
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Psychiatry, 12 March 2021
Sec. Addictive Disorders
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.634309
This article is part of the Research TopicDrug and Behavioral Addictions During Social-Distancing for the COVID-19 PandemicView all 51 articles
 Florian Scheibein1
Florian Scheibein1 M. J. Stowe2
M. J. Stowe2 Sidharth Arya3
Sidharth Arya3 Nirvana Morgan4Tomohiro Shirasaka5
Nirvana Morgan4Tomohiro Shirasaka5 Paolo Grandinetti6
Paolo Grandinetti6 Noha Ahmed Saad7Abhishek Ghosh8
Noha Ahmed Saad7Abhishek Ghosh8 Ramyadarshni Vadivel9
Ramyadarshni Vadivel9 Woraphat Ratta-apha10
Woraphat Ratta-apha10 Sagun Ballav Pant11
Sagun Ballav Pant11 Ramdas Ransing12
Ramdas Ransing12 Rodrigo Ramalho13
Rodrigo Ramalho13 Angelo Bruschi14
Angelo Bruschi14 Tanay Maiti15
Tanay Maiti15 Anne Yee HA16
Anne Yee HA16 Mirjana Delic17
Mirjana Delic17 Shobhit Jain18
Shobhit Jain18 Eric Peyron19
Eric Peyron19 Kristiana Siste20
Kristiana Siste20 Joy Onoria21
Joy Onoria21 Saïd Boujraf22
Saïd Boujraf22 Lisa Dannatt23Arnt Schellekens24
Lisa Dannatt23Arnt Schellekens24 Tanya Calvey25*
Tanya Calvey25*Following the classification of the Coronavirus disease (COVID-19) as a pandemic by the World Health Organization (WHO), countries were encouraged to implement urgent and aggressive actions to change the course of the disease spread while also protecting the physical and mental health and well-being of all people. The challenges and solutions of providing prevention, treatment, and care for those affected with issues related to substance use and addictive behaviors are still being discussed by the global community. Several international documents have been developed for service providers and public health professionals working in the field of addiction medicine in the context of the pandemic (1–3), however, less is known about country-level responses. In the current paper we, as individual members of the Network of Early Career Professionals working in Addiction Medicine (NECPAM), discuss emerging country-level guidelines developed in the 6 months following the outbreak.
We identified a number of pertinent, country-level documents in the 17 countries represented here and we summarized country-level briefing notes, practice documents, guidelines, discussion papers and other documents containing recommendations on prevention, harm reduction, treatment, and care for people who use drugs (PWUD). Documents were identified in 12 out of the 17 countries. These documents are summarized and charted in Table 1. Additionally, several documents were under development at the time of our exercise in the Netherlands, Slovenia, and Paraguay and have not been included in this work. No specific documents or intentions to develop any were identified in Egypt, Uganda, or South Africa. Below we provide a summary of the identified documents.
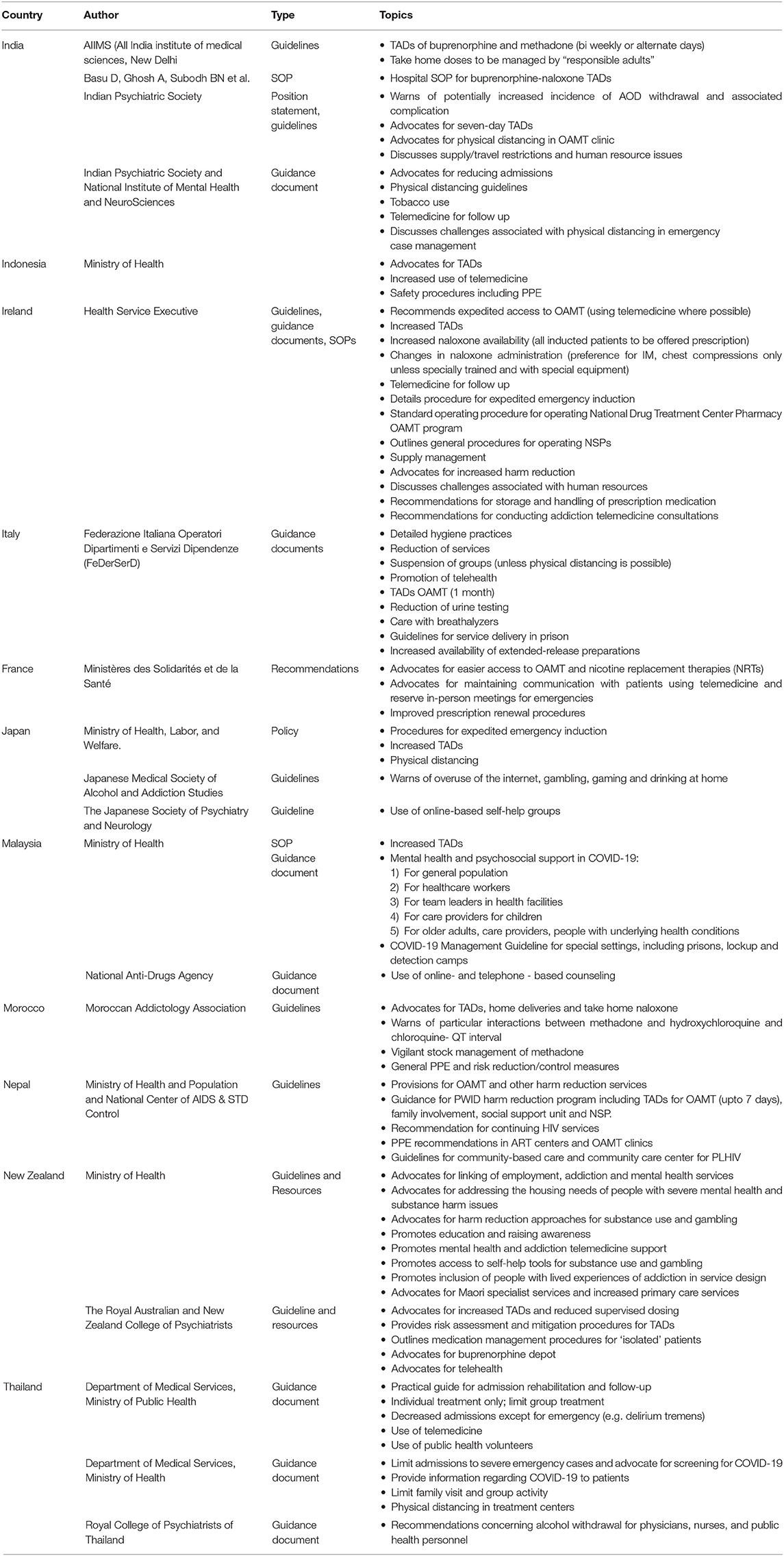
Table 1. Country specific COVID-19 guidance documents for clinical practice in addiction medicine.
Documents developed in Indonesia (4), Italy (5), and Nepal (6) discuss the use of personal and protective equipment (PPE). Malaysian (7), Moroccan (8), New Zealand (9–11), and Australian (12) organizations published documents which outlined risk assessment and mitigation practices. Documents in India (13), Malaysia (7), and Thailand (14, 15) discussed reducing admission of patients. Documents in India (16), Indonesia (17), and Japan (18) outlined strategies for maintaining physical distance in clinics and Standard Operating Procedures (SOP) were developed for isolation units in Ireland (19).
Italian (20) and Thai (15) documents discussed reducing addiction services and limiting group meetings. Documents in France (21), India (13), Italy (20), Ireland (19), Japan (22), Malaysia (7), New Zealand (11), and Thailand (15) advocated for the increased use of telemedicine to address the reduction in services.
Documents published in India (23) and Thailand (24) addressed substance withdrawal. The Thai document included strategies for the management of alcohol withdrawal that may have occurred due to local restrictions on alcohol sales. In Japan (22), there were discussions regarding the potential increase in the use of the internet, gambling, gaming, and higher prevalence of drinking at home during the COVID-19 pandemic.
Documents in France (21), Japan (25), and Ireland (26) described emerging practices of expedited access to opioid agonist maintenance treatment (OAMT). Documents in Ireland (26), India (23), Italy (20), Japan (25), Malaysia (7), Morocco (8), Nepal (6), and New Zealand (11) advocated for increased take-home doses (TADs) of OAMT. SOPs for buprenorphine-naloxone TADs in a hospital context have been developed in India (27) and documents in Indonesia (17), Nepal (6), Malaysia (7), and Italy (5) advocated for increased TADs of OAMT to 7 days, 14 days and 1 month, respectively. An Irish document (26) advocated for prescriptions for naloxone for all new OAMT patients and changes in the naloxone administration procedure (move toward intramuscular injection and chest compression in the absence of specialized equipment during opioid overdose interventions).
Guidelines, SOPs and recommendations in Nepal (6), Ireland (28, 29), and France (21), respectively, have also advocated for increased access to harm reduction services. In New Zealand, guidelines addressed practices of adopting a health equity/social determinant lens, developing culturally and trauma informed approaches, awareness, and education efforts, development of self-help resources and the inclusion of people with lived experience of substance use and gambling into the evaluation of interventions (10, 11).
A range of practices have been suggested at the country-level to deal with the challenges brought about by the ongoing pandemic. These include those around mitigating the spread of the corona virus, managing the risks associated with lockdown policies and changing trends in substance use and addictive behaviors.
In order to limit the spread of COVID-19, guidance has been drawn up to limit in-person meetings, physical support meetings, and contact time with physicians. Guidance suggests that this be operationalised through shifting services online, increased availability of TADs of OAMT, increased duration of TADs and increased availability of naloxone and injecting equipment allocations. Protocols have also been drawn up for the operation of clinics and outreach services for patients in isolation.
Several potential negative effects associated with the pandemic and resulting lockdown procedures have been identified which may require service adaptions. These include increased risks of substance withdrawal (30), access to service issues and potential changes in trends related to gambling, gaming, and internet related disorders. Several guidance documents discuss meeting these challenges through increased access to TADs, expedited access to OAMT and increased availability of online-based self-help groups and other services (11, 17–30). The increased commitment to TADs, telemedicine and access to harm reduction supplies are likely to address several issues brought about by the pandemic for people who use opioids and/or inject drugs. However, few documents explicitly discuss the increased availability of harm reduction supplies (for example, naloxone and injecting equipment) and service adaptions for people who use non-opioid drugs and/or engage in addictive behaviors (such as gambling and gaming) continue to be neglected by most documents.
There are also concerns regarding the implementation of COVID-19-related policy documents as a recent global survey indicates that among 130 countries, 60% reported disruptions to mental health services for vulnerable people, 67% reported disruptions to counseling and psychotherapy, 35% reported disruptions to emergency interventions, and 30% reported disruptions to access for medications for mental, neurological, and substance use disorders (31). The combination of a reduction in the availability of services, increased reliance on telemedicine, physical distancing protocols, and travel restrictions may exasperate underlying health inequities in terms of access to addiction services (31–34). This seems to disproportionately affect the most marginalized and socioeconomically disadvantaged patients (32) who may lack access to internet-enabled devices, sufficient internet, the necessary private spaces to engage in telemedicine and means of transport to services.
The lack of representation of country-level documents from the Americas, Eastern Europe, the Middle East, Africa, and other regions is a limitation of this paper. Future research should document emerging practices in additional regions and monitor and evaluate the implementation of country-level policies. Country-level documents may be useful as they may allow clinicians to adapt to their given local context. Such documents should consider best emerging practices as it relates to issues surrounding a wide range of substances, addictive behaviors, harm reduction, and health inequities exasperated by the pandemic and restrictions.
FS and TC developed the initial draft of the document. The commentary was then reviewed by MS and NM. All authors subsequently reviewed their sections and the overall document. All authors identified their own local documents or confirmed the lack of their existence.
This research was funded by the South African Medical Research Council grant held by TC.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to acknowledge NECPAM and its members. We would also like to acknowledge Dr. Dzmitry Krupchanka who provided feedback for this commentary.
1. Dunlop A, Lokuge B, Masters D, Sequeira M, Saul P, Dunlop G, et al. Challenges in maintaining treatment services for people who use drugs during the COVID-19 pandemic. Harm Reduct. J. (2020) 17:26. doi: 10.1186/s12954-020-00370-7
2. European Monitoring Center for Drugs and Drug Addiction. EMCDDA Update on the Implications of COVID-19 for People Who Use Drugs (PWUD) and Drug Service Providers. Lisbon: European Monitoring Centre for Drugs and Drug Addiction; 2020). Available online at: https://www.emcdda.europa.eu/system/files/publications/12879/emcdda-covid-update-1-25.03.2020v2.pdf (accessed July 2, 2020).
3. United Nations Office on Drugs and Crime. Suggestions About Treatment, Care and Rehabilitation of People With Drug Use Disorder in the Context of the COVID-19 Pandemic. Vienna: United Nations Office of Drugs and Crime (2020). Available online at: https://www.unodc.org/documents/drug-prevention-and-treatment/Drug_treatment_and_care_services_and_COVID19.pdf (accessed July 02, 2020).
5. Federazione Italiana Operatori Dipartimenti e Servizi Dipendenze Fase 2 della infezione da SARS-CoV-2 Indicazioni operative per I Servizi delle Dipendenze. 2020. Available online at: http://www.federserd.it/files/novita/Documento_FEDERSERD_Linee_operative_COVID19_agg_30_maggio_2020.pdf (accessed October 02, 2020).
6. Ministry of Health and Population and National Center of AIDS & STD Control. Interim Guidance for Managing PLHIV and Harm Reduction Program for PWID During COVID-19 Response. (2020). (accessed 02, October 2020).
8. Association Marocain d'Addictologie. Recommandations de l'Association Marocain d'Addictologie (AMA) destinées auxusagers de substances psychoactives, aux professionnels en santé mentale et enaddictologie durant la pandémie Covid-19. Association Marocain d'Addictologie (AMA) (2020).
9. Ministry of Health. Psychosocial and Mental Wellbeing Recovery Plan. Ministry of Health – Manatu Hauora. New Zealand: Ministry of Health. (2020). Available online at: https://www.health.govt.nz/publication/covid-19-psychosocial-and-mental-wellbeing-recovery-plan
10. New Zealand Ministry of Health. Guidance for Specialist Mental Health and Addiction Services During the COVID-19 Alert Levels 3 and 4. Ministry of Health – Manatu Hauora (2020). Available online at: https://www.health.govt.nz/system/files/documents/pages/covid-19_guidance_for_specialist_mental_health_and_addiction_services_29_april_2020.pdf (accessed July 02, 2020).
11. New Zealand Ministry of Health. Guidance for Mental Health and Addiction Residential Service Providers during the COVID-19 Alert Levels 3 & 4 Restriction Period. Ministry of Health – Manatu Hauora. 2020. Available online at: https://www.health.govt.nz/system/files/documents/pages/covid-19_guidance_for_mental_health_and_addiction_ngo_sector_11_may_2020.pdf (accessed July 02, 2020).
12. Lintzeris N, Hayes V, Arunogiri S. Interim Guidance for the Delivery of Medication Assisted Treatment of Opioid Dependence in Response to COVID-19: a National Response. Sydney: The Australasian Professional Society on Alcohol and other Drugs (ASPAD) (2020). Available online at: https://www.apsad.org.au/images/covid-19/interim-guidance-delivery-of-medication-assisted-treatment-of-opiod-dependence-covid-19.pdf (accessed July 02, 2020).
13. Indian Psychiatric Society. IPS: Interim Guidelines for Opioid Substitution Therapy (OST) during COVID-19 outbreak. Gurgaon: Indian Psychiatric Society. (2020). Available online at: online: https://indianpsychiatricsociety.org/ips-interim-guidelines-for-opioid-substitution-therapy-ost-during-covid-19-outbreak/ (accessed July 02, 2020).
14. Ministry of Public Health. Guidelines for prevention and control of the outbreak of COVID-19 for management of substance use disorder patients in health care and prisons-based settings. (2020). Available online at: http://dmsic.moph.go.th/index/detail/8102 (accessed July 02, 2020).
15. Ministry of Public Health. Guidelines for prevention and control the outbreak of COVID-19 for management of substance use disorder patients in compulsory drug treatment system. (2020). Available online at: http://dmsic.moph.go.th/index/detail/8102 (accessed July 02, 2020).
16. Indian Psychiatric Society and National Institute of Mental Health and NeuroSciences. Mental Health Challenges During COVID-19 Pandemic Guidance for Psychiatrists. (2020). Available online at: https://indianpsychiatricsociety.org/wp-content/uploads/2020/05/IPS-NIMHANS-COVID-19-Final-30-4-20.pdf (accessed July 02, 2020).
17. Indonesian Ministry of Health. Protocol Pelaksanaan Layanan HIV AIDS selama Pandemi COVID-19. (2020).
18. Japansese Ministry of Health. Labour, and Welfare. Policies for Prevention and Control of the Novel Coronavirus 2020. Available online at: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/newpage_00032.html (accessed July 02, 2020).
19. Health Service Executive. COVID 19 Pharmacy SOP for Clients in Isolation. (2020). Available online at: https://www.hse.ie/eng/about/who/primarycare/socialinclusion/other-areas/health-inequalities/dispensing-for-clients-in-isolation.pdf (accessed July 02, 2020).
20. Federazione Italiana Operatori Dipartimenti e Servizi Dipendenze. Strumenti terapeutici innovativi nei SerD per la cura dei tossicodipendenti e per contrastare la diffusione del SARS-CoV-2 2020. (2020). Available online at: http://www.federserd.it/files//novita/FEDERSERD_strumenti_terapeutici_innovativi_nei_SERD.pdf (accessed July 02, 2020).
21. Ministères des Solidarités et de la Santé. Recommandations applicables á l'organisation des prises en charge en ambulatoire dans les services de psychiatrie et les éstablissements sanitaires autorisés en psychiatrie. Paris: Ministères des Solidarités et de la Santé.
22. Japanese Medical Society of Alcohol and Addiction Studies. Worried About the New Coronavirus Problem Addictions Such as Alcoholism and Game Disorders. (2020). Available online at: http://www.f.kpu-m.ac.jp/k/jmsas/ (accessed July 02, 2020).
23. Indian Psychiatric Society. Indian Psychiatric Society: Position Statement on COVID-19 Pandemic, Mental Health Issues. Gurgaon: Indian Psychiatric Society (2020). Available online at: https://indianpsychiatricsociety.org/250411-2 (accessed July 02, 2020).
24. Royal College of Psychiatrists of Thailand. Recommendations concerning alcohol withdrawal for physician, nurse, and public health personnel. (2020). Available online at: https://www.rcpsycht.org/th/organization/laws-regulations (accessed July 02, 2020).
25. Japanese Ministry of Health. Labour, and Welfare. Policies for Prevention and Control of the Novel Coronavirus. (2020). Available online at: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/newpage_00032.html (accessed July 02, 2020).
26. Health Service Executive. Contingency Planning for People who use Drugs. (2020). Available online at: https://www.hse.ie/eng/about/who/primarycare/socialinclusion/other-areas/health-inequalities/contingency-planning-for-people-who-use-drugs.pdf (accessed July 02, 2020).
27. Basu D, Ghosh A, Subodh BN, Mattoo SK. Opioid substitution therapy with buprenorphine-naloxone during COVID-19 outbreak in India: sharing our experience and interim standard operating procedure. Indian J Psychiatr. (2020) 62:322–6. Available online at: http://www.indianjpsychiatry.org/text.asp?2020/62/3/322/284448
28. Health Service Executive. Example SOP for emergency induction of OST during COVID CRISIS. (2020). Available online at: https://www.hse.ie/eng/about/who/primarycare/socialinclusion/other-areas/health-inequalities/example-sop-for-emergency-induction-of-ost.pdf (accessed July 02, 2020).
29. Health Service Executive. Needle Exchange Provision in COVID-19 Pandemic. (2020). Available online at: https://www.hse.ie/eng/about/who/primarycare/socialinclusion/other-areas/health-inequalities/needle-exchange-provision-in-covid.pdf (accesssed July 02, 2020).
30. Calvey T, Scheibein F, Saad NA, Shirasaka T, Dannatt L, Stowe MJ, et al. The changing landscape of alcohol use and alcohol use disorder during the covid-19 pandemic-perspectives of early career professionals in 16 countries. J Addict Med. (2020) 14:e284–6.
31. Stowe MJ, Calvey T, Scheibein F, Arya S, Saad NA, Shirasaka T, et al. Access to healthcare and harm reduction services during the COVID-19 pandemic for people who use drugs. J Addict Med. (2020) 14:e287–9.
32. WHO. COVID-19 Disrupting Mental Health Services in Most Countries, WHO Survey. (2020). Available online at: https://www.who.int/news/item/05-10-2020-covid-19-disrupting-mental-health-services-in-most-countries-who-survey (accessed online October 2020).
33. Radfar SR, De Jong CA, Farhoudian A, Ebrahimi M, Rafei P, Vahidi M, et al. Reorganization of substance use treatment and harm reduction services during the COVID-19 pandemic: a global survey. medRxiv [Preprint]. (2020).
34. Policy brief: Covid-19 and the need for action on Mental Health. (2020). Available online at: https://unsdg.un.org/sites/default/files/2020-05/UN-Policy-Brief-COVID-19-and-mental-health.pdf
Keywords: COVID-19, drug policy, addiction medicine, substance use, behaviourial addictions, best practice, guidelines
Citation: Scheibein F, Stowe MJ, Arya S, Morgan N, Shirasaka T, Grandinetti P, Saad NA, Ghosh A, Vadivel R, Ratta-apha W, Pant SB, Ransing R, Ramalho R, Bruschi A, Maiti T, HA AY, Delic M, Jain S, Peyron E, Siste K, Onoria J, Boujraf S, Dannatt L, Schellekens A and Calvey T (2021) Responding to COVID-19: Emerging Practices in Addiction Medicine in 17 Countries. Front. Psychiatry 12:634309. doi: 10.3389/fpsyt.2021.634309
Received: 27 November 2020; Accepted: 15 February 2021;
Published: 12 March 2021.
Edited by:
Hironobu Fujiwara, Kyoto University Hospital, JapanReviewed by:
Kentaro Kawabe, Ehime University, JapanCopyright © 2021 Scheibein, Stowe, Arya, Morgan, Shirasaka, Grandinetti, Saad, Ghosh, Vadivel, Ratta-apha, Pant, Ransing, Ramalho, Bruschi, Maiti, HA, Delic, Jain, Peyron, Siste, Onoria, Boujraf, Dannatt, Schellekens and Calvey. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tanya Calvey, dGFueWFjQHBvbGthLmNvLnph
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.