
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 01 April 2021
Sec. Schizophrenia
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.601742
This article is part of the Research Topic Understanding the Link Between Structural Differences in the Brain in Patients with Schizophrenia View all 6 articles
 Martin Jáni1,2
Martin Jáni1,2 Zora Kikinis3
Zora Kikinis3 Jan Lošák1
Jan Lošák1 Ofer Pasternak3,4
Ofer Pasternak3,4 Filip Szczepankiewicz4,5
Filip Szczepankiewicz4,5 Carina Heller3,6
Carina Heller3,6 Sophia Swago3Annelise Silva3
Sophia Swago3Annelise Silva3 Sylvain Bouix3,4Marek Kubicki3,4,7
Sylvain Bouix3,4Marek Kubicki3,4,7 Libor Ustohal1
Libor Ustohal1 Petr Kudlička2
Petr Kudlička2 Lubomír Vojtíšek2
Lubomír Vojtíšek2 Carl-Frederik Westin4
Carl-Frederik Westin4 Tomáš Kašpárek1*
Tomáš Kašpárek1*Objectives: We assessed the relationship between emotional awareness (e.g., the ability to identify and differentiate our own feelings and feelings of others) and regional brain volumes in healthy and in schizophrenia groups.
Methods: Magnetic resonance images of 29 subjects with schizophrenia and 33 matched healthy controls were acquired. Brain gray matter was parcellated using FreeSurfer and 28 regions of interest associated with emotional awareness were analyzed. All participants were assessed using the Levels of Emotional Awareness Scale (LEAS) of Self and of Other. LEAS scores were correlated with gray matter volume for each hemisphere on the 14 brain regions of the emotional awareness network.
Results: Individuals with schizophrenia showed decreased emotional awareness on both LEAS Self and LEAS Other compared to healthy controls. There were no statistically significant between-group differences in gray matter volumes of the emotional awareness network. The performance on LEAS Other correlated negatively with right precuneus gray matter volume only in the schizophrenia group.
Conclusion: Our findings suggest a relationship between gray matter volume of the right precuneus and deficits in understanding of emotional states of others in schizophrenia.
Schizophrenia is commonly associated with decreased everyday social functioning and quality of life. Previous research has focused primarily on neurocognition as a predictor of functional outcome. However, a meta-analysis of studies on neurocognition and on social cognition demonstrated that the strongest predictor of functional outcome in schizophrenia is social cognition (1). Though most social cognition research in schizophrenia has focused on theory of mind and the perception of emotions in others (2), emotional awareness of both, self and of others, has been reported to play an important role in functional outcome (3, 4).
Emotional awareness is the ability to consciously experience, describe and identify emotions (5). Deficits in emotional awareness have been observed in patients with schizophrenia and in other mental disorders. The term alexithymia, literally translated as a deficiency in reading emotions, was introduced to describe individuals with deficits in describing and identifying emotions, e.g., with diminished emotional awareness (6, 7). Emotional awareness is most often assessed by tests that are largely based on self-report, such as the Toronto Alexithymia Scale (TAS-20 and TAS-26) (8) or the Bermond-Vorst Alexithymia Questionnaire (BVAQ) (9). A meta-analysis (10) of clinical studies using the TAS-20 in schizophrenia reports that patients show difficulties in identifying and describing feelings, although the results were highly heterogeneous.
Emotional awareness is considered a cognitive ability developed during childhood and adolescence (11, 12) and its deficit can be regarded as a trait feature (13). It has not been established yet whether the deficits in emotional awareness in schizophrenia are associated with abnormalities in cortical gray matter. To our knowledge, only one study has investigated an association between gray matter volume and alexithymia measured by the self-report using the TAS-20 in schizophrenia (14). These investigators reported that decreased volume of left supramarginal gyrus was associated with higher alexithymia in subjects with schizophrenia but not in healthy controls.
In healthy populations, multiple brain regions have been proposed to be involved in emotional awareness. For example, a functional imaging study on healthy volunteers found direct engagement of the temporal pole, posterior and anterior cingulate cortex, medial frontal gyrus, inferior frontal gyrus, precuneus, right anterior insular cortex and ventromedial prefrontal cortex (VMPFC) when evaluating emotional states of self (15). In terms of neuroimaging studies of alexithymia, two meta-analyses in the general population have been conducted (see Table 1). First, Van der Velde et al. (16) focused on functional Magnetic Resonance Imaging (MRI) studies that measured brain activation while viewing emotional stimuli and the correlates of alexithymia were measured by either TAS-20 or BVAQ. They consistently found an association of alexithymia with increased activation of anterior cingulate cortex (ACC) while processing positive and negative emotional valence. In addition, alexithymia was associated with a diminished response of the amygdala, supplementary motor and premotor brain areas, and in the dorsomedial prefrontal cortex during the processing of negative stimuli. Decreased activation was also noted in the right insula and precuneus during processing of positive stimuli. Van der Velde et al. (16) speculated that decreased engagement of amygdala, right insula and precuneus is connected with decreased emotional awareness. A second meta-analysis by Xu and colleagues (17) focused on structural neuroimaging studies of alexithymia that used the self-report tests of TAS-20 or BVAQ. They reported reduced volume in the orbitofrontal and dorsolateral cortices, left insula, amygdala and striatal regions that is associated with increased alexithymia (17) (see Table 1). The above-mentioned studies are important in order to narrow down brain regions that might be involved in emotional awareness.
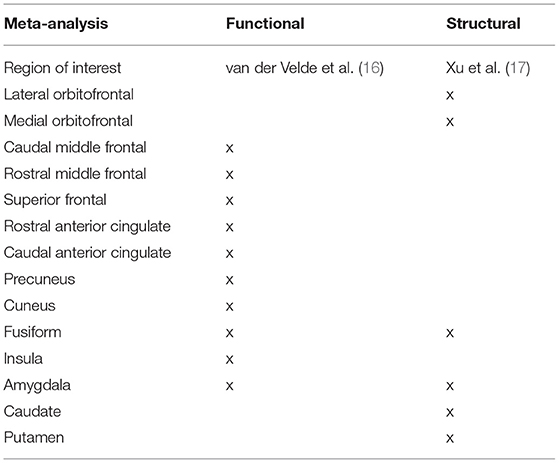
Table 1. Brain regions involved in emotional awareness across studies.
Notably, there are concerns regarding the assessment of emotional awareness using a self-report approach, as such assessments assume some level of insight and self-reflection that is difficult for some patients with schizophrenia. Thus, the use of self-report tests poses a risk of not detecting emotional awareness deficits (3). Therefore, in the current study, we use the Levels of Emotional Awareness Scale (LEAS), a written performance-based test, to control for the self-report problem. As part of the test, the participant is asked to describe their own feelings, and the feelings of another person in 20 different scenarios instead of just being asked in self-report “How good are you in describing feelings?” The score is based on the degree of differentiation in the use of emotion words, where more differentiated emotion words receive higher score, and represent greater awareness of emotional complexity (18). Lane et al. (19) suggests that the LEAS measures the person's ability to make mental representations of emotional states, while TAS-20 merely measures these difficulties in emotional awareness that are so extensive that the person is aware of his/her own deficit. Accordingly, studies using the LEAS have shown decreased emotional awareness in patients with schizophrenia (3, 20), even when the participant reported no self-perceived alexithymia (21).
Emotional awareness is closely related to theory of mind or perspective-taking, the ability to imagine and understand mental states of others (19). The problems with theory of mind constitutes one of the core features of schizophrenia (2). While the relationship of emotional awareness and theory of mind was also illustrated with LEAS overall score (19), there are some indications that the differentiation between emotional awareness for self and other would be beneficial. First, there is a possible conceptual distinction between the two, with emotional awareness for self-referring to the ability of identifying and describing one's own emotional states, while emotional awareness for others involves associated processes such as perspective-taking of others. Second, the benefit to differentiate for self and other is supported by studies where LEAS subscales for self and others were included and, accordingly, indicated distinct attributes of these subscales. Differences between schizophrenia and healthy controls were reported only in LEAS for self but not others (21). However, when only complex scenarios of LEAS were selected, schizophrenia patients had significantly lower score in LEAS for others (but not for self), which also solely correlated with the self-perceived quality of life (3). To summarize, the LEAS test is superior to the traditionally used self-report tests and the differentiation of assessing emotional awareness of self and other is an important feature to assess emotional awareness in people with schizophrenia and in healthy population.
In the present study, we investigated the relationship between brain structure and abnormalities in emotional awareness of self and others. We used the LEAS test to measure emotional awareness of self and others, in healthy controls and in patients with schizophrenia. We used structural MRI of the brain to determine volumes of gray matter regions that were identified as relevant for emotional awareness in previously published studies (see Table 1 for list of regions). To uncover the association between brain regions and emotional awareness, we correlated the scores on LEAS Self and LEAS Other with the volumes of the brain regions. We hypothesized that reduced volumes of gray matter regions would be associated with lower performance on emotional awareness.
The study included 29 (11 female) schizophrenia subjects and 33 (13 female) age, education and gender matched control subjects. The patients were in stable condition, recruited while they were either inpatients (hospitalized for a psychotic episode, during their last week at the hospital) or outpatients in the Department of Psychiatry at University Hospital Brno, Brno, Czech Republic. The diagnosis of schizophrenia was assessed using the Structured Clinical Interview for DSM5–Research version (SCID-RV) criteria (22). Schizophrenia symptoms were evaluated using the Positive and Negative Symptoms Scale (PANSS) (23). Those diagnosed with schizophrenia were taking antipsychotic medication. The healthy controls were recruited using advertising within the local community, Brno, Czech Republic and had no history of psychiatric illness themselves [assessed with Mini-International Neuropsychiatric Interview (24)] or up to second degree relatives. Exclusion criteria for both groups included history of neurological injury, brain disorder, substance abuse, and inability to undergo MRI. All participants signed informed consent. The study was approved by the Institutional Ethical committee of the University Hospital Brno.
The Levels of Emotional Awareness Scale, LEAS (18) consists of 20 written descriptions of situations designed to elicit four emotions: anger, fear, happiness, or sadness. After reading each situation, the participant responded in writing to two questions: “How would you feel?” and “How would the other person feel?” This resulted in two subscales: first, emotional awareness for self (LEAS Self) and second, emotional awareness for others (LEAS Other). Qualitative assessment of responses is described in detail in the manual. In short, the test quantifies the participant's ability to describe specific emotions. The more elaborate descriptions of feelings are scored higher on a scale between 0 to 4, that is a score of 0 for reflection of cognitive states, score of 1 for bodily or physical sensations, score of 2 for undifferentiated feelings like “good” or “bad,” score of 3 for specific elaborate emotions like “sad” or “disappointed” and score of 4 for combination of two or more elaborate and differentiated emotions. In total, higher score indicates higher levels of emotional awareness. The LEAS consists of two versions, A and B, each consisting of 10 situations. Version A of LEAS was used in this study. LEAS has been validated as a reliable tool for measurement of alexithymia (25).
Neurocognition was assessed using the Czech version (26) of the MATRICS Consensus Cognitive Battery [MCCB, (27)]. MCCB composite score was computed without the managing emotions subtest. It has been recommended recently to exclude this emotional subtest from MCCB and report it separately as a domain of social cognition (28).
The structural MRI data were collected on a 3T Siemens Magnetom Prisma (Erlangen, Germany) with 64 channel Head-Neck coil. Subjects lay in the supine position with their heads supported and immobilized using foam padding. A whole brain, high-resolution three-dimensional T1-weighted magnetization prepared rapid gradient echo (MPRAGE) sequence scan was collected (240 sagittal slices, field of view = 224 × 224 mm2, 1 mm3 isotropic voxel, TR = 2.3 s, TE = 2.33 ms, flip angle = 8°).
Volumetric measures of brain regions were obtained from MRI data using FreeSurfer, Version 6 (http://surfer.nmr.mgh.harvard.edu). FreeSurfer software performs a surface-based estimation of regional gray matter volume and parcellates each individual brain in an automated approach into 78 cortical and seven subcortical regions (29). Based on the published meta-analyses of neuroimaging studies of alexithymia (16, 17), we focused on brain regions that were relevant for emotional awareness (Table 1) and selected the corresponding 28 regions of interest (ROI), 14 in each hemisphere, from FreeSurfer parcellations. We normalized the volumes using total brain volume excluding ventricles to control for the size of the head.
First, we assessed the normality of our data. Volumes of nine gray matter regions were not distributed normally (medial orbitofrontal cortex, precuneus, insula, caudate and putamen in the left hemisphere and caudal middle frontal gyrus, precuneus, cuneus and caudate in the right hemisphere). To achieve normal distribution of the data, all volumes were transformed with log-10 transformation. The log transformed data was used in further analyses.
Between group differences (schizophrenia patients and healthy controls) were analyzed using ANCOVA, with age and sex included as covariates of no interest. Then, we evaluated the interaction effect of group and gray matter volume on emotional awareness. We used hierarchical model with first controlling for age and sex, then adding main effects of group and ROI volume and finally the interaction effect. Separate models were used for each ROI and LEAS subscale. Subsequently, the association between volumes of the brain regions and emotional awareness was assessed in each group separately by Spearman's ρ to counter for possible non-linear relationship. For the healthy control group, we conducted partial correlations with age, sex and MCCB composite score as covariates. For the schizophrenia group, in addition to age, sex and MCCB, to counter the clinical confounds, we also included medication, PANSS total score and number of episodes as covariates. Finally, we conducted additional bivariate correlations to assess relationship between LEAS subscales and demographic/clinical variables. As the normalization of the Czech version of MCCB is still in progress, we used standardized z-scores for neurocognition. We used False-discovery rate (FDR) to correct for multiple testing of 28 selected ROIs (14 ROIs on each of the brain hemisphere). Alpha level was set to 0.05 for all tests with FDR correction. Statistic tests were computed using JASP (JASP Team, version 0.9), SPSS (IBM Corp., version 23.0) and R (R Core Team, version 3.6.0).
The groups did not differ in age, gender nor education. Patients showed statistically significant cognitive deficit in all MCCB domains (Table 2).
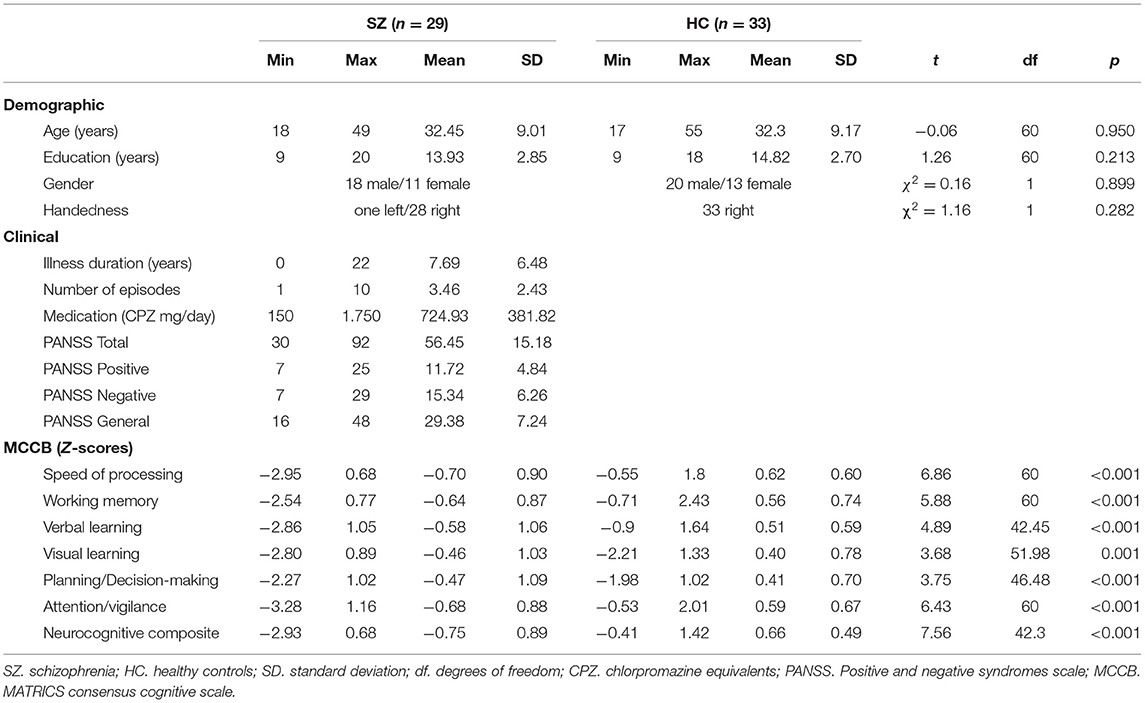
Table 2. Demographical, clinical and neurocognitive characteristics.
Most notably, patients presented with statistically significant decreases in total scores of emotional awareness, on both LEAS subscales, the emotional awareness for self and for others (Table 3).
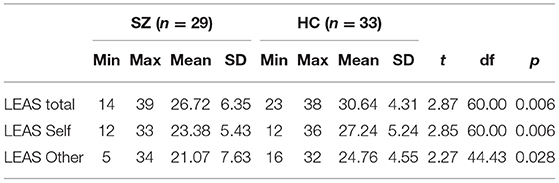
Table 3. Group differences in emotional awareness.
ROI analysis revealed no statistically significant differences after FDR correction (see Supplementary Table 1).
We found significant effect on emotional awareness by interaction of group with right precuneus volume accounting for 38.1% of variation [and 15.4% of unique variation, F(6, 54) = 5.54, p = 0.016, FDR corrected], when controlling for age and sex [accounting for 18% of variation, F(3, 57) = 4.21, p = 0.009] and including main effects of group and gray matter volume of the ROI [4.5% of variation, F(2, 55) = 1.61, p = 0.208]. No other interaction effect was significant. Complete statistics for model of each ROI are given in the Supplementary Table 2.
The scores on LEAS Other were highly significantly and negatively associated with the volume of right precuneus in schizophrenia group (r = −0.68, p < 0.05, FDR corrected, controlled for age, sex, medication, MCCB, PANSS and number of episodes). This relationship was non-significant in the control group. The relationship between LEAS Other and the volume of right precuneus in both groups is plotted in Figure 1. The results of correlations of all brain regions are given in the Supplementary Table 3.
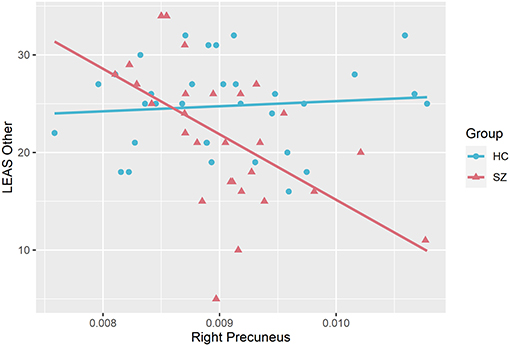
Figure 1. Correlations between emotional awareness for others (LEAS Other) and gray matter volume of right precuneus significant in schizophrenia group (SZ) but not in healthy controls (HC).
We explored whether demographic, clinical or general cognition functioning were related to emotional awareness. No significant correlations between psychopathology (PANSS), antipsychotic medication, illness duration, or neurocognition (MCCB composite) with emotional awareness were found. We found significant correlations between age and LEAS Self in the healthy group (r = −0.48, p = 0.005) and in the combined group (r = −0.36, p = 0.004). We also found significant correlations between verbal learning and LEAS Self in the healthy group (r = 0.56, p = 0.005) and in the combined group (r = 0.57, p < 0.001). No differences were found between gender and in LEAS Self (p = 0.108) or LEAS Other (p = 0.093).
On the behavioral level, we found decreased emotional awareness for both LEAS Self and LEAS Other in the schizophrenia group when compared to the healthy controls, which is in accordance with previously published findings (20). Although some studies suggest selective impairment of emotional awareness of either only self (21), or others (3), our study supports a general impairment of emotional awareness in individuals with schizophrenia. We did not find any association between LEAS and PANSS subscales, illness duration, medication or neurocognition (MCCB composite). To the best of our knowledge, the association between anatomical brain substrates and the LEAS is a novel finding. Increased score on LEAS Other was associated with decreased volume of the right precuneus in patients with schizophrenia, but not in the healthy control group.
Findings of no volumetric differences between schizophrenia and healthy controls is surprising, but not unexpected. Meta-analytic findings report widespread frontotemporal and subcortical reductions of gray matter volume in schizophrenia (30, 31). Our negative findings might be attributed to the relatively small sample and subtle differences that might have remained undetected, while volumetric studies usually require large samples to find between subject differences. In addition, the large variance of age in our sample (including both first episodes and chronic patients) might have obscured the results, as gray matter volume alterations in schizophrenia are characterized by progressive change during the lifespan (32, 33).
Performance on LEAS Other was associated with right precuneus volume. Interestingly, this association was present in the schizophrenia group but not in healthy subjects, suggesting an association specific to schizophrenia between this region and emotional awareness for others. In contrast to our hypothesis of smaller volumes associated with lower performance on emotional awareness, we found that larger volume of right precuneus is associated with LEAS for others. This association was significant even when controlling for age, sex, neurocognition and clinical (psychopathology symptoms, number of episodes and medication) effects.
Precuneus plays major role in higher order self-processes, including shifting between 1st and 3rd person perspective (34) and the attribution of emotion to self and others (35). Previously published research shows functional abnormalities in precuneus in connection to schizophrenia, such as that patients with schizophrenia show altered activity in precuneus when taking the perspective of others (36). In our study while we do not find any changes in volume of the precuneus between the healthy and the schizophrenia group, we report that increased precuneus volume was associated with decreased emotional awareness to others in the schizophrenia group. In the general population, the precuneus is involved in perspective-taking by assigning first-person perspective (35, 37, 38), and the increase of its gray matter volume is associated with greater tendency to recall episodic memories from egocentric perspective (39, 40). Therefore, we speculate that increased precuneus volume might contribute to egocentricity bias, that is a failure to suppress one's own perspective in order to be able to effectively imagine the perspective of others (41). The larger precuneus volume in schizophrenia group might then lead to exuberant focus on egocentric perspective, thus failing to switch the perspective from self to the others when asked about emotional states of others. This might in turn lead to decreased ability to attribute emotions effectively and impair the emotional awareness for others.
Apart from right precuneus, we found no relationship between gray matter volume and emotional awareness in schizophrenia nor in healthy controls. Previous studies indicate association between alexithymia and structural brain changes in general population (17) and also in schizophrenia (14). First, it is possible that our healthy controls did not show enough variance to detect any impairment in emotional awareness. Second, our study is novel in that it used performance-based assessment of emotional awareness, the LEAS, while previous studies relied on self-report questionnaires, limiting the comparability. In addition, given the nature of the emotional awareness, self-report measures can only detect deficit that is so severe that is apparent also to the participant (19), while LEAS might detect subtle deficits, that are not evident in the gray matter alterations.
There are several limitations concerning this study. First, this is an exploratory correlation study, investigating the associations between subject's performance on LEAS and the volumes of specific brain regions. Because we selected 14 specific brain regions that were reported earlier as the areas associated with emotional awareness, we did not explore the entire brain and thus our results are limited to those regions only. In addition, we explored only the volume, the most studied measure in emotional awareness, providing us a framework for our research, a hypothesis and comparability with previous studies. Measures of cortical thickness and cortical areas should be included in future studies. Second, we used FreeSurfer to parcellate the brain into anatomical areas, although volumetric changes in smaller, but functionally relevant subareas might remain undetected. Third, several variables could have influenced the results. Clinical variables such as state of psychosis, antipsychotic medication, or illness duration did not correlate with LEAS, which is in line with previous studies using LEAS in schizophrenia (3, 20, 21). Therefore, the effect of clinical variables is unlikely, suggesting rather stable, trait like nature of the emotional awareness deficit. However, the emotional awareness of self deteriorates with age, which is in accordance with previous research (42). This age effect was observed in the combined group and in the healthy control group, but not in the schizophrenia group, which could possibly be explained by abnormal neurodevelopmental trajectory of the general cognitive impairment in schizophrenia, which has been established even before the prodromal phase and remains stable during remission (43).
We report that patients with schizophrenia exhibit less emotional awareness on both, the LEAS Self and LEAS Other, subtests. We also report that scores on the LEAS Other correlated with one specific region, the right precuneus, in the schizophrenia group, but not in the healthy group. In conclusion, we demonstrated that dysfunction in understanding of emotional states of others is related to a distinct neurobiological substrate, and that volumetric alterations of the right precuneus constitute a key pathology underlying the reduced emotional awareness of others observed in schizophrenia.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by University Etická komise FN Brno (Ethics committee of University Hospital Brno) Jihlavská 20, 625 00 Brno, Czech Republic. The patients/participants provided their written informed consent to participate in this study.
MJ: conceptualization, methodology, formal analysis, investigation, writing - original draft, visualization, and data curation. ZK: conceptualization, methodology, validation, resources, formal analysis, writing - original draft, and data curation. JL: investigation, writing - review and editing, and data curation. OP, FS, CH, SS, AS, and SB: software, validation, writing - review, and editing. MK: resources, writing - review and editing, and funding acquisition. LU: investigation, writing - review, and editing. PK: software, validation, investigation, resources, writing - review, and editing. LV: software, validation, resources, writing - review, and editing. C-FW: software, validation, resources, writing - review and editing, and funding acquisition. TK: conceptualization, writing - review and editing, supervision, project administration, funding acquisition, and resources. All authors contributed to the article and approved the submitted version.
This research was supported by The Ministry of Education, Youth and Sports, Czech Republic (MEYS CR), grant number MUNI/A/1469/2018 (MJ), NIH grants R01 HD090641 and R01 MH112748 (SB), R21MH106793-01A1 (ZK), R01 MH074794 and P41EB015902 (C-FW). We acknowledge the core facility MAFIL of CEITEC supported by the Czech-BioImaging large RI project (LM2018129 funded by MEYS CR) for their support with obtaining scientific data presented in this paper.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.601742/full#supplementary-material
1. Fett A-KJ, Viechtbauer W, Dominguez M-G, Penn DL, van Os J, Krabbendam L. The relationship between neurocognition and social cognition with functional outcomes in schizophrenia: a meta-analysis. Neurosci Biobehav Rev. (2011) 35:573–88. doi: 10.1016/j.neubiorev.2010.07.001
2. Green MF, Horan WP, Lee J. Social cognition in schizophrenia. Nat Rev Neurosci. (2015) 16:620–31. doi: 10.1038/nrn4005
3. Baslet G, Termini L, Herbener E. Deficits in emotional awareness in schizophrenia and their relationship with other measures of functioning. J Nerv Ment Dis. (2009) 197:655–60. doi: 10.1097/NMD.0b013e3181b3b20f
4. Kimhy D, Vakhrusheva J, Jobson-Ahmed L, Tarrier N, Malaspina D, Gross JJ. Emotion awareness and regulation in individuals with schizophrenia: implications for social functioning. Psychiatry Res. (2012) 200:193–201. doi: 10.1016/j.psychres.2012.05.029
5. Larsen JK, Brand N, Bermond B, Hijman R. Cognitive and emotional characteristics of Alexithymia: a review of neurobiological studies. J Psychosom Res. (2003) 54:533–41. doi: 10.1016/S0022-3999(02)00466-X
6. Sifneos PE. Alexithymia: past and present. Am J Psychiatry. (1996) 153:137–42. doi: 10.1176/ajp.153.7.137
7. Goerlich KS. The multifaceted nature of alexithymia – a neuroscientific perspective. Front Psychol. (2018) 9:1614. doi: 10.3389/fpsyg.2018.01614
8. Zech E, Luminet O, Rimé B, Wagner H. Alexithymia and its measurement: confirmatory factor analyses of the 20-item Toronto Alexithymia Scale and the Bermond-Vorst Alexithymia Questionnaire. Eur J Pers. (1999) 13:511–32. doi: 10.1002/(SICI)1099-0984(199911/12)13:6<511::AID-PER347>3.0.CO;2-0
9. Vorst HC, Bermond B. Validity and reliability of the Bermond–Vorst Alexithymia Questionnaire. Pers Individ Dif. (2001) 30:413–34. doi: 10.1016/S0191-8869(00)00033-7
10. O'Driscoll C, Laing J, Mason O. Cognitive emotion regulation strategies, alexithymia and dissociation in schizophrenia, a review and meta-analysis. Clin Psychol Rev. (2014) 34:482–95. doi: 10.1016/j.cpr.2014.07.002
11. Smith R, Quinlan D, Schwartz GE, Sanova A, Alkozei A, Lane RD. Developmental contributions to emotional awareness. J Pers Assess. (2019) 101:150–8. doi: 10.1080/00223891.2017.1411917
12. Mancini G, Agnoli S, Trombini E, Baldaro B, Surcinelli P. Predictors of emotional awareness during childhood. Health (Irvine Calif). (2013) 05:375–80. doi: 10.4236/health.2013.53050
13. Ciarrochi J, Caputi P, Mayer JD. The distinctiveness and utility of a measure of trait emotional awareness. Pers Individ Dif. (2003) 34:1477–90. doi: 10.1016/S0191-8869(02)00129-0
14. Kubota M, Miyata J, Hirao K, Fujiwara H, Kawada R, Fujimoto S, et al. Alexithymia and regional gray matter alterations in schizophrenia. Neurosci Res. (2011) 70:206–13. doi: 10.1016/j.neures.2011.01.019
15. Terasawa Y, Fukushima H, Umeda S. How does interoceptive awareness interact with the subjective experience of emotion? An fMRI study. Hum Brain Mapp. (2013) 34:598–612. doi: 10.1002/hbm.21458
16. van der Velde J, Servaas MN, Goerlich KS, Bruggeman R, Horton P, Costafreda SG, et al. Neural correlates of alexithymia: a meta-analysis of emotion processing studies. Neurosci Biobehav Rev. (2013) 37:1774–85. doi: 10.1016/j.neubiorev.2013.07.008
17. Xu P, Opmeer EM, van Tol MJ, Goerlich KS, Aleman A. Structure of the alexithymic brain: a parametric coordinate-based meta-analysis. Neurosci Biobehav Rev. (2018) 87:50–5. doi: 10.1016/j.neubiorev.2018.01.004
18. Lane RD, Quinlan DM, Schwartz GE, Walker PA, Zeitlin SB. The levels of emotional awareness scale: a cognitive-developmental measure of emotion. J Pers Assess. (1990) 55:124–34. doi: 10.1207/s15327752jpa5501&2_12
19. Lane RD, Hsu CH, Locke DEC, Ritenbaugh C, Stonnington CM. Role of theory of mind in emotional awareness and alexithymia: Implications for conceptualization and measurement. Conscious Cogn. (2015) 33:398–405. doi: 10.1016/j.concog.2015.02.004
20. Harrison BJ, Yücel M, Pujol J, Pantelis C. Task-induced deactivation of midline cortical regions in schizophrenia assessed with fMRI. Schizophr Res. (2007) 91:82–6. doi: 10.1016/j.schres.2006.12.027
21. Henry JD, Bailey PE, von Hippel C, Rendell PG, Lane A. Alexithymia in schizophrenia. J Clin Exp Neuropsychol. (2010) 32:890–7. doi: 10.1080/13803391003596462
22. First MB. Structured Clinical Interview for the DSM (SCID). In: The Encyclopedia of Clinical Psychology. Hoboken, NJ, USA: John Wiley & Sons, Inc. (2015). p. 1–6. doi: 10.1002/9781118625392.wbecp351
23. Kay SR, Fiszbein A, Opler LA. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
24. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59:22–33.
25. Sloan DM, Kring AM. Measuring changes in emotion during psychotherapy: conceptual and methodological issues. Clin Psychol Sci Pract. (2007) 14:307–22. doi: 10.1111/j.1468-2850.2007.00092.x
26. Bezdicek O, Michalec J, Kališová L, Kufa T, Děchtěrenko F, Chlebovcová M, et al. Profile of cognitive deficits in schizophrenia and factor structure of the Czech MATRICS Consensus Cognitive Battery. Schizophr Res. (2020) 218:85–92. doi: 10.1016/j.schres.2020.02.004
27. Green MF, Penn DL, Bentall R, Carpenter WT, Gaebel W, Gur RC, et al. Social cognition in schizophrenia: an NIMH workshop on definitions, assessment, and research opportunities. Schizophr Bull. (2008) 34:1211–20. doi: 10.1093/schbul/sbm145
28. Green MF, Harris JG, Nuechterlein KH. The MATRICS consensus cognitive battery: what we know 6 years later. Am J Psychiatry. (2014) 171:1151–4. doi: 10.1176/appi.ajp.2014.14070936
29. Desikan RS, Ségonne F, Fischl B, Quinn BT, Dickerson BC, Blacker D, et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage. (2006) 31:968–80. doi: 10.1016/j.neuroimage.2006.01.021
30. Bora E, Fornito A, Radua J, Walterfang M, Seal M, Wood SJ, et al. Neuroanatomical abnormalities in schizophrenia: a multimodal voxelwise meta-analysis and meta-regression analysis. Schizophr Res. (2011) 127:46–57. doi: 10.1016/j.schres.2010.12.020
31. Haijma SV, Van Haren N, Cahn W, Koolschijn PCMPP, Hulshoff Pol HE, Kahn RS. Brain volumes in schizophrenia: a meta-analysis in over 18 000 subjects. Schizophr Bull. (2013) 39:1129–38. doi: 10.1093/schbul/sbs118
32. Vita A, De Peri L, Deste G, Sacchetti E. Progressive loss of cortical gray matter in schizophrenia: a meta-analysis and meta-regression of longitudinal MRI studies. Transl Psychiatry. (2012) 2:e190. doi: 10.1038/tp.2012.116
33. Olabi B, Ellison-Wright I, McIntosh AM, Wood SJ, Bullmore E, Lawrie SM. Are there progressive brain changes in schizophrenia? A meta-analysis of structural magnetic resonance imaging studies. Biol Psychiatry. (2011) 70:88–96. doi: 10.1016/j.biopsych.2011.01.032
34. Cavanna AE, Trimble MR. The precuneus: a review of its functional anatomy and behavioural correlates. Brain. (2006) 129:564–83. doi: 10.1093/brain/awl004
35. Ochsner KN, Knierim K, Ludlow DH, Hanelin J, Ramachandran T, Glover G, et al. Reflecting upon feelings: an fmri study of neural systems supporting the attribution of emotion to self and other. J Cogn Neurosci. (2004) 16:1746–72. doi: 10.1162/0898929042947829
36. Jáni M, Kašpárek T. Emotion recognition and theory of mind in schizophrenia: a meta-analysis of neuroimaging studies. World J Biol Psychiatry. (2017) 113:1–11. doi: 10.1080/15622975.2017.1324176
37. Vogeley K, Fink GR. Neural correlates of the first-person-perspective. Trends Cogn Sci. (2003) 7:38–42. doi: 10.1016/S1364-6613(02)00003-7
38. Vogeley K, May M, Ritzl A, Falkai P, Zilles K, Fink GR. Neural correlates of first-person perspective as one constituent of human self-consciousness. J Cogn Neurosci. (2004) 16:817–27. doi: 10.1162/089892904970799
39. Freton M, Lemogne C, Bergouignan L, Delaveau P, Lehéricy S, Fossati P. The eye of the self: precuneus volume and visual perspective during autobiographical memory retrieval. Brain Struct Funct. (2014) 219:959–68. doi: 10.1007/s00429-013-0546-2
40. Hebscher M, Levine B, Gilboa A. The precuneus and hippocampus contribute to individual differences in the unfolding of spatial representations during episodic autobiographical memory. Neuropsychologia. (2018) 110:123–33. doi: 10.1016/j.neuropsychologia.2017.03.029
41. Pronin E. How we see ourselves and how we see others. Science. (2008) 320:1177–80. doi: 10.1126/science.1154199
42. Mattila AK, Salminen JK, Nummi T, Joukamaa M. Age is strongly associated with alexithymia in the general population. J Psychosom Res. (2006) 61:629–35. doi: 10.1016/j.jpsychores.2006.04.013
Keywords: MRI, schizophrenia, psychopathology, emotional awareness, alexithymia
Citation: Jáni M, Kikinis Z, Lošák J, Pasternak O, Szczepankiewicz F, Heller C, Swago S, Silva A, Bouix S, Kubicki M, Ustohal L, Kudlička P, Vojtíšek L, Westin C-F and Kašpárek T (2021) Emotional Awareness in Schizophrenia Is Associated With Gray Matter Volume of Right Precuneus. Front. Psychiatry 12:601742. doi: 10.3389/fpsyt.2021.601742
Received: 01 September 2020; Accepted: 09 March 2021;
Published: 01 April 2021.
Edited by:
Francesco Papaleo, Italian Institute of Technology (IIT), ItalyReviewed by:
Massimo Tusconi, University of Cagliari, ItalyCopyright © 2021 Jáni, Kikinis, Lošák, Pasternak, Szczepankiewicz, Heller, Swago, Silva, Bouix, Kubicki, Ustohal, Kudlička, Vojtíšek, Westin and Kašpárek. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tomáš Kašpárek, dG9tYXMua2FzcGFyZWtAY2VudHJ1bS5jeg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.