
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry , 17 August 2021
Sec. Psychopharmacology
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.608499
This article is part of the Research Topic Assessing the Consequences of Childhood Trauma on Behavioral Issues and Mental Health Outcomes View all 16 articles
 Eduardo Jorge Muniz Magalhães1
Eduardo Jorge Muniz Magalhães1 Luciana Maria Sarin1
Luciana Maria Sarin1 Lorena Catarina Del Sant1
Lorena Catarina Del Sant1 Ana Cecília Lucchese1
Ana Cecília Lucchese1 Carolina Nakahira1Marco Aurélio Tuena1
Carolina Nakahira1Marco Aurélio Tuena1 Camila Brito Puertas1Victor Augusto Rodovalho Fava1Rodrigo Simonini Delfino1,2
Camila Brito Puertas1Victor Augusto Rodovalho Fava1Rodrigo Simonini Delfino1,2 Juliana Surjan1,2Matheus Souza Steglich1,2
Juliana Surjan1,2Matheus Souza Steglich1,2 Matheus Ghossain Barbosa1Guilherme Abdo1José Alberto Del Porto1,2
Matheus Ghossain Barbosa1Guilherme Abdo1José Alberto Del Porto1,2 Charles B. Nemeroff3
Charles B. Nemeroff3 Hugo Cogo-Moreira1,4
Hugo Cogo-Moreira1,4 Acioly Luiz Tavares Lacerda1,2,5,6†
Acioly Luiz Tavares Lacerda1,2,5,6† Andrea Feijo Mello1,7*†
Andrea Feijo Mello1,7*†Background: A history of child sexual abuse (CSA) is related to higher suicide rates and poor treatment outcomes in depressed adult patients. Twenty years after the first study investigating the effects of ketamine/esketamine on depression and suicide, there is a lack of data on the CSA effects on this emerging treatment. Here, we assess the impact of CSA on adjunctive subcutaneous (SC) esketamine for treatment-resistant depression (TRD).
Methods: A directed acyclic graphic (DAG) was designed to identify clinical confounders between CSA and esketamine predictors of response. The confounders were applied in a statistical model to predict depression symptom trajectory in a sample of 67 TRD outpatients.
Results: The patient sample had a relatively high prevalence rate of CSA (35.82%). Positive family history of first-degree relatives with alcohol use disorder and sex were clinical mediators of the effects of esketamine in a CSA adult population. Overall, the presence of at least one CSA event was unrelated to esketamine symptom reduction.
Conclusions: Unlike responses to conventional antidepressants and psychotherapy, CSA does not appear to predict poor response to esketamine.
The adverse effects of childhood abuse on health are substantial and well-documented. The WHO estimated in 2002 that 150 million girls and 73 million boys under the age of 18 had suffered various forms of sexual violence (1). Females have a two- or threefold higher risk compared with males to be sexually abused during childhood (2), resulting in a worldwide prevalence of 15–19.7% for women and 7.6–8% for men (3). Regrettably, most studies solely include reports from children's protection services, detecting only a small fraction of cases (4). This type of trauma can be considered as “toxic” and causes a prolonged activation of the body's stress response system (5). It impairs and affects regulation, impulse control, sense of self, socialization (6), and the brain changes have enduring consequences throughout life, mediating a negative trajectory to mood disorders in this population (7).
Depression is a disorder long known to be associated with CSA (8); poorer outcomes are related to CSA severity (9). Meta-analytic reviews have found evidence of associations between CSA and adult depression (10, 11). Despite the significant correlations between childhood abuse and adult depression, little is known about its specific effects on treatment (12), although, it is associated with reduced responsiveness to antidepressant pharmacotherapy and psychotherapy (13).
In view of the need for more effective treatments for individuals with TRD and CSA history, we sought to determine whether a subpopulation of patients with CSA and a current TRD episode would benefit from an investigational protocol with multiple subcutaneous (SC) esketamine injections. The subcutaneous route of administration is a reasonable alternative that leads to similar plasma concentrations and more feasible procedure for many clinics (14). A recent study outlined the cardiovascular safety of multiple SC esketamine injections in TRD (15).
To answer our research question, the relationship between exposure and outcome can be clarified using information from previous studies on CSA and predictors of response to ketamine. We can encode these evidences, and the links thereof, in an illustrative way, applying a directed acyclic graph (DAG). It is a useful method to identify and exemplify the concepts of exposure, outcome, causation, and confounding (16), especially when considering the complexities of CSA. DAG graphically sheds light on presumed relationships among variables, allowing bias adjustments in a standardized manner.
Our sample consisted of 70 outpatients (men and women, aged 15 to 66 years) experiencing TRD episode (unipolar and bipolar) referred by psychiatrists to the esketamine clinic in the Department of Psychiatry of the Federal University of São Paulo, Brazil, between April 2017 to December 2018. Eligibility criteria included: (a) TRD defined as the absence of response (<50% symptomatology reduction) in the current episode to at least two medication trials over an adequate period of time and with a minimal dose approved for the treatment; (b) the Montgomery-Åsberg Depression Rating Scale (MADRS) (17) severity score ≥25; and (c) stable physical health assessed by medical history. Exclusionary criteria were as follows: (a) history of hypersensitivity and/or allergy to esketamine; (b) diagnosis of esketamine abuse or dependence; (c) uncontrolled hypertension; or (d) pregnancy or breastfeeding.
Each patient had one baseline assessment in which a certified psychiatrist conducted a structured clinical interview. This survey included socio-demographical questions and inquired about the medical history from the patients and their first-degree relatives, including the presence of alcohol and substances use disorders. A current major depressive episode diagnosis was confirmed applying the Mini-International Neuropsychiatric Interview (MINI)-plus 5.0 (18), and patient's history of childhood sexual trauma was assessed using the Early Trauma Inventory Self Report-Short Form (ETISR-SF) (19).
The ETISR-SF comprises six dichotomous (yes/no) questions about CSA posed in a steadily increasing emotional intensity whereby favoring its assessment (19). For this study, CSA is defined as yes responses to any of these six items. The scoring strategy is the simple method of counting the number of events that had occurred. The version translated and validated on Brazilian–Portuguese was applied. It was used in this study for being a brief (about 15 min) and feasible screening tool for quantitative and Qualitative childhood trauma in clinical practice. The Brazilian–Portuguese version has been shown to be suitable in terms of both validity and internal consistency for assessing traumatic experiences (alpha value for the total scale = 0.83 and alpha value for sexual events = 0.73; test–retest reliability = 0.78–0.90) (20).
The MADRS measured depression symptom severity at baseline and throughout the treatment.
A titrating dose protocol with SC esketamine injection once a week for up to 4 weeks was conducted (Figure 1) (22). This protocol was administered by a certified psychiatrist with ACLS training and a nurse. Each patient had the same weekly schedule. Pre-injection ratings included the MADRS and vital signs (measurement of blood pressure, heart rate, and digital pulse oximetry). In the first session, all patients received 0.5 mg/kg of ketamine (ideal body weight) injected SC in the abdomen. We monitored vital signs at 15-min intervals for 120 min. A clinical assessment was performed before the patient was discharged, and they were accompanied by a close acquaintance.
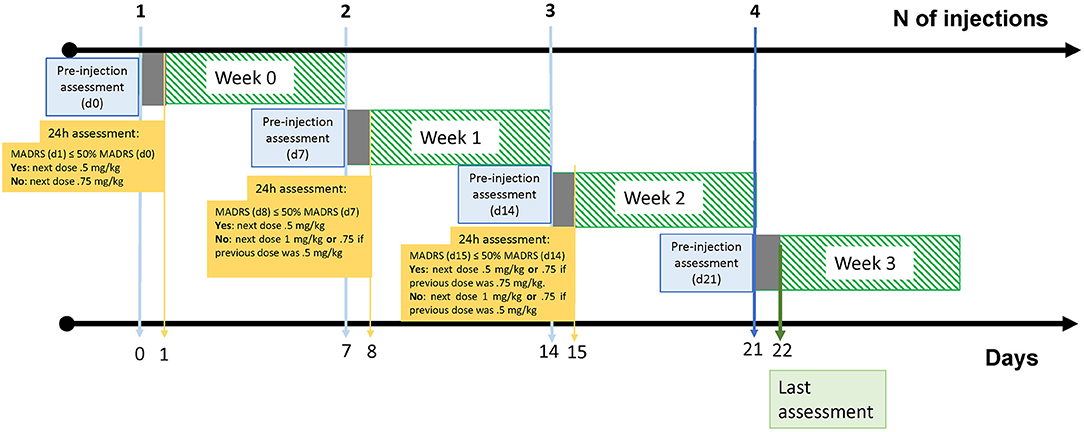
Figure 1. Graphical representation of the 4-week protocol. Days 0, 7, 14 and 21 represents the days of dosing. Days 1, 8 and 15 correspond to 24 h post-injection MADRS assessment for dose titration. At the day 0 in week 0, all patients received a.5 mg/kg dosing which could be augmented to.75 up to 1.0 mg/kg in the following weeks. Day 22 in week 3 represents the end of follow-up. Graphical design according to Schneeweiss, 2019 (21).
Participants remained on their prescribed psychotropic medications, and all subjects provided written informed consent after a complete description of the protocol. This study was approved by the Federal University of São Paulo ethics committee.
Given the observational study design (i.e., non-experimental design), the relationship between exposure and outcome and potential confounders can be clarified using information from previous studies on the health consequences of CSA and predictors of response to depressive symptoms following treatments using ketamine; therefore, we conducted a search in the literature for retrieving those predictors. Then, we constructed a first DAG linking these predictors using the DAGitty graphical interface (23), in which the users promptly check changes in the diagram assessing the modifications of causal and biasing effects (24).
The main advantage in using this template is to select the confounders needed to adjust for (condition on) in the latent growth model to the extent that it would be possible to make valid inferences, answering the research question (25) based on findings that had been replicated in studies with greater samples. Finally, we removed the variables that were not in the path for confounding (i.e., covariates, which are not confounders per se), and created a summarized DAG for a clearer depiction. The medications currently prescribed for the participating patients (SSRI, SNRI, other classes of antidepressants, mood stabilizers, drugs for anxiety and insomnia, antipsychotics, and stimulants) were not employed as confounders.
To estimate the effect of CSA, we fitted a latent growth model (26) using Mplus version 8.3 (27), where a latent intercept and a latent slope were estimated common to all individuals. The intercept is the systematic part of the variation in the outcome variable at baseline (i.e., time point zero) and slope growth factor is the trend, the growth rate, being the systematic part of the decrease (or increasing) in the outcome variable for a time score increase of one unit.
Latent growth model does not require complete data to estimate latent variables because under the assumption of missing at random mechanism, missingness is estimated unbiased via full-information maximum likelihood. Consequently, even when few patients had not responded to all evaluations, they were still considered in the analysis in an intention-to-treat approach given the maximum likelihood estimator.
Model fit was evaluated using the comparative fit index (CFI), root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). CFI values >0.95, RMSEA values of <0.06, and SRMR values >0.06, and a non-significant χ2 statistic were considered a good model fit (28).
Three patients were excluded from the initial sample (n = 70) because of missing 24-h post-injection data. The demographic and clinical characteristics of the 67 patients included are presented in Table 1.
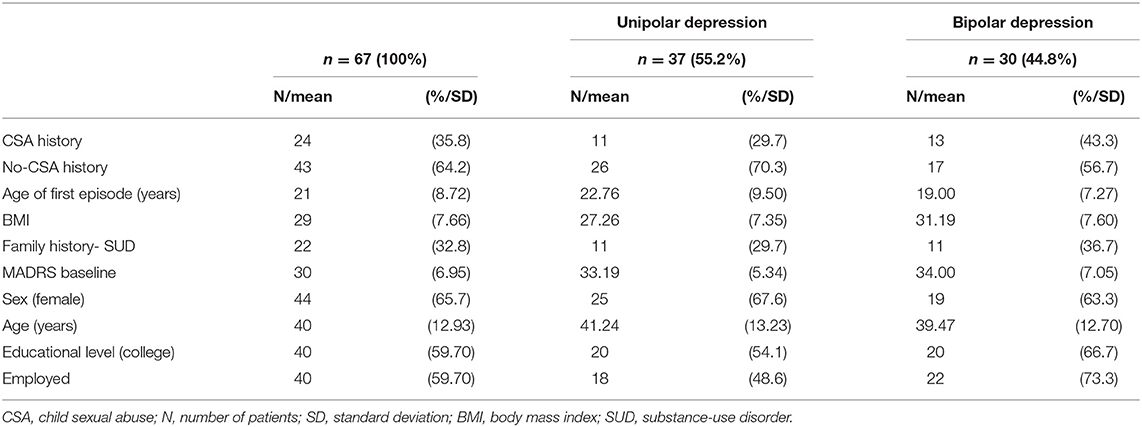
Table 1. Clinical and demographic characteristics of patients (total n = 67) at the enrollment.
The prevalence of CSA among the 67 patients was 35.82%, with a sexual trauma load of 1 or higher (mean 1; SD: 1.45). Among patients reporting a CSA history, the proportions within the six ETISR-SF items were as follows: 31.3% disclosed a history of uncomfortable touching in intimate parts; 17.9% for having someone rubbing their genitals; 10.5% for being forced to touch genital parts; 7.5% for forced kiss; 7.5% for forced genital sex, and 4.5% for being forced to perform oral sex.
The summarized DAG (Figure 2) showed that the presence of first-degree relatives with alcohol use disorder (+FH) and sex is a minimum set for adjustment (i.e., confounders) when analyzing the effects of esketamine in adults with CSA. These confounders were included in the latent growth model to minimize bias.
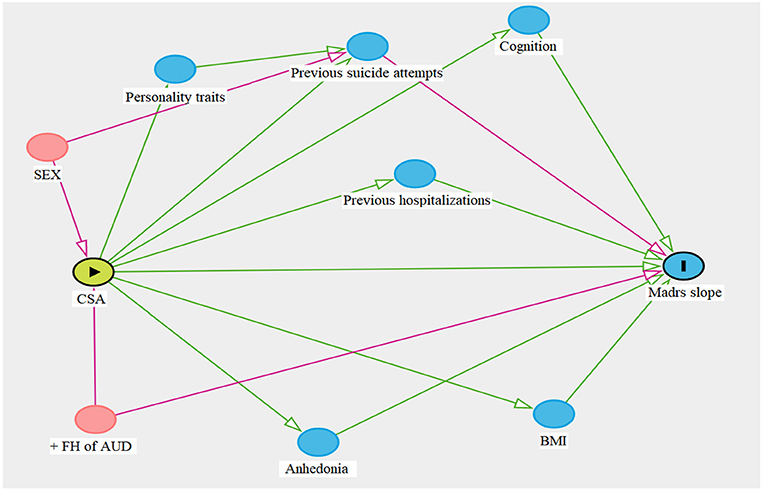
Figure 2. Summarized directed acyclic graphic (DAG). Previous studies were used to rule out the design process, during which the dagitty platform automatically generates red paths and nodes (sex and +FH of AUD), indicating which variables should be controlled in the statistical analysis; whereas green paths and blue nodes do not disrupt the interaction between exposure (▸) and outcome (■). Sex and +FH of AUD should be considered key moderating factors when investigating the effects of CSA on esketamine treatment. Personality traits, previous suicide attempts, hospitalizations, cognition, anhedonia, and BMI are predictors of treatment response, yet they do not disturb the relationship between the variables of interest. CSA, child sexual abuse; + FH AUD, positive family history of a first-degree relative with alcohol use disorder; BMI, body mass index.
For our main hypothesis, we observed that the overall presence of at least one CSA event was not a statistically significant predictor of the trajectory of symptom reduction [β (csa) = 0.386; p = 0.225; 95% CI = −0.137:0.909].
Table 2 displays mean MADRS scores according to the presence of CSA and depression subtype.
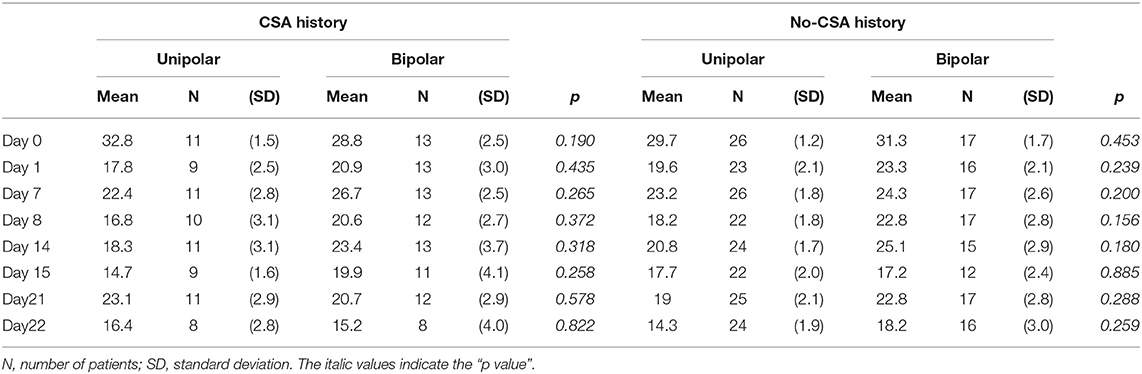
Table 2. Mean Montgomery–Åsberg depression rating scale (MADRS) score according to CSA history and depression subtype.
To our knowledge, this is the first protocol investigating CSA as a clinical predictor of response of multiple subcutaneous esketamine injections in treatment-resistant depression.
In our model, +FH of alcohol use disorder and sex were highlighted as sources of bias between CSA and symptoms trajectory. Being raised by an alcohol-abusing parent increases the likelihood of sexual abuse exposure (29), and esketamine has been reported to be more effective in treatment-resistant depressed patients with a first-degree relative with alcohol use disorder (30). Child sexual abuse and +FH of alcohol use disorder are related to long-lasting neurodevelopmental or genetic/epigenetic variations (30) that predispose to depression in later life.
Female sex has a robust link to childhood sexual trauma and suicidal behaviors (2, 31). CSA is associated with a 2-fold increased risk for suicidal ideation, 3-fold risk for suicide attempts, and an 18-fold higher risk for dying by suicide (32). Conversely, esketamine has demonstrated rapid reductions in suicidal ideation (33). According to the diagrammed DAG, a way for clarifying the path among sex, suicidal ideation, and treatment outcome was controlling for sex as a confounder.
We hypothesized a negative effect of CSA on MADRS scores after repeated esketamine SC injections. However, even after adjustments for confounding factors (+FH of alcohol use disorder and sex), there was a lack of evidence of the effect of CSA and the esketamine response.
When investigating the effect of CSA on treatment response, it is essential to consider that abused patients have an increased probability of having suffered additional untoward experiences that may modify treatment response, disrupting data analysis. An advantageous method to avoid this not-randomizable limitation is by using a schematic representation for recognizing confounders. To this end, we first gathered knowledge from previous investigations, not constrained to our measured variables, thereby identifying common associations between CSA and outcome. Then, these relations were standardized in a DAG. This alternative approach allows a clearer perception of bias while measuring multiple potential confounders without creating other sources of distortions. It focuses on the understanding of prior empirical evidence between exposure and outcome, managing the selection of variables needed to be controlled in the statistical analysis (34). Hence, we could use a clear theoretical rationale to elect appropriate confounders, reducing bias and improving statistical data interpretation (35).
The outcomes from this naturalistic study suggests that, in contrast to the poorer response to conventional antidepressants, we have a lack of evidence that childhood sexual trauma results in a poorer response of depression symptoms to SC esketamine in the sample of patients participating in this study. Thus, the practical relevance of these findings is the need to screen for childhood trauma, detect patients that may not benefit from standard first-line antidepressants, and utilize adjunctive interventions, such as esketamine, especially for those with high suicide risk. Therefore, mental health providers should be conscious of the cumulative effect of CSA, assess child abuse not only as a hallmark of treatment-resistance but rather as a chronic treatment-resistant depression subtype.
Our study has several limitations, including the characteristics inherent to real-world analysis such as broad inclusion criteria, absence of a placebo-treated group, lack of randomization, small sample size, short length of follow-up, concomitant administration of different classes of psychotropic medications, and the usual scoring method of retrospective assessment of reported CSA in which detailed features of severity are not considered. Another limitation was the employment of the same protocol to unipolar and bipolar depression. However, Lucchese et al. (36) reported that there were no statistical associations between diagnosis and response to SC esketamine in this same sample (36). The results should be cautiously interpreted, and replication is essential.
The follow-up period of 4 weeks may have been too brief. As previously reported in an open-label trial of algorithm-guided pharmacotherapy, the rate of symptom improvement increases more slowly in patients with a history of childhood adversity. The difference in remission was more significant by the end of 12 weeks (32% compared with 44% of patients without abuse history) (13). The lack of early improvement at 2 to 4 weeks may be a predictor of later antidepressant non-response/non-remission (37). Therefore, we might theorize that the presence of CSA could slow even the rapid antidepressant response of esketamine, adding a potential need for treatment maintenance and more complexity in the care of this population.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics committee of the Federal University of São Paulo. The patients/participants provided their written informed consent to participate in this study.
EM, LS, LD, ACL, CN, MT, CP, VR, RD, JS, MS, MB, GA, and AM: substantial contributions to the conception of the study and data acquisition. EM, LS, HC-M, and AM: analysis, or interpretation of data for the work. EM: drafting of the manuscript. LS, CBN, HC-M, JD, ALTL, and AM: critical review for important intellectual content. EM, LS, LD, ACL, CN, MT, CP, VR, RD, JS, MS, MB, GA, HC-M, JD, ALTL, and AM: final approval of the version to be published. All authors involved in this manuscript agree to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
EM reports non-financial support from Torrent Pharma and non-financial support from Hypera Pharma, outside of the submitted work. LS reports personal fees from Daiichi Sankyo Brasil, Lundbeck Brasil, Pfizer, and Janssen, and non-financial support from Takeda Brasil, Moksha8 Brasil, Torrent Pharma, outside of the submitted work. CN reports non-financial support from Eurofarma, Cristália, and Sanofi, outside of the submitted work. Dr. Oliveira reports personal fees from Janssen outside of the submitted work. CBN research is supported by the NIMH grant MH-117293 and the National Institute on Alcohol Abuse and Alcoholism grant AA-024933. CBN has served as a consultant for Acadia Pharmaceuticals, Axsome, Compass Pathways, EMA Wellness, Epiodyne, Gerson Lehrman Group, Intra-Cellular Therapies, Janssen Research and Development, Magnolia CNS, Magstim, Navitor Pharmaceuticals, Signant Health, Sophos, Sunovion Pharmaceuticals, Taisho Pharmaceutical, Takeda, TC MSO, and Xhale, he is a stockholder in AbbVie, Antares, BI Gen Holdings, Celgene, Corcept Therapeutics Pharmaceuticals Company, EMA Wellness, OPKO Health, Seattle Genetics, TC MSO, Trends in Pharma Development, and Xhale, he has served on scientific advisory boards for the American Foundation for Suicide Prevention, the Anxiety Disorders Association of America (ADAA), the Brain and Behavior Research Foundation, the Laureate Institute for Brain Research, Magnolia CNS, Signant Health, Skyland Trail, and Xhale, he has served on boards of directors for ADAA, Gratitude America, and Xhale Smart, he has income sources or equity of $10,000 or more from American Psychiatric Association Publishing, CME Outfitters, EMA Wellness, Intra-Cellular Therapies, Magstim, Signant Health, and Xhale, and he has patents on a method and devices for transdermal delivery of lithium (US 6,375,990B1), on a method of assessing antidepressant drug therapy via transport inhibition of monoamine neurotransmitters by ex vivo assay (US 7,148,027B2), and on compounds, compositions, methods of synthesis, and methods of treatment (CRF receptor-binding ligand) (US 8,551,996B2). ALTL has received consulting fees from Janssen Pharmaceutical, Daiichi Sankyo Brasil, Cristalia Produtos Químicos e Farmacêuticos, Pfizer, Mantecorp Indústria Química e Farmacêutica, Libbs Farmacêutica, and Sanofi-Aventis over the last 24 months, and has received research fees from Janssen Pharmaceutical, Eli Lilly, H. Lundbeck A/S, Servier Laboratories, Hoffman-La Roche, and Forum Pharmaceuticals, not related to the submitted manuscript. AM has received non-financial support from Lundbeck not related to the present research.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
This study was supported by the Coordination of Improvement of Higher Education Personnel-Brazil (CAPES)-Financing Code 001. Roseli Cursio, Conceição Tavares, and Renata Oliveira Alves contributed to patient care during the protocol sessions.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.608499/full#supplementary-material
1. Pinheiro P. The World Report on Violence against Children. Geneva: United Nations Secretary-General's Study on Violence against Children (2006).
2. Barth J, Bermetz L, Heim E, Trelle S, Tonia T. The current prevalence of child sexual abuse worldwide: a systematic review and meta-analysis. Int J Public Health. (2013) 58:469–83. doi: 10.1007/s00038-012-0426-1
3. Sanjeevi J, Houlihan D, Bergstrom KA, Langley MM, Judkins J. A review of child sexual abuse: impact, risk, and resilience in the context of culture. J Child Sex Abus. (2018) 27:622–41. doi: 10.1080/10538712.2018.1486934
4. Stoltenborgh M, Bakermans-Kranenburg MJ, Alink LRA, van Ijzendoorn MH. The prevalence of child maltreatment across the globe: review of a series of meta-analyses. Child Abuse Rev. (2015) 24:37–50. doi: 10.1002/car.2353
5. Shonkoff JP, Garner AS. The lifelong effects of early childhood adversity and toxic stress. Pediatrics. (2012) 129:e232–46. doi: 10.1542/peds.2011-2663
6. De Bellis MD, Keshavan MS, Clark DB, Casey BJ, Giedd JN, Boring AM, et al. AE bennett research award. Developmental traumatology. Part II: brain development. Biol Psychiatry. (1999) 45:1271–84. doi: 10.1016/S0006-3223(99)00045-1
7. Molnar BE, Buka SL, Kessler RC. Child sexual abuse and subsequent psychopathology: results from the national comorbidity survey. Am J Public Health. (2001) 91:753–60. doi: 10.2105/AJPH.91.5.753
8. Putnam FW. Ten-year research update review: child sexual abuse. J Am Acad Child Adolesc Psychiatry. (2003) 42:269–78. doi: 10.1097/00004583-200303000-00006
9. Varese F, Smeets F, Drukker M, Lieverse R, Lataster T, Viechtbauer W, et al. Childhood adversities increase the risk of psychosis: a meta-analysis of patient-control, prospective- and cross-sectional cohort studies. Schizophr Bull. (2012) 38:661–71. doi: 10.1093/schbul/sbs050
10. Infurna MR, Reichl C, Parzer P, Schimmenti A, Bifulco A, Kaess M. Associations between depression and specific childhood experiences of abuse and neglect: a meta-analysis. J Affect Disord. (2016) 190:47–55. doi: 10.1016/j.jad.2015.09.006
11. Mandelli L, Petrelli C, Serretti A. The role of specific early trauma in adult depression: a meta-analysis of published literature. Childhood trauma and adult depression. Eur Psychiatry. (2015) 30:665–80. doi: 10.1016/j.eurpsy.2015.04.007
12. Pandina G, Turkoz I, Bossie C. Impact of self-reported juvenile abuse on treatment outcome in patients with major depressive disorder. J Affect Disord. (2013) 151:384–91. doi: 10.1016/j.jad.2013.01.053
13. Klein DN, Arnow BA, Barkin JL, Dowling F, Kocsis JH, Leon AC, et al. Early adversity in chronic depression: clinical correlates and response to pharmacotherapy. Depress Anxiety. (2009) 26:701–10. doi: 10.1002/da.20577
14. Loo CK, Galvez V, O'Keefe E, Mitchell PB, Hadzi-Pavlovic D, Leyden J, et al. Placebo-controlled pilot trial testing dose titration and intravenous, intramuscular and subcutaneous routes for ketamine in depression. Acta Psychiatr Scand. (2016) 134:48–56. doi: 10.1111/acps.12572
15. Del Sant LC, Sarin LM, Magalhães EJ, Lucchese AC, Tuena MA, Nakahira C, et al. Effects of subcutaneous esketamine on blood pressure and heart rate in treatment-resistant depression. J Psychopharmacol. (2020) 34:1155–62. doi: 10.1177/0269881120922955
16. Greenland S, Pearl J, Robins JM. Causal diagrams for epidemiologic research. Epidemiology. (1999) 10:37–48. doi: 10.1097/00001648-199901000-00008
17. Montgomery SA, Smeyatsky N, de Ruiter M, Montgomery DB. Profiles of antidepressant activity with the montgomery-asberg depression rating scale. Acta Psychiatr Scand Suppl. (1985) 320:38–42. doi: 10.1111/j.1600-0447.1985.tb08073.x
18. Sheehan D V, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The mini-international neuropsychiatric interview (MINI): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59(Suppl. 2):22–57.
19. Bremner JD, Bolus R, Mayer EA. Psychometric properties of the early trauma inventory-self report. J Nerv Ment Dis. (2007) 195:211–8. doi: 10.1097/01.nmd.0000243824.84651.6c
20. Osorio FL, Salum GA, Donadon MF, Forni-Dos-Santos L, Loureiro SR, Crippa JAS. Psychometrics properties of early trauma inventory self-report - short form (ETISR-SR) for the brazilian context. PLoS ONE. (2013) 8:e76337. doi: 10.1371/journal.pone.0076337
21. Schneeweiss S, Rassen JA, Brown JS, Rothman KJ, Happe L, Arlett P, et al. Graphical depiction of longitudinal study designs in health care databases. Ann Intern Med. (2019) 170:398–406. doi: 10.7326/M18-3079
22. DAGitty Online Browser. Available online at: http://www.dagitty.net/dags.html (accessed May 17, 2019).
23. Textor J, Hardt J, Knuppel S. DAGitty: a graphical tool for analyzing causal diagrams. Epidemiology. (2011) 22:745. doi: 10.1097/EDE.0b013e318225c2be
24. Suttorp MM, Siegerink B, Jager KJ, Zoccali C, Dekker FW. Graphical presentation of confounding in directed acyclic graphs. Nephrol Dial Transplant. (2015) 30:1418–23. doi: 10.1093/ndt/gfu325
25. Barbosa MG, Sarin LM, Tuena MA, Del Sant LC, Nakahira C, Magalhães EJ, et al. Heterogeneous trajectory of depressive symptoms after repeated subcutaneous esketamine injections. J Affect Disord Rep. (2021) 3:100053. doi: 10.1016/j.jadr.2020.100053
27. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. (1999) 6:1–55. doi: 10.1080/10705519909540118
28. Dube SR, Anda RF, Felitti VJ, Croft JB, Edwards VJ, Giles WH. Growing up with parental alcohol abuse: exposure to childhood abuse, neglect, and household dysfunction. Child Abuse Negl. (2001) 25:1627–40. doi: 10.1016/S0145-2134(01)00293-9
29. Romeo B, Choucha W, Fossati P, Rotge J-Y. Facteurs prédictifs de la réponse antidépressive à la kétamine dans les épisodes dépressifs majeurs résistants: revue de la littérature. Encephale. (2017) 43:354–62. doi: 10.1016/j.encep.2016.06.005
30. Comstock SM, Vaidya JG, Niciu MJ. Neurophysiological correlates and differential drug response in subjects with a family history of an alcohol use disorder. Chronic Stress. (2019) 3:1–13. doi: 10.1177/2470547019865267
31. Turecki G BD. Suicide and suicidal behaviour. Lancet. (2017) 387:1227–39. doi: 10.1016/S0140-6736(15)00234-2
32. Angelakis I, Gillespie EL, Panagioti M. Childhood maltreatment and adult suicidality: a comprehensive systematic review with meta-analysis. Psychol Med. (2019) 49:1057–78. doi: 10.1017/S0033291718003823
33. Canuso CM, Singh JB, Fedgchin M, Alphs L, Lane R, Lim P, et al. Efficacy and safety of intranasal esketamine for the rapid reduction of symptoms of depression and suicidality in patients at imminent risk for suicide: results of a double-blind, randomized, placebo-controlled study. Focus. (2019) 17:55–65. doi: 10.1176/appi.focus.17105
34. Evans D, Chaix B, Lobbedez T, Verger C, Flahault A. Combining directed acyclic graphs and the change-in-estimate procedure as a novel approach to adjustment-variable selection in epidemiology. BMC Med Res Methodol. (2012) 12:156. doi: 10.1186/1471-2288-12-156
35. Sauer B, VanderWeele TJ. Use of directed acyclic graphs. In: Velentgas P, Dreyer NA, Nourjah P, et al., editors. Developing a Protocol for Observational Comparative Effectiveness Research: A User's Guide. Rockville, MD: Agency for Healthcare Research and Quality (2013). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK126189/ (accessed November 15, 2020).
36. Lucchese AC, Sarin LM, Magalhães EJ, Del Sant LC, B Puertas C, Tuena MA, et al. Repeated subcutaneous esketamine for treatment-resistant depression: impact of the degree of treatment resistance and anxiety comorbidity. J Psychopharmacol. (2021) 35:142–9. doi: 10.1177/0269881120978398
37. Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, Bhat V, Blier P, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: Section 3. Pharmacological Treatments. Can J Psychiatry. (2016) 61:540–60. doi: 10.1177/0706743716659417
Keywords: child sex abuse, treatment-resistant depression, esketamine, sex, directed acyclic graph
Citation: Magalhães EJ, Sarin LM, Del Sant LC, Lucchese AC, Nakahira C, Tuena MA, Puertas CB, Rodovalho Fava VA, Delfino RS, Surjan J, Steglich MS, Barbosa MG, Abdo G, Del Porto JA, Nemeroff CB, Cogo-Moreira H, Lacerda ALT and Mello AF (2021) A Clinical Rationale for Assessing the Impact of Childhood Sexual Abuse on Adjunctive Subcutaneous Esketamine for Treatment-Resistant Depression. Front. Psychiatry 12:608499. doi: 10.3389/fpsyt.2021.608499
Received: 20 September 2020; Accepted: 12 July 2021;
Published: 17 August 2021.
Edited by:
Marijn Lijffijt, Baylor College of Medicine, United StatesReviewed by:
Brittany O'Brien, Baylor College of Medicine, United StatesCopyright © 2021 Magalhães, Sarin, Del Sant, Lucchese, Nakahira, Tuena, Puertas, Rodovalho Fava, Delfino, Surjan, Steglich, Barbosa, Abdo, Del Porto, Nemeroff, Cogo-Moreira, Lacerda and Mello. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Feijo Mello, YWFmZWlqb21lbGxvQGljbG91ZC5jb20=
†These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.