preferred not to say their gender identity vs. females/males. These specific groups of students exhibited higher mental health symptom scores, higher rates of probable diagnoses, and lower scores for self-esteem, quality of life, and resilience.
We interpret participants answering “other” to the question of their gender identity as belonging to a gender minority, including transgender or gender non-conforming. For participants who preferred not to answer the demographics question on gender identity, some presumably identified as female or male but did not want to say so, while others presumably identified as a gender minority, including transgender or gender-non-conforming. Given that the group who preferred not to answer exhibited significantly worse mental health results than those identifying as female or male, we suspect that a majority of the group who preferred not to answer in fact belonged to a gender minority, including transgender or gender-non-conforming.
The finding of worse mental health scores in females compared to males is consistent with a previous report of higher rates of mental health symptoms post-natural disaster in females vs. males (75). We are not aware of any previous studies examining the impact of natural disaster on the mental health of gender minorities, including transgender and gender non-conforming individuals. It is a benefit of our population study approach, with its large sample size, that we are able to do so for the first time. More generally, our results are consistent with previous reports indicating higher rates of mental health symptoms in gender minorities, including transgender and gender-non-conforming individuals, both adults and youth (76–79). Resilience scores were lower for females vs. males and for gender minorities vs. females/males, which is consistent with previous studies showing an association between lesser resilience and worse mental health outcomes following disaster (28, 35, 70, 71). This suggests that reduced resilience may have been a factor in specific groups' developing more negative mental health symptoms.
The destructive nature of disasters tends to attract funding from government and charities to address the immediate aftermath of a disaster. Our results provide an example of worsening mental health impacts in youth during the period 1.5–3.5 years following a wildfire disaster. This has occurred in the context of an ongoing, whole-of-community “build back better” approach to post-wildfire recovery in the area (80), as well as multiple challenges that have faced the community since the 2016 wildfire, including a downturn in the economy (Additional challenges include disastrous flooding following the 2020 spring ice breakup and the outbreak of the COVID-19 pandemic in 2020, though these occurred after the last survey data collection was completed in 2019). Our results underscore the need for multi-year funding, interventions, and policies to address not only the short-term physical damage but also the long-term negative mental health effects of natural disasters.
In addition to focusing on symptomatology, there is a need to investigate factors associated with post-disaster recovery processes, as well as efficacy of psychosocial strategies during later phases of recovery relative to early interventions, while also recognising complex and evolving, social-ecological post-disaster contexts. As an example, given that specific groups exhibited greater negative mental health effects, namely older youth, females, and gender minorities, interventions and policies may be more effective if they take into account developmental stage and gender identity with respect to mitigating these effects.
Our analysis included a large dataset of 9,376 survey responses. Conducting full clinical interviews with this large number of participants is not feasible, and so we used clinical measures based on self-report questionnaires, which is a limitation of the study. As noted above, in addition to the 2016 wildfire, Fort McMurray has experienced an economic downturn since 2014. The resulting job losses and financial impacts on families also likely had an effect on youth mental health in addition to the 2016 wildfire. We are not aware of any study specifically on the effects of Alberta's economic downturn on youth mental health, though one report found a negative mental health impact in adults (81). Additionally, given that this study utilised anonymous data, we were not able to identify longitudinal trends in individuals, only in groups.
This study presents a cross-sectional statistical analysis of longitudinal mental health measurements in a population of Fort McMurray youth in Grades 7–12 during the period of 1.5–3.5 years following the 2016 Alberta wildfire. Findings indicate that there was a long-term trend of worsening mental health during that period. These observations support previous reports that youth and communities experience long-term mental health impacts following major natural disasters, such as wildfires. Our findings emphasise the need for multi-year funding and programs to support child and youth mental health in communities that have experienced such disasters.
Some portions of the manuscript, in the Materials and Methods section, are based on similar material from two previous papers (12, 13) presenting findings from separate analyses of the data from Fort McMurray collected in 2017 only.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. Requests for data access should be made by email to the corresponding author.
This study involving human participants was reviewed and approved by the University of Alberta's Health Research Ethics Board (ethics protocol number Pro00072669 approved June 26, 2017). Data were collected as part of the Fort McMurray Public and Catholic Schools' standard curriculum to evaluate their support programs. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study, in accordance with the national legislation and the institutional requirements. Parents/guardians were notified of the study 2 weeks prior and were given the opportunity to opt their child(ren) out of the study. Participants themselves were given the opportunity to opt out of the study, as was explained to them at the beginning of each study survey session.
MB, VA, AG, PB-M, JD, CM-H, JO, MM, SN, DK, and PS: study design. MM, SN, and DK: data collection. MB, HP, IC, and PS: analysis. MB, HP, AG, IC, PB-M, JD, CM-H, BL, and PS: manuscript preparation. All authors contributed to the article and approved the submitted version.
Funding to support the Fort McMurray schools in developing their survey and to conduct statistical analyses and reporting was provided by a collaborative grant from the Canadian Institutes of Health Research, Canadian Red Cross, and Alberta Innovates Health Solutions (Grant No. 201600546).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank Fort McMurray Public and Catholic School Boards for allowing us to analyze an anonymous dataset derived from their survey. We also thank all individuals involved in the survey data collection including Fort McMurray teachers, counsellors, and other staff members.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.676256/full#supplementary-material
CPSS, Child PTSD Symptom Scale; CRAFFT, CRAFFT Questionnaire (proper name of the questionnaire is CRAFFT); CYRM-12, Child and Youth Resilience Measure; EMPATHY, Empowering a Multimodal Pathway Towards Healthy Youth project; FDR, false discovery rate; HADS, Hospital Anxiety and Depression Scale; Kidscreen-10, Kidscreen Questionnaire; PHQ-A, The Patient Health Questionnaire, Adolescent version; PTSD, post-traumatic stress disorder; Rosenberg, Rosenberg Self-Esteem Scale.
1. CBC. Devastating Fort McMurray Wildfire Declared Out 15 Months Later. CBC (2017). Available online at: http://www.cbc.ca/news/canada/edmonton/fort-mcmurray-fire-beast-extinguished-out-1.4271604 (accessed February 16, 2021).
2. Cryderman K. Fort McMurray Wildfires to Cost Insurers $3.6-Billion - The Globe and Mail. (2016). Available online at: https://www.theglobeandmail.com/report-on-business/fort-mcmurray-wildfire-damage-to-cost-36-billion-insurance-bureau/article30788517/ (accessed February 16, 2021).
3. Cohan CL, Cole SW. Life course transitions and natural disaster: marriage, birth, and divorce following hurricane hugo. J Fam Psychol. (2002) 16:14–25. doi: 10.1037/0893-3200.16.1.14
4. Bonanno GA, Brewin CR, Kaniasty K, Greca AM. Weighing the costs of disaster: consequences, risks, and resilience in individuals, families, and communities. Psychol Sci Public Interest. (2010) 11:1–49. doi: 10.1177/1529100610387086
5. Speier AH. Psychosocial Issues for Children and Adolescents in Disasters. 2nd ed. Rockville, MD. (2000). Available online at: http://cretscmhd.psych.ucla.edu/nola/Video/MHR/Governmentreports/Psychosocial%20Issues%20for%20Children%20and%20Adolescents%20in%20Disasters.pdf (accessed February 16, 2021).
6. Peek L. Children and disasters: understanding vulnerability, developing capacities, and promoting resilience - an introduction. Child Youth Environ. (2008) 18:1–29.
7. Substance Abuse and Mental Health Services Administration (SAMHSA). Disaster Technical Assistance Center Supplemental Research Bulletin: Behavioral Health Conditions in Children and Youth Exposed to Natural Disasters. Rockville, MD (2018). Available online at: https://www.samhsa.gov/sites/default/files/srb-childrenyouth-8-22-18.pdf (accessed February 16, 2021).
8. Norris FH, Friedman MJ, Watson PJ, Byrne CM, Diaz E, Kaniasty K. 60,000 disaster victims speak: part I. An empirical review of the empirical literature, 1981-2001. Psychiatry. (2002) 65:207–39. doi: 10.1521/psyc.65.3.207.20173
9. Norris FH, Friedman MJ, Watson PJ. 60,000 disaster victims speak: part II. Summary and implications of the disaster mental health research. Psychiatry. (2002) 65:240–60. doi: 10.1521/psyc.65.3.240.20169
10. Peek L, Fothergill A. Post-Disaster decline: understanding children's vulnerability before, during, and after katrina. Dialogue Can Philos Assoc. (2014) 10:1–13. Available online at: https://www.samhsa.gov/sites/default/files/dialogue-vol10-issue3.pdf
11. World Health Organization. Adolescent Mental Health. WHO (2019). Available online at: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health (accessed February 16, 2021).
12. Brown MRG, Agyapong V, Greenshaw AJ, Cribben I, Brett-MacLean P, Drolet J, et al. After the Fort McMurray wildfire there are significant increases in mental health symptoms in grade 7–12 students compared to controls. BMC Psychiatry. (2019) 19:18. doi: 10.1186/s12888-019-2074-y
13. Brown MRG, Agyapong V, Greenshaw AJ, Cribben I, Brett-MacLean P, Drolet J, et al. Significant PTSD and other mental health effects present 18 months after the Fort McMurray wildfire: findings from 3,070 grades 7–12 students. Front Psychiatry. (2019) 10:623. doi: 10.3389/fpsyt.2019.00623
14. Rubens SL, Felix ED, Hambrick EP. A meta-analysis of the impact of natural disasters on internalizing and externalizing problems in youth. J Trauma Stress. (2018) 31:332–41. doi: 10.1002/jts.22292
15. Jones RT, Ribbe DP, Cunningham PB, Weddle JD, Langley AK. Psychological impact of fire disaster on children and their parents. Behav Modif. (2002) 26:163–86. doi: 10.1177/0145445502026002003
16. Psarros C, Theleritis C, Economou M, Tzavara C, Kioulos KT, Mantonakis L, et al. Insomnia and PTSD one month after wildfires: evidence for an independent role of the “fear of imminent death.” Int J Psychiatry Clin Pract. (2017) 21:137–41. doi: 10.1080/13651501.2016.1276192
17. Bryant RA, Gibbs L, Gallagher HC, Pattison P, Lusher D, MacDougall C, et al. Longitudinal study of changing psychological outcomes following the victorian black saturday bushfires. Aust New Zeal J Psychiatry. (2017) 52:542–51. doi: 10.1177/0004867417714337
18. McDermott BM, Lee EM, Judd M, Gibbon P. Posttraumatic stress disorder and general psychopathology in children and adolescents following a wildfire disaster. Can J Psychiatry. (2005) 50:137–43. doi: 10.1177/070674370505000302
19. Papadatou D, Giannopoulou I, Bitsakou P, Bellali T, Talias MA, Tselepi K. Adolescents' reactions after a wildfire disaster in Greece. J Trauma Stress. (2012) 25:57–63. doi: 10.1002/jts.21656
20. Kulig JC, Townshend I, Botey AP, Shepard B. ‘Hope is in our hands:' impacts of the slave lake wildfires in Alberta, Canada on children. In: Szente J, editor. Assisting Young Children Caught in Disasters. Educating the Young Child (Advances in Theory and Research, Implications for Practice), Vol. 13. Cham: Springer International Publishing (2018). p. 143–56. doi: 10.1007/978-3-319-62887-5_14
21. Kulig JC, Dabravolskaj J. The psychosocial impacts of wildland fires on children, adolescents and family functioning: a scoping review. Int J Wildl Fire. (2020) 29:93–103. doi: 10.1071/WF18063
22. Townshend I, Awosoga O, Kulig J, Pujadas BA, Shepard B, McFarlane B. Impacts of wildfires on school children: a case study of Slave Lake. Int J Mass Emerg Disasters. (2015) 33:148–187.
23. Agyapong VIO, Ritchie A, Brown MRG, Noble S, Mankowsi M, Denga E, et al. Long-term mental health effects of a devastating wildfire are amplified by socio-demographic and clinical antecedents in elementary and high school staff. Front Psychiatry. (2020) 11:448. doi: 10.3389/fpsyt.2020.00448
24. Ritchie A, Sautner B, Omege J, Denga E, Nwaka B, Akinjise I, et al. Long-term mental health effects of a devastating wildfire are amplified by sociodemographic and clinical antecedents in college students. Disaster Med Public Health Prep. (2020) 1–11. doi: 10.1017/dmp.2020.87
25. Kirsch KR, Feldt BA, Zane DF, Haywood T, Jones RW, Horney JA. Longitudinal community assessment for public health emergency response to wildfire, Bastrop County, Texas. Heal Secur. (2016) 14:93–104. doi: 10.1089/hs.2015.0060
26. Papanikolaou V, Adamis D, Mellon RC, Prodromitis G. Psychological distress following wildfires disaster in a rural part of Greece: a case-control population-based study. Int J Emerg Ment Health. (2011) 13:11–26.
27. Freedy JR, Saladin ME, Kilpatrick DG, Resnick HS, Saunders BE. Understanding acute psychological distress following natural disaster. J Trauma Stress. (1994) 7:257–73. doi: 10.1002/jts.2490070207
28. Afifi WA, Felix ED, Afifi TD. The impact of uncertainty and communal coping on mental health following natural disasters. Anxiety, Stress Coping. (2012) 25:329–47. doi: 10.1080/10615806.2011.603048
29. Freedy J, Resnick H, Kilpatrick D. Conceptual framework for evaluating disaster impact: implications for clinical intervention. In: Austin LS, editor. Responding to Disaster: A Guide for Mental Health Professionals Washington, DC: American Psychiatry Press (1992). p. 3–23.
30. Marshall GN, Schell TL, Elliott MN, Rayburn NR, Jaycox LH. Psychiatric disorders among adults seeking emergency disaster assistance after a wildland-urban interface fire. Psychiatr Serv. (2007) 58:509–14. doi: 10.1176/ps.2007.58.4.509
31. Paveglio TB, Kooistra C, Hall T, Pickering M. Understanding the effect of large wildfires on residents' well-being: what factors influence wildfire impact? For Sci. (2016) 62:59–69. doi: 10.5849/forsci.15-021
32. Caamano-Isorna F, Figueiras A, Sastre I, Montes-Martínez A, Taracido M, et al. Respiratory and mental health effects of wildfires: an ecological study in galician municipalities (north-west Spain). Environ Health. (2011) 10:48. doi: 10.1186/1476-069X-10-48
33. Langley AK. Coping Efforts and Efficacy, Acculturation, and Post-Traumatic Symptomatology in Adolescents Following Wildfire: A Latent Variable Path Analysis. (Unpublished Ph.D., dissertation) (2000). Available online at: https://vtechworks.lib.vt.edu/handle/10919/26473
34. Weems CF, Graham RA. Resilience and trajectories of posttraumatic stress among youth exposed to disaster. J Child Adolesc Psychopharmacol. (2014) 24:2–8. doi: 10.1089/cap.2013.0042
35. Goldmann E, Galea S. Mental health consequences of disasters. Annu Rev Public Health. (2014) 35:169–83. doi: 10.1146/annurev-publhealth-032013-182435
36. Kar N. Psychological impact of disasters on children: review of assessment and interventions. World J Pediatr. (2009) 5:5–11. doi: 10.1007/s12519-009-0001-x
37. Tang B, Liu X, Liu Y, Xue C, Zhang L. A meta-analysis of risk factors for depression in adults and children after natural disasters. BMC Public Health. (2014) 14:623. doi: 10.1186/1471-2458-14-623
38. Dai W, Chen L, Lai Z, Li Y, Wang J, Liu A. The incidence of post-traumatic stress disorder among survivors after earthquakes: a systematic review and meta-analysis. BMC Psychiatry. (2016) 16:188. doi: 10.1186/s12888-016-0891-9
39. Kõlves K, Kõlves KE, De Leo D. Natural disasters and suicidal behaviours: a systematic literature review. J Affect Disord. (2013) 146:1–14. doi: 10.1016/j.jad.2012.07.037
40. Masten AS, Osofsky JD. Disasters and their impact on child development: introduction to the special section. Child Dev. (2010) 81:1029–39. doi: 10.1111/j.1467-8624.2010.01452.x
41. Forresi B, Soncini F, Bottosso E, Di Pietro E, Scarpini G, Scaini S, et al. Post-traumatic stress disorder, emotional and behavioral difficulties in children and adolescents 2 years after the 2012 earthquake in Italy: an epidemiological cross-sectional study. Eur Child Adolesc Psychiatry. (2020) 29:227–38. doi: 10.1007/s00787-019-01370-0
42. McFarlane AC, Van Hooff M. Impact of childhood exposure to a natural disaster on adult mental health: 20-Year longitudinal follow-up study. Br J Psychiatry. (2009) 195:142–8. doi: 10.1192/bjp.bp.108.054270
43. Fergusson DM, Horwood LJ, Boden JM, Mulder RT. Impact of a major disaster on the mental health of a well-studied cohort. JAMA Psychiatry. (2014) 71:1025–31. doi: 10.1001/jamapsychiatry.2014.652
44. Gao X, Leng Y, Guo Y, Yang J, Cui Q, Geng B, et al. Association between earthquake experience and depression 37 years after the tangshan earthquake: a cross-sectional study. BMJ Open. (2019) 9:e026110. doi: 10.1136/bmjopen-2018-026110
45. Isaranuwatchai W, Coyte PC, McKenzie K, Noh S. The 2004 tsunami and mental health in Thailand: a longitudinal analysis of one-and two-year post-disaster data. Disasters. (2017) 41:150–70. doi: 10.1111/disa.12188
46. Bryant RA, Waters E, Gibbs L, Gallagher HC, Pattison P, Lusher D, et al. Psychological outcomes following the victorian black saturday bushfires. Aust N Z J Psychiatry. (2014) 48:634–43. doi: 10.1177/0004867414534476
47. Schwartz RM, Gillezeau CN, Liu B, Lieberman-Cribbin W, Taioli E. Longitudinal impact of hurricane sandy exposure on mental health symptoms. Int J Environ Res Public Health. (2017) 14:957. doi: 10.3390/ijerph14090957
48. Raker EJ, Lowe SR, Arcaya MC, Johnson ST, Rhodes J, Waters MC. Twelve years later: the long-term mental health consequences of hurricane katrina. Soc Sci Med. (2019) 242:112610. doi: 10.1016/j.socscimed.2019.112610
49. Self-Brown S, Lai BS, Thompson JE, McGill T, Kelley M Lou. Posttraumatic stress disorder symptom trajectories in hurricane katrina affected youth. J Affect Disord. (2013) 147:198–204. doi: 10.1016/j.jad.2012.11.002
50. Kronenberg ME, Hansel TC, Brennan AM, Osofsky HJ, Osofsky JD, Lawrason B. Children of katrina: lessons learned about postdisaster symptoms and recovery patterns. Child Dev. (2010) 81:1241–59. doi: 10.1111/j.1467-8624.2010.01465.x
51. Kleber RJ. Trauma and public mental health: a focused review. Front Psychiatry. (2019) 10:451. doi: 10.3389/fpsyt.2019.00451
52. Dückers MLA. Five essential principles of post-disaster psychosocial care: looking back and forward with Stevan Hobfoll. Eur J Psychotraumatol. (2013) 4:21914. doi: 10.3402/ejpt.v4i0.21914
53. Foa EB, Johnson KM, Feeny NC, Treadwell KR. The child PTSD symptom scale: a preliminary examination of its psychometric properties. J Clin Child Psychol. (2001) 30:376–84. doi: 10.1207/S15374424JCCP3003_9
54. Johnson JG, Harris ES, Spitzer RL, Williams JBW. The patient health questionnaire for adolescents: validation of an instrument for the assessment of mental disorders among adolescent primary care patients. J Adolesc Health. (2002) 30:196–204. doi: 10.1016/S1054-139X(01)00333-0
55. Spitzer RL, Kroenke K, Williams JBW, Group the PHQPCS. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. JAMA. (1999) 282:1737. doi: 10.1001/jama.282.18.1737
56. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
57. Knight JR, Shrier LA, Bravender TD, Farrell M, Vander Bilt J, Shaffer HJ. A new brief screen for adolescent substance abuse. Arch Pediatr Adolesc Med. (1999) 153:591–6. doi: 10.1001/archpedi.153.6.591
58. Knight JR, Sherritt L, Harris SK, Gates EC, Chang G. Validity of brief alcohol screening tests among adolescents: a comparison of the AUDIT, POSIT, CAGE, and CRAFFT. Alcohol Clin Exp Res. (2003) 27:67–73. doi: 10.1111/j.1530-0277.2003.tb02723.x
59. Rosenberg M. Society and the Adolescent Self-Image. Princeton, NJ: Princeton University Press (1965).
60. Ravens-Sieberer U, Erhart M, Rajmil L, Herdman M, Auquier P, Bruil J, et al. Reliability, construct and criterion validity of the KIDSCREEN-10 score: a short measure for children and adolescents' well-being and health-related quality of life. Qual Life Res. (2010) 19:1487–500. doi: 10.1007/s11136-010-9706-5
61. Liebenberg L, Ungar M, LeBlanc JC. The CYRM-12: a brief measure of resilience. Can J Public Health. (2013) 104:e131–5. doi: 10.1007/BF03405676
62. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
63. Richardson LP, McCauley E, Grossman DC, McCarty CA, Richards J, Russo JE, et al. Evaluation of the patient health questionnaire-9 item for detecting major depression among adolescents. Pediatrics. (2010) 126:1117–23. doi: 10.1542/peds.2010-0852
64. Snaith RP. The hospital anxiety and depression scale. Health Qual Life Outcomes. (2003) 1:29. doi: 10.1186/1477-7525-1-29
65. Stewart RW, Ebesutani C, Drescher CF, Young J. The child PTSD symptom scale: an investigation of its psychometric properties. J Interpers Violence. (2015) 32:2237–56. doi: 10.1177/0886260515596536
66. Mrklas K, Shalaby R, Hrabok M, Gusnowski A, Vuong W, Surood S, et al. Prevalence of perceived stress, anxiety, depression, and obsessive-compulsive symptoms in health care workers and other workers in alberta during the COVID-19 pandemic: cross-sectional survey. JMIR Ment Health. (2020) 7:e22408. doi: 10.2196/22408
67. ISSTS. Child PTSD Symptom Scale. Available online at: https://istss.org/clinical-resources/assessing-trauma/child-ptsd-symptom-scale-for-dsm-5-(cpss-5) (accessed February 16, 2021).
68. Weems CF, Osofsky JD, Osofsky HJ, King LS, Hansel TC, Russell JD. Three-year longitudinal study of perceptions of competence and well-being among youth exposed to disasters. Appl Dev Sci. (2018) 22:29–42. doi: 10.1080/10888691.2016.1219229
69. Ford T, Goodman R, Meltzer H. The british child and adolescent mental health survey 1999: the prevalence of DSM-IV disorders. J Am Acad Child Adolesc Psychiatry. (2003) 42:1203–11. doi: 10.1097/00004583-200310000-00011
70. Bryant RA, Gallagher HC, Gibbs L, Pattison P, MacDougall C, Harms L, et al. Mental health and social networks after disaster. Am J Psychiatry. (2017) 174:277–85. doi: 10.1176/appi.ajp.2016.15111403
71. Felix E, Afifi T, Kia-Keating M, Brown L, Afifi W, Reyes G. Family functioning and posttraumatic growth among parents and youth following wildfire disasters. Am J Orthopsychiatry. (2015) 85:191–200. doi: 10.1037/ort0000054
72. Davydov DM, Stewart R, Ritchie K, Chaudieu I. Resilience and mental health. Clin Psychol Rev. (2010) 30:479–95. doi: 10.1016/j.cpr.2010.03.003
73. Herrman H, Stewart DE, Diaz-Granados N, Berger EL, Jackson B, Yuen T. What is resilience? Can J Psychiatry. (2011) 56:258–65. doi: 10.1177/070674371105600504
74. Zolkoski SM, Bullock LM. Resilience in children and youth: a review. Child Youth Serv Rev. (2012) 34:2295–303. doi: 10.1016/j.childyouth.2012.08.009
75. Lowe SR, Bonumwezi JL, Valdespino-Hayden Z, Galea S. Posttraumatic stress and depression in the aftermath of environmental disasters: a review of quantitative studies published in 2018. Curr Environ Heal reports. (2019) 6:344–60. doi: 10.1007/s40572-019-00245-5
76. Surace T, Fusar-Poli L, Vozza L, Cavone V, Arcidiacono C, Mammano R, et al. Lifetime prevalence of suicidal ideation and suicidal behaviors in gender non-conforming youths: a meta-analysis. Eur Child Adolesc Psychiatry. (2020) 1:3. doi: 10.1007/s00787-020-01508-5
77. Valentine SE, Shipherd JC. A systematic review of social stress and mental health among transgender and gender non-conforming people in the United States. Clin Psychol Rev. (2018) 66:24–38. doi: 10.1016/j.cpr.2018.03.003
78. Reisner SL, Katz-Wise SL, Gordon AR, Corliss HL, Austin SB. Social epidemiology of depression and anxiety by gender identity. J Adolesc Health. (2016) 59:203–8. doi: 10.1016/j.jadohealth.2016.04.006
79. Streed CG, McCarthy EP, Haas JS. Association between gender minority status and self-reported physical and mental health in the United States. JAMA Intern Med. (2017) 177:1210–2. doi: 10.1001/jamainternmed.2017.1460
80. Regional Municipality of Wood Buffalo. RMWB 2016 Wildfire Recovery Plan. (2018) Available online at: https://fusesocial.ca/wp-content/uploads/2018/05/RMWB-recovery-plan2106.pdf (accessed February 19, 2021).
81. Cheung S, Marriott B. Impact of an Economic Downturn on Addiction and Mental Health Service Utilization: A Review of the Literature. (2015). Available online at: https://www.albertahealthservices.ca/assets/info/res/mhr/if-res-mhr-kn-12-economic-downturn.pdf (accessed February 22, 2021).
Keywords: youth, population mental health, wildfire natural disaster, post-traumatic stress disorder (PTSD), depression, anxiety, alcohol and substance use, resilience
Citation: Brown MRG, Pazderka H, Agyapong VIO, Greenshaw AJ, Cribben I, Brett-MacLean P, Drolet J, McDonald-Harker CB, Omeje J, Lee B, Mankowsi M, Noble S, Kitching DT and Silverstone PH (2021) Mental Health Symptoms Unexpectedly Increased in Students Aged 11–19 Years During the 3.5 Years After the 2016 Fort McMurray Wildfire: Findings From 9,376 Survey Responses. Front. Psychiatry 12:676256. doi: 10.3389/fpsyt.2021.676256
Received: 04 March 2021; Accepted: 15 April 2021;
Published: 20 May 2021.
Edited by:
Lawrence T. Lam, University of Technology Sydney, AustraliaReviewed by:
Je-Yeon Yun, Seoul National University Hospital, South KoreaCopyright © 2021 Brown, Pazderka, Agyapong, Greenshaw, Cribben, Brett-MacLean, Drolet, McDonald-Harker, Omeje, Lee, Mankowsi, Noble, Kitching and Silverstone. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peter H. Silverstone, cGV0ZXIuc2lsdmVyc3RvbmVAdWFsYmVydGEuY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.