 Shen Menglu
Shen Menglu Liu Ruiwen1
Liu Ruiwen1 Yang Suyong
Yang Suyong Zhu Dong
Zhu Dong
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Psychiatry , 10 June 2021
Sec. Addictive Disorders
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.653229
This article is part of the Research Topic Human Connection as a Treatment for Addiction View all 20 articles
Purpose: Exercise improves the health and mental status of drug dependents. The way by which Tai Chi (TC) as a special exercise treatment affects executive functions (EFs) of methamphetamine (MA) dependents is yet to be established. This study aimed to explore the effects of TC on the EFs and physical fitness of MA dependents.
Methods: A total of 76 female MA dependents were randomly assigned to the exercise and control groups. The exercise group underwent three 60-min sessions of TC training per week for 12 weeks. The control group was trained with conventional exercises including the 9th Guang Bo Ti Cao and square dance. Physical fitness and EF assessments that evaluated inhibitory control (IC, go/no-go task), working memory (3-back task) and cognitive flexibility (switching task) were performed at baseline and at 12 weeks. A repeated-measures ANOVA was applied to analyze the differences of group and time.
Results: The exercise group showed decreased response time (RT) with a significant main effect of time on the go/no-go task [F(1, 68) = 9.6, p < 0.05]. The interaction effect between time and group was significant on accuracy [F(1, 61) = 4.73, p < 0.05], and the main effect of time was significant on RT [F(1, 61) = 4.66, p < 0.05] in the 3-back task of the exercise group. Significant changes in BMI [F(1, 68) = 19.57, p < 0.05], vital capacity [F(1, 68) = 6.00, p < 0.05], and systolic blood pressure [F(1, 68) = 6.11, p < 0.05] were observed in the exercise group.
Conclusion: These findings showed that 3 months of TC training can improve the IC and maintain the working memory and cognitive flexibility of MA dependents. Other data implied that TC may improve the physical fitness of MA dependents.
Clinical Trial Registration: http://www.chictr.org.cn/, ChiCTR1900022091.
Methamphetamine (MA) dependence is a growing global concern that has a negative impact on public health (1). MA is reportedly the most widely used illicit drug, second only to cannabis (2). Besides the rapid increase in MA use in Europe (3) and the USA (4), the prevalence of MA use and abuse in Asian has advanced to an alarming degree (5). Approximately 9.9 million of the world's MA users are reportedly living in Asia; and ~1.2 million MA users are residing in China in 2019 (6). Long-term use of MA and other illicit drugs can lead to impairments in the physical health of users (7–10). Several physical fitness aspects of drug dependents (e.g., motor movement, mental status, and cardiopulmonary function) are reportedly poorer than those of normal individuals (11, 12). As a highly addictive psycho-stimulant drug, MA negatively affects individuals' brain structure and function, thus, resulting in behavioral impairments (13, 14). A neuropsychological study found that individuals' cognitive function was significantly impaired after long-term exposure to MA, and such impairment was associated with the abnormal brain function and metabolism due to MA use (15). Compared with dependence to other drugs, MA dependence reportedly causes a more severe impairment in cognitive function (16).
Executive function (EF) is a critical mental process consisting of inhibition, including inhibitory control (IC), working memory, and cognitive flexibility, which are the three core functions of EF (17, 18). EFs are skills essential for mental and physical health (19). Addiction is one of the causes of executive impairments, and similarly, an inseparable relationship exists between poor EF and substance abuse (19). Generally, illicit drug dependents manifest higher impulsiveness in behavior and decision-making than healthy individuals (20–27) due to their impaired EFs. Cognitive studies suggested that individuals who are chronically exposed to illicit drugs have difficulties in execution, inhibition, and decision-making (28). IC is a factor in the prediction of successful recovery in drug dependents (16, 29, 30) and in the maintenance of addiction (31). In executive tasks, MA dependents and other illicit drug users always show poor IC under drug-related stimuli (words or sentences describe MA or scene of MA abuse) (27). Previous studies also found that alcohol, cocaine, nicotine, and Internet dependents have poorer attention span, response time (RT), and accuracy under related stimuli in some EF tasks, indicating their poor IC (32–36). Working memory is the ability to temporarily store the information in the mind; this memory is put to work during the process of executing cognitive tasks (37). A close relationship is reported between working memory and IC; IC is supported by working memory to guide individuals' behaviors to avoid mistakes. When EF is needed, the working memory will shift its function and work together with IC (19). However, drug dependents reportedly have impaired working memory (38, 39). Cognitive flexibility is built on the other two EFs (19), and accumulating evidence indicates that MA dependents exhibit impaired cognitive flexibility (39). The core EFs of the MA dependents are impaired, and the impairment is likely associated, at least in part, with continued drug seeking and using (39).
In recent years, the use of exercise as an intervention to drug dependence has attracted considerable attention (40, 41). Exercise has been proved to greatly ameliorate the EF impairments (42, 43). A systematic review also clarified the positive effects of physical exercise on the enhancement of EF (44). Acute and aerobic exercises were proved to exert positive effects on IC (45–47) according to the results of go/no-go task, which is a psychological task usually used to assess IC (48). Moderate-intensity exercise was also reported to improve working memory performance (49). Moderate-intensity exercise has good effects on EFs because the effect of moderate exercise on IC is superior to other exercises (50, 51). Meanwhile, exercise can improve the health of illicit drug dependents (52). Both short- and long-term moderate-intensity aerobic exercises can enhance their physical fitness and life quality (53). Recent research reported that physical fitness, which includes body mass index (BMI), vital capacity, flexibility, balance and muscle strength, of illicit drug dependents significantly improved after aerobic exercise (54). Withdrawal symptoms of drug users and the likelihood of relapse can also be greatly relieved and reduced by exercises (55, 56).
Tai Chi (TC) is one of the globally renowned Chinese traditional mind–body exercises with a long history. It is the most used intervention method among Chinese tradition exercises because it can mobilize many parts of the body (e.g., dynamic posture control, symmetrical body activities, and body–hand–eye coordination) and reach a certain exercise intensity simultaneously. TC has attracted an increasing amount of attention as a potentially effective method to improve brain health and cognition, and to slow brain aging (57, 58). Several systematic reviews and meta-analysis reported the improved cognition and EF in older adults after TC exercise (59, 60). Studies using brain function test instruments all showed improvements in parameters related to decision-making ability and IC after TC intervention compared with other exercises (61, 62). Nevertheless, studies focusing on the effect of TC on EFs of MA dependents are relatively few. Researchers have focused on the effects of TC on physical and mental health of both male and female drug users, and they reached the consensus that TC exercise has positive influences on mind-body health, specifically on cardiopulmonary function, physical functional performance, and mental status (63–65). A related study provided evidences of the remarkable effects of TC on blood pressure, vital capacity, flexibility, and aerobic endurance in drug users (66). Significant improvements in the physical fitness of hand grip, sit-and-reach, push-up and balance ability, and decreased craving were observed after several months of TC intervention in amphetamine-type dependents (54). Similarly, enhanced life quality of illicit drug users was found following 12 weeks of TC exercise (67). TC also had a beneficial effect on the depression and anxiety symptoms of drug dependents (68). Therefore, TC may be an effective intervention for the physical fitness and EFs of female MA dependents.
Exercise is reportedly beneficial for illicit drug dependents. As a traditional exercise, TC has potential application in the rehabilitation of illicit drug dependents. However, few studies investigated the effects of TC on the EFs of illicit drug dependents. Accordingly, the present study aimed to investigate the effects of TC training on the EFs (IC, working memory, and cognitive flexibility) and physical fitness of female MA dependents. Considering that illicit drug dependents showed improvements in cognition after exercising (41, 69), we hypothesized that TC would exert a positive impact on the EF and improve the physical condition of MA dependents.
The study is a single-blind randomized controlled trial (ChiCTR1900022091), in which the effect of TC on the EF and physical fitness of MA dependents was examined.
Potential participants were recruited by posting research information in the Shanghai Female Mandatory Detoxification and Rehabilitation Center (SFMDRC). All the participants took part in the study voluntarily. Subjects who participated in the trial and completed the whole study under regulations were rewarded with increased frequency of family calls. Eligible participants were randomized in a 1:1 ratio to the exercise or control group. The randomization sequence was created by SPSS version 25.0 and was unknown to the research staff performing the study procedures. All participants were scheduled to complete a 12-week intervention program post-randomization. The results of EF tasks, including go/no-go, 3-back and switching task, which related to individuals' IC, working memory, and executive control, were measured at baseline and after the intervention. Physical fitness parameters were also assessed simultaneously. The Institutional Review Board of Shanghai University of Sport and Chinese Clinical Trial Register approved the study. Informed consent was obtained from all participants in accordance with the Declaration of Helsinki.
The inclusion criteria were as follows: (1) female, aged 18–65 years old; (2) reported history of using MA; (3) no severe medical or mental disease; and (4) educational attainment of primary school or above. The exclusion criteria were as follows: (1) currently diagnosed with Axis I psychiatric disorders, neurological illnesses or trauma affecting the central nervous system; (2) underwent pharmacological treatment with psychotropic medications during or before the study; (3) have anti-social personality disorder and borderline personality disorder; and (4) unwillingness to accept the assigned intervention conditions. Eighty participants were enrolled. Among them, four were excluded for not meeting the criteria. Among these four, three were excluded due to personnel mobilization, and one was excluded due to judicial detention. The final sample comprised 72 participants (Figure 1).
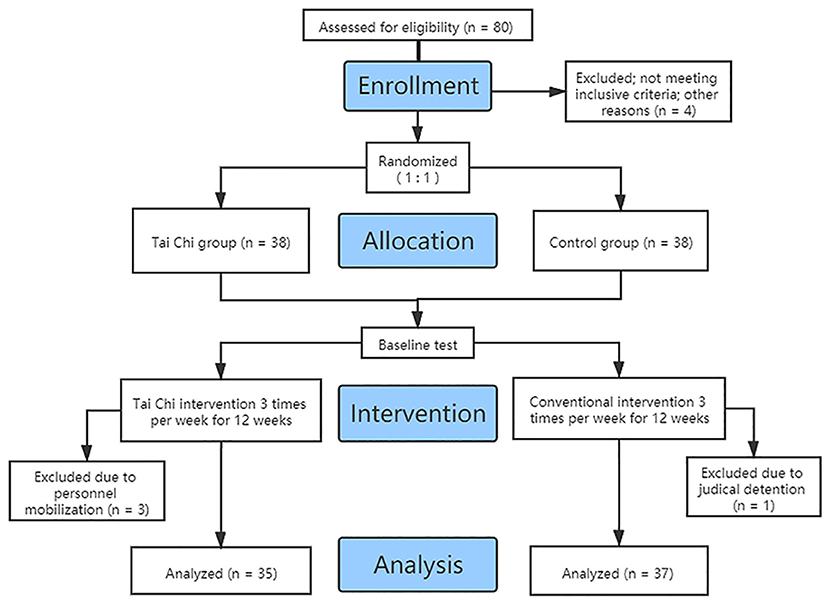
Figure 1. Flowchart of participant enrollment.
Blood pressure was measured using OMRON 7113, and the average value was calculated after three consecutive measurements. The maximum lung capacity was recorded after two measurements using an electronic spirometer (FCS-10000, China). A stopwatch was used to measure the length of time the subjects stood on one leg with eyes closed, which reflected their balance ability. Timing was terminated when subjects moved their legs or opened their eyes. The average value was calculated after two measurements. A sit and reach tester was used to measure the flexibility index. The maximum distance was recorded after two measurements. BMI was calculated as weight in kilograms divided by height in meters squared. A grip strength device was used to measure hand grip. Subjects were instructed to grasp the device for a few seconds while exerting their maximum strength. Table 1 summarizes the demographic characteristics and physical fitness parameters of the two groups at baseline.
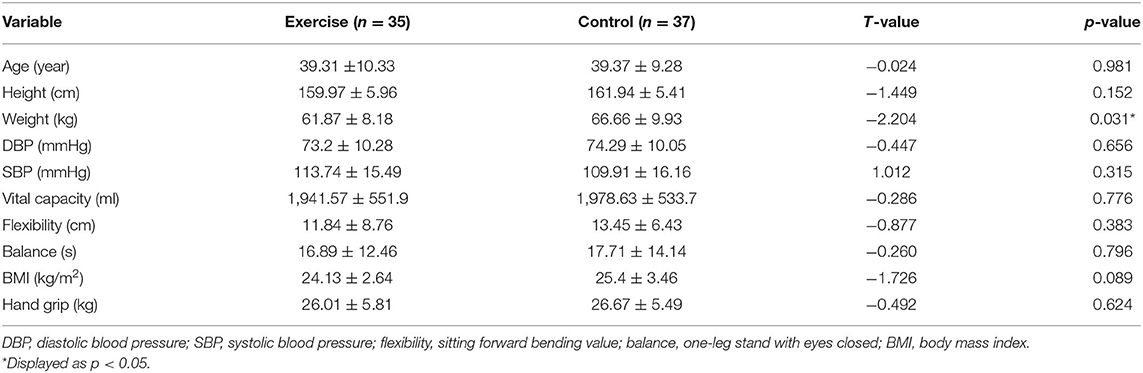
Table 1. Details of the anthropometric information and physical fitness parameters ( ± SD).
The exercise group performed a 40 min TC session thrice per week for 12 consecutive weeks. The TC intervention was conducted in the afternoon every Monday, Wednesday, and Friday in the SFMDRC. They were trained in TC, which was based on a simplified 24-form TC that included Ye Ma Feng Zong, Shou Hui Pi Ba, Dao Juan Hong, and other TC styles. Each session consisted of 5 min warm-up, 30 min TC exercise and 5 min cool-down. Participants in the exercise group were instructed by a professional TC instructor two sessions per week. The other session was instructed by a rehab administrator who had been trained for a certain time before the study. The exercise intensity of TC is around 4.5 METs (Metabolic Equivalent of Energy), and individual's heart rate is ~100/beat a session (67).
The control group was trained with conventional exercises, including the 9th Guang Bo Ti Cao and square dance, under the supervision of administrators. The Guang Bo Ti Cao was designed by the China General Administration of Sports, which was divided into eight sections lasting 5 min. The square dance is a moderate-intensity exercise based on the basic movements of aerobics. Each session in the control group involved muscle stretching as warm-up (5 min), square dance and two rounds of Guang Bo Ti Cao as the main intervention (30 min) and cool-down (5 min). The interventions of the two groups were conducted simultaneously in the SFMDRC with short breaks of <60 s and controlled by supervisors.
The go/no-go and switching tasks were selected in the study to assess the core EFs of IC and cognitive flexibility, as they were classic and widely used tasks in psychological studies (19). N-back task, which is often used to assess working memory, was also selected (70). The main analysis was focused on RT and accuracy results. All cognitive tasks were performed manually on a laptop using E-Prime 2.0 software.
The stimuli were positive (go stimuli) and inverted triangle (no-go stimuli) of the same size (7 × 7 cm) on a gray background placed at the center of the display (brightness set at 60 CD/m2). Subjects were instructed to press “F” on the keyboard when the positive triangle appeared as quickly and accurately as possible and to remain seated when the inverted triangle appeared. The stimuli were presented for 100 ms at random order followed by a blank screen with a duration of 1,500 ms. The whole procedure included 20 trials for exercise and 200 trials for the formal task. The accuracy and go RT data were recorded (Figure 2).
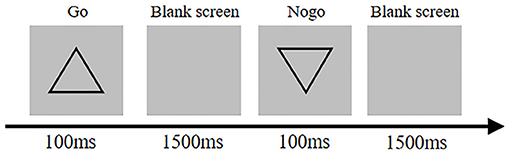
Figure 2. Go/no-go task diagram.
Each trial consisted of a fixation in the center of the screen for 500 ms, followed by 45 numbers presenting continuously for 500 ms with a duration of 2,500 ms. Subjects determined if the presented number matched the next-to-last letter and to respond as quickly and accurately as possible. The task included two conditions, namely, congruent (number matched) and incongruent (number does not match). A short practice trial was given before the formal trial began. The whole procedure comprised 20 trials. The accuracy and RT data were recorded (Figure 3).
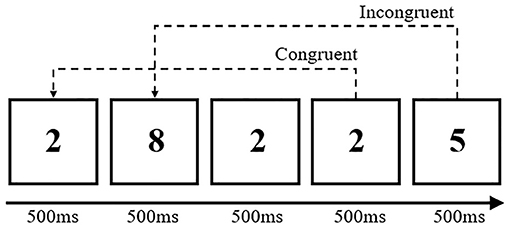
Figure 3. 3-back task diagram.
Each trial consisted of a fixation in the center of the screen for 500 ms. This was followed by a stimulus for 500 ms on the screen with an interval duration of 1,000 ms. When the color of the letter turned blue, subjects were instructed to determine whether the whole part (large letter) was S or H and then press the corresponding key (S or H). When the color of the letter appeared green, they were asked to determine whether the part (small letter) was S or H and then press the key (S or H). The formal task included nine sets of stimuli, each comprising 20 trials. The stimuli for each task were presented randomly, and the whole procedure comprised 240 trials. The RT of correct response data were recorded (Figure 4).

Figure 4. Switching task diagram.
Data were analyzed using SPSS version 25.0. The data for each task were expressed as mean ± SD. Preliminary analyses were conducted to ensure that participant factors did not differ between groups. Univariate analyses also examined whether the observed effects differed depending on participant's characteristics. For the 3-back task, the RTs (congruent and incongruent) and accuracy (congruent and incongruent) were analyzed using 2 (group: exercise vs. control) × 2 (time point: pre-test vs. post-test) repeated measures analysis of variance (ANOVA). The go RT, accuracy (go, no-go) in go/no-go task and RT in switching task were analyzed using repeated measures ANOVA. Physical fitness parameters assessed before and after exercise were analyzed using repeated measures ANOVA. The statistical significance was set at p < 0.05.
The analysis of accuracy revealed significant main effects of time [F(1, 68) = 9.6, p < 0.05, η2 = 0.12], condition [F(1, 68) = 43.4, p < 0.001, η2 = 0.39] and the interaction between time and condition [F(1, 68) = 20.52, p < 0.001, η2 = 0.23]. Post-hoc test showed that the overall post-test (97 ± 0.3%) accuracy was higher than the pre-test (96 ± 0.2%) accuracy and that the no-go accuracy (95 ± 0.5%) was significantly lower than the go accuracy (99 ± 0.3%). Simple effect analysis showed that the overall pre-test accuracy (94 ± 0.7%) under no-go condition was significantly lower than post-test accuracy (96 ± 0.4%, p < 0.01), but the accuracy under the go condition did not differ between time and condition (p > 0.05).
RT analysis revealed a significant main effect of time [F(1, 68) = 16.86, p < 0.001, η2 = 0.2]. Post-hoc test showed that post-test (408.23 ± 6.52 ms) RT was lower than pre-test (426.65 ± 6.45 ms) RT (Table 2 and Figure 5).

Table 2. Behavioral data for the go/no-go task in the exercise and control groups (mean ± SD).

Figure 5. Go response time of the go/no-go task in each group. **Displayed as p < 0.01.
The analysis of accuracy showed the significant main effects of time [F(1, 61) = 15.43, p < 0.001, η2 = 0.20], condition [F(1, 61) = 17.59, p < 0.001, η2 = 0.22] and an interaction between time and group [F(1, 61) = 4.73, p < 0.05, η2 = 0.07]. Post-hoc test showed that the post-test (37 ± 2.0%) accuracy was lower than the pre-test (45 ± 2.0%) accuracy and that the overall incongruent accuracy (46 ± 2.0%) was significantly higher than the congruent accuracy (36 ± 2.0%). Simple effect analysis showed that the overall post-test accuracy (35 ± 3.0%) of the control group was significantly lower than the pre-test accuracy (47 ± 2.0%) (Figures 6A,B).

Figure 6. (A) Congruent accuracy of the 3-back task in each group. (B) Incongruent accuracy of the 3-back task in each group. (C) Congruent response time of the 3-back task in each group. (D) Incongruent response time of the 3-back task in each group.
The analysis of RT revealed significant main effects of time [F(1, 61) = 4.66, p < 0.05, η2 = 0.07]. Post-hoc test showed that the overall post-test RT (622.73 ± 16.45 ms) was significantly higher than the pre-test RT (575.59 ± 20.68 ms) (Figures 6C,D). No other interaction effects were observed.
RT analysis showed no significant main effects of time and interaction between time and group (p > 0.05) (Table 3).

Table 3. RT of switch task in the exercise and control groups (mean ± SD).
Results of physical fitness parameter analysis indicated significant differences in the within-group factor in terms of systolic blood pressure [F(1, 68) = 6.105, p < 0.05, η2 = 0.082], vital capacity [F(1, 68) = 5.998, p < 0.05, η2 = 0.081] and BMI [F(1, 68) = 19.569, p < 0.05, η2 = 0.223] after 12 weeks of TC intervention. No significant difference was found between groups and interactions of group × time in systolic blood pressure, vital capacity and BMI (Table 4).
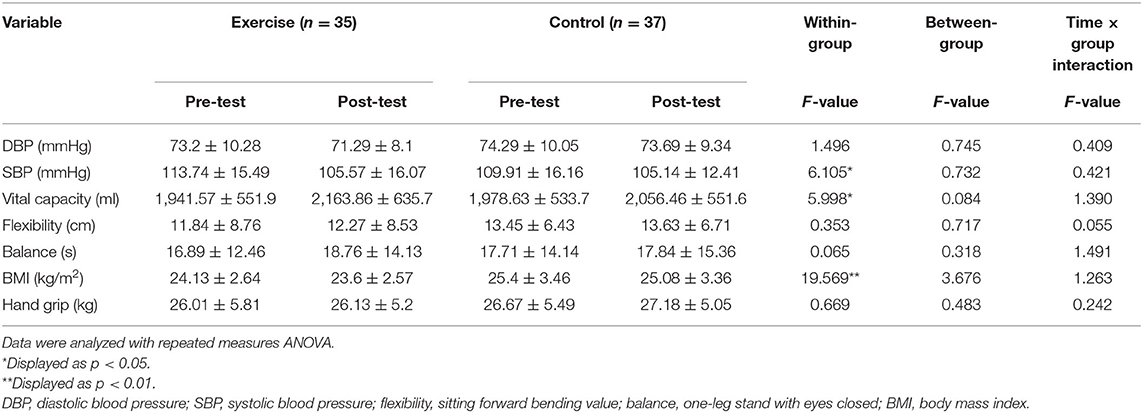
Table 4. Physical data in the two groups pre- and post-intervention (mean ± SD).
The present study provided the initial evidence on how TC training affects the EFs and physical fitness of MA dependents. The provision of a supervised TC training thrice per week for 3 months improved the IC of MA dependents. Meanwhile, their working memory and cognitive flexibility remained stable until the end of the intervention. Positive changes in blood pressure and vital capacity were also observed after 3 months of TC training.
EF deficits, such as response inhibition, decision making, and cognitive flexibility, were found in MA dependents (15, 71). The cognitive performances of illicit drug users can be recovered after a long period of abstinence (72). Meanwhile, exercise can reverse the neurological damage caused by drug dependence (72). The combination of exercise and pharmacological therapy, as an indispensable method of drug withdrawal management, exerted an overall positive effect on drug users (73, 74).
In the go/no-go task, higher accuracy was observed in the exercise group after the TC intervention under no-go condition, whereas lower accuracy was observed in the control group under the go condition in the post-test. Lower RT was found in the exercise group under the go condition in the post-test (Figure 5) compared with the control group.
The positive results in the exercise group were also similar to a previous study which reported that TC intervention can enhance individuals' IC and EF (62). Evidence proved that moderate-intensity aerobic exercise can enhance the executive control ability of both MA addicts and normal individuals (75, 76). TC was considered an integration exercise of aerobic exercise and cognitive training, which may exert more potential effects on executive cognitive ability (62). It was found through a brain research that TC exercise can activate the prefrontal cortex (PFC) and increase oxyhemoglobin and total hemoglobin in this brain region (77). This kind of enhanced brain activation was considered to be correlated with improved cognitive performances (62). Additionally, the effects of TC exercise on mind–body benefits were reportedly more significant than those of regular aerobic exercise (63). A dose–response relationship was also found between the length of TC training and the improvements in EF of individuals. Electrophysiological investigation showed that individuals who consistently participated in TC exercise showed better IC during EF tasks than those in the regular exercise and control groups (61). Therefore, MA dependents may receive facilitated IC through 12 weeks of TC training and may gain benefits from long-term TC training.
Although the literature showed evidence that exercise can ameliorate the working memory (78), the present study failed to discover positive changes through the 3-back task. The adverse trend of accuracy and RT in the control group was more obvious than that in the exercise group (Figure 6). Moreover, the exercise group maintained relatively stable levels of accuracy and RT. Previous studies also demonstrated the positive effects of TC on the working memory of normal older population (60). One possible mechanism explained by the researchers was that TC training enhances and activates the brain activity of individuals (77). The movement form of TC is characterized by repetition, similarity, complexity, and diversity. During TC practice, the route and name of each movement needed to be memorized repeatedly, which may require the utilization of the working memory of MA dependents. Therefore, TC training has the potential to stabilize and maintain working memory.
In previous studies, TC enhances individuals' switching function (79). One research found that individuals' overall cognitive function, processing speed and attention improved after TC intervention (60). Although no significant improvement was found in the present study, the post-test results of the control group showed higher RT compared with baseline and the exercise group, whereas a stable RT was observed in the exercise group. The cognitive flexibility of MA dependents can be well-maintained through TC training.
Exercise can improve the overall health and basic life quality of MA dependents (80) and is associated with notable improvements in cardiopulmonary health in individuals using MA (52). This study showed significant differences in systolic blood pressure and vital capacity in the exercise group, which was in accordance with many previous studies (81–84). TC exerted influence on the activity of parasympathetic nervous system and the sensitivity of baroreceptor, thereby leading to the positive change of blood pressure (85–87). The vital capacity of the exercise group increased from 1,941.57 ± 551.9 ml to 2,163.86 ± 635.7 ml. This result was similar to a previous study that found MA dependents showed remarkable improvements in vital capacity after moderate-intensity TC intervention (88, 89). TC exercise was also been suggested to normalized BMI in MA users (66). Similarly, decreased BMI was found in the exercise group in the current study, which was the same as the findings of a previous TC intervention study (90).
The duration of one-leg stand with eyes closed increased in the exercise group compared with baseline, which was similar to the finding of another study (54). The fact that TC can improve balance ability for all kinds of people has been proved by many researchers (91, 92). Although no significant differences were found in balance ability, the prolonged standing time indicated that TC had the tendency and potential to improve the balance ability of MA dependents. No significant change in flexibility was observed between the two groups, which was different from the finding that suggest long-term TC practice can increase flexibility (54). However, the improved flexibility found in this study was achieved from 1-year TC intervention, which was longer than the duration used in the current study. Therefore, insufficient duration of intervention may explain the results of our study.
Numerous studies confirmed the benefits of aerobic exercise on cognitive function (93, 94). The present study showed that TC maintained and improved EFs of MA dependents to some extent. The general mechanism can be explained as follows: Exercise increased the concentration of brain-derived neurotrophic factor (BDNF) (95, 96), which is an important substance that causes neuroplasticity in the brain (96). Exercise training interventions can improve BDNF levels in healthy adults (97, 98), and BDNF has long been implicated in cognition (99). The training-induced BDNF changes reportedly induce cognitive improvement through hippocampal and peripheral levels in humans (99). A neurophysiological study showed that TC improves individuals' memory and other component of EF possibly via the upregulation of BDNF (79). Second, MA can cause reduction in striatal and cortical cerebral blood flow via dopamine receptor D2 (124) (100), and the blood-brain barrier of individuals can be impaired under the induction of MA (101). However, several studies proved that exercise attenuated MA-induced alterations in neurogenesis and oxidative stress in brain microvessels and protected against blood-brain barrier impairment (102, 103). The neurophysiological effects of exercise to improve blood flow, neurotransmitter levels and brain health have all been proved by evidences (104). This may be the possible mechanism by which TC maintain the EFs of MA dependents in a steadier status. Additionally, as a mind-body exercise, the mindfulness during exercise may influence the brain region involving EFs, such as the anterior cingulate cortex, which is intensely activated during exercise (105). The improvement in EF may due to the neurological flexibility or structural and functional changes in the brain caused by mindfulness practices (106). Additionally, research suggested that long-term TC exercise may contribute to the neural substrates of EF (107).
Therefore, we infer that the improvement of EFs in MA dependents with cognitive deficits may be affected by the combination of the mechanism mentioned above. However, further studies are still necessary to clarify the mechanism.
This study has several limitations. First, participants were all managed by administrators in the drug rehabilitation center. Thus, the blinding of the study may be affected by the relationship between administrator (intervention supervisor) and participants, as they may already know the supervisor. Second, although the general exercise intensity of TC was mentioned in the study, tools or instruments were not used to monitor the exercise intensity of participants in the current study, which may influence the experimental results. Additionally, the use of prolonged intervention duration will add reliability to make up the current study's limitation of having a relative short intervention period. The baseline test on detailed information (e.g., use of drug type, year of drug use, and duration of abstinence before the study) will address the limitation in future studies. The effect of TC exercise on male drug users to enrich the research field can be the focus of future studies, instead of concentrating on females only.
Three months of moderate-intensity TC exercise improved the IC, maintained working memory and cognitive flexibility of EFs and ameliorated the physical function of female MA dependents. TC was an effective exercise intervention for drug users. However, some changes of EF parameters were not remarkable, which may be due to the short intervention time. Thus, the long-term effects of TC on EF should be explored in the future.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by The Institutional Review Board of Shanghai University of Sport. The patients/participants provided their written informed consent to participate in this study.
SM participated in the design of the study and drafted the manuscript. LR conducted the design of the study, exercise intervention, and partial manuscript writing. ZD participated in the design of this study, coordination of intervention conducted in Shanghai detoxification, and rehabilitation center. YS participated in manuscript revision and study design. All authors read and approved the final manuscript.
This work was supported by the Shanghai Municipal Science and Technology Commission (19080503200) and National Key Research and Development (2018YFC0807405). The funding sponsors (Shanghai Municipal Science and Technology Commission, 19080503200; National Key Research and Development, 2018YFC0807405) were not involved in the study design, collection, analysis, and interpretation of data in the writing of the report.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Glasner-Edwards S, Mooney LJ, Marinelli-Casey P, Hillhouse M, Ang A, Rawson R. Clinical course and outcomes of methamphetamine-dependent adults with psychosis. J Subst Abuse Treat. (2008) 35:445–50. doi: 10.1016/j.jsat.2007.12.004
2. Siefried KJ, Acheson LS. Pharmacological treatment of methamphetamine/amphetamine dependence: a systematic review. CNS Drugs. (2020) 34:337–65. doi: 10.1007/s40263-020-00711-x
3. Kohno M, Beste C, Pilhatsch M. Editorial: the global methamphetamine problem: approaches to elucidate the neurobiology, epidemiology, therapeutic effectiveness. Front Psychiatry. (2020) 11:850. doi: 10.3389/fpsyt.2020.00850
4. Hussen SA, Camp DM, Jones MD, Patel SA, Crawford ND, Holland DP, et al. Exploring influences on methamphetamine use among Black gay, bisexual and other men who have sex with men in Atlanta: a focus group study. Int J Drug Policy. (2021) 90:103094. doi: 10.1016/j.drugpo.2020.103094
6. Office of China National Narcotics Control Commission Publication OoCNNCC. China's Drug Situation Report. (2019). Available online at: http://www.nncc626.com/2020-06/24/c_1210675813.htm (accessed June 24, 2020).
7. Gonzales R, Mooney L, Rawson RA. The methamphetamine problem in the United States. Annu Rev Public Health. (2010) 31:385–98. doi: 10.1146/annurev.publhealth.012809.103600
8. Marshall BD, Werb D. Health outcomes associated with methamphetamine use among young people: a systematic review. Addiction. (2010) 105:991–1002. doi: 10.1111/j.1360-0443.2010.02932.x
9. McKetin R, Kelly E, McLaren J, Proudfoot H. Impaired physical health among methamphetamine users in comparison with the general population: the role of methamphetamine dependence and opioid use. Drug Alcohol Rev. (2008) 27:482–9. doi: 10.1080/09595230801914776
10. Varner KJ, Ogden BA, Delcarpio J, Meleg-Smith S. Cardiovascular responses elicited by the “binge” administration of methamphetamine. J Pharmacol Exp Ther. (2002) 301:152–9. doi: 10.1124/jpet.301.1.152
11. Anglin MD, Burke C, Perrochet B, Stamper E, Dawud-Noursi S. History of the methamphetamine problem. J Psychoactive Drugs. (2000) 32:137–41. doi: 10.1080/02791072.2000.10400221
12. Darke S, Kaye S, McKetin R, Duflou J. Major physical and psychological harms of methamphetamine use. Drug Alcohol Rev. (2008) 27:253–62. doi: 10.1080/09595230801923702
13. Belcher AM, O'dell SJ, Marshall JF. Long-term changes in dopamine-stimulated gene expression after single-day methamphetamine exposure. Synapse. (2009) 63:403–12. doi: 10.1002/syn.20617
14. Panenka WJ, Procyshyn RM, Lecomte T, MacEwan GW, Flynn SW, Honer WG, et al. Methamphetamine use: a comprehensive review of molecular, preclinical and clinical findings. Drug Alcohol Depend. (2013) 129:167–79. doi: 10.1016/j.drugalcdep.2012.11.016
15. Scott JC, Woods SP, Matt GE, Meyer RA, Heaton RK, Atkinson JH, et al. Neurocognitive effects of methamphetamine: a critical review and meta-analysis. Neuropsychol Rev. (2007) 17:275–97. doi: 10.1007/s11065-007-9031-0
16. Feil J, Sheppard D, Fitzgerald PB, Yücel M, Lubman DI, Bradshaw JL. Addiction, compulsive drug seeking, and the role of frontostriatal mechanisms in regulating inhibitory control. Neurosci Biobehav Rev. (2010) 35:248–75. doi: 10.1016/j.neubiorev.2010.03.001
17. Lehto JE, Juujarvi P, Kooistra L, Pulkkinen L. Dimensions of executive functioning: evidence from children. Br J Dev Psychol. (2003) 21:59. doi: 10.1348/026151003321164627
18. Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: a latent variable analysis. Cogn Psychol. (2000) 41:49–100. doi: 10.1006/cogp.1999.0734
19. Diamond A. Executive functions. Annu Rev Psychol. (2013) 64:135–68. doi: 10.1146/annurev-psych-113011-143750
20. Harris M, Penfold RB, Hawkins A, Maccombs J, Wallace B, Reynolds B. Dimensions of impulsive behavior and treatment outcomes for adolescent smokers. Exp Clin Psychopharmacol. (2014) 22:57–64. doi: 10.1037/a0034403
21. Hess ARB, Menezes CB, Almeida RMM. Inhibitory control and impulsivity levels in women crack users. (2018) 53:972–9. doi: 10.1080/10826084.2017.1387568
22. Jones HW, Dean AC, Price KA, London ED. Increased self-reported impulsivity in methamphetamine users maintaining drug abstinence. Am J Drug Alcohol Abuse. (2016) 42:500–6. doi: 10.1080/00952990.2016.1192639
23. Kale D, Stautz K, Cooper A. Impulsivity related personality traits and cigarette smoking in adults: a meta-analysis using the UPPS-P model of impulsivity and reward sensitivity. Drug Alcohol Depend. (2018) 185:149–67. doi: 10.1016/j.drugalcdep.2018.01.003
24. Mashhoon Y, Betts J, Farmer SL, Lukas SE. Early onset tobacco cigarette smokers exhibit deficits in response inhibition and sustained attention. Drug Alcohol Depend. (2018) 184:48–56. doi: 10.1016/j.drugalcdep.2017.11.020
25. Moallem NR, Courtney KE, Ray LA. The relationship between impulsivity and methamphetamine use severity in a community sample. Drug Alcohol Depend. (2018) 187:1–7. doi: 10.1016/j.drugalcdep.2018.01.034
26. Potvin S, Stavro K, Rizkallah E, Pelletier J. Cocaine and cognition: a systematic quantitative review. J Addict Med. (2014) 8:368–76. doi: 10.1097/ADM.0000000000000066
27. Smitha JL, Matticka RP, Jamadarb J, Iredalead JM. Deficits in behavioural inhibition in substance abuse and addiction: a meta-analysis. Drug Alcohol Depend. (2014) 145:1–33. doi: 10.1016/j.drugalcdep.2014.08.009
28. Baicy K, London ED. Corticolimbic dysregulation and chronic methamphetamine abuse. Addiction. (2007) 102(Suppl. 1):5–15. doi: 10.1111/j.1360-0443.2006.01777.x
29. Baler RD, Volkow ND. Drug addiction: the neurobiology of disrupted self-control. Trends Mol Med. (2006) 12:559–66. doi: 10.1016/j.molmed.2006.10.005
30. Garavan H, Weierstall K. The neurobiology of reward and cognitive control systems and their role in incentivizing health behavior. Prev Med. (2012) 55:S17–23. doi: 10.1016/j.ypmed.2012.05.018
31. Volkow ND, Li TK. Drug addiction: the neurobiology of behaviour gone awry. Nat Rev Neurosci. (2004) 5:963–70. doi: 10.1038/nrn1539
32. Dong G, Zhou H, Zhao X. Male Internet addicts show impaired executive control ability: evidence from a color-word Stroop task. Neurosci Lett. (2011) 499:114–8. doi: 10.1016/j.neulet.2011.05.047
33. Fehr T, Wiedenmann P, Herrmann M. Nicotine Stroop and addiction memory–an ERP study. Int J Psychophysiol. (2006) 62:224–32. doi: 10.1016/j.ijpsycho.2006.01.011
34. Field M, Christiansen P, Cole J, Goudie A. Delay discounting and the alcohol Stroop in heavy drinking adolescents. Addiction. (2007) 102:579–86. doi: 10.1111/j.1360-0443.2007.01743.x
35. Hester R, Dixon V, Garavan H. A consistent attentional bias for drug-related material in active cocaine users across word and picture versions of the emotional Stroop task. Drug Alcohol Depend. (2006) 81:251–7. doi: 10.1016/j.drugalcdep.2005.07.002
36. Lusher J, Chandler C, Ball D. Alcohol dependence and the alcohol Stroop paradigm: evidence and issues. Drug Alcohol Depend. (2004) 75:225–31. doi: 10.1016/j.drugalcdep.2004.03.004
38. Bechara A, Martin EM. Impaired decision making related to working memory deficits in individuals with substance addictions. Neuropsychology. (2004) 18:152–62. doi: 10.1037/0894-4105.18.1.152
39. Mizoguchi H, Yamada K. Methamphetamine use causes cognitive impairment and altered decision-making. Neurochem Int. (2019) 124:106–13. doi: 10.1016/j.neuint.2018.12.019
40. Abrantes AM, Blevins CE. Exercise in the context of substance use treatment: key issues and future directions. Curr Opin Psychol. (2019) 30:103–8. doi: 10.1016/j.copsyc.2019.04.001
41. Lynch WJ, Peterson AB, Sanchez V, Abel J, Smith MA. Exercise as a novel treatment for drug addiction: a neurobiological and stage-dependent hypothesis. Neurosci Biobehav Rev. (2013) 37:1622–44. doi: 10.1016/j.neubiorev.2013.06.011
42. Northey JM, Cherbuin N. Exercise interventions for cognitive function in adults older than 50: a systematic review with meta-analysis. Br J Sports Med. (2018) 52:154–60. doi: 10.1136/bjsports-2016-096587
43. Ziereis S, Jansen P. Effects of physical activity on executive function and motor performance in children with ADHD. Res Dev Disabil. (2015) 38:181–91. doi: 10.1016/j.ridd.2014.12.005
44. Verburgh L, Königs M, Scherder EJA, Oosterlaan J. Physical exercise and executive functions in preadolescent children, adolescents and young adults: a meta-analysis. Br J Sports Med. (2014) 48:973–9. doi: 10.1136/bjsports-2012-091441
45. Akatsuka K, Yamashiro K, Nakazawa S, Mitsuzono R, Maruyama A. Acute aerobic exercise influences the inhibitory process in the go/no-go task in humans. Neurosci Lett. (2015) 600:80–4. doi: 10.1016/j.neulet.2015.06.004
46. Memarmoghaddam M, Torbati HT, Sohrabi M, Mashhadi A, Kashi A. Effects of a selected exercise programon executive function of children with attention deficit hyperactivity disorder. J Med Life. (2016) 9:373–9.
47. Wang D, Zhou C, Chang Y-K. Acute exercise ameliorates craving and inhibitory deficits in methamphetamine: an ERP study. Physiol Behav. (2015) 147:38–46. doi: 10.1016/j.physbeh.2015.04.008
48. Cragg L, Nation K. Go or no-go? Developmental improvements in the efficiency of response inhibition in mid-childhood. Dev Sci. (2008) 11:819–27. doi: 10.1111/j.1467-7687.2008.00730.x
49. Moriya M, Aoki C, Sakatani K. Effects of physical exercise on working memory and prefrontal cortex function in post-stroke patients. Adv Exp Med Biol. (2016) 923:203–8. doi: 10.1007/978-3-319-38810-6_27
50. Smith M, Tallis J, Miller A, Clarke ND, Guimarães-Ferreira L, Duncan MJ. The effect of exercise intensity on cognitive performance during short duration treadmill running. J Hum Kinet. (2016) 51:27–35. doi: 10.1515/hukin-2015-0167
51. Wang D, Zhou C, Zhao M, Wu X, Chang YK. Dose-response relationships between exercise intensity, cravings, and inhibitory control in methamphetamine dependence: an ERPs study. Drug Alcohol Depend. (2016) 161:331–9. doi: 10.1016/j.drugalcdep.2016.02.023
52. Morris L, Stander J, Ebrahim W, Eksteen S, Meaden OA, Ras A, et al. Effect of exercise versus cognitive behavioural therapy or no intervention on anxiety, depression, fitness and quality of life in adults with previous methamphetamine dependency: a systematic review. Addict Sci Clin Pract. (2018) 13:4. doi: 10.1186/s13722-018-0106-4
53. Giménez-Meseguer J, Tortosa-Martínez J, Cortell-Tormo JM. The benefits of physical exercise on mental disorders and quality of life in substance use disorders patients. Systematic review and meta-analysis. Int J Environ Res Public Health. (2020) 17:3680. doi: 10.3390/ijerph17103680
54. Yanguang Y, Jingyi C, XiaoWu P, Menglu S, Suyong Y, Ding X., et al. Comparison of physical effect between two training methods for individuals with substance use disorder. BMC Sports Sci Med Rehabil. (2021) 13:1–11. doi: 10.1186/s13102-021-00234-y
55. Bock BC, Marcus BH, King TK, Borrelli B, Roberts MR. Exercise effects on withdrawal and mood among women attempting smoking cessation. Addict Behav. (1999) 24:399–410. doi: 10.1016/S0306-4603(98)00088-4
56. Taylor AH, Ussher MH, Faulkner G. The acute effects of exercise on cigarette cravings, withdrawal symptoms, affect and smoking behaviour: a systematic review. Addiction. (2007) 102:534–43. doi: 10.1111/j.1360-0443.2006.01739.x
57. Bherer L, Erickson KI, Liu-Ambrose T. A review of the effects of physical activity and exercise on cognitive and brain functions in older adults. J Aging Res. (2013) 2013:1–8. doi: 10.1155/2013/657508
58. Loprinzi PD, Herod SM, Cardinal BJ, Noakes TD. Physical activity and the brain: a review of this dynamic, bi-directional relationship. Brain Res. (2013) 1539:95–104. doi: 10.1016/j.brainres.2013.10.004
59. Miller SM, Taylor-Piliae RE. Effects of Tai Chi on cognitive function in community-dwelling older adults: a review. Geriatr Nurs. (2014) 35:9–19. doi: 10.1016/j.gerinurse.2013.10.013
60. Wu Y, Wang Y, Burgess EO, Wu J. The effects of Tai Chi exercise on cognitive function in older adults: a meta-analysis. J Sport Health Sci. (2013) 2:193–203. doi: 10.1016/j.jshs.2013.09.001
61. Chen C-Y, Muggleton NG. Electrophysiological investigation of the effects of Tai Chi on inhibitory control in older individuals. Prog Brain Res. (2020) 253:229–42. doi: 10.1016/bs.pbr.2020.05.031
62. Yang Y, Chen T, Shao M, Yan S, Yue GH, Jiang C. Effects of Tai Chi Chuan on inhibitory control in elderly women: an fNIRS study. Front Hum Neurosci. (2019) 13:476. doi: 10.3389/fnhum.2019.00476
63. Chenchen W, Schmid CH, Fielding RA, Harvey WF, Reid KF, Price LL, et al. Effect of tai chi versus aerobic exercise for fibromyalgia: comparative effectiveness randomized controlled trial. BMJ. (2018) 360:k851. doi: 10.1136/bmj.k851
64. Li H, Chen J, Xu G, Duan Y, Huang D, Tang C, et al. The effect of Tai Chi for improving sleep quality: a systematic review and meta-analysis. J Affect Disord. (2020) 274:1102–12. doi: 10.1016/j.jad.2020.05.076
65. Webster CS, Luo AY, Krägeloh C, Moir F, Henning M. A systematic review of the health benefits of Tai Chi for students in higher education. Prev Med Rep. (2016) 3:103–12. doi: 10.1016/j.pmedr.2015.12.006
66. Zhu D, Jiang M, Xu D, Schollhorn WI. Long-term effects of mind-body exercises on the physical fitness and quality of life of individuals with substance use disorder-a randomized trial. Front Psychiatry. (2020) 11:528373. doi: 10.3389/fpsyt.2020.528373
67. Zhu D, Xu D, Dai G, Wang F, Xu X, Zhou D. Beneficial effects of Tai Chi for amphetamine-type stimulant dependence: a pilot study. Am J Drug Alcohol Abuse. (2016) 42:469–78. doi: 10.3109/00952990.2016.1153646
68. Liu F, Cui J, Liu X, Chen KW, Chen X, Li R. The effect of tai chi and Qigong exercise on depression and anxiety of individuals with substance use disorders: a systematic review and meta-analysis. BMC Complement Med Ther. (2020) 20:161. doi: 10.1186/s12906-020-02967-8
69. Wang D, Wang Y, Wang Y, Li R, Zhou C. Impact of physical exercise on substance use disorders: a meta-analysis. PLoS ONE. (2014) 9:e110728. doi: 10.1371/journal.pone.0110728
70. Owen AM, McMillan KM, Laird AR, Bullmore E. N-back working memory paradigm: a meta-analysis of normative functional neuroimaging studies. Hum Brain Mapp. (2005) 25:46–59. doi: 10.1002/hbm.20131
71. Plas EAA, Crone EA, Wildenberg WPM, Tranel D, Bechara A. Executive control deficits in substance-dependent individuals: a comparison of alcohol, cocaine, and methamphetamine and of men and women. J Clin Exp Neuropsychol. (2009) 31:706–19. doi: 10.1080/13803390802484797
72. Schilt T, Win MML, Jager G, Koeter MW, Ramsey NF, Schmand B, et al. Specific effects of ecstasy and other illicit drugs on cognition in poly-substance users. Psychol Med. (2007) 38:1309–17. doi: 10.1017/S0033291707002140
73. Ashdown-Franks G, Firth J, Carney R, Carvalho AF, Hallgren M, Koyanagi A, et al. Exercise as medicine for mental and substance use disorders: a meta-review of the benefits for neuropsychiatric and cognitive outcomes. Sports Med. (2020) 50:151–70. doi: 10.1007/s40279-019-01187-6
74. Linke SE, Ussher M. Exercise-based treatments for substance use disorders: evidence, theory, and practicality. Am J Drug Alcohol Abuse. (2015) 41:7–15. doi: 10.3109/00952990.2014.976708
75. Hao R, Jia-ning L, Xu-dong L, Cheng-lin Z, Yi-fan C. A study of the brain mechanism of aerobic exercise improving the execution control ability of methamphetamine addicts. J Phys Educ. (2019) 26:7. doi: 10.16237/j.cnki.cn44-1404/g8.2019.03.019
76. Yanagisawa H, Dan I, Tsuzuki D, Kato M, Okamoto M, Kyutoku Y, et al. Acute moderate exercise elicits increased dorsolateral prefrontal activation and improves cognitive performance with Stroop test. Neuroimage. (2010) 50:1702–10. doi: 10.1016/j.neuroimage.2009.12.023
77. Tsang WWN, Chan KK, Cheng CN, Hu FSF, Mak CTK, Wong JWC. Tai Chi practice on prefrontal oxygenation levels in older adults: a pilot study. Complement Ther Med. (2019) 42:132–6. doi: 10.1016/j.ctim.2018.11.005
78. Imboden C, Gerber M, Beck J, Holsboer-Trachsler E, Pühse U, Hatzinger M. Aerobic exercise or stretching as add-on to inpatient treatment of depression: similar antidepressant effects on depressive symptoms and larger effects on working memory for aerobic exercise alone. J Affect Disord. (2020) 276:866–76. doi: 10.1016/j.jad.2020.07.052
79. Sungkarat S, Boripuntakul S, Kumfu S, Lord SR, Chattipakorn N. Tai Chi improves cognition and plasma BDNF in older adults with mild cognitive impairment: a randomized controlled trial. Neurorehabil Neural Repair. (2018) 32:142–9. doi: 10.1177/1545968317753682
80. Jiakuan W, Chenglin Z, Jia H, Witchalls J, Waddington G. Can methamphetamine-dependent individuals improve fitness and quality of life through aerobic exercise? J Sci Med Sport. (2019) 22:S35. doi: 10.1016/j.jsams.2019.08.204
81. Chan AWK, Chair SY, Lee DTF, Leung DYP, Sit JWH, Cheng HY, et al. Tai Chi exercise is more effective than brisk walking in reducing cardiovascular disease risk factors among adults with hypertension: a randomised controlled trial. Int J Nurs Stud. (2018) 88:44–52. doi: 10.1016/j.ijnurstu.2018.08.009
82. Leung LY, Chan AW, Sit JW, Liu T, Taylor-Piliae RE. Tai Chi in Chinese adults with metabolic syndrome: a pilot randomized controlled trial. Complement Ther Med. (2019) 46:54–61. doi: 10.1016/j.ctim.2019.07.008
83. Park JA, Kim SY. Effects of Tai Chi exercise on physical fitness and quality of life in elderly women. Korean J Rehabil Nurs. (2014) 17:38–47. doi: 10.7587/kjrehn.2014.38
84. Zhang Y, Han P, Yin N, Huang Y, Li C, Lian H, et al. The effects of long-term Tai-Chi practice on blood pressure under normal conditions. Am J Med Sci. (2020) S0002-9629(20)30494-8. doi: 10.1016/j.amjms.2020.11.008
85. Floras JS, Wesche J. Haemodynamic contributions to post-exercise hypotension in young adults with hypertension and rapid resting heart rates. J Hum Hypertens. (1992) 6:265–9.
86. Maris SA, Winter CR, Paolone VJ, Headley SAE. Comparing the changes in blood pressure after acute exposure to Tai Chi and walking. Int J Exerc Sci. (2019) 12:77–87.
87. Motivala SJ, Sollers J, Thayer J, Irwin MR. Tai Chi Chih acutely decreases sympathetic nervous system activity in older adults. J Gerontol A Biol Sci Med Sci. (2006) 61:1177–80. doi: 10.1093/gerona/61.11.1177
88. Kantatong T, Panpanich R, Deesomchok A, Sungkarat S, Siviroj P. Effects of the tai chi qigong programme on functional capacity, and lung function in chronic obstructive pulmonary disease patients: a ramdomised controlled trial. J Tradit Complement Med. (2020) 10:354–9. doi: 10.1016/j.jtcme.2019.03.008
89. Reychler G, Poncin W, Montigny S, Luts A, Caty G, Pieters T. Efficacy of yoga, tai chi and qi gong on the main symptoms of chronic obstructive pulmonary disease: a systematic review. Respir Med Res. (2019) 75:13–25. doi: 10.1016/j.resmer.2019.04.002
90. Hui SS, Xie YJ, Woo J, Kwok TC. Practicing Tai Chi had lower energy metabolism than walking but similar health benefits in terms of aerobic fitness, resting energy expenditure, body composition and self-perceived physical health. Complement Ther Med. (2016) 27:43–50. doi: 10.1016/j.ctim.2016.05.006
91. Scianni A. Tai Chi improves balance and prevents falls in people with Parkinson's disease. J Physiother. (2015) 61:44. doi: 10.1016/j.jphys.2014.11.008
92. Zhong D, Xiao Q, Xiao X, Li Y, Ye J, Xia L, et al. Tai Chi for improving balance and reducing falls: an overview of 14 systematic reviews. Ann Phys Rehabil Med. (2020) 63:505–17. doi: 10.1016/j.rehab.2019.12.008
93. Bahdur K, Gilchrist R, Park G, Nina L, Pruna R. Effect of HIIT on cognitive and physical performance. Apunts Med l'Esport. (2019) 54:113–7. doi: 10.1016/j.apunts.2019.07.001
94. Loprinzi PD, Frith E, Edwards MK, Sng E, Ashpole N. The effects of exercise on memory function among young to middle-aged adults: systematic review and recommendations for future research. Am J Health Promot. (2018) 32:691–704. doi: 10.1177/0890117117737409
95. Huang T, Larsen KT, Ried-Larsen M, Møller NC, Andersen LB. The effects of physical activity and exercise on brain-derived neurotrophic factor in healthy humans: a review. Scand J Med Sci Sports. (2014) 24:1–10. doi: 10.1111/sms.12069
96. Knaepen K, Goekint M, Heyman EM, Meeusen R. Neuroplasticity—exercise-induced response of peripheral brain-derived neurotrophic factor: a systematic review of experimental studies in human subjects. Sports Med. (2010) 40:765–801. doi: 10.2165/11534530-000000000-00000
97. Abbasian S, Ravasib AA. The effect of antecedent-conditioning high-intensity interval training on BDNF regulation through PGC-1α pathway following cerebral ischemia. Brain Res. (2020) 1729:146618. doi: 10.1016/j.brainres.2019.146618
98. Dinoff A, Herrmann N, Swardfager W, Lanctôt KL. The effect of acute exercise on blood concentrations of brain-derived neurotrophic factor in healthy adults: a meta-analysis. Eur J Neurosci. (2017) 46:1635–46. doi: 10.1111/ejn.13603
99. Leckie RL, Oberlin LE, Voss MW, Prakash RS, Szabo-Reed A, Chaddock-Heyman L, et al. BDNF mediates improvements in executive function following a 1-year exercise intervention. Front Hum Neurosci. (2014) 8:985. doi: 10.3389/fnhum.2014.00985
100. Chung YA, Peterson BS, Yoon SJ, Cho SN, Chai S, Jeong J, et al. In vivo evidence for long-term CNS toxicity, associated with chronic binge use of methamphetamine. Drug Alcohol Depend. (2010) 111:155–60. doi: 10.1016/j.drugalcdep.2010.04.005
101. Małkiewicz MA, Małecki A, Toborek M, Szarmach A, Winklewski PJ. Substances of abuse and the blood brain barrier: interactions with physical exercise. Neurosci Biobehav Rev. (2020) 119:204–16. doi: 10.1016/j.neubiorev.2020.09.026
102. Park M, Levine H, Toborek M. Exercise protects against methamphetamine-induced aberrant neurogenesis. Sci Rep. (2016) 6:34111. doi: 10.1038/srep34111
103. Toborek M, Seelbach MJ, Rashid CS, András IE, Chen L, Park M, et al. Voluntary exercise protects against methamphetamine-induced oxidative stress in brain microvasculature and disruption of the blood-brain barrier. Mol Neurodegener. (2013) 8:22. doi: 10.1186/1750-1326-8-22
105. Hölzel BK, Ott U, Hempel H, Hackl A, Wolf K, Stark R, et al. Differential engagement of anterior cingulate and adjacent medial frontal cortex in adept meditators and non-meditators. Neurosci Lett. (2007) 421:16–21. doi: 10.1016/j.neulet.2007.04.074
106. Tang Y-Y, Posner MI. Tools of the trade: theory and method in mindfulness neuroscience. Soc Cogn Affect Neurosci. (2013) 8:118–. doi: 10.1093/scan/nss112
Keywords: Tai Chi, methamphetamine, executive function, physical fitness, inhibitory control
Citation: Menglu S, Ruiwen L, Suyong Y and Dong Z (2021) Effects of Tai Chi on the Executive Function and Physical Fitness of Female Methamphetamine Dependents: A Randomized Controlled Trial. Front. Psychiatry 12:653229. doi: 10.3389/fpsyt.2021.653229
Received: 14 January 2021; Accepted: 22 April 2021;
Published: 10 June 2021.
Edited by:
Human Friedrich Unterrainer, University of Vienna, AustriaReviewed by:
Lisza Gaiswinkler, Pension Insurance Authority Austria, Rehabilitation Center Bad Aussee, AustriaCopyright © 2021 Menglu, Ruiwen, Suyong and Dong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhu Dong, emh1ZG9uZ0BzdXMuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.