
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 17 March 2021
Sec. Psychopathology
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.635502
This article is part of the Research TopicNeurocognitive and Translational Science of Binge Eating: Understanding Mechanisms of Change.View all 8 articles
 Cristina Segura-Garcia1,2*†
Cristina Segura-Garcia1,2*† Marianna Rania2,3†
Marianna Rania2,3† Elvira Anna Carbone1,2†
Elvira Anna Carbone1,2† Renato de Filippis2,3†
Renato de Filippis2,3† Matteo Aloi2,3†
Matteo Aloi2,3† Mariarita Caroleo2,3†Gloria Grasso1,2Giuseppina Calabrò2,3Gilda Fazia2,3Filippo Antonio Staltari2,3Antonella Falvo2,3
Mariarita Caroleo2,3†Gloria Grasso1,2Giuseppina Calabrò2,3Gilda Fazia2,3Filippo Antonio Staltari2,3Antonella Falvo2,3 Valentina Pugliese2,3Raffaele Gaetano2,3
Valentina Pugliese2,3Raffaele Gaetano2,3 Luca Steardo Jr.2,3†Pasquale De Fazio2,3†
Luca Steardo Jr.2,3†Pasquale De Fazio2,3†Background: Binge eating disorder (BED) is clinically relevant by virtue of the global impairment, poor quality of life, and increased overall medical morbidity. The high comorbidity with psychiatric disorders, particularly depression, has received attention as a possible mediator of the poor outcome. Further, BED and depression share cognitive dysfunctions. This naturalistic and uncontrolled pilot study aimed at evaluating the efficacy of vortioxetine (VTX) on depressive symptoms in patients with BED, secondly the efficacy in improving a broad array of executive functions, and third to explore the effect on eating behavior and body weight.
Methods: This pilot study involved 30 patients with BED and comorbid MDD, treated with VTX for 24 weeks. Assessments were run at baseline (t0), 4 (t1), 8 (t2), 12 (t3), and 24 (t4) weeks. Changes in depressive symptoms (HDRS and BDI), executive functions, eating behaviors (binge frequency and severity, night eating, food addiction), and body weight were estimated after treatment with VTX through GLM.
Results: Significant improvements emerged after treatment with VTX in: depression (HDRS p < 0.001; BDI p = 0.002) regardless the dose of VTX and first diagnosis (BED/MDD), working memory (RAVLT acquisition p = 0.01, delay recall p < 0.001, RCFT percentage of recall p = 0.01, and Attentional Matrices p = 0.05), binge days frequency (p < 0.001), binge eating severity (BES p < 0.001), night eating (p = 0.001), food addiction (YFAS 2.0 p = 0.039), and body weight (p = 0.039). The improvement in depressive symptoms was associated with the concurrent improvement in night eating as assessed by the I-NEQ.
Conclusions: VTX can be a valid therapeutic choice for patients with BED with comorbid depression in controlling the depressive symptoms, working memory, and eating behavior. Indeed, by acting on affective symptoms, neurocognitive functioning, and eating behaviors, it confirms the results already obtained with VTX in other disorders, expanding them to BED.
Binge eating disorder (BED) is the most frequent among eating disorders. According to recent data, 0.85–3.6% of adults (1–4) meet the DSM-5 criteria for BED (5) and women are 1.3–3 times more likely than men to be affected (6, 7).
BED is clinically relevant by virtue of its psychological burden, global impairment and poor quality of life (1, 6, 8–11), as well as increased overall medical morbidity (12–14) and access to healthcare resources.
Notwithstanding the strong association with medical conditions, some evidence suggests that medical comorbidity alone does not fully explain the overall impairment observed in individuals suffering from BED (15, 16). To this extent, the high comorbidity with psychiatric disorders, particularly depression, has received attention as a possible moderator of the poor outcome in BED (6, 15, 16).
To date, up to 65.5 and 32.8% of individuals suffering from BED self-report a lifetime prevalence of major depressive disorder (MDD) and diagnosis of persistent depression, respectively (14). Further, individuals with BED suffer from cognitive dysfunctions (i.e., poor decision making, set-shifting, inhibitory control, planning, and working memory) (17–24) and depression has been associated with pronounced cognitive dysfunctions as well (25). Even though the exact mechanisms underlying the co-occurrence and inter-relationship between depression, cognitive deficits, and BED are not fully understood, the “common-cause” model (26) may suit with this comorbidity, with cognitive inefficiency underpinning either depression and BED.
On the other hand, in line with the emotional regulation theory (27), binge eating is hypothesized to occur as a strategy to cope with negative emotional affect, in the absence of more adaptive emotional regulation strategies that are under cognitive control. Accordingly, taking into account cognitive inefficiency, depression should be considered as either a trigger or a maintaining factor associated with BED.
Given that a greater loss of control over eating has been demonstrated in BED when depressive symptoms combine with cognitive dysfunction (28), and that evidence suggests that depression and BED should be studied together rather than as distinct and independent elements (15, 29, 30), approaching simultaneously depression, cognitive disturbances, and eating behaviors may theoretically provide a more complete understanding of the clinical complexity, and potentially result in more tailored treatment strategies and improved patient's outcome (31).
The recommended first-line approach for BED includes psychological treatments, such as cognitive behavioral and interpersonal therapies (32, 33); however, about one-third of patients do not fully benefit from these treatments (34) and the reduction in binging episodes and weight loss seems to be short-lasting (35–37).
Moreover, access to such interventions may be limited by local availability and costs. Various pharmacological treatments have been used so far and have shown some effectiveness in addressing binging and weight (topiramate, naltrexone), appetite regulation (sibutramine), obsessive thoughts and compulsive behaviors (lisdexamfetamine), and reducing anxiety and affective symptoms [e.g., selective serotonin reuptake inhibitors (SSRIs), serotonin–norepinephrine reuptake inhibitors (SNRIs), and bupropion], but none of these exhibited a combined effect on all the clinical features and they showed poor tolerability and negative or no effect on cognitive symptoms (38, 39). Current treatments for BED are poor in the long term and often insufficient, therefore additional clinical trials are needed to identify effective pharmacotherapies (40).
Vortioxetine (VTX) is an innovative antidepressant with a multimodal mechanism of action that associates blocking of the reuptake of the serotonin transporter with action on multiple serotonergic receptors (5-HT3, 5-HT7, and 5-HT1D receptor antagonists, 5-HT1A receptor agonist and 5-HT1B receptor partial agonist), as well as acting on other neurotransmitters such as noradrenaline, dopamine, acetylcholine, and glutamate (41–43). VTX has a favorable tolerability profile and seems to have the pharmacodynamic properties needed to improve both depression, and cognitive functioning (44, 45).
One double-blind, placebo-controlled study (46) examined the use of VTX in eighty subjects diagnosed with BED, finding no differences in binge-eating frequency, weight, and BMI between the VTX and placebo groups. Authors argued several explanations such as insufficient length of administration of the drug (12 weeks), high attrition rates, and high placebo effect. More importantly, comorbidity with major depressive disorder was voluntary considered an exclusion criterion, and it may have contributed to recruit less severe cases and prevented to observe those cases in which the efficacy on binge-eating is secondary to the amelioration of depressive symptoms.
Based on the above, this naturalistic and uncontrolled pilot study aimed at expanding actual knowledge, by evaluating the efficacy of 24-week treatment with VTX in individuals with comorbid BED and MDD. Changes in depressive symptoms were considered primary outcome. Secondly, the study examined the efficacy of VTX in improving a broad array of executive functions. Finally, the third objective was to explore if VTX has an effect on improving eating behavior (e.g., intended as severity of eating psychopathology and dysfunctional eating behaviors) and body weight. Our hypothesis is that VTX treatment will improve not only the depressive symptoms but also the neurocognitive functioning and altered eating behaviors of individuals suffering from both BED and MDD.
The study took place at the Center for Clinical Research and Treatment of Eating Disorders in Catanzaro (Italy), a tertiary multidisciplinary service providing outpatient mental health care to individuals with EDs, subsumed under the outpatient service of general psychiatry, University Hospital “Mater Domini”, Catanzaro (Italy). Individuals that consecutively referred to the outpatient unit since August 2017 to October 2019 for the treatment of BED, were screened for concurrent MDD, and considered eligible. Inclusion criteria were age 18–65 years, Binge Eating Scale (BES) (47) score > 17, Hamilton Depression Rating Scale (HDRS) (48) score > 17 and capable of answering self-report questionnaires and expressing valid consent. Participants were deemed ineligible if: diagnosis of intellectual disability from mild to severe according to DSM-5 (corresponding to IQ <70) (49); history of chronic medical illness or neurological conditions or medications affecting cognitive functioning; drug dependence and/or abuse; other severe medical comorbidities (e.g., epilepsy); pregnant, recently given birth or breastfeeding; previous diagnosis of diabetes mellitus or medications affecting glucose metabolism; known inflammatory disease; or a history of malignant disease.
The main researcher (CS-G) informed each participant individually about the aim of the study, the procedures, the voluntary nature of participation, and the management and storage of data. Participants were duly informed about the possible side effects with VTX, given the chance to leave the study at any time and asked to sign written informed consent to participate before any procedure took place. A statistical power analysis was performed with Gpower 3.1 for sample size estimation; with an alpha = 0.05 and a power = 0.80, the projected sample size needed with an effect size = 0.25 was minimum 24 participants. A total of 41 individuals were found to be eligible for the study.
The study was designed as follows: initial clinical interview, psychometric assessment and prescription of VTX were considered baseline (t0), and then psychometric assessment was rerun according to the study design timing (t1: 4 weeks; t2: 8 weeks; t3: 12 weeks; t4: 24 weeks) during the 24-week follow-up period (Table 1). Eleven participants were excluded from the study for the following reasons: four (3 males, 1 female) were not interested; two (1 man, 1 woman) had personal problems that prevented them from participating in the assessments; one became pregnant between t2 and t3; and four dropped out due to side effects (between t0 and t2). Data collection began in August 2017 and stopped in October 2019, when 24 weeks of data for all 30 patients had been retrieved.
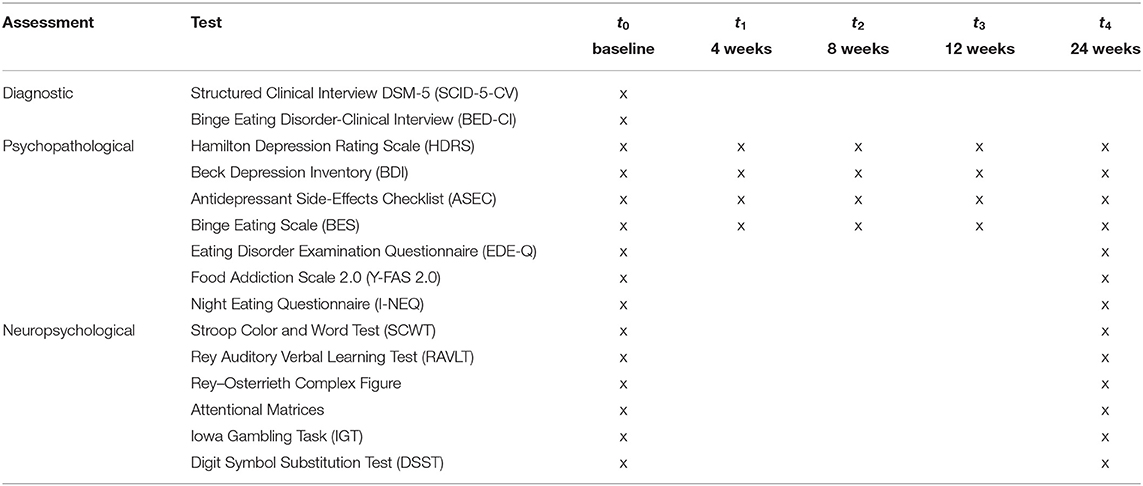
Table 1. Evaluation schedule of assessments.
Participants were asked not to modify either their eating habits or physical activity during the 24 weeks of treatment in order to avoid possible confounding effects on body weight; no additional therapy (e.g., psychotherapy, pharmacotherapy) other than VTX was prescribed.
The investigation was approved by the Ethical Committee of “Regione Calabria, sezione Area Centro” (identifier: 185/D.G. 20.07.2017), in accordance with the latest version of the Declaration of Helsinki (50).
Well-trained psychiatrists in the ED field evaluated each patient the day of the first registration to the ED unit: patients underwent a clinical interview resulting in a DSM-5 diagnosis (mean time: 45 min), completed the HDRS with the same psychiatrist and answered the BES and the Beck Depression Inventory (BDI) (51). Diagnosis were based on the Structured Clinical Interview for DSM-5 (SCID-5-CV) (52) and the Binge Eating Disorder-Clinical Interview (BED-CI) (53). Once the diagnosis was clear, patients were invited to participate in the study. After a maximum of 1 week, the patients signed the informed consent and completed the baseline evaluation; this assessment took on average 70 min and included psychopathological (around 20 min) and neuropsychological (around 50 min) tests performed by a trained psychologist.
Psychopathological tests included the Eating Disorder Examination Questionnaire (EDE-Q) (54), the Night Eating Questionnaire (I-NEQ) (55) and the Yale Food Addiction Scale 2.0 (YFAS 2.0) (56). Neuropsychological assessment included: the Stroop Color and Word Test (SCWT; 45 s test period for each of the three sheets) (57), the Rey-Osterreith Complex Figure Test (RCFT) (58), the Iowa Gambling Task (IGT) (59), the Attentional Matrices (45 s test period for each of the three matrices) (60), the Rey Auditory Verbal Learning Test (RAVLT) (61), and the Digit Symbol Substitution Test (DSST; 45 s test period) (62). Successive administrations of psychometric tests/questionnaire followed the study design and timeline (Table 1).
Patients were measured wearing light indoor clothing and no shoes by means of a portable stadiometer and a balance scale; their height to the nearest 0.1 cm and weight to the nearest 0.1 kg were taken and their body mass index (BMI, kg/m2) was calculated. BMI was measured at each assessment.
Patient started therapy with VTX the day after completing all the evaluations at baseline. VTX is taken once daily without any regard to meals. The starting dosage was 5 mg/day, which was up- or down-titrated within the range of 5–20 mg/day according to efficacy (investigator's clinical judgement) and tolerability. Side effects were recorded at each assessment using the Antidepressant Side-Effects Checklist (ASEC) (63).
IBM SPSS Statistics (version 26.0) software was used for database construction and statistical analysis. Data are presented as means, standard deviations (SD), frequencies, and percentages (%). Missing data were managed with the regression imputation method, which replaces the missing data with estimated values. Instead of deleting any case that has a missing value, this approach preserves all cases by replacing the missing data with a probable value estimated by other available information. In the regression imputation, the existing variables are used to make a prediction and then the predicted value is substituted as if it were an actual obtained value. After all missing values have been replaced by this approach, the dataset was analyzed using standard techniques for complete data.
A General Linear Model (GLM) with repeated measures was used to evaluate the changes of measures across time. Possible confounding variables were included in the analysis as covariates (i.e., depressive symptomatology improvement, BED/MDD as first diagnosis). Eta-squared (η2) was used as a measure of the side effects of the GLM, considering values of 0.01, 0.06, and 0.14 as indicating small, medium, and large effects, respectively. The IGT, RCFT, RAVLT, SCWT, DSST, and Attentional Matrices were not normally distributed according to the Kolmogorov-Smirnov test, therefore the Wilcoxon test was run to analyse the differences between t0 and t4; r was calculated as a measure of the effect size of the Wilcoxon test, considering values of 0.10–0.29, 0.30–0.49, and ≥ 0.5 to be indicative of small, moderate, and large effects, respectively. McNemar non-parametric test was used to compare the proportion of patients positive to YFAS 2.0 before and after treatment. Considering the exploratory and naturalistic approach, p < 0.05 was considered to be significant. The Benjamini-Hochberg procedure (64, 65) was used to correct for multiple comparisons.
A total of 30 from 35 participants (85.7%) completed the study. Causes of dropouts were: one patient became pregnant between t2 and t3, three patients had moderate to severe nausea (between t0 and t1), and one patient suffered unbearable vomiting (between t2 and t3).
The mean daily dose of VTX taken by completers was 15.8 ± 5.6 mg (median = 20 mg) and the mean dose among dropouts was 12.6 ± 5.6 mg (median = 15 mg). Table 2 shows the main demographics. Women, high school education level and people not occupationally active were the most frequent parameters. Twenty participants (66.7%) referred an earlier onset of BED with respect to MDD (Table 2).
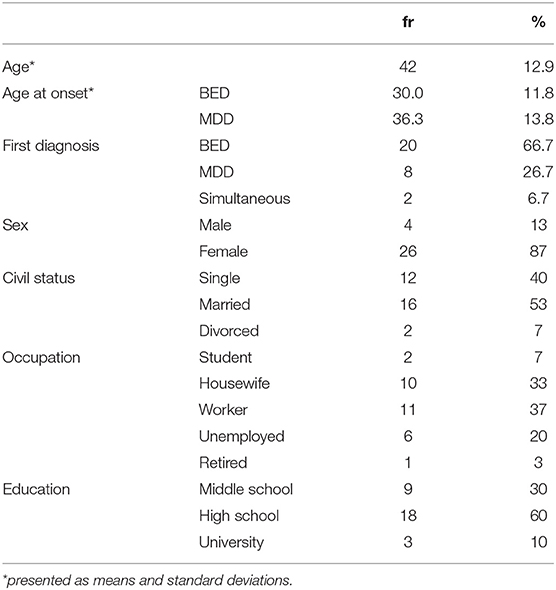
Table 2. Sample description.
The primary endpoint was the change in HDRS and BDI scores from baseline. Depression significantly reduced overtime, as demonstrated by both the HDRS (p < 0.001) and the BDI (p = 0.002) scores (Figure 1). Large effect sizes were evident in all cases. Differences remained significant when controlling for VTX dosage and first diagnosis (i.e., BED/MDD onset). The rates of remission were respectively, 36.7% and 23.3 for HDRS (≤7) and BDI (≤9).
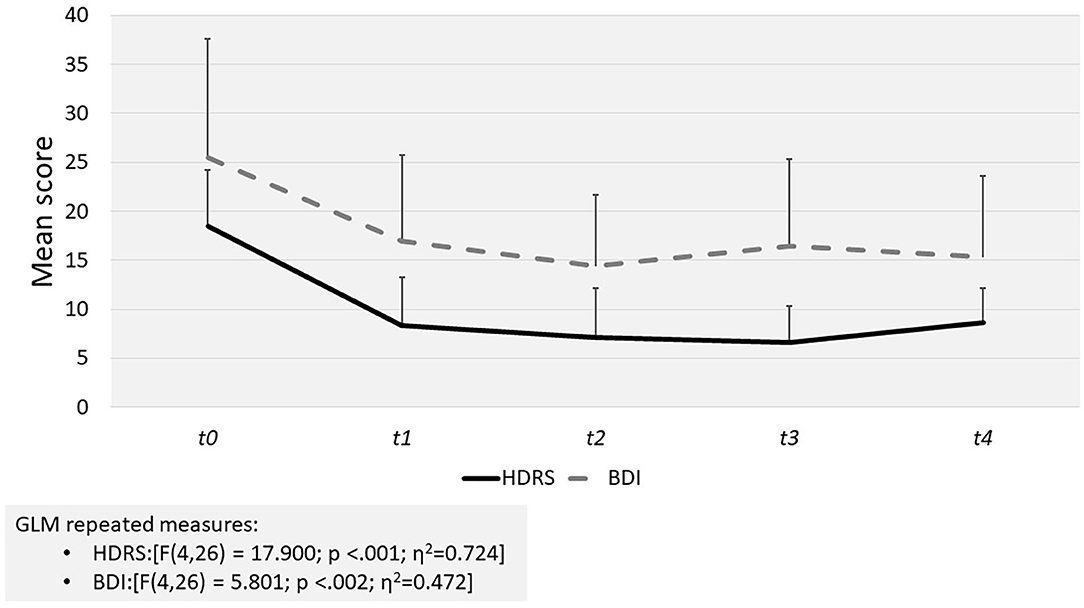
Figure 1. Results of GLM repeated measures for self-report (BDI) and clinician rated (HDRS) depression tests scores.
The secondary endpoint was the change in neurocognition scores (Table 3). Significant improvement was evident in the RCFT percentage of recall (p = 0.01), the RAVLT acquisition (p = 0.01), and delay recall (p < 0.001) and Attentional Matrices (p = 0.05) after treatment, otherwise an improvement in the RCFT order (p = 0.069) was observed. No differences related to the IGT, SCWT, and DSST scores were found.
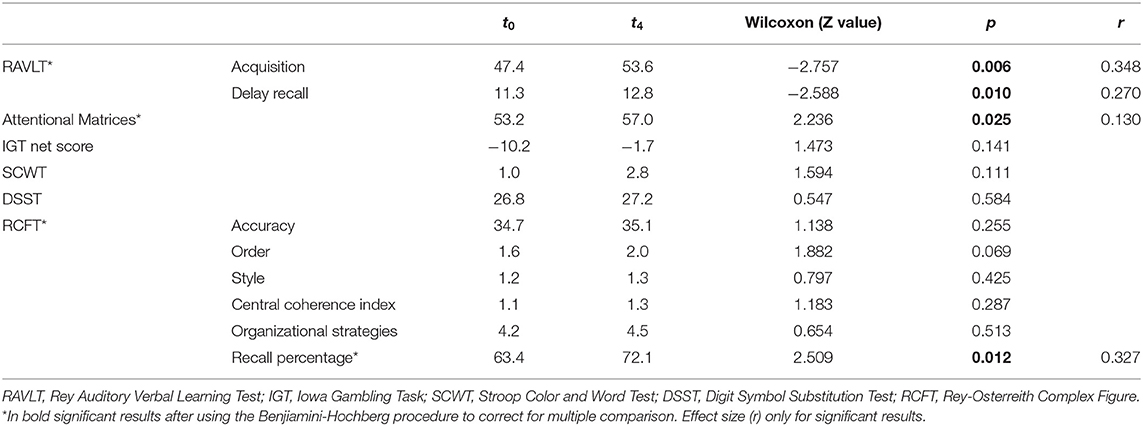
Table 3. Neurocognitive testing: Wilcoxon test.
The third endpoint were the changes in eating behavior and body weight (Table 4). Mean BMI decreased after treatment (p = 0.039) but the reduction was not significant after applying the Benjamini-Hochberg procedure for multiple comparison (p < 0.03); instead, significant reductions in the BES (p < 0.001), and I-NEQ (p = 0.001) scores were evident; the EDE-Q did not change. The percentage of patients meeting the criteria for food addiction (YFAS 2.0) was significantly lower after treatment (t0 = 70% vs. t4 = 46.7%; McNemar's test = 4.000; p = 0.039). The average frequency of weekly binge days significantly decreased from t0 = 4.9 ± 1.9 days a week to t4 = 2.7 ± 2.4 days a week (p < 0.001). After controlling for changes in depression and first diagnosis (i.e., BED or MDD), the reduction in BES and the weekly binge days remained significant; on the other hand, a significant effect of changes in depression on I-NEQ score emerged (p = 0.009).
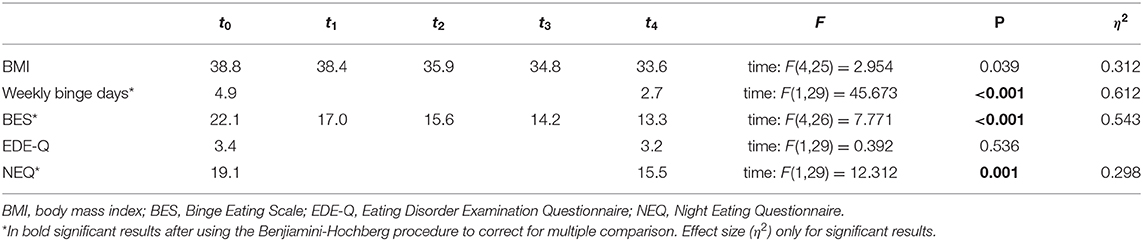
Table 4. Body Mass Index and eating behavior: GLM repeated measures.
This study aimed at evaluating the efficacy of VTX on depressive symptoms, executive functions, eating behavior, and body weight in individuals with comorbid BED and MDD. BED most likely involves abnormalities in three domains regulating eating behavior: the ancestral 'peripheral-hypothalamic' feedback system, the reward system, and the top-down control circuitry (66). Thus, on a neurochemical level, BED may be related to the dysfunction of the serotonergic, dopaminergic, noradrenergic, and glutamatergic pathways (67). This tri-monoaminergic neurotransmitter system, with the recent focusing on glutamate, is the pathophysiology basis of depression as well, and still leads existing treatment options (68, 69). Therefore, a medication to target binge eating, as well as BED in comorbidity with depression, needs to be multi-modal in terms of its pharmacology, and VTX pharmacological profile theoretically addresses all these needs (70).
The main finding of the study was an improvement of depressive symptoms, working memory and disordered eating behavior following treatment with VTX. To the best of our knowledge, this is the first study to show this improvement.
VTX has already confirmed its efficacy in major depressive episode, in adults and elderly patients, with specific effect on cognitive impairment and physical symptoms (71–77), nonetheless, there are still no studies demonstrating its effectiveness in patients suffering from depression and BED.
As above mentioned, only one study examined the use of VTX in BED, and voluntarily excluded comorbidity with MDD in order “to avoid the confounding variable in a small sample of depression possibly worsening the binge behavior” (46). However, the role of depressive symptoms in BED is still debated and current evidence suggests that the two phenomena should be studied together rather than as distinct and independent elements (15, 29, 30).
In this regard, our results showed an improvement in both self-report and clinician-rated depression, independent of which disorder came first (i.e., BED or MDD). Thus, the reduction of depressive symptoms among patients with MDD and BED is comparable to that reported in the literature for other patients with MDD without this comorbidity treated with VTX (78–80).
The low number of dropouts confirms the good tolerability of VTX. Common side effects were similar to those previously reported (45, 81–83), quite easy to manage and not life-threatening. The favorable tolerability profile of VTX can promote adherence to treatment, which is an important factor for therapeutic success.
Working memory significantly improved within the treatment. Working memory is crucial for several cognitive processes in daily life (84, 85), and depression affects both the phonological loop and visuospatial sketch pad of working memory (86).
Our results put in evidence the improvement of verbal (i.e., the RAVLT) and visual (i.e., the RCFT recall) memory, although the DSST score was unchanged after treatment. Other studies previously examined the efficacy of VTX on the RAVLT in patients with depression and reported significant improvement in the verbal memory domain (75, 87, 88).
This is the first study reporting a positive change in visual memory using the RCFT (i.e., RCFT recall) in the context of the efficacy of VTX. These results should be read in light of the concurrent observed improvement in the attentional domain (i.e., Attentional Matrices). It can be speculated that there is an interplay between attentional capabilities and further working memory performance. This is very important because previous studies demonstrated visuospatial memory deficits (89) and impaired performance on the RCFT recall due to poor visual attention (17, 19) among BED patients.
In our study, slight but not significant changes were evident for the IGT, SCWT, and DSST after treatment. The difference between ours and others' studies deserves further explanation. The first difference regards the sample: ours are patients with comorbid BED and MDD; instead, in most studies (75, 87, 90) patients had only the diagnosis of MDD. Other researchers reported significant differences in these tests after treatment with VTX (91); nonetheless, it is known that positive outcomes of treatment on cognitive functioning are bigger among those patients occupationally active independently of the improvement of depression (90), whilst our different results could be explained not only by the smaller sample size but also in that people who did not work were overrepresented in our sample. Importantly, previous protocols used a longer administration time for the DSST (i.e., 90–120 s vs. 45 of our protocol) enabling the comparison with present results (87, 88).
Notwithstanding the improvement in different cognitive functions, it is not possible to ascertain if this effect remained over and beyond the improvement in depression as previous studies reported in patients with MDD (75, 92–94). Recently, the potential role of depression on neuropsychological performances of patients with eating disorders, in particular patients with Anorexia Nervosa (AN) (95, 96) and Bulimia Nervosa (BN) (97, 98) have been investigated. More specifically, the association between poor performance on the neuropsychological tests and the diagnosis of AN weakened after adjusting for depression, and the authors argued that cognitive impairment may be overestimated if depression is not taken into account. Contrarily to AN, who still perform worse than HC after controlling for depressive symptoms, depression explains the whole cognitive impairment among patients with BN (98). Summing up, although previous studies demonstrated a direct effect of VTX on cognitive improvement independent of changes in depressive symptoms (75, 92–94), future studies should ascertain the unique effect of VTX on the neurocognitive profile of patients with comorbid BED and MDD.
The peculiar multimodal mechanism of action of VTX has previously been demonstrated not to affect the body weight of patients in the short or long term (41, 83), even though a clinically significant weight reduction was observed in previous clinical studies (45, 99, 100). A nearly statistically significant weight reduction (overall, 5 points of BMI) after 24 weeks of treatment with VTX was evident in our sample. As the participants were patients with BED and we controlled weight loss after a longer follow-up, our results are not comparable with the above-mentioned studies.
Present results confirm that binge eating frequency reduced across the time under treatment with VTX, supporting Grant et al. (46) findings. On the contrary, we additionally found a significant improvement of BES score after 24 weeks, probably due to the longer duration of our trial. A modest efficacy of antidepressants in the short-term reduction of binge episodes in BED, with no significant impact on weight, emerged in a recent meta-analysis but the results in long-term studies are disappointing (101). SSRI antidepressants seem relatively well-tolerated but some patients experienced side effects (39). Moreover, weight gain is a common adverse event associated with some SSRIs and SNRIs (102–104). Studies with other classes of antidepressants, such as SNRIs (105) and bupropion (106), have shown discordant results on binge improvement or weight loss in BED. More recently, the association of naltrexone/bupropion (extended release) has proved to be effective in reducing BMI and altered eating behaviors in obese patients with BED in a 16-week study (107); however, the authors did not find changes in depressive symptoms. Herein, although depressive symptoms improved, they did not affect the improvement in binge eating outcomes, that most likely improved by virtue of the multimodal targeted action of VTX on the serotoninergic pathways.
The NEQ scores also decreased after treatment with VTX. Of note, this improvement was associated with the concurrent improvement in depressive symptoms. Previous studies supported an association between night eating and both depressed mood (108) and BED (109). Others pointed out that nocturnal hyperphagia or binging behaviors, and the consequential weight gain in these patients may reflect an alteration in the serotonin system for regulating appetite and food intake (110). Present results suggest a direct mediation effect of depression improvement in night eating behavior.
Food addiction is uniquely associated with BED, with prevalence estimates of food addiction up to 92% in individuals with BED (111, 112). Given the high co-occurrence and symptoms overlap (e.g., loss of control over eating, access to food despite negative consequences, failed attempts to quit) (113), BED and food addiction may be hard to disentangle. Furthermore, food addiction positively correlates with depressive symptoms in non-clinical adolescent sample (114) and in adolescents with obesity seeking weight-loss treatment (115), and the more severe depressive symptoms, the more likely the odds of having severe food addiction is (OR = 13.2, for severe depression; OR = 15.6 for extremely severe depression) (116).
In present study, the percentage of patients with MDD and BED fulfilling diagnostic threshold for food addiction significantly decreased after treatment. To date, there is no evidence of pharmacological interventions targeting food addiction. Given that some of the major symptoms of food addiction are thought to be under the serotoninergic control (e.g., craving, impulsivity) (117, 118), this result could be explained with the unique effect of VTX. However, the mediating effect of the improvement in both binge eating and depression cannot be excluded, then this result should be taken cautiously, and need to be replicated.
General eating psychopathology did not improve within the treatment with VTX. A possible explanation may be that EDE-Q total score mostly assesses cognitive domains related to eating disorders, such as eating concern, shape concern, and weight concern, and only considers restriction among eating behaviors. Accordingly, we can speculate that the EDE-Q total score may not be so accurate in detecting short-term improvements in patients with BED, especially considering that higher levels of restriction after treatment might be expected.
BED and MDD may share underpinning dysfunctions of the serotonergic, dopaminergic, noradrenergic, and glutamatergic pathways (66). Therefore, a multimodal medication in terms of its pharmacology, and the pharmacological profile such as VTX, may be theoretically an effective option to target the comorbidity between BED and MDD (70).
Study strengths include rigid inclusion criteria, which avoided the introduction of unmeasured bias (e.g., other treatments), and strict analysis controlling for multiple testing. The selection of patients with concurrent BED and MDD let us consider a subsample with more severe general psychopathology, which may respond better in terms of eating psychopathology thanks to the treatment for depression itself. In fact, excluding these patients from the evaluation could introduce severity bias, and a failure in detecting those improvements in eating psychopathology accounted by concurrent depressive symptoms. Therefore, either self-report and clinician rated depression severity was evaluated, giving more consistency and completeness to results. HDRS is considered the gold standard for evaluating depression in trials (119, 120), showing good sensitivity in capturing the effectiveness of pharmacological treatments (121, 122).
Notwithstanding the efficacy of VTX on BED and concurrent depression, present results should be read in light of some limitations. The naturalistic uncontrolled design, specifically the lack of a control group, prevented to conclude if the efficacy of VTX is comparable to other treatments currently used for BED (pharmacological or psychotherapy) or placebo. The follow-up was large enough to catch psychopathological and anthropometrical improvements (titration time plus latency time before efficacy of VTX), however we cannot support this improvement is maintained in the long-term. Failure in outcomes in the long-term is one of the most critical points in the existing literature on BED, so further studies, with larger follow-up are encouraged to confirm present results. Lastly, we selected seeking-active treatment patients with BED and concurrent MDD, given the very high comorbidity of these two disorders in the real-life clinical setting. However, these patients may suffer from more severe psychopathology, accordingly present results cannot be generalized to patients with BED without the comorbidity or to patients that actually do not seek treatment or to less severe cases.
In summary, this longitudinal open-label study shows that VTX may be a valid therapeutic choice for patients with BED with comorbid depression in controlling their depressed mood, their working memory and their eating behavior. Indeed, by acting on affective symptoms, neurocognitive functioning and eating behaviors, it confirms some results already obtained with VTX in other disorders, expanding them to BED. Finally, a better characterization of patients with BED that takes into account other psychiatric comorbidities, especially mood disorders, seems necessary.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethical Committee of Regione Calabria, sezione Area Centro (identifier: 185/D.G. 20.07.2017). The patients/participants provided their written informed consent to participate in this study.
CS-G and PDF contributed to the conception and design of the study. MC, GC, GF, FS, AF, and GG organized the database. CS-G performed the statistical analysis. RdF, MA, MR, EC, and LS wrote the first draft of the manuscript. VP and RG critically revised the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
This study was supported by a grant from Lundbeck Italy. This study was carried out independently by the centre, receiving only a partial unrestricted grant from Lundbeck Italia. The sponsor had no role in the design and the conduct of the study, collection, management, analysis, and interpretation of the data. The authors have independently written the manuscript; the preparation, review, or approval and the decision to submit the manuscript for publication was autonomously taken by the authors.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors are grateful to patients who took part in this study.
ASEC, Antidepressant Side-Effects Checklist; BDI, Beck Depression Inventory; BED, Binge eating disorder; BED-CI, Binge Eating Disorder-Clinical Interview; BES, Binge Eating Scale; BMI, body mass index; DSST, Digit Symbol Substitution Test; EDE-Q, Eating Disorder Examination Questionnaire; GLM, General Linear Model; HDRS, Hamilton Depression Rating Scale; IGT, Iowa Gambling Task; NEQ, Night Eating Questionnaire; RAVLT, Rey Auditory Verbal Learning Test; RCFT, Rey-Osterreith Complex Figure Test; SCID-5-CV, Structured Clinical Interview for DSM-5; SCWT, Stroop Color and Word Test; SD, standard deviation; SNRIs, serotonin–norepinephrine reuptake inhibitors; SSRIs, selective serotonin reuptake inhibitors; VTX, vortioxetine; YFAS 2.0, Yale Food Addiction Scale 2.0.
1. Udo T, Grilo CM. Prevalence and correlates of DSM-5-defined eating disorders in a nationally representative sample of U.S. adults. Biol Psychiatry. (2018) 84:345–54. doi: 10.1016/j.biopsych.2018.03.014
2. Stice E, Marti CN, Rohde P. Prevalence, incidence, impairment, and course of the proposed DSM-5 eating disorder diagnoses in an 8-year prospective community study of young women. J Abnorm Psychol. (2013) 122:445–57. doi: 10.1037/a0030679
3. Cossrow N, Pawaskar M, Witt EA, Ming EE, Victor TW, Herman BK, et al. Estimating the prevalence of binge eating disorder in a community sample from the United States: comparing DSM-IV-TR and DSM-5 criteria. J Clin Psychiatry. (2016) 77:e968–74. doi: 10.4088/JCP.15m10059
4. Hudson JI, Coit CE, Lalonde JK, Pope HG. By how much will the proposed new DSM-5 criteria increase the prevalence of binge eating disorder? Int J Eat Disord. (2012) 45:139–41. doi: 10.1002/eat.20890
5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. DSM-5. 5th ed. Arlington, VA: American Psychiatric Publishing (2013). doi: 10.1176/appi.books.9780890425596
6. Hudson JI, Hiripi E, Pope HG, Kessler RC. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol Psychiatry. (2007) 61:348–58. doi: 10.1016/j.biopsych.2006.03.040
7. Hay P, Girosi F, Mond J. Prevalence and sociodemographic correlates of DSM-5 eating disorders in the Australian population. J Eat Disord. (2015) 3:19. doi: 10.1186/s40337-015-0056-0
8. Vancampfort D, De Herdt A, Vanderlinden J, Lannoo M, Soundy A, Pieters G, et al. Health related quality of life, physical fitness, and physical activity participation in treatment-seeking obese persons with and without binge eating disorder. Psychiatry Res. (2014) 216:97–102. doi: 10.1016/j.psychres.2014.01.015
9. Hsu LKG, Mulliken B, McDonagh B, Das SK, Rand W, Fairburn CG, et al. Binge eating disorder in extreme obesity. Int J Obes. (2002) 26:1398–403. doi: 10.1038/sj.ijo.0802081
10. Rieger E, Wilfley DE, Stein RI, Marino V, Crow SJ. A comparison of quality of life in obese individuals with and without binge eating disorder. Int J Eat Disord. (2005) 37:234–40. doi: 10.1002/eat.20101
11. Dakanalis A, Riva G, Serino S, Colmegna F, Clerici M. Classifying adults with binge eating disorder based on severity levels. Eur Eat Disord Rev. (2017) 25:268–74. doi: 10.1002/erv.2518
12. Succurro E, Segura-Garcia C, Ruffo M, Caroleo M, Rania M, Aloi M, et al. Obese patients with a binge eating disorder have an unfavorable metabolic and inflammatory profile. Medicine. (2015) 94:e2098. doi: 10.1097/MD.0000000000002098
13. Thornton LM, Watson HJ, Jangmo A, Welch E, Wiklund C, von Hausswolff-Juhlin Y, et al. Binge-eating disorder in the Swedish national registers: somatic comorbidity. Int J Eat Disord. (2017) 50:58–65. doi: 10.1002/eat.22624
14. Udo T, Grilo CM. Psychiatric and medical correlates of DSM-5 eating disorders in a nationally representative sample of adults in the United States. Int J Eat Disord. (2019) 52:42–50. doi: 10.1002/eat.23004
15. Singleton C, Kenny TE, Hallett D, Carter JC. Depression partially mediates the association between binge eating disorder and health-related quality of life. Front Psychol. (2019) 10:209. doi: 10.3389/fpsyg.2019.00209
16. Masheb RM, Grilo CM. Quality of life in patients with binge eating disorder. Eat Weight Disord. (2004) 9:194–9. doi: 10.1007/BF03325066
17. Aloi M, Rania M, Caroleo M, Bruni A, Palmieri A, Cauteruccio MA, et al. Decision making, central coherence and set-shifting: a comparison between binge eating disorder, anorexia nervosa and healthy controls. BMC Psychiatry. (2015) 15:6. doi: 10.1186/s12888-015-0395-z
18. Kittel R, Brauhardt A, Hilbert A. Cognitive and emotional functioning in binge-eating disorder: a systematic review. Int J Eat Disord. (2015) 48:535–54. doi: 10.1002/eat.22419
19. Aloi M, Rania M, de Filippis R, Segura-Garcia C. Weight and age do not account for a worse executive functioning among BED-obese patients. Eat Weight Disord. (2020) 25:373–7. doi: 10.1007/s40519-018-0608-9
20. Blume M, Schmidt R, Hilbert A. Executive functioning in obesity, food addiction, and binge-eating disorder. Nutrients. (2018) 11:54. doi: 10.3390/nu11010054
21. Kollei I, Rustemeier M, Schroeder S, Jongen S, Herpertz S, Loeber S. Cognitive control functions in individuals with obesity with and without binge-eating disorder. Int J Eat Disord. (2018) 51:233–40. doi: 10.1002/eat.22824
22. Giel KE, Teufel M, Junne F, Zipfel S, Schag K. Food-related impulsivity in obesity and binge eating disorder-a systematic update of the evidence. Nutrients. (2017) 9:1170. doi: 10.3390/nu9111170
23. Eneva KT, Arlt JM, Yiu A, Murray SM, Chen EY. Assessment of executive functioning in binge-eating disorder independent of weight status. Int J Eat Disord. (2017) 50:942–51. doi: 10.1002/eat.22738
24. Caroleo M, Primerano A, Rania M, Aloi M, Pugliese V, Magliocco F, et al. A real world study on the genetic, cognitive, and psychopathological differences of obese patients clustered according to eating behaviours. Eur Psychiatry. (2018) 48:58–64. doi: 10.1016/j.eurpsy.2017.11.009
25. Roberts ME, Tchanturia K, Treasure JL. Exploring the neurocognitive signature of poor set-shifting in anorexia and bulimia nervosa. J Psychiatr Res. (2010) 44:964–70. doi: 10.1016/j.jpsychires.2010.03.001
26. Lilenfeld LRR, Wonderlich S, Riso LP, Crosby R, Mitchell J. Eating disorders and personality: a methodological and empirical review. Clin Psychol Rev. (2006) 26:299–320. doi: 10.1016/j.cpr.2005.10.003
27. Waller G, Ohanian V, Meyer C, Osman S. Cognitive content among bulimic women: the role of core beliefs. Int J Eat Disord. (2000) 28:235–41. doi: 10.1002/1098-108X(200009)28:2<235::AID-EAT15>3.0.CO;2-1
28. Dingemans AE, Visser H, Paul L, van Furth EF. Set-shifting abilities, mood, and loss of control over eating in binge eating disorder: an experimental study. Psychiatry Res. (2015) 230:242–8. doi: 10.1016/j.psychres.2015.09.001
29. Lenzo V, Barberis N, Cannavò M, Filastro A, Verrastro V, Quattropani M. The relationship between alexithymia, defense mechanisms, eating disorders, anxiety, and depression. Riv Psichiatr. (2020) 55:24–30. doi: 10.1708/3301.32715
30. Kim O, Kim MS, Kim J, Lee JE, Jung H. Binge eating disorder and depressive symptoms among females of child-bearing age: the Korea Nurses' Health Study. BMC Psychiatry. (2018) 18:13. doi: 10.1186/s12888-018-1601-6
31. Pincus HA, Tew JD, First MB, First MB. Psychiatric comorbidity: is more less? World Psychiatry. (2004) 3:18–23.
32. Grilo CM. Psychological and behavioral treatments for binge-eating disorder. J Clin Psychiatry. 78(Suppl. 1):20–4. doi: 10.4088/JCP.sh16003su1c.04
33. Wilson GT. Treatment of binge eating disorder. Psychiatr Clin North Am. (2011) 34:773–83. doi: 10.1016/j.psc.2011.08.011
34. Linardon J. Rates of abstinence following psychological or behavioral treatments for binge-eating disorder: meta-analysis. Int J Eat Disord. (2018) 51:785–97. doi: 10.1002/eat.22897
35. John M. Eisenberg Center for Clinical Decisions and Communications Science. Management and outcomes of binge-eating disorder in adults: current state of the evidence. In: Comparative Effectiveness Review Summary Guides for Clinicians. Rockvil, MD: Agency for Healthcare Research and Quality (US) (2016).
36. Smink FRE, Van Hoeken D, Hoek HW. Epidemiology, course, and outcome of eating disorders. Curr Opin Psychiatry. (2013) 26:543–8. doi: 10.1097/YCO.0b013e328365a24f
37. Berkman ND, Brownley KA, Peat CM, Lohr KN, Cullen KE, Morgan LC, et al. Management and outcomes of binge-eating disorder. Comp Eff Rev. (2015) 160:1–203.
38. Appolinario JC, Nardi AE, McElroy SL. Investigational drugs for the treatment of binge eating disorder (BED): an update. Expert Opin Investig Drugs. (2019) 28:1081–94. doi: 10.1080/13543784.2019.1692813
39. Amodeo G, Cuomo A, Bolognesi S, Goracci A, Trusso MA, Piccinni A, et al. Pharmacotherapeutic strategies for treating binge eating disorder. Evidence from clinical trials and implications for clinical practice. Expert Opin Pharmacother. (2019) 20:679–90. doi: 10.1080/14656566.2019.1571041
40. Hilbert A. Binge-eating disorder. Psychiatr Clin North Am. (2019) 42:33–43. doi: 10.1016/j.psc.2018.10.011
41. de Bartolomeis A, Fagiolini A, Maina G. Vortioxetine in the treatment of major depression. Riv Psichiatr. (2016) 51:215–30. doi: 10.1708/2596.26720
42. Chen G, Højer AM, Areberg J, Nomikos G. Vortioxetine: clinical pharmacokinetics and drug interactions. Clin Pharmacokinet. (2018) 57:673–86. doi: 10.1007/s40262-017-0612-7
43. Leiser SC, Li Y, Pehrson AL, Dale E, Smagin G, Sanchez C. Serotonergic regulation of prefrontal cortical circuitries involved in cognitive processing: a review of individual 5-HT receptor mechanisms and concerted effects of 5-HT receptors exemplified by the multimodal antidepressant vortioxetine. ACS Chem Neurosci. (2015) 6:970–86. doi: 10.1021/cn500340j
44. Sanchez C, Asin KE, Artigas F. Vortioxetine, a novel antidepressant with multimodal activity: review of preclinical and clinical data. Pharmacol Ther. (2015) 145:43–57. doi: 10.1016/j.pharmthera.2014.07.001
45. Gonda X, Sharma SR, Tarazi FI. Vortioxetine: a novel antidepressant for the treatment of major depressive disorder. Expert Opin Drug Discov. (2019) 14:81–9. doi: 10.1080/17460441.2019.1546691
46. Grant JE, Valle S, Cavic E, Redden SA, Chamberlain SR. A double-blind, placebo-controlled study of vortioxetine in the treatment of binge-eating disorder. Int J Eat Disord. (2019) 52:786–94. doi: 10.1002/eat.23078
47. Gormally J, Black S, Daston S, Rardin D. The assessment of binge eating severity among obese persons. Addict Behav. (1982) 7:47–55. doi: 10.1016/0306-4603(82)90024-7
48. Bagby RM, Ryder AG, Schuller DR, Marshall MB. The Hamilton Depression Rating Scale: has the gold standard become a lead weight? Am J Psychiatry. (2004) 161:2163–77. doi: 10.1176/appi.ajp.161.12.2163
49. Gluck S. Mild, Moderate, Severe Intellectual Disability Differences. HealthyPlace (2014). Available online at: https://www.healthyplace.com/neurodevelopmental-disorders/intellectual-disability/mild-moderate-severe-intellectual-disability-differences (accessed February 8, 2021).
50. World Medical Association. WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects. (2018). Available online at: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/
51. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. (1961) 4:561–71. doi: 10.1001/archpsyc.1961.01710120031004
52. First MB. SCID-5-CV: Structured Clinical Interview for DSM-5 Disorders, Clinician Version. Arlington, VA: American Psychiatric Association (2016).
53. Spitzer R, Yanovsky S, Marcus M. Binge Eating Clinical Interview. Pittsburgh, PA: HaPI Record (1994).
54. Fairburn CG, Beglin SJ. Assessment of eating disorders: interview or self-report questionnaire? Int J Eat Disord. (1994) 16:363–70.
55. Aloi M, Rania M, De Fazio P, Vinai P, Tagliabue A, Allison KC, et al. Validation of the italian version of the night eating questionnaire (INEQ). J Psychopathol. (2017) 23:137–47. Available online at: https://www.jpsychopathol.it/wp-content/uploads/2018/02/01_Garcia-1.pdf (accessed June 6, 2019).
56. Aloi M, Rania M, Rodríguez Muñoz RC, Jiménez Murcia S, Fernández-Aranda F, Fazio PD, et al. Validation of the Italian version of the Yale Food Addiction Scale 2.0 (I-YFAS 2.0) in a sample of undergraduate students. Eat Weight Disord. (2017) 22:527–33. doi: 10.1007/s40519-017-0421-x
57. Golden C. Stroop Color and Word Test: A Manual for Clinical and Experimental Uses. Chicago: Skoelting (1978).
58. Rey A. L'examen psychologique dans les cas d'encéphalopathie traumatique. Arch de Psychol. (1941) 28:286–340.
59. Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition. (1994) 50:7–15. doi: 10.1016/0010-0277(94)90018-3
60. Spinnler H, Tognoni G. Standardizzazione e taratura italiana di test neuropsicologici. Ital J Neu. (1987) S8:1–113.
62. Wechsler D. Wechsler Adult Intelligence Scale. 3rd ed. San Antonio, TX: Psychological Corporation (1997). doi: 10.1037/t49755-000
63. Uher R, Farmer A, Henigsberg N, Rietschel M, Mors O, Maier W, et al. Adverse reactions to antidepressants. Br J Psychiatry. (2009) 195:202–10. doi: 10.1192/bjp.bp.108.061960
64. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Ser B. (1995) 57:289–300. doi: 10.1111/j.2517-6161.1995.tb02031.x
65. Huque MF. Validity of the Hochberg procedure revisited for clinical trial applications. Stat Med. (2016) 35:5–20. doi: 10.1002/sim.6617
66. Kessler RM, Hutson PH, Herman BK, Potenza MN. The neurobiological basis of binge-eating disorder. Neurosci Biobehav Rev. (2016) 63:223–8. doi: 10.1016/j.neubiorev.2016.01.013
67. Grace AA. Dysregulation of the dopamine system in the pathophysiology of schizophrenia and depression. Nat Rev Neurosci. (2016) 17:524–32. doi: 10.1038/nrn.2016.57
68. Niciu MJ, Ionescu DF, Richards EM, Zarate CA Jr. Glutamate and its receptors in the pathophysiology and treatment of major depressive disorder. J Neural Transm. (2014) 121:907–24. doi: 10.1007/s00702-013-1130-x
69. Nutt DJ. Relationship of neurotransmitters to the symptoms of major depressive disorder. J Clin Psychiatry. (2008) 69(Suppl. E):4–7.
70. Stahl S. Modes and nodes explain the mechanism of action of vortioxetine, a multimodal agent (MMA): enhancing serotonin release by combining serotonin (5HT) transporter inhibition with actions at 5HT receptors (5HT1A, 5HT1B, 5HT1D, 5HT7 receptors). CNS Spectr. (2015) 20:93–7. doi: 10.1017/S1092852915000139
71. Tovilla-Zárate CA, Pérez-Mandujano A, Ramírez-González IR, Fresan A, Suarez-Mendez S, Martínez-Villaseñor E, et al. Vortioxetine versus sertraline in metabolic control, distress and depression in Mexican patients with type 2 diabetes. Ann Transl Med. (2019) 7:656. doi: 10.21037/atm.2019.10.56
72. Beyer J, Johnson K. Advances in pharmacotherapy of late-life depression. Curr Psychiatry Rep. (2018) 20:34. doi: 10.1007/s11920-018-0899-6
73. Salagre E, Grande I, Solé B, Sanchez-Moreno J, Vieta E. Vortioxetine: a new alternative for the treatment of major depressive disorder. Rev Psiquiatr Salud Ment. (2018) 11:48–59. doi: 10.1016/j.rpsmen.2018.02.005
74. Christensen MC, Florea I, Lindsten A, Baldwin DS. Efficacy of vortioxetine on the physical symptoms of major depressive disorder. J Psychopharmacol. (2018) 32:1086–97. doi: 10.1177/0269881118788826
75. McIntyre RS, Lophaven S, Olsen CK. A randomized, double-blind, placebo-controlled study of vortioxetine on cognitive function in depressed adults. Int J Neuropsychopharmacol. (2014) 17:1557–67. doi: 10.1017/S1461145714000546
76. Katona C, Hansen T, Olsen CK. A randomized, double-blind, placebo-controlled, duloxetine-referenced, fixed-dose study comparing the efficacy, and safety of Lu AA21004 in elderly patients with major depressive disorder. Int Clin Psychopharmacol. (2012) 27:215–23. doi: 10.1097/YIC.0b013e3283542457
77. Mahableshwarkar AR, Zajecka J, Jacobson W, Chen Y, Keefe RSE. A randomized, placebo-controlled, active-reference, double-blind, flexible-dose study of the efficacy of vortioxetine on cognitive function in major depressive disorder. Neuropsychopharmacology. (2015) 40:2025–37. doi: 10.1038/npp.2015.52
78. David L, Ravishankara A, Kodros J, Pierce J, Venkataraman C, Sadavarte P. Premature mortality due to PM2.5 over india: effect of atmospheric transport and anthropogenic emissions. GeoHealth. (2019) 3:2–10. doi: 10.1029/2018GH000169
79. Long J. Vortioxetine for depression in adults. Issues Ment Health Nurs. (2019) 40:819–20. doi: 10.1080/01612840.2019.1604920
80. Thase ME, Mahableshwarkar AR, Dragheim M, Loft H, Vieta E. A meta-analysis of randomized, placebo-controlled trials of vortioxetine for the treatment of major depressive disorder in adults. Eur Neuropsychopharmacol. (2016) 26:979–93. doi: 10.1016/j.euroneuro.2016.03.007
81. Al-Sukhni M, Maruschak NA, McIntyre RS. Vortioxetine: a review of efficacy, safety and tolerability with a focus on cognitive symptoms in major depressive disorder. Expert Opin Drug Saf. (2015) 14:1291–304. doi: 10.1517/14740338.2015.1046836
82. He H, Wang W, Lyu J, Zheng J, Guo L, An X, et al. Efficacy and tolerability of different doses of three new antidepressants for treating major depressive disorder: a PRISMA-compliant meta-analysis. J Psychiatr Res. (2018) 96:247–59. doi: 10.1016/j.jpsychires.2017.10.018
83. Baldwin DS, Florea I, Jacobsen PL, Zhong W, Nomikos GG. A meta-analysis of the efficacy of vortioxetine in patients with major depressive disorder (MDD) and high levels of anxiety symptoms. J Affect Disord. (2016) 206:140–50. doi: 10.1016/j.jad.2016.07.015
84. Klingberg T. Training and plasticity of working memory. Trends Cogn Sci. (2010) 14:317–24. doi: 10.1016/j.tics.2010.05.002
85. Björkdahl A, Åkerlund E, Svensson S, Esbjörnsson E. A randomized study of computerized working memory training and effects on functioning in everyday life for patients with brain injury. Brain Inj. (2013) 27:1658–65. doi: 10.3109/02699052.2013.830196
86. Christopher G, MacDonald J. The impact of clinical depression on working memory. Cogn Neuropsychiatry. (2005) 10:379–99. doi: 10.1080/13546800444000128
87. Levada OA, Troyan AS. Cognitive-functional relationships in major depressive disorder: Crucial data from a Ukrainian open-label study of vortioxetine versus escitalopram. J Affect Disord. (2019) 250:114–22. doi: 10.1016/j.jad.2019.03.040
88. Vieta E, Sluth LB, Olsen CK. The effects of vortioxetine on cognitive dysfunction in patients with inadequate response to current antidepressants in major depressive disorder: a short-term, randomized, double-blind, exploratory study versus escitalopram. J Affect Disord. (2018) 227:803–9. doi: 10.1016/j.jad.2017.11.053
89. Eneva KT, Murray SM, Chen EY. Binge-eating disorder may be distinguished by visuospatial memory deficits. Eat Behav. (2017) 26:159–62. doi: 10.1016/j.eatbeh.2017.04.001
90. McIntyre RS, Florea I, Tonnoir B, Loft H, Lam RW, Christensen MC. Efficacy of vortioxetine on cognitive functioning in working patients with major depressive disorder. J Clin Psychiatry. (2017) 78:115–21. doi: 10.4088/JCP.16m10744
91. Bennabi D, Haffen E, Van Waes V. Vortioxetine for cognitive enhancement in major depression: from animal models to clinical research. Front Psychiatry. (2019) 10:771. doi: 10.3389/fpsyt.2019.00771
92. Baune BT, Sluth LB, Olsen CK. The effects of vortioxetine on cognitive performance in working patients with major depressive disorder: a short-term, randomized, double-blind, exploratory study. J Affect Disord. (2018) 229:421–8. doi: 10.1016/j.jad.2017.12.056
93. McIntyre R, Harrison J, Loft H, Jacobson W, Olsen C. The effects of vortioxetine on cognitive function in patients with major depressive disorder: a meta-analysis of three randomized controlled trials. Int J Neuropsychopharmacol. (2016) 19:pyw055. doi: 10.1093/ijnp/pyw055
94. Nierenberg AA, Loft H, Olsen CK. Treatment effects on residual cognitive symptoms among partially or fully remitted patients with major depressive disorder: a randomized, double-blinded, exploratory study with vortioxetine. J Affect Disord. (2019) 250:35–42. doi: 10.1016/j.jad.2019.02.006
95. Abbate-Daga G, Buzzichelli S, Marzola E, Aloi M, Amianto F, Fassino S. Does depression matter in neuropsychological performances in anorexia nervosa? A descriptive review. Int J Eat Disord. (2015) 48:736–45. doi: 10.1002/eat.22399
96. Giel KE, Wittorf A, Wolkenstein L, Klingberg S, Drimmer E, Schönenberg M, et al. Is impaired set-shifting a feature of “pure” anorexia nervosa? Investigating the role of depression in set-shifting ability in anorexia nervosa and unipolar depression. Psychiatry Res. (2012) 200:538–43. doi: 10.1016/j.psychres.2012.06.004
97. Galderisi S, Bucci P, Mucci A, Bellodi L, Cassano GB, Santonastaso P, et al. Neurocognitive functioning in bulimia nervosa: the role of neuroendocrine, personality and clinical aspects. Psychol Med. (2011) 41:839–48. doi: 10.1017/S0033291710001303
98. Weider S, Indredavik MS, Lydersen S, Hestad K. Neuropsychological function in patients with anorexia nervosa or bulimia nervosa. Int J Eat Disord. (2015) 48:397–405. doi: 10.1002/eat.22283
99. Alam MY, Jacobsen PL, Chen Y, Serenko M, Mahableshwarkar AR. Safety, tolerability, and efficacy of vortioxetine (Lu AA21004) in major depressive disorder: Results of an open-label, flexible-dose, 52-week extension study. Int Clin Psychopharmacol. (2014) 29:36–44. doi: 10.1097/YIC.0000000000000010
100. Baldwin DS, Chrones L, Florea I, Nielsen R, Nomikos GG, Palo W, et al. The safety and tolerability of vortioxetine: analysis of data from randomized placebo-controlled trials and open-label extension studies. J Psychopharmacol. (2016) 30:242–52. doi: 10.1177/0269881116628440
101. Stefano SC, Bacaltchuk J, Blay SL, Appolinário JC. Antidepressants in short-term treatment of binge eating disorder: systematic review and meta-analysis. Eat Behav. (2008) 9:129–36. doi: 10.1016/j.eatbeh.2007.03.006
102. Hu XH, Bull SA, Hunkeler EM, Ming E, Lee JY, Fireman B, et al. Incidence and duration of side effects and those rated as bothersome with selective serotonin reuptake inhibitor treatment for depression: Patient report versus physician estimate. J Clin Psychiatry. (2004) 65:959–65. doi: 10.4088/JCP.v65n0712
103. Thase ME, Haight BR, Richard N, Rockett CB, Mitton M, Modell JG, et al. Remission rates following antidepressant therapy with bupropion or selective serotonin reuptake inhibitors: a meta-analysis of original data from 7 randomized controlled trials. J Clin Psychiatry. (2005) 66:974–81. doi: 10.4088/JCP.v66n0803
104. Uguz F, Sahingoz M, Gungor B, Aksoy F, Askin R. Weight gain and associated factors in patients using newer antidepressant drugs. Gen Hosp Psychiatry. (2015) 37:46–8. doi: 10.1016/j.genhosppsych.2014.10.011
105. Guerdjikova AI, McElroy SL, Winstanley EL, Nelson EB, Mori N, McCoy J, et al. Duloxetine in the treatment of binge eating disorder with depressive disorders: a placebo-controlled trial. Int J Eat Disord. (2012) 45:281–9. doi: 10.1002/eat.20946
106. White MA, Grilo CM. Bupropion for overweight women with binge-eating disorder: a randomized, double-blind, placebo-controlled trial. J Clin Psychiatry. (2013) 74:400–6. doi: 10.4088/JCP.12m08071
107. Carbone EA, Caroleo M, Rania M, Calabrò G, Staltari FA, de Filippis R, et al. An open-label trial on the efficacy and tolerability of naltrexone/bupropion SR for treating altered eating behaviours and weight loss in binge eating disorder. Eat Weight. (2020). doi: 10.1007/s40519-020-00910-x. [Epub ahead of print].
108. Orhan FO, Ozer UG, Ozer A, Altunoren O, Celik M, Karaaslan MF. Night eating syndrome among patients with depression. Isr J Psychiatry Relat Sci. (2011) 48:212–7.
109. Allison KC, Lundgren JD, O'Reardon JP, Geliebter A, Gluck ME, Vinai P, et al. Proposed diagnostic criteria for night eating syndrome. Int J Eat Disord. (2010) 43:241–7. doi: 10.1002/eat.20693
110. McCuen-Wurst C, Ruggieri M, Allison KC. Disordered eating and obesity: associations between binge-eating disorder, night-eating syndrome, and weight-related comorbidities. Ann N Y Acad Sci. (2018) 1411:96–105. doi: 10.1111/nyas.13467
111. Pursey KM, Stanwell P, Gearhardt AN, Collins CE, Burrows TL. The prevalence of food addiction as assessed by the yale food addiction scale: a systematic review. Nutrients. (2014) 6:4552–90. doi: 10.3390/nu6104552
112. Carter JC, Van Wijk M, Rowsell M. Symptoms of ‘food addiction’ in binge eating disorder using the Yale Food Addiction Scale version 2.0. Appetite. (2019) 133:362–9. doi: 10.1016/j.appet.2018.11.032
113. Schulte EM, Grilo CM, Gearhardt AN. Shared and unique mechanisms underlying binge eating disorder and addictive disorders. Clin Psychol Rev. (2016) 44:125–39. doi: 10.1016/j.cpr.2016.02.001
114. Zhao Z, Ma Y, Han Y, Liu Y, Yang K, Zhen S, et al. Psychosocial correlates of food addiction and its association with quality of life in a non-clinical adolescent sample. Nutrients. (2018) 10:837. doi: 10.3390/nu10070837
115. Meule A, Hermann T, Kübler A. Food addiction in overweight and obese adolescents seeking weight-loss treatment. Eur Eat Disord Rev. (2015) 23:193–8. doi: 10.1002/erv.2355
116. Burrows T, Hides L, Brown R, Dayas CV, Kay-Lambkin F. Differences in dietary preferences, personality and mental health in Australian adults with and without food addiction. Nutrients. (2017) 9:285. doi: 10.3390/nu9030285
117. Wurtman RJ, Wurtman JJ. Brain serotonin, carbohydrate-craving, obesity, and depression. Adv Exp Med Biol. (1996) 398:35–41. doi: 10.1007/978-1-4613-0381-7_4
118. Rothman RB, Blough BE, Baumann MH. Dual dopamine/serotonin releasers as potential medications for stimulante and alcohol addictions. AAPS J. (2007) 9:E1–10. doi: 10.1208/aapsj0901001
119. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. (1960) 23:56–62. doi: 10.1136/jnnp.23.1.56
120. Colasanti V, Marianetti M, Micacchi F, Amabile G, Mina C. Tests for the evaluation of depression in the elderly: a systematic review. Arch Gerontol Geriatr. (2010) 50:227–30. doi: 10.1016/j.archger.2009.04.001
121. Bent-Hansen J, Lunde M, Klysner R, Andersen M, Tanghøj P, Solstad K, et al. The validity of the depression rating scales in discriminating between citalopram and placebo in depression recurrence in the maintenance therapy of elderly unipolar patients with major depression. Pharmacopsychiatry. (2003) 36:313–6. doi: 10.1055/s-2003-45120
Keywords: vortioxetine, Binge Eating Disorder, depression, neurocognition, eating behavior, weight, treatment, efficacy
Citation: Segura-Garcia C, Rania M, Carbone EA, de Filippis R, Aloi M, Caroleo M, Grasso G, Calabrò G, Fazia G, Staltari FA, Falvo A, Pugliese V, Gaetano R, Steardo L Jr and De Fazio P (2021) Naturalistic and Uncontrolled Pilot Study on the Efficacy of Vortioxetine in Binge Eating Disorder With Comorbid Depression. Front. Psychiatry 12:635502. doi: 10.3389/fpsyt.2021.635502
Received: 30 November 2020; Accepted: 18 February 2021;
Published: 17 March 2021.
Edited by:
Phillipa Jane Hay, Western Sydney University, AustraliaReviewed by:
Susana Jiménez-Murcia, Bellvitge University Hospital, SpainCopyright © 2021 Segura-Garcia, Rania, Carbone, de Filippis, Aloi, Caroleo, Grasso, Calabrò, Fazia, Staltari, Falvo, Pugliese, Gaetano, Steardo and De Fazio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Segura-Garcia, c2VndXJhQHVuaWN6Lml0
†ORCID: Cristina Segura-Garcia orcid.org/0000-0002-5756-3045
Marianna Rania orcid.org/0000-0001-7742-7086
Elvira Anna Carbone orcid.org/0000-0001-5521-6552
Renato de Filippis orcid.org/0000-0001-6928-1224
Matteo Aloi orcid.org/0000-0001-5585-6488
Mariarita Caroleo orcid.org/0000-0001-5856-5344
Luca Steardo Jr. orcid.org/0000-0002-7077-3506
Pasquale De Fazio orcid.org/0000-0001-5375-3565
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.