 Barbara Hinterbuchinger
Barbara Hinterbuchinger Nilufar Mossaheb
Nilufar Mossaheb
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Psychiatry, 29 March 2021
Sec. Schizophrenia
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.582392
Assuming a continuum between psychotic experiences and psychotic symptoms aligned between healthy individuals and patients with non-psychotic and psychotic disorders, recent research has focused on subclinical psychotic experiences. The wide variety of definitions, assessment tools, and concepts of psychotic-like experiences (PLEs) might contribute to the mixed findings concerning prevalence and persistence rates and clinical impact. In this narrative review, we address the panoply of terminology, definitions, and assessment tools of PLEs and associated concerns with this multitude. Moreover, the ambiguous results of previous studies regarding the clinical relevance of PLEs are described. In conclusion, we address clinical implications and highly suggest conceptual clarity and consensus concerning the terminology and definition of PLEs. The development of an agreed upon use of a “gold standard” assessment tool seems essential for more comparable findings in future research.
In the last decades, contrary to the categorical approach of the “Kraepelinian dichotomy” (1), research has hypothesized a dimensional approach toward psychosis assuming a continuum of psychotic experiences and symptoms aligned between clinical and non-clinical populations (2). The assumption of a temporal and phenomenological psychosis continuum resulted in the examination of psychotic-like experiences (PLEs) in non-help-seeking individuals from the general population (3) to psychotic symptoms in individuals with “non-psychotic” disorders as well as manifest psychotic disorders in individuals with schizophrenia-spectrum disorders (4). Moreover, the concept of “at-risk mental state” (ARMS), and as a result, the implementation of operationalized criteria for the detection of individuals at ultra-high risk of psychosis (UHR) are well-established in clinical and research scope nowadays (5–7). Schizotypy, defined as a combination of personality traits with symptoms and experiences similar but not identical in intensity and phenomenology to schizophrenia spectrum disorders, was suggested as another endophenotype on the spectrum toward psychosis (8, 9).
The concept of psychosis as a transdiagnostic and extended phenotype (10) has resulted in the discussion about the redefinition of the concept and name of schizophrenia (11) and, moreover, in the examination of subclinical psychotic experiences (12–14) and the identification of PLEs as early indicators of psychosis onset (15, 16). However, the variety of definitions and assessment tools of PLEs has been postulated to contribute to the discrepancy of findings regarding prevalence rates (17–20) and persistence rates (21–24). Thus, in this narrative review, we aim to address the challenge concerning the variety of definitions and assessment tools regarding PLEs.
Regarding the definition and terminology of PLEs, comparable confusion was reported as described for different concepts of ARMS/UHR (19, 25, 26): Originally, the term PLE was used for “subschizophrenic” symptoms located on a continuum ranging from normal experiences to “genuine” psychotic symptoms including hallucinations and delusions (27). A recently developed and widely used definition of PLEs describes them as “psychotic symptoms in the absence of illness” (28). Others referred to PLEs as psychotic symptoms in non-clinical populations (3), a “subclinical psychosis phenotype” (29) or referred to doubts about their true psychotic nature due to an uncertainty about the validity of their assessment (30). Van Os et al. differentiated between subclinical psychotic experiences and subclinical psychotic symptoms, whereas the latter were associated with distress and help-seeking behavior but not necessarily with a clinical psychotic disorder (17). In a recent systematic review, three main approaches regarding the definition of PLEs were described: PLEs defined by preset criteria, PLEs defined by assessment tools with a predetermined threshold, and PLEs defined by assessment tools without a predetermined threshold or criteria (19). The authors stated that the majority of papers defined PLEs quantitatively using widely varying assessment tools without specific phenomenological definitions, which might contribute to mixed findings in research (19). Preti et al. (31) differentiated between broadly and narrowly defined PLEs: While the former are defined as incidental and non-distressful unusual subjective experiences with uncertain appraisal, narrowly defined PLEs were suggested to be distressful unusual subjective experiences appraised with certainty. The authors stated that the expression “psychotic-like experiences” might be overinclusive and misleading and suggested the use of the expression “unusual subjective experiences” (USEs) aiming to avoid stigmatization.
Associated phenomena are anomalous self-experiences (ASEs) defined as disturbances in the subjective experiences of the self (32, 33) and described as first symptoms to appear in the prodrome predicting developing psychosis (34). Phenomenologically, these disturbances of self-affection result in a lack of own identity, distance between self and experience, and an alienation from the shared experience within a social context (35, 36). The similar concept of basic symptoms, often described as integral part of the anomalous self-experiences (37, 38), defines symptoms that are subtle, subjectively, and subclinically experienced disturbances in drive, affect, thinking, speech, perception, motor action, central vegetative functions, and stress tolerance also regarded as earliest symptoms within the development of psychosis (39, 40).
Overall, until now, there is no general consensus concerning the definition and conceptualizations of PLEs or associated phenomena, which may result or at least contribute to inconsistent findings and problems concerning the interpretation of results.
In this section, we aim to address various concerns associated with different aspects of PLE assessment tools. First of all, one major concern relates to the assessment of PLEs in the general population with self-report questionnaires, since a majority of individuals who rate positive for PLEs with self-scoring instruments could be identified as false positive after clinical assessment (41). Schultze-Lutter et al. reported a several-fold overestimation of the prevalence of clinician-rated psychotic symptoms when PLEs were assessed with self-report instruments including Peters et al. Delusion Inventory (PDI) and the revised Launay–Slade Hallucination Scale (LSHS-R) (42). Mixed results concerning the validity of PLE screening instruments were also found in adolescent populations (43, 44). However, self-reported subthreshold psychotic experiences in epidemiological non-help-seeking samples were found to index risk for the development of later psychotic disorders (45). Moreover, even “false positive” psychotic experiences were found to be associated with the later development of psychotic disorders (46), clinically relevant psychotic symptoms, mood and anxiety disorders, and reduced functioning (47). Second, there is a large heterogeneity concerning the inquired symptoms of PLE assessment tools as well as the measured “outcome” and inferences resulting from the answered items/questions: While the Magical Ideation Scale (MIS) examines magical ideation defined as an indicator of schizotypy and schizophrenia proneness (48), the Community Assessment of Psychic Experiences (CAPE), one of the most frequently used PLE self-rating instruments, was developed to assess the lifetime prevalence of PLEs in the general population by examining subclinical positive, negative, and depressive symptoms (49). Different questionnaires have different interpretations of PLEs leading to different findings regarding prevalence rates, persistence rates, and prognosis of PLEs. While most PLEs assessment tools assessed both thoughts and perceptions, some only assessed either thoughts or perceptions. Associated psychological factors including distress were assessed only in a few of the studied assessment tools (19). Needless to say, that related or phenomenologically similar phenomena as anomalous self-experiences (ASEs) are measured with separate assessment tools including the Inventory for Psychotic-Like Anomalous Experiences (IPASE) or the Examination of Anomalous Self-Experiences (EASE) (34, 50).
New approaches aiming for more subtle signs of reality distortion have created assessment tools for “exceptional experiences” (EEs) defined as deviations from experiences consistent with typical “reality models” (51) including hearing voices of beloved dead ones, déjà-vus, or out-of-body experiences (52). While EEs were first assumed as PLEs at the healthy end of the psychosis spectrum, the association with psychological problems (52) might need further clarification (13). Until now, there is no consensus about an agreed upon “gold standard” PLE assessment tool, and the multitude of assessment tools examining PLEs is striking. In Table 1, we give an overview of screening instruments for PLEs, psychotic symptoms, and high risk for psychosis.
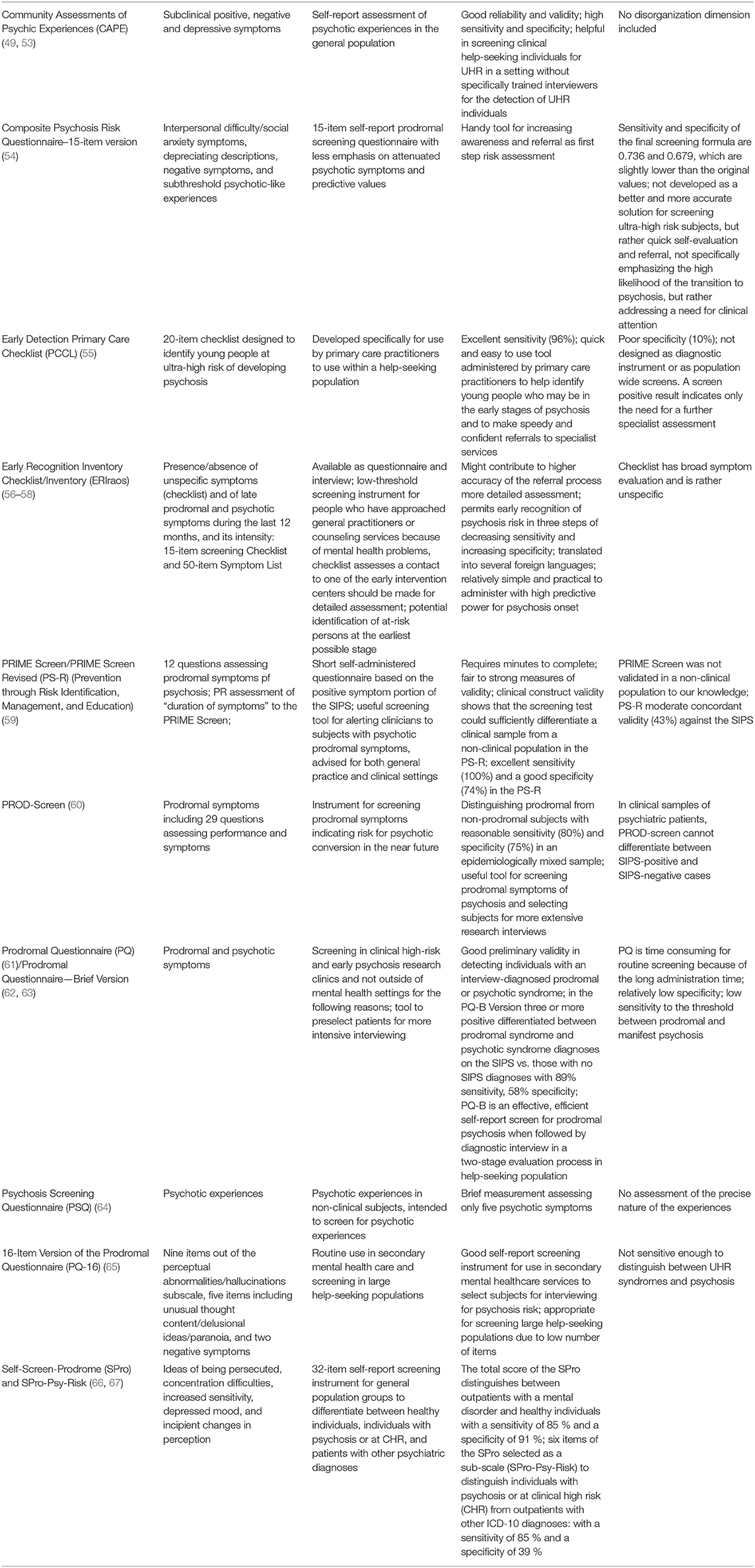
Table 1. Screening instruments for psychotic-like experiences/psychosis/high risk for psychosis.
Albeit generally assumed as non-clinical phenomena, PLEs have been identified as early indicators of psychosis (15, 68, 69) forecasting the development of a psychotic disorder with a 4-fold increased risk in non-help-seeking individuals (45). Moreover, PLEs were identified as markers for risk of suicidal behavior and severe psychopathology including multi-morbidity and poor functioning (70). However, clinical relevance was shown to be associated with different subtypes of PLEs and the level of associated distress, need for treatment (71, 72), impact on comorbidities, functioning, and vulnerability toward psychosis (72–74). While the subdimension of persecutory ideation (72) and hallucinations, delusions, and paranoia (71) were strongly correlated with distress, subdimensions of grandiosity and paranormal beliefs did not correlate with distress and general measures of psychopathology (71).
Since negative associations were reported between some specific PLE subtypes and psychopathological dimensions as depression (75) and physical anhedonia (76), in line with the concept of the “healthy schizotype” (77), some specific PLE subtypes might not be associated with clinical impact but are being discussed to constitute a coping mechanisms and response helping to maintain mental functioning (78).
In line with other researchers, we support the idea of conceptual clarity, consensus, and clear definitions regarding PLEs and associated concepts (9, 13, 25).
As previously suggested, an empirically established and agreed upon consensus catalog of terms, definitions, criteria, and categorization of PLEs according to psychopathological significance can help to achieve more standardized research and comparable data (25). To develop consensus, future research aiming for a better understanding of the phenomenology of PLEs seems crucial, especially since most studies did not focus on phenomenology of PLEs but rather quantitative measures (19). Since different subtypes of PLEs vary widely according to distress, associated psychopathology, help seeking, and clinical outcome (72, 79, 80), further research on the heterogenous character of different PLEs and associated psychological factors might help to differ between subclinical and clinically relevant psychotic experiences, improve risk screening, and foster new treatment and prevention strategies. The analysis of mediating factors between PLEs and clinical relevance including resilience, persistence of PLEs, environmental exposures, trauma, stressful life events, and cognitive impairments events might contribute to a better understanding of the evolution of mental disorders, especially psychosis spectrum disorders (23, 81–83). Moreover, the development and agreed upon use of a or a few “gold standard” assessment tools might help to gather more comparable data on PLEs concerning prevalence rates, prognosis, and other outcomes. As stated by other authors (13), longitudinal studies on PLEs and especially different PLE subtypes, might help to give more insight into the question why some individuals with PLEs develop mental disorders and others stay at the healthy end of the psychosis spectrum. Consequently, untangling this entanglement of PLE terms, definitions, and assessment tools might result in gathering more knowledge toward new prevention strategies and treatment approaches.
Well-validated screening instruments might help to detect distressed people with PLEs seeking help in general medical practice or in non-specialized psychiatric services. These may then be further assessed, in a clinical interview, in order to differentiate between actual psychotic symptoms or a clinical high-risk syndrome or PLEs without reaching any of the above. Finally, as part of a future consensus, not only definitions and assessments should be agreed upon but also the semantics used: Psychotic experiences in individuals from the healthy general population without associated distress should not be termed as symptoms (or “psychotic symptoms in the absence of illness,” which is in itself an oxymoron) (28) but as experiences. Whereas, in people with PLEs associated with distress, help-seeking behavior or any–not necessarily psychotic–psychiatric disorder, it is suggested that they be termed as symptoms. Some also argue that the term “psychotic” should not be used when referring to individuals fulfilling criteria for UHR/CHR, since only a minority of those continue to experience an actual psychotic disorder (84). We propose for the relevant proponents to engage in a continuing discussion aiming for an evidence-based consensus.
BH contributed to the concept of the review, the literature search, and draft of the manuscript. NM contributed to the concept of the review, supervision, and writing of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Kraepelin E. Manic depressive insanity and paranoia. J Nerv Ment Dis. (1921) 53:350. doi: 10.1097/00005053-192104000-00057
2. Van Os J, Hanssen M, Bijl RV, Ravelli A. Strauss (1969) revisited: a psychosis continuum in the general population? Schizophr Res. (2000) 45:11–20. doi: 10.1016/S0920-9964(99)00224-8
3. Verdoux H, van Os J. Psychotic symptoms in non-clinical populations and the continuum of psychosis. Schizophr Res. (2002) 54:59–65. doi: 10.1016/S0920-9964(01)00352-8
4. Hanssen M, Peeters F, Krabbendam L, Radstake S, Verdoux H, Van Os J. How psychotic are individuals with non-psychotic disorders? Soc Psychiatry Psychiatr Epidemiol. (2003) 38:149–54. doi: 10.1007/s00127-003-0622-7
5. Fusar-Poli P, Rutigliano G, Stahl D, Davies C, De Micheli A, Ramella-Cravaro V, et al. Long-term validity of the At Risk Mental State (ARMS) for predicting psychotic and non-psychotic mental disorders. Eur Psychiatry. (2017) 42:49–54. doi: 10.1016/j.eurpsy.2016.11.010
6. Yung AR, Phillips LJ, Yuen HP, Francey SM, McFarlane CA, Hallgren M, et al. Psychosis prediction: 12-month follow up of a high-risk (“prodromal”) group. Schizophr Res. (2003) 60:21–32. doi: 10.1016/S0920-9964(02)00167-6
7. Schultze-Lutter F, Michel C, Schmidt SJ, Schimmelmann B, Maric N, Salokangas R, et al. EPA guidance on the early detection of clinical high risk states of psychoses. Eur Psychiatry. (2015) 30:405–16. doi: 10.1016/j.eurpsy.2015.01.010
8. Meehl PE. Schizotaxia, schizotypy, schizophrenia. Am Psychol. (1962) 17:827. doi: 10.1037/h0041029
9. Grant P, Green MJ, Mason OJ. Models of schizotypy: the importance of conceptual clarity. Schizophr Bull. (2018) 44:S556–63. doi: 10.1093/schbul/sby012
10. Johns LC, Van Os J. The continuity of psychotic experiences in the general population. Clin Psychol Rev. (2001) 21:1125–41. doi: 10.1016/S0272-7358(01)00103-9
11. Comparelli, Raballo A, Pompili M, Galderisi S. Beyond the transnosographic emphasis on psychosis: nosological perspectives on schizophrenia and its prevention. Front Psychiatry. (2019) 10:666. doi: 10.3389/fpsyt.2019.00666
12. Unterrassner L, Wyss TA, Wotruba D, Ajdacic-Gross V, Haker H, Rössler W. Psychotic-like experiences at the healthy end of the psychosis continuum. Front Psychol. (2017) 8:775. doi: 10.3389/fpsyg.2017.00775
13. Unterrassner L. Subtypes of Psychotic-Like Experiences and Their Significance for Mental Health, Psychosis-Biopsychosocial and Relational Perspectives. London: IntechOpen (2018). doi: 10.5772/intechopen.78691
14. Hinterbuchinger B, Litvan Z, Meyer EL, Friedrich F, Kaltenboeck A, Gruber M, et al. Psychotic-like experiences in esoterism: a twilight zone? Schizophr Res. (2018) 193:240–3. doi: 10.1016/j.schres.2017.08.009
15. Nuevo R, Van Os J, Arango C, Chatterji S, Ayuso-Mateos J. Evidence for the early clinical relevance of hallucinatory-delusional states in the general population. Acta Psychiatr Scand. (2013) 127:482–93. doi: 10.1111/acps.12010
16. Tandon N, Montrose D, Shah J, Rajarethinam R, Diwadkar VA, Keshavan MS. Early prodromal symptoms can predict future psychosis in familial high-risk youth. J Psychiatr Res. (2012) 46:105–10. doi: 10.1016/j.jpsychires.2011.09.019
17. Van Os J, Linscott RJ, Myin-Germeys I, Delespaul P, Krabbendam L. A systematic review and meta-analysis of the psychosis continuum: evidence for a psychosis proneness-persistence-impairment model of psychotic disorder. Psychol Med. (2009) 39:179. doi: 10.1017/S0033291708003814
18. Nelson B, Fusar-Poli P, Yung AR. Can we detect psychotic-like experiences in the general population? Curr Pharma Des. (2012) 18:376–85. doi: 10.2174/138161212799316136
19. Lee KW, Chan KW, Chang WC, Lee EHM, Hui CLM, Chen EYH. A systematic review on definitions and assessments of psychotic-like experiences. Early Interv Psychiatry. (2016) 10:3–16. doi: 10.1111/eip.12228
20. McGrath JJ, Saha S, Al-Hamzawi A, Alonso J, Bromet EJ, Bruffaerts R, et al. Psychotic experiences in the general population: a cross-national analysis based on 31,261 respondents from 18 countries. JAMA Psychiatry. (2015) 72:697–705. doi: 10.1001/jamapsychiatry.2015.0575
21. Downs JM, Cullen AE, Barragan M, Laurens KR. Persisting psychotic-like experiences are associated with both externalising and internalising psychopathology in a longitudinal general population child cohort. Schizophr Res. (2013) 144:99–104. doi: 10.1016/j.schres.2012.12.009
22. Dominguez M, Wichers M, Lieb R, Wittchen HU, van Os J. Evidence that onset of clinical psychosis is an outcome of progressively more persistent subclinical psychotic experiences: an 8-year cohort study. Schizophr Bull. (2011) 37:84–93. doi: 10.1093/schbul/sbp022
23. Cougnard A, Marcelis M, Myin-Germeys I, De Graaf R, Vollebergh W, Krabbendam L, et al. Does normal developmental expression of psychosis combine with environmental risk to cause persistence of psychosis? A psychosis proneness–persistence model. Psychol Med. (2007) 37:513–27. doi: 10.1017/S0033291706009731
24. Wiles NJ, Zammit S, Bebbington P, Singleton N, Meltzer H, Lewis G. Self-reported psychotic symptoms in the general population: results from the longitudinal study of the British National Psychiatric Morbidity Survey. Br J Psychiatry. (2006) 188:519–26. doi: 10.1192/bjp.bp.105.012179
25. Schultze-Lutter F, Schimmelmann BG, Ruhrmann S. The Near Babylonian Speech Confusion in Early Detection of Psychosis. Oxford: Oxford University Press (2011). doi: 10.1093/schbul/sbr039
26. Rössler W, Ajdacic-Gross V, Müller M, Rodgers S, Haker H, Hengartner MP. Assessing sub-clinical psychosis phenotypes in the general population—a multidimensional approach. Schizophr Res. (2015) 161:194–201. doi: 10.1016/j.schres.2014.11.033
27. Strauss JS. Hallucinations and delusions as points on continua function: rating scale evidence. Archiv Gen Psychiatry. (1969) 21:581–6. doi: 10.1001/archpsyc.1969.01740230069010
28. Kelleher, Cannon M. Psychotic-like experiences in the general population: characterizing a high-risk group for psychosis. Psychol Med. (2011) 41:1–6. doi: 10.1017/S0033291710001005
29. Linscott RJ, van Os J. Systematic reviews of categorical versus continuum models in psychosis: evidence for discontinuous subpopulations underlying a psychometric continuum. Implications for DSM-V, DSM-VI, and DSM-VII. Annu Rev Clin Psychol. (2010) 6:391–419. doi: 10.1146/annurev.clinpsy.032408.153506
30. Hanssen M, Bijl R, Vollebergh W, Van Os J. Self-reported psychotic experiences in the general population: a valid screening tool for DSM-III-R psychotic disorders? Acta Psychiatr Scand. (2003) 107:369–77. doi: 10.1034/j.1600-0447.2003.00058.x
31. Preti A, Cella M, Raballo A, Vellante M. Psychotic-like or unusual subjective experiences? The role of certainty in the appraisal of the subclinical psychotic phenotype. Psychiatry Res. (2012) 200:669–73. doi: 10.1016/j.psychres.2012.07.014
33. Parnas J. A disappearing heritage: the clinical core of schizophrenia. Schizophr Bull. (2011) 37:1121–30. doi: 10.1093/schbul/sbr081
34. Cicero DC, Neis AM, Klaunig MJ, Trask CL. The Inventory of Psychotic-Like Anomalous Self-Experiences (IPASE): development and validation. Psychol Assess. (2017) 29:13. doi: 10.1037/pas0000304
35. Sass LA, Parnas J. Schizophrenia, consciousness, the self. Schizophr Bull. (2003) 29:427–44. doi: 10.1093/oxfordjournals.schbul.a007017
36. Nelson B, Sass LA, Thompson A, Yung AR, Francey SM, Amminger GP, et al. Does disturbance of self underlie social cognition deficits in schizophrenia and other psychotic disorders? Early Interv Psychiatry. (2009) 3:83–93. doi: 10.1111/j.1751-7893.2009.00112.x
37. Parnas J. The core Gestalt of schizophrenia. World Psychiatry. (2012) 11:67. doi: 10.1016/j.wpsyc.2012.05.002
38. Schultze-Lutter F, Theodoridou A. The concept of basic symptoms: its scientific and clinical relevance. World Psychiatry. (2017) 16:104. doi: 10.1002/wps.20404
39. Schultze-Lutter F. Subjective symptoms of schizophrenia in research and the clinic: the basic symptom concept. Schizophr Bull. (2009) 35:5–8. doi: 10.1093/schbul/sbn139
40. Huber G, Gross G. The concept of basic symptoms in schizophrenic and schizoaffective psychoses. Recent Prog Med. (1989) 80:646–52.
41. Nordgaard J, Buch-Pedersen M, Hastrup LH, Haahr UH, Simonsen E. Measuring psychotic-like experiences in the general population. Psychopathology. (2019) 52:240–7. doi: 10.1159/000502048
42. Schultze-Lutter F, Renner F, Paruch J, Julkowski D, Klosterkötter J, Ruhrmann S. Self-reported psychotic-like experiences are a poor estimate of clinician-rated attenuated and frank delusions and hallucinations. Psychopathology. (2014) 47:194–201. doi: 10.1159/000355554
43. Laurens KR, Hodgins S, Maughan B, Murray RM, Rutter ML, Taylor EA. Community screening for psychotic-like experiences and other putative antecedents of schizophrenia in children aged 9–12 years. Schizophr Res. (2007) 90:130–46. doi: 10.1016/j.schres.2006.11.006
44. Horwood J, Salvi G, Thomas K, Duffy L, Gunnell D, Hollis C, et al. IQ and non-clinical psychotic symptoms in 12-year-olds: results from the ALSPAC birth cohort. Br J Psychiatry. (2008) 193:185–91. doi: 10.1192/bjp.bp.108.051904
45. Kaymaz N, Drukker M, Lieb R, Wittchen HU, Werbeloff N, Weiser M, et al. Do subthreshold psychotic experiences predict clinical outcomes in unselected non-help-seeking population-based samples? A systematic review and meta-analysis, enriched with new results. Psychol Med. (2012) 42:2239–53. doi: 10.1017/S0033291711002911
46. Bak M, Delespaul P, Hanssen M, de Graaf R, Vollebergh W, van Os J. How false are “false” positive psychotic symptoms? Schizophr Res. (2003) 62:187–9. doi: 10.1016/s0920-9964(02)00336-5
47. van der Steen Y, Myin-Germeys I, van Nierop M, Ten Have M, de Graaf R, van Dorsselaer S, et al. ‘False-positive'self-reported psychotic experiences in the general population: an investigation of outcome, predictive factors and clinical relevance. Epidemiol Psychiatr Sci. (2019) 28:532. doi: 10.1017/S2045796018000197
48. Eckblad M, Chapman LJ. Magical ideation as an indicator of schizotypy. J Consult Clin Psychol. (1983) 51:215. doi: 10.1037/0022-006X.51.2.215
49. Konings M, Bak M, Hanssen M, Van Os J, Krabbendam L. Validity and reliability of the CAPE: a self-report instrument for the measurement of psychotic experiences in the general population. Acta Psychiatr Scand. (2006) 114:55–61. doi: 10.1111/j.1600-0447.2005.00741.x
50. Parnas J, Møller P, Kircher T, Thalbitzer J, Jansson L, Handest P, et al. EASE: examination of anomalous self-experience. Psychopathology. (2005) 38:236. doi: 10.1159/000088441
51. Metzinger T. Being No One: The Self-Model Theory of Subjectivity. Cambridge, MA; London: MIT Press (2004). doi: 10.7551/mitpress/1551.001.0001
52. Fach W, Atmanspacher H, Landolt K, Wyss T, Rössler W. A comparative study of exceptional experiences of clients seeking advice and of subjects in an ordinary population. Front Psychol. (2013) 4:65. doi: 10.3389/fpsyg.2013.00065
53. Mossaheb N, Becker J, Schaefer MR, Klier CM, Schloegelhofer M, Papageorgiou K, et al. The Community Assessment of Psychic Experience (CAPE) questionnaire as a screening-instrument in the detection of individuals at ultra-high risk for psychosis. Schizophr Res. (2012) 141:210–4. doi: 10.1016/j.schres.2012.08.008
54. Liu CC, Tien YJ, Chen CH, Chiu YN, Chien YL, Hsieh MH, et al. Development of a brief self-report questionnaire for screening putative pre-psychotic states. Schizophr Res. (2013) 143:32–7. doi: 10.1016/j.schres.2012.10.042
55. French P, Owens J, Parker S, Dunn G. Identification of young people in the early stages of psychosis: validation of a checklist for use in primary care. Psychiatry Res. (2012) 200:911–6. doi: 10.1016/j.psychres.2012.07.040
56. Häfner H, Maurer K, Ruhrmann S, Bechdolf A, Klosterkötter J, Wagner M, et al. Early detection and secondary prevention of psychosis: facts and visions. Eur Archiv Psychiatry Clin Neurosci. (2004) 254:117–28. doi: 10.1007/s00406-004-0508-z
57. Maurer K, Zink M, Rausch F, Häfner H. The early recognition inventory ERI raos assesses the entire spectrum of symptoms through the course of an at-risk mental state. Early Interv Psychiatry. (2018) 12:217–28. doi: 10.1111/eip.12305
58. Hurlemann R, Jessen F, Wagner M, Frommann I, Ruhrmann S, Brockhaus A, et al. Interrelated neuropsychological and anatomical evidence of hippocampal pathology in the at-risk mental state. Psychol Med. (2008) 38:843–51. doi: 10.1017/S0033291708003279
59. Kobayashi H, Nemoto T, Koshikawa H, Osono Y, Yamazawa R, Murakami M, et al. A self-reported instrument for prodromal symptoms of psychosis: testing the clinical validity of the PRIME Screen—Revised (PS-R) in a Japanese population. Schizophr Res. (2008) 106:356–62. doi: 10.1016/j.schres.2008.08.018
60. Heinimaa M, Salokangas R, Ristkari T, Plathin M, Huttunen J, Ilonen T, et al. PROD-screen–a screen for prodromal symptoms of psychosis. Int J Methods Psychiatr Res. (2003) 12:92–104. doi: 10.1002/mpr.146
61. Loewy RL, Bearden CE, Johnson JK, Raine A, Cannon TD. The prodromal questionnaire (PQ): preliminary validation of a self-report screening measure for prodromal and psychotic syndromes. Schizophr Res. (2005) 79:117–25. doi: 10.1016/j.schres.2005.03.007
62. Loewy RL, Pearson R, Vinogradov S, Bearden CE, Cannon TD. Psychosis risk screening with the Prodromal Questionnaire—brief version (PQ-B). Schizophr Res. (2011) 129:42–6. doi: 10.1016/j.schres.2011.03.029
63. Kline E, Wilson C, Ereshefsky S, Denenny D, Thompson E, Pitts SC, et al. Psychosis risk screening in youth: a validation study of three self-report measures of attenuated psychosis symptoms. Schizophr Res. (2012) 141:72–7. doi: 10.1016/j.schres.2012.07.022
64. Bebbington P, Nayani T. The psychosis screening questionnaire. Int J Methods Psychiatr Res. (1995) 5:11–9. doi: 10.1037/t30040-000
65. Ising HK, Veling W, Loewy RL, Rietveld MW, Rietdijk J, Dragt S, et al. The validity of the 16-item version of the Prodromal Questionnaire (PQ-16) to screen for ultra high risk of developing psychosis in the general help-seeking population. Schizophr Bull. (2012) 38:1288–96. doi: 10.1093/schbul/sbs068
66. Kammermann J, Stieglitz R, Riecher-Rössler A. “Self-screen prodrome”–self-rating for the early detection of mental disorders and psychoses. Fortschr Neurol Psychiatrie. (2009) 77:278–84. doi: 10.1055/s-0028-1109227
67. Müller M, Vetter S, Buchli-Kammermann J, Stieglitz RD, Stettbacher A, Riecher-Rössler A. The Self-screen-Prodrome as a short screening tool for pre-psychotic states. Schizophr Res. (2010) 123:217–24. doi: 10.1016/j.schres.2010.08.018
68. Welham J, Scott J, Williams G, Najman J, Bor W, O'callaghan M, et al. Emotional and behavioural antecedents of young adults who screen positive for non-affective psychosis: a 21-year birth cohort study. Psychol Med. (2009) 39:625. doi: 10.1017/S0033291708003760
69. Poulton R, Caspi A, Moffitt TE, Cannon M, Murray R, Harrington H. Children's self-reported psychotic symptoms and adult schizophreniform disorder: a 15-year longitudinal study. Archiv Gen Psychiatry. (2000) 57:1053–8. doi: 10.1001/archpsyc.57.11.1053
70. Kelleher, Devlin N, Wigman JT, Kehoe A, Murtagh A, Fitzpatrick C, et al. Psychotic experiences in a mental health clinic sample: implications for suicidality, multimorbidity and functioning. Psychol Med. (2014) 44:1615–24. doi: 10.1017/S0033291713002122
71. Wigman JT, Vollebergh WA, Raaijmakers QA, Iedema J, Van Dorsselaer S, Ormel J, et al. The structure of the extended psychosis phenotype in early adolescence—a cross-sample replication. Schizophr Bull. (2011) 37:850–60. doi: 10.1093/schbul/sbp154
72. Yung AR, Nelson B, Baker K, Buckby JA, Baksheev G, Cosgrave EM. Psychotic-like experiences in a community sample of adolescents: implications for the continuum model of psychosis and prediction of schizophrenia. Aust N Z J Psychiatry. (2009) 43:118–28. doi: 10.1080/00048670802607188
73. Brett C, Peters E, McGuire P. Which psychotic experiences are associated with a need for clinical care? Eur Psychiatry. (2015) 30:648–54. doi: 10.1016/j.eurpsy.2014.12.005
74. van Os J, Reininghaus U. Psychosis as a transdiagnostic and extended phenotype in the general population. World Psychiatry. (2016) 15:118–24. doi: 10.1002/wps.20310
75. Yung AR, Buckby JA, Cotton SM, Cosgrave EM, Killackey EJ, Stanford C, et al. Psychotic-like experiences in nonpsychotic help-seekers: associations with distress, depression, and disability. Schizophr Bull. (2006) 32:352–9. doi: 10.1093/schbul/sbj018
76. Unterrassner L, Wyss TA, Wotruba D, Haker H, Rössler W. The intricate relationship between psychotic-like experiences and associated subclinical symptoms in healthy individuals. Front Psychol. (2017) 8:1537. doi: 10.3389/fpsyg.2017.01537
77. McCreery C, Claridge G. Healthy schizotypy: the case of out-of-the-body experiences. Pers Indiv Differ. (2002) 32:141–54. doi: 10.1016/S0191-8869(01)00013-7
78. Perkins SL, Allen R. Childhood physical abuse and differential development of paranormal belief systems. J Nerv Ment Dis. (2006) 194:349–55. doi: 10.1097/01.nmd.0000217832.85665.c5
79. Wigman JT, Vollebergh WA, Jacobs N, Wichers M, Derom C, Thiery E, et al. Replication of the five-dimensional structure of positive psychotic experiences in young adulthood. Psychiatry Res. (2012) 197:353–5. doi: 10.1016/j.psychres.2011.09.015
80. Turley D, Drake R, Killackey E, Yung AR. Perceived stress and psychosis: the effect of perceived stress on psychotic-like experiences in a community sample of adolescents. Early Interv Psychiatry. (2019) 13:1465–9. doi: 10.1111/eip.12795
81. Barahmand U, Heydari Sheikh Ahmad R. Psychotic-like experiences and psychological distress: the role of resilience. J Am Psychiatr Nurses Assoc. (2016) 22:312–9. doi: 10.1177/1078390316653802
82. J. Wigman, van Winkel R, Raaijmakers QA, Ormel J, Verhulst FC, Reijneveld S, et al. Evidence for a persistent, environment-dependent and deteriorating subtype of subclinical psychotic experiences: a 6-year longitudinal general population study. Psychol Med. (2011) 41:2317–29. doi: 10.1017/S0033291711000304
83. Schofield K, Claridge G. Paranormal experiences and mental health: schizotypy as an underlying factor. Pers Indiv Differ. (2007) 43:1908–16. doi: 10.1016/j.paid.2007.06.014
84. Moritz S, Gaweda Ł, Heinz A, Gallinat J. Four reasons why early detection centers for psychosis should be renamed and their treatment targets reconsidered: we should not catastrophize a future we can neither reliably predict nor change. Psychol Med. (2019) 49:2134–40. doi: 10.1017/S0033291719001740
Keywords: psychotic-like experiences, psychosis continuum, subclinical psychosis, psychosis phenotype, psychotic disorder
Citation: Hinterbuchinger B and Mossaheb N (2021) Psychotic-Like Experiences: A Challenge in Definition and Assessment. Front. Psychiatry 12:582392. doi: 10.3389/fpsyt.2021.582392
Received: 04 September 2020; Accepted: 16 February 2021;
Published: 29 March 2021.
Edited by:
Peter Uhlhaas, University of Glasgow, United KingdomReviewed by:
Sarah Tosato, University of Verona, ItalyCopyright © 2021 Hinterbuchinger and Mossaheb. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Barbara Hinterbuchinger, YmFyYmFyYS5oaW50ZXJidWNoaW5nZXJAbWVkdW5pd2llbi5hYy5hdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.