
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 10 May 2021
Sec. Mood Disorders
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.664228
This article is part of the Research TopicObsessive-Compulsive Disorder (OCD) Across the Lifespan: Current Diagnostic Challenges and the Search for Personalized Treatment View all 26 articles
 Humberto Nicolini1*
Humberto Nicolini1* José Jaime Martínez-Magaña1
José Jaime Martínez-Magaña1 Alma Delia Genis-Mendoza1,2
Alma Delia Genis-Mendoza1,2 Jorge Ameth Villatoro Velázquez3,4
Jorge Ameth Villatoro Velázquez3,4 Beatriz Camarena5
Beatriz Camarena5 Clara Fleiz Bautista3,4Marycarmen Bustos-Gamiño3
Clara Fleiz Bautista3,4Marycarmen Bustos-Gamiño3 Alejandro Aguilar García5Nuria Lanzagorta6
Alejandro Aguilar García5Nuria Lanzagorta6 María Elena Medina-Mora3,4*
María Elena Medina-Mora3,4*Recent studies suggest that the endocannabinoid system could play an important role in the physiopathology of obsessive-compulsive disorder (OCD). There are reports of effective treatment with derivatives of tetrahydrocannabinol (THC). The study of the genetic factor associated with psychiatric disorders has made possible an exploration of its contribution to the pharmacological response. However, very little is known about the genetic factor or the prevalence of cannabis use in the Mexican population with OCD. The objective of this study is to compare the prevalence of use and dependence on cannabis in individuals with obsessive-compulsive symptomatology (OCS) with that of individuals with other psychiatric symptoms (psychosis, depression, and anxiety), and to explore the association between genetic risk and use. The study includes a total of 13,130 individuals evaluated in the second stage of the 2016 National Survey of Drug, Alcohol, and Tobacco Use (Encodat 2016), with genetic analysis (polygenic risk scoring) of a subsample of 3,521 individuals. Obsessive symptomatology had a prevalence of 7.2% and compulsive symptomatology a prevalence of 8.6%. The proportion of individuals with OCS who had ever used cannabis was 23.4%, and of those with cannabis dependency was 2.7%, the latter figure higher than that in individuals with other psychiatric symptoms (hypomania, 2.6%; anxiety, 2.8%; depression, 2.3%), except psychosis (5.9%). Individuals with OCS who reported using cannabis had an increased genetic risk for cannabis dependence but not for OCD. We thus cannot know how the increased genetic risk of cannabis dependence in people with OCD is influenced by their pharmacological response to derivatives of THC. The results, however, suggest paths for future studies.
Obsessive-compulsive disorder (OCD) is a chronic disorder that affects 1–3% of the population worldwide (1–3). Its diagnosis is based on the presence of obsessions, compulsions, or both (4). The obsessions usually take the form of recurrent thoughts, impulses, or images that can cause anxiety, while the compulsions are repetitive behaviors or mental acts that respond to the obsession (5). People diagnosed with OCD have a high rate of comorbidity with other disorders: an estimated 75.0% present an additional during their lifetime (6). OCD is a symptomatological spectrum, which has made it difficult to clarify its etiology, but there are some known risk factors, including a genetic factor and alterations in neurotransmitters and brain function (7). Genes have recently been discovered that may play an important role in the alteration of glutamatergic signaling (8), and OCD is one of the mental disorders most accompanied by alterations in brain function, mainly in the cortical-striatal-thalamic circuit (9–11). Alterations have also been reported in the levels of neurotransmitters such as serotonin, dopamine, and glutamate (7).
Another neurotransmission system associated with OCD, which has gained importance as a target for the development of possible pharmacological treatments, has been the endocannabinoid system (12–15). Some studies have shown that treatment with derivatives of tetrahydrocannabinol (THC), a partial agonist of the cannabinoid B1 receptor, could diminish anxiety-related symptoms in individuals with post-traumatic stress (13, 14, 16). Currently, the main pharmacological treatment for OCD is serotonin reuptake inhibitors, and the search for new treatments and growing approval of THC derivatives has produced favorable results in case studies (17). However, we cannot disregard the relationship between cannabis use and the development of dependence (18–20), which is inheritable, complex, and associated with mental health disorders (21, 22). A recent study explored genetic factors associated with lifetime use of cannabis and found ~35 genes in a sample of more than 180,000 individuals (23). Cannabis use with dependence has increased in Mexico from 2.4% in 2008 to 5.2% in 2016 (24), and Mexico is known for cannabis production (25).
Neither the prevalence of OCD, its relationship with the use of and dependence on cannabis, nor the genetic risk factors have been estimated on a populational level in Mexico. The objective of this study is thus to compare the prevalence of use and dependence on cannabis in individuals with obsessive-compulsive symptomatology (OCS) with that in individuals with other psychiatric symptoms (psychosis, depression, and anxiety) in a populational sample, and to explore the genetic risks associated with its use.
The study included a total of 13,130 Mexican respondents from the second stage of the National Survey on Drug, Alcohol, and Tobacco Use (Encuesta Nacional de Consumo de Drogas, Alcohol y Tabaco 2016; Encodat 2016). The Encodat 2016 is a household survey aimed at assessing the patterns of use of different psychoactive drugs and certain mental health problems in the Mexican population. The survey was cross-sectional, with a multi-stage, probabilistic, and stratified design, and a confidence level of 90%. The sampling universe for the primary sampling units (PSUs) was the sum of the Basic Geographical Statistical Areas (BGSAs), stratified according to state and urban-rural character. Participants were 12–65 years of age, from urban and rural communities, and living at home. Wherever possible, following the household questionnaire, one adult aged 18–65 and one teenager aged 12–17 were presented with the individual questionnaire, according to a simple random sampling in each age group. The Encodat 2016 was nationally representative, with a total response rate (household + individual) of 73.6% and a final sample of 56,877 complete interviews: 27,463 men and 29,414 women; 9,563 teenagers and 47,314 adults.
The sample was obtained in two representative blocks: two independent national samples. However, it was in the second national sample that the symptomatology screening section was included with the psychiatric standard questionnaire on alcohol, tobacco, and drugs. The latter was performed for those who agreed to provide a DNA sample, with the screening questionnaire of the Diagnostic Interview for Psychosis and Affective Disorders (DI-PAD screener, version 1.5) (26–28), which is based on the Diagnostic Interview for Genetic Studies and is linked to the Operational Criteria for Psychotic Illness (OPCRIT, version 4.0). The DI-PAD screener was applied by an interviewer with specialized training in its use. Of the total of 28,770 participants in this second sample, 13,130 agreed to provide a DNA sample (Table 1) and answer the screener questions. This sample was weighted to obtain data that were representative on the national level.
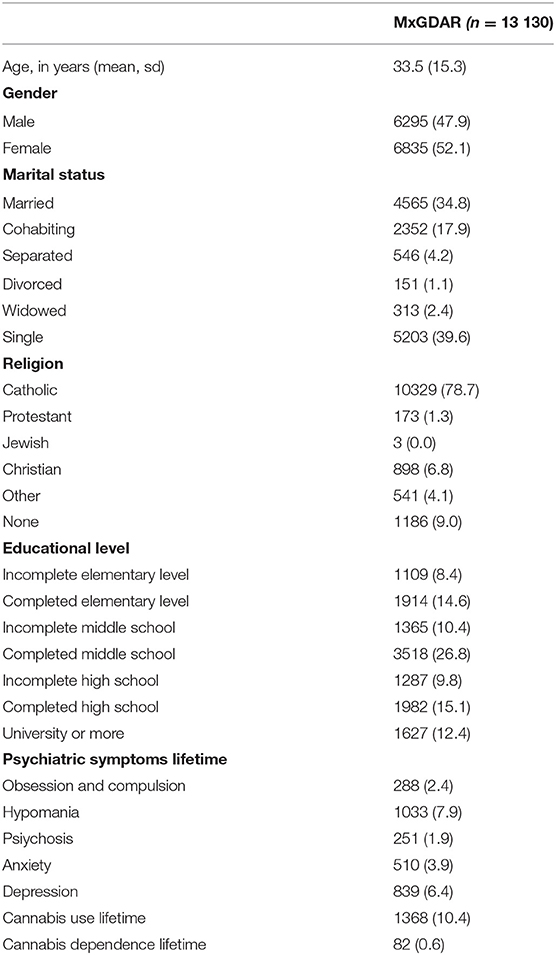
Table 1. Sociodemographic and clinical characteristics of the total sample.
Participants were evaluated for lifetime psychiatric symptomatology using the following questions regarding obsessive symptomatology (OS) and compulsive symptomatology (CS):
OS symptomatology: “Have you ever had repetitive thoughts or images, much more exaggerated than normal worries, that you couldn't get out of your head, that were intrusive and uncomfortable, and that lasted an hour or more a day?”
CS symptomatology: “Have you ever had to repeat certain behaviors over and over for an hour or more a day? (Examples: washing your hands or checking the locks over and over again, or repeating words or counting things in your head.)”
Obsessive-Compulsive symptomatology (SOC): affirmative response to both of the above.
Definitions for other psychiatric symptomatologies (psychosis, hypomania, anxiety, and depression) were as following:
1. Hypomania.
To define a case must meet the following criteria:
- Have you ever been diagnosed with bipolar disorder (or manic depressive disorder)?
If you do not meet the above criteria, must meet the following two criteria:
- Have you ever had a period of time that lasted 3 days or more in which you felt unusually cheerful, irritable, energetic, or hyperactive, so much so that you felt or acted in a way that was clearly different from your normal character?
- Have you ever had a period of time that lasted 3 days or more in which you didn't need much sleep (or no sleep at all) without feeling tired, or even had more energy than normal?
2. Psychosis.
To define a case must meet the following criteria:
- Have you ever been diagnosed with schizophrenia?
- If you do not meet the above criteria, must meet the following two criteria:
- Have you ever had a period of time when you heard voices when no one was actually present, had visions, or saw things that other people couldn't see?
- Have you ever had beliefs or ideas that other people did not share with you or that you later discovered were not true?
3. Anxiety.
To define a case must meet the following three criteria:
- Have you ever had an experience where you suddenly felt very anxious or fearful?
- When you had this experience, did you feel rapid heartbeat, chest pain, feeling short of breath or strangulation, nausea, sweating, weakness, thinking you would go crazy or die?
- Did these problems get worse or stronger in the first 10 min?
4. Depression.
To define a case must meet the following criteria:
- Have you ever felt depressed, sad, down, or discouraged most of the day, almost every day, for 2 weeks or more?
In addition, must meet at least one of the following criteria:
- Have you had a period of 2 weeks or more in which you lost most or all interest in your normal activities?
- During this period, did you also have feelings of worthlessness or guilt, or did you spend a lot of time with thoughts of death, suicide, or self-harm?
- During this period, did you notice a significant change in your appetite, unexpected weight gain or loss, experienced changes in your normal sleep pattern, or had difficulty concentrating?
The use of or dependence on cannabis was evaluated in this study under the criteria of the Composite International Diagnostic Interview (CIDI). Dependence was considered to be three or more of the following symptoms: tolerance, abstinence, a longer time or a greater amount of use, persistent or uncontrollable cravings, excessive time spent in getting drugs or recuperating from their effects, reduction in social, work, or recreational activities, or continued use in spite of awareness of harmful effects.
All participants provided written informed consent or assent. The protocols were carried out based on international norms and the Helsinki Declaration; they were reviewed and approved by the research and ethics committees of the Instituto Nacional de Psiquiatría (Approval No. CEI/C/083/2015) and the Instituto Nacional de Medicina Genómica (Approval No. 01/2017/I).
DNA was collected from cheek swabs, using a modified salting-out method with the Puregen commercial kit (Qiagen, USA). The quality and integrity of the DNA was evaluated with a NanoDrop spectrophotometer (Thermofisher, USA) and a 2% agarose gel. The procedure produced 7,170 samples of sufficient quality for microarray analysis. The genotyping was carried out with an Infinium Psycharray commercial microarray (Illumina, USA). The fluorescence intensities were read with iScan (Illumina, USA). The genotyping procedure was carried out in the high-technology microarray unit of the National Institute of Genomic Medicine. Genotyping was performed on a subsample of 3,600 individuals. A random sampling of the 7,170 samples was performed to select 60% with psychiatric symptomatology and 40% as controls.
The fluorescence intensities were transformed to genotypes using the software GenomeStudio (Illumina, USA), and quality control was performed with the Plink program (29). Single nucleotide variants (SNVs) with a call rate >95% were removed, as were those with a minor allele frequency (MAF) >1%, a p-value > 1e-6 for a chi-square Hardy-Weinberg equilibrium test, and A/T or G/C variants (to avoid the flip strand effect). Individuals with a genotyping of <95% were removed. To correct cryptic relationships, all pairs of individuals with an identity-by-state value >1.6 were marked, and the individual with the lowest rate of genotyping was removed (30).
To evaluate the genetic risk for obsessive-compulsive disorder and lifetime use of cannabis, polygenic risk scores (PRS) were calculated, using summary statistics for cannabis dependence (23) and the scores reported by the Psychiatric Genomic Consortium for obsessive-compulsive disorder (8). Polymorphisms were selected with p-values < 0.05, as reported in the summary statistics, which had good genotyping quality control. The PRS were correlated with the principal components of ancestry. Genetic ancestry was estimated using principal component analysis with the PC-AiR package (31) and the reference base of the Human Genome Diversity Project (32). The standardized residuals for comparison between groups were obtained based on the correlations of the PRS with ten principal components of genetic ancestry. The comparisons of the PRS were performed using ANOVA or Student's t-test.
The prevalence of obsessive symptomatology (OS) was 7.1% (n = 866), of compulsive symptomatology (CS) was 8.2% (n = 1,004), and of obsessive-compulsive symptomatology (OCS) was 2.4% (n = 288). Differences were found in the presence of OCS between men (42.3%) and women (57.7%), but these were not statistically significant compared with gender differences in those without OCS (?2 = 1.4, p = 0.8620). The average age of those with OCS was less (m = 30.1, SD = 15.4) than those without such symptomatology (m = 33.4, SD = 15.7) (T = −3.9, p < 0.0001).
The prevalence of having ever used cannabis was 24.4% (n = 70) in individuals with OCS (n = 288), greater than that reported for the population as a whole (9.7%) and greater than that for those with other psychiatric symptoms (hypomania, 20.9%; anxiety, 19.5%; and depression, 15.1%) except psychosis (25.5%) (Figure 1). The prevalence of having ever used cannabis was similar in those with only OS (15.8%, n = 149) as in those with only CS (15.2%, n = 172).
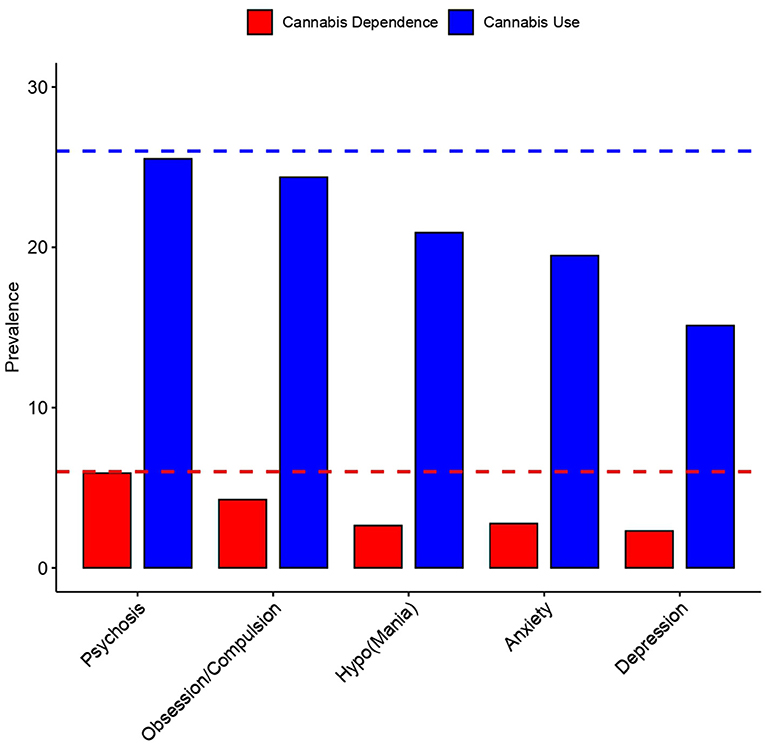
Figure 1. Prevalence of Cannabis use and dependence in the population. Cannabis dependence is shown in red, and cannabis use in blue. The prevalence was divided in the psychiatric symptomatology.
The prevalence of having ever been dependent on cannabis in individuals with OCS was greater (4.3%, n = 12) than that found in the population as a whole (0.6%). Greater dependence was also observed in this group than in individuals with other psychiatric symptomatologies (hypomania, 2.6%; anxiety, 2.8%; depression, 2.3%) except psychosis (5.9%). However, dependence was greater in individuals with only CS (2.2%, n = 22) than in those with only OS (1.8%, n = 15).
The subsample used for genotyping had the following distribution: 81.8% (n = 2,658 individuals) with no cannabis use or OCS, 14.9% (n = 485 individuals) having ever used cannabis but with no OCS, 2.1% (n = 68 individuals) with OCS but no cannabis use, and 1.2% (n = 38 individuals) with OCS and having ever used cannabis. The PRS for OCD was constructed using 11,959 SNPs, which passed the quality control test. The OCD-PRS comparison found no statistically significant differences between the different groups (F = 1.5, p = 0.2020) (Figure 2).
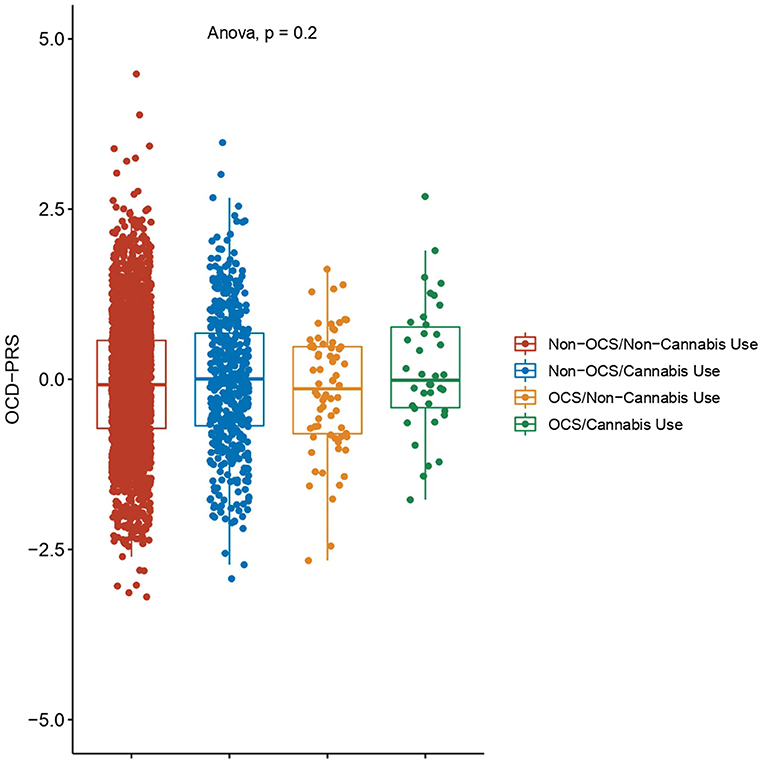
Figure 2. Polygenic risk score for obsessive-compulsive disorder (OCD-PRS). The OCD-PRS was calculated with data reported by the Psychiatric Genomics Consortium and standardized by ancestry. Differences between the four groups were evaluated by ANOVA. Non-OCS: individuals without OCS symptoms; Non-Cannabis Use: individuals who had never used cannabis; OCS: individuals with OCS symptoms; and Cannabis Use; individuals who had ever used cannabis.
The PRS for dependence on cannabis was constructed using 13,485 SNPs, which passed the quality control test. The CannabisDep-PRS comparison found statistically significant differences between the different groups (F = 3.3, p = 0.0192) (Figure 3). The post-hoc comparisons found that the CannabisDep-PRS between individuals with OCS with cannabis use were not significantly different from those of individuals with OCS but with no cannabis use (p = 0.2010). Individuals with OCS and cannabis use had the highest CannabisDep-PRS value (m = 0.3151), and the difference from the value for those without OCS or cannabis use was statistically significant (p = 0.0390).
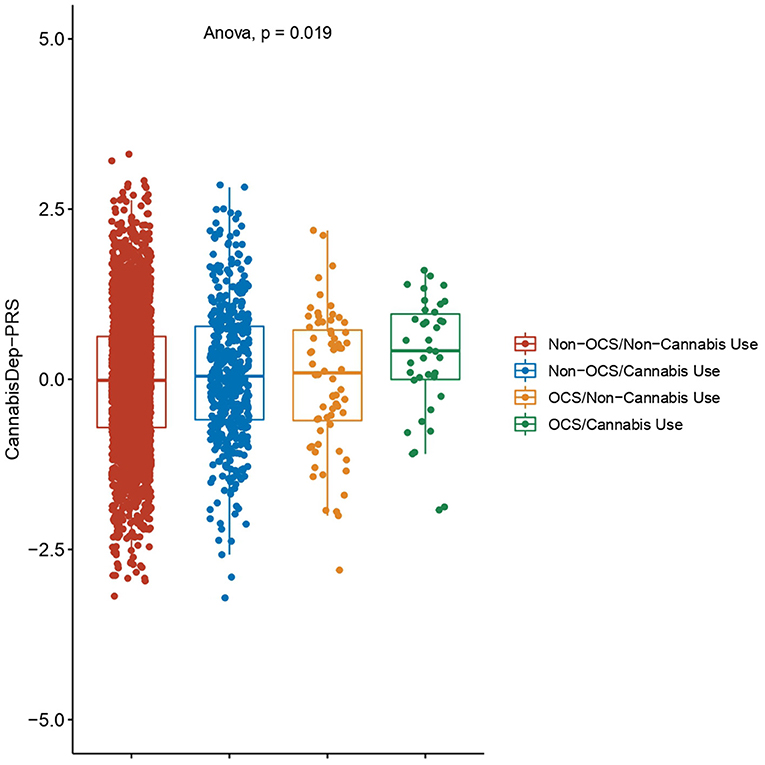
Figure 3. Polygenic risk score for cannabis dependence (CannabisDep-PRS). The CannabisDep-PRS was calculated with data reported from the Psychiatric Genomics Consortium and standardized by ancestry. Differences between the four groups were evaluated by ANOVA. Non-OCS: individuals without OCS symptoms; Non-Cannabis Use: individuals who had never used cannabis; OCS: individuals with OCS symptoms; and Cannabis Use: individuals who had ever used cannabis.
Cannabis dependence and use has increased in recent years, as have proposals for the use of THC derivatives as pharmacological agents in areas such as psychiatry and oncology (33–36). In psychiatry, these derivatives could improve the symptomatology of some disorders, mainly those related to stress, such as Tourette's syndrome, anxiety, and post-traumatic stress disorder (16, 22, 37–40). Even a non-psychoactive derivative (cannabidiol) has been used to treat substance use disorders (41, 42). There are case studies that suggest a possible improvement in OCD after treatment with THC derivatives (17). A pilot clinical trial found that use of THC derivatives with exposure therapy has a synergic effect on the treatment of obsession and compulsion on individuals diagnosed with OCD (43), and its use as a therapeutic agent should still be explored. But we cannot disregard the effect of the continuous use of cannabis on the development of cannabis use disorder where its use is already problematic. We found that the prevalence of cannabis dependence in individuals with obsessive-compulsive symptomatology (OCS) was second (at 4.3%) only to its prevalence in those with psychosis (5.9%) (44). This prevalence in those with OCS is interesting, given that psychosis, but not OCD, has been strongly associated with use of or dependence on cannabis (45). Such an association has been found for other psychiatric disorders, including depression, anxiety, and suicide attempts, and for psychosis manifested at earlier ages (45–48). We do not, however, know of its effect on OCS or on the development of psychosis.
One of the important aspects to consider in the relationship between cannabis and OCD is the development of cannabis dependence either through recreational use or in pharmacological applications. This development has been thought of as a complex phenotype that must include different risk factors, such as the genetic one, in its development (49–51). The genome scans have found hundreds or thousands of associated genetic variations that have been used to calculate polygenic risk scores (PRS) (52–55). We have found that the PRS for cannabis dependence was greater in those with OCD who used cannabis than in those who did not use it. Individuals with a high genetic risk who use cannabis might thus increase their risk of dependence either through recreational use or with pharmacological derivatives of THC. PRS have been used not only as predictors of risk, but also as markers of pharmacological response to psychoactive agents and in pharmacogenomic studies (56–59). It might be hypothesized that the use of the PRS for cannabis dependence could be useful in predicting which individuals are at high risk, and to determine whether pharmacological treatment based on THC derivatives would be useful, or would exacerbate obsessive-compulsive symptomatology.
Although we found associations between obsessive-compulsive symptomatology and the use of or dependence on cannabis, a limitation of this study is its lack of direct psychiatric diagnostic evaluation of the individuals surveyed. A further limitation was our inability to conduct a longitudinal evaluation of OCD symptoms, before or after cannabis use, to evaluate the symptomatological changes brought about by that use. Finally, because of the sample size, our analysis of genetic risk was able to evaluate only the use of cannabis, and not dependence.
The use of and dependence on cannabis was found to be greater in the Mexican population among individuals with obsessive-compulsive symptomatology than in those with anxiety or depression, but less than in those with psychosis. The genetic risk for cannabis dependence was also associated with cannabis use in individuals with obsessive-compulsive symptomatology. It may be possible in future pharmacogenomic studies to determine the response rates of individuals with different genetic risk scores.
The genomic datasets generated for this study can be found in the European Variation Archive (EVA, PRJEB37766).
The studies involving human participants were reviewed and approved by the research and ethics committees of the Instituto Nacional de Psiquiatría Ramón de la Fuente Muñiz and the Instituto Nacional de Medicina Genómica. Written informed consent was provided by the participants or their parents or legal guardians.
HN, NL, JM-M, AG-M, and JV developed the analyses and wrote the first version of the manuscript. JM-M, JV, and MB-G performed bioinformatics and statistical analyses. JV, CF, MB-G, and MM-M contributed to data collection. BC, AA, JM-M, and AG-M contributed to the genetic experiments. HN, MM-M, and JV conceived, designed, and coordinated the genetic analysis. All authors contributed to the article and approved the submitted version.
This study received funding from the Instituto Nacional de Medicina Genómica (Grant No. 23/2015/I), and from the Comisión Nacional de Ciencia y Tecnología (CONACyT) 2016 Fund for the Development of Scientific Projects to Address National Problems (Grant No. PN22296). The development of the surveys was funded by the Comisión Nacional Contra las Adicciones (CONADIC).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We wish to thank the work committee and the field coordination team of the Encodat 2016, the microarray unit of the Instituto Nacional de Medicina Genómica, and Rául Mojica Espinoza and the expression and microarray unit of INMEGEN, for technical assistance with microarray processing.
1. Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the national comorbidity survey replication. Mol Psychiatry. (2010) 15:53–63. doi: 10.1038/mp.2008.94
2. Subramaniam M, Abdin E, Vaingankar JA, Chong SA. Obsessive-compulsive disorder: prevalence, correlates, help-seeking and quality of life in a multiracial asian population. Soc Psychiatry Psychiatr Epidemiol. (2012) 47:2035–2043. doi: 10.1007/s00127-012-0507-8
3. Fontenelle LF, Mendlowicz MV, Versiani M. The descriptive epidemiology of obsessive-compulsive disorder. Prog Neuro-Psychopharmacology Biol Psychiatry. (2006) 30:327–37. doi: 10.1016/j.pnpbp.2005.11.001
4. Leckman JF, Denys D, Simpson HB, Mataix-Cols D, Hollander E, Saxena S, et al. Obsessive-compulsive disorder: a review of the diagnostic criteria possible subtypes dimensional specifiers for DSM-V. Depress Anxiety. (2010) 27:507–27. doi: 10.1002/da.20669
5. Nicolini H. Serotonin transporter gene polymorphisms & obsessive-compulsive disorder. Indian J Med Res. (2010) 132:663–665. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3102452/ (accessed December 17, 2020).
6. Pallanti S, Grassi G, Cantisani A, Sarrecchia E, Pellegrini M. Obsessive–compulsive disorder comorbidity: clinical assessment and therapeutic implications. Front Psychiatry. (2011) 2:70. doi: 10.3389/fpsyt.2011.00070
7. Stein DJ, Costa DLC, Lochner C, Miguel EC, Reddy YCJ, Shavitt RG, et al. Obsessive–compulsive disorder. Nat Rev Dis Prim. (2019) 5:52. doi: 10.1038/s41572-019-0102-3
8. Smit DJA, Cath D, Zilhão NR, Ip HF, Denys D, den Braber A, et al. Genetic meta-analysis of obsessive–compulsive disorder and self-report compulsive symptoms. Am J Med Genet Part B Neuropsychiatr Genet. (2020) 183:208–16. doi: 10.1002/ajmg.b.32777
9. Hazari N, Narayanaswamy J, Venkatasubramanian G. Neuroimaging findings in obsessive-compulsive disorder: a narrative review to elucidate neurobiological underpinnings. Indian J Psychiatry. (2019) 61:S9–29. doi: 10.4103/psychiatry.IndianJPsychiatry_525_18
10. Saxena S, Bota RG, Brody AL. Brain-behavior relationships in obsessive-compulsive disorder. Semin Clin Neuropsychiatry. (2001) 6:82–101. doi: 10.1053/scnp.2001.21833
11. Whiteside SP, Port JD, Abramowitz JS. A meta-analysis of functional neuroimaging in obsessive-compulsive disorder. Psychiatry Res Neuroimaging. (2004) 132:69–79. doi: 10.1016/j.pscychresns.2004.07.001
12. Kayser RR, Snorrason I, Haney M, Lee FS, Simpson HB. The endocannabinoid system: a New treatment target for obsessive compulsive disorder? Cannabis Cannabinoid Res. (2019) 4:77–87. doi: 10.1089/can.2018.0049
13. Rabinak CA, Angstadt M, Sripada CS, Abelson JL, Liberzon I, Milad MR, et al. Cannabinoid facilitation of fear extinction memory recall in humans. Neuropharmacology. (2013) 64:396–402. doi: 10.1016/j.neuropharm.2012.06.063
14. Rabinak CA, Angstadt M, Lyons M, Mori S, Milad MR, Liberzon I, et al. Cannabinoid modulation of prefrontal-limbic activation during fear extinction learning and recall in humans. Neurobiol Learn Mem. (2014) 113:125–34. doi: 10.1016/j.nlm.2013.09.009
15. Bowers ME, Ressler KJ. An overview of translationally informed treatments for posttraumatic stress disorder: animal models of pavlovian fear conditioning to human clinical trials. Biol Psychiatry. (2015) 78:e15–27. doi: 10.1016/j.biopsych.2015.06.008
16. Lutz B, Marsicano G, Maldonado R, Hillard CJ. The endocannabinoid system in guarding against fear, anxiety and stress. Nat Rev Neurosci. (2015) 16:705–18. doi: 10.1038/nrn4036
17. Szejko N, Fremer C, Müller-Vahl KR. Cannabis improves obsessive-compulsive disorder—Case report and review of the literature. Front Psychiatry. (2020) 11:1. doi: 10.3389/fpsyt.2020.00681
18. Zehra A, Burns J, Liu CK, Manza P, Wiers CE, Volkow ND, et al. Cannabis addiction and the brain: a review. J Neuroimmune Pharmacol. (2018) 13:438–52. doi: 10.1007/s11481-018-9782-9
19. Kroon E, Kuhns L, Hoch E, Cousijn J. Heavy cannabis use, dependence and the brain: a clinical perspective. Addiction. (2020) 115:559–72. doi: 10.1111/add.14776
20. Santaella-Tenorio J, Levy NS, Segura LE, Mauro PM, Martins SS. Cannabis use disorder among people using cannabis daily/almost daily in the united states, 2002–20. Drug Alcohol Depend. (2019) 205:107621. doi: 10.1016/j.drugalcdep.2019.107621
21. Memedovich KA, Dowsett LE, Spackman E, Noseworthy T, Clement F. The adverse health effects and harms related to marijuana use: an overview review. C Open. (2018) 6:E339–46. doi: 10.9778/cmajo.20180023
22. Lowe DJE, Sasiadek JD, Coles AS, George TP. Cannabis and mental illness: a review. Eur Arch Psychiatry Clin Neurosci. (2019) 269:107–20. doi: 10.1007/s00406-018-0970-7
23. Pasman JA, Verweij KJH, Gerring Z, Stringer S, Sanchez-Roige S, Treur JL, et al. GWAS of lifetime cannabis use reveals new risk loci, genetic overlap with psychiatric traits, and a causal influence of schizophrenia. Nat Neurosci. (2018) 21:1161–70. doi: 10.1038/s41593-018-0206-1
24. Villatoro J, Medina-Mora ME, Fleiz Bautista C, Moreno López M, Robles NO, Bustos Gamiño M, et al. El consumo de drogas en méxico: resultados de la encuesta nacional de adicciones. https://www.researchgate.net/journal/Salud-Mental-0186-761X Salud Mental. (2012) 35:447–57. doi: 10.17711/SM.0185-3325.2012.001
25. Medina-Mora ME, Real T. The drug scene in mexico and the road ahead. Adicciones. (2013) 25:294–99. doi: 10.20882/adicciones.29
26. Pato MT, Sobell JL, Medeiros H, Abbott C, Sklar BM, Buckley PF, et al. The genomic psychiatry cohort: partners in discovery. Am J Med Genet B Neuropsychiatr Genet. (2013) 162B:306–12. doi: 10.1002/ajmg.b.32160
27. Docherty AR, Bigdeli TB, Edwards AC, Bacanu S, Lee D, Neale MC, et al. Genome-wide gene pathway analysis of psychotic illness symptom dimensions based on a new schizophrenia-specific model of the OPCRIT. Schizophr Res. (2015) 164:181–6. doi: 10.1016/j.schres.2015.02.013
28. Hartz SM, Pato CN, Medeiros H, Cavazos-Rehg P, Sobell JL, Knowles JA, et al. Comorbidity of severe psychotic disorders with measures of substance use. JAMA Psychiatry. (2014) 71:248–54. doi: 10.1001/jamapsychiatry.2013.3726
29. Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MAR, Bender D, et al. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet. (2007) 81:559–75. doi: 10.1086/519795
30. Marees AT, de Kluiver H, Stringer S, Vorspan F, Curis E, Marie-Claire C, et al. A tutorial on conducting genome-wide association studies: quality control and statistical analysis. Int J Methods Psychiatr Res. (2018) 27:e1608. doi: 10.1002/mpr.1608
31. Conomos MP, Miller MB, Thornton TA. Robust inference of population structure for ancestry prediction and correction of stratification in the presence of relatedness. Genet Epidemiol. (2015) 39:276–93. doi: 10.1002/gepi.21896
32. Cavalli-Sforza LL. The human genome diversity project: past, present and future. Nat Rev Genet. (2005) 6:333–40. doi: 10.1038/nrg1596
33. Bridgeman MB, Abazia DT. Medicinal cannabis: history, pharmacology, and implications for the acute care setting. P T. (2017) 42:180–1. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5312634/ (accessed December 17, 2020).
34. Pratt M, Stevens A, Thuku M, Butler C, Skidmore B, Wieland LS, et al. Benefits and harms of medical cannabis: a scoping review of systematic reviews. Syst Rev. (2019) 8:320. doi: 10.1186/s13643-019-1243-x
35. Mouhamed Y, Vishnyakov A, Qorri B, Sambi M, Frank SMS, Nowierski C, et al. Therapeutic potential of medicinal marijuana: an educational primer for health care professionals. Drug Healthc Patient Saf. (2018) 10:45–66. doi: 10.2147/DHPS.S158592
36. National Academies of Sciences Engineering and Medicine Health and Medicine Division Board on Population Health and Public Health Practice Committee on the Health Effects of Marijuana: An Evidence Review and Research Agenda. Therapeutic effects of cannabis and cannabinoids. In: The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington, DC: National Academies Press (2017). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK425767/ (accessed December 17, 2020).
37. Müller-Vahl KR. Treatment of tourette syndrome with cannabinoids. Behav Neurol. (2013) 27:119–24. doi: 10.1155/2013/294264
38. Müller-Vahl KR, Prevedel H, Theloe K, Kolbe H, Emrich HM, Schneider U. Treatment of tourette syndrome with delta-9-tetrahydrocannabinol (Δ9-THC): no influence on neuropsychological performance. Neuropsychopharmacology. (2003) 28:384–8. doi: 10.1038/sj.npp.1300047
39. Müller-Vahl KR, Schneider U, Prevedel H, Theloe K, Kolbe H, Daldrup T, et al. Δ9-tetrahydrocannabinol (THC) is effective in the treatment of tics in Tourette syndrome: A 6-week randomized trial. J Clin Psychiatry. (2003) 64:459–65. doi: 10.4088/JCP.v64n0417
40. Mergler M, Driessen M, Havemann-Reinecke U, Wedekind D, Lüdecke C, Ohlmeier M, et al. Differential relationships of PTSD and childhood trauma with the course of substance use disorders. J Subst Abuse Treat. (2018) 93:57–63. doi: 10.1016/j.jsat.2018.07.010
41. Chye Y, Christensen E, Solowij N, Yücel M. The endocannabinoid system and cannabidiol's promise for the treatment of substance use disorder. Front Psychiatry. (2019) 10:63. doi: 10.3389/fpsyt.2019.00063
42. Gonzalez-Cuevas G, Martin-Fardon R, Kerr TM, Stouffer DG, Parsons LH, Hammell DC, et al. Unique treatment potential of cannabidiol for the prevention of relapse to drug use: preclinical proof of principle. Neuropsychopharmacology. (2018) 43:2036–45. doi: 10.1038/s41386-018-0050-8
43. Kayser RR, Raskin M, Snorrason I, Hezel DM, Haney M, Simpson HB. Cannabinoid augmentation of exposure-Based psychotherapy for obsessive-compulsive disorder. J Clin Psychopharmacol. (2020) 40:207–10. doi: 10.1097/JCP.0000000000001179
44. Sherman BJ, McRae-Clark AL. Treatment of cannabis use disorder: current science and future outlook. Pharmacotherapy. (2016) 36:511–35. doi: 10.1002/phar.1747
45. Hasan A, von Keller R, Friemel CM, Hall W, Schneider M, Koethe D, et al. Cannabis use and psychosis: a review of reviews. Eur Arch Psychiatry Clin Neurosci. (2020) 270:403–12. doi: 10.1007/s00406-019-01068-z
46. Subodh BN, Sharma N, Shah R. Psychosocial interventions in patients with dual diagnosis. Indian J Psychiatry. (2018) 60:S494–500. doi: 10.4103/psychiatry.IndianJPsychiatry_18_18
47. Kedzior KK, Laeber LT. A positive association between anxiety disorders and cannabis use or cannabis use disorders in the general population- a meta-analysis of 31 studies. BMC Psychiatry. (2014) 14:136. doi: 10.1186/1471-244X-14-136
48. Naji L, Rosic T, Dennis B, Bhatt M, Sanger N, Hudson J, et al. The association between cannabis use and suicidal behavior in patients with psychiatric disorders: an analysis of sex differences. Biol Sex Differ. (2018) 9:22. doi: 10.1186/s13293-018-0182-x
49. Kosty DB, Seeley JR, Farmer RF, Stevens JJ, Lewinsohn PM. Trajectories of cannabis use disorder: risk factors, clinical characteristics and outcomes. Addiction. (2017) 112:279–87. doi: 10.1111/add.13557
50. Courtney KE, Mejia MH, Jacobus J. Longitudinal studies on the etiology of cannabis use disorder: a review. Curr Addict Reports. (2017) 4:43–52. doi: 10.1007/s40429-017-0133-3
51. Dugas EN, Sylvestre MP, Ewusi-Boisvert E, Chaiton M, Montreuil A, O'Loughlin J. Early risk factors for daily cannabis use in young adults. Can J Psychiatry. (2019) 64:329–37. doi: 10.1177/0706743718804541
52. Lewis CM, Vassos E. Prospects for using risk scores in polygenic medicine. Genome Med. (2017) 9:96. doi: 10.1186/s13073-017-0489-y
53. Wray NR, Lin T, Austin J, McGrath JJ, Hickie IB, Murray GK, et al. From basic science to clinical application of polygenic risk scores: a primer. JAMA Psychiatry. (2020) 78:101–9. doi: 10.1001/jamapsychiatry.2020.3049
54. Murray GK, Lin T, Austin J, McGrath JJ, Hickie IB, Wray NR. Could polygenic risk scores be useful in psychiatry? a review. JAMA Psychiatry. (2020) 78:210–219. doi: 10.1001/jamapsychiatry.2020.3042
55. Eeltink E, van der Horst MZ, Zinkstok JR, Aalfs CM, Luykx JJ. Polygenic risk scores for genetic counseling in psychiatry: lessons learned from other fields of medicine. Neurosci Biobehav Rev. (2020) 121:119–27. doi: 10.1016/j.neubiorev.2020.11.021
56. Gibson G. On the utilization of polygenic risk scores for therapeutic targeting. PLoS Genet. (2019) 15:e1008060. doi: 10.1371/journal.pgen.1008060
57. Santoro ML, Ota V, de Jong S, Noto C, Spindola LM, Talarico F, et al. Polygenic risk score analyses of symptoms and treatment response in an antipsychotic-naive first episode of psychosis cohort. Transl Psychiatry. (2018) 8:174. doi: 10.1038/s41398-018-0230-7
58. Zhang JP, Robinson D, Yu J, Gallego J, Fleischhacker WW, Kahn RS, et al. Schizophrenia polygenic risk score as a predictor of antipsychotic efficacy in first-episode psychosis. Am J Psychiatry. (2019) 176:21–8. doi: 10.1176/appi.ajp.2018.17121363
Keywords: obsessive-compulsive symptoms, cannabis use, Mexican population, polygenic risk score, cannabis dependence
Citation: Nicolini H, Martínez-Magaña JJ, Genis-Mendoza AD, Villatoro Velázquez JA, Camarena B, Fleiz Bautista C, Bustos-Gamiño M, Aguilar García A, Lanzagorta N and Medina-Mora ME (2021) Cannabis Use in People With Obsessive-Compulsive Symptomatology: Results From a Mexican Epidemiological Sample. Front. Psychiatry 12:664228. doi: 10.3389/fpsyt.2021.664228
Received: 04 February 2021; Accepted: 12 April 2021;
Published: 10 May 2021.
Edited by:
Odile Van Den Heuvel, VU University Medical Center, NetherlandsReviewed by:
Massimo Pasquini, Sapienza University of Rome, ItalyCopyright © 2021 Nicolini, Martínez-Magaña, Genis-Mendoza, Villatoro Velázquez, Camarena, Fleiz Bautista, Bustos-Gamiño, Aguilar García, Lanzagorta and Medina-Mora. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Elena Medina-Mora, bWV0bW1vcmFAZ21haWwuY29t; Humberto Nicolini, aG5pY29saW5pQGlubWVnZW4uZ29iLm14
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.