
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry, 10 December 2020
Sec. Forensic Psychiatry
Volume 11 - 2020 | https://doi.org/10.3389/fpsyt.2020.614409
 Christina Spinelli1*
Christina Spinelli1* Etienne Paradis-Gagné2
Etienne Paradis-Gagné2 Megan Per1
Megan Per1 Matthew H. Fleischmann1
Matthew H. Fleischmann1 Viktoriya Manova1
Viktoriya Manova1 Aimée Wallace1
Aimée Wallace1 Bassam Khoury1
Bassam Khoury1Forensic inpatients (i. e., individuals found not responsible for a criminal offense on account of mental illness) represent an often marginalized and difficult-to-treat population. This has led to the need for research exploring the effectiveness of novel interventions. A Canadian forensic hospital has developed an 8-weeks mindfulness and yoga training program (MTP). This pilot study examined the potential effects of this program on patients' mindfulness, stress, and use of cognitive and emotion regulation strategies. A sample of 13 forensic inpatients (male = 92%) participating in the MTP program completed self-report measures assessing dispositional mindfulness, perceived stress, and use of cognitive emotion regulation strategies at baseline, post-intervention, and a 3-months follow-up. Repeated measure ANOVAs found a significant increase in the describe facet of mindfulness (p = 0.03) with a large effect size (ηp2 = 0.26) and a significant decrease in stress (p = 0.003) with a large effect size (ηp2 = 0.39). Pairwise comparisons revealed medium to large significant changes between baseline and post-intervention for both the describe facet (p = 0.03, Hedge's g = 0.55) and stress (p = 0.003, Hedge's g = 0.70). However, comparisons were insignificant between baseline and follow-up. No significant main effects were found on the use of cognitive emotion regulation strategies. This pilot study offers preliminary support for the use of the MTP as an adjunctive therapy in forensic inpatient treatment. Further investigation is needed into the long-term impacts of this training.
Mindfulness is the process of being purposefully present, alert, and attentive in the moment (1). The goal of mindfulness is to teach one to self-observe in an objective and detached manner and to be reflective rather than reflexive (2–4). One modality of practicing mindfulness is yoga, which has been described as mindfulness in motion and encompasses a group of integrative physical and spiritual practices with the goal to transform the mind and body (2, 5). Unlike many other mindfulness strategies which tend to be sedentary, yoga involves movement and focuses awareness onto one's physical body, and one's motion in the present. Scientific reports on mindfulness training support its use as an intervention for a variety of physical and psychological difficulties (6–8). In particular, yoga is suggested to be an effective treatment for stress, anxiety, depression, and substance abuse (2, 5, 9–11).
Despite the growing interest in mindfulness research on various settings and populations, the research on the effectiveness of mindfulness-based and yoga interventions for forensic inpatient populations is in its infancy. These individuals have been found not criminally responsible for an offense on account of mental illness and are sent to a forensic facility for treatment (12). As they represent a marginalized population and can be considered difficult-to-treat, there is a need to explore adjunctive treatments (13). Mindfulness has been argued to be effective as it reduces risk factors and addresses three main concerns: (1) poor affective self-regulation, (2) poor anger control, and (3) impulsivity (14).
Furthermore, forensic inpatients share similarities with incarcerated and psychiatric populations. First, forensic inpatients have committed a criminal offense and are mandated to be in a psychiatric facility. Second, the National Trajectory Project examined the NCR population in Canada and found (1) the most common primary diagnosis was a psychotic spectrum disorder, (2) 33% had a severe mental illness and an associated substance use disorder, and (3) 72% had at least one prior psychiatric hospitalization (15). Mindfulness interventions have been used with both incarcerated [e.g., (16–22)] and psychiatric [e.g., (23–27)] populations, and there is a larger body of research into their effectiveness.
In incarcerated populations, it is proposed that mindfulness training offers a healthy coping mechanism for inmates to better manage the stress of prison life and be less reactive to intense emotional states. A recent meta-analysis found that mindfulness-based interventions significantly reduce psychological outcomes (e.g., depression) and criminogenic needs (e.g., impulsivity) in pre-post studies (28). A pilot RCT also found reductions in risk behavior following release from incarceration (29). Small but positive effects of yoga on psychological behavioral functioning have also been found (2). For populations with severe mental illness (including psychosis), it has been proposed that mindfulness aids in alleviating the distress associated with psychosis by helping patients relate differently to their psychotic experience (8, 30). Individuals learn to see psychotic sensations as transient and recognize these sensations do not fundamentally define them as individuals (31). Khoury et al. (8) found a moderate effect of mindfulness interventions on reducing negative symptoms of psychosis and increasing functioning and quality of life. Mindfulness practice also appears feasible and acceptable for inpatients, with more active interventions (e.g., yoga) possibly being most appropriate (26).
Taken together, mindfulness and yoga training appear beneficial for incarcerated populations and individuals with severe mental illness. This adds to the argument that such training can be useful adjunctive interventions with forensic inpatients. However, the present literature is limited. Singh et al. (32) examined the effects of a mindfulness meditation program on aggression in forensic in patients with mild intellectual disabilities. Data collected by staff members indicated substantial reductions in physical and verbal aggression. A more recent mixed-methods study by Singh et al. (33) examined mindfulness meditation as treatment for adult sexual offenders with intellectual disabilities in a forensic facility. They found that the three participants were more successful at controlling their deviant sexual arousal when using the learned mindfulness exercises.
Most recently, Sistig et al. (34) conducted a preliminary evaluation of mindful-yoga as an adjunctive treatment for forensic inpatients in New Zealand. To our knowledge, this study is the first to assess the use of mindful-yoga with forensic inpatient adults. They examined the effectiveness of an 8-weeks mindful-yoga program on 26 inpatients and conducted baseline, post-intervention, and 2-months follow-up assessments. A mixed-methods design was used to examine trait mindfulness, stress, anxiety, depression, and general distress. 92% of participants reported that the delivery of the program was acceptable. In addition, they found subjective increases in body and breath awareness, greater relaxation, and a trend toward reduced anxiety and increased mindfulness (on the observing facet). Although the study lacked statistically significant results, benefit-consistent trends were found. Furthermore, the qualitative findings suggest the suitability of mindful-yoga for forensic patients and that there are perceived physical, emotional, and social benefits of this program.
The research on mindfulness and yoga as adjunctive therapies for forensic inpatients is limited both in number and by methodological concerns; indicating a need for further research. There is also a lack of research examining Canadian populations. Currently, a Canadian forensic hospital runs an 8-weeks mindfulness and yoga training program (MTP) for adults suffering from various psychiatric disorders (e.g., schizophrenia, personality disorders). We conducted a pilot study examining the program's effects on patients' mindfulness, stress, and cognitive and emotional regulation strategies.
Thirty-six adult forensic inpatients expressed interest in participation. They were included in the study if they had self-selected to be enrolled in an 8-weeks mindfulness training program (MTP) and were 18 years or older. In addition, the hospital staff could exclude any individual when clinical judgment deemed them unsuitable to participate. Twenty-three were removed because they either did not complete the consent form (n = 3), did not complete the measures at all timepoints (n = 15), completed the MTP previously (n = 2), attended <3 sessions (n = 2), or found out they were leaving the facility and stated this likely impacted their results (n = 1). This left 13 participants in the final analysis.
The study took place at a Canadian forensic hospital, and the MTP was developed by the staff of the hospital with the objectives of enhancing the practice of meditation and mindfulness, establishing a sense of calm and serenity, developing concentration and creativity, and learning to be aware of and manage anxiety as well as other negative emotions. Twice a year, two MTP groups were facilitated concurrently; leading to four periods of recruitment across 2 years (2016 to 2018). The program was designed as an adjunctive therapy and all participants continued to receive their psychiatric treatment-as-usual. Each session was 1.5–2 h long and included meditation and/or yoga practice. A brief description of the 8-weeks syllabus can be found in Table 1. During the first session, participants received a CD containing mindfulness and yoga exercises they could practice outside the sessions. Participants also received ongoing support and tools as well as readings throughout each session. This program had been established for 4 years prior to the start of this study and was facilitated by the two developers: (1) a nurse-clinician trained in mindfulness therapeutic practices, and (2) a specialized educator who is also a yoga instructor. Both were employed at the hospital and had worked in mental health for over 25 years.
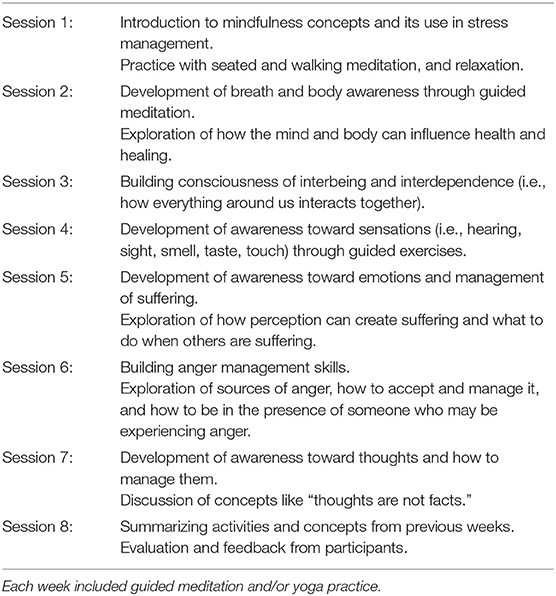
Table 1. Description of the weekly activities in the mindfulness training program.
The MTP was presented by the two facilitators on all units of the hospital. Those who were interested could then subscribe to the program. Patients who could not leave their units for clinical reasons (e.g., high risk of violence or psychotic decompensation) were not able to participate in the program as it was held in a room outside of the units. The facilitators had discussions with the care team and the unit psychiatrist to identify participants who would be eligible to participate.
Participants enrolled in the MTP were then approached by the clinic nurse specialist (E.P.G.) and a trained research assistant. Patients were verbally informed of the study and were explicitly told that their decision to accept or decline to participate would not impact their spot in the MTP. Those agreeing to participate gave informed consent and completed measures in English or French at baseline, post-MTP, and 3-months follow-up. Participants were assisted when filling in the questionnaires and were able to take breaks. We initially sought to obtain a convenience sample of control participants by asking individuals who were not interested in participating in the MTP or were not enrolled at that time if they would be interested in completing questionnaires. However, this was not possible due to low interest. All procedures were approved by the Research Ethics Board at the hospital and McGill University.
A brief questionnaire with questions about age, diagnosis, race, sex, and hospitalizations. Information was obtained through self-report and consulting medical records.
The Five Facet Mindfulness Questionnaire [FFMQ; (35, 36)] is a 39-item measure of dispositional mindfulness that assesses five facets, specifically: (1) observing, (2) describing, (3) acting with awareness, (4) non-judging of, and (5) non-reactivity to inner experience. A 5-point Likert scale is used and ranges from Never or Very Rarely True to Very often or Always True. The FFMQ has been previously used with inpatient forensic populations (34) and other clinical populations (37). The psychometric properties of this measure were generally good across timepoints [total score [α = 0.86 to α = 0.94], describing [α = 0.81 to α = 0.92], acting with awareness [α = 0.84 to α = 0.89], and non-judging [α = 0.79 to α = 0.83]]. However, the observing (α = 0.52 to α = 0.83) and non-reactivity facets (α = 0.49 to α = 0.80) had poorer psychometric properties; suggesting the need for caution during interpretation.
The Perceived Stress Scale [PSS; (38–40)] is a 10-item measure that evaluates the extent one sees common life situations as being stressful over the last month. A 5-point Likert scale is used and ranges from Never to Very Often. The PSS has been used with forensic (34) and incarcerated populations (17). There was strong internal consistency (ranging from α = 0.81 to α = 0.93) within this sample across the three timepoints.
The Cognitive Emotion Regulation Questionnaire [CERQ; (41, 42)] is a 36-item questionnaire that evaluates nine cognitive and emotion regulation strategies used when responding to negative circumstances. A 5-point Likert scale is used and ranges from Almost Never to Almost Always. Strong properties were found with positive refocusing (α = 0.90 to α = 0.95), positive reappraisal (α = 0.79 to α = 0.90), and other-blame (α = 0.81 to α = 0.89). The psychometric strength varied from acceptable to strong depending on the time point for acceptance (α = 0.59 to α = 0.74), refocus on planning (α = 0.63 to α = 0.95), putting into perspective (α = 0.52 to α = 0.86)], catastrophizing (α = 0.64 to α = 0.86), and rumination (α = 0.50 to α = 0.82). Finally, self-blame's psychometric properties were inadequate (α < 0.5); as such, this subscale was removed from our analyses.
One-way repeated-measures analysis of variances (ANOVA) were conducted using IBM SPSS Statistics (Version 25 for Windows). Pairwise comparisons were used to contrast timepoints. In addition, Bayesian repeated measure ANOVAs were conducted using JASP (Version 0.14 for Windows) to further assess our findings (43). Uninformative prior odds were used due to the scarcity and limitations of previous studies. One missing value was resolved through subscale mean replacement. An outlier (±3.5 SD) was removed from the observing and non-reactivity facets.
The sample was predominately male (92%), ranging in age from 19 to 48 years (Mage = 33.54, SD = 9.87). The majority of the participants were white (n = 10, 76.9%) and three participants (23.1%) were from another racial background. The average number of years spent in school were 10.5 (SD = 2.71; Range = 8–17 years). The majority of participants had a primary psychiatric diagnosis of schizophrenia (n = 5, 38.5%), followed by schizoaffective disorder (n = 3, 23%). A substantial number of participants (n = 8, 61.5%) had more than one psychiatric diagnosis and 38.5% of participants (n = 5) had comorbidity with a personality disorder and/or substance-use disorder. Clozapine (n = 4, 31%) was the most frequently prescribed antipsychotic medication. Most participants committed a form of assault (n = 9; 69.2%) followed by murder (n = 3, 23.1%). 38.5% of participants had no prior history of arrest (n = 5), 30.8% of participants reported one prior arrest (n = 4), and 23.1% of participants reported two prior arrest incidents (n = 2). The average number of prior hospitalizations were 5.27 and ranged from 1 to 20 visits. Most participants were enrolled in other treatment programs in the facility such as individual psychotherapy (n = 7; 53.8%), relapse prevention program (n = 4; 30.8%), and anger management program (n = 2; 15.4%). Individual psychotherapy is offered by a team of psychologists using different psychotherapy approaches. The relapse prevention and anger management groups are facilitated by clinicians and utilize motivational and cognitive-behavioral approaches, respectively.
Mean values, standard deviations, and effect sizes (partial eta squared effect sizes and Hedge's g) for all outcomes (i.e., mindfulness facets, stress, and cognitive emotion regulation strategies) at each time point as well as the one-way repeated measures ANOVA statistics can be found in Table 2. Additional pairwise comparisons can be found in Table 3.
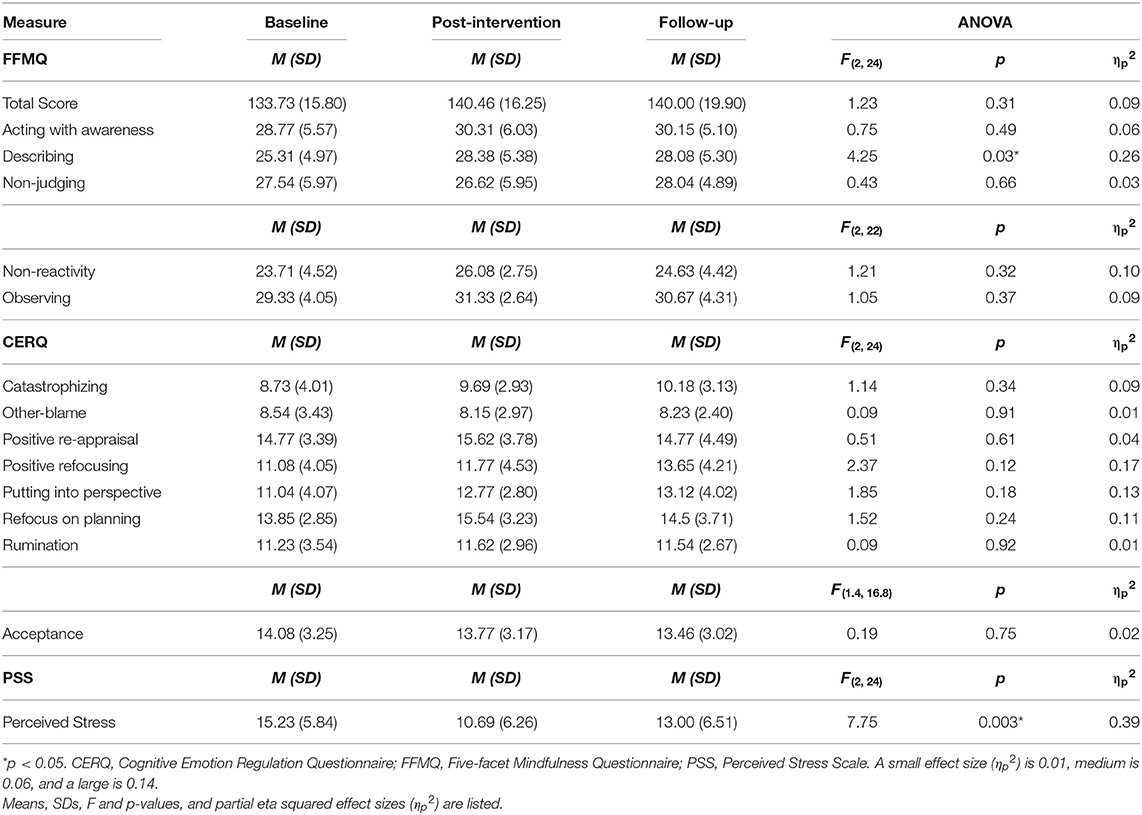
Table 2. Statistics of one-way repeated-measures ANOVA tests for the total score on mindfulness (and its five facets), perceived stress, and cognitive emotion regulation strategies.
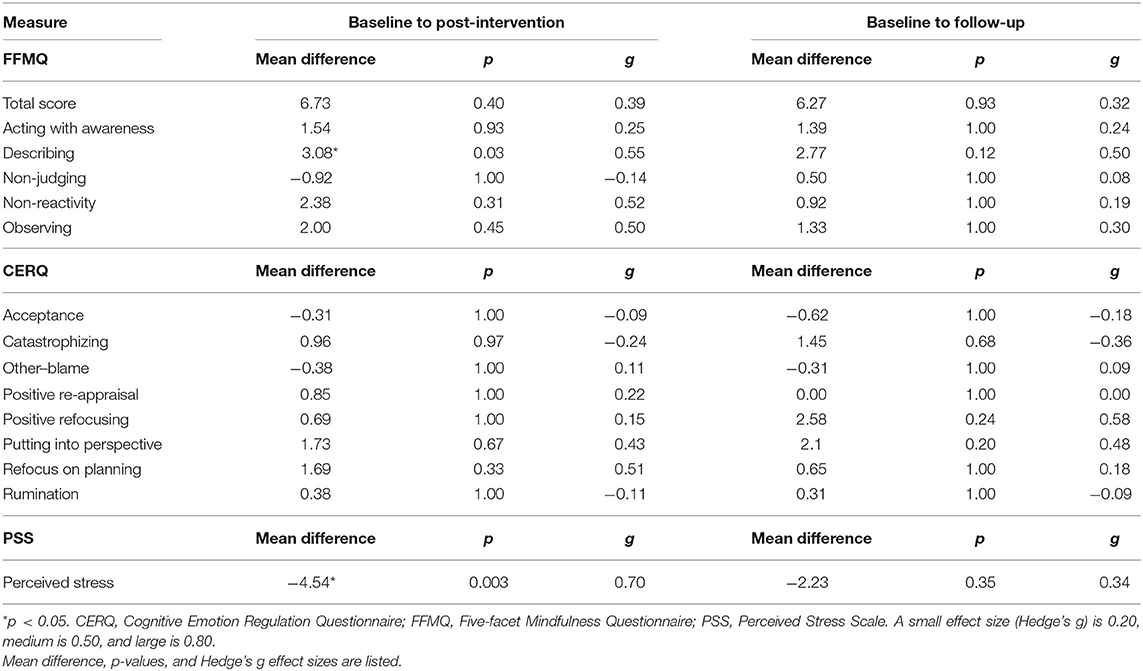
Table 3. Pairwise comparisons at baseline, post-intervention and follow-up for the total score on mindfulness (and its five facets, perceived stress, and cognitive emotion regulation strategies.
A large significant main effect of the MTP was found on the describing facet, F(2, 24) = 4.25, p = 0.03, ηp2 = 0.26 and on stress, F(2, 24) = 7.75, p = 0.003, ηp2 = 0.39. Further pairwise comparisons (using a Bonferroni correction) revealed a significant increase between baseline and post-intervention for describing (p = 0.03; Hedge's g = 0.55) and stress (p = 0.003; Hedge's g = 0.70). However, the increase was non-significant between baseline and follow-up. No main effects were found on overall mindfulness, its other facets, and the CERQ subscales. The results of the Bayesian analyses revealed similar findings to the inferential statistics and can be found in the Supplementary Material.
There has been evidence of increased mindfulness through mindfulness-based interventions in prison and psychiatric populations (8, 28). For forensic inpatients, prior research has demonstrated an increasing trend in the observing facet in their study on mindful-yoga training with forensic inpatients (34). This facet examines one's sensory awareness and has been argued to develop earlier in the process of learning mindfulness. Likewise, An et al. (44) found significant increases in the observing and non-reactivity facets in prisoners who completed a mindfulness training as compared to a waitlist control. In contrast, we found a significant increase in the describing facet which was driven by the change between baseline and post-intervention. The describing facet explores an individual's ability to label and share their experiences using words, and it negatively correlates with alexithymia [i.e., difficulty in describing one's emotional states; (35)]. Day (45) summarized research that suggests offenders score highly on alexithymia. Furthermore, treatment engagement is arguably affected by their ability to describe feelings. Thus, changes in the describing facet may be important for this population and may provide a potential understanding for how the MTP is helping participants. In addition, learning to describe one's emotional state is a skill that can potentially benefit other treatments. For example, many participants were engaged in therapy and other groups for which expressing one's feelings would be pertinent. Exploring this impact is beyond the scope of our study, but future researchers could elucidate other ways mindful-yoga impacts patient well-being and treatment.
Researchers of incarcerated populations have noted prison is a stressful environment (2), and the present investigation found a significant decrease in perceived stress from baseline to post-intervention, but not at follow-up. While quantitative and qualitative studies examining the impact of mindfulness and/or yoga on stress have shown significant reductions in prison populations [e.g., (28)] and in psychiatric inpatients [e.g., (46)], others have not found reductions in perceived stress [e.g., (34)]. Interestingly, although Sistig et al. (34) did not have significant quantitative findings, the forensic inpatients qualitatively reported mindful-yoga training aided in stress management. It is possible the equivocal findings are due to external factors. The stressful environment and circumstantial factors (e.g., changes in medication) could impact participant responses. Qualitative reports may offer a more comprehensive understanding of how participants perceive stress; highlighting the importance of such feedback in this line of research.
Howells et al. (14) highlighted how forensic inpatients may have poor self-regulation strategies and argued how mindfulness training and practice may aid in developing such skills. In exploring the impact of the MTP on the use of different cognitive and emotion regulation strategies, no significant changes were noted. These findings are aligned with another study examining mindfulness training with early psychosis patients (25, 47). It is possible that these nonsignificant findings are due to the variable psychometric properties of the subscales. When focusing on the three subscales with the strongest properties (i.e., positive refocusing, positive reappraisal, and other-blame), benefit-consistent changes are noted. In particular, the increase in positive refocusing persists into follow-up. Positive refocusing is a strategy wherein the individual seeks to focus on pleasant ideas rather than what might be causing distress. As the MTP program emphasizes directing attention in a positive direction and includes in-depth discussions about happiness and what that means for an individual, it is understandable that positive refocusing emerges as a potentially important strategy. Further exploration of these different strategies would be important.
For the two significant changes observed in this study, significant pairwise comparisons were noted only between baseline and post-intervention. At the 3-months follow up, the describe facet had decreased while stress had increased again albeit the means did not reach baseline levels. In contrast, the qualitative findings on stress reported by Sistig et al. (34) appeared to be maintained at follow-up along with their benefit consistent trend for the observe mindfulness facet. It should be noted that our follow-up period (3-months) is slightly longer than their 2-months follow-up. Taken together, the findings suggest the long-term effects of the MTP are unclear and warrant further exploration. In particular, it would be of interest to explore how the participants engage with mindfulness and yoga following program completion. How much participants engage in the taught activities in the subsequent months would be an in important moderating factor. In addition, exploring important life changes between the completion of the program and the follow-up would be of value. For example, changes in social interaction or treatment could impact findings.
There are seven key limitations to be noted: (1) small sample size and large attrition, (2) the increase familywise error rate from multiple statistical analyses was not controlled due to the small sample and preliminary nature of the study, (3) measures are limited by psychometric strength and focus on clinical measures, (4) qualitative measures on program acceptability were not included, (5) program fidelity was not assessed, (6) most patients participated in other therapeutic groups, and (7) statements on the generalizability of our findings are limited by the small sample and the inclusion of only one institution. Based on these limitations, we recommend future studies include more comprehensive quantitative measures (i.e., including nonclinical outcomes): (1) at baseline, post-intervention, and follow-up, and (2) before and after each weekly session. We further suggest adding qualitative measures regarding program feasibility, impact, and the types of mindfulness practiced independently. It would have been of interest to know how patients felt about the program, whether they would recommend it to others, and what benefits they perceived from participation. Finally, a controlled research design with a longer follow-up period is needed to ascertain the impact of such programs.
This is the second study examining the impact of mindful-yoga on forensic inpatients, and the first exploring Canadians. The significant findings may support the MTP's use as an adjunctive intervention; specifically, the reduction in stress and increase in the describing facet may support patients with transitioning into the facility and engaging in other treatments. As a vulnerable population who are in need of well-researched adjunctive therapies, the present pilot study is an important attempt at quantifying the effects of mindfulness and yoga training on forensic inpatients and supports the potential for expansion to other facilities in Canada.
The datasets presented in this article are not readily available because our ethics certificate did not include sharing any data with a third party even if it is non-identifiable. Requests to access the datasets should be directed to YmFzc2FtLmVsLWtob3VyeUBtY2dpbGwuY2E=.
The studies involving human participants were reviewed and approved by the ethics review board of l'Institut Philippe-Pinel de Montréal and McGill University. The patients/participants provided their written informed consent to participate in this study.
Written informed consent was obtained from all individual participants included in the study.
CS, BK, and EP-G conducted the literature searches and designed the study. EP-G aided in the study design, collected data, and contributed to editing the final manuscript. MP, MF, VM, and AW aided in analyzing the data and creating the tables as well as the writing and editing of the manuscript. BK supported the study design and provided feedback on the final manuscript. All authors have approved the final version of the manuscript for submission.
We would like to acknowledge the financial support of the Pinel Foundation and the Ordre Régional des Infirmières et Infirmiers de Montréal/Laval (ORIIML).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank Kimberly Carrière for her support with data collection, Marim Ibrahim for her work on data imputation, as well as Samsith So and Paul Pelletier for facilitating the program.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2020.614409/full#supplementary-material
1. Kabat-Zinn J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness. New York, NY: Delta (1990).
2. Auty KM, Cope A, Liebling A. A systematic review and meta-analysis of yoga and mindfulness meditation in prison. Int J Offender Ther Comp Criminol. (2017) 61:689–710. doi: 10.1177/0306624x15602514
3. Bishop SR, Lau M, Shapiro S, Carlson L, Anderson ND, Carmody J, et al. Mindfulness: a proposed operational definition. Clin Psychol. (2004) 11:230–41. doi: 10.1093/clipsy.bph077
4. Teasdale JD, Segal Z, Williams JMG. How does cognitive therapy prevent depressive relapse and why should attentional control (mindfulness) training help? Behav Res Ther. (1995) 33:25–39. doi: 10.1016/0005-7967(94)e0011-7
5. Salmon P, Lush E, Jablonski M, Sephton SE. Yoga and mindfulness: clinical aspects of an ancient mind/dody practice. Cogn. Behav. Practice. (2009) 16:59–72. doi: 10.1016/j.cbpra.2008.07.002
6. Keng SL, Smoski MJ, Robins CJ. Effects of mindfulness on psychological health: a review of empirical studies. Clin Psych Rev. (2011) 31:1041–56. doi: 10.1016/j.cpr.2011.04.006
7. Khoury B, Lecomte T, Fortin G, Masse M, Therien P, Bouchard V, et al. Mindfulness-based therapy: a comprehensive meta-analysis. Clin Psychol Rev. (2013) 33:763–71. doi: 10.1016/j.cpr.2013.05.005
8. Khoury B, Lecomte T, Gaudiano BA, Paquin K. Mindfulness interventions for psychosis: A meta-analysis. Schizoph Res. (2013) 150:176–84. doi: 10.1016/j.schres.2013.07.055
9. Brown RP, Gerbarg PL. Sudarshan kriya yogic breathing in the treatment of stress, anxiety, and depression. Part II - clinical applications and guidelines J Altern Compl Med. (2005) 11:711–7. doi: 10.1089/acm.2005.11.711
10. Meyer HB, Katsman A, Sones AC, Auerbach DE, Ames D, Rubin RT. Yoga as an ancillary treatment for neurological and psychiatric disorders: a review. J Neuropsych Clin Neurosci. (2012) 24:152–64. doi: 10.1176/appi.neuropsych.11040090
11. Prathikanti S, Rivera R, Cochran A, Tungol JG, Fayazmanesh N, Weinmann E. Treating major depression with yoga: a prospective, randomized, controlled pilot trial. PLoS ONE. (2017) 12:e0173869. doi: 10.1371/journal.pone.0173869
12. Latimer J, Lawrence A. The Review Board Systems in Canada: An Overview of Results From the Mentally Disordered Accused Data Collection Study. (2006). Research report. Department of Justice of Canada. Available online at: https://www.justice.gc.ca/eng/rp-pr/csj-sjc/jsp-sjp/rr06_1/index.html. Accessed 21 October 2019.
13. Askola R, Nikkonen M, Paavilainen E, Soininen P, Putkonen H, Louheranta O. Forensic psychiatric patients' perspectives on their care: a narrative view. Perspect PsychiatrCare. (2018) 54:64–73. doi: 10.1111/ppc.12201
14. Howells K, Tennant A, Day A, Elmer R. Mindfulness in forensic mental health: does it have a role? Mindfulness. (2010) 1:4–9. doi: 10.1007/s12671-009-0001-x
15. Crocker AG, Nicholls TL, Seto MC, Charette Y, Cote G, Caulet M. The national trajectory project of individuals found not criminally responsible on account of mental disorder in Canada. Part 2: The people behind the label. Canad J Psychiatry(2015) 60:106–16. doi: 10.1177/070674371506000305
16. Dafoe T, Stermac L. Mindfulness meditation as an adjunct approach to treatment within the correctional system. J Offend Rehabil. (2013) 52:198–216. doi: 10.1080/10509674.2012.752774
17. Ferszt GG, Miller RJ, Hickey JE, Maull F, Crisp K. The impact of a mindfulness based program on perceived stress, anxiety, depression and sleep of incarcerated women. Int J Environ Res Public Health. (2015) 12:11594–607. doi: 10.3390/ijerph120911594
18. Himelstein S. Meditation research: the state of the art in correctional settings. Int J Offender Ther Compar Criminol. (2011) 55:646–61. doi: 10.1177/0306624x10364485
19. Lyons T, Womack VY, Cantrell WD, Kenemore T. Mindfulness-based relapse prevention in a jail drug treatment program. Subst Use Misuse. (2019) 54:57–64. doi: 10.1080/10826084.2018.1491054
20. Perelman AM, Miller SL, Clements CB, Rodriguez A, Allen K, Cavanaugh R. Meditation in a deep south prison: a longitudinal study of the effects of vipassana. J Offender Rehab. (2012) 51:176–98. doi: 10.1080/10509674.2011.632814
21. Samuelson M, Carmody J, Kabat-Zinn J, Bratt MA. Mindfulness-based stress reduction in Massachusetts correctional facilities. Prison J. (2007) 87:254–68. doi: 10.1177/0032885507303753
22. Shonin E, Van Gordon W, Slade K, Griffiths MD. Mindfulness and other Buddhist-derived interventions in correctional settings: A systematic review. Aggression and Violent Behavior. (2013) 18:365–72. doi: 10.1016/j.avb.2013.01.002
23. Ashcroft K, Barrow F, Lee R, MacKinnon K. Mindfulness groups for early psychosis: a qualitative study. Psychol Psychoth. (2012) 85:327–34. doi: 10.1111/j.2044-8341.2011.02031.x
24. Chadwick P. Mindfulness for psychosis. Br J Psychiatry. (2014) 204:333–4. doi: 10.1192/bjp.bp.113.136044
25. Khoury B, Lecomte T, Comtois G, Nicole L. Third-wave strategies for emotion regulation in early psychosis: a pilot study. Early Interv Psychiatry. (2015) 9:76–83. doi: 10.1111/eip.12095
26. Nikolitch K, Laliberte V, Yu C, Strychowsky N, Segal M, Looper KJ, et al. Tolerability and suitability of brief group mindfulness-oriented interventions in psychiatric inpatients: a pilot study. Int J Psychiatry Clin Practice. (2016) 20:170–4. doi: 10.1080/13651501.2016.1197276
27. Tong AC, Lin JJ, Cheung VY, Lau NK, Chang WC, Chan SK, et al. A low-intensity mindfulness-based intervention for mood symptoms in people with early psychosis: development and pilot evaluation. Clin Psychol Psychoth. (2016) 23:550–60. doi: 10.1002/cpp.1981
28. Per M, Spinelli C, Sadowski I, Schmelefske E, Anand L, Khoury B. Evaluating the effectiveness of mindfulness-based interventions in incarcerated populations: a meta-analysis. Crim Justice Behav. (2019) 40:1–21. doi: 10.1177/0093854819891457
29. Malouf ET, Youman K, Stuewig J, Witt EA, Tangney JP. A pilot RCT of a values-based mindfulness group intervention with jail inmates: evidence for reduction in post-release risk behavior. Mindfulness. (2017) 8:603–14. doi: 10.1177/s12671-016-0636-3
30. Abba N, Chadwick P, Stevenson C. Responding mindfully to distressing psychosis: A grounded theory analysis. Psychoth Res. (2008) 18:77–87. doi: 10.1080/10503300701367992
31. Chadwick P, Taylor KN, Abba N. Mindfulness groups for people with psychosis. Behav Cogn Psychoth. (2005) 33:351–9. doi: 10.1017/S1352465805002158
32. Singh NN, Lancioni GE, Winton AS, Singh AN, Adkins AD, Singh J. Clinical and benefit–cost outcomes of teaching a mindfulness-based procedure to adult offenders with intellectual disabilities. Behav Modif. (2008) 32:622–37. doi: 10.1177/0145445508315854
33. Singh NN, Lancioni GE, Winton ASW, Singh AN, Adkins AD, Singh J. Can adult offenders with intellectual disabilities use mindfulness-based procedures to control their deviant sexual arousal? Psychol Crime Law. (2011) 17:165–79. doi: 10.1080/10683160903392731
34. Sistig B, Friedman SH, McKenna B, Consedine NS. Mindful yoga as an adjunct treatment for forensic inpatients: a preliminary evaluation. J Foren Psychiatry Psychol. (2015) 26:824–46. doi: 10.1080/14789949.2015.1062996
35. Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment. (2006) 13:27–45. doi: 10.1177/1073191105283504
36. Heeren A, Douilliez C, Peschard V, Debrauwere L, Philippot P. Cross-cultural validity of the five facets mindfulness questionnaire: adaptation and validation in a French-speaking sample. Europ Rev Appl Psychol. (2011) 61:147–51. doi: 10.1016/j.erap.2011.02.001
37. Cash M, Whittingham K. What facets of mindfulness contribute to psychological well-being and depressive, anxious, and stress-related symptomatology? Mindfulness. (2010) 1:177–82. doi: 10.1007/s12671-010-0023-4
38. Bruchon–Schweitzer M. Psychologie de la santé: Modèles, concepts et méthodes. Paris, France: Dunod (2002).
39. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
40. Lesage FX, Berjot S, Deschamps F. Psychometric properties of the French versions of the perceived stress scale. Int J Occupat Med Environ Health. (2012) 25:178–84. doi: 10.2478/s13382-012-0024-8
41. Garnefski N, Kraaij V. The cognitive emotion regulation questionnaire: psychometric features and prospective relationships with depression and anxiety in adults. Europ J Psychol Assess. (2007) 23:141–9. doi: 10.1027/1015-5759.23.3.141
42. Jermann F, Van der Linden M, d'Acremont M, Zermatten A. Cognitive emotion regulation questionnaire (CERQ): confirmatory factor analysis and psychometric properties of the French translation. Europ J Psychol Assess. (2006) 22:126–31. doi: 10.1027/1015-5759.22.2.126
43. JASP Team. JASP (Version 0.14) [Computer software] (2020). Retrieved from: https://jasp-stats.org/
44. An Y, Zhou Y, Huang Q, Jia K, Li W, Xu W. The effect of mindfulness training on mental health in long-term Chinese male prisoners. Psychol Health Med. (2019) 24:167–76. doi: 10.1080/13548506.2018.1510130
45. Day A. Offender emotion and self-regulation: implications for offender rehabilitation programming. Day A. Offender emotion and self-regulation: implications for offender rehabilitation programming. Psychol. Crime Law. (2009) 15:119–30. doi: 10.1080/10683160802190848
46. Sistig B, Lambrecht I, Friedman SH. Journey back into body and soul – an exploration of mindful yoga with psychosis. Psychosis. (2015) 7:25–36. doi: 10.1080/17522439.2014.885556
Keywords: mindfulness, yoga, forensic inpatients, stress, cognitive and emotion regulation
Citation: Spinelli C, Paradis-Gagné E, Per M, Fleischmann MH, Manova V, Wallace A and Khoury B (2020) Evaluating the Use of Mindfulness and Yoga Training on Forensic Inpatients: A Pilot Study. Front. Psychiatry 11:614409. doi: 10.3389/fpsyt.2020.614409
Received: 06 October 2020; Accepted: 19 November 2020;
Published: 10 December 2020.
Edited by:
Johann Brink, University of British Columbia, CanadaReviewed by:
Märta Wallinius, Lund University, SwedenCopyright © 2020 Spinelli, Paradis-Gagné, Per, Fleischmann, Manova, Wallace and Khoury. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christina Spinelli, Y2hyaXN0aW5hLnNwaW5lbGxpQG1haWwubWNnaWxsLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.