
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Psychiatry , 28 April 2021
Sec. Public Mental Health
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.611243
This article is part of the Research Topic Digital Phenotyping/Digital Biomarkers to Monitor Psychiatric Disorders View all 15 articles
 Keisuke Izumi1,2,3
Keisuke Izumi1,2,3 Kazumichi Minato4Kiko Shiga4Tatsuki Sugio4Sayaka Hanashiro4Kelley Cortright4
Kazumichi Minato4Kiko Shiga4Tatsuki Sugio4Sayaka Hanashiro4Kelley Cortright4 Shun Kudo4
Shun Kudo4 Takanori Fujita3,5,6
Takanori Fujita3,5,6 Mitsuhiro Sado4,7Takashi Maeno8Toru Takebayashi3,9
Mitsuhiro Sado4,7Takashi Maeno8Toru Takebayashi3,9 Masaru Mimura4
Masaru Mimura4 Taishiro Kishimoto3,4,10*
Taishiro Kishimoto3,4,10*Introduction: Mental disorders are a leading cause of disability worldwide. Depression has a significant impact in the field of occupational health because it is particularly prevalent during working age. On the other hand, there are a growing number of studies on the relationship between “well-being” and employee productivity. To promote healthy and productive workplaces, this study aims to develop a technique to quantify stress and well-being in a way that does not disturb the workplace.
Methods and analysis: This is a single-arm prospective observational study. The target population is adult (>20 years old) workers at companies that often engage in desk work; specifically, a person who sits in front of a computer for at least half their work hours. The following data will be collected: (a) participants' background characteristics; (b) participants' biological data during the 4-week observation period using sensing devices such as a camera built into the computer (pulse wave data extracted from the facial video images), a microphone built into their work computer (voice data), and a wristband-type wearable device (electrodermal activity data, body motion data, and body temperature); (c) stress, well-being, and depression rating scale assessment data. The analysis workflow is as follows: (1) primary analysis, comprised of using software to digitalize participants' vital information; (2) secondary analysis, comprised of examining the relationship between the quantified vital data from (1), stress, well-being, and depression; (3) tertiary analysis, comprised of generating machine learning algorithms to estimate stress, well-being, and degree of depression in relation to each set of vital data as well as multimodal vital data.
Discussion: This study will evaluate digital phenotype regarding stress and well-being of white-collar workers over a 4-week period using persistently obtainable biomarkers such as heart rate, acoustic characteristics, body motion, and electrodermal activity. Eventually, this study will lead to the development of a machine learning algorithm to determine people's optimal levels of stress and well-being.
Ethics and dissemination: Collected data and study results will be disseminated widely through conference presentations, journal publications, and/or mass media. The summarized results of our overall analysis will be supplied to participants.
Registration: UMIN000036814
Mental disorders are a leading cause of disability worldwide and, among mental disorders, major depressive disorder was ranked number 1 in years lived with disability in 2017 (1). The lifetime prevalence of depression in Japan is estimated at 6.2% (2002–2006 estimate), which makes it the country's most common mental illness (2). The disease costs are also enormous and are estimated to exceed 3.09 trillion Japanese Yen (~30 billion U.S. dollars) per year (3). Depression has a significant impact in the field of occupational health because it is particularly prevalent during working age (20–65 years of age). It is estimated that more than half of the social loss due to depression is attributed to loss of labor productivity through absenteeism and presenteeism (2). The Japanese government has implemented measures against long working hours (Standards on limits of overtime work in 1998; the revision of the Industrial Safety and Health Act in 2006) and has introduced the stress check system (enforced as of December 2015), but there has not been a significant impact from those measures. In fact, the number of workers' compensation claims related to mental disorders are increasing each year.
On the other hand, there are a growing number of studies on the relationship between “well-being” and employee productivity. The happiness of employees has been reported to be associated with creativity and productivity (4). As the birthrate continues to decline and the aging population continues to increase in Japan, the working age population is also decreasing, requiring each employee to make the most of his/her abilities. Therefore, preventing negative factors such as depression and promoting well-being are major challenges for health management in the workplace and ensuring a stable economy.
Conventionally, it is known that heart rate variability (HRV) reflects autonomic nerve activity and serves as an index of psychological and physical stress. There are many suggested indicators for stress, including standard deviation of all normal-to-normal R-R intervals (SDNN) and the percentage of successive R-R intervals that differ by >50 ms (pNN50) with time domain variables and low frequency (LF), high frequency (HF), and their ratio (LF/HF) as frequency domain variables (5).
In addition, techniques for estimating emotions and depressive symptoms have been developed based on the analysis of speech including formant frequencies (6). The autonomic nervous system and voice characteristics are closely related to each other because most of the vocal fold movement is stimulated by the recurrent nerve, which branches off from the vagus nerve. Johannes et al. reported that speech fundamental frequency increased with psychological load while there was no significant difference with physical load, suggesting that speech fundamental frequency is a good indicator of psychological stress (7). Nakatsu et al. reported that combination of linear prediction cepstral coefficients and pitch-related characteristics predicted classification of 8 emotions using artificial neural network (8).
Furthermore, electrodermal activity measured by a wearable device can reflect the activity of eccrine sweat glands that are controlled only by sympathetic nerve activity, and is therefore expected to be a stress indicator (9). Previous studies have used the above mentioned approaches to measure subjects' degree of stress; however, this prior research comprises only feasibility studies that have simply verified device performance, and/or studies with only a small number of patients or healthy individuals (10, 11).
Moreover, such approaches are only used to evaluate the so-called “short-term stress” of the study period, and are not necessarily reflective of the effects of medium- to long-term stress. In a workplace environment, it is expected that regardless of whether employees experience temporary stress, there should also be situations where people feel a sense of freedom and accomplishment when a task is completed or a problem overcome. To date, very few studies have revealed the relationship between vital data and mid- to long-term stress and well-being in the workplace (12).
With the development of information and communication technology, similar approaches trying to utilize such biological and/or behavioral data to identify depression are reported recently. For example, in the case of HRV, Dell'Acqua et al. reported that HRV reduction can be the predictor for depression as HRV of individuals with dysphoria and in those with past depression was lower than controls (13). Kemp et al. in their meta-analysis on HRV and antidepressant treatment, reported that depression was associated with reduced HRV, which decreased with increasing depression severity (14).
We have reported that the timing related speech features can reflect the severity of depression. Speech rate, pause time, and response time showed significant associations with the total score of Hamilton Depression Rating Scale (15, 16). We have also reported that body movement captured by infrared sensor can be reflective of depression severity (15, 17).
Not only using single modality but combining multimodal data and with machine learning approach it may be more realistic to screen depression or to predict severity of depression. Utilizing wrist band-type wearable device that record three-axis acceleration, heart rate, body temperature, and ultraviolet light exposure, we have reported that it was possible to identify patients with depression with an accuracy of 0.76, and to predict depression severity with a 0.61 correlation coefficient with Hamilton Depression Rating Scale score (15, 18).
This study, which is funded by the Japan Agency for Medical Research and Development (AMED), is an industry-academia collaborative research project that aims to develop new techniques for evaluating mid- to long-term stress and well-being using technologies that will not obstruct normal work environments. By doing so, we hope to promote healthy workplaces and, in the end, to prevent depression in the prime of life.
The general aim of this study is to develop a technique to quantify stress and well-being in a way that does not disturb the workplace. Our specific objectives are: (1) To evaluate the relationship between the obtained questionnaire-based stress and well-being scores and the employees' vital data, which are collected using: a technique for extracting pulse waves from an image captured by a camera attached to the employee's computer, a technique for extracting emotional components from speech, and a technique for measuring electrodermal activity using a wristband-type wearable device; and (2) to gather information regarding how and when employees are coping to reduce stress or promote enhanced well-being by comparing questionnaire-based stress and well-being scores and the employees' vital data.
This is a single-arm prospective observational study.
Adult (>20 years old) workers at companies that often engage in desk work; specifically, a person who sits in front of a computer for at least half their work hours (3.5 h a day or more).
People who correspond to any of the following groups are excluded from this study:
(1) People currently receiving treatment for mental illness, such as depression;
(2) People who suffer from diseases that may affect the acquisition of biometric information. For example, those who have a disease or disorder that affects pulse wave data measurement (persons who have paralysis or involuntary movements on their faces, or heart disease), those who have a disease or disorder that affects speech data measurement (speech difficulty caused by vocal cord extraction, etc.), or those who have a disease or disorder that affects measurement with wearable devices (persons with paralysis of the extremities or involuntary movement, etc.);
(3) People who have difficulty operating a computer, such as using email or the internet;
(4) People who cannot offer biometric information to researchers due to business/security reasons.
This study was supported by AMED at the stage of developing proof of concept for quantification of stress and well-being using pulse, speech, body motion, and electrodermal data. The study design was made by industrial doctors who served as consultants for some of the companies for which the participants of this study work. These industrial doctors, who are members of our research team, conducted preliminary meetings with the participants, and based on those meetings, they arrived at the question this study hopes to answer: whether stress and well-being can be quantified by pulse, speech, and electrodermal data. The results of this study will be made available to participants through debriefing sessions at each participating company.
Data will be collected according to the observation period schedule in Table 1.
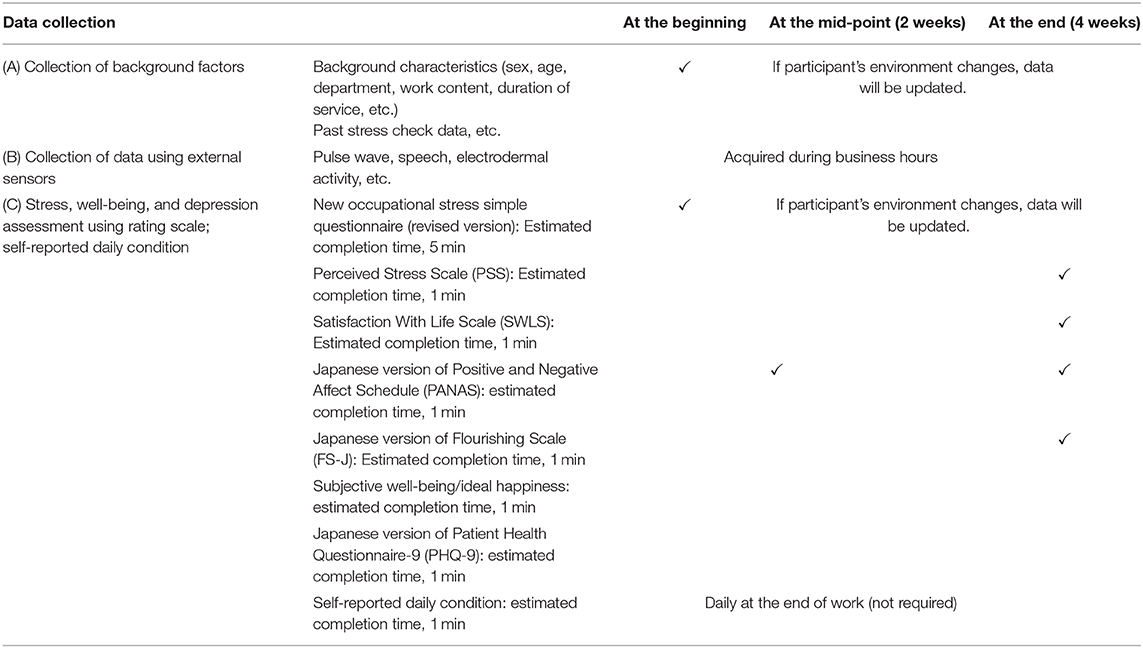
Table 1. Schedule for data collection and evaluations during the study's observation period.
(A) Collection of background factors
After obtaining written consent, the following information will be obtained from each participant:
(1) Sex, age, job department, job content, duration of service, position/title, family composition, work commute, household income, etc.;
(2) Information on past medical checkups and stress check information (with consent of participant);
(3) Any current illnesses and prescriptions.
(B) Collection of biological data with sensing devices
Biological information will be recorded at participants' workplaces during the 4-week observation period using methods B-1 through B-3, as described below:
(B-1) Pulse wave data
Participants install software on their work computers that uses a camera built into or connected to the computer to record video images of the participant; the pulse wave data is extracted from the facial video images. The pulse wave data is automatically sent to cloud storage through the software. Participants are asked to start the software when they arrive for work; the software must also be restarted if the participant's computer is put into sleep mode. This contactless pulse wave sensing system has a strong correlation in the R-R interval values compared to data obtained using ECG (r2 = 0.978, p < 0.00001) (19).
(B-2) Voice data
Participants install software on their work computers that uses a microphone built into or connected to their work computer to record the emotional components (pitch, speed, etc.) of participants' speech data. The emotional component data is automatically sent to cloud storage through the software. Participants are asked to start the software when they arrive for work; the software must also be restarted if the participant's computer is put into sleep mode.
(B-3) Electrodermal activity data, body motion data, and body temperature
Participants are asked to wear the Embrace2 wristband-type wearable device, made by Empatica, Inc., continuously during work hours. The device is equipped with an electrodermameter, accelerometer, gyroscope, and thermometer (20, 21).
(C) Collection of stress, well-being, and depression rating scale assessment data; self-reported daily condition
Researchers will send participants an email with a unique URL link for a unique website where participants can answer questionnaires on stress and well-being online. The evaluation scales and their estimated completion times are as follows (see Table 1 for the evaluation schedule):
• New Occupational Stress Questionnaire (modified version) (22)
• Perceived Stress Scale (PSS) (23)
• Satisfaction With Life Scale (SWLS) (24)
• Japanese version of Positive and Negative Affect Schedule (PANAS) (25)
• Japanese Flourishing Scale (FS-J) (26)
• Subjective Well-being/Ideal Happiness (27, 28)
• Japanese version of Patient Health Questionnaire-9 (PHQ-9) (29)
• Self-reported daily condition: an email with a unique URL will be sent to participants every business day; participants will input their condition (stress level, emotions, etc.) and sleep quality for the day in Likert scales, and include any special notes in 1–2 sentences (e.g., “I had a tough day,” “I was praised by my boss today,” etc.).
The data of background factors (Data A) will be recorded on paper by the researcher and then entered by the researcher into the password-locked computer in the laboratory of the researcher and stored.
Pulse wave and voice data (Data B-1 and B-2) will be quantified and automatically uploaded to the server used by the researcher team through a Secure Sockets Layer (SSL) connection. The research team will download this data via an SSL connection to a research computer in the laboratory and analyzes it.
Data of electrodermal activity, body motion, and body temperature (Data B-3) will be captured by the wearable device and transferred to Empatica's cloud in encrypted form using proprietary software, where the raw data from the device will be analyzed and transformed into skin potential, heart rate, body movement, and temperature data. These sensing data will be eventually downloaded to the computers of the Keio University research team for analysis via an SSL connection.
The web-input data (Data C) such as stress, well-being, depression rating scale assessment data, and self-reported daily condition will be entered directly by participants by accessing an input format on a secure cloud computing service created by the research team. The entered data will be stored on the cloud, and the research team will access the cloud and downloads them to the laboratory's computer through an SSL connection.
All data above will be not accessible by the participants' employers.
The analysis workflow is as follows: (1) primary analysis, comprised of using software to digitalize participants' vital information; (2) secondary analysis, comprised of examining the relationship between the quantified vital data from (1), stress, well-being, and depression; (3) tertiary analysis, comprised of generating machine learning algorithms to estimate stress, well-being, and degree of depression in relation to each set of vital data as well as multimodal vital data. The primary analysis is conducted with technology already established by Panasonic and NEC, who are industrial collaborators in this study. In this research, the results of the primary analysis are used to generate machine learning algorithms for the secondary and tertiary analyses.
Software from Panasonic installed on participants' work computers uses a camera to capture facial images of participants using facial detection. Based on skin color changes from blood flow in the images, the software extracts pulse wave data for the participant. The pulse wave data will then be clarified using filtering and noise removal techniques. SDNN, root mean square of successive differences in R-R intervals (RMSSD), Lorentz plot (Longitudinal axis/Transverse axis value), LH/HF ratio, and Tone-Entropy are calculated from the facial video images (1/30 s unit).
Software from Panasonic installed on participants' work computers uses a microphone to acquire speech data from participants. From this data, voice activity detection (VAD; presence/absence of voice), power (volume of speech), pitch, tension (strength of speech), and speech rate data are extracted (in units of 0.5 s), and an emotion estimate is calculated based on the results.
The Embrace2 wristband-type wearable device from Empatica, Inc., is equipped with an electrodermameter, accelerometer, gyroscope, and thermometer, which are used to record and analyze electrodermal activity, acceleration, angular velocity, and skin temperature.
Each result from the primary analyses of pulse wave, speech, and electrodermal activity data will be compared with the self-assessment results for stress, well-being, and depression. Then, we will determine the relationships between the vital data, stress, well-being, and depression. For example, such an investigation could be done by comparing the stress and well-being score quartiles with the vital data, or comparing them among subjects grouped according to depression symptom severity. Multiple regression analysis will be performed in order to predict stress, well-being, or depression using various kinds of vital data. Moreover, cluster analysis will be performed to find a group of people that have similar digital phenotypes and to seek for the potential relationships with clinical phenotypes.
We will attempt to build a machine learning model to predict depression, stress, or well-being based on single modalities. Various methods, such as support vector machine, decision tree, and deep learning, are used for the machine learning analysis. Machine learning algorithms that estimate stress, well-being, and degree of depression are generated from each of these vital data sets. We will attempt to build a model not only for single modalities, but also one that can utilize all the modalities, namely pulse wave data, voice data, electrodermal activity data, body motion data, and body temperature data, together.
Based on the data obtained from the pilot study (28 cases) conducted prior to this study, we estimated the PSS scores using machine learning analysis of pulse wave and speech data. A gradient boosting decision tree was used for the machine learning algorithm, and hyper parameter was adapted by random search. Accuracy verification is based on 3-fold cross validation. In order to examine the accuracy for each data size, an arbitrary number of data points were extracted at random, and the accuracy for the data size was calculated. The pilot study sample size of 28 subjects was divided and incremented for prediction. The error in the PSS score range of 0–40 corresponds to a score of 2 when an error in the predicted value of PSS of up to around 5% is warranted. When aiming for a root mean square error of 2 or less, we found that 200 cases are required, as shown in Figure 1. Regarding dropouts, we considered that the 4-week-long observation as well as filling out multiple self-rating scales can be burdensome to participants, and the dropout rate can be high. Considering the dropout rate would be 30–35%, we will aim to recruit 300 cases.
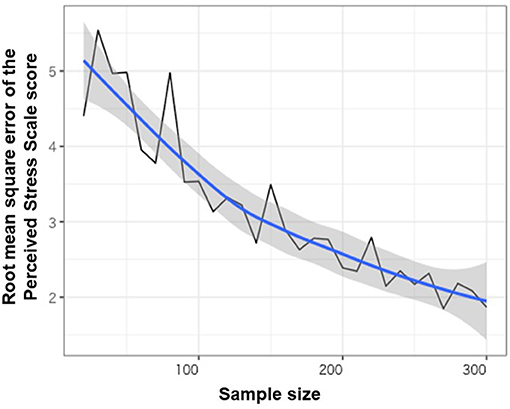
Figure 1. Sample size and root mean square error of the PSS score in the pilot study.
The main aim of this study is to develop a technique to quantify stress and well-being in a way that does not disturb the workplace using vital data. Depression is a major problem in the field of occupational health, with its high incidence, especially among people of working age. The social significance of our project will be great because the occurrence of psychiatric disorders such as depression may be suppressed through self-management and improvement of working conditions in the companies if the quantitative measurement of stress and well-being, which is the ultimate goal of this study, can be achieved.
In this study, biometric information such as pulse wave, voice, and skin potential will be collected without any special intervention while the research collaborators are working. In addition, the research collaborators will be asked to cooperate in data entry through questionnaires, but as described below, the burden will be kept to a certain extent. We will use a web camera, a microphone, a wrist-band wearable device to obtain pulse, voice, and skin potential data, and a web-based questionnaire, which may cause psychological, physical, and time burdens. However, we believe that the burden will be small because we will not intervene and the questionnaire will be administered in a way that will not interfere with normal work and it takes a maximum of about 10 min per session.
The study will also include a rating scale for depression, on which significantly higher scores are presumed to indicate a higher risk of depression. If a recruited person will present any psychiatric disorder during the study, he or she will receive information that would not have been available to him or her if he or she had not participated in the study. The possibility that this may lead to a psychological burden on the individual cannot be denied. Only individuals who agreed that he or she will be informed of accidental findings are recruited. In addition, when the score of the rating scale for depression indicates he or she may have depression, an appropriate action should be taken, such as referring the participant to an appropriate medical institution if he or she wishes to do so. Moreover, the participant will be informed that sensing can be discontinued by shutting down the software or removing the wearable device, and that he or she may do so temporarily if it causes a psychological burden. Prior to the study, consent with the field companies will be obtained using a memorandum of understanding to ensure the privacy of research collaborators (e.g., not to disclose data without the participant's consent).
Challenges of the study are as follows. First, there will be a potential bias that those who are originally interested in the physical and mental health conditions may collaborate in the study. For this reason, participants who are currently being treated for psychiatric disorders, such as depression, will be excluded from the study, and efforts will be made to recruit a wide range of participants. Second, there will be also the issue of adherence. Failure to fill out the questionnaire or not obtaining biometric data may be considered. The researchers will try to reduce the burden on research participants as much as possible to minimize the time and effort required for inputting information and improve adherence. The researchers also consider rewarding each participant based on the response rate to the survey and the amount of time the participant will spend using the devices. Third, as the data collection is done in a natural setting in workplaces, we will lack the control data such as setting participants an experimental task where we can compare the data under strong stress.
Our study has received approval from the institutional review board at Keio University School of Medicine. Approval was granted on April 22, 2019. This study is registered in the University Hospital Medical Information Network (UMIN) (UMIN000036814). Participants' inclusion will be voluntary. Written consent will be obtained from every participant. Participants will be free to withdraw from the study at any time.
KI, KM, and TK conceived the original study concept. KI designed and managed the study, and wrote the initial draft of the manuscript. KM and KS designed and managed the study. TK designed and supervised the study, and assisted in drafting the manuscript. All authors contributed to the design of the study, protocol development, its implementation, critically reviewed the manuscript, approved the final version of the manuscript, agree to be responsible for the accuracy, and integrity of the work.
This work was supported by the Japan Agency for Medical Research and Development (AMED) (Grant No. 18le0110008h0001; Unobtrusive Sensing Technology for Quantifying Stress and Well-being to Promote a Healthy Workplace).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors are grateful to Ms. Momoko Kitazawa, Mr. Shunya Kurokawa, Mr. Michitaka Yoshimura, Mr. Kuo-ching Liang, Mr. Asuka Koshi, Ms. Yuki Ishikawa, Ms. Yoko Usami, Ms. Kumiko Hiza, and Ms. Hiromi Mikami for supporting data collection and management in this study. The authors are grateful to Mr. Yuichiro Suzuki (Panasonic) and Mr. Yoshifumi Onishi (NEC) for technical support in this study. This manuscript has been released as a pre-print at medRxiv (30).
1. James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1789–858. doi: 10.1016/S0140-6736(18)32279-7
2. Kawakami N. A study on epidemiological survey on mental health: comprehensive research report: 2004-2006 Ministry of Health, Labour and Welfare Grant-in-Aid for Health Science Research Project. (2007). Available online at: https://www.khj-h.com/wp/wp-content/uploads/2018/05/soukatuhoukoku19.pdf
3. Ministry of Health. Labour and Welfare Disability Welfare Promotion Project Subsidy: ‘Estimation of Social Cost of Mental Illness’ Business Report. (2011). Available online at: https://www.mhlw.go.jp/bunya/shougaihoken/cyousajigyou/dl/seikabutsu30-2.pdf
4. Lyubomirsky S, King L, Diener E. The benefits of frequent positive affect: does happiness lead to success? Psychol Bull. (2005) 131:803–55. doi: 10.1037/0033-2909.131.6.803
5. Shaffer F, Ginsberg JP. An overview of heart rate variability metrics and norms. Front Public Heal. (2017) 5:1–17. doi: 10.3389/fpubh.2017.00258
6. Koolagudi SG, Rao KS. Emotion recognition from speech: a review. Int J Speech Technol. (2012) 15:99–117. doi: 10.1007/s10772-011-9125-1
7. Johannes B, Wittels P, Enne R, Eisinger G, Castro CA, Thomas JL, et al. Non-linear function model of voice pitch dependency on physical and mental load. Eur J Appl Physiol. (2007) 101:267–76. doi: 10.1007/s00421-007-0496-6
8. Nakatsu R, Nicholson J, Tosa N. Emotion recognition and its application to computer agents with spontaneous interactive capabilities. Knowledge Based Syst. (2000) 13:497–504. doi: 10.1016/S0950-7051(00)00070-8
9. Sano A, Phillips AJ, Yu AZ, McHill AW, Taylor S, Jaques N, et al. Recognizing academic performance, sleep quality, stress level, and mental health using personality traits, wearable sensors and mobile phones. In: 2015 IEEE 12th International Conference on Wearable and Implantable Body Sensor Networks 2015. IEEE. (2015). p. 1–6. doi: 10.1109/BSN.2015.7299420
10. Dogan E, Sander C, Wagner X, Hegerl U, Kohls E. Smartphone-based monitoring of objective and subjective data in affective disorders: where are we and where are we going? Systematic review. J Med Internet Res. (2017) 19:e262. doi: 10.2196/jmir.7006
11. Dang M, Mielke C, Diehl A, Haux R. Accompanying depression with FINE - a smartphone-based approach. Stud Health Technol Inform. (2016) 228:195–9. doi: 10.3233/978-1-61499-678-1-195
12. Alberdi A, Aztiria A, Basarab A. Towards an automatic early stress recognition system for office environments based on multimodal measurements: a review. J Biomed Inform. (2016) 59:49–75. doi: 10.1016/j.jbi.2015.11.007
13. Dell'Acqua C, Dal Bò E, Benvenuti SM, Palomba D. Reduced heart rate variability is associated with vulnerability to depression. J Affect Disord Rep. (2020) 1:100006. doi: 10.1016/j.jadr.2020.100006
14. Kemp AH, Quintana DS, Gray MA, Felmingham KL, Brown K, Gatt JM. Impact of depression and antidepressant treatment on heart rate variability: a review and meta-analysis. Biol Psychiatr. (2010) 67:1067–74. doi: 10.1016/j.biopsych.2009.12.012
15. Kishimoto T, Takamiya A, Liang KC, Funaki K, Fujita T, Kitazawa M, et al. The project for objective measures using computational psychiatry technology. (PROMPT): Rationale, design, and methodology. Contemp Clin Trials Commun. (2020) 19:100649. doi: 10.1016/j.conctc.2020.100649
16. Yamamoto M, Takamiya A, Sawada K, Yoshimura M, Kitazawa M, Liang KC, et al. Using speech recognition technology to investigate the association between timing-related speech features and depression severity. PLoS ONE. (2020) 15:e0238726. doi: 10.1371/journal.pone.0238726
17. Horigome T, Sumali B, Kitazawa M, Yoshimura M, Liang KC, Tazawa Y, et al. Evaluating the severity of depressive symptoms using upper body motion captured by RGB-depth sensors and machine learning in a clinical interview setting: a preliminary study. Compr Psychiatr. (2020) 98:152169. doi: 10.1016/j.comppsych.2020.152169
18. Tazawa Y, Liang KC, Yoshimura M, Kitazawa M, Kaise Y, Takamiya A, et al. Evaluating depression with multimodal wristband-type wearable device: screening and assessing patient severity utilizing machine-learning. Heliyon. (2020) 6:e03274. doi: 10.1016/j.heliyon.2020.e03274
19. Suga K, Hori H, Katsuki A, Ohashi M, Tezuka T, Matsuo M, et al. The contactless vital sensing system precisely reflects R-R interval in electrocardiograms of healthy subjects. PACE. (2017) 40:514–5. doi: 10.1111/pace.13057
20. Nakashima Y, Umematsu T, Tsujikawa M, Onishi Y. An Effectiveness Comparison between the Use of Activity State Data and That of Activity Magnitude Data in Chronic Stress Recognition. In: 2019 8th International Conference on Affective Computing and Intelligent Interaction Workshops and Demos, ACIIW 2019. IEEE (2019). p. 239–43. doi: 10.1109/ACIIW.2019.8925222
21. Empatica Embrace2 device website. Available online at: https://www.empatica.com/en-int/embrace2/
22. Tsutsumi A, Shimazu A, Eguchi H, Inoue A, Kawakami N. A Japanese stress check program screening tool predicts employee long-term sickness absence: a prospective study. J Occup Health. (2018) 60:55–63. doi: 10.1539/joh.17-0161-OA
23. Sumi K. Reliability and validity of the Japanese version of the perceived stress scale. Jpn J Heal Psychol. (2006) 19:44–53. doi: 10.11560/jahp.19.2_44
24. Diener E, Emmons RA, Larsen RJ GS. The satisfaction with life scale. J Pers Assess. (1985) 49:71–5. doi: 10.1207/s15327752jpa4901_13
25. Sato A. Development of the Japanese version of Positive and Negative Affect Schedule. (PANAS) scales. Jpn J Personal. (2001) 9:138–9. doi: 10.2132/jjpjspp.9.2_138
26. Sumi K. Temporal stability of the japanese versions of the flourishing scale and the scale of positive and negative experience. J Psychol Psychother. (2014) 4:1–5. doi: 10.4172/2161-0487.1000140
27. Huppert FA, Marks N, Michaelson J, Vázquez C, Vittersø J. ESS6 - 2012/3 Question Module Design Final Template. (2013). Available online at: https://www.europeansocialsurvey.org/docs/round6/questionnaire/ESS6_final_personal_and_social_well_being_module_template.pdf
28. Takahashi Y. The effect of culture on happiness in Japan: verification by ideal happiness. J Behav Econ Financ. (2018) 11:S9–12. doi: 10.11167/jbef.11.S13
29. Inagaki M, Ohtsuki T, Yonemoto N, Kawashima Y, Saitoh A, Oikawa Y, et al. Validity of the Patient Health Questionnaire (PHQ)-9 and PHQ-2 in general internal medicine primary care at a Japanese rural hospital: a cross-sectional study. Gen Hosp Psychiatr. (2013) 35:592–7. doi: 10.1016/j.genhosppsych.2013.08.001
Keywords: adult psychiatry, mental health, occupational & industrial medicine, wearabe sensors, well-being, stress, protocols, depression
Citation: Izumi K, Minato K, Shiga K, Sugio T, Hanashiro S, Cortright K, Kudo S, Fujita T, Sado M, Maeno T, Takebayashi T, Mimura M and Kishimoto T (2021) Unobtrusive Sensing Technology for Quantifying Stress and Well-Being Using Pulse, Speech, Body Motion, and Electrodermal Data in a Workplace Setting: Study Concept and Design. Front. Psychiatry 12:611243. doi: 10.3389/fpsyt.2021.611243
Received: 28 September 2020; Accepted: 23 March 2021;
Published: 28 April 2021.
Edited by:
Qiang Luo, Fudan University, ChinaReviewed by:
Anke Maatz, University of Zurich, SwitzerlandCopyright © 2021 Izumi, Minato, Shiga, Sugio, Hanashiro, Cortright, Kudo, Fujita, Sado, Maeno, Takebayashi, Mimura and Kishimoto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Taishiro Kishimoto, dGFpc2hpcm8ta0BtdGkuYmlnbG9iZS5uZS5qcA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.