
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry, 07 June 2021
Sec. Neuroimaging
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.646569
This article is part of the Research TopicNeural Bases of Neurological and Psychiatric Disorders and Their Neuromodulation TreatmentsView all 36 articles
 Clément Dondé1,2,3*
Clément Dondé1,2,3* Jerome Brunelin4,5,6
Jerome Brunelin4,5,6 Jean-Arthur Micoulaud-Franchi7,8
Jean-Arthur Micoulaud-Franchi7,8 Julia Maruani9,10,11
Julia Maruani9,10,11 Michel Lejoyeux12,13
Michel Lejoyeux12,13 Mircea Polosan1,2,3
Mircea Polosan1,2,3 Pierre A. Geoffroy12,13,14
Pierre A. Geoffroy12,13,14Transcranial Electrical Stimulation (tES) is a promising non-invasive brain modulation tool. Over the past years, there have been several attempts to modulate sleep with tES-based approaches in both the healthy and pathological brains. However, data about the impact on measurable aspects of sleep remain scattered between studies, which prevent us from drawing firm conclusions. We conducted a systematic review of studies that explored the impact of tES on neurophysiological sleep oscillations, sleep patterns measured objectively with polysomnography, and subjective psychometric assessments of sleep in both healthy and clinical samples. We searched four main electronic databases to identify studies until February 2020. Forty studies were selected including 511 healthy participants and 452 patients. tES can modify endogenous brain oscillations during sleep. Results concerning changes in sleep patterns are conflicting, whereas subjective assessments show clear improvements after tES. Possible stimulation-induced mechanisms within specific cortico-subcortical sleep structures and networks are discussed. Although these findings cannot be directly transferred to the clinical practice and sleep-enhancing devices development for healthy populations, they might help to pave the way for future researches in these areas. PROSPERO registration number 178910.
Sleep plays a vital role in well-being and good health throughout life. It is essential for many brain processes including the consolidation of memories (1, 2), alertness, processing speed, and decision-making (3). Healthy regulation of these processes by sleep has a significant relationship with scores of quality of life and global functioning (4). Sleep disorders, as medically defined, have significant public health implications, with insomnia complaints reported by nearly one third of the general population, and excessive daytime sleepiness affecting up to one fourth (5). In addition, it has been demonstrated that alteration of sleep is a marker of risk for numerous physical and mental disorders (6, 7). Abnormal fluctuations in sleep duration and efficiency (8–10), regularity of sleep cycle (11), subjective sleep quality (12), attentive wakefulness (13), and timing of sleep (14) are associated with greater risk of adverse general health outcomes including death. More specifically, sleep disruptions are associated with higher risk of diabetes, stroke, coronary heart disease and heart attack (10, 15), obesity (16), as well as mental disorders (7). Moreover, sleep complaints are often integral and important parts of a large range of diagnosed chronic medical conditions (17, 18).
Several tools have been developed to measure and assess objective and subjective aspects of sleep. Electroencephalography (EEG) studies have provided numerous indicators of the sleep course and quality. For instance, slow-wave oscillations have been demonstrated as accurate indexes of sleep homeostasis (19). In parallel, sleep patterns including architecture, timing, and stages differentiation can be measured with standardized polysomnography. Finally, several psychometric rating scales and brief interviews have been validated to assess subjective aspects of sleep and are widely used in clinical trials as main outcomes (20).
The functioning of brain areas and networks can be modified by applying electrical currents over the scalp. To modulate brain activity and eventually restore altered functions, transcranial Electrical Stimulation (tES) has recently emerged as a non-invasive painless brain modulation tool that involves the application of a weak (0.5–2 mA) current via two scalp electrodes (a cathode and an anode) overlying targeted cortical areas (21, 22). The electrical current flowing between the electrodes induces changes in neuronal excitability and activity through specific molecular mechanisms that mediate synaptic plasticity (23). tES studies have traditionally used direct current modalities for stimulation (tDCS: transcranial direct stimulation), where a constant unidirectional low current flows inward under the anode and outward under the cathode. Besides, other stimulation modalities have been developed for tES involving random noise frequencies (tRNS) or alternating (tACS) patterns of the current (24, 25). In healthy samples, an increasing number of studies have reported that tES can enhance various cognitive functions including memory, learning and attention, especially during learning of the task (26–28). In parallel, tDCS has shown promising results in treating psychiatric disorders such as major depressive disorder (29), various clinical symptoms and cognitive impairments in bipolar disorder (30, 31), auditory hallucinations (32), and negative symptoms (33) in schizophrenia, as well as numerous others (34).
Arousal and sleep are physiologically modulated by “top-down” cortico-subcortical loops (35) that are known to be altered in some sleep disorders such as insomnia (36). The “top-down” concept raises the idea of modulating sleep with external stimulation of the neocortex. Given that tES has primarily cortical direct effects, this approach appears thus as a relevant therapeutic strategy. Over the past years, there have been several attempts to modulate sleep with tES-based approaches targeting “top-down” networks in both the healthy and pathological brains. However, in addition to heterogeneous and inconsistent results, studies strongly differ in terms of the number of samples, tES protocols, and type of measures. Furthermore, despite a growing interest in sleep modulations with electric current, data about the impact of tES in sleep remain scattered between studies and have not been systematically reviewed, which prevent from drawing definitive conclusions on the effect of tES on measurable aspects of sleep.
To gather knowledge about the specific effects of brain tES on core measurable aspects of sleep, we conducted a systematic review of studies that explored the impact of such procedure on neurophysiological sleep oscillations, sleep patterns measured objectively with polysomnography and subjective psychometric assessments of sleep. Here, we focus on the specific impact of tES on these sleep-related outcomes in both healthy and clinical populations; for details about the effect of tES during sleep on wake cognitive processes, we refer the interested reader to the exhaustive review recently published by Barham et al. (37). Results presented in our review will contribute to the understanding of underlying mechanisms of tES on sleep and improvement of sleep health, sleep complaints, and sleep disorders with tES. In parallel, this review may lend insight for further enhancement of sleep induction/stability, as well as physiological effects of sleep (e.g., memory strengthening) with innovative techniques of neuromodulation in healthy people.
Recommendations of the PRISMA guidelines for systematic review and meta-analysis were followed (38). The protocol was prospectively registered at the PROSPERO register (ID: 178910) (39).
The criteria for inclusion were as follows: (i) English language studies published in peer-review journals, (ii) participants' age from 10–80 years. (iii) oscillatory data measured with electroencephalography and/or sleep pattern data reported from polysomnographic (or actigraphy) recordings and/or subjective sleep data assessed with validated rating scale, and (iv) measures collected pre-to-post and/or during the tES procedure. If two publications reported findings from the same dataset, the authors were contacted to identify the most appropriate data to review.
We searched the MEDLINE, Embase, ScienceDirect, and Clinical Trials databases using the following Medical Subject Heading (MeSH) terms in reference title, abstract, or keywords with no limitation of date until February 2020:
- (i) Sleep: “sleep,” “insomnia,” “hypersomnia,” “sleepiness,” “sleep apnea,” “somnolence,” “snoring,” “restless legs syndrome,” “periodic limb movements disorder,” “REM sleep behavior disorder,” “obstructive sleep apnea,” “sleep-wake disruption,” “parasomnia,” “bruxism,” “circadian rhythm sleep disorder.”
- (ii) tES: “Transcranial stimulation,” “tES,” “Transcranial Electrical Stimulation,” “tDCS,” “Transcranial Direct Current Stimulation,” “tRNS,” “Transcranial Random Noise Stimulation,” “tACS,” “Transcranial Alternating Current Stimulation.”
After excluding duplicate references, two reviewers (CD and PAG) independently screened the title and abstract of each study identified by the search and applied the inclusion criteria. Following this first screen, we applied the same procedure to the full text of eligible studies. Discrepancies between reviewers were resolved by discussion with a third member of the authorship. The “similar articles” findings in MEDLINE and Reference lists in identified studies were also reviewed for additional studies, although none were identified in this manner. The literature search strategy is detailed in the flow chart diagram (Figure 1).
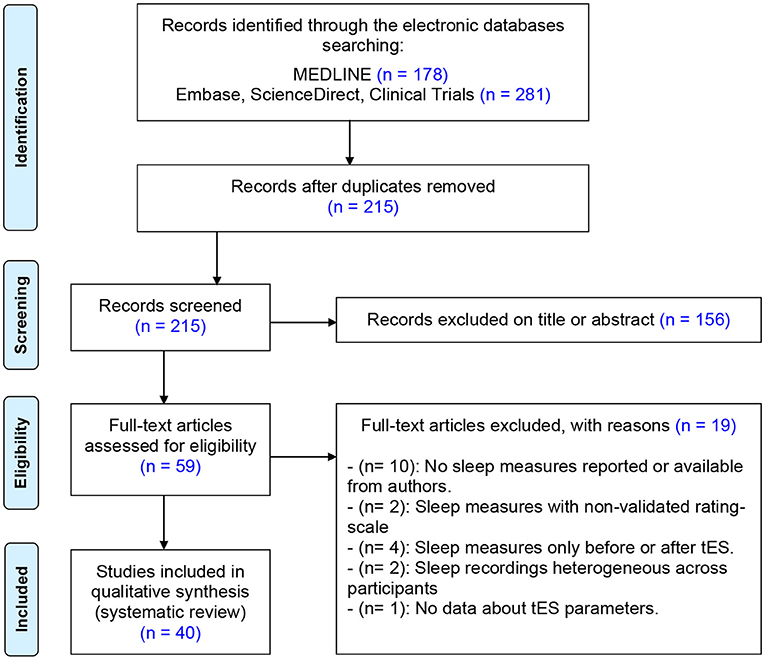
Figure 1. Flow diagram for the systematic review.
Two reviewers (CD and PAG) independently extracted the following data when present: (i) population data (sample size, gender ratio, disorder, or healthy status), (ii) study design (parallel or crossover groups, controlled or uncontrolled), (iii) tES protocol (anode and cathode placement; electrode size; current density and intensity; number, frequency, and duration of sessions; period and condition of stimulation), (iv) neurophysiological outcomes as measured with electroencephalography and/or sleep pattern outcomes as measured with polysomnographic (or actigraphy) recordings and/or subjective sleep outcomes as assessed with validated rating scale, and (v) adverse effects of the tES procedure.
To measure the overall quality of the included references, a global rating score was calculated for each study using the Standard Quality Assessment [QualSyst tool (40)].
As shown in Figure 1, the initial search returned 459 references after duplicate removal. Following preliminary screening of the titles and/or abstracts, 215 were excluded accordingly. Among the 59 references that were reviewed in detail, 40 studies were selected for systematic review including 511 healthy participants and 452 patients. The age of the participants varied from 12.3 to 73.4 years. Only 8 studies out of 40 reported transient adverse effects associated to the tES procedure (41–48). Overall, the quality assessment was satisfactory (mean: 22.1 ± 3.99). Total scores and details of the assessment are given in the Supplementary Table 1. Highlights of major significant effects of tES on sleep are pictured in Figure 2 and detailed in Supplementary Table 2.
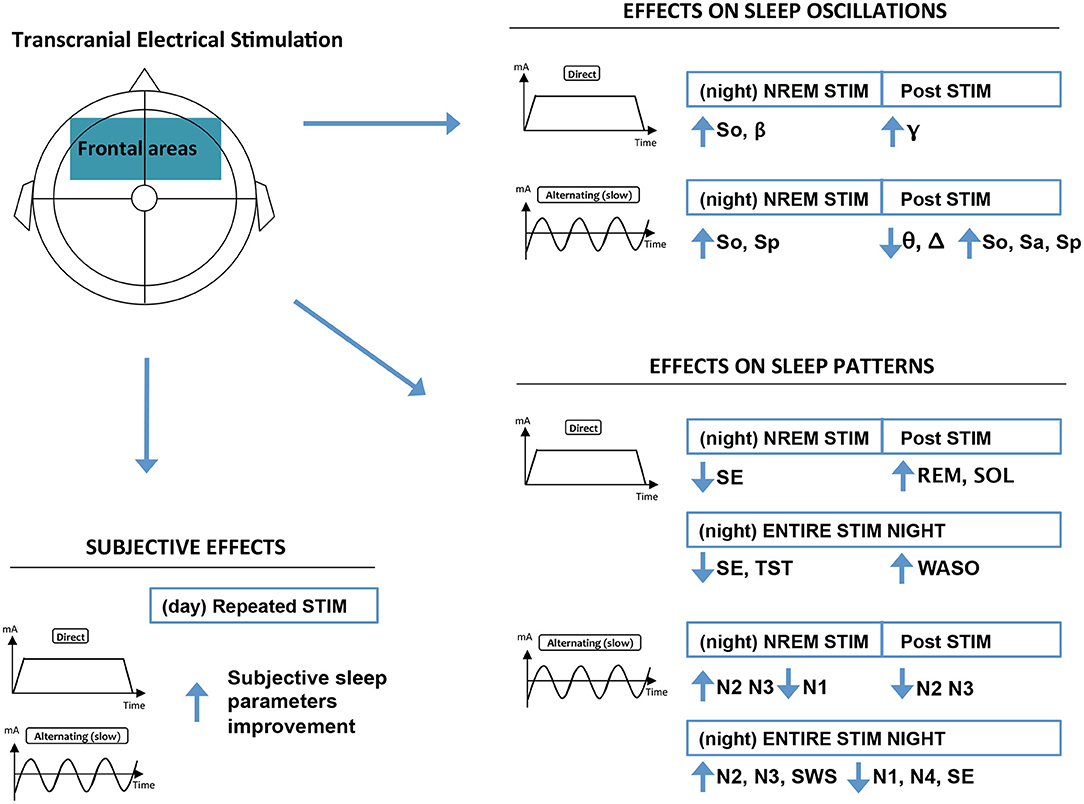
Figure 2. Highlights of major significant effects of frontal tES on sleep. Results regarding non-frontal tES, tES during REM, and fast alternating tES were scarce, and thus omitted from the figure. Effect on sleep patterns: NREM, non-rapid eye movement sleep; N1–4, NREM sleep stages relative duration; REM, rapid eye movement sleep; SE, sleep efficiency; SWS, slow wave sleep relative duration; SOL, sleep onset latency; WASO, wake after sleep onset. Effects on sleep oscillations: β, beta power (15–25 Hz); Δ, delta power (1–4 Hz); γ, gamma power (>25 Hz); θ, theta power (4–8 Hz); NREM, non-rapid eyes movement sleep; So, slow oscillations power (0.5–1 Hz); Sa, slow activity power (0.5–4 Hz); Sp, spindle power (10–15 Hz).
Twenty-four studies investigated the impact of tES on oscillatory aspects of sleep in healthy populations (45, 47, 49–64) and clinical populations (65–70). All used a crossover sham-controlled design with days-to-week washout periods between conditions, with the exception of two studies that included parallel arms of participants (60, 69). Study details are described in Table 1.
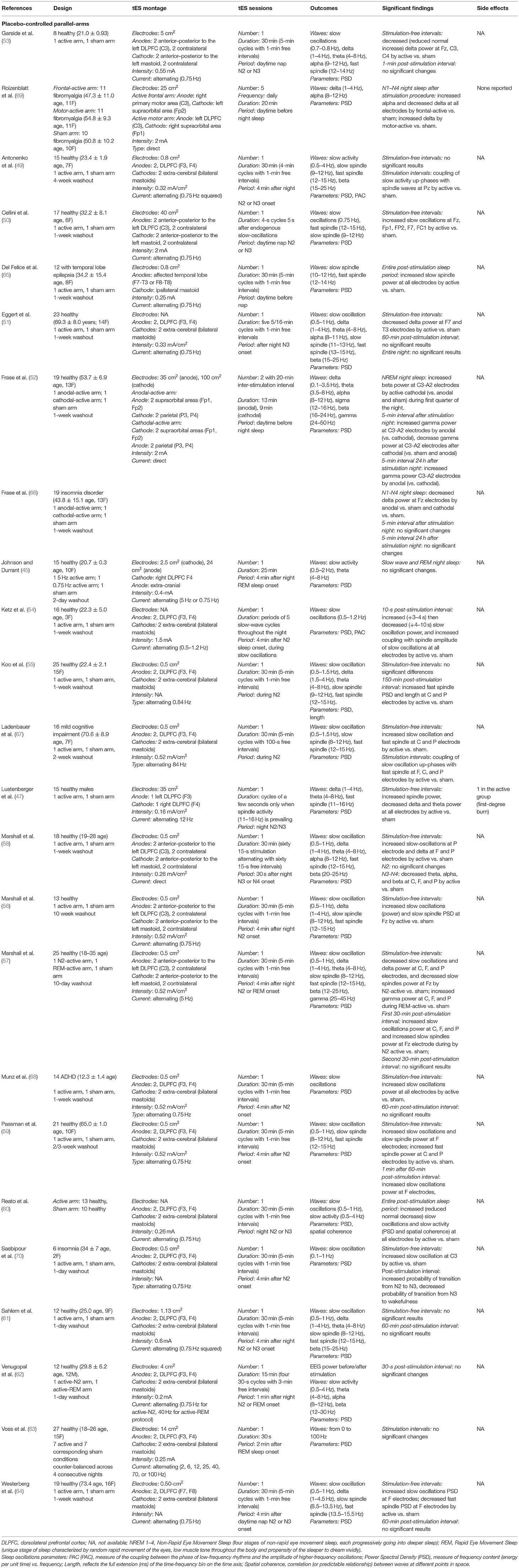
Table 1. Impact of transcranial electrical stimulation on oscillatory aspects of sleep.
Most research groups aimed for “top-down” effects and gave a single tES session targeting bilateral frontal areas with returning electrodes overlying the mastoids or the vertex. In these studies, the stimulation applied cycles of slow alternating current (around 0.75 Hz, interspersed by stimulation-free intervals) that were triggered during early stages NREM sleep (47, 49, 51, 55–57, 59, 61, 64, 67, 68). This specific design was employed after Marshall et al. original study to test if the prefrontal slow oscillations enhancement by tES during NREM is associated with increased hippocampal–neocortical-dependent declarative memory consolidation. This hypothesis is based on evidence that slow oscillations are the hallmark of neurophysiological activity during NREM being associated with neutral declarative memory (58). A subsequent enhancement of slow oscillations PSD by direct (58) and slow alternating (50, 56, 59, 64) tES vs. sham was repeatedly observed during stimulation-free intervals at the stimulated areas. In addition, increased spindle waves PSD (56, 59) and decreased delta/theta PSD (51, 53) were reported during these intervals. Another study from Marshall's group that involved higher-frequency alternating current (5 Hz) observed opposite patterns of changes, i.e., decreased slow oscillations, delta, and slow spindle power by tES (57). In contrast, one experiment using a slow spindle-like alternating current (12 Hz) observed an increase of power after tES in this specific frequency range (47).
An increase in slow oscillations and spindle waves power by active tES against sham was mainly demonstrated by several studies during long intervals after both slow-wave (0.75 Hz) and theta (5 Hz) alternating NREM stimulation (46, 57, 59, 60). However, recordings during post-stimulation periods were highly heterogeneous in terms of intervals where oscillations were measured and averaged. Regarding per-stimulation recordings, a single study using specific filtering procedures demonstrated a significant coupling between NREM slow oscillations up-phases and spindle waves at parietal electrodes concomitant to active tES vs. sham (49). No significant changes in sleep oscillations were observed when taking into consideration the entire stimulation night (51). In parallel, some research groups stimulated the brain with slow alternating current during REM (rapid-eye movement sleep). An increase in gamma power during stimulation-free intervals was demonstrated (57), but no significant changes were reported during stimulation intervals and entire sleep periods (45, 63).
Two studies used a bifrontal tES montage involving direct stimulating current (52, 58). It was observed that direct cathodal stimulation during daytime before sleep increased beta power at central sites during the first NREM night sleep cycle vs. both anodal and sham stimulation. By contrast, anodal stimulation induced an increase in gamma band power after the stimulation night compared with the other stimulation conditions (52). In parallel, Marshall and colleagues demonstrated that direct tES concomitant to NREM increases delta power in stimulation-free intervals and decreases higher-frequency band power during post-stimulation periods of slow wave sleep (58). No long-term effects were investigated across studies.
Six studies investigated the effect of a single brain tES session on oscillatory aspects of sleep in clinical populations. All were sham-controlled crossover trials. Two studies involved patients with insomnia disorder. Decreased NREM delta power after a single frontal anodal direct stimulation during daytime (66) and increased slow oscillation power during NREM stimulation-free intervals by alternating slow current vs. sham were observed in this population (70). In parallel, an increase of slow oscillation power during NREM stimulation-free intervals by alternating slow current vs. sham was reported in a group of patients with ADHD (Attention Deficit/Hyperactivity Disorder) (68). A similar tES montage also increased slow oscillations in patients with mild cognitive impairment, along with increased spindle power during NREM stimulation-free intervals (67). A three-arm study involving patients with fibromyalgia reported an increased alpha and decreased delta power after five sessions of frontal stimulation vs. sham and an increased delta power after five sessions of motor stimulation vs. sham (69). Finally, stimulation of the affected temporal lobe of patients with temporal lobe epilepsy before a nap induced an increase of slow spindle wave power (65).
Twenty studies investigated the impact of tES on sleep patterns in healthy (45, 47, 49–52, 55–61, 63, 64) and clinical (65–70) populations. Studies explored tES-induced changes in patterns of sleep including continuity (e.g., total sleep time, sleep efficiency, wake after sleep onset, and sleep onset latency) and architecture (i.e., sleep stages relative duration—expressed as percentage of total sleep time—and latency). Study details are described in Table 2.
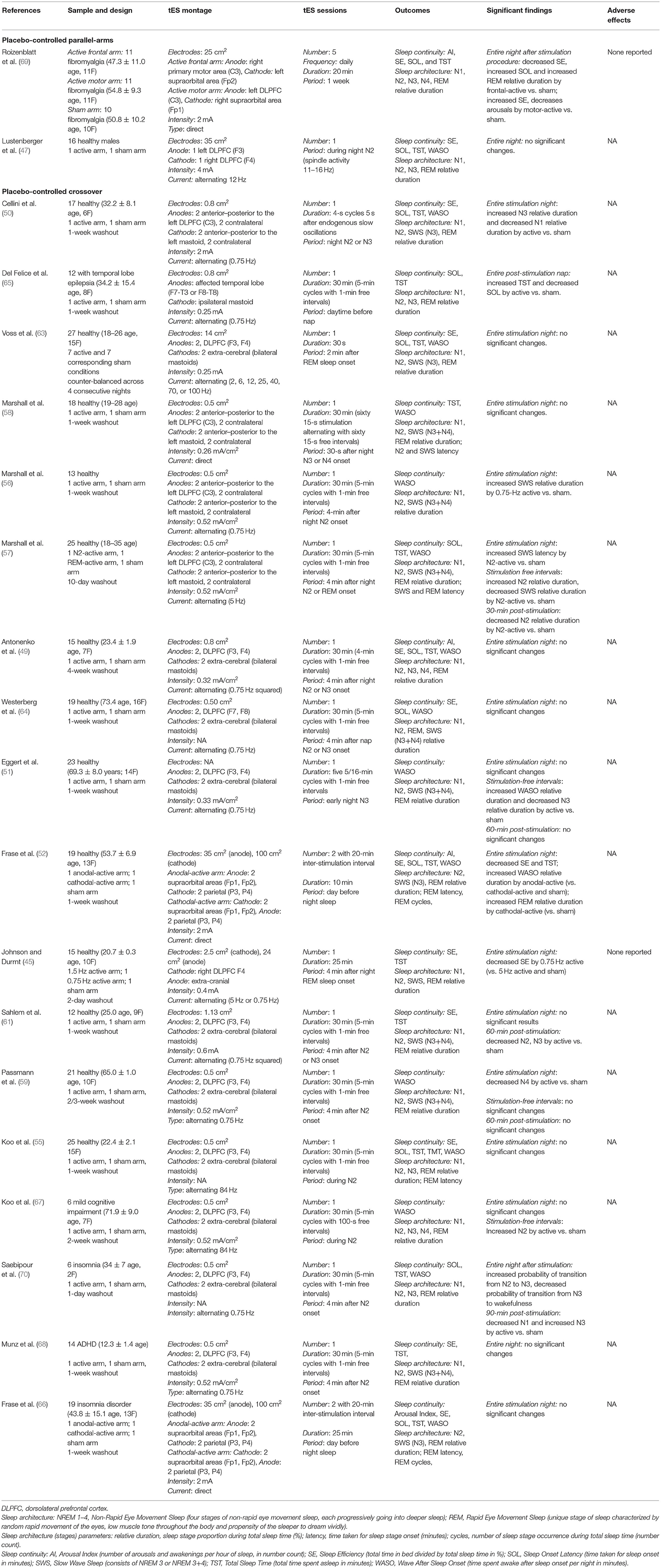
Table 2. Impact of transcranial electrical stimulation on pattern aspects of sleep.
Fourteen studies investigated the effect of a single brain tES session on sleep patterns in healthy samples (45, 47, 49–52, 55–61, 63, 64). All used a crossover sham-controlled design with days-to-week washout periods between conditions.
Most studies used the Marshall's bifrontal montage (58) with alternating current (49–51, 56–58, 64). Only a minority of studies reported significant results, and these were highly heterogeneous. Over the entire stimulation night, two reports demonstrated an increase in the relative duration of late NREM stages (N3, N4) by active stimulation vs. sham (50, 56). However, a study Passmann et al. found the opposite (59). One study observed a decreased relative duration of stage N1 (50). During stimulation-free intervals, an increased relative duration of stage N2 and wake after sleep onset was found, while later NREM stages were decreased (51, 57). During post-stimulation periods, two studies reported a decrease of N2 and N3 relative duration by active vs. sham (57, 61). A research group that explored the effect of the same montage during REM sleep—in order to trigger conscious awareness in dreams—reported no effect on sleep architecture (63). In parallel, a protocol using bifrontal tES reported a significant decrease of sleep efficiency over the entire stimulation night by alternating stimulation (0.75 Hz) as compared to sham and faster stimulation (5.0 Hz) during REM (45).
Regarding non-bifrontal montages, a single study studied the effect of direct current tES before sleep using fronto-parietal electrode placements (52). These authors reported decreased total sleep time and sleep efficiency when anodes were placed over the frontal cortex and cathodes over the parietal areas, in comparison to the reverse and sham montages. By contrast, REM relative duration was increased by frontal cathodal stimulation in comparison to anodal (52). Finally, a single session of tES during early NREM with the anode overlying the left prefrontal cortex and a contralateral cathode induced no significant changes in sleep architecture parameters of a healthy sample (47).
Six studies investigated the effect of a single brain tES session on sleep patterns in clinical samples (65–70). Two crossover sham-controlled studies involved individuals with insomnia disorder. The first demonstrated that a single session of active bifrontal alternating current during early NREM decreases N1 and increases N3 relative duration in the post-stimulation periods as compared to sham (70). The second study showed no significant changes in sleep patterns across the entire night after two fronto-parietal direct current tES sessions during daytime (66). In parallel, a crossover sham-controlled study that gave a single session of bifrontal active alternating current in subjects with ADHD failed to demonstrate significant changes across the entire stimulation night (68). By contrast, a research group that used the same protocol in six elder subjects with mild cognitive impairment found an increase of N2 relative duration during stimulation-free intervals (67). A three-arm study involving participants with fibromyalgia observed a significant sham-controlled effect of five consecutive direct current tES sessions that was specific to the stimulation site, such as anodal stimulation of the left primary motor area increased sleep efficiency and decreased number of arousals, whereas anodal stimulation of the left prefrontal cortex was associated with an increase of sleep latency and REM relative duration, and a decrease in sleep efficiency (69). Finally, a protocol stimulating the affected temporal lobe of patients with temporal lobe epilepsy before a nap demonstrated a significant increase of total sleep time and decrease of sleep onset latency by active vs. sham stimulation (65).
Fifteen studies investigated the impact of tES on subjective aspects of sleep in healthy (45, 52, 71–73) and clinical samples (41–44, 46, 48, 66, 74–81). Most used parallel arms (45, 52, 66, 72) or crossover-controlled designs (41–43, 46, 71, 73, 74, 78, 80, 81). The others were uncontrolled series or case reports. Studies details are described in Table 3.

Table 3. Impact of transcranial electrical stimulation on subjective aspects of sleep.
Five studies investigated the impact of a single tES session during wake periods on the subjective sleep parameters in healthy groups. One that used high-definition direct current tES targeting the left prefrontal cortex in elders observed an increase in subjective sleep duration and sleep efficiency in the active group vs. a waiting list group (73). Similarly, a crossover study that tested slow alternating tES during sleep found higher sleep quality and efficiency after active vs. sham stimulation (72). A study that specifically investigated frontal stimulation in athletes observed a global improvement in subjective sleep after two consecutive active stimulation sessions in comparison to a group that received sham stimulations (71). Finally, no significant changes were observed in sleepiness scales neither after two frontal tES sessions during daytime (52) nor during REM sleep (45).
All studies used direct current tES (tDCS). Parkinson's disease was the most represented neuropsychiatric disorder. A crossover placebo-controlled trial investigated the effect of 10 consecutive days of tDCS treatment on non-motor symptoms (80). No significant differences between groups were seen in the Epworth Sleepiness Scale (ESS) at week 2 and week 14 following treatment. Similarly, a sham-controlled study that gave eight bifrontal tES sessions reported no significant changes in the Epworth Sleepiness Scale both after the procedure and at long term (74). An uncontrolled study reported an absence of significant effects on the PROMISTM sleep assessment after 10 sessions of bifrontal tDCS (transcranial direct current stimulation) (44). By contrast, another study observed a significant improvement of the Pittsburgh Sleep Quality Index (PSQI) sleep latency subscore and total score after 10 sessions of a tDCS montage involving two anodes placed between the primary motor area and the prefrontal cortex, and two cathodes placed over the supraorbital areas (77).
In parallel, a single placebo-controlled trial in individuals with post-polio syndrome observed a significant PSQI improvement after 15 consecutive sessions of tDCS with two anodes targeting primary motor areas (41). Besides, studies exploring the impact of tDCS targeting the inferior frontal cortex in HIV patients (43) and targeting the motor areas in patients with restless legs syndrome (46) and chronic pain associated with insomnia (78) yielded negative results.
Regarding mood disorders, a non-controlled tDCS protocol placing the anode over the prefrontal cortex and the cathode over the cerebellum significantly improved sleep quality with 46% improvement of the PSQI in a sample of euthymic patients with bipolar disorder (79). In contrast, no effect of bifrontal tDCS was observed on the sleep item of the Montgomery–Asberg Depression Rating Scale (MADRS) in a randomized controlled trial involving participants with depression (42).
No significant changes were reported for subjective parameters including tiredness and alertness in a crossover study involving two bifrontal tES sessions in patients with insomnia disorder (66). By contrast, a recent randomized placebo-controlled trial demonstrated that 20 daily consecutive sessions of frontal tES with alternating current significantly improved PSQI both after the procedure and at 2 months follow-up (81).
A case series of idiopathic hypersomnia showed that 4 weeks of bifrontal tDCS can reduce excessive daytime sleepiness, as assessed by the ESS (76). Finally, case reports observed daytime vigilance and sleep quality improvement using specific rating scales in organic hypersomnia (75) and after-stroke condition (48), respectively.
Through this systematic literature review, we observe that tES can modify endogenous brain oscillations during sleep and that subjective assessments show clear improvements after tES, while relationships with concomitant changes in sleep architecture warrant validations (see Figure 2 and Supplementary Table 2 for a summary of main results). Tolerability profile of tES appears good with few non-severe side effects reported across studies.
The main neurophysiological finding of our systematic review is that anodal tES of the frontal areas with a slow alternating or direct current during NREM sleep can immediately enhance the power spectral density (PSD) of endogenous slow oscillations at the stimulated areas (50, 56, 58, 59, 64). Slow oscillatory activity originates in the centro-frontal neocortex and coordinates widespread firing synchrony across other brain regions, including adjacent cortices and subcortical structures such as the thalamus and brainstem nuclei (82–84). This crosstalk is essential for the generation of oscillatory cycles that orchestrate brain activity during sleep (85). Regarding our results, although tES has primarily cortical direct effects, it is likely that external stimulation of the neocortex spreads to the entire cortico-subcortical network through top-down mechanisms to facilitate slow oscillatory activity. This rationale is supported by preclinical results demonstrating that the modulatory effects of electrical stimulation of centro-frontal cortices extend to subcortical arousal networks (86, 87). Moreover, it has been reported that stimulating the prefrontal region can reach deeper structures and lead to subcortical dopamine release in the ventral striatum (88). In parallel, slow alternating stimulation during NREM sleep has been shown to facilitate corticocortical network activity, which can explain the observed enhancement of sleep-dependent restorative processes of tES with respect to declarative memory in healthy participants (45, 47, 50), as well as behavioral inhibition and executive functions in patients with ADHD (68). For more details about the effect of tES during sleep on memory processes, we refer the interested reader to this exhaustive review (37). At the cellular level, it is likely that enhancement of slow oscillatory activity is related to tES-induced anodal polarization, which corroborates previous demonstrations that endogenous negative potentials arising during late stages of NREM sleep and facilitating specific shifts in extracellular ionic concentration play a supportive role in the generation of slow oscillations (84, 89, 90).
In parallel, it was shown that slow oscillation PSD immediately following tES is negatively correlated with measures of slow oscillation spectral power and coherence immediately preceding stimulation, suggesting that tES may be more effective when applied during less synchronized and more “quiet” periods of brain activity (50). This put forward the importance of the baseline cortical activation state on the impact of tES (91). As observed during magnetic stimulation of the brain (92), these findings imply that tES effect interacts with the ongoing activity of the sleeping brain at the time of stimulation.
In addition to modulating corresponding spectral ranges, it was shown that slow oscillatory frontal tES induces collateral modulation and enhancement of spindle waves (47, 49, 56, 59). These observations support the conclusion that slow alternating tES enhances physiologically normal conditions in which slow alternating activity drives the generation of spindle, which implies that spindle activity is maximal during late stages of NREM sleep (i.e., transition to slow wave sleep) (93–95). These neurophysiological changes were also observed during post-stimulation intervals (46, 57, 59, 60), suggesting short-term plasticity effect induced with regard to putative synaptic mechanism consequences described above. Spike timing-dependent plasticity has been proposed for the observed after-effects of tES. According to this form of brain plasticity, when the frequency of an externally induced driving force (i.e., tES) is matched with a neural circuit resonance frequency, spike timing-dependent plasticity can strengthen synapses in this circuit (96). However, changes were not replicated when taking into consideration the entire stimulation night (51), which could be attributed to the decreasing levels of slow oscillations typically observed across a sleep period (97). Regarding lower-frequency ranges, significant delta modulations induced by frontal slow alternating or direct tES during NREM sleep suggest potential cross-frequency coupling mechanisms (51, 53, 58).
Only a minority of studies reported significant changes in sleep architecture, namely, increased sleep stage NREM2 and decreased further slow wave sleep stages relative duration (51, 57, 67), indicating a potential sleep-stabilizing effect of slow oscillatory tES (single session) during NREM sleep. In parallel, an absence of tES beneficial effects on polysomnographic measures of sleep was repeatedly observed across studies conducted in both clinical and healthy samples. It is likely that potential improvement of sleep continuity has been missed due to a ceiling effect in good sleepers. A few studies observed tES-induced sleep continuity disruption, which may be related to potential increase of external disturbance or unwanted modulation of vigilance control circuits (45, 57, 66). Thus, when performing tES especially in the clinical population, stimulation sessions upon awakening should be recommended in order to avoid adverse effects on sleep continuity. Interestingly, a study observed a relative stronger decrease of sleep continuity in healthy controls following tES, but not in patients with insomnia disorder. It is proposed that this differential effect of tES is related to persistent hyperarousal in this clinical population, preventing the arousal-inducing effect of anodal active tES in healthy controls (66).
A significant number of studies observed significant improvements of subjective sleep after tES in both healthy (71–73) and a large range of neuropsychiatric diseases (41, 48, 75–77, 79, 81). The positive results were observed across various rating instruments, suggesting large impact of tES on subjective components of sleep. Notably, all studies showing significant improvements used tES montages that stimulated frontal and/or motor areas. This is not surprising since neuroimaging methods identified that cortical topography of slow waves during sleep are primarily associated with activity in a core set of cortical areas that are mainly located in the prefrontal cortex and motor regions (98, 99). Although conventional tES current may spread to other regions than the targeted area (100), studies showing a subjective improvement of sleep after tES used comprehensive stimulation protocols assuring activation of the major cortical areas involved in sleep regulation which, in turn, reflected on subjective sleep measures. It is reported that complementary biological mechanisms of subjective sleep improvement by tES can involve stimulation of the reticular formation (41), which plays a central role in states of consciousness like sleep. In addition, sleep promotion induced by decoupling functional connectivity between wakeful-active default mode network and subcortical structures (73) and activation of non-motor function of the cerebellum such as sleep regulation (101) may underlie subjective sleep improvement by tES.
These results hold promises for the use of tES to target sleep symptoms in various clinical populations with neuropsychiatric disorders. Furthermore, significant correlations were observed between subjective sleep parameters and non-sleep parameters, such as depressive symptoms (77) and attention performance (76). Further investigations are well-warranted to identify if other clinical dimensions are improved through improvement of sleep.
The main limitation of comparisons across reviewed studies relies on the high heterogeneity of results and the important rate of negative results. A main shortcoming that may explain this limitation is the very high heterogeneity of stimulation protocol parameters that could influence the effect on sleep and sleep measures, such as the device type, duration of stimulation on/offsets, electrode impedance, and electrode placement across studies. Slight methodological variations regarding the stimulation signal (direct vs. alternating) and the applied current density may also impact observations. For instance, current ramping at the beginning and at the end of each stimulation interval is likely to influence short-lasting stimulation-dependent entrainments of the specific oscillatory activity (51, 58). In addition, heterogeneity of samples sizes, sleep variations according to age and gender (102, 103), and the considerable interindividual and intraindividual differences commonly observed in sleep recordings may have accounted for the conflicting results. Another potential explanation for inconsistent effects of tES on endogenous oscillations and sleep patterns, which are derived from physiological recordings, is the difficulty in collecting high-quality stable long-term measurements during sleep due to a number of issues such as movement artifacts (rapid eye movements, tossing, turning, etc.) and slippage in the placement of electrodes through the night. As pointed out in a few recent studies (104, 105), the effects of tES on endogenous oscillations can systematically vary through the course of the night due to refractory effects—so future studies need to track stimulation-induced biomarkers for the outcomes of interest during sleep. Finally, no quantitative meta-analyses were applicable due to the high heterogeneity of studies included in this systematic review.
Regarding changes in sleep oscillations, a potential “endogenous” explanation is that the stimulation was likely given in different sleep stages across studies, especially since not all studies controlled stimulation-free intervals of neurophysiological measurement for ongoing sleep stage. Given the interindividual variability of sleep architecture and fragmentation and the fact that oscillatory stimulation effects are strongly dependent on ongoing brain state and network activity, this may have accounted for heterogeneity (106).
Some discrepancies were observed between healthy and clinical samples. It might be that the latter may have different responses to tES with different response/activation threshold, as for instance in insomnia vs. healthy subjects, who met hyperarousal symptoms (66). It is also possible that subjective sleep alterations are secondary to other symptoms such as pain (78), whose neurobiological bases are not directly targeted by tES in sleep-oriented studies. In addition, the strong placebo response observed in neuropsychiatric disorders might have hampered the observation of sleep improvement under active stimulation (80).
Finally, it should be noted that the vast majority of studies included in this systematic review involve frontal stimulation, which prevents us from concluding on a general effect of tES on sleep. A review focusing only on studies stimulating frontal areas could have indeed led to a more homogeneous picture. Nevertheless, we a priori defined the aim of our study to conduct an exhaustive systematic review of tES on sleep with the objective to account for all the existing literature and all possible stimulation areas.
tES-based approaches have a significant impact on oscillatory neurophysiological parameters of sleep. Furthermore, studies suggest their enhancement as physiological restorative processes that could serve as a potential therapeutic target in neuropsychiatric disorders. While the conflicting effects of tES on sleep patterns shed some doubt on its potential utility to improve sleep continuity, the significance of subjective aspects of sleep in various populations invites further development of non-invasive stimulation treatments for sleep conditions that are among the most prevalent health problems worldwide. Given the important heterogeneity of stimulation protocols and samples, future studies should examine the impact of these variables on the effect of tES on sleep measures. Furthermore, several major questions should be investigated to define optimal application of tES for sleep improvement, in terms of stimulation parameters (e.g., current type, duration, sessions), stimulation location, and type of brain state (e.g., wake/sleep, sleep stage) during stimulation.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
CD designed the study, performed the literature review, and wrote the first draft of the manuscript. PG supervised the study. JB, J-AM-F, JM, ML, and MP provided critical inputs to the manuscript. All authors reviewed and approved the manuscript in its final form.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.646569/full#supplementary-material
ADHD, Attention Deficit/Hyperactivity Disorder; EEG, electroencephalography; ESS, Epworth Sleepiness Scale; MeSH, Medical Subject Heading; MADRS, Montgomery-Asberg Depression Rating Scale; NREM, Non-Rapid Eye Movement (sleep); PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analysis; PROSPERO, International prospective register of systematic reviews; PSQI, The Pittsburgh Sleep Quality Index; REM, Rapid-Eye Movement (sleep); QualSyst, Standard Quality Assessment; SWS, Slow Wave Sleep; tACS, transcranial Alternating Current Stimulation; tDCS, transcranial Direct Current Stimulation; tES, transcranial Electrical Stimulation; tRNS, transcranial Random Noise Stimulation.
1. Pennartz CM, Uylings HB, Barnes CA, McNaughton BL. Memory reactivation and consolidation during sleep: from cellular mechanisms to human performance. Prog Brain Res. (2002) 138:143–66. doi: 10.1016/S0079-6123(02)38076-2
2. Walker MP. The role of slow wave sleep in memory processing. J Clin Sleep Med. (2009) 5:S20–6. doi: 10.5664/jcsm.5.2S.S20
3. Dorrian J, Dinges DF. Psychomotor Vigilance Performance: Neurocognitive Assay Sensitive to Sleep Loss. New York, NY: Marcel Dekker (2005). doi: 10.1201/b14100-5
4. Verster J, Pandi-Perumal SR, Streiner DL. Sleep and Quality of Life in Clinical Medicine. Totowa, NJ: Humana Press (2008). doi: 10.1007/978-1-60327-343-5
5. Ohayon MM. Epidemiological Overview of sleep Disorders in the General Population. Sleep Med Res. (2011) 1:1–9. doi: 10.17241/smr.2011.2.1.1
6. Buysse DJ. Sleep health: can we define it? Does it matter? Sleep. (2014) 37:9–17. doi: 10.5665/sleep.3298
7. Geoffroy PA, Tebeka S, Blanco C, Dubertret C, Le Strat Y. Shorter and longer durations of sleep are associated with an increased twelve-month prevalence of psychiatric and substance use disorders: Findings from a nationally representative survey of US adults (NESARC-III). J Psychiatr Res. (2020) 124:34–41. doi: 10.1016/j.jpsychires.2020.02.018
8. Cappuccio FP, D'Elia L, Strazzullo P, Miller MA. Sleep duration and all-cause mortality: a systematic review and meta-analysis of prospective studies. Sleep. (2010) 33:585–92. doi: 10.1093/sleep/33.5.585
9. Medic G, Wille M, Hemels ME. Short- and long-term health consequences of sleep disruption. Nat Sci Sleep. (2017) 9:151–61. doi: 10.2147/NSS.S134864
10. Yin J, Jin X, Shan Z, Li S, Huang H, Li P, et al. Relationship of sleep duration with all-cause mortality and cardiovascular events: a systematic review and dose-response meta-analysis of prospective cohort studies. J Am Heart Assoc. (2017) 6:e005947. doi: 10.1161/JAHA.117.005947
11. Lunsford-Avery JR, Engelhard MM, Navar AM, Kollins SH. Validation of the sleep regularity index in older adults and associations with cardiometabolic risk. Sci Rep. (2018) 8:14158. doi: 10.1038/s41598-018-32402-5
12. Hoevenaar-Blom MP, Spijkerman AM, Kromhout D, van den Berg JF, Verschuren WM. Sleep duration and sleep quality in relation to 12-year cardiovascular disease incidence: the MORGEN study. Sleep. (2011) 34:1487–92. doi: 10.5665/sleep.1382
13. Newman AB, Spiekerman CF, Enright P, Lefkowitz D, Manolio T, Reynolds CF, et al. Daytime sleepiness predicts mortality and cardiovascular disease in older adults. The Cardiovascular Health Study Research Group. J Am Geriatr Soc. (2000) 48:115–23. doi: 10.1111/j.1532-5415.2000.tb03901.x
14. Knutsson A. Health disorders of shift workers. Occup Med. (2003) 53:103–8. doi: 10.1093/occmed/kqg048
15. Nuyujukian DS, Anton-Culver H, Manson SM, Jiang L. Associations of sleep duration with cardiometabolic outcomes in American Indians and Alaska Natives and other race/ethnicities: results from the BRFSS. Sleep Health. (2019) 5:344–51. doi: 10.1016/j.sleh.2019.02.003
16. Li L, Zhang S, Huang Y, Chen K. Sleep duration and obesity in children: a systematic review and meta-analysis of prospective cohort studies. J Paediatr Child Health. (2017) 53:378–85. doi: 10.1111/jpc.13434
17. Spiegelhalder K, Regen W, Nanovska S, Baglioni C, Riemann D. Comorbid sleep disorders in neuropsychiatric disorders across the life cycle. Curr Psychiatry Rep. (2013) 15:364. doi: 10.1007/s11920-013-0364-5
18. Taylor DJ, Mallory LJ, Lichstein KL, Durrence HH, Riedel BW, Bush AJ. Comorbidity of chronic insomnia with medical problems. Sleep. (2007) 30:213–8. doi: 10.1093/sleep/30.2.213
19. Dijk DJ. EEG slow waves and sleep spindles: windows on the sleeping brain. Behav Brain Res. (1995) 69:109–16. doi: 10.1016/0166-4328(95)00007-G
20. Devine EB, Hakim Z, Green J. A systematic review of patient-reported outcome instruments measuring sleep dysfunction in adults. Pharmacoeconomics. (2005) 23:889–912. doi: 10.2165/00019053-200523090-00003
21. Nitsche MA, Cohen LG, Wassermann EM, Priori A, Lang N, Antal A, et al. Transcranial direct current stimulation: state of the art 2008. Brain Stimul. (2008) 1:206–23. doi: 10.1016/j.brs.2008.06.004
22. Nitsche MA, Paulus W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J Physiol. (2000) 3:633–9. doi: 10.1111/j.1469-7793.2000.t01-1-00633.x
23. Rroji O, van Kuyck K, Nuttin B, Wenderoth N. Anodal tDCS over the primary motor cortex facilitates long-term memory formation reflecting use-dependent plasticity. PLoS ONE. (2015) 10:e0127270. doi: 10.1371/journal.pone.0127270
24. Donde C, Brevet-Aeby C, Poulet E, Mondino M, Brunelin J. Potential impact of bifrontal transcranial random noise stimulation (tRNS) on the semantic Stroop effect and its resting-state EEG correlates. Neurophysiol Clin. (2019) 49:243–8. doi: 10.1016/j.neucli.2019.03.002
25. Yavari F, Nitsche MA, Ekhtiari H. Transcranial electric stimulation for precision medicine: a spatiomechanistic framework. Front Hum Neurosci. (2017) 11:159. doi: 10.3389/fnhum.2017.00159
26. Coffman BA, Clark VP, Parasuraman R. Battery powered thought: enhancement of attention, learning, and memory in healthy adults using transcranial direct current stimulation. Neuroimage. (2014) 85:895–908. doi: 10.1016/j.neuroimage.2013.07.083
27. Dayan E, Censor N, Buch ER, Sandrini M, Cohen LG. Noninvasive brain stimulation: from physiology to network dynamics and back. Nat Neurosci. (2013) 16:838–44. doi: 10.1038/nn.3422
28. Levasseur-Moreau J, Brunelin J, Fecteau S. Non-invasive brain stimulation can induce paradoxical facilitation. Are these neuroenhancements transferable and meaningful to security services? Front Hum Neurosci. (2013) 7:449. doi: 10.3389/fnhum.2013.00449
29. Moffa AH, Martin D, Alonzo A, Bennabi D, Blumberger DM, Bensenor IM, et al. Efficacy and acceptability of transcranial direct current stimulation (tDCS) for major depressive disorder: An individual patient data meta-analysis. Prog Neuropsychopharmacol Biol Psychiatry. (2020) 99:109836. doi: 10.1016/j.pnpbp.2019.109836
30. Donde C, Amad A, Nieto I, Brunoni AR, Neufeld NH, Bellivier F, et al. Transcranial direct-current stimulation (tDCS) for bipolar depression: a systematic review and meta-analysis. Prog Neuropsychopharmacol Biol Psychiatry. (2017) 78:123–31. doi: 10.1016/j.pnpbp.2017.05.021
31. Donde C, Neufeld NH, Geoffroy PA. The Impact of Transcranial Direct Current Stimulation (tDCS) on bipolar depression, mania, and euthymia: a systematic review of preliminary data. Psychiatr Q. (2018) 89:855–67. doi: 10.1007/s11126-018-9584-5
32. Mondino M, Sauvanaud F, Brunelin J. A review of the effects of transcranial direct current stimulation for the treatment of hallucinations in patients with schizophrenia. J ECT. (2018) 34:164–71. doi: 10.1097/YCT.0000000000000525
33. Valiengo L, Goerigk S, Gordon PC, Padberg F, Serpa MH, Koebe S, et al. Efficacy and safety of transcranial direct current stimulation for treating negative symptoms in schizophrenia: a randomized clinical trial. JAMA Psychiatry. (2019) 77:121–9. doi: 10.1001/jamapsychiatry.2019.3199
34. Lefaucheur JP, Antal A, Ayache SS, Benninger DH, Brunelin J, Cogiamanian F, et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin Neurophysiol. (2017) 128:56–92. doi: 10.1016/j.clinph.2016.10.087
35. Krone L, Frase L, Piosczyk H, Selhausen P, Zittel S, Jahn F, et al. Top-down control of arousal and sleep: Fundamentals and clinical implications. Sleep Med Rev. (2017) 31:17–24. doi: 10.1016/j.smrv.2015.12.005
36. Riemann D, Nissen C, Palagini L, Otte A, Perlis ML, Spiegelhalder K. The neurobiology, investigation, and treatment of chronic insomnia. Lancet Neurol. (2015) 14:547–58. doi: 10.1016/S1474-4422(15)00021-6
37. Barham MP, Enticott PG, Conduit R, Lum JA. Transcranial electrical stimulation during sleep enhances declarative (but not procedural) memory consolidation: Evidence from a meta-analysis. Neurosci Biobehav Rev. (2016) 63:65–77. doi: 10.1016/j.neubiorev.2016.01.009
38. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) 4:1. doi: 10.1186/2046-4053-4-1
39. Chien PF, Khan KS, Siassakos D. Registration of systematic reviews: PROSPERO. BJOG. (2012) 119:903–5. doi: 10.1111/j.1471-0528.2011.03242.x
40. Kmet L, Lee R, Cook L. Standard Quality Assessment Criteria For Evaluating Primary Research Papers From a Variety of Fields, Edmonton, AB: Alberta Heritage Foundation for Medical Research Suite (2004).
41. Acler M, Bocci T, Valenti D, Turri M, Priori A, Bertolasi L. Transcranial direct current stimulation (tDCS) for sleep disturbances and fatigue in patients with post-polio syndrome. Restor Neurol Neurosci. (2013) 31:661–8. doi: 10.3233/RNN-130321
42. Brunoni AR, Junior RF, Kemp AH, Lotufo PA, Bensenor IM, Fregni F. Differential improvement in depressive symptoms for tDCS alone and combined with pharmacotherapy: an exploratory analysis from the Sertraline vs. Electrical current therapy for treating depression clinical study. Int J Neuropsychopharmacol. (2014) 17:53–61. doi: 10.1017/S1461145713001065
43. Cody SL, Fazeli PL, Crowe M, Kempf MC, Moneyham L, Stavrinos D, et al. Effects of speed of processing training and transcranial direct current stimulation on global sleep quality and speed of processing in older adults with and without HIV: A pilot study. Appl Neuropsychol Adult. (2019) 27:267–78. doi: 10.1080/23279095.2018.1534736
44. Dobbs B, Pawlak N, Biagioni M, Agarwal S, Shaw M, Pilloni G, et al. Generalizing remotely supervised transcranial direct current stimulation (tDCS): feasibility and benefit in Parkinson's disease. J Neuroeng Rehabil. (2018) 15:114. doi: 10.1186/s12984-018-0457-9
45. Johnson JM, Durrant SJ. The effect of cathodal transcranial direct current stimulation during rapid eye-movement sleep on neutral and emotional memory. R Soc Open Sci. (2018) 5:172353. doi: 10.1098/rsos.172353
46. Koo YS, Kim SM, Lee C, Lee BU, Moon YJ, Cho YW, et al. Transcranial direct current stimulation on primary sensorimotor area has no effect in patients with drug-naive restless legs syndrome: a proof-of-concept clinical trial. Sleep Med. (2015) 16:280–7. doi: 10.1016/j.sleep.2014.07.032
47. Lustenberger C, Boyle MR, Alagapan S, Mellin JM, Vaughn BV, Frohlich F. Feedback-controlled transcranial alternating current stimulation reveals a functional role of sleep spindles in motor memory consolidation. Curr Biol. (2016) 26:2127–36. doi: 10.1016/j.cub.2016.06.044
48. Sanchez-Kuhn A, Medina Y, Garcia-Perez M, De Haro P, Flores P, Sanchez-Santed F. Transcranial direct current stimulation treatment in chronic after-stroke dysphagia: A clinical case. Psicothema. (2019) 31:179–83. doi: 10.7334/psicothema2018.310
49. Antonenko D, Diekelmann S, Olsen C, Born J, Molle M. Napping to renew learning capacity: enhanced encoding after stimulation of sleep slow oscillations. Eur J Neurosci. (2013) 37:1142–51. doi: 10.1111/ejn.12118
50. Cellini N, Shimizu RE, Connolly PM, Armstrong DM, Hernandez LT, Polakiewicz AG, et al. Short duration repetitive transcranial electrical stimulation during sleep enhances declarative memory of facts. Front Hum Neurosci. (2019) 13:123. doi: 10.3389/fnhum.2019.00123
51. Eggert T, Dorn H, Sauter C, Nitsche MA, Bajbouj M, Danker-Hopfe H. No effects of slow oscillatory transcranial direct current stimulation (tDCS) on sleep-dependent memory consolidation in healthy elderly subjects. Brain Stimul. (2013) 6:938–45. doi: 10.1016/j.brs.2013.05.006
52. Frase L, Piosczyk H, Zittel S, Jahn F, Selhausen P, Krone L, et al. Modulation of Total Sleep Time by Transcranial Direct Current Stimulation (tDCS). Neuropsychopharmacology. (2016) 41:2577–86. doi: 10.1038/npp.2016.65
53. Garside P, Arizpe J, Lau CI, Goh C, Walsh V. Cross-hemispheric alternating current stimulation during a nap disrupts slow wave activity and associated memory consolidation. Brain Stimul. (2015) 8:520–7. doi: 10.1016/j.brs.2014.12.010
54. Ketz N, Jones AP, Bryant NB, Clark VP, Pilly PK. Closed-loop slow-wave tACS improves sleep-dependent long-term memory generalization by modulating endogenous oscillations. J Neurosci. (2018) 38:7314–26. doi: 10.1523/JNEUROSCI.0273-18.2018
55. Koo PC, Molle M, Marshall L. Efficacy of slow oscillatory-transcranial direct current stimulation on EEG and memory - contribution of an inter-individual factor. Eur J Neurosci. (2018) 47:812–23. doi: 10.1111/ejn.13877
56. Marshall L, Helgadottir H, Molle M, Born J. Boosting slow oscillations during sleep potentiates memory. Nature. (2006) 444:610–3. doi: 10.1038/nature05278
57. Marshall L, Kirov R, Brade J, Molle M, Born J. Transcranial electrical currents to probe EEG brain rhythms and memory consolidation during sleep in humans. PLoS ONE. (2011) 6:e16905. doi: 10.1371/journal.pone.0016905
58. Marshall L, Molle M, Hallschmid M, Born J. Transcranial direct current stimulation during sleep improves declarative memory. J Neurosci. (2004) 24:9985–92. doi: 10.1523/JNEUROSCI.2725-04.2004
59. Passmann S, Kulzow N, Ladenbauer J, Antonenko D, Grittner U, Tamm S, et al. Boosting slow oscillatory activity using tDCS during early nocturnal slow wave sleep does not improve memory consolidation in healthy older adults. Brain Stimul. (2016) 9:730–9. doi: 10.1016/j.brs.2016.04.016
60. Reato D, Gasca F, Datta A, Bikson M, Marshall L, Parra LC. Transcranial electrical stimulation accelerates human sleep homeostasis. PLoS Comput Biol. (2013) 9:e1002898. doi: 10.1371/journal.pcbi.1002898
61. Sahlem GL, Badran BW, Halford JJ, Williams NR, Korte JE, Leslie K, et al. Oscillating square wave transcranial direct current stimulation (tDCS) delivered during slow wave sleep does not improve declarative memory more than sham: a randomized sham controlled crossover study. Brain Stimul. (2015) 8:528–34. doi: 10.1016/j.brs.2015.01.414
62. Venugopal R, Sasidharan A, Marigowda V, Kumar G, Nair AK, Sharma S, et al. Beyond hypnograms: assessing sleep stability using acoustic and electrical stimulation. Neuromodulation. (2019) 22:911–5. doi: 10.1111/ner.12847
63. Voss U, Holzmann R, Hobson A, Paulus W, Koppehele-Gossel J, Klimke A, et al. Induction of self awareness in dreams through frontal low current stimulation of gamma activity. Nat Neurosci. (2014) 17:810–2. doi: 10.1038/nn.3719
64. Westerberg CE, Florczak SM, Weintraub S, Mesulam MM, Marshall L, Zee PC, et al. Memory improvement via slow-oscillatory stimulation during sleep in older adults. Neurobiol Aging. (2015) 36:2577–86. doi: 10.1016/j.neurobiolaging.2015.05.014
65. Del Felice A, Magalini A, Masiero S. Slow-oscillatory transcranial direct current stimulation modulates memory in temporal lobe epilepsy by altering sleep spindle generators: a possible rehabilitation tool. Brain Stimul. (2015) 8:567–73. doi: 10.1016/j.brs.2015.01.410
66. Frase L, Selhausen P, Krone L, Tsodor S, Jahn F, Feige B, et al. Differential effects of bifrontal tDCS on arousal and sleep duration in insomnia patients and healthy controls. Brain Stimul. (2019) 12:674–83. doi: 10.1016/j.brs.2019.01.001
67. Ladenbauer J, Ladenbauer J, Kulzow N, de Boor R, Avramova E, Grittner U, et al. Promoting sleep oscillations and their functional coupling by transcranial stimulation enhances memory consolidation in mild cognitive impairment. J Neurosci. (2017) 37:7111–24. doi: 10.1523/JNEUROSCI.0260-17.2017
68. Munz MT, Prehn-Kristensen A, Thielking F, Molle M, Goder R, Baving L. Slow oscillating transcranial direct current stimulation during non-rapid eye movement sleep improves behavioral inhibition in attention-deficit/hyperactivity disorder. Front Cell Neurosci. (2015) 9:307. doi: 10.3389/fncel.2015.00307
69. Roizenblatt S, Fregni F, Gimenez R, Wetzel T, Rigonatti SP, Tufik S, et al. Site-specific effects of transcranial direct current stimulation on sleep and pain in fibromyalgia: a randomized, sham-controlled study. Pain Pract. (2007) 7:297–306. doi: 10.1111/j.1533-2500.2007.00152.x
70. Saebipour MR, Joghataei MT, Yoonessi A, Sadeghniiat-Haghighi K, Khalighinejad N, Khademi S. Slow oscillating transcranial direct current stimulation during sleep has a sleep-stabilizing effect in chronic insomnia: a pilot study. J Sleep Res. (2015) 24:518–25. doi: 10.1111/jsr.12301
71. Charest J, Marois A, Bastien CH. Can a tDCS treatment enhance subjective and objective sleep among student-athletes? J Am Coll Health. (2019) 14:1–12. doi: 10.1080/07448481.2019.1679152
72. Robinson CSH, Bryant NB, Maxwell JW, Jones AP, Robert B, Lamphere M, et al. The benefits of closed-loop transcranial alternating current stimulation on subjective sleep quality. Brain Sci. (2018) 8:204. doi: 10.3390/brainsci8120204
73. Sheng J, Xie C, Fan DQ, Lei X, Yu J. High definition-transcranial direct current stimulation changes older adults' subjective sleep and corresponding resting-state functional connectivity. Int J Psychophysiol. (2018) 129:1–8. doi: 10.1016/j.ijpsycho.2018.05.002
74. Forogh B, Rafiei M, Arbabi A, Motamed MR, Madani SP, Sajadi S. Repeated sessions of transcranial direct current stimulation evaluation on fatigue and daytime sleepiness in Parkinson's disease. Neurol Sci. (2017) 38:249–54. doi: 10.1007/s10072-016-2748-x
75. Frase L, Maier JG, Zittel S, Freyer T, Riemann D, Normann C, et al. Bifrontal anodal transcranial direct current stimulation (tDCS) improves daytime vigilance and sleepiness in a patient with organic hypersomnia following reanimation. Brain Stimul. (2015) 8:844–6. doi: 10.1016/j.brs.2015.05.009
76. Galbiati A, Abutalebi J, Iannaccone S, Borsa VM, Musteata S, Zucconi M, et al. The effects of transcranial direct current stimulation (tDCS) on idiopathic hypersomnia: a pilot study. Arch Ital Biol. (2016) 154:1–5. doi: 10.12871/00039829201611
77. Hadoush H, Al-Sharman A, Khalil H, Banihani SA, Al-Jarrah M. Sleep quality, depression, and quality of life after bilateral anodal transcranial direct current stimulation in patients with Parkinson's disease. Med Sci Monit Basic Res. (2018) 24:198–205. doi: 10.12659/MSMBR.911411
78. Harvey MP, Lorrain D, Martel M, Bergeron-Vezina K, Houde F, Seguin M, et al. Can we improve pain and sleep in elderly individuals with transcranial direct current stimulation? - Results from a randomized controlled pilot study. Clin Interv Aging. (2017) 12:937–47. doi: 10.2147/CIA.S133423
79. Minichino A, Bersani FS, Spagnoli F, Corrado A, De Michele F, Calo WK, et al. Prefronto-cerebellar transcranial direct current stimulation improves sleep quality in euthymic bipolar patients: a brief report. Behav Neurol. (2014) 2014:876521. doi: 10.1155/2014/876521
80. Shill HA, Obradov S, Katsnelson Y, Pizinger R. A randomized, double-blind trial of transcranial electrostimulation in early Parkinson's disease. Mov Disord. (2011) 26:1477–80. doi: 10.1002/mds.23591
81. Wang HX, Wang L, Zhang WR, Xue Q, Peng M, Sun ZC, et al. Effect of transcranial alternating current stimulation for the treatment of chronic insomnia: a randomized, double-blind, parallel-group, placebo-controlled clinical trial. Psychother Psychosom. (2020) 89:38–47. doi: 10.1159/000504609
82. Crunelli V, Hughes SW. The slow (<1 Hz) rhythm of non-REM sleep: a dialogue between three cardinal oscillators. Nat Neurosci. (2010) 13:9–17. doi: 10.1038/nn.2445
83. Leger D, Debellemaniere E, Rabat A, Bayon V, Benchenane K, Chennaoui M. Slow-wave sleep: from the cell to the clinic. Sleep Med Rev. (2018) 41:113–32. doi: 10.1016/j.smrv.2018.01.008
84. Neske GT. The slow oscillation in cortical and thalamic networks: mechanisms and functions. Front Neural Circuits. (2015) 9:88. doi: 10.3389/fncir.2015.00088
85. Krueger JM, Rector DM, Roy S, Van Dongen HP, Belenky G, Panksepp J. Sleep as a fundamental property of neuronal assemblies. Nat Rev Neurosci. (2008) 9:910–9. doi: 10.1038/nrn2521
86. Chauvette S, Volgushev M, Timofeev I. Origin of active states in local neocortical networks during slow sleep oscillation. Cereb Cortex. (2010) 20:2660–74. doi: 10.1093/cercor/bhq009
87. Steriade M, Contreras D, Curro Dossi R, Nunez A. The slow (<1 Hz) oscillation in reticular thalamic and thalamocortical neurons: scenario of sleep rhythm generation in interacting thalamic and neocortical networks. J Neurosci. (1993) 13:3284–99. doi: 10.1523/JNEUROSCI.13-08-03284.1993
88. Fonteneau C, Redoute J, Haesebaert F, Le Bars D, Costes N, Suaud-Chagny MF, et al. Frontal transcranial direct current stimulation induces dopamine release in the ventral striatum in human. Cereb Cortex. (2018) 28:2636–46. doi: 10.1093/cercor/bhy093
89. Amzica F, Steriade M. Neuronal and glial membrane potentials during sleep and paroxysmal oscillations in the neocortex. J Neurosci. (2000) 20:6648–65. doi: 10.1523/JNEUROSCI.20-17-06648.2000
90. Bazhenov M, Timofeev I, Steriade M, Sejnowski TJ. Model of thalamocortical slow-wave sleep oscillations and transitions to activated States. J Neurosci. (2002) 22:8691–704. doi: 10.1523/JNEUROSCI.22-19-08691.2002
91. Hsu TY, Juan CH, Tseng P. Individual differences and state-dependent responses in transcranial direct current stimulation. Front Hum Neurosci. (2016) 10:643. doi: 10.3389/fnhum.2016.00643
92. Silvanto J, Pascual-Leone A. State-dependency of transcranial magnetic stimulation. Brain Topogr. (2008) 21:1–10. doi: 10.1007/s10548-008-0067-0
93. Molle M, Marshall L, Gais S, Born J. Grouping of spindle activity during slow oscillations in human non-rapid eye movement sleep. J Neurosci. (2002) 22:10941–7. doi: 10.1523/JNEUROSCI.22-24-10941.2002
94. Niethard N, Ngo HV, Ehrlich I, Born J. Cortical circuit activity underlying sleep slow oscillations and spindles. Proc Natl Acad Sci USA. (2018) 115:E9220–9. doi: 10.1073/pnas.1805517115
95. Steriade M, Timofeev I. Neuronal plasticity in thalamocortical networks during sleep and waking oscillations. Neuron. (2003) 37:563–76. doi: 10.1016/S0896-6273(03)00065-5
96. Zaehle T, Rach S, Herrmann CS. Transcranial alternating current stimulation enhances individual alpha activity in human EEG. PLoS ONE. (2010) 5:e13766. doi: 10.1371/journal.pone.0013766
97. Bliwise DL. Sleep in normal aging and dementia. Sleep. (1993) 16:40–81. doi: 10.1093/sleep/16.1.40
98. Murphy M, Huber R, Esser S, Riedner BA, Massimini M, Ferrarelli F, et al. The cortical topography of local sleep. Curr Top Med Chem. (2011) 11:2438–46. doi: 10.2174/156802611797470303
99. Murphy M, Riedner BA, Huber R, Massimini M, Ferrarelli F, Tononi G. Source modeling sleep slow waves. Proc Natl Acad Sci USA. (2009) 106:1608–13. doi: 10.1073/pnas.0807933106
100. Romero Lauro LJ, Rosanova M, Mattavelli G, Convento S, Pisoni A, Opitz A, et al. TDCS increases cortical excitability: direct evidence from TMS-EEG. Cortex. (2014) 58:99–111. doi: 10.1016/j.cortex.2014.05.003
101. DelRosso LM, Hoque R. The cerebellum and sleep. Neurol Clin. (2014) 32:893–900. doi: 10.1016/j.ncl.2014.07.003
102. Mander BA, Winer JR, Walker MP. Sleep and Human Aging. Neuron. (2017) 94:19–36. doi: 10.1016/j.neuron.2017.02.004
103. Mong JA, Cusmano DM. Sex differences in sleep: impact of biological sex and sex steroids. Philos Trans R Soc Lond B Biol Sci. (2016) 371:20150110. doi: 10.1098/rstb.2015.0110
104. Jones AP, Choe J, Bryant NB, Robinson CSH, Ketz NA, Skorheim SW, et al. Dose-dependent effects of closed-loop tACS delivered during slow-wave oscillations on memory consolidation. Front Neurosci. (2018) 12:867. doi: 10.3389/fnins.2018.00867
105. Ngo HV, Miedema A, Faude I, Martinetz T, Molle M, Born J. Driving sleep slow oscillations by auditory closed-loop stimulation-a self-limiting process. J Neurosci. (2015) 35:6630–8. doi: 10.1523/JNEUROSCI.3133-14.2015
Keywords: sleep, transcranial electrical stimulation, sleep oscillations, sleep pattern, subjective sleep, systematic review
Citation: Dondé C, Brunelin J, Micoulaud-Franchi J-A, Maruani J, Lejoyeux M, Polosan M and Geoffroy PA (2021) The Effects of Transcranial Electrical Stimulation of the Brain on Sleep: A Systematic Review. Front. Psychiatry 12:646569. doi: 10.3389/fpsyt.2021.646569
Received: 27 December 2020; Accepted: 19 April 2021;
Published: 07 June 2021.
Edited by:
Kai Wang, Anhui Medical University, ChinaReviewed by:
Wolnei Caumo, Clinical Hospital of Porto Alegre (HCPA), BrazilCopyright © 2021 Dondé, Brunelin, Micoulaud-Franchi, Maruani, Lejoyeux, Polosan and Geoffroy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Clément Dondé, Y2xlbWVudC5kb25kZUB1bml2LWdyZW5vYmxlLWFscGVzLmZy; orcid.org/0000-0002-5121-8769
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.