
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 14 December 2020
Sec. Mood Disorders
Volume 11 - 2020 | https://doi.org/10.3389/fpsyt.2020.593629
This article is part of the Research Topic Mechanisms Underlying Mood Disorders View all 12 articles
 Liangfeng Kuang1
Liangfeng Kuang1 Dong Cui1
Dong Cui1 Qing Jiao1*
Qing Jiao1* Yongxin Guo1
Yongxin Guo1 Weifang Cao1Weijia Gao2
Weifang Cao1Weijia Gao2 Jianfeng Qiu1Linyan Su3Guangming Lu4
Jianfeng Qiu1Linyan Su3Guangming Lu4Introduction: It remains unknown whether volumetric alterations of ventricles are similar or not in pediatric bipolar disorder (PBD) among different mood states. The present study aims to estimate ventricular volumetric alteration of PBD patients in manic and euthymic status, as well as the relationship between this alteration and cognitive changes.
Methods: T1 magnetic resonance images were obtained from 20 manic PBD patients, 21 euthymic PBD patients, and 19 healthy controls (HCs). Ventricular volumes were automatically obtained via FreeSurfer 6.0 software. Ventricular volumes and cognitive indices were compared among the three groups, and the relationship between ventricular volumes and cognitive/clinical indices was analyzed.
Results: In contrast to HCs, manic and euthymic PBD patients exhibited decreased cognitive scores of the Stroop color-word test and the digit span subtest. Manic PBD subjects presented enlarged volumes in the bilateral ventricles, third ventricle, and whole ventricles, and euthymic PBD participants displayed increased volumes in the third ventricle, fourth ventricle, and whole ventricles. No significant differences in cognitive performance and ventricular volumes were found between PBD groups. No significant correlation was discovered between ventricular volumes and cognitive/clinical indices in both manic and euthymic PBD patients.
Conclusions: No significant differences in cognitive performance and ventricle volume were observed between euthymic and manic PBD groups, which may imply that the alterations are not specific to mood state. It may indicate structural and functional damage of corresponding brain circuits in euthymic PBD patients similar with that of manic PBD, which may provide clues to the diagnosis and treatment of euthymic PBD.
Pediatric bipolar disorder (PBD) is a severe psychiatric illness that recurrently attacks patients, marked by manic or hypomanic depressed episodes, and separated by euthymic periods. Manic PBD can feature extreme joy or rage, full vigorousness and inattention, difficultly falling asleep and reduced sleep needs, and racing thoughts and increased speech, while depressed PBD is characterized by inattention and suicidal tendencies, increased sleep needs, and emotional instability, and euthymic PBD generally shows no clinical psychiatric manifestations. With heritability of about 59% (1), bipolar disorder (BD) is reported to relate with considerably high prevalence and psychiatric comorbidity rate (2), high risk of suicide (3), and impaired cognition (4).
It has been found that BD patients exhibit alterations of ventricular volume (5). Some studies reported enlarged lateral ventricular volume in adult BD patients (6–10), while other researchers reported no difference in lateral ventricular volume between adult BD patients and healthy controls (HCs) (11, 12). Most studies have focused on ventricles' alterations in one mood state of BD. In the manic state, the third and lateral ventricle volumes in the first episode of adult BD (13) and the cerebral ventricular size in young male BD patients were shown to be increased (14). In euthymic adult BD, the width of the third ventricle exhibited an increase (15). Nevertheless, different results have also been reported, such as finding no lateral ventricle volume alteration in euthymic and manic BD adults (16–18). One study compared the width of the third ventricle in depressed, manic, and euthymic adult BD type I (BD I), and the researchers found increased width of the third ventricle in BD patients. No width difference of the third ventricle was displayed among the three patient groups (19). Several studies focused on ventricles in PBD and found increased lateral ventricle volume (20), enlarged lateral ventricles, and ventricle asymmetry in manic PBD subjects (21). The ratio of ventricle cerebrospinal fluid to cerebral total tissue volume, showing no difference between PBD and HCs, has also been reported (22). The above studies mostly involved one mood state of BD and have only reported alteration of the lateral and third ventricles. However, the difference in ventricular volume among different mood states and the relationship between ventricular volume alteration and cognitive tests remains unknown in PBD.
In the current study, we aimed to investigate alterations of the ventricular volumes of PBD patients in manic and euthymic states. According to prior research, we hypothesized that the volumes of four ventricles would be larger in PBD patients than those of the HCs. The current study was designed to: (1) evaluate cognitive functions of the three groups; (2) compare volumes of the left lateral ventricle, right lateral ventricle, third ventricle, fourth ventricle, and whole ventricles (adding bilateral ventricles, third ventricle, and fourth ventricle) among the three groups; (3) evaluate left lateral ventricle-to-brain ratio (LLVBR), right lateral ventricle-to-brain ratio (RLVBR), third ventricle-to-brain ratio (TVBR), fourth ventricle-to-brain ratio (FVBR), and whole ventricle-to-brain ratio (WVBR) among the three groups; and (4) conduct a correlation analysis between ventricular volumes with cognitive and clinical variables.
In the current study, 60 subjects were enrolled, including 20 manic PBD patients, 21euthymic PBD patients, and 19 age- and gender-matched HCs. All of the PBD patients were recruited from the clinical psychiatric department in the Second Xiangya Hospital of Central South University, while HCs were enlisted via advertisement. This study was conducted from January 2012 to July 2014.
The inclusion criteria of PBD patients were: (a) having met the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM-IV) criteria for BD with current manic and euthymic episodes; (b) manic PBD conformed to hypomania (≥4 days) or mania (≥7 days) and euthymic PBD patients were needed to have experienced a remission period for more than four consecutive weeks prior to the study; (c) 10–18 years old; and (d) right-handedness.
Exclusion criteria for all of the subjects were: (a) score of intelligence quotient (IQ) <80; (b) contraindications for MRI scanning, including the presence of a pacemaker, artificial metal heart valves, aneurysm clip, other foreign metal matter in the body, or claustrophobia; (c) history of alcohol or substance abuse in the 2 months prior to the study; (d) history of cranial trauma; and (e) other psychiatric illnesses, including schizophrenia, attention-deficit hyperactivity disorder, or anxiety disorder.
The study obtained approval from the Ethics Committee of the Second Xiangya Hospital of Central South University. All of the participants and at least one parent or legal guardian signed informed consent documents.
The children and at least one parent or legal guardian were assessed employing Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL) (23) by clinical interviews. The diagnosis of PBD was carried out by two senior child psychiatrists who had extensive clinical experience of diagnosis in PBD. Demographic, clinical, and neurocognitive information was collected for all subjects. Clinical scales, including IQ, Young Mania Rating Scale (YMRS), Mood and Feelings Questionnaire (MFQ) scores, onset age, illness duration, and onset frequency, were recorded. YMRS (24) and MFQ (25) were used to evaluate the severity of manic and depressive symptoms, respectively.
Cognitive functions were measured by Stroop color-word test (SCWT), trail making test (TMT), and digit span subtest (DST). SCWT was utilized to examine processing speed, perceptual conversion, selective attention, and inhibition of habitual response patterns and sensibility for plasticity of mental control and response (26, 27). SCWT fell into three categories: word reading test (SCWT-A), color naming test (SCWT-B), and color word interference (SCWT-C). In SCWT-A, the subjects were asked to name the word printed on a white piece of paper (e.g., the word “red” printed in black) as quickly as possible. In SCWT-B, words printed in three colors were presented (e.g., “red” printed in red), and the subjects were asked to name the color as quickly as possible. In SCWT-C, the subjects were asked to name the color of words whose meanings were different from the ink color (e.g., “blue” printed in red) as quickly as possible, while trying to ignore the meaning of the word. Participants were requested to finish every test within 45 s, and the number of correct answers was recorded as the SCWT score. TMT was used to assess the participants' abilities in mental processing speed, attention, cognitive order, spatial perception, eye and hand coordination, and flexibility in thinking. TMT was divided into TMT-A and TMT-B. In TMT-A, 25 consecutive numbers surrounded by circles were randomly shown on a paper, and subjects were asked to sequentially connect each circle in ascending order (e.g., 1-2-3…) as quickly as possible. In TMT-B, 25 consecutive numbers and 25 letters enclosed by circles were randomly displayed on a piece of paper, and participants were asked to alternately link every circle by numerical ascending order and alphabetical order (e.g., 1-a-2-b-3-c…). The score of TMT was the time taken to complete the task. DST is a part of the Wechsler scale of intelligence and it is utilized to test short-term memory attention, concentration, and memory. It includes forward DST (DST-F) and backward DST (DST-B). The subjects were required to repeat a series of random numbers from 1–9 in sequential order (DST-F) and in reverse order (DST-B) after hearing them. The DST score was recorded as the maximum number of digits that the subject was able to repeat correctly.
For the study, MRI scans were conducted using a Siemens 3.0T Trio scanner (Siemens, Munich, Germany). During the MRI scanning, foam pads were placed on two sides of the heads of the subjects to restrict head motion, and cotton earplugs were used to reduce noise and protect the hearing of the subjects. Every subject was requested to stay awake with eyes closed and not to think specific thoughts during the MRI scan. T1-weighted images were obtained by employing three-dimensional magnetization-prepared rapid acquisition gradient echo (3D MPRAGE) protocol. Acquisition parameters covering the whole brain included: repetition time (TR) = 2,300 ms, echo time (TE) = 2.98 ms, inversion time = 900 ms, thickness = 1 mm, gap = 0 mm, field of view (FOV) = 256 mm × 256 mm, matrix = 256 × 256, and flip angle = 9°.
T1-weighted images were processed by FreeSurfer 6.0 software (http://surfer.nmr.mgh.harvard.edu/). Ventricular volumes and total intracranial volume (TIV) were obtained by recon stream (“recon-all”). The procedure included steps such as: (a) Motion correction was performed to reduce the effect of head movement during scanning; (b) Skull stripping was conducted to remove the skull and extract the brain; (c) Talairach transformation was carried out for affine transformation from the original volume to the MNI305 atlas; (d) Intensity normalization was conducted to reduce the intensity difference in the same tissue due to a non-uniform magnetic field or other factors; (e) The brain was divided into gray matter, white matter, and cerebrospinal fluid (CSF); and (f) A transform was created in linear transform array format. In addition, the tessellation of the boundary was conducted between white and gray matter. To ensure proper segmentation of ventricles, a trained physician re-inspected all segmented ventricle borders and corrected them manually, if required. The volumes of five ventricles, namely, the bilateral ventricles, third ventricle, fourth ventricle, and whole ventricles, were used for analysis in the current study. Ventricle-to-brain ratio (VBR) was the value of dividing ventricle volume by TIV, and then multiplying by 100 (22). LLVBR, RLVBR, TVBR, FVBR, and WVBR were calculated for each subject.
Statistical analysis was conducted using IBM SPSS (version 25.0, Armonk, NY, United States). The Pearson chi-square test was employed to evaluate categorical variables, including gender, psychotic symptoms, BD subtype, and familial BD history. Parametric tests were used when data satisfied both normal distribution and homogeneity of variance at the same time. When data did not satisfy normal distribution or homogeneity of variance, non-parametric tests were used. Shapiro-Wilk test and Levene's test were used to assess the normality of distribution and homogeneity of variance.
Age and gender were deemed as covariates in the comparison of cognitive variables and VBR. TIV, age, and gender were considered as covariates in the comparison of ventricular volumes. One-way ANCOVA or Kruskal-Wallis H test was applied for comparison of cognitive variables, ventricular volumes, and VBR among the three groups. False discovery rate (FDR) correction (http://www.sdmproject.com/utilities/?show=FDR) was used in the comparison of the main effects. Two-sample t-test or Kruskal–Wallis H test was employed for post hoc analysis and Bonferroni correction was used for correction of multiple comparisons. Because the sample size in each group was relatively small, statistical power (Cohen's d) was provided to show differences between the PBD patients and the HCs. Pearson correlation analysis was employed to assess correlations between ventricular volumes and cognitive and clinical indices, with age, gender, and TIV as covariates. Significant level for all of the analyses was set as p < 0.05. Normal distributed data were expressed as mean ± standard, and non-normal distributed data were reported as median and inter-quartile range [M(QU-QL)].
As shown in Table 1, there was no significant difference among the three groups in gender, age, education, IQ, or MFQ scores. YMRS scores showed a significant difference among the three groups. No significant difference was found between manic and euthymic patients in onset age, illness duration, onset frequency, psychotic symptoms, BD subtype, and familial BD history.
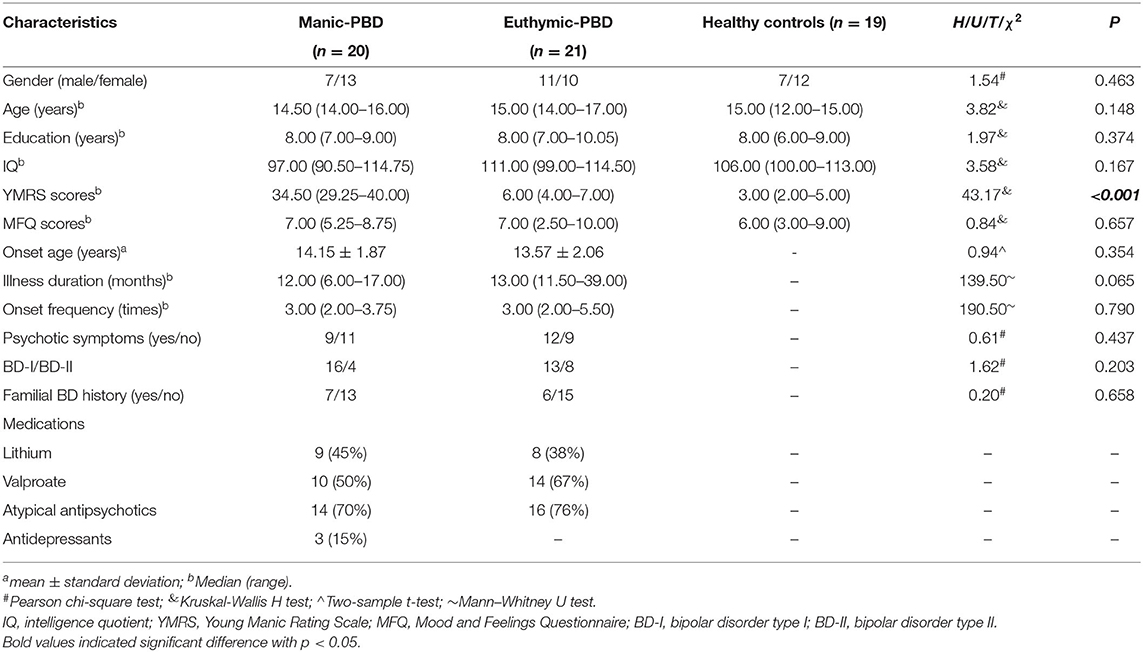
Table 1. Demographic and clinical information of the participants.
As shown in Table 2, significant differences of cognitive variables among the three groups were found in SCWT-A, SCWT-B, SCWT-C, and DST-B. In comparison with the HCs group, the manic group and the euthymic group presented reductions of score in SCWT-A, SCWT-B, SCWT-C, and DST-B.
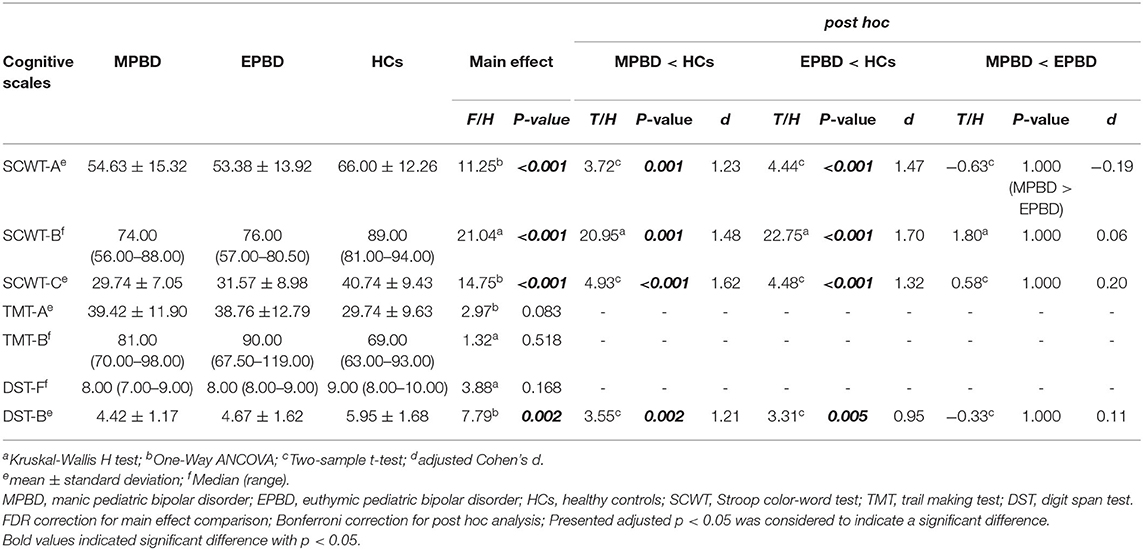
Table 2. Cognitive variables in Manic-PBD, Euthymic-PBD, and Healthy controls.
As shown in Table 3, significant differences of ventricular volumes among the three groups were found in five ventricles, namely, the left lateral ventricle, right lateral ventricle, third ventricle, fourth ventricle, and whole ventricles. In comparison with the HCs group, the manic group presented enlarged volumes in the left lateral ventricle, right lateral ventricle, third ventricle, and whole ventricles, and the euthymic group displayed increased volumes in the third ventricle, fourth ventricle, and whole ventricles. No difference in ventricle volume was found between the manic and euthymic PBD patients.

Table 3. Ventricular volumes in Manic-PBD, Euthymic-PBD, and Healthy controls.
As shown in Table 4, no significant difference of VBR among the three groups was found in five ratios: LLVBR, RLVBR, TVBR, FVBR, and WVBR.
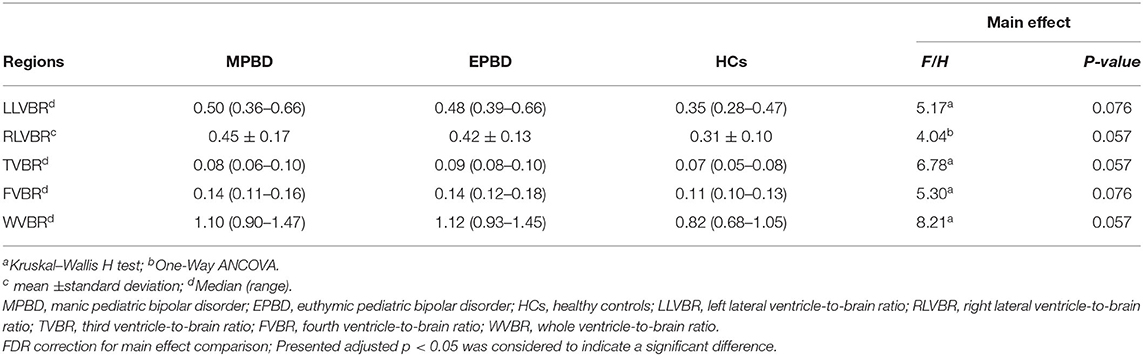
Table 4. Ventricle-to-brain ratio in Manic-PBD, Euthymic-PBD, and Healthy controls.
Pearson correlation analysis was performed between ventricular volumes with clinical and cognitive indices. No significant correlation (p > 0.05) was found between ventricular volumes or VBR with clinical and cognitive indices in either the manic PBD groups or euthymic PBD groups.
In the current study, cognitive function and brain ventricle volumes were evaluated among manic PBD patients, euthymic PBD patients, and healthy adolescents. When compared with HCs, the manic and euthymic PBD patients showed decreased scores of SCWT and DST-B. In terms of ventricle volume comparison, larger bilateral ventricle volumes in the manic PBD group, larger fourth ventricle volume in the euthymic PBD group, and enlarged third ventricle and whole ventricle volumes were found in both PBD groups.
In the current study, the manic as well as euthymic PBD patients exhibited significant impairment in cognitive tests compared with the HCs. The damage in cognition included poor performance in tests of processing speed, concentration and attention, working memory, and executive function. Specifically, the manic and euthymic PBD patients performed worse on SCWT and DST-B compared with the HCs. SCWT is a test of processing speed, cognitive flexibility, and response inhibition. Deficits of SCWT may imply that the manic and euthymic PBD subjects were damaged in brain areas such as the anterior cingulate cortex, dorsolateral prefrontal cortex, lingual gyrus, and extrastriate cortex, which are involved in executive control, speed of color processing, and word-form processing (28). Current results were in line with those of a previous study, that showed poorer performance of SCWT was discovered in PBD patients than in HCs (29). DST is a test of attention and concentration. A prior study found that DST-B of BD was obviously different than HCs, while no difference was displayed in DST-F between adult BD and HCs (30). Impairment of executive function was found in the manic, depressive, and euthymic BD I patients, including initial reaction, inhibition control, and strategic thinking (31). It had been reported that euthymic PBD patients exhibited impairment of cognitive functions, including verbal learning and working memory (32). That more severe damage of the DST-B in PBD patients than that of the HCs shown in the current study suggests a related dysfunction of executive control of phonological information in the manic and euthymic PBD patients. It is worth noting that manic and euthymic PBD patients exhibited similar cognitive damage, and no significant difference in SCWT and DST was found between the two groups. This may imply that although euthymic PBD patients expressed relatively stable mood states, they had cognitive impairment similar to that of manic patients, indicating impairment of brain structures and function in related cognitive circuits in euthymic PBD patients.
Bilateral ventricles' volumes were found to be increased in manic PBD compared to those of HCs in the study. No significant difference of lateral ventricles' volumes was found between euthymic patients and HCs, or between euthymic and manic patients. Similar results were reported in a study of adult BD, which showed the larger lateral ventricular volumes were related to the number of manic episodes in adult BD (10). It had been shown that patients with 22q11.2 deletion syndrome (22q11DS) exhibited enlarged lateral ventricle volumes compared with HCs (33). The 22q11DS, which affected multiple genes involved in neurodevelopment, was also reported to be related with early-onset BD (34). This may imply that the 22q11DS is a genetic risk factor for BD. In animal experiments with mice, ongoing dysregulation of neural cell adhesion molecules in neuropsychiatric disorders led to an increase in lateral ventricular volumes, and affected cognitive function via learning, synaptic plasticity, and long-term potentiation influences (35).
Concerning the third ventricle, we found that third ventricular volume in manic and euthymic PBD patients was larger than that of the HCs, and that third ventricle volume was not an obvious discrepancy between manic and euthymic patients. The result in PBD was not in line with that of previous studies in which adult BD patients were grouped into those with and without psychotic forms, and enlarged third ventricle volume was only discovered in psychotic BD patients (36). Increased third volume may be related to the surrounding anatomical boundary, such as decreased volumes of the thalamus and hypothalamus (5). In post-mortem BD research, total selective neurons robustly decreased by about 50% in the paraventricular nucleus of hypothalamus (37). In other ongoing research, we found a decrease of thalamic volume in the same PBD samples, matching the increased third ventricular volumes in the current study.
We found that the fourth ventricle of euthymic PBD was markedly greater than that of HCs. The shape and size of the fourth ventricle was believed to be influenced by the surrounding brainstem structure. The variation of CACNA1C gene was reported to increase the risk of mental diseases, particularly BD, and to affect brainstem volume (38). Few previous studies focused on the volume of the fourth ventricle in PBD. However, two studies reported larger volumes of the fourth ventricle in schizophrenia (39, 40). To some extent, previous findings elucidated that BD and schizophrenia partially shared heritability and showed some similar clinical features (1, 41, 42). In mental disorders, the region of the brainstem reticular activating system may play an essential role in supporting attention, but it was easily influenced by environmental and genetic influences, and these influences may be the etiology of attention impairment (43, 44). These research studies disclosed that impaired subcortical structures near the fourth ventricle likely indicated pathophysiology of sustained inattention in psychiatric disorders. Considering that euthymic PBD patients also show daily clinical presentation of inattention, the increased fourth ventricular volume exhibited in the current study may indirectly indicate a similar inattention mechanism in euthymic PBD with that of schizophrenia.
In the current study, increased whole ventricular volumes were found in manic and euthymic PBD patients compared to those of HCs. The differences in RLVBR, TVBR, and WVBR among the three groups closely reached statistical significance and the three ratios in manic and euthymic PBD patients were larger than those of the HCs, as shown in Table 4. Previous studies found increased LVBR in older BD patients (45) or else no alterations of LVBR and TVBR in adult BD patients (46). Nevertheless, two studies did not find the volumetric alteration of ventricles in adult BD (47, 48). The underlying mechanisms for BD seemed different in adults and children (49). Our results regarding whole ventricular volume and VBR provided more clues in the field of PBD.
Several limitations should be acknowledged in the current study. First, the sample size of our study was relatively small, which may cause an inability to observe some subtle changes in the ventricular volume or significant correlations between alterations of ventricular volume and cognitive and clinical indices. In our future work, much more data will be extracted to make the study more convincing. Second, medical treatment was a potential obstruction in interpreting the present results. Some studies, however, reported no significant effect of medication in behavioral (50) and neural differences between patients and HCs (51). Third, the ventricular volume corrected by the two methods in the present study, that is, the regression-based residuals in calculating brain volume (the residual method, Table 3) and the region-to-ICV ratio (the proportion method, Table 4), were different. After FDR correction, the significant differences in VBR among the three groups disappeared. This may be due to the influence of random errors, which were combined in the numerator and denominator, and then the sources of the error were hidden in the final ratio values (52). In future work, some improvement may be needed to reduce the influence of the random errors.
In the current study, enlarged ventricle volumes were found in manic and euthymic PBD patients compared with those of HCs, which may provide some new clues to brain structural impairment of child and adolescent BD patients. No significant difference of cognitive performance and ventricle volume was observed between manic and euthymic PBD patients, which may imply that the alterations are not specific to mood state. However, when in remission, euthymic PBD patients behaved with similar abnormalities in cognition and ventricle volume as the manic patients, which may indicate damage of the brain structure and function of corresponding brain circuits in euthymic PBD patients.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of the Second Xiangya Hospital of Central South University. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
QJ and GL: conception and study design. WG and LS: data collection or acquisition and clinical support. DC and LK: statistical analysis. YG and JQ: interpretation of results. LK and WC: drafting the manuscript or revising it critically for important intellectual content. All authors: approval of the final version to be published and agreement to be accountable for the integrity and accuracy of all aspects of the work. All authors contributed to the article and approved the submitted version.
The present work was supported by the Funds for the National Natural Science Foundation of China (81371531 to Qing Jiao; 81901730 to Weifang Cao), Science and Technology Project of the Education Department of Shandong Province (J18KA262 to Weifang Cao), High-level cultivation program of Shandong First Medical University & Shandong Academy of Medical Sciences (2017GCC11 to Weifang Cao), Taishan Scholars Program of Shandong Province (TS201712065 to Jianfeng Qiu), and the Academic promotion programme of Shandong First Medical University (2019QL009).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors would like to thank all of the participants who took part in the current study and the experts at the Magnetic Resonance Center of Hunan Provincial People's Hospital for providing scan time and technical assistance.
1. Lichtenstein P, Yip BH, Bjork C, Pawitan Y, Cannon TD, Sullivan PF, et al. Common genetic determinants of schizophrenia and bipolar disorder in Swedish families: a population-based study. Lancet. (2009) 373:234–9. doi: 10.1016/S0140-6736(09)60072-6
2. Frias A, Palma C, Farriols N. Comorbidity in pediatric bipolar disorder: prevalence, clinical impact, etiology and treatment. J Affect Disord. (2015) 174:378–89. doi: 10.1016/j.jad.2014.12.008
3. Goldstein TR. Suicidality in pediatric bipolar disorder. Child Adolesc Psychiatr Clin N Am. (2009) 18:339–52, viii. doi: 10.1016/j.chc.2008.11.005
4. Martinez-Aran A, Vieta E, Reinares M, Colom F, Torrent C, Sanchez-Moreno J, et al. Cognitive function across manic or hypomanic, depressed, and euthymic states in bipolar disorder. Am J Psychiatry. (2004) 161:262–70. doi: 10.1176/appi.ajp.161.2.262
5. Beyer JL, Krishnan KR. Volumetric brain imaging findings in mood disorders. Bipolar Disord. (2002) 4:89–104. doi: 10.1034/j.1399-5618.2002.01157.x
6. Arnone D, Cavanagh J, Gerber D, Lawrie SM, Ebmeier KP, McIntosh AM. Magnetic resonance imaging studies in bipolar disorder and schizophrenia: meta-analysis. Br J Psychiatry. (2009) 195:194–201. doi: 10.1192/bjp.bp.108.059717
7. Kempton MJ, Geddes JR, Ettinger U, Williams SC, Grasby PM. Meta-analysis, database, and meta-regression of 98 structural imaging studies in bipolar disorder. Arch Gen Psychiatry. (2008) 65:1017–32. doi: 10.1001/archpsyc.65.9.1017
8. Nakamura M, Salisbury DF, Hirayasu Y, Bouix S, Pohl KM, Yoshida T, et al. Neocortical gray matter volume in first-episode schizophrenia and first-episode affective psychosis: a cross-sectional and longitudinal MRI study. Biol Psychiatry. (2007) 62:773–83. doi: 10.1016/j.biopsych.2007.03.030
9. McDonald C, Zanelli J, Rabe-Hesketh S, Ellison-Wright I, Sham P, Kalidindi S, et al. Meta-analysis of magnetic resonance imaging brain morphometry studies in bipolar disorder. Biol Psychiatry. (2004) 56:411–7. doi: 10.1016/j.biopsych.2004.06.021
10. Strakowski SM, DelBello MP, Zimmerman ME, Getz GE, Mills NP, Ret J, et al. Ventricular and periventricular structural volumes in first- versus multiple-episode bipolar disorder. Am J Psychiatry. (2002) 159:1841–7. doi: 10.1176/appi.ajp.159.11.1841
11. Brambilla P, Harenski K, Nicoletti M, Mallinger AG, Frank E, Kupfer DJ, et al. MRI study of posterior fossa structures and brain ventricles in bipolar patients. J Psychiatr Res. (2001) 35:313–22. doi: 10.1016/S0022-3956(01)00036-X
12. Lim KO, Rosenbloom MJ, Faustman WO, Sullivan EV, Pfefferbaum A. Cortical gray matter deficit in patients with bipolar disorder. Schizophr Res. (1999) 40:219–27. doi: 10.1016/S0920-9964(99)00063-8
13. Strakowski SM, Wilson DR, Tohen M, Woods BT, Douglass AW, Stoll AL. Structural brain abnormalities in first-episode mania. Biol Psychiatry. (1993) 33:602–9. doi: 10.1016/0006-3223(93)90098-X
14. Nasrallah HA, McCalley-Whitters M, Jacoby CG. Cerebral ventricular enlargement in young manic males. A controlled CT study. J Affect Disord. (1982) 4:15–9. doi: 10.1016/0165-0327(82)90014-3
15. Cousins DA, Moore PB, Watson S, Harrison L, Ferrier IN, Young AH, et al. Pituitary volume and third ventricle width in euthymic patients with bipolar disorder. Psychoneuroendocrinology. (2010) 35:1074–81. doi: 10.1016/j.psyneuen.2010.01.008
16. Lopez-Jaramillo C, Vargas C, Diaz-Zuluaga AM, Palacio JD, Castrillon G, Bearden C, et al. Increased hippocampal, thalamus and amygdala volume in long-term lithium-treated bipolar I disorder patients compared with unmedicated patients and healthy subjects. Bipolar Disord. (2017) 19:41–9. doi: 10.1111/bdi.12467
17. Arumugham SS, Torres IJ, Lang DJ, Su W, Lam RW, Honer WG, et al. Subcortical structural volumes in recently remitted first episode mania. J Affect Disord. (2017) 222:23–7. doi: 10.1016/j.jad.2017.06.051
18. McDonald WM, Krishnan KR, Doraiswamy PM, Blazer DG. Occurrence of subcortical hyperintensities in elderly subjects with mania. Psychiatry Res. (1991) 40:211–20. doi: 10.1016/0925-4927(91)90013-G
19. Krogias C, Hoffmann K, Eyding J, Scheele D, Norra C, Gold R, et al. Evaluation of basal ganglia, brainstem raphe and ventricles in bipolar disorder by transcranial sonography. Psychiatry Res. (2011) 194:190–7. doi: 10.1016/j.pscychresns.2011.04.002
20. Friedman L, Findling RL, Kenny JT, Swales TP, Stuve TA, Jesberger JA, et al. An MRI study of adolescent patients with either schizophrenia or bipolar disorder as compared to healthy control subjects. Biol Psychiatry. (1999) 46:78–88. doi: 10.1016/S0006-3223(98)00351-5
21. Botteron KN, Vannier MW, Geller B, Todd RD, Lee BC. Preliminary study of magnetic resonance imaging characteristics in 8- to 16-year-olds with mania. J Am Acad Child Adolesc Psychiatry. (1995) 34:742–9. doi: 10.1097/00004583-199506000-00014
22. Chang K, Barnea-Goraly N, Karchemskiy A, Simeonova DI, Barnes P, Ketter T, et al. Cortical magnetic resonance imaging findings in familial pediatric bipolar disorder. Biol Psychiatry. (2005) 58:197–203. doi: 10.1016/j.biopsych.2005.03.039
23. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. (1997) 36:980–8. doi: 10.1097/00004583-199707000-00021
24. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
25. Wood A, Kroll L, Moore A, Harrington R. Properties of the mood and feelings questionnaire in adolescent psychiatric outpatients: a research note. J Child Psychol Psychiatry. (1995) 36:327–34. doi: 10.1111/j.1469-7610.1995.tb01828.x
26. Rivera D, Perrin PB, Stevens LF, Garza MT, Weil C, Saracho CP, et al. Stroop color-word interference test: normative data for the Latin American Spanish speaking adult population. NeuroRehabilitation. (2015) 37:591–624. doi: 10.3233/NRE-151281
27. Baune BT, Air T. Clinical, functional, and biological correlates of cognitive dimensions in major depressive disorder—rationale, design, and characteristics of the cognitive function and mood study (CoFaM-Study). Front Psychiatry. (2016) 7:150. doi: 10.3389/fpsyt.2016.00150
28. Roelofs A, Hagoort P. Control of language use: cognitive modeling of the hemodynamics of Stroop task performance. Brain Res Cogn Brain Res. (2002) 15:85–97. doi: 10.1016/S0926-6410(02)00218-5
29. Karakurt MN, Karabekirogllu MZ, Yuce M, Baykal S, Senses A. [Neuropsychological profiles of adolescents with bipolar disorder and adolescents with a high risk of bipolar disorder]. Turk Psikiyatri Derg. (2013) 24:221–30. doi: 10.5080/u7185
30. Soni A, Singh P, Shah R, Bagotia S. Impact of cognition and clinical factors on functional outcome in patients with bipolar disorder. East Asian Arch Psychiatry. (2017) 27:26–34.
31. Dixon T, Kravariti E, Frith C, Murray RM, McGuire PK. Effect of symptoms on executive function in bipolar illness. Psychol Med. (2004) 34:811–21. doi: 10.1017/S0033291703001570
32. Elias LR, Miskowiak KW, Vale AM, Kohler CA, Kjaerstad HL, Stubbs B, et al. Cognitive impairment in euthymic pediatric bipolar disorder: a systematic review and meta-analysis. J Am Acad Child Adolesc Psychiatry. (2017) 56:286–96. doi: 10.1016/j.jaac.2017.01.008
33. Ching CRK, Gutman BA, Sun D, Villalon Reina J, Ragothaman A, Isaev D, et al. Mapping subcortical brain alterations in 22q11.2 deletion syndrome: effects of deletion size and convergence with idiopathic neuropsychiatric illness. Am J Psychiatry. (2020) 77:589–600. doi: 10.1176/appi.ajp.2019.19060583
34. Aneja A, Fremont WP, Antshel KM, Faraone SV, AbdulSabur N, Higgins AM, et al. Manic symptoms and behavioral dysregulation in youth with velocardiofacial syndrome (22q11.2 deletion syndrome). J Child Adolesc Psychopharmacol. (2007) 17:105–14. doi: 10.1089/cap.2006.0023
35. Vawter MP. Dysregulation of the neural cell adhesion molecule and neuropsychiatric disorders. Eur J Pharmacol. (2000) 405:385–95. doi: 10.1016/S0014-2999(00)00568-9
36. Bhadoria R, Watson D, Danson P, Ferrier IN, McAllister VI, Moore PB. Enlargement of the third ventricle in affective disorders. Indian J Psychiatry. (2003) 45:147–50.
37. Manaye KF, Lei DL, Tizabi Y, Davila-Garcia MI, Mouton PR, Kelly PH. Selective neuron loss in the paraventricular nucleus of hypothalamus in patients suffering from major depression and bipolar disorder. J Neuropathol Exp Neurol. (2005) 64:224–9. doi: 10.1093/jnen/64.3.224
38. Franke B, Vasquez AA, Veltman JA, Brunner HG, Rijpkema M, Fernandez G. Genetic variation in CACNA1C, a gene associated with bipolar disorder, influences brainstem rather than gray matter volume in healthy individuals. Biol Psychiatry. (2010) 68:586–8. doi: 10.1016/j.biopsych.2010.05.037
39. Juuhl-Langseth M, Rimol LM, Rasmussen IA Jr., Thormodsen R, Holmen A, Emblem KE, et al. Comprehensive segmentation of subcortical brain volumes in early onset schizophrenia reveals limited structural abnormalities. Psychiatry Res. (2012) 203:14–23. doi: 10.1016/j.pscychresns.2011.10.005
40. Andreone N, Tansella M, Cerini R, Rambaldelli G, Versace A, Marrella G, et al. Cerebral atrophy and white matter disruption in chronic schizophrenia. Eur Arch Psychiatry Clin Neurosci. (2007) 257:3–11. doi: 10.1007/s00406-006-0675-1
41. Brainstorm C, Anttila V, Bulik-Sullivan B, Finucane HK, Walters RK, Bras J, et al. Analysis of shared heritability in common disorders of the brain. Science. (2018) 360:8757. doi: 10.1126/science.aap8757
42. Cross-Disorder Group of the Psychiatric Genomics C, Lee SH, Ripke S, Neale BM, Faraone SV, Purcell SM. Genetic relationship between five psychiatric disorders estimated from genome-wide SNPs. Nat Genet. (2013) 45:984–94. doi: 10.1038/ng.2711
43. Lindsley DB, Bowden JW, Magoun HW. Effect upon the EEG of acute injury to the brain stem activating system. Electroencephalogr Clin Neurophysiol. (1949) 1:475–86. doi: 10.1016/0013-4694(49)90221-7
44. Mirsky AF, Duncan CC. Pathophysiology of mental illness: a view from the fourth ventricle. Int J Psychophysiol. (2005) 58:162–78. doi: 10.1016/j.ijpsycho.2005.06.004
45. Young RC, Nambudiri DE, Jain H, de Asis JM, Alexopoulos GS. Brain computed tomography in geriatric manic disorder. Biol Psychiatry. (1999) 45:1063–5. doi: 10.1016/S0006-3223(98)00201-7
46. Dewan MJ, Haldipur CV, Lane EE, Ispahani A, Boucher MF, Major LF. Bipolar affective disorder. I. Comprehensive quantitative computed tomography. Acta Psychiatr Scand. (1988) 77:670–6. doi: 10.1111/j.1600-0447.1988.tb05186.x
47. Harvey I, Persaud R, Ron MA, Baker G, Murray RM. Volumetric MRI measurements in bipolars compared with schizophrenics and healthy controls. Psychol Med. (1994) 24:689–99. doi: 10.1017/S0033291700027847
48. Dutt A, McDonald C, Dempster E, Prata D, Shaikh M, Williams I, et al. The effect of COMT, BDNF, 5-HTT, NRG1 and DTNBP1 genes on hippocampal and lateral ventricular volume in psychosis. Psychol Med. (2009) 39:1783–97. doi: 10.1017/S0033291709990316
49. Terry J, Lopez-Larson M, Frazier JA. Magnetic resonance imaging studies in early onset bipolar disorder: an updated review. Child Adolesc Psychiatr Clin N Am. (2009) 18:421–39, ix-x. doi: 10.1016/j.chc.2008.12.004
50. Delvecchio G, Fossati P, Boyer P, Brambilla P, Falkai P, Gruber O, et al. Common and distinct neural correlates of emotional processing in bipolar disorder and major depressive disorder: a voxel-based meta-analysis of functional magnetic resonance imaging studies. Eur Neuropsychopharmacol. (2012) 22:100–13. doi: 10.1016/j.euroneuro.2011.07.003
51. Jiang X, Fu S, Yin Z, Kang J, Wang X, Zhou Y, et al. Common and distinct neural activities in frontoparietal network in first-episode bipolar disorder and major depressive disorder: preliminary findings from a follow-up resting state fMRI study. J Affect Disord. (2020) 260:653–9. doi: 10.1016/j.jad.2019.09.063
Keywords: Pediatric bipolar disorder (PBD), mania, euthymia, ventricle volume, cognition
Citation: Kuang L, Cui D, Jiao Q, Guo Y, Cao W, Gao W, Qiu J, Su L and Lu G (2020) Alterations of Cognition and Cerebral Ventricle Volume in Manic and Euthymic Pediatric Bipolar Disorder. Front. Psychiatry 11:593629. doi: 10.3389/fpsyt.2020.593629
Received: 12 August 2020; Accepted: 24 November 2020;
Published: 14 December 2020.
Edited by:
Polymnia Georgiou, University of Maryland, Baltimore, United StatesReviewed by:
Ezra Wegbreit, Cazenovia College, United StatesCopyright © 2020 Kuang, Cui, Jiao, Guo, Cao, Gao, Qiu, Su and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qing Jiao, YmluZ2JhbzE3QDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.