
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 04 March 2021
Sec. Social Psychiatry and Psychiatric Rehabilitation
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.627661
This article is part of the Research Topic Gender Dysphoria: Diagnostic Issues, Clinical Aspects and Health Promotion View all 9 articles
 Bianca Machado Borba Soll1*
Bianca Machado Borba Soll1* Anna Martha Fontanari2
Anna Martha Fontanari2 Angelo Brandelli Costa2
Angelo Brandelli Costa2 Ítala Chinazzo1
Ítala Chinazzo1 Dhiordan Cardoso Silva1
Dhiordan Cardoso Silva1 Fernanda Guadagnin1Silzá Tramontina1
Fernanda Guadagnin1Silzá Tramontina1 Maria Inês Rodrigues Lobato1
Maria Inês Rodrigues Lobato1Since 2014, the Gender Identity Program (PROTIG) of Hospital de Clínicas de Porto Alegre (HCPA) has been assisting transgender youth seeking gender-affirmative treatment offered at a public health-care service specializing in gender in southern Brazil. This article aims to analyze sociodemographic and clinical data regarding the diagnoses of gender dysphoria and gender incongruence, psychiatric comorbidities, and clinical aspects of a sample of transgender youths seeking health care in the gender identity program. The research protocol consisted of a survey of the data collected in the global psychological evaluation performed at the health-care service for youths diagnosed with gender incongruence and their caretakers. Participating in this research were 24 transgender youths between 8 and 16 years old with diagnostic overlap of gender dysphoria [Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)] and gender incongruence [International Classification of Diseases, 11th Revision (ICD-11)] and 34 of their caregivers. Of the young people, 45.8% were positive for some psychiatric comorbidity throughout their lives, with almost half (45.4%) having two or more psychiatric comorbidities in addition to gender dysphoria. The mental health professionals comprising affirmation care teams face the challenge of adapting the care protocols to the uniqueness of each demand by developing individualized forms to promote healthy development. This can be done by focusing not only on medical and physical interventions for gender affirmation but also on the promotion of mental health and general emotional well-being. Thus, the gender affirmation model, which advocates for global assessment and personalized guidance, proved to be adequate. Nevertheless, access to multidisciplinary health services specializing in gender is essential for promoting the general well-being of the population of transgender youth.
In recent years, there has been an increase in the seeking of assessment at specialized services for gender identity for youths who self-define as transgender people, requiring actions that promote the qualification of professionals focusing on this age group and technical protocols aiming at assistance standardization (1–3). The term transgender is a popular expression to include a broad spectrum of gender expressions (gender variance or gender non-conformity) that have been identified in our current society, while cisgender conceptualizes people who do not have a gender identity variant of the sex designated at birth. These expressions are not scientific terms and do not appear in any current diagnostic manual (4).
Among different possible care models for this population segment (transgender youth), what has been widely discussed and implemented today is the so-called “affirmative gender model,” which starts from the conceptual premise of the existence of different expressions and gender identities in society and the concept that each individual can be encouraged to discover his or her own expression, if he or she has a suitable environment for it, thus enhancing his or her emotional well-being (5). Because it is an approach that values the uniqueness of each experience and the context in which the young person is inserted, affirmative gender practice involves careful assessment and considers family dynamics, psychological profiles, the presence of diagnostic criteria for gender dysphoria (GD)/gender incongruence (GI), possible secondary gains, and the occurrence of clinical and/or psychiatric comorbidities (6). It should be noted that this care model also considers the complexity of factors that involve the specific stage of development (transition from childhood to adulthood), such as the age of legal majority, which can differ from country to country (7), the freedom or not of gender expression in the individual's social group and the assistance support that is available. Despite being a relatively new approach and still lacking scientific research, it is not limited to assessing whether young people should simply start the medical gender-affirmative treatments available for them but focuses on the global assessment of development (8).
Recent research with groups of transgender youth who access specialized health-care services has shown a high level of vulnerabilities in mental health when compared with cisgender groups of the same age, including suicide risk, use of psychoactive substances, anxiety disorders, depression, eating disorders, and autism spectrum disorders (9–18). Another factor that interferes with the well-being of young transgender people is the high level of violence to which they are exposed. Another factor is that violence against transgender people is often perpetuated by people known to the victim, including family members (19–21). It is known that the transgender population is systematically exposed to social stigma, prejudice, and rejection (minority stress), rendering it vulnerable to the emergence of psychiatric symptoms, and this factor is in isolation is possibly the main factor responsible for the psychological suffering caused in this population (22, 23). However, there is evidence that this fact can be strongly neutralized by simple access to specialized assistance (24, 25).
In Brazil, anyone who meets the criteria for GI [International Classification of Diseases, 11th Revision (ICD-11); WHO] has access to public health services for gender-affirmative treatment. According to a resolution of the Federal Council of Medicine (resolution CFM 2265/2020)—the document that regulates the attendance of gender-affirmative care in the Brazilian Unified Health System (SUS)—young people who self-define as transgender must be attended by a specialized multidisciplinary team and can have access to hormonal treatment when they reach 16 years of age if they desired and if the youth has the consent of the legal caregiver. Treatment with hormonal blockers intended for prepubescent children can be administered when there is a demand, only for research purposes. Even though there is a regulation of health services, there are many social barriers to this population for accessing these health-care services. Specialized health services remain extremely limited, and the wait for access to the health system in Brazil is long: 9 years on average (26). Therefore, it is very important for people to have access to health services and vulnerability prevention. The quality of interventions is associated with how early such service is established, preferably before adolescence (27, 28).
Thus, due to the lack of studies in our country regarding this population profile, this article aims to describe, from sociodemographic, clinical, diagnostic, and comorbid points of view, a sample of youths self-defining as transgender people who sought specialized assistance for gender affirmation in a public hospital in southern Brazil.
This research was approved by the Ethics Committee of the Hospital de Clínicas de Porto Alegre (HCPA) (protocol no. 140275). All of the participants, both young people and their caregivers, were informed of the purposes of this research and then invited to participate. All of the subjects provided written informed consent.
A total of 24 young people participated, aged 8 to 16 years, who met the diagnostic criteria for GD [Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)]/GI (ICD-11). All of the families of the young people were invited to participate to complement the history data and to participate in therapeutic planning. Twenty-one mothers (aged between 27 and 61 years) and 13 fathers (aged between 30 and 64 years) accepted the invitation. The exclusion criterion was a lack of a GI diagnosis (ICD-11).
The research protocol consisted of the systematization of the data collected in the global psychological evaluation performed during the initial health-care encounter of the young people and family members who sought help at the Gender Identity Program (PROTIG) at the HCPA. For the present study, the following techniques were considered: psychological clinical interview, psychiatric evaluations, structured interviews, cognitive testing, and psychopathology evaluation instruments—applied to each individual and to the caregiver present throughout the entire care.
In this evaluation, made with young people and with caregivers, three interviews were conducted by a childhood and adolescence psychologist aiming at (1) the establishment of a therapeutic alliance; (2) evaluation of emotional development; (3) evaluation of family dynamics; (4) evaluation of the social support network; (5) evaluation of knowledge about legal rights; and (6) evaluation of the level of self-recognition and expression of the youth's gender identity.
This evaluation, conducted by a psychiatrist specializing in childhood and adolescence, is conducted on young people and caregivers. The number of meetings varied according to individual needs and depended on the presence of psychiatric morbidities, and they were involved in monitoring and evaluating the therapeutic response to drugs.
For this interview, a questionnaire used in the Brazilian field study for the ICD-11 (WHO) was applied, which overlapped the diagnostic criteria for GI (ICD-11-2018) with the diagnostic criteria of DG (DSM-5-2013) (26, 29, 30). The survey instrument, based on participants' reports, evaluated a particular period of time, that is, when they first became consciously aware that they might be trans (incongruence between one's experienced gender and assigned sex). For this research, three clusters from the questionnaire were used: (1) diagnostic criteria; (2) degree of psychological distress; and (3) loss of social functioning (here represented by school dropouts due to gender incongruity). The intensity of emotion, as well as the intensity of discomfort with sexual characteristics, was assessed using a Likert scale ranging from 1 (very little) to 5 (very much). This interview was administered by a trained psychologist and was aimed at young people, but the questions can also be adapted to be answered by caregivers. If it made the participants feel more comfortable, the caregivers could participate.
In this evaluation, made with young people and performed by a psychologist trained in its application, the validated version for the Brazilian population of the Wechsler Intelligence Scale for Children (WISC-VI) scale was used, consisting of 15 subtests (10 main and five supplementary) and four indices, namely, the Verbal Comprehension Index, the Perceptual Reasoning Index, the Working Memory Index, and the Processing Speed Index. In total, these scales comprise the Full-Scale IQ (FSIQ) (31).
This semistructured interview is conducted with young people and with caregivers and performed by a psychologist and/or psychiatrist trained in its application. The validated version for the Brazilian population of the Kiddie-Sads scale was used to estimate the presence of psychopathology and diagnostic status over the lifetime of the youths according to the DSM-IV criteria (32).
Descriptive and statistical analyses were performed using SPSS software (version 21.0). For the present study, 41 variables were selected from the database. Categorical variables (sex designated at birth, gender identity, school evasion, commencement of social gender transitions, use of hormones, etc.) were expressed by frequencies and percentages. The ordinal variables (age, years of study, age of parents, age of perceived gender incongruity by participant, age of perceived gender incongruity by participants' parents, age of social transition, FSIQ, etc.) were expressed through means and standard deviation.
The sample consisted of 24 young people (average age = 13.88 ± 2.455 years) and 34 of their caregivers, of whom 21 were mothers (average age = 43 ± 9 years) and 13 were fathers (average age = 45.8 ± 9.5 years). Most of the caregivers (74.3%) were employed at the time of the evaluation, and 35.3% had college degrees. Of the youths, half had the sex designated at birth as female and identified with the male gender (50%), and the other half had the sex at birth designated as male and identified with the female gender (50%).
Table 1 shows the sociodemographic data of these young people.
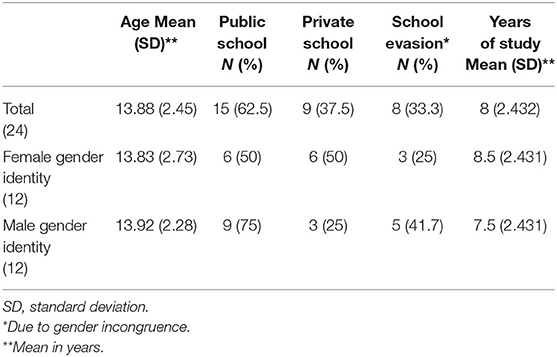
Table 1. Sociodemographic data referring to the studied youth population.
All of the participants had the diagnosis of GI (ICD-11).
Most of the participants (79.2%) had already started social gender transitions when they sought gender-affirmative health care.
Table 2 shows the mean age that the subject realized that his or her gender was incongruous with the sex designated at birth (age of perceived gender incongruity by participant); the mean age at which the parents perceived that their daughter/son exhibited some socially unexpected gender behavior for the assigned sex (age of perceived gender incongruity by participants' parents); and the mean age at which these youths started the social transition of gender roles (age of social transition).
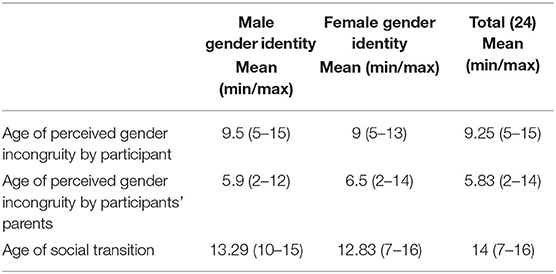
Table 2. Gender perception and social gender transition.
Only two young people (8.3%) used hormones without medical supervision before entering gender-affirmative health care. Regarding discomfort with sexual characteristics, 58.3% (n = 14) reported feeling strong or very strong discomfort with the genitals, and only one (4.2%) reported not feeling any discomfort with the genitals. Only two subjects (8.3%) reported not feeling any discomfort with the breasts; however, 75% reported that their discomfort was strong or very strong. Regarding the tone of the voice, half (50%) reported not feeling discomfort, and seven subjects (29.2%) reported strong or very strong discomfort with the tone of voice.
Table 3 shows the level of discomfort with sexual characteristics (discomfort about his or her sexual anatomy or anticipated secondary sex characteristics) divided by gender identity.
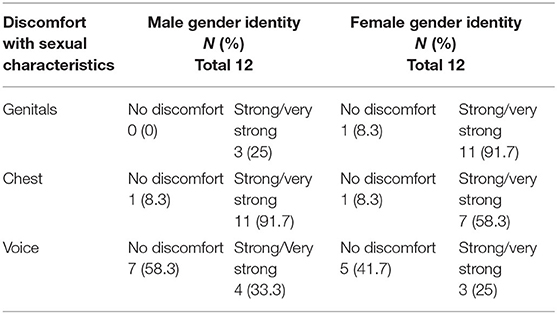
Table 3. Level of discomfort with sexual characteristics.
Slightly more than half of the participants (54.2%) claimed to have felt rejected because of their gender incongruity. All of the subjects (100%) said they felt significant distress (sadness and anxiety) associated with their gender incongruity in an intense fashion and for a period longer than 6 months. Of these cases, 91.7% (n = 22) associated this psychological distress with the conflict between having a biological body incongruent with the gender of identity, and two of them, 8.3%, associated their psychological distress with reactions of social stigma and prejudice. Of those who had school evasion (n = 8) (see Table 1), 37.5% claimed that it was due to the conflict between having a biological body incongruent with the gender identity, and 62.5% claimed that it was due to social reactions regarding their expressed gender.
Table 4 shows the occurrence of psychiatric morbidities present in the sample and the mean of the FSIQ.
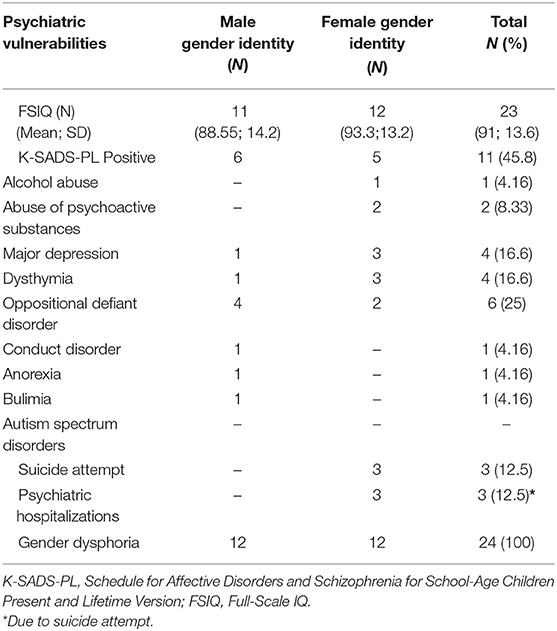
Table 4. Occurrence of psychiatric vulnerabilities and diagnosis status in the present and/or past lifetime and full-scale IQ.
Of the young people, 45.8% were positive for some psychiatric comorbidity throughout their lives, and of these people, almost half (45.4%) had some diagnostic co-occurrence; that is, they were positive for two or more psychiatric diagnoses in addition to DG/GI. Of the youths who tested positive for Schedule for Affective Disorders and Schizophrenia for School-Age Children Present and Lifetime Version (K-SADS-PL), 81% (10) had a qualitative FSIQ less than the average (<89 composite points).
The DSM-5 classifies the presence of psychological distress or social dysfunction due to gender incongruity as a required criterion for the diagnosis of GD. The ICD-11, conversely, does not require the presence of the criterion “psychological distress” for the diagnosis of GI since it understands that transgender people might not present this type of suffering experience. In our study, most of the youths associated this psychological distress with the conflict regarding gender incongruity itself; thus, it came as a consequence of the emotional conflict of realizing the incongruity of their biological bodies with their gender identity, and a minority associated psychological distress with the social stigma and prejudice resulting from their expressed gender variance. However, stigma and prejudice were perceived as the main reasons for school evasion. Many schools are still aligned with rigid structures of binary gender roles, such as wearing uniforms and toilets divided by sex, making transgender youth inclusion difficult. This result provides evidence that the stigma and prejudice suffered by these people directly affect their social functionality. Other studies have emphasized the negative social and emotional impacts of stigma and prejudice on the lives of transgender people (19, 20) and have reinforced the need for interventions in different social structures. Thus, positive public policies can guarantee that transgender people have their rights preserved and that their gender expression is not a limiting factor or seen as harmful in their social spheres.
Discomfort with existing or anticipated sexual characteristics is one of the main factors why young people seek gender-affirming health-care services. Discomfort with the genitals, the chest, and the voice are still the most reported; however, the results showed a personal and gender identity variation regarding the level of this discomfort (see Table 3). Regarding medical treatment of gender affirmation, a minority (8.3%) started using hormones without adequate health monitoring. In a similar study conducted with a group of adult individuals diagnosed with GD in health care at a Brazilian specialized gender service, at least one affirmative gender intervention without medical monitoring (use of hormones and/or aesthetic procedure) was found in 62.1% of individuals (26). These contrasting findings reinforce the need to offer specialized gender care services to transgender youth to avoid possible iatrogenic procedures. Regarding aspects of gender transition that do not involve medical interventions, most young people arrived at the affirmative care service with the social transition already started. Social transition refers to the process by which someone advances his or her experience in the gender role with which he or she identifies, affirming his or her gender identity, such as using a name or pronoun and/or wearing clothes that align more with gender identity than with sex assigned at birth. Currently, in most cases, this initiative seems to be attributed to a decision by the family nucleus that does not use specialized support to initiate a social gender transition that does not involve medical procedures. The results show that the beginning of the social transition is much later than the age of the subject's perception of their gender and of the age at which parents perceive the gender incongruity of their son or daughter (Table 2). Gender perception variables were raised using a structured interview that directly asks the subject's age of perception. This is combined with the psychological evaluation data in which the young people and their caregivers reported perceiving the expression of a deeply essential gender identity discordant from assigned sex. Researchers have maintained that there is the possibility of recognizing a stable transgender identity from childhood. They show that, in general, the onset age of the first behavioral manifestations occurs during preschool years, younger than five (33–37). It has been increasingly accepted among many gender theorists and practitioners that an individual's gender is evolutionary across the life span. Gender-affirmative care places substantial significance on a child's understanding of their own gender and allows the youth, and their knowledge of their gender, to lead the way to interventions. This includes the phase in which the young people and their families feel safe commencing the social gender transition (34).
In the present study, a high index of impairment in cognitive function was found in people who had a mental health diagnosis in addition to GI/GD. It is known that it is common to find the co-occurrence of intellectual disabilities and psychiatric disorders in children and adolescents (38, 39). Together with gender issues, mental disorders and intellectual disabilities are substantial public health problems. This fact has proved to be another challenge for health teams that provide health prevention strategies, adherence to treatment, and improvement in quality of life in all spheres, both personal and social, requiring individualized interventions. During the transition from childhood to adulthood, addressing the changes in a body that cannot be identified is a highly emotionally demanding task in itself and can certainly be detrimental to psychological, intellectual, and social development in transgender people.
The removal of transgender identities from the mental health category in the ICD-11/WHO is an important milestone in the attempt to not stigmatize gender identities (29). However, our study revealed that almost half of the sample was diagnosed with some psychiatric comorbidity throughout their lives. The above findings are in line with the results of other centers serving transgender youths in different countries and cultures (40, 41). Additionally, these results are close to those found in the population of transgender adult people who sought specialized gender health-care services in Brazil, in which 42.7% of the sample had some psychiatric comorbidity (42). These findings emphasize the need for the presence of a qualified mental health team in gender-affirming clinical care. In contrast, positive findings regarding mental health in recent studies have shown a reduction in psychopathology after simple access to health-care services (24, 25, 43, 44).
However, clinical practice with transgender youth challenges health teams to develop care protocols that focus on singular interventions that cover the different social structures that make up the individual's environment, as well as specific and appropriate interventions for each situation regarding the demand for medical treatment of gender affirmation and social transition. In light of the complexity of serving this population, it is necessary to invest in multidisciplinary teams that develop individualized ways to promote healthy development. Thus, the gender affirmation model, which advocates for a global assessment and personalized guidelines, proved to be adequate for the clinical follow-up of young people who sought specialized gender health-care services, therefore, focusing on the promotion of mental health, general emotional well-being, and recognition of legal and social rights in different spheres of the environment and not only medical procedures and physical interventions of gender affirmation.
The entire conduct of the gender-affirmative clinical process must be undertaken from a scientific/practical perspective (from evaluation to intervention) so that it can support best ethical practices and facilitate the selection and monitoring of therapeutic efficacy. Nevertheless, access to multidisciplinary health services specializing in gender is essential for promoting the general well-being of the population of transgender youth.
The main limitation present in the study is the sample size. The specialized gender services for minors are still recent in Brazil. In addition, there are many social barriers to this population for accessing health-care services. This study analyzes the average of a group and cannot be used to characterize an individual within the group.
The original contributions generated for this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by This research was approved by the Ethics Committee of the Hospital de Clínicas de Porto Alegre/HCPA (protocol no. 140275). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
BS, AB, and ML conceived of the presented idea. BS performed the research protocol. ST helped supervise the project. ÍC, DS, AF, and FG contributed to the interpretation of the results. All authors discussed the results and contributed to the final manuscript.
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance code 001and Fundo de Incentivo à Pesquisa e Eventos (FIPE) do Hospital de Clínicas de Porto Alegre.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Bouman WP, de Vries AL, T'Sjoen G. Gender dysphoria and gender incongruence: an evolving inter-disciplinary field. Int Rev Psychiatry. (2016) 28:1–4. doi: 10.3109/09540261.2016.1125740
2. Aitken M, Steensma TD, Blanchard R, VanderLaan DP, Wood H, Fuentes A, et al. Evidence for an altered sex ratio in clinic-referred adolescents with gender dysphoria. J Sex Med. (2015) 12:756–63. doi: 10.1111/jsm.12817
3. Wiepjes CM, Nota NM, de Blok CJM, Klaver M, de Vries ALC, Wensing-Kruger SA, et al. The Amsterdam cohort of gender dysphoria study (1972–2015): trends in prevalence, treatment, and regrets. J Sex Med. (2018) 15:582–90. doi: 10.1016/j.jsxm.2018.01.016
4. Drescher J. Queer diagnoses: parallels and contrasts in the history of homosexuality, gender variance, and the diagnostic and statistical manual. Arch Sex Behav. (2010) 39:427–60. doi: 10.1007/s10508-009-9531-5
5. Hidalgo MA, Ehrensaft D, Tishelman AC, Clark LF, Garofalo R, Rosenthal SM, et al. The gender affirmative model: what we know and what we aim to learn. Hum Develop. (2013) 56:285–90. doi: 10.1159/000355235
6. Edwards-Leeper L, Leibowitz S, Sangganjanavanich VF. Affirmative practice with transgender and gender nonconforming youth: expanding the model. Psychol Sex Orient Gender Diversity. (2016) 3:165–72. doi: 10.1037/sgd0000167
7. Conselho Federal de Medicina. (2020). Resolução n°2265: Dispõe sobre o cuidado específico à pessoa com incongruência de gênero ou transgênero. Available online at: https://www.in.gov.br/web/dou/-/resolucao-n-2.265-de-20-de-setembro-de-2019-237203294 (accessed October 28, 2020).
8. Chen D, Tishelman A, Edwards-Leeper L, Stancin T. Introduction: advancing the practice of pediatric psychology with transgender youth. Am Psychol Assoc. (2019) 7:211–6. doi: 10.1037/cpp0000300
9. Peterson CM, Matthews A, Copps-Smith E, Conard LA. Suicidality, self-harm, and body dissatisfaction in transgender adolescents and emerging adults with gender dysphoria. Suicide Life Threat Behav. (2017) 47:475–82. doi: 10.1111/sltb.12289
10. Bechard M, VanderLaan DP, Wood H, Wasserman L, Zucker KJ. Psychosocial and psychological vulnerability in adolescents with gender dysphoria: a “proof of principle” study. J Sex Marital Ther. (2016) 43:678–88. doi: 10.1080/0092623X.2016.1232325
11. Reisner SL, Greytak EA, Parsons JT, Ybarra ML. Gender minority social stress in adolescence: disparities in adolescente bullying and substance use by gender identity. J Sex Res. (2015) 52:243–56. doi: 10.1080/00224499.2014.886321
12. Witcomb GL, Claes L, Bouman WP, Nixon E, Motmans J, Arcelus J. Experiences and psychological wellbeing outcomes associated with bullying in treatment-seeking transgender and gender-diverse youth. LGBT Health. (2019) 6:216–26. doi: 10.1089/lgbt.2018.0179
13. Rimes KA, Goodship N, Ussher G, Baker D, West E. Non-binary and binary transgender youth: comparison of mental health, self-harm, suicidality, substance use and victimization experiences. Int J Transgend. (2017) 20:1–11. doi: 10.1080/15532739.2017.1370627
14. Fontanari AMV, Pase PF, Churchill S, Soll BMB, Schwarz K, Schneider MA, et al. Dealing with gender-related and general stress: substance use among Brazilian transgender youth. Addict Behav Rep. (2019) 9:100166. doi: 10.1016/j.abrep.2019.100166
15. Thorne N, Witcomb GL, Nieder T, Nixon E, Yip A, Arcelus J. A comparison of mental health symptomatology and levels of social support in young treatment seeking transgender individuals who identify as binary and non-binary. Int J Transgend. (2019) 20:241–50. doi: 10.1080/15532739.2018.1452660
16. Becerra-Culqui TA, Liu Y, Nash R, Cromwell L, Flanders D, Getahun D, et al. Mental health of transgender and gender nonconforming youth compared with their peers. Pediatrics. (2018) 141:5. doi: 10.1542/peds.2017-3845
17. Donaldson AA, Hall A, Neukirch J, Kasper V, Simones S, Gagnon S, et al. Multidisciplinary care considerations for gender nonconforming adolescents with eating disorders: a case series. Int J Eat Disord. (2018) 51:475–9. doi: 10.1002/eat.22868
18. De Vries ALC, Noens ILJ, Cohen-Kettenis PT, van Berckelaer- Onnes IA, Doreleijers TAH. Autism spectrum disorders in gender dysphoric children and adolescents. J Autism Dev Disord. (2010) 40:930–6. doi: 10.1007/s10803-010-0935-9
19. Bockting WO, Miner MH, Swinburne Romine RE, Hamilton A, Coleman E. Stigma, mental health, and resilience in an online sample of the US transgender population. Am J Public Health. (2013) 103:943–51. doi: 10.2105/AJPH.2013.301241
20. Hughto JMW, Reisner SL, Pachankis JE. Transgender stigma and health: a critical review of stigma determinants, mechanisms, and interventions. Soc Sci Med. (2015) 147:222–31. doi: 10.1016/j.socscimed.2015.11.010
21. Stotzer RL. Violence against transgender people: a review of United States data. Aggress Violent Behav. (2009) 14:170–9. doi: 10.1016/j.avb.2009.01.006
22. Meyer IH. Minority stress and mental health in gay men. J Health Soc Behav. (1995) 36:38–56. doi: 10.2307/2137286
23. Rood BA, Reisner SL, Surace FI, Puckett JA, Maroney MR, Pantalone DW. Expecting rejection: Understanding the minority stress experiences of transgender and gender-nonconforming individuals. Transgender Health. (2016) 1:151–64. doi: 10.1089/trgh.2016.0012
24. Dhejne C, Van Vlerken R, Heylens G, Arcelus J. Mental health and gender dysphoria: a review of the literature. Int Rev Psychiatry. (2016) 28:44–57. doi: 10.3109/09540261.2015.1115753
25. Fontanari AMV, Vilanova F, Schneider MA, Chinazzo I, Soll BMB, Schwarz K, et al. Gender affirmation is associated with transgender and gender nonbinary youth mental health improvement. LGBT Health. (2020) 7:237–47. doi: 10.1089/lgbt.2019.0046
26. Soll BM, Robles-García R, Costa AB, Mori D, Mueller A, Fontanari AMV, et al. Gender incongruence: a comparative study using ICD-10 and DSM-5 diagnostic criteria. Braz J Psychiatry. (2018) 40:174–80. doi: 10.1590/1516-4446-2016-2224
27. Drescher J, Cohen-Kettenis PT, Reed GM. Gender incongruence of childhood in the ICD-11: controversies, proposal, and rationale. Lancet Psychiatry. (2016) 3:297–304. doi: 10.1016/S2215-0366(15)00586-6
28. Leibowitz S, de Vries ALC. Gender dysphoria in adolescence. Int Rev Psychiatry. (2016) 28:21–35. doi: 10.3109/09540261.2015.1124844
29. Robles RG, Fresa'n A, Vega-Rami'rez H, Cruz-Islas J, Rodri'guezPe'rez V, Domi'nguez-Marti'nez T, et al. Removing transgender identity from the classification of mental disorders: a Mexican field study for ICD-11. Lancet Psychiatry. (2016) 3:850–9. doi: 10.1016/S2215-0366(16)30165-1
30. Lobato MI, Soll BM, Costa AB, Saadeh A, Gagliotti DA, Fresán A, et al. Psychological distress among transgender people in Brazil: frequency, intensity and social causation–an ICD-11 field study. Braz J Psychiatry. (2019) 41:4. doi: 10.1590/1516-4446-2018-0052
31. Wechsler D. Escala Wechsler de Inteligência para Crianças (WISCIV): manual de instruções para aplicação e avaliação. São Paulo: Casa do Psicólogo Press. (2013).
32. Brasil HH, Bordin IA. Convergent validity of K-SADS-PL by comparison with CBCL in a Portuguese speaking outpatient population. BMC Psychiatry. (2010) 10:83. doi: 10.1186/1471-244X-10-83
33. Gülgöz S, Glazier JJ, Enright EA, Alonso DJ, Durwood LJ, Fast AA, et al. Similarity in transgender and cisgender children's gender development. Proc Natl Acad Sci U S A. (2019) 116:24480–5. doi: 10.1073/pnas.1909367116
34. Ehrensaft D, Giammattei SV, Storck K, Tishelman AC, Keo-Meier C. Prepubertal social gender transitions: what we know; what we can learn: a view from a gender affirmative lens. Int J Transgender. (2018) 19:251–68. doi: 10.1080/15532739.2017.1414649
35. Temple Newhook J, Pyne J, Winters K, Feder S, Holmes C, Tosh J, et al. A critical commentary on follow-up studies and “desistance” theories about transgender and gender-nonconforming children. Int J Transgender. (2018) 19:2212–24. doi: 10.1080/15532739.2018.1456390
36. Nieder TO, Herff M, Cerwenka S, Preuss WF, Cohen-Kettenis PT, De Cuypere G, et al. Age of onset and sexual orientation in transsexual males and females. J Sex Med. (2011) 8:783–91. doi: 10.1111/j.1743-6109.2010.02142.x
37. Ristori J, Cocchetti C, Castellini G, Pierdominici M, Cipriani A, Testi D, et al. Hormonal treatment effect on sexual distress in transgender persons: 2-year follow-up data. J Sex Med. (2020) 17:142–51. doi: 10.1016/j.jsxm.2019.10.008
38. Einfeld SL, Ellis LA, Emerson E. Comorbidity of intellectual disability and mental disorder in children and adolescents: a systematic review. J Intellect Dev Disabil. (2011) 36:137–43. doi: 10.1080/13668250.2011.572548
39. Bass N, Skuse D. Genetic testing in children and adolescents with intellectual disability. Curr Opin Psychiatry. (2018) 31:490–5. doi: 10.1097/YCO.0000000000000456
40. De Vries AL, Steensma TD, Cohen-Kettenis PT, Vander Laan DP, Zucker KJ. Poor peer relations predict parent-and self-reported behavioral and emotional problems of adolescents with gender dysphoria: a cross-national, cross-clinic comparative analysis. Eur Child Adolesc Psychiatry. (2015) 25:579–88. doi: 10.1007/s00787-015-0764-7
41. Olson J, Schrager SM, Belzer M, Simons LK, Clark LF. Baseline physiologic and psychosocial characteristics of transgender youth seeking care for gender dysphoria. J Adolesc Health. (2015) 57:374–80. doi: 10.1016/j.jadohealth.2015.04.027
42. Lobato MI, Koff WJ, Schestatsky SS, Chaves CPDV, Petry A, Crestana T, et al. Clinical characteristics, psychiatric comorbidities, and sociodemographic profile of transsexual patients from an outpatient clinic in Brazil. Int J Transgender. (2007) 10:69–77. doi: 10.1080/15532730802175148
43. Birkett M, Newcomb ME, Mustanski B. Does it get better? A longitudinal analysis of psychological distress and victimization in lesbian, gay, bisexual, transgender, and questioning youth. J Adolesc Health. (2015) 56:280–5. doi: 10.1016/j.jadohealth.2014.10.275
Keywords: gender incongruence, gender dysphoria, transgender youth, healthcare service specialized in gender, gender-affirmative treatment model
Citation: Soll BMB, Fontanari AM, Brandelli Costa A, Chinazzo Í, Silva DC, Guadagnin F, Tramontina S and Lobato MIR (2021) Descriptive Study of Transgender Youth Receiving Health Care in the Gender Identity Program in Southern Brazil. Front. Psychiatry 12:627661. doi: 10.3389/fpsyt.2021.627661
Received: 09 November 2020; Accepted: 22 January 2021;
Published: 04 March 2021.
Edited by:
Hector Wing Hong Tsang, Hong Kong Polytechnic University, Hong KongReviewed by:
Daniel Kwasi Ahorsu, Hong Kong Polytechnic University, Hong KongCopyright © 2021 Soll, Fontanari, Brandelli Costa, Chinazzo, Silva, Guadagnin, Tramontina and Lobato. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bianca Machado Borba Soll, YmlhbmNhc29sbC5wc2lAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.