
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 31 March 2021
Sec. Aging Psychiatry
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.631518
This article is part of the Research Topic “We know what we are, but know not what we may be”: Metacognition and Self-awareness in the Aging Brain View all 7 articles
 Christine Bastin1,2*
Christine Bastin1,2* Fabrice Giacomelli1Frédéric Miévis1Christian Lemaire1Bénédicte Guillaume3Eric Salmon1,4
Fabrice Giacomelli1Frédéric Miévis1Christian Lemaire1Bénédicte Guillaume3Eric Salmon1,4While anosognosia is often present in Alzheimer's disease, the degree of awareness of cognitive difficulties in the earlier stages, such as Mild Cognitive Impairment (MCI), is less clear. Using a questionnaire and Feeling-of-Knowing tasks, the aims of this study were (1) to test the hypothesis that anosognosia is present specifically in prodromal AD stage in patients that, owing to a more severe AD neuropathology, will rapidly progress to overt dementia and (2) to assess the neural bases of self-awareness for memory functioning. A group of 44 patients with amnestic MCI and a group of 29 healthy older participants (CTRL) performed two Feeling-of-Knowing tasks (episodic and semantic FOK) and responded to the Functional Memory Scale (MARS), also completed by one of their relatives. They underwent FDG-PET and structural MRI. The participants were followed clinically for 4 years. At the end of follow-up, 23 patients with MCI developed Alzheimer's disease (converters) and 21 patients still presented symptoms of MCI without progression (non-converters). The analyses focused on the data from inclusion stratified according to clinical status 4 years later (converters, non-converters, CTRL). On the episodic FOK task, converters patients overestimated their ability to later recognize unrecalled words and they showed prediction accuracy (Hamann coefficient) at the level of chance. No difficulty was observed in any group with the semantic FOK task. On the MARS, converters patients had a higher anosognosia score than non-converters patients and CTRL, which did not differ from each other. Correlations between self-awareness scores and neuroimaging data using small volume correction analyses in a priori regions of interest in converters indicated that inaccurate episodic FOK judgments was related to changes in brain areas that might support interpretation of retrieved content for judging the likelihood of recognition. For the MARS, the association between anosognosia and decreased gray matter density of the left inferior prefrontal cortex in converters might indicate poor inhibition over outdated personal knowledge. In amnestic MCI, anosognosia could be an early sign of neurodegeneration in brain areas that would support control mechanisms over memory representations.
Patients with Alzheimer's disease (AD) frequently show poor awareness of their cognitive and functional deficits, a symptom which has been designated by various terms such as anosognosia, unawareness, loss of insight, impaired self-awareness, or self-consciousness (1). Anosognosia in AD has been demonstrated by various methods which address different dimensions of the complex concept of self-awareness. The two most frequently used methods take some measure as reference against which to compare the patient's self-judgment: patient-informant discrepancy on questionnaires and prediction of performance. Such methods showed that poor awareness in AD affects various dimensions of cognitive functioning, instrumental activities of daily living, behavioral changes and mood modifications [(2), for a review]. Here, we will only consider memory, which is the main cognitive domain to decline in typical forms of AD, as well as in its prodromal stage, Mild Cognitive Impairment (MCI). For instance, using the Memory Awareness Rating Scale-Functional scale, Clare et al. (3) reported a large discrepancy between patient and informant's assessment as a sign of poor awareness of memory deficits by AD patients. In addition to self—and hetero-assessment questionnaires, there exist more objective methods to evaluate memory awareness, developed in the metamemory literature (4). They consist in asking participants to judge their performance during a task. A typical measure is Feeling-of-Knowing (FOK) judgments during which participants provide item-by-item predictions of future recognition in case of failure to recall. Most studies using these prediction paradigms in AD reported impaired memory monitoring abilities [for reviews (5, 6)]. Interestingly, the difficulty for AD patients to monitor memory performance seems particularly pronounced in episodic memory tasks, while metamemory judgments are better preserved during a semantic memory task (7, 8).
Amnestic Mild Cognitive Impairment (aMCI) represents a condition with high risk to develop AD (9). Given that memory complaints form part of the diagnosis criteria (10), there is interest in knowing whether this complaint reflects the actual cognitive status of the patients or is underestimated. Studies that examined self-awareness of memory in aMCI using questionnaires provided mixed findings [(11), for a review]. Several studies showed that aMCI patients have poor insight into their memory deficits, underestimating them (12–18). But, according to other reports, aMCI patients retain some ability to correctly apprehend the extent of their memory impairments (19–24). Finally, aMCI patients can also overestimate their cognitive difficulties (25, 26). Of note, a meta-analysis on existing studies on self-awareness in MCI indicated that no reliable difference in awareness was observed between MCI and controls, and that patients with more memory problems (i.e., aMCI subtype) seemed accurate in assessing their cognitive status (27).
In contrast to evaluation of memory awareness via questionnaires, there has been little investigation of memory monitoring capacities in aMCI with the use of metamemory measures. In a study by Galeone et al. (12), global prediction of recall performance before and after study was found to be less accurate in aMCI patients compared to controls. MCI patients also overestimated their cognitive performance in various tasks including memory during post-test ratings (28). In contrast, Clare et al. (25) found that MCI patients were as good as controls in the rating of their performance in the Rivermead Behavioral Memory Test after each subtest completion. Perrotin et al. (29) and Anderson and Schmitter-Edgecombe (30) evaluated the accuracy of episodic FOK in aMCI and found that the patients had a decreased accuracy in predicting subsequent recognition of forgotten words. This poor metamemory appraisal was driven by overestimation of performance, with greater rates of incorrect prediction of subsequent recognition in aMCI. Moreover, FOK accuracy in the patients correlated with memory neuropsychological scores, suggesting that poor recollection of details relative to studied items prevented accurate judgments about the possibility to recognize the items. In controls, FOK accuracy was rather associated with executive functions scores, possibly reflecting support to the search in memory and evaluation of the retrieval process (29). More generally, insight measures in MCI have been found to correlate with memory and language scores as well as global cognitive decline (MMSE) (27). Finally, Ryals et al. (31) explored several metamemory measures in aMCI and observed impaired global prediction of performance, inaccurate confidence ratings, and altered episodic FOK for verbal stimuli, but not visual stimuli. However, in their meta-analysis, Piras et al. (27) reported that MCI patients were good (actually even better than controls) at predicting their memory performance in learning tasks and that their self-report of cognitive proficiency matched objective cognitive performance.
Part of the inconsistencies between studies assessing anosognosia in aMCI may relate to the fact that aMCI is a heterogeneous syndromic entity. While some aMCI patients present with a purely amnestic profile, others have additional cognitive deficits and are called “multiple-domain” (10). Even though AD is the most common cause of aMCI, especially in single-domain amnestic subtype, the patient may actually be in the very early stage of another type of dementia (10). Cognitive impairments can sometimes also be related to late-life depression (32). Moreover, some individuals remain stable or even improve to the point that they no longer have memory deficits (33). A few studies have suggested that anosognosia revealed by patient-informant discrepancy scores or self-ratings-objective performance divergence may only be seen in aMCI patients who progress to AD in the following years. Indeed, longitudinal studies provided evidence that poor awareness of deficits in memory (34, 35), executive functions (36), various cognitive domains (37, 38), and functional abilities (39) predicts future dementia in people with aMCI. Consistently, aMCI patients who harbor amyloid pathology demonstrate anosognosia for memory deficits (40). However, one study reported poor predictive power of unawareness for memory decline in detecting MCI individuals who progressed to dementia 2 years later (41). Piras et al. (27) observed that MCI patients with more cognitive decline had less accurate self-awareness, especially when considering samples mixing different MCI subtypes and samples referred by physicians.
The cognitive mechanisms that are involved in self-awareness have been developed in some theoretical models of anosognosia. Among them, two have been most influential (42, 43). In the Cognitive Awareness Model (42), incoming information concerning an event of memory failure enters short-term memory, then long-term memory. The event is compared, using mnemonic comparators within the central executive system, with the semantic personal knowledge base (PKB). In cases of mismatch detected by the comparator, the PKB is updated, and information from the PKB is directed to a metacognitive awareness level. Mnemonic anosognosia occurs if one is able to perceive and detect memory failure in an online fashion, using links between episodic memory and conscious awareness, but PKB is not updated, leading to a “petrified self” (44). Executive anosognosia corresponds to an inability to perceive incidents of memory failure due to faulty memory comparators. In their model, Toglia and Kirk (43) proposed that awareness of ones' own functioning arises from the dynamic interplay between pre-existing knowledge and beliefs related to oneself on the one hand and the ability to monitor performance online during task performance [see (45) for a similar view]. Piras et al. (27) proposed to merge the two views by integrating the self-monitoring mechanism as a critical component for metacognitive awareness. Mechanisms that support such memory monitoring are further elaborated in metamemory theories (46, 47). We will focus on cognitive processes underlying FOK judgments as they were used in the current study. According to the accessibility model (48), in situations of recall failure, a rapid assessment of the cue familiarity is performed, and if the cue evokes a sufficient degree of familiarity, a search-and-retrieval process of the solicited target is engaged. During this search, the amount of partial information that is retrieved regarding the target is evaluated to judge how accessible the target memory is (i.e., prediction of future recognition is related to sufficient feeling of knowing the target).
The examination of the neural correlates of lack of awareness provides insight about the possible neurocognitive mechanisms explaining anosognosia. In AD, increased level of anosognosia correlates with structural and functional changes in the inferior and superior frontal gyrus, the anterior cingulate and orbitofrontal cortex, the medial frontal gyrus, the medial temporal lobe, the posterior cingulate cortex, and the insula [for a review (49)]. Several of these regions belong to the Default Mode Network (DMN), which supports cognitive processing of the self and autobiographical memory (50). Accordingly, lack of awareness in AD is also associated with decreased functional connectivity between brain areas within the DMN or between DMN and other brain regions (51–54). Interpreted at the light of the Cognitive Awareness Model, the neural correlates of anosognosia in AD suggest that several difficulties can explain lack of awareness for memory deficits in the patients. Decreased connectivity between frontal, temporal, and parietal areas on the one hand and medial temporal lobe regions on the other hand would contribute to failure of updating the personal knowledge base; medial prefrontal and posterior cingulate damage would affect the efficacy of self-referential processing during explicit performance evaluation; and deficient error monitoring caused by damage to the anterior cingulate cortex and insula would disturb comparator mechanisms (51, 55).
In MCI though, there are still debates about the presence of anosognosia and little knowledge about possible underlying mechanisms. The few studies that examined the neural correlates of anosognosia in MCI reported association with frontal, temporoparietal and cortical midline regional dysfunction [(56), for a review]. In this context, the current study had several objectives: (1) To test the hypothesis that anosognosia for memory impairment would be predominantly observed in prodromal AD stage in patients that will rapidly progress to overt dementia. This was assessed via a longitudinal approach that evaluated self-awareness of memory in MCI as a function of clinical outcome after a 4 year follow-up period. (2) To compare self-awareness across different methods: a self-vs.-hetero-assessment of memory in daily life and an online performance prediction measure for episodic and semantic memory (FOK). Based on previous studies, we should observe in MCI patients (especially those who rapidly progressed to AD) overestimation of daily life memory functioning and inaccurate episodic FOK judgments, but preserved semantic FOK accuracy. (3) To relate self-awareness scores to brain metabolism (FDG-PET) and gray matter density (structural MRI) in an attempt to unravel the neurocognitive basis of anosognosia in the very early phase of AD.
The patient group consisted of 44 participants (18 women) who met the criteria for amnestic MCI following the Mayo Clinic criteria (9) at inclusion (n = 39 single-domain aMCI; n = 5 multiple-domain aMCI). They were referred by neurologists working in memory clinics and were selected on the basis of a general examination, neurological and neuropsychological assessments, neuroimaging, and laboratory evaluation. The patients demonstrated both subjective and objective memory decline. They did not experience many difficulties in their daily activities and they did not fulfill the criteria for dementia. During the 4 year follow-up period, the patients were re-evaluated at least once with a neuropsychological test battery and a neurological assessment. Follow-up stopped when the patient met the clinical diagnosis of Alzheimer's disease (57) or after 4 years if the patient still met aMCI criteria. The current analyses were performed on the inclusion data as a function of follow-up outcome. The patient groups included in the analyses consisted of 23 MCI patients who progressed to AD 6 to 42 months after inclusion (converters, mean time to conversion: 21.4 months ± 11.8), and 21 patients who still presented with MCI 4 years after inclusion (non-converters).
A control group of 29 healthy older participants (20 women) also participated in the study. At inclusion, subjects in this group had to perform within norms on the Dementia Rating Scale (58). A follow-up consisting of a neuropsychological assessment was also proposed to controls. One participant demonstrated cognitive decline compatible with a degenerative process at follow-up and was therefore excluded from the analyses.
For all participants (aMCI and controls), exclusion criteria were the following: depressive symptoms as indicated by above-cut-off scores on the Geriatric Depression Scale (>6), not being native French-speaker, psychiatric antecedents, neurological antecedents (such as stroke, tumor), anxiolytic or anti-depressive medication, excessive consumption of alcohol (>14 units/week), and uncorrected deficient hearing and vision.
The demographic and clinical characteristics at inclusion of the three groups are presented in Table 1. The converters, non-converters, and control groups were matched in terms of age, education, and vocabulary abilities [Mill Hill test (59)]. On the Geriatric Depression Scale (60), converters patients scored higher than the other two groups, F(2, 68) = 3.3, p < 0.05, η2p = 0.08. The converters patients had a poorer score on the Dementia Rating Scale (61) than non-converters patients, who themselves performed more poorly than controls, F(2, 69) = 17.2, p < 0.001, η2p = 0.33.
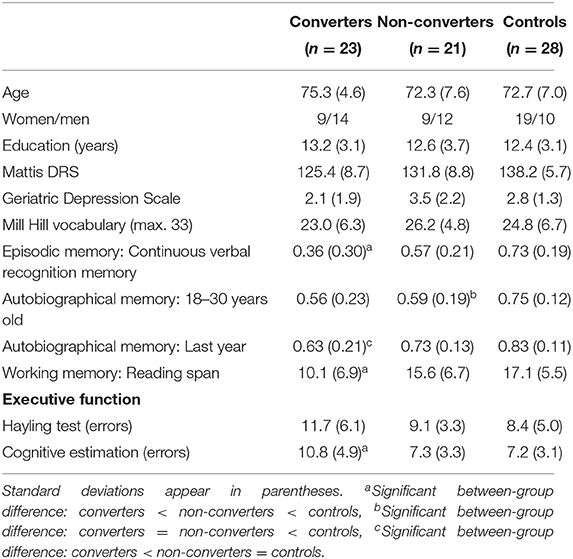
Table 1. Demographic, clinical, and neuropsychological characteristics of the converters, non-converters, and control groups.
All three groups performed several experimental neuropsychological tests as part of the protocol (Table 1). Verbal episodic memory was assessed by means of a continuous recognition memory task adapted from Treyer et al. (62). Words were presented for 2.5 s each. Twenty-five words appeared twice after random delays, and 10 words appeared only once. Participants had to indicate for each word whether s/he had seen it before in the series. Recognition memory performance was computed as the proportion of hits (correct identification of repetition) minus the proportion of false alarms (incorrect “yes” response to non-repeated words). Episodic autobiographical memory was assessed by the TEMPau questionnaire (63, 64). The episodic quality of reported memories was indexed by the proportion of internal/episodic details out of the total number of information contained in the narratives (65). The reading span test (66, 67) was administered to evaluate working memory. Participants read series of 2 to 6 sentences and had to remember the last word of each sentence. Performance was indexed by the total number of words correctly recalled. In such task, intrusions are very rare. The Hayling test (68, 69) evaluated the ability to inhibit a predominant semantic answer. The number of errors for part B (inhibition) of the task was measured. As another measure of executive functioning, cognitive estimation evaluated participants' ability to provide an estimate of time, speed, weight or size from semantic knowledge (70).
The comparison of the three groups showed that converters patients were significantly impaired compared to non-converters and controls in working memory, cognitive estimation, verbal episodic memory, and autobiographical memory. Non-converters were impaired compared to controls in working memory, cognitive estimation, verbal episodic memory, and remote autobiographical memory (see Table 1).
The tasks that all participants completed at inclusion consisted of two feeling-of-knowing tasks (episodic and semantic conditions) and the Memory Awareness Rating Scale. Participants were tested individually. According to the Declaration of Helsinki, all participants gave their written consent to participate to the study, which was approved by the ethics committee of the University Hospital of Liège.
The episodic and semantic feeling-of-knowing (FOK) tasks were adapted from Souchay et al. (71). The stimuli consisted of 40 target French words, each paired with a weakly associated word, which served as a cue in the episodic FOK task. The stimuli were randomly divided into two sets of 20 items, in order to create two versions of each task, so that each target word appeared equally often in the episodic and the semantic FOK tasks. All participants were randomly assigned one version of the episodic and semantic FOK tasks. Stimuli were presented in the center of a computer screen.
The episodic FOK task contained a study phase, a cued recall phase with FOK judgments and a recognition memory phase. In the study phase, participants were presented with 20 cue-target pairs. The cue word was printed in lowercase letters next to the target word, which was printed in capital letters. Participants were instructed to try and remember the pairs because their memory for the second (target) word would be tested later by using the first word as a cue. The pairs were shown in random order and each remained on the screen for 5 s. After a short delay filled with instructions, the cued recall phase began. The cues were presented in random order. The participants were asked to recall the target word that was associated with each cue during the study phase. They had the possibility to say that they did not know (omission). Whatever their response (correct target word, incorrect answer or omission), they had next to give a feeling-of-knowing judgement, indicating whether they thought they would be able to recognize the target in a subsequent forced-choice recognition test. They provided a “yes” or a “no” answer. For the analysis of FOK accuracy, only the trials where the participants could not recall any word (omissions) were included. Finally, a five-alternative forced-choice recognition phase was administered. Each of the 20 target words was presented with 4 semantically related distracter words. The participants had to indicate which word they had seen in the study phase. Moreover, for each response, they were asked to give a Remember/Know/Guess judgement. Participants were instructed that a Remember response corresponded to the recollection of specific information relative to the stimulus encoded at the study phase; that a Know response referred to recognition on the basis of familiarity without recollection; and that a Guess response could be used when they were unsure about their response. Remember/Know data will not be analyzed here.
The semantic FOK task contained a word cued recall phase (based on general knowledge), with FOK judgments and a recognition memory phase. In the cued recall phase, participants were presented with a series of 20 general information statements corresponding to definitions of the target words. For each question, they had to try to provide the word corresponding to the definition and could say if they did not know the answer (omission). As for the episodic task, for each trial, participants had to indicate whether they thought they would be able to recognize the target in a subsequent forced-choice recognition test. Only FOK judgments given after omissions were included in the analyses of FOK accuracy. For the forced-choice recognition memory phase, each question was shown with 5 possible words and participants had to choose the one that they believe fitted the best the definition.
Awareness of memory functioning in everyday life was evaluated with the Memory Functioning Scale from the Memory Awareness Rating Scale (MARS-MFS) (3). Thirteen questions about memory ability in various areas of everyday memory functioning were presented to the participant as well as to an informant (either the participant's spouse or child). For each situation, the frequency with which difficulties occur in the participant's life was assessed with a 5-point scale (from 0 “never able to do that” to 4 “always able to do that”). Awareness of memory functioning was evaluated by comparing self- (MFS-S) and informant (MFS-I) ratings by means of a corrected discrepancy score [(MFS-S – MFS-I)/((MFS-S + MFS-I)/2)] averaged across the 13 items (72). Scores that are close to zero indicate good agreement between the participant and his/her informant. Positive scores reflect overestimation of memory functioning (participants rate themselves more positively than do their informants), whereas negative scores correspond to underestimation of memory functioning (participants rate themselves less positively than do their informants).
Cerebral glucose metabolism was measured with FDG-PET in 22 converters patients, 20 non-converters patients and 26 controls. Structural MRI was performed in 19 converters patients, 17 non-converters patients and 22 controls.
For each participant, a FDG-PET image was acquired on a Siemens/CTI (Knoxville, TN) ECAT HR+ scanner (3D mode; 63 image planes; 15.2 cm axial field of view; 5.6 mm transaxial resolution and 2.4 mm slice interval) during quiet wakefulness with eyes closed and ears unplugged after intravenous injection of 2-[18F]fluoro-2-deoxy-D-glucose (FDG, 152 to 290 MBq) (73). Images of tracer distribution in the brain were used for analysis: scan start time was 30 min after tracer injection and scan duration was 20 min. Images were reconstructed using filtered backprojection including correction for measured attenuation and scatter using standard software. FDG-PET image analyses were performed using SPM12 (Wellcome Department of Cognitive Neurology, London, UK). The PET data were subjected to an affine and non-linear spatial normalization onto the PET brain template. A mean image was then generated from all the resulting normalized images and smoothed using an 8-mm full-width at half-maximum isotropic Gaussian filter. This mean image served as a brain template specific to the whole sample. Each PET image was then spatially normalized onto this group-specific brain template. Finally, images were smoothed with a 12-mm full-width at half-maximum filter.
A high-resolution T1-weighted image (3D MDEFT) was acquired on a 3T Siemens Allegra scanner using the following parameters: TR/TE/TI = 7.92/2.4/910 ms, FA = 15°, FOV = 256 × 240 × 176 mm2, 1 mm isotropic spatial resolution (74). Normalized modulated images of gray matter density were extracted with default parameters via the VBM toolbox in SPM.
The accuracy of episodic and semantic FOK judgments was first analyzed by means of the proportions of correct and incorrect yes and no predictions. Correct yes/no predictions correspond to cases where the FOK judgment matched the actual recognition performance (e.g., a correct yes prediction is seen when a participant predicted that s/he will be able to recognize the word and was indeed correct when choosing the target during the recognition phase). In contrast, incorrect yes/no predictions refer to a mismatch between the FOK prediction and recognition performance: “yes” judgments associated with incorrect recognition represent an overestimation indicator, and “no” judgments associated with correct recognition represent an underestimation indicator. Second, the accuracy of episodic and semantic FOK judgments was analyzed by the Hamann coefficient (75) that measures the degree to which FOK predictions match correct and incorrect recognition performance. The coefficient is obtained by [H = ((a+d)−(b+c))/((a+d) + (b+c))], where (a) refers to the correct yes predictions, (d) correct no predictions, (b) incorrect yes predictions and (c) incorrect no predictions. For the MARS, the measure of interest was the discrepancy score.
Metamemory measures were submitted to analyses of variance (ANOVAs) with group (controls, converters, non-converters) as between-subject variable. The statistical threshold was set at p < 0.05.
For all analyses, SPM12 statistical analyses were performed by estimating parameters according to the general linear model at each voxel. Moreover, in order to control for individual variation in global FDG uptake, images were proportionally scaled to values from a cluster of preserved activity in the patients situated in the sensorimotor area (76). As a first analysis, group comparisons were performed by using a factorial design with the preprocessed PET images of the three groups. Linear contrasts examined regions that were less active in converters patients than controls, in non-converters patients than controls, in converters patients than in non-converters patients and vice versa. Four additional whole-brain analyses were conducted to evaluate the correlations between cerebral metabolism and each of 4 self-awareness measures: number of correct “yes” predictions in episodic FOK task, Hamann coefficient in episodic FOK task, Hamann coefficient in semantic FOK task, and discrepancy score in the MARS. Linear contrasts assessed correlations with accuracy of self-awareness in each group as well as correlations that were specific to a group of patients compared to the other (correlations in converters > non-converters, correlations in non-converters > converters). For whole-brain statistical analyses, the statistical threshold was set at p < 0.05 FWE-corrected for multiple comparisons at the voxel-level. Moreover, we assessed correlations in regions of interest (ROI) with a priori hypotheses. Coordinates described as significant correlates of self-awareness in studies using the same kind of tasks as the ones used here (see Table 2) were labeled with the anatomical automatic labeling (AAL) atlas (97) and AAL regions were selected as a priori ROIs if they appear in more than one article. For correlational analyses, small volume correction analyses (thresholded at p < 0.05 corrected for multiple comparisons) were applied on these a priori ROIs.

Table 2. A priori AAL ROIs for correlations between self-awareness measures and brain metabolism and structure.
Gray matter density images from VBM were entered in SPM12 analyses with parameter estimation using a general linear model. The first analysis compared the images between groups in order to identify regions of lower gray matter density in converters and non-converters patients. The other analyses were correlational analyses examining correlations between gray matter density and the 4 self-awareness measures (number of correct “yes” predictions in episodic FOK task, Hamann coefficient in episodic FOK task, Hamann coefficient in semantic FOK task, and discrepancy score in the MARS). As for the analyses of PET images, correlations were searched in each group individually and in each patient group by comparison to the other. For whole-brain analyses, the statistical threshold was set at p < 0.05 FWE-corrected for multiple comparisons. Moreover, correlational analyses on a priori ROIs (Table 2) were conducted with small volume corrections analyses (thresholded at p < 0.05 corrected for multiple comparisons).
Scores for the FOK tasks as a function of group are presented in Table 3.
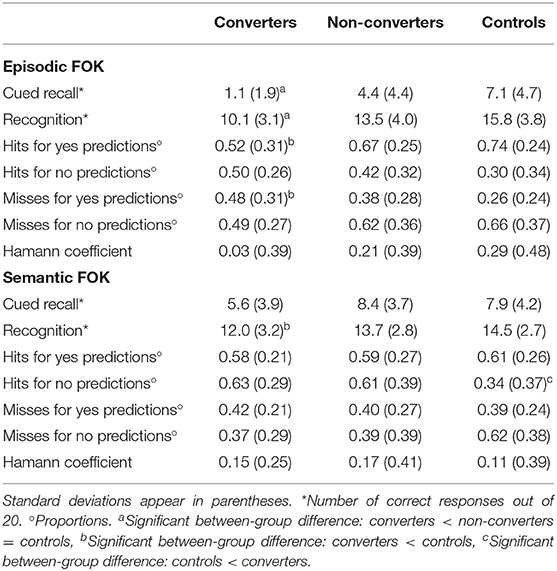
Table 3. Feeling-of-knowing scores.
Episodic FOK. Episodic memory performance was measured by the number of correctly recalled word in the cued recall phase and the number of correct recognition decisions in the forced-choice recognition phase. There were significant group differences in cued recall performance, F(2, 69) = 14.5, p < 0.001, η2p = 0.29. A HSD Tukey post-hoc test indicated that converters patients had poorer recall scores than non-converters and controls groups (ps < 0.05), who differed only marginally from each other (p = 0.07). Recognition memory performance also differed between groups, F(2, 69) = 15.3, p < 0.001, η2p = 0.30, with poorer performance in converters patients compared to the other two groups (ps < 0.05). The accuracy of FOK judgments was first analyzed by means of the proportions of correct and incorrect yes and no predictions. There were group differences with moderate effect sizes for correct, F(2, 67) = 3.96, p < 0.05, η2p = 0.11, and incorrect, F(2, 69) = 3.67, p < 0.05, η2p = 0.09, yes predictions only. Converters patients made less correct (p < 0.05) and more incorrect (p < 0.05) yes predictions than controls, indicating that converters overestimated their ability to subsequently recognize unrecalled words. Prediction accuracy in non-converters patients did not differ from that of controls, nor of converters patients. No significant group differences were found for correct and incorrect “no” predictions. Second, with regard to Hamann coefficient, the ANOVA on the Hamman coefficient did not yield any significant group differences, F(2, 69) = 2.27, p = 0.11, η2p = 0.06. However, the coefficient was significantly above 0 in controls, t(28) = 3.16, p < 0.01, and non-converters patients, t(21) = 2.47, p < 0.05, suggesting accurate FOK judgments. In contrast, in converters patients, the coefficient did not differ from zero, t(23) = 0.41, p = 0.67, revealing that predictions did not correspond to actual recognition performance in that group.
Semantic FOK. Performance for general knowledge recall and recognition phases was measured by the number of correctly produced (cued recall) words in response to the definition and the number of correctly identified words in the forced-choice recognition phase. There was a group difference for cued recall, F(2, 69) = 3.14, p < 0.05, η2p = 0.08, but HSD Tukey post-hoc tests only indicated a trend for poorer performance in converters compared to non-converters (p = 0.06). For recognition performance, the effect of group was significant, F(2, 69) = 4.81, p < 0.05, η2p = 0.12, and was due to poorer performance in converters compared to controls (p < 0.05). With regard to FOK accuracy, the analyses of the proportions of correct and incorrect yes and no predictions only revealed group differences for correct no predictions, F(2, 54) = 4.01, p < 0.05, η2p = 0.12, which were higher in converters than controls (p < 0.05). The Hamann coefficient did not differ between groups, F(2, 68) = 0.21, p = 0.81, η2p = 0.001. It was reliably non-zero only in the converters group, t(23) = 2.84, p < 0.01. The coefficient was not significantly above zero for the controls, t(27) = 1.40, p = 0.17, and only marginally for non-converters patients, t(21) = 1.91, p = 0.07. This indicated that converters patients were good at predicting their ability to identify the word corresponding to the definition in the recognition phase, whereas controls were not and tended to underestimate their recognition performance1.
The discrepancy score indexing awareness of memory functioning is presented in Figure 1. It was close to zero both in the control and non-converters groups, suggesting good agreement between the participant's and the informant's evaluation of memory functioning. The ANOVA revealed a significant group difference with a large effect size, F(2, 66) = 8.44, p < 0.001, η2p = 0.20, reflecting higher discrepancy scores in the converters group than in the other two groups (HSD Tukey post-hoc tests, ps < 0.01). The high positive score indicated that converters patients overestimated their memory functioning in everyday life situations.
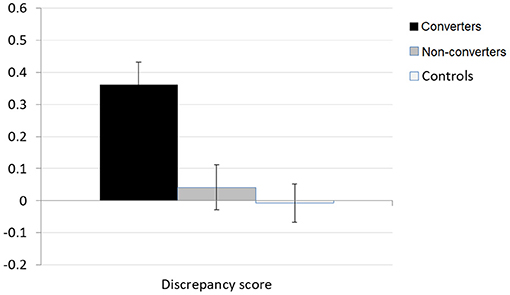
Figure 1. MARS-MFS discrepancy score.
Given that the three groups differed in terms of the presence of depression symptoms (Geriatric Depression Scale –GDS- scores), we verified whether the above-mentioned metacognitive measures were correlated with the GDS scores. None of the correlations was significant (all ps > 0.11). We also repeated the ANOVAs by including GDS scores as a covariate. The results of all analyses, except one, remained the same as reported above. The ANCOVA on the proportion of correct no predictions in the semantic FOK task did not reveal any more group differences, F(1, 54) = 3.0, p = 0.057, η2p = 0.10.
In order to assess whether poor awareness in converters observed in the FOK task for episodic material was related to poor awareness on the everyday questionnaire MARS, Pearson correlations were computed between proportions of correct and incorrect yes predictions and Hamann coefficient from the episodic FOK tasks on the one hand, and discrepancy index from the MARS scale on the other hand. None of these correlations reached significance (ps > 0.35). Additionally, converters patients were divided into aware and unaware patients by means of a z-score comparing each patient's MARS discrepancy score to the controls' mean and standard deviation. A patient was called unaware if his/her discrepancy score deviated from the controls' means by more than 2 standard deviations. A majority of converters patients were found to be unaware of their memory functioning (n = 18 out of 23), while only five patients were classified as aware of their memory functioning. FOK performance of these subgroups were compared with non-parametric Mann-Whitney tests. No significant difference was found for any measure (ps > 0.43). Altogether, lack of awareness for everyday life memory difficulties was not found to be associated with impaired monitoring during episodic memory retrieval, suggesting that these measures reflect different aspects of memory awareness.
SPM12 group comparisons on PET images of cerebral metabolism (Figure 2A) showed a large pattern of hypometabolism in converters patients compared to controls involving the posterior cingulate cortex and bilateral fronto-temporo-parietal regions. Non-converters patients demonstrated mainly a hypometabolic posterior cingulate cortex. Direct patients group comparison indicated that, compared to non-converters patients, converters patients had diminished activity in temporo-parietal areas and in the right dorsolateral prefrontal cortex. There was no region showing less metabolic activity in non-converters patients than converters patients.
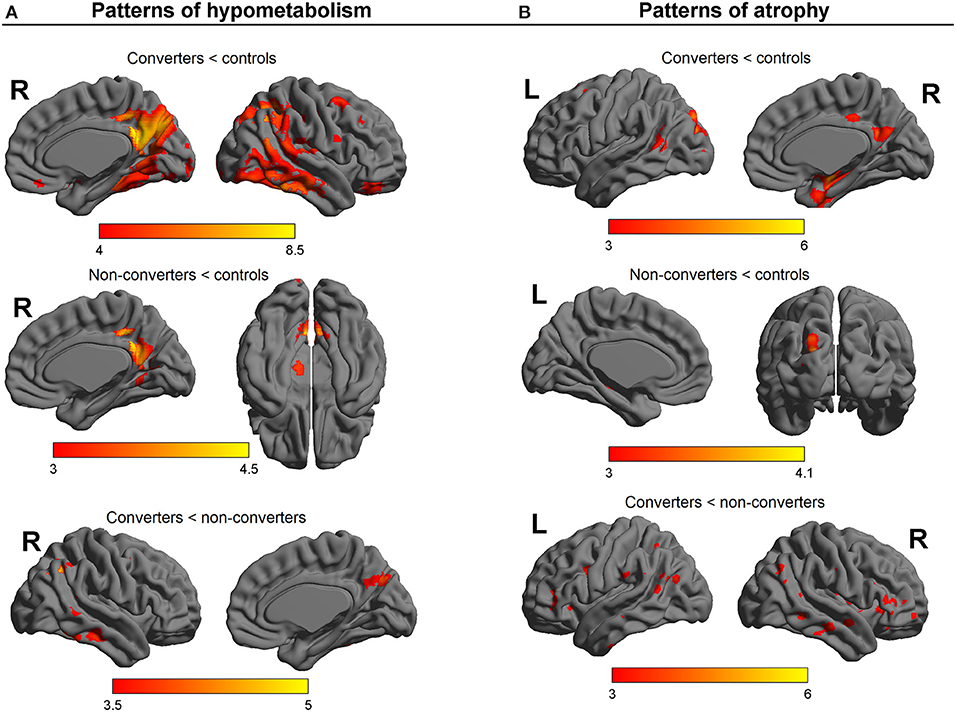
Figure 2. SPM results of group comparisons on (A) PET images of cerebral metabolism and (B) MR images of gray matter density. Color scale: T values.
The images of gray matter density extracted with VBM were also compared between groups. The results of the SPM comparisons are presented in Figure 2B. Compared to controls, converters patients presented with lower gray matter density predominantly in the hippocampi and left temporal regions. Converters patients also showed reduced gray matter density in bilateral parietal areas and precuneus, occipital regions, insula, and right dorsolateral prefrontal cortex. When compared to controls, non-converters patients appeared to have lower gray matter density in left parieto-occipital areas and the posterior hippocampus. By comparison to non-converters patients, converters patients displayed lower gray matter density in frontal, parietal and temporal regions, the insula, the precuneus, as well as occipital areas and the cerebellum. No region showed less gray matter density in non-converters patients than converters patients.
No region survived the statistical threshold of p < 0.05 corrected for multiple comparisons for whole-brain correlation analyses. The results of small volume correction analyses performed on a priori ROIs are presented in Table 4.
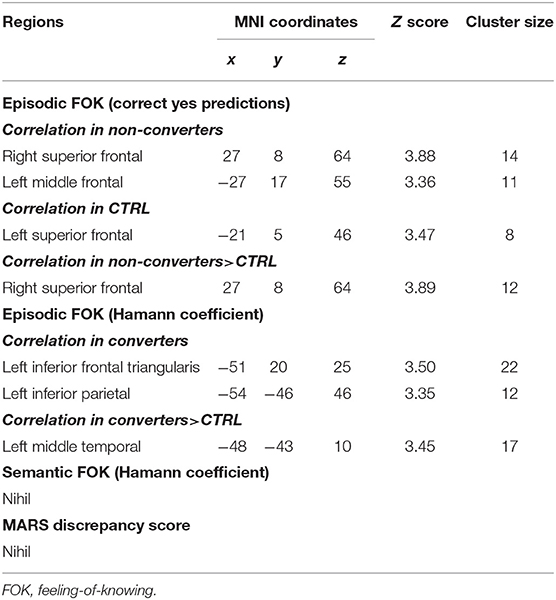
Table 4. SPM results: Significant correlations between regional metabolism and self-awareness measures (small volume correction, p < 0.05 FWE-corrected for multiple comparisons).
Episodic FOK. In non-converters patients, the proportion of correct prediction of subsequent recognition correlated positively with metabolism of the right superior (non-converters > CTRL) and left middle prefrontal cortex. In controls, the proportion of correct “yes” predictions correlated with metabolism of the left superior prefrontal cortex. In converters patients, FOK accuracy as indexed by Hamann coefficient correlated positively with metabolism of the left inferior prefrontal cortex and left inferior parietal cortex, as well as of the left middle temporal cortex (the latter showing more correlation in converters compared to CTRL).
Semantic FOK. There was no significant cognitive-metabolic correlation for semantic FOK score.
MARS discrepancy score. No region was found to show correlation with self-awareness of daily life memory functioning.
No region survived the statistical threshold of p < 0.05 corrected for multiple comparisons for whole-brain correlation analyses. The results of small volume correction analyses performed on a priori ROIs are presented in Table 5.
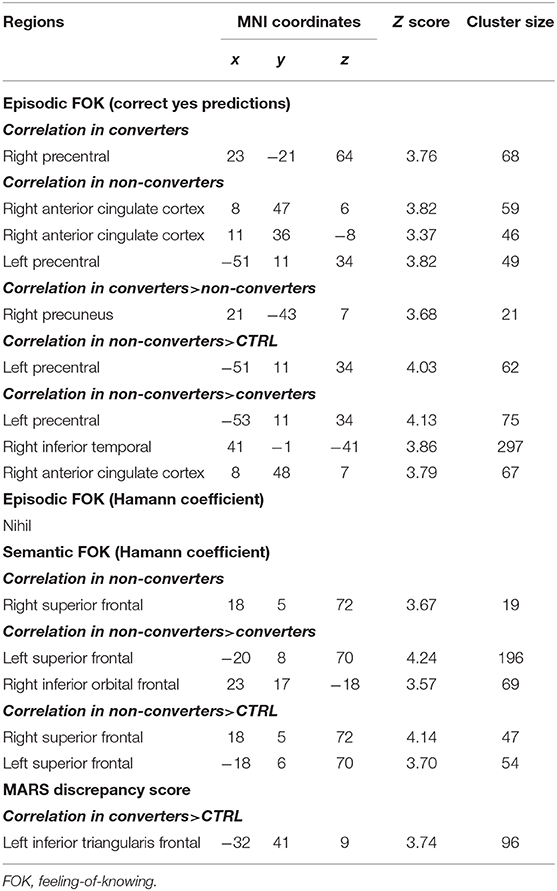
Table 5. SPM results: Significant correlations between regional gray matter density and self-awareness measures (small volume correction, p < 0.05 FWE-corrected for multiple comparisons).
Episodic FOK. Correlations were observed for the proportion of correct “yes” predictions, but not for Hamann coefficient. In converters patients, accurate predictions of subsequent recognition correlated positively with gray matter density of the precentral cortex and the right precuneus (for the latter, converters > non-converters). In non-converters patients more than in converters and controls, greater correct “yes” predictions was associated with greater gray matter density in the right anterior cingulate cortex, the left precentral cortex, and the right inferior temporal cortex.
Semantic FOK. In non-converters patients more than in the other groups, FOK accuracy in the semantic task correlated positively with gray matter density in the superior frontal cortex bilaterally and the inferior orbitofrontal cortex.
MARS discrepancy score. In converters patients more than in controls, lower self-awareness of memory functioning was associated with lower gray matter density in the left inferior prefrontal cortex.
Although it is well-established that patients with Alzheimer's disease often present with anosognosia, the findings are less clear in the earlier stages of the disease, such as MCI. Yet, given that the prodromal stage of AD is a window for interventions, identifying lack of awareness as a potential brake to treatment is important. In the current study, we evaluated self-awareness of memory functioning in MCI using two kinds of measures: FOK judgments assessing online monitoring of performance and patient vs. informant assessment of daily life memory functioning. Given the heterogeneous nature of MCI, self-awareness measures were analyzed as a function of the clinical outcome of a 4 year follow-up in order to test the hypothesis that poor self-awareness of memory should be observed mainly in those MCI who are in the prodromal stage and who rapidly progress to overt dementia (converters). Finally, FDG-PET and structural MRI were used to evaluate the neural correlates of self-awareness for memory in converters and non-converters.
Using two different measures of self-awareness for episodic memory functioning, the current study indicates that decreased appraisal of one's memory deficits exists in MCI, taking the form of overestimation of performance as indicated in previous reports (12, 13, 15, 17, 29, 30). Importantly, this lack of awareness appears to characterize mainly those MCI patients who progressed (converted) to Alzheimer's disease in the subsequent years. In the episodic FOK task, the accuracy of FOK judgments was at chance level and patients claimed that they would recognize the target words, but actually did not. In the MARS, converters patients rated their everyday memory functioning as better than did their informants. Non-converters patients' self-awareness profile was closer to that of control participants, with above zero episodic FOK accuracy and self-assessment of everyday memory that matched those of their informants. Nevertheless, for episodic FOK, no significant difference was observed with converters' scores, nor with controls' scores, suggesting that even if metacognitive appraisal was above chance, non-converters might be in-between converters and controls in terms of performance. The finding is consistent with previous longitudinal studies that suggested that anosognosia would be a characteristic of prodromal AD (34–39). Therefore, poor self-awareness for memory deficits in aMCI patients would be both an alerting signal about the likely progression toward dementia of the patient and a symptom deserving specific treatment given its consequences for the patient and the caregivers (98, 99).
The current study brings some information about the nature of the neurocognitive difficulties in converters relative to self-awareness of memory. First, even if converters patients overestimated their memory capacities in both the episodic FOK task and the MARS, there was no correlation between the two measures. In that regard, previous studies had mixed findings: some found a significant association between scores across measures (e.g., task-based metamemory measures vs. self-awareness as assessed by questionnaires or clinician's rating) (100, 101), but others did not (12, 102). Here, we argue that the lack of correlation may reflect the fact that the episodic FOK task and the MARS actually represent two distinct dimensions of metamemory: while the MARS would rather assess general knowledge and beliefs about ones' memory, the episodic FOK task would evaluate the ability to monitor memory processes as they unfold. Knowledge and monitoring are the two main components of metamemory (43, 47), and although they interact, they are independent mechanisms. In the current study, converters patients appear to have independent difficulties affecting both dimensions of metamemory.
Second, if we consider specifically the FOK tasks, it seems that metamemory difficulties in prodromal AD are restricted to monitoring of episodic retrieval mechanisms. In contrast, monitoring of episodic encoding processes was previously shown to be preserved in MCI (103). Moreover, metamemory in semantic memory tasks is intact in MCI, as shown here for semantic FOK and in another study on confidence judgments for general knowledge questions (104). Therefore, converters patients appear to have a specific difficulty in making metamemory decisions about the content of episodic memory retrieval.
In converters patients, correlations with neuroimaging data indicated that episodic FOK accuracy was associated with metabolism of the left inferior prefrontal cortex, the left inferior parietal cortex and the left middle temporal cortex. Moreover, the overestimation of subsequent recognition (less correct yes prediction) was associated with decreased gray matter density in the right precentral cortex and precuneus in the patients. At overlapping coordinates, the inferior prefrontal cortex was activated when young participants reported the subjective experience of knowing that an item is available for retrieval (82, 88). But in episodic memory tasks, this area is thought to support a more general selection process that operates post-retrieval to resolve competition among active representations (105). In FOK task, this process might help decide whether partial cues about the sought-for item are decisive or not for the likelihood of retrieval. In fMRI studies, the left inferior parietal cortex and the left middle temporal cortex were found to be activated specifically for episodic FOK judgments by contrast to semantic FOK judgments (77, 82) and to track the intensity of feelings of knowing (81). An influential view of the role of parietal regions in episodic memory suggests that the inferior parietal cortex supports bottom-up attraction of attention toward reactivated memory content, especially during recollection (106). As for the middle temporal cortex, it is usually associated with semantic processing and could reflect access to some personal information about memory abilities (107). The right precentral cortex is also activated during FOK tasks, but is common to both episodic and semantic tasks (81, 82, 86, 87, 107). As part of the dorsal attention network (108), the precentral cortex may track the effort engaged in a memory task (109). Finally, in FOK judgments, the precuneus is specifically involved in episodic tasks (77, 82). Its connection with the frontal and parietal areas during self-appraisal would bring self-referential processes in line with cognitive control over the content of memory retrieval (16). Altogether, the neural correlates of episodic FOK judgments in converters suggest that their difficulties are mainly related to mechanisms supporting attribution processes interpreting the activated memory content (such as partial cues) in an attempt to rate the likelihood of subsequent recognition (110).
Contrary to converters patients, non-converters patients showed above-chance episodic FOK judgments. Variability in the accuracy of positive predictions was mainly related to the structural and functional integrity of dorsolateral prefrontal regions and anterior cingulate cortex. Therefore, efficient metamemory decisions would depend on the efficacy of cognitive control and error monitoring during the episodic retrieval process (111, 112). Similarly, in non-converters patients, the structural integrity of the superior prefrontal cortex was associated with the accuracy of FOK judgments in the semantic memory task. Consistently, in Reggev et al. (82), the superior frontal cortex was commonly activated by episodic and semantic FOK judgments. This brain region is among those that are engaged when control needs to be exerted over assessment of mental states (113). In brief, the neural correlates of FOK judgments in non-converters patients involve mainly areas contributing to the control and manipulation of mental contents.
With regard to patient-informant discrepancy on the MARS, the current study indicated that only converters patients overestimated their memory abilities in everyday life. Moreover, patients who showed more anosognosia had lower gray matter density in the left inferior prefrontal cortex. This is consistent with a previous study showing that, in MCI patients who progressed to dementia, lack of awareness of memory functioning assessed with a questionnaire correlated also with gray matter density of the ventrolateral prefrontal cortex, although it was right-sided in that study (35). As mentioned above, the left inferior prefrontal cortex is thought to select among competitive responses during memory tasks (105), especially within semantic memory tasks during which it is crucial to inhibit predominant but irrelevant conceptual representations for the task at hand (114). In the framework of the Cognitive Awareness Model (42), this inhibition mechanism may operate during the comparison processes when a mismatch is detected between knowledge about oneself and the occurrence of memory failures. Outdated personal representations should be inhibited, in order to refer to more recent self-views of impaired functioning. Although speculative, this hypothesis would suggest that anosognosia would start in the prodromal phase of AD by deficient inhibitory mechanisms over different facets of memory representations.
The current study have some limitations. First, besides neurodegeneration markers, Alzheimer pathology was not confirmed by measures of amyloid and tau accumulation. Second, metacognitive measures focused on monitoring and did not include measures of control which designates the ability to adapt one's behavior based on a priori knowledge (47), nor other measures of factors that could affect self-assessment of performance in FOK tasks, such as self-image, anxiety sensations, or environmental noise.
In brief, the current study indicated that two dimensions of self-awareness -monitoring of retrieval in episodic memory and knowledge about ones' memory abilities- are impaired in MCI patients who progressed to AD, but not (or at least less so) in MCI patients who remained stable at mid-term follow-up. The neural correlates of these deficits suggest an hypothetical contribution of decreased controlled mechanisms during interpretation of retrieved memory content in the generation of FOK judgements and deficient inhibitory selection of semantic traces during appraisal of everyday life memory functioning. Such speculative mechanisms should be tested in future longitudinal studies tracking regularly self-awareness as well as cognitive functioning and brain integrity in order to explore the hypothesis that anosognosia emerges when some critical neurocognitive mechanisms allowing awareness of memory functioning fail.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of Liège University Hospital, Liège, Belgium. The patients/participants provided their written informed consent to participate in this study.
CB and ES contributed to the conception and design of the study. FG, FM, and CL produced FDG for neuroimaging acquisition. BG and ES recruited and screened patients. CB and ES acquired behavioral and neuroimaging data and drafted the manuscript. CB analyzed the data. All authors contributed to the article and approved the submitted version.
This work was supported by the SAO-FRA [grant #08612], by the University of Liège (grant FSR-F-M-19/6762), and by the F.R.S.-Fonds National de la Recherche Scientifique (grant 3.4513.11). CB is a Research Associate at F.R.S.-FNRS.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank Céline Souchay for providing the materials of the task.
1. ^The results relative to FOK accuracy were not due to an excessive liberal use of “yes” predictions in patients. In the episodic FOK task, converters patients made significantly less “yes” FOK judgments than the other groups, F(2, 69) = 5.3, p < 0.01, whereas in the semantic FOK task, there was no group difference in the proportion of “yes” judgments, F(2, 69) = 0.7, p = 0.48.
2. Starkstein SE. Anosognosia in Alzheimer's disease: diagnosis, frequency, mechanism and clinical correlates. Cortex. (2014) 61:64–73. doi: 10.1016/j.cortex.2014.07.019
3. Clare L, Wilson BA, Carter G, Roth I, Hodges JR. Assessing awareness in early-stage Alzheimer's disease: development and piloting of the Memory Awareness Rating Scale. Neuropsychol Rehabil. (2002) 12:341–62. doi: 10.1080/09602010244000129
4. Sunderaraman P, Cosentino S. Integrating the constructs of anosognosia and metacognition: a review of recent findings in dementia. Curr Neurol Neurosci Rep. (2017) 17:27. doi: 10.1007/s11910-017-0734-1
5. Ernst A, Moulin CJA, Souchay C, Mograbi DC, Morris R. Anosognosia and metacognition in Alzheimer's disease: insights from experimental psychology. In: Dunlosky J, Tauber SUK, editors. The Oxford Handbook of Metamemory. Oxford: Oxford University Press (2015). pp. 451–72.
6. Souchay C. Metamemory in Alzheimer's disease. Cortex. (2007) 43:987–1003. doi: 10.1016/S0010-9452(08)70696-8
7. Genon S, Simon J, Bahri MA, Collette F, Souchay C, Jaspar M, et al. Relating pessimistic memory predictions to Alzheimer's disease brain structure. Cortex. (2016) 85:151–64. doi: 10.1016/j.cortex.2016.09.014
8. Souchay C, Isingrini M, Gil M. Alzheimer's disease and feeling-of-knowing in episodic memory. Neuropsychologia. (2002) 40:2386–96. doi: 10.1016/S0028-3932(02)00075-1
9. Petersen RC, Negash S. Mild cognitive impairment: an overview. CNS Spectr. (2008) 13:45–53. doi: 10.1017/S1092852900016151
10. Petersen RC, Doody R, Kurz A, Mohs RC, Morris JC, Rabins PV, et al. Current concepts in Mild Cognitive Impairment. Arch Neurol. (2001) 58:1985–92. doi: 10.1001/archneur.58.12.1985
11. Roberts JL, Clare L, Woods RT. Subjective memory complaints and awareness of memory functioning in mild cognitive impairment: a systematic review. Dement Geriatr Cogn Disord. (2009) 28:95–109. doi: 10.1159/000234911
12. Galeone F, Pappalardo S, Chieffi S, Iavarone A, Carlomagno S. Anosognosia for memory deficit in amnestic mild cognitive impairment and Alzheimer's disease. Int J Geriatr Psychiatry. (2011) 26:695–701. doi: 10.1002/gps.2583
13. Hanyu H, Sakurai H, Iwamoto T. Are subjective memory complaints mandatory for the diagnosis of mild cognitive impairment? Intern Med. (2007) 46:791–2. doi: 10.2169/internalmedicine.46.6241
14. Mak E, Chin R, Ng LT, Yeo D, Hameed S. Clinical associations of anosognosia in mild cognitive impairment and Alzheimer's disease. Int J Geriatr Psychiatry. (2015) 30:1207–14. doi: 10.1002/gps.4275
15. Onor ML, Trevisiol M, Negro C, Aguglia E. Different perception of cognitive impairment, behavioral distrubances, and functional diabilities between persons with mild cognitive impairment and mild Alzheimer's disease and their caregivers. J Alzheimer's Dis. (2006) 21:333–8. doi: 10.1177/1533317506292454
16. Vannini P, Hanseeuw B, Munro CE, Amariglio RE, Marshall GA, Rentz DM, et al. Anosognosia for memory deficits in mild cognitive impairment: insight into the neural mechanism using functional and molecular imaging. Neuroimage Clin. (2017) 15:408–14. doi: 10.1016/j.nicl.2017.05.020
17. Vogel A, Hasselbach SG, Gade A, Ziebell M, Waldemar G. Cognitive and functional neuroimaging correlates for anosognosia in mild cognitive impairment and Alzheimer's disease. Int J Geriatr Psychiatry. (2005) 20:238–46. doi: 10.1002/gps.1272
18. Vogel A, Stokholm J, Gade A, Andersen BB, Hejl AM, Waldemar G. Awareness of deficits in mild cognitive impairment and Alzheimer's disease: do MCI patients have impaired insight? Dement Geriatr Cogn Disord. (2004) 17:181–7. doi: 10.1159/000076354
19. Clément F, Belleville S, Gauthier S. Cognitive complaint in mild cognitive impairment and Alzheimer's disease. J Int Neuropsychol Soc. (2008) 14:222–32. doi: 10.1017/S1355617708080260
20. Cook S, Marsiske M. Subjective memory beliefs and cognitive performance in normal and mildly impaired older adults. Aging Ment Health. (2006) 10:413–23. doi: 10.1080/13607860600638487
21. Greenop KR, Xiao J, Almeida OP, Flicker L, Beer C, Foster JK, et al. Awareness of cognitive deficits in older adults with cognitive-impairment-no-dementia (CIND): comparison with informant report. Alzheimer Dis Assoc Disord. (2011) 25:24–33. doi: 10.1097/WAD.0b013e3181f81094
22. Marri L, Modugno M, Iacono S, Renzetti C, De Vreese LP, Neri M. Metamemory and self-perceived health in mild cognitive impairment. Arch Gerontol Geriatr Suppl. (2001) 7:235–44. doi: 10.1016/S0167-4943(01)00144-3
23. Nobili F, Mazzei D, Dessi B, Morbelli S, Brugnolo A, Barbieri P, et al. Unawareness of memory deficit in amnestic MCI: FDG-PET findings. J Alzheimer's Dis. (2010) 22:993–1003. doi: 10.3233/JAD-2010-100423
24. Orfei MD, Varsi AE, Blundo C, Celia E, Casini AR, Caltagirone C, et al. Anosognosia in mild cognitive impairment and mild Alzheimer's disease: frequency and neuropsychological correlates. Am J Geriatr Psychiatry. (2010) 18:1133–40. doi: 10.1097/JGP.0b013e3181dd1c50
25. Clare L Whitaker CJ Roberts JL Nelis SM Martyr A Marková IS . Memory awareness profiles differentiate mild cognitive impairment from early-stage dementia: evidence from assessments of performance monitoring and evaluative judgement. Dement Geriatr Cogn Disord. (2013) 35:266–79. doi: 10.1159/000346735
26. Kalbe E, Salmon E, Perani D, Holthoff V, Sorbi S, Elsner A, et al. Anosognosia in very mild Alzheimer's disease but not in mild cognitive impairment. Dement Geriatr Cogn Disord. (2005) 19:349–56. doi: 10.1159/000084704
27. Piras F, Piras F, Orfei MD, Caltagirone C, Spalletta G. Self-awareness in Mild Cognitive Impairment: quantitative evidence from systematic review and meta-analysis. Neurosci Biobehav Rev. (2016) 61:90–107. doi: 10.1016/j.neubiorev.2015.10.002
28. Fragkiadaki S, Kontaxopoulou D, Beratis IN, Andronas N, Economou A, Yannis G, et al. Self-awareness of cognitive efficiency: differences between healthy elderly and patients with mild cognitive impairment (MCI). J Clin Exp Neuropsychol. (2016) 38:1144–57. doi: 10.1080/13803395.2016.1198469
29. Perrotin A, Belleville S, Isingrini M. Metamemory monitoring in mild cognitive impairment: evidence of a less accurate episodic feeling-of-knowing. Neuropsychologia. (2007) 45:2811–26. doi: 10.1016/j.neuropsychologia.2007.05.003
30. Anderson JW, Schmitter-Edgecombe M. Mild cognitive impairment and feeling-of-knowing in episodic memory. J Clin Exp Neuropsychol. (2010) 32:505–14. doi: 10.1080/13803390903224944
31. Ryals AJ, O'Neil JT, Mesulam MM, Weintraub S, Voss JL. Memory awareness disruptions in amnestic mild cognitive impairment: comparison of multiple awareness types for verbal and visuospatial material. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn. (2019) 26:577–98. doi: 10.1080/13825585.2018.1503994
32. Butters MA, Young JB, Lopez O, Aizenstein HJ, Mulsant BH, Reynolds CF III., et al. Pathways linking late-life depression to persistent cognitive impairment and dementia. Dialogues Clin Neurosci. (2008) 10:345–57. doi: 10.31887/DCNS.2008.10.3/mabutters
33. Palmer K, Fratiglioni L, Winblad B. What is mild cognitive impairment? Variations in definitions and evolution of nondemented persons with cognitive impairment. Acta Neurol Scand. (2003) 107:14–20. doi: 10.1034/j.1600-0404.107.s179.2.x
34. Hanseeuw BJ, Scott MR, Sikkes SAM, Properzi M, Gatchel JR, Salmon E, et al. Evolution of anosognosia in Alzheimer's disease and its relationship to amyloid. Ann Neurol. (2020) 87:267–80. doi: 10.1002/ana.25649
35. Spalletta G, Piras F, Piras F, Sancesario G, Iorio M, Fratangeli C, et al. Neuroanatomical correlates of awareness of illness in patients with amnestic mild cognitive impairment who will or will not convert to Alzheimer's disease. Cortex. (2014) 61:183–95. doi: 10.1016/j.cortex.2014.10.010
36. Scherling CS, Wilkins SE, Zakrezewski J, Kramer JH, Miller BL, Weiner MW, et al. Decreased self-appraisal accuracy on cognitive tests of executive functioning is a predictor of decline in mild cognitive impairment. Front Aging Neurosci. (2016) 8:120. doi: 10.3389/fnagi.2016.00120
37. Gerretsen P, Chung JK, Shah P, Plitman E, Iwata Y, Caravaggio F, et al. Anosognosia is an independent predictor of conversion from mild cognitive impairment to Alzheimer's disease and is associated with reduced brain metabolism. J Clin Psychiatry. (2017) 78:e1187–96. doi: 10.4088/JCP.16m11367
38. Therriault J, Ng KP, Pascoal TA, Mathotaarachchi S, Kang MS, Struyfs H, et al. Anosognosia predicts default mode network hypometabolism and clinical progression to dementia. Neurology. (2018) 90:e932–9. doi: 10.1212/WNL.0000000000005120
39. Tabert MH, Albert SM, Borukhova-Milov L, Camacho Y, Pelton G, Liu X, et al. Functional deficits in patients with mild cognitive impairment: prediction of AD. Neurology. (2002) 58:758–64. doi: 10.1212/WNL.58.5.758
40. Vannini P, Amariglio R, Hanseeuw B, Johnson KA, McLaren DG, Chhatwal J, et al. Memory self-awareness in the preclinical and prodromal stages of Alzheimer's disease. Neuropsychologia. (2017) 99:343–9. doi: 10.1016/j.neuropsychologia.2017.04.002
41. Silva MR, Moser D, Pfluger M, Pusswald G, Stogmann E, Dal-Bianco P, et al. Self-reported and informant-reported memory functioning and awareness in patients with mild cognitive impairment and Alzheimer s disease. Neuropsychiatrie. (2016) 30:103–12. doi: 10.1007/s40211-016-0185-y
42. Morris RG, Mograbi DC. Anosognosia, autobiographical memory and self knowledge in Alzheimer's disease. Cortex. (2013) 49:1553–65. doi: 10.1016/j.cortex.2012.09.006
43. Toglia J, Kirk U. Understanding awareness deficits following brain injury. Neurorehabilitation. (2000) 15:57–70. doi: 10.3233/NRE-2000-15104
44. Mograbi DC, Brown RG, Morris RG. Anosognosia in Alzheimer's disease: the petrified self. Conscious Cogn. (2009) 18:989–1003. doi: 10.1016/j.concog.2009.07.005
45. Rosen HJ. Anosognosia in neurodegenerative disease. Neurocase. (2011) 17:231–41. doi: 10.1080/13554794.2010.522588
46. Koriat A. How do we know that we know? The accessibility model of the feeling of knowing. Psychol Rev. (1993) 100:609–39. doi: 10.1037/0033-295X.100.4.609
47. Nelson TO, Narens L. Metamemory: a theoretical framework and some new findings. In: GH. Bower, editor. The Psychology of Learning and Motivation, Vol. 26. San Diego, CA: Academic Press (1990). pp. 125–73.
48. Koriat A, Levy-Sadot R. The combined contributions of the cue-familiarity and accessibility heuristics to feelings of knowing. J Exp Psychol Learn Mem Cogn. (2001) 27:34–53. doi: 10.1037/0278-7393.27.1.34
49. Hallam B, Chan J, Gonzalez Costafreda S, Bhome R, Huntley J. What are the neural correlates of meta-cognition and anosognosia in Alzheimer's disease? A systematic review. Neurobiol Aging. (2020) 94:250–64. doi: 10.1016/j.neurobiolaging.2020.06.011
50. Buckner RL, Andrews-Hanna JR, Schacter DL. The brain's default network. Ann N Y Acad Sci. (2008) 1124:1–38. doi: 10.1196/annals.1440.011
51. Antoine N, Bahri MA, Bastin C, Collette F, Phillips C, Balteau E, et al. Anosognosia and default mode subnetwork dysfunction in Alzheimer's disease. Hum Brain Mapp. (2019) 40:5330–40. doi: 10.1002/hbm.24775
52. Berlingeri M, Ravasio A, Cranna S, Basilico S, Sberna M, Bottini G, et al. Unrealistic representations of “the self”: a cognitive neuroscience assessment of anosognosia for memory deficit. Conscious Cogn. (2015) 37:160–77. doi: 10.1016/j.concog.2015.08.010
53. Perrotin A, Desgranges B, Landeau B, Mezenge F, La Joie R, Egret S, et al. Anosognosia in Alzheimer disease: disconnection between memory and self-related brain networks. Ann Neurol. (2015) 78:477–86. doi: 10.1002/ana.24462
54. Ries ML, McLaren DG, Bendlin BB, Xu G, Rowley HA, Birn R, et al. Medial prefrontal functional connectivitiy: relation to memory self-appraisal accuracy in older adults with and without memory disorders. Neuropsychologia. (2012) 50:603–11. doi: 10.1016/j.neuropsychologia.2011.12.014
55. Lenzoni S, Morris RG, Mograbi DC. The petrified self 10 years after: current evidence for Mnemonic anosognosia. Front Psychol. (2020) 11:465. doi: 10.3389/fpsyg.2020.00465
56. Mondragon JD, Maurits NM, De Deyn PP. Functional neural correlates of anosognosia in Mild Cognitive Impairment and Alzheimer's disease: a systematic review. Neuropsychol Rev. (2019) 29:139–65. doi: 10.1007/s11065-019-09410-x
57. McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CRJr, Kawas CH, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. (2011) 7:263–9. doi: 10.1016/j.jalz.2011.03.005
58. Pedraza O, Lucas JA, Smith GE, Petersen RC, Graff-Radford NR, Ivnik RJ. Robust and expanded norms for the Dementia Rating Scale. Arch Clin Neuropsychol. (2010) 25:347–58.
59. Deltour JJ. Echelle de vocabulaire de Mill Hill de J.C. Raven. Adaptation francaise et normes comparées du Mill Hill et du Standard Progressive Matrices (PM 38). Manuel. Braine-le-Château: Editions l'Application des Techniques Modernes (1993).
60. Yesavage JA, Brink TL, Rose TL, Lum V, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. (1983) 17:37–49. doi: 10.1016/0022-3956(82)90033-4
62. Treyer V, Buck A, Schnider A. Selection of currently relevant words: an auditory verbal memory study using positron emission tomography. Neuroreport. (2006) 17:323–7. doi: 10.1097/01.wnr.0000199457.78670.44
63. Piolino P, Desgranges B, Belliard S, Matuszweski V, Laleve C, De La Sayette V, et al. Autobiographical memory and autonoetic consciousness: triple dissociation in neurodegenerative diseases. Brain. (2003) 126:2203–19. doi: 10.1093/brain/awg222
64. Piolino P, Desgranges B, Benali K, Eustache F. Episodic and semantic remote autobiographical memory in ageing. Memory. (2002) 10:239–57. doi: 10.1080/09658210143000353
65. Levine B, Svoboda E, Hay JF, Winocur G, Moscovitch M. Aging and autobiographical memory: dissociating episodic from semantic retrieval. Psychol Aging. (2002) 17:677–89. doi: 10.1037/0882-7974.17.4.677
66. Daneman M, Carpenter PA. Individual differences in working memory and reading. J Verbal Learn Verbal Behav. (1980) 19:450–66. doi: 10.1016/S0022-5371(80)90312-6
67. Desmette D, Hupet M, Van der Linden M. Adaptation en langue française du “Reading span test” de Daneman et Carpenter 1980. L'Année Psychol. (1995) 95:459–82. doi: 10.3406/psy.1995.28842
68. Andrés P, Van der Linden M. Age-related differences in supervisory attentional system functions. J Gerontol Psychol Sci. (2000) 55B:373–80. doi: 10.1093/geronb/55.6.P373
69. Burgess PW, Shallice T. Confabulation and the control of recollection. Memory. (1996) 4:359–411. doi: 10.1080/096582196388906
70. Levinoff EJ, Phillips NA, Verret L, Babins L, Kelner N, Akerib V, et al. Cognitive estimation impairment in Alzheimer disease and mild cognitive impairment. Neuropsychology. (2006) 20:123–32. doi: 10.1037/0894-4105.20.1.123
71. Souchay C, Moulin CJA, Clarys D, Taconnat L, Isingrini M. Diminished episodic memory awareness in older adults: evidence from feeling-of-knowing and recollection. Conscious Cogn. (2007) 16:769–84. doi: 10.1016/j.concog.2006.11.002
72. Clare L, Whitaker CJ, Nelis SM. Appraisal of memory functioning and memory performance in healthy ageing and early-stage Alzheimer's disease. Aging Neuropsychol Cogn. (2010) 17:462–91. doi: 10.1080/13825580903581558
73. Lemaire C, Bamhaut P, Lauricella B, Mosdzianowski C, Morelle JL, Monclus M, et al. Fast [18 F]FDG synthesis by alkaline hydrolysis on a low polarity solid phase support. J Label Comp Radiopharm. (2002) 45:435–47. doi: 10.1002/jlcr.572
74. Deichmann R, Schwarzbauer C, Turner R. Optimisation of the 3D MDEFT sequence for anatomical brain imaging: technical implications at 1.5 and 3 T. Neuroimage. (2004) 21:757–67.
75. Schraw G. Measures of feeling of knowing accuracy: a new look at an old problem. Appl Cogn Psychol. (1995) 9:321–32. doi: 10.1002/acp.2350090405
76. Yakushev I, Landvogt C, Buchholz HG, Fellgiebel A, Hammers A, Scheurich A, et al. Choice of reference area in studies of Alzheimer's disease using positron emission tomography with fluorodeoxyglucose-F18. Psychiatry Res Neuroimaging. (2008) 164:143–53. doi: 10.1016/j.pscychresns.2007.11.004
77. Elman JA, Klostermann EC, Marian DE, Verstaen A, Shimamura AP. Neural correlates of metacognitive monitoring during episodic and semantic retrieval. Cogn Affect Behav Neurosci. (2012) 12:599–609. doi: 10.3758/s13415-012-0096-8
78. Maril A, Simons JS, Mitchell JP, Schwartz BL, Schacter DL. Feeling-of-knowing in episodic memory: an event-related fMRI study. Neuroimage. (2003) 18:827–36. doi: 10.1016/S1053-8119(03)00014-4
79. Bertrand E, Azar M, Rizvi B, Brickman AM, Huey ED, Habeck C, et al. Cortical thickness and metacognition in cognitively diverse older adults. Neuropsychology. (2018) 32:700–10. doi: 10.1037/neu0000458
80. Modirrousta M, Fellows LK. Medial prefrontal cortex plays a critical and selective role in “feeling of knowing” meta-memory judgments. Neuropsychologia. (2008) 46:2958–65. doi: 10.1016/j.neuropsychologia.2008.06.011
81. Schnyer DM, Nicholls L, Verfaellie M. The role of VMPC in metamemorial judgments of content retrievability. J Cogn Neurosci. (2005) 17:832–46. doi: 10.1162/0898929053747694
82. Reggev N, Zuckerman M, Maril A. Are all judgments created equal? An fMRI study of semantic and episodic metamemory predictions. Neuropsychologia. (2011) 49:1332–42. doi: 10.1016/j.neuropsychologia.2011.01.013
83. Jing L, Niki K, Xiaoping Y, Yue-Jia L. Knowing that you know and knowing that you don't know: a fMRI study on Feeling-of-Knowing (FOK). Acta Psychol Sin. (2004) 36:426–33. Available online at: http://www.luojlab.cn/media/files/65.pdf
84. Cosentino S, Brickman AM, Griffith E, Habeck C, Cines S, Farrell M, et al. The right insula contributes to memory awareness in cognitively diverse older adults. Neuropsychologia. (2015) 75:163–9. doi: 10.1016/j.neuropsychologia.2015.05.032
85. Chua EF, Schacter DL, Sperling RA. Neural correlates of metamemory: a comparison of feeling-of-knowing and retrospective confidence judgments. J Cogn Neurosci. (2009) 21:1751–65. doi: 10.1162/jocn.2009.21123
86. Kikyo H, Miyashita Y. Temporal lobe activations of “feeling-of-knowing” induced by face-name associations. Neuroimage. (2004) 23:1348–57. doi: 10.1016/j.neuroimage.2004.08.013
87. Kikyo H, Ohki K, Miyashita Y. Neural correlates for feeling-of-knowing: an fMRI parametric analysis. Neuron. (2002) 36:177–86. doi: 10.1016/S0896-6273(02)00939-X
88. Maril A, Simons JS, Weaver JJ, Schacter DL. Graded recall success: an event-related fMRI comparison of tip of the tongue and feeling of knowing. Neuroimage. (2005) 24:1130–8. doi: 10.1016/j.neuroimage.2004.10.024
89. Salmon E, Perani D, Herholz K, Marique P, Kalbe E, Holthoff V, et al. Neural correlates of anosognosia for cognitive impairment in Alzheimer's disease. Hum Brain Mapp. (2006) 27:588–587. doi: 10.1002/hbm.20203
90. Ford AH, Almeida OP, Flicker L, Garrido GJ, Greenop KR, Foster JK, et al. Grey matter changes associated with deficit awareness in mild cognitive impairment: a voxel-based morphometry study. J Alzheimer's Dis. (2014) 42:1251–9. doi: 10.3233/JAD-132678
91. Shibata K, Narumoto J, Kitabayashi Y, Ushijima Y, Fukui K. Correlation between anosognosia and regional cerebral blood flow in Alzheimer's disease. Neurosci Lett. (2008) 435:7–10. doi: 10.1016/j.neulet.2008.01.065
92. Ries ML, Jabbar BM, Schmitz TW, Trivedi MA, Gleason CE, Carlsson CM, et al. Anosognosia in mild cognitive impairment: relationship to activation of cortical midline structures involved in self-appraisal. J Int Neuropsychol Soc. (2007) 13:450–61. doi: 10.1017/S1355617707070488
93. Valera-Bermejo JM, De Marco M, Mitolo M, McGeown WJ, Venneri A. Neuroanatomical and cognitive correlates of domain-specific anosognosia in early Alzheimer's disease. Cortex. (2020) 129:236–46. doi: 10.1016/j.cortex.2020.04.026
94. Zamboni G, Drazich E, McCulloch E, Filippini N, Mackay CE, Jenkinson M, et al. Neuroanatomy of impaired self-awareness in Alzheimer's disease and mild cognitive impairment. Cortex. (2013) 49:668–78. doi: 10.1016/j.cortex.2012.04.011
95. Bastin C, Bahri MA, Meyer F, Manard M, Delhaye E, Plenevaux A, et al. In vivo imaging of synaptic loss in Alzheimer's disease with [18F]UCB-H positron emission tomography. Eur J Nucl Med Mol Imaging. (2020) 47:390–402. doi: 10.1007/s00259-019-04461-x
96. Tondelli M, Barbarulo AM, Vinceti G, Vincenzi C, Chiari A, Nichelli PF, et al. Neural correlates of anosognosia in Alzheimer's disease and mild cognitive impairment: a multi-method assessment. Front Behav Neurosci. (2018) 12:100. doi: 10.3389/fnbeh.2018.00100
97. Tzourios-Mazoyer N, Landeau B, Papathanassiou D, Crivello F, Etard O, Delcroix N, et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage. (2002) 15:273–89. doi: 10.1006/nimg.2001.0978
98. Engel L, Chui A, Goverover Y, Dawson DR. Optimising activity and participation outcomes for people with self-awareness impairments related to acquired brain injury: an interventions systematic review. Neuropsychol Rehabil. (2019) 29:163–98. doi: 10.1080/09602011.2017.1292923
99. Fleming JM, Ownsworth T. A review of awareness interventions in brain injury rehabilitation. Neuropsychol Rehabil. (2006) 16:474–500. doi: 10.1080/09602010500505518
100. Cosentino S, Metcalfe J, Butterfield B, Stern Y. Objective metamemory testing captures awareness of deficit in Alzheimer's disease. Cortex. (2007) 43:1004–19. doi: 10.1016/S0010-9452(08)70697-X
101. Gallo DA, Cramer SJ, Wong JT, Bennett DA. Alzheimer's disease can spare local metacognition despite global anosognosia: revisiting the confidence-accuracy relationship in episodic memory. Neuropsychologia. (2012) 50:2356–64. doi: 10.1016/j.neuropsychologia.2012.06.005
102. Leicht H, Berwig M, Gertz HJ. Anosognosia in Alzheimer's disease: the role of impairment levels in assessment of insight across domains. J Int Neuropsychol Soc. (2010) 16:463–73. doi: 10.1017/S1355617710000056
103. Akhtar S, Moulin CJA, Bowie PCW. Are people with mild cognitive impairment aware of the benefits of errorless learning? Neuropsychol Rehabil. (2006) 16:329–46. doi: 10.1080/09602010500176674
104. Chi SY, Chua EF, Kieschnick DW, Rabin LA. Retrospective metamemory monitoring of semantic memory in community-dwelling older adults with subjective cognitive decline and mild cognitive impairment. Neuropsychol Rehabil. (2020). 1–35. doi: 10.1080/09602011.2020.1831552. [Epub ahead of print].
105. Badre D, Wagner AD. Left ventrolateral prefrontal cortex and the cognitive control of memory. Neuropsychologia. (2007) 45:2883–901. doi: 10.1016/j.neuropsychologia.2007.06.015
106. Ciaramelli E, Grady CL, Moscovitch M. Top-down and bottom-up attention to memory: a hypothesis (AtoM) on the role of the posterior parietal cortex in memory retrieval. Neuropsychologia. (2008) 46:1828–51. doi: 10.1016/j.neuropsychologia.2008.03.022
107. Binder JR, Desai RH. The neurobiology of semantic memory. Trends Cogn Sci. (2011) 15:527–36. doi: 10.1016/j.tics.2011.10.001
108. Corbetta M, Shulman GL. Control of goal-directed and stimulus-driven attention in the brain. Nat Rev Neurosci. (2002) 3:201–15. doi: 10.1038/nrn755
109. Kurth S, Bahri MA, Collette F, Phillips C, Majerus S, Bastin C, et al. Alzheimer's disease patients activate attention networks in a short-term memory task. Neuroimage Clin. (2019) 23:101892. doi: 10.1016/j.nicl.2019.101892
110. Bastin C, Besson G, Simon J, Delhaye E, Geurten M, Willems S, et al. An Integrative Memory model of recollection and familiarity to understand memory deficits. Behav Brain Sci. (2019) 42:1–60. doi: 10.1017/S0140525X19000621
111. Carter CS, Van Veen V. Anterior cingulate cortex and conflict detection: an update of theory and data. Cogn Affect Behav Neurosci. (2007) 7:367–79. doi: 10.3758/CABN.7.4.367
112. Simons JS, Spiers HJ. Prefrontal and medial temporal lobe interactions in long-term memory. Nat Rev Neurosci. (2003) 4:637–48. doi: 10.1038/nrn1178
113. Hartwright CE, Apperly IA, Hansen PC. Representation, control, or reasoning? Distinct functions for theory of mind within the medial prefrontal cortex. J Cogn Neurosci. (2014) 26:683–98. doi: 10.1162/jocn_a_00520
Keywords: anosognosia, self-awareness, metamemory, Mild Cognitive Impairment, feeling-of-knowing, Alzheimer's disease, FDG-PET, MRI
Citation: Bastin C, Giacomelli F, Miévis F, Lemaire C, Guillaume B and Salmon E (2021) Anosognosia in Mild Cognitive Impairment: Lack of Awareness of Memory Difficulties Characterizes Prodromal Alzheimer's Disease. Front. Psychiatry 12:631518. doi: 10.3389/fpsyt.2021.631518
Received: 20 November 2020; Accepted: 08 March 2021;
Published: 31 March 2021.
Edited by:
Sergio Starkstein, University of Western Australia, AustraliaReviewed by:
Maria Donata Orfei, IMT School for Advanced Studies Lucca, ItalyCopyright © 2021 Bastin, Giacomelli, Miévis, Lemaire, Guillaume and Salmon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christine Bastin, Y2hyaXN0aW5lLmJhc3RpbkB1bGllZ2UuYmU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.