 Gérard Niveau
Gérard Niveau Camille Jantzi†
Camille Jantzi†- University Center of Legal Medicine, Geneva University Hospitals, Geneva, Switzerland
Background and Aims: In the field of mental health, the fundamental right to liberty is a point of tension between the practice of psychiatric commitment on the one hand and the universal concept of human rights on the other. The European Court of Human Rights (ECtHR) is a very specific means of safeguarding human rights because it allows an individual to not only assert their rights but also compel a state to bring its legislation into conformity with the principles of the European Convention on Human Rights. The aim of this study was to gather the case-law of the ECtHR on psychiatric commitment over the last 60 years and to determine how this case-law has affected national legislation and therefore psychiatric practice.
Methods: Jurisprudence data were collected from the HUDOC ECtHR database, and the direct effects of the ECtHR judgements on the legislations of the countries concerned were collected from the HUDOC EXEC database of the Council of Europe. The case-law of the Court included 118 judgements and 56 decisions and concerned 31 of the 45 countries that have ratified the Convention.
Results: This study therefore showed a direct effect of the Court's case-law on the legislation on psychiatric commitment in the various countries that have ratified the Convention. It was also possible to detect an indirect effect of this case-law through the directives of international institutions such as the directives of the Committee of Ministers of the Council of Europe concerning respect for people with mental disorders.
Conclusions: The ECtHR case-law therefore has a major influence on the psychiatric practice in all Council of Europe countries.
Introduction
Liberty is a fundamental human right recognized across all democratic states. This principle is, however, subject to many exceptions that are precisely defined by the national laws of each country. Psychiatric commitment is one of these exceptions. Psychiatry is a particular medical specialty in that it uses deprivation of liberty as a therapeutic means. Therefore, according to Gostin, there is “a fundamental relationship between mental health and human rights” (1). History shows that psychiatry has often been used as a means of social repression and that cases of psychiatric abuse are numerous (2). The principle that people with mental disorders have the same rights as other citizens is relatively recent (3). All democratic states have gradually organized a set of laws that determine the conditions for the implementation of psychiatric commitment and the remedies available to patients to assert their rights and oppose the deprivation of liberty. However, the regulation of psychiatric commitment is always complex because it must allow both respect for the rights of patients and respect for public safety, including the safety of the patient himself (4). Infringing a fundamental right as a means of treatment represents a risky situation for the rights of patients (5).
When a citizen believes that he or she has had his rights violated, specifically the right to liberty during psychiatric commitment, he or she must have the ability to resort to an authority of justice to enforce his rights. In the conflict between the citizen and the State, even in democratic countries, the risk of inequality is significant. However, in countries that have ratified the European Convention of Human Rights, the European Court of Human Rights (ECtHR or the Court) gives citizens an exceptional means of defending their rights (6). The ECtHR is a very particular supranational legal system because it gives an individual the ability to not only assert his rights but also have a state condemned and, in certain cases, be at the origin of a judgement that will force the state to modify its legislation to conform to the principles of respect for fundamental rights. By filing an application with the ECtHR, a patient who has been deprived of his liberty due to psychiatric commitment can therefore not only assert his rights but also influence the national jurisdiction of the country where he or she was involuntarily hospitalized (7).
The organization of the ECtHR is relatively complex, and it has evolved over the years, both in substance and in form. Currently, 45 countries have ratified the Convention and are therefore affected by the ECtHR. An application can be made to the Court only when all domestic remedies have been exhausted. The processing of applications before the ECtHR takes place in several stages. Requests are first systematically examined for admissibility by a filtering section and a single judge. Potentially admissible applications are then examined by a one of the five Chambers of seven judges. The Chamber makes a determination on the merits as to whether the Convention has been violated. If one of the parties petitions successfully for the case to be re-heard at a higher level, the Grand Chamber becomes involved. In simplified terms, the case law of the Court therefore consists of decisions concerning the admissibility of applications and judgements concerning the violation of the articles of the Convention. A friendly settlement can occur at any time during the procedure and lead to the classification of the case (7).
If the Grand Chamber pronounces a judgement, it is transmitted to the Committee of ministers who must have it enforced. The state that is the subject of the judgement must satisfy individual obligations toward the applicant and general obligations so as to avoid a further similar violation of fundamental rights. Among these general obligations may be those that modify the legislative system, the dysfunctions of which led to the violation(s) (8).
The work of the ECtHR began in 1960; and in 2019, the organization celebrated its 60th anniversary. The aims of this study are to describe the activity of the ECtHR in the field of the legal regulation of psychiatric commitment, to expose the main cases with exemplary value and to determine which legal cases have led to changes in national legislations.
Materials and Methods
Case-Law of the ECtHR
All the data concerning the case-law were extracted from the HUDOC database. HUDOC is the official case-law database of the ECtHR (9). This database is open access and allows direct access to all the Court's case-law since 1960.
A search in HUDOC was carried out for the period from January 1, 1960, to December 31, 2019. The two keywords “(Art. 5-1-e) Alcoholics” and “(Art. 5-1-e) Persons of unsound mind” were used with the Boolean operator OR. The language filter was used to remove duplicates by using the “English OR French” selection.
The case-law data have been classified in accordance with the Court's method, which distinguishes four degrees of importance of decisions and judgements: the key cases, the level 1 cases, the level 2 cases and the level 3 cases. The key cases refer to situations concerning large groups of identical cases that are derived from the same underlying problem. The judgement of the Court permits to identify the dysfunction under national law that is the root of a violation and to give indications to the government to create a domestic remedy capable of dealing with similar cases. Level 1 cases, which are of high importance, refer to situations that make a significant contribution to the development, clarification or modification of the Court's case-law, either generally or in relation to a particular state. Level 2 cases, which are of medium importance, refer to situations that do not make a significant contribution to the case-law but go beyond merely applying existing case-law. Level 3 cases, which are of low importance, refer to situations of little legal interest.
Effects of ECtHR Judgements and Decisions on Domestic Laws
To underscore the influence of the Court on national jurisdictions concerning psychiatric commitment, the measures taken by the governments of the different countries concerned by the key cases and the level 1 cases were sought. This research was carried out using the HUDOC EXEC database of the Department for the Execution of Judgements of the ECtHR of the Council of Europe (10). A specific search was carried out for each judgement or decision by referring to the case code number assigned by the ECtHR. Among the decisions taken by governments, only those concerning changes in laws or the application of laws were noted. The decisions concerning the “dissemination of the Court's judgement” were not noted.
Results
Case-Law of the ECtHR
Among the 22,536 judgements and 26,887 decisions of the Court between December 31, 1960, and December 31, 2019, the research in the HUDOC database identified 174 cases of case law concerning psychiatric commitment. This case-law included 56 decisions on the admissibility of applications, and 118 judgements of the Court concerning violations of articles of the Convention.
Table 1 gives the number of ECtHR decisions and judgements classified by country and by degree of importance. The 56 decisions, taken by a Chamber or by the Commission (up to 31 October 1999), consisted of 25 applications declared inadmissible, 15 applications declared partially admissible and partially inadmissible, and 16 applications declared admissible. The 118 judgements were divided into 12 key cases, 14 level 1 cases, 63 level 2 cases, and 84 level 3 cases.
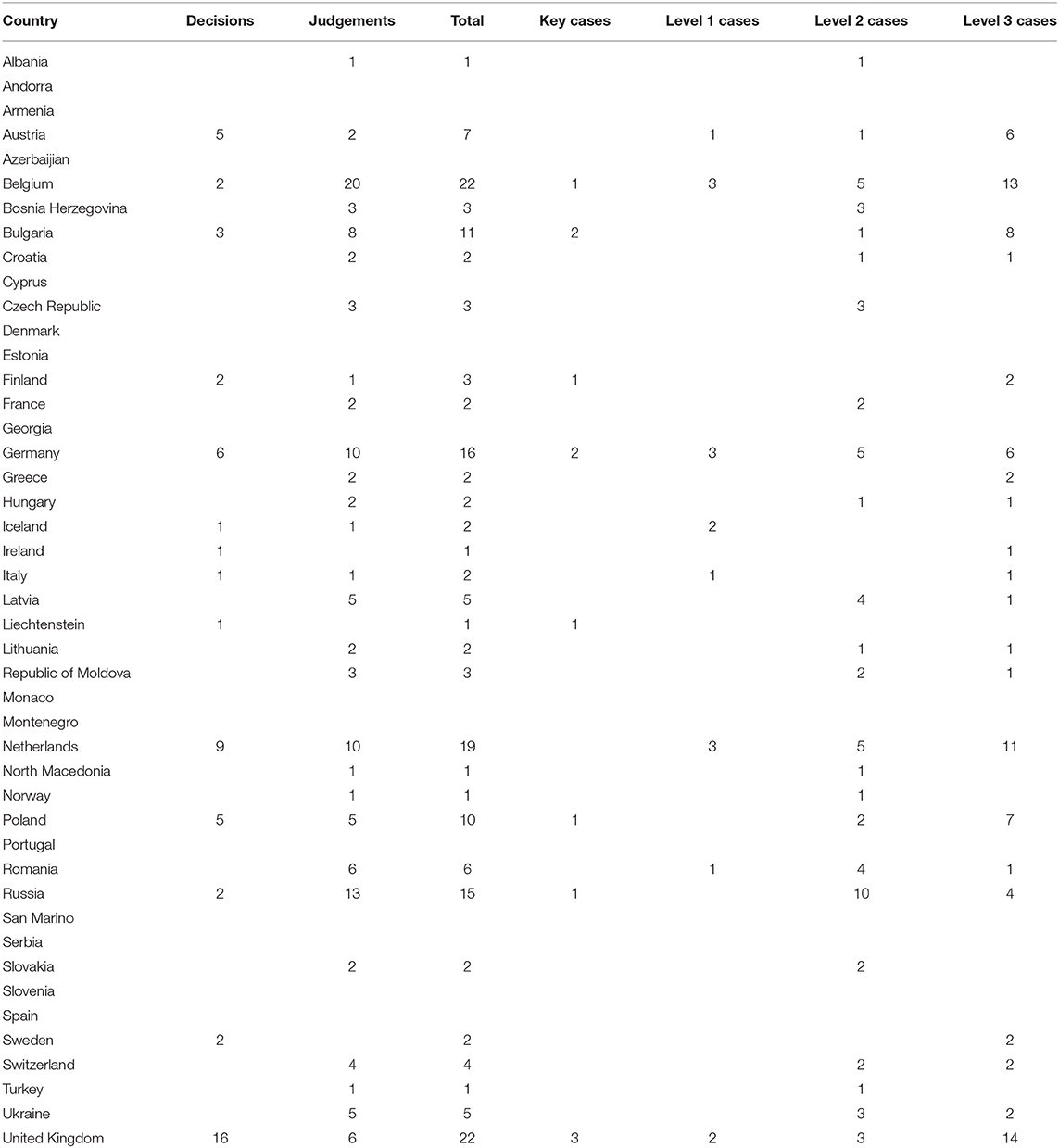
Table 1. ECtHR judgements and decisions by country and by level of importance.
The key cases are summarized in Table 2 and the level 1 cases are summarized in Table 3. It can be seen that the requests relating to the deprivation of liberty during psychiatric commitment can also relate to other aspects of Human Rights, in particular to Article 3 of the Convention (prohibition of inhuman and degrading treatment) and to Article 6 of the Convention (right to a fair trial). In the event of a violation of an article of the Convention, two situations may arise: either there is a national law that protects the rights of the patient, but this law has not been respected; or the national law is not in conformity with the principles of the Convention for the protection of the rights of the patient. It is especially in these fault situations that the judgement of the Court leads to the obligation of the government of the country concerned to amend its national legislation. The non-conformity of the national law with the principles of the Convention can relate to very different aspects, but it often acts of a failure in the establishment of the statement of mental illness or a defect in the possibilities for the patient to appeal against his deprivation of liberty or even an excessively long duration of the procedures.
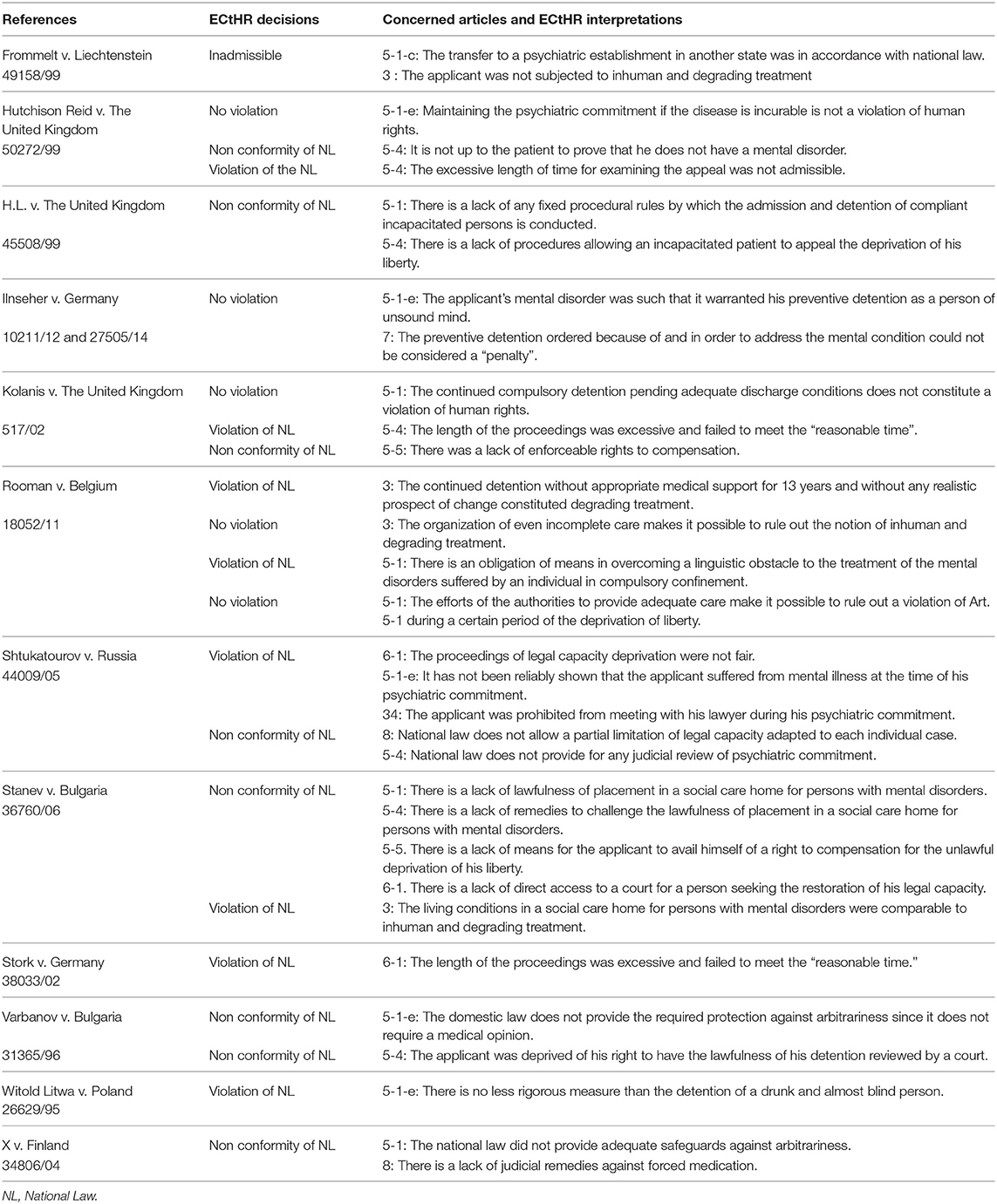
Table 2. ECtHR pilot case law concerning psychiatric commitment.
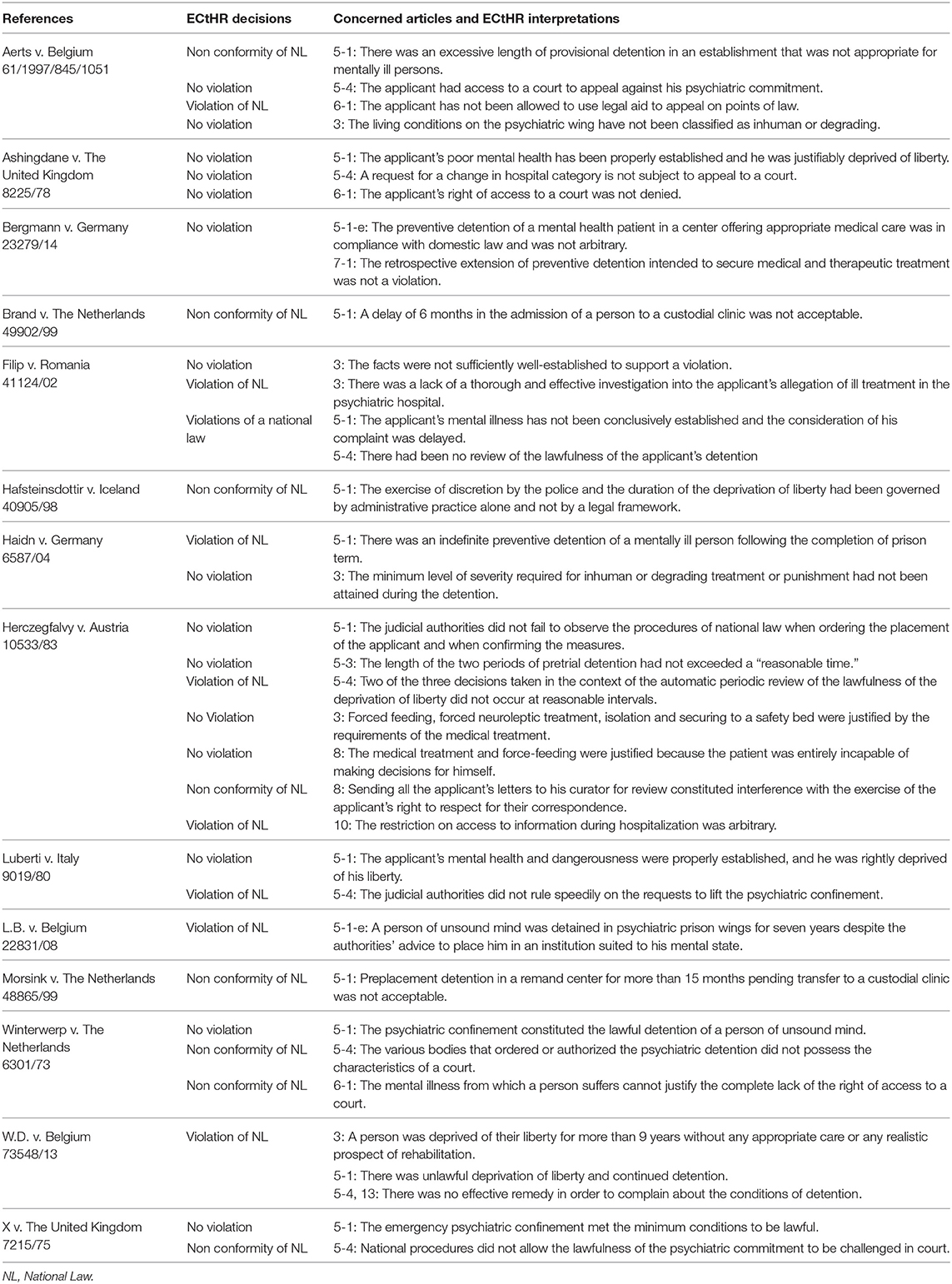
Table 3. ECtHR level 1 case law concerning psychiatric commitment.
Effects of ECtHR Judgements and Decisions on Domestic Laws
The effects of ECtHR judgements in key cases and level 1 cases are summarized in Tables 4, 5, respective. It is possible to note that Austria, Belgium, Bulgaria, Germany, Iceland, the Netherlands, Romania, and the United Kingdom have modified their national laws concerning psychiatric commitment as direct consequences of ECtHR judgements. The modifications varied according to the domestic laws, but it is possible to note that the changes were always in the direction of improvement with respect to the rights of the patients, in particular regarding the aspects of the initial conditions of the commitment, of the right of appeal against the placement decision, of the reduction in the length of the procedures, and of the improvement of the living conditions and treatments of interned persons.
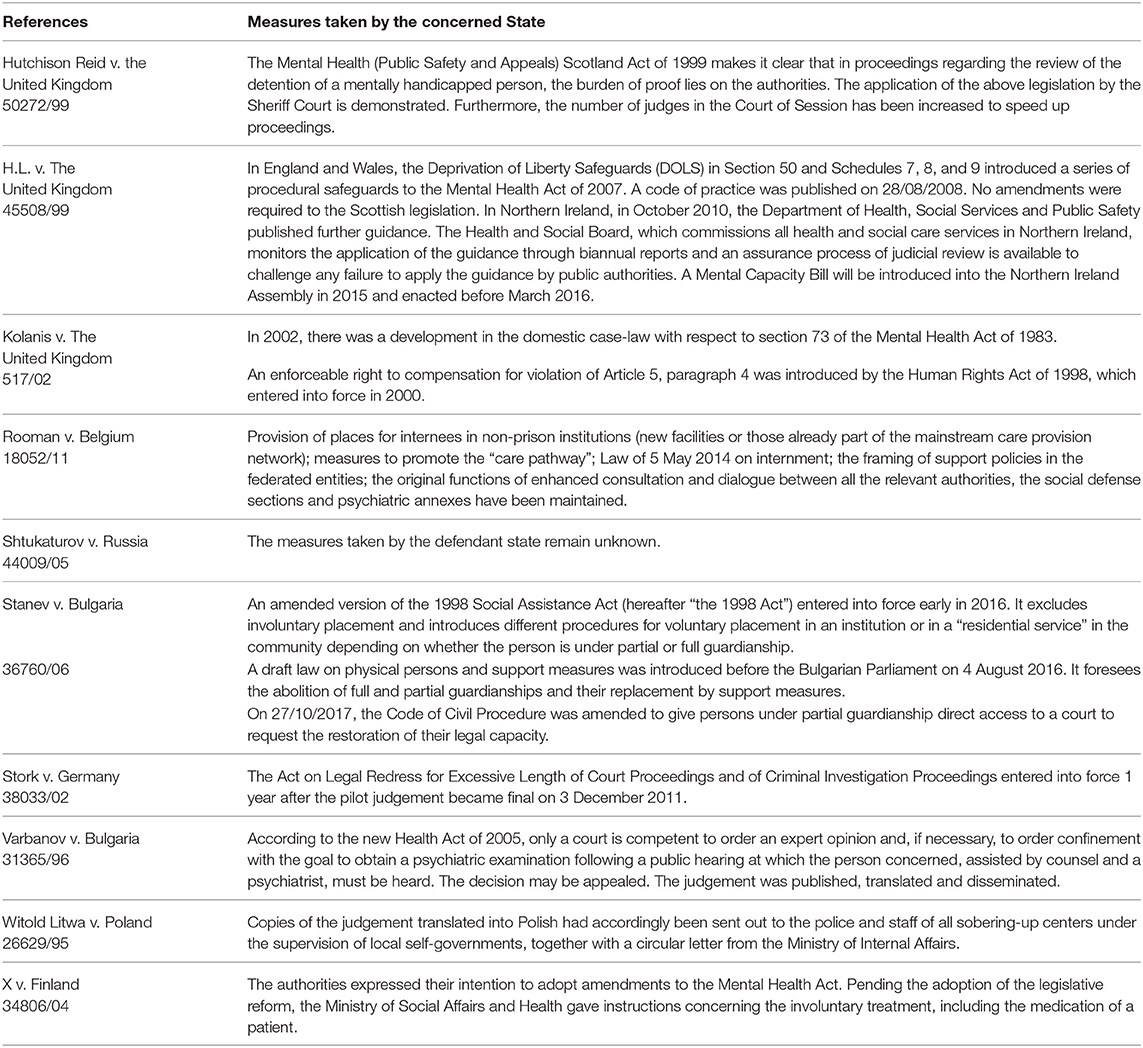
Table 4. Consequences of the pilot case law of the ECtHR on national legislations (text extracted from the Council of Europe HUDOC EXEC database).
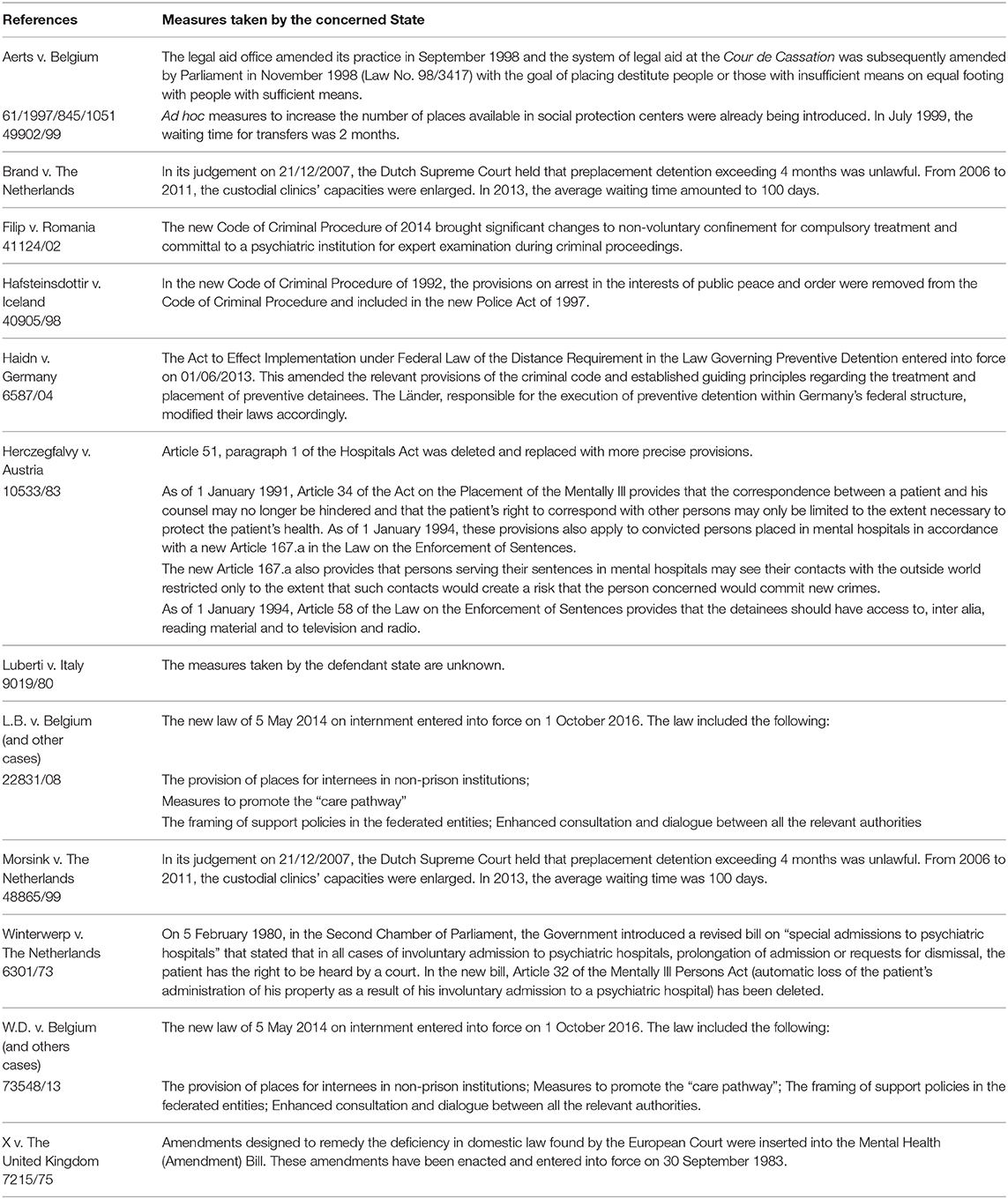
Table 5. Consequences of the level 1 case law of the ECtHR on national legislations (text extracted from the of the Council of Europe HUDOC EXEC database).
It should also be noted that not all countries follow the decisions of the judgments of the Court. Russia is notorius for changing nothing, despite the convictions by the Court. It is difficult to know precisely, by reading the requests and judgments, the reality of what is happening in these countries for patients interned in psychiatric hospitals. The action of organizations which intervene directly in places of detention, such as the CPT, is therefore essential in denouncing the persistence of human rights violations.
Discussion
This study of the case-law of the ECtHR shows that 31 of the 45 countries that have ratified the Convention have been affected by a decision or a judgement of the Court concerning psychiatric commitment. The number and nature of changes required by the Court's judgements, however, vary widely from country to country. In fact, there are multiple reasons why a country is the subject of decisions or judgements of the ECtHR, and there is no direct relation to the quality of their legislation concerning psychiatric commitment. For example, the size of the country's population and the time since it has ratified the Convention are obvious factors. It is also possible to observe that countries with very developed legal systems and where the defense of the rights of the citizens is well represented, such as Belgium, the Netherlands, Germany, or the United Kingdom, are subject to many applications to the Court and therefore more decisions or judgements (11). It is therefore irrelevant to compare countries with one another in terms of the number of judgements of the ECtHR. The activity of the ECtHR must be understood as a global process of improving jurisdiction throughout the geographical area covered by the activity of the Court. The study of the ECtHR case law and of the database of the Department for the Execution of judgements of the ECtHR of the Council of Europe clearly shows the direct and concrete favorable effects of the ECtHR on the rights of patients affected by psychiatric confinement (12). Reading the proceedings of the Court also reveals the essential role of dedicated and committed counsel in ensuring the representation of applicants and asserting their rights (13).
However, it would be wrong to believe that the influence of the Court is limited to these direct effects. From a historical point of view, during the 60 years from the first judgements of the Court in 1960 until 2019, many changes have been made in the laws of Council of Europe countries concerning psychiatric commitment without these countries being directly affected by judgements of the Court but drawing inspiration from the case law of the ECtHR (14). First, the key cases and the level 1 cases serve as references for legislators when they design a change in law or create new laws. Second, on the basis of its own case law, the ECtHR gives guidelines on the main points that should structure national laws. Regarding psychiatric commitment, the ECtHR's guidelines were updated in December 2019 in the Guide to Article 5 of the European Convention on Human Rights (15):
• The detention of persons of unsound mind is an exception to the general principle of Art. 5 of the Convention. An essential point of the case law is therefore to determine what the term person of “unsound mind” means. The Court has always been careful not to depend on local or specific definitions of a law or a social context (Rakevich v. Russia, Petschulies v. Germany, Ilnseher v. Germany).
• The ECtHR defines three minimum conditions for an individual to be deprived of his liberty as being of “unsound mind”:
➢ The first condition is that unless it is an emergency situation, an objective medical expert must establish that the individual is of unsound mind (Ruiz Rivera v. Switzerland, S.R. v. the Netherlands). If a medical examination of the person is not possible, the Court accepts that the expert can make a determination based on the case file (Constancia v. the Netherlands). The mental disorder must be of a certain seriousness to be considered a “true” mental disorder, that is, it must necessitate treatment in an institution appropriate for mental health patients (Glien v. Germany, Ilnseher v. Germany, and Petschulies v. Germany). The existence of the mental disorder must be conclusively established as soon as the person concerned is in psychiatric commitment (Ilnseher v. Germany, O.H. v. Germany). The evolution of mental health after placement must be taken into account and the medical reports on which the authorities are based must be sufficiently recent (Ilnseher v. Germany, Kadusic v. Switzerland).
➢ The second condition is that the individual's mental disorder must justify the compulsory confinement. In the case-law of the Court, this condition concerns not only the need for treatment but also the need for control and supervision to prevent the person from harming himself or other persons (Ilnseher v. Germany, Hutchison Reid v. the United Kingdom, and N. v Romania).
➢ The third condition is that the trouble must persist throughout the period of the deprivation of the individual's liberty. This means that as soon as the mental disorder is no longer present, the person concerned must be released. However, the Court recognizes that the authorities may have a short period of time to examine whether the detention can be lifted (Luberti v Italy). Psychiatric commitment, however, cannot be maintained for administrative reasons (R.L. and M.-J.D. v. France).
• The place of psychiatric commitment gave rise to the case-law of the Court. Normally, the placement of a person of unsound mind should be carried out in “a hospital, a clinic or an appropriate institution authorized for the detention of such persons” (L.B. v. Belgium, Ashingdane v. the United Kingdom, and O.H. v. Germany). However, if the time limit is short, the psychiatric commitment will take place temporarily in an establishment not specifically designed for this kind of placement (Pankiewicz v. Poland, Morsink v. the Netherlands, and Brand v. the Netherlands).
• The Court has regularly noted that the administration of suitable therapy is one of the legal conditions justifying the deprivation of liberty of a person of unsound mind. The psychiatric commitment has the function of treating or curing the patients on the one hand and, if necessary, reducing or managing their dangerousness on the other hand (Rooman v. Belgium). These two functions constitute the concept of “appropriate institution.”
• The application of Article 5-1-e of the Convention includes procedural safeguards related to the procedure of involuntary hospitalization (M.S. v. Croatia, n°2). A fair procedure must allow the interned person to have access to a means of protection against arbitrariness (V.K. v. Russia, X. v. Finland). It therefore seems particularly important that a person in psychiatric commitment should have access to a court and be heard either in person or through a representative. Each interned person must have access to legal assistance for any procedure relating to the deprivation of liberty (N. v. Romania). The Court noted that legal assistance should not only be formal, but it should be effective and controlled by competent domestic courts [M.S. v. Croatia (n°2), V.K. v. Russia].
• Concerning the application of Article 5-1-e to situations of the deprivation of liberty of people under the influence of alcohol, the Court considered that the term “alcoholics” concerns not only people dependent on alcohol but also people whose consumption of alcohol poses a danger to themselves and to others. (Kharin v. Russia, Hilda Hafsteinsdottir v. Iceland). However, according to the Court, Article 5-1-e does not allow the deprivation of liberty of a person solely because he or she consumes alcohol (Petschulies v. Germany, Witold Litwa v. Poland).
The case law of the ECtHR determines the profile of the judicial procedures allowing the internment of people of unsound mind when it is necessary while preserving the rights of those concerned. However, it is not the role of the Court to determine an ideal psychiatric commitment procedure that could be applied universally. The case law of the ECtHR is constantly in line with the historical and cultural particularities of the States. However, inspired by the work of the ECtHR and that of the CPT, the Committee of Ministers of the Council of Europe in 2004 issued recommendations to member States concerning the respect of people with mental disorders, and in Articles 17–25 they included recommendations concerning the involuntary hospitalization of people suffering from mental disorders (16). These articles set out the conditions under which a person may be placed in a hospital involuntarily, the essential remedies and the conditions for the termination of the placement. Several European countries, such as Austria, France, Germany, Italy and Spain, have modified or amended their laws on psychiatric commitment according to the directives of the Council of Europe (14). It is therefore appropriate to consider that the case-law of the ECtHR has, in addition to the direct effects due to judgements, indirect effects by inspiring changes in the legislation of many countries. Finally, in a movement of reciprocal influence, it can be noted that the ECtHR itself has cited in recent judgments (Asalya v. Turkey, Kuttner v. Australia) Article 14 of the Convention on the Rights of Persons with Disabilities (17).
Conclusion
Whatever the country and whatever the time, psychiatric involuntary hospitalization is and will remain a situation of conflict and confrontation between an individual and a State. Psychiatric commitment is a paradigmatic expression of the question of human rights expressed in the field of psychiatry. A just law must strike a balance between the rights of the individual and the protection of society. The correctness of the law is essential for respecting patients' rights and therefore for safeguarding ethics in the practice of caregivers and hospital doctors. The case law of the ECtHR is a constant source of inspiration for improving the laws on psychiatric commitment and for the proper implementation of this law in the practice of care and treatment. Other sensitive areas of psychiatry, such as forced treatment or measures restricting freedom, are also the subject of an ECtHR case law that is often not well known.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
All authors have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Gostin LO. Human rights of persons with mental disabilities. The European Convention of Human Rights. Int J Law Psychiatry. (2000) 23:125–59. doi: 10.1016/S0160-2527(99)00039-4
2. Tort-Herrando V, Tataru N, Barrios-Flores F-L. National laws and their history. In: Goethals K, editor. Forensic Psychiatry and Psychology in Europe. Cham: Springer (2018). p. 19–30.
3. Puras D, Gooding P. Mental health and human rights in the 21st century. World Psychiatry. (2019) 18:42. doi: 10.1002/wps.20599
4. Davidson L. Human rights vs. public protection: English mental health law in crisis? Int J Law Psychiatry. (2002) 25:491–515. doi: 10.1016/S0160-2527(02)00142-5
5. Phillips L, Matravers W. Liberty: human rights and mental health. Comm L. World Rev. (2002) 31:107.
6. Harding TW. The application of the European Convention of Human Rights to the field of psychiatry. Int J Law Psychiatry. (1989) 12:245–62. doi: 10.1016/0160-2527(89)90017-4
7. European Court of Human Rights. Rules of Court (2020). Retrieved from: https://echr.coe.int/Pages/home.aspx?p=basictexts/rules&c= (accessed October 2, 2020).
8. Departement for the Execution of judgements of the European Court of human Rights. Rules and Working Methods of the Committee of Ministers (2020). Retrieved from: https://www.coe.int/en/web/execution/rules-and-working-methods (accessed October 2, 2020).
9. European Court of Human Rights. HUDOC Database. Retrieved from: https://www.echr.coe.int/Pages/home.aspx?p=caselaw/HUDOC&c= (accessed 2 October 2020).
10. Department for the Execution of Judgements of the ECHR of the Council of Europe. HUDOC EXEC (2020). Retrieved from: https://hudoc.exec.coe.int/eng# (accessed October 2, 2020).
11. Niveau G, Materi J. Psychiatric commitment: over 50 years of case law from the European Court of Human Rights. Eur Psychiatry. (2007) 22:59–67. doi: 10.1016/j.eurpsy.2006.05.004
12. Kingdon D, Jones R, Lönnqvist J. Protecting the human rights of people with mental disorder: new recommendations emerging from the Council of Europe. Br J Psychiatry. (2004) 185:277–9. doi: 10.1192/bjp.185.4.277
13. Perlin ML. Striking for the guardians and protectors of the mind: the convention on the rights of persons with mental disabilities and the future of guardianship law. Penn St L Rev. (2012) 117:1159.
14. European Union Agency for Fundamental Rights. Involuntary Placement and Involuntary Treatment of Persons With Mental Health Problems (2012). Retrieved from: https://fra.europa.eu/en/publication/2012/involuntary-placement-and-involuntary-treatment-persons-mental-health-problems (accessed 2 October 2020).
15. European Court of Human Rights. Guide on Article 5 of the European Convention Human Rights. Retrieved from: https://www.echr.coe.int/documents/guide_art_5_eng.pdf (accessed 2 October 2020)
16. Council of Europe. Recommendation NO.REC(2004)10 of the Committee of Ministers to member States concerning the protection of the human rights and dignity of persons with mental disorder and its Explanatory Memorandum (2004). Retrieved from: https://www.coe.int/t/dg3/healthbioethic/Activities/08_Psychiatry_and_human_rights_en/Rec(2004)10%20EM%20E.pdf (accessed 2 October 2020).
Keywords: psychiatric commitment, involuntary hospitalization, human rights, ECtHR, forensic psychiatry
Citation: Niveau G, Jantzi C and Godet T (2021) Psychiatric Commitment: Sixty Years Under the Scrutiny of the European Court of Human Rights. Front. Psychiatry 12:656791. doi: 10.3389/fpsyt.2021.656791
Received: 21 January 2021; Accepted: 31 March 2021;
Published: 04 May 2021.
Edited by:
Birgit Angela Völlm, University of Rostock, GermanyReviewed by:
Peter Bartlett, University of Nottingham, United KingdomMichael Perlin, New York Law School, United States
George Szmukler, King's College London, United Kingdom
Copyright © 2021 Niveau, Jantzi and Godet. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gérard Niveau, R2VyYXJkLk5pdmVhdUBoY3VnZS5jaA==
†These authors have contributed equally to this work and share last authorship