 José Gallego1
José Gallego1 Adolfo J. Cangas2*
Adolfo J. Cangas2* José M. Aguilar2
José M. Aguilar2 Rubén Trigueros2
Rubén Trigueros2 Noelia Navarro2
Noelia Navarro2 Blanca Galván2
Blanca Galván2 Konstantin Smyshnov3
Konstantin Smyshnov3 Melanie Gregg4
Melanie Gregg4- 1Department of Education, Health Research Centre, University of Almería, Almería, Spain
- 2Department of Psychology, Health Research Centre, University of Almería, Almería, Spain
- 3Faculty of Physical Culture, North-Caucasian Federal University, Stavropol, Russia
- 4Department of Kinesiology and Applied Health, University of Winnipeg, Winnipeg, MB, Canada
One of the main obstacles to integrating individuals with severe mental disorders into society today is the stigma directed at them. Although breakthroughs in treatment have been made in recent years, many professionals continue to admit that they do not possess enough training to combat this problem. Considering this situation, the present study analyzes the existing stigma among University Education students in three countries with different education systems and cultures, namely Spain, Russia, and Canada. A total of 1,542 students from these three countries participated in the study. ANOVA, MANOVA, and Multigroup Confirmatory Factor Analysis were applied in the data analysis. The results showed that the highest rates of stigma were in Spain and the lowest were in Canada, while Russia displayed intermediate values. This work addresses the relevance of these results, the influence that cultural difference may have on education policies, and the need to implement anti-stigma programs in countries like Spain, which has a relatively high level of social stigma and where these programs are practically not applied at all.
Introduction
Currently, one of the difficulties associated with recovery from severe mental disorders is stigma (1–3). Albeit, the problems directly related to the symptoms of these disorders, which can be severe, are intermittent in nature and increasingly treated more effectively, the problems derived from stigma are more stable over time and more resistant to change (4).
The degree to which these circumstances hinder patient recovery has ultimately led stigma to be considered a “second illness” (5). As a result, different international, national, and regional organizations have worked to promote various campaigns seeking to eradicate or diminish this problem (6). Not only is stigma common among the general population, but it is also present in other sectors, such as healthcare (7–11), so much so that several studies demonstrate the importance of including specific training as part of the education of doctors and healthcare professionals (12–14).
Similar findings regarding stigma toward mental health have also been obtained in the education sector. The value of applying specialized training among education professionals has not been investigated to the same extent, despite the prevalence of mental health problems in school environments (15). In fact, epidemiological studies conducted in different countries underline the high prevalence of such problems among children and adolescents, revealing that between 5 and 15% of minors fulfill enough criteria to warrant a psychiatric diagnosis. Furthermore, research reveals that these figures tend to increase each year (16).
The main anti-stigma programs applied to reduce mental health-related stigma in university or college students utilize social contact with people with mental problems, videos that describe the lives of people with mental illness, and text or lectures that describe the features of mental illness, yet the first two methods have displayed the best results (17).
Several recent works reflect the positive impact of carrying out interventions with education professionals (18–20). In fact, many workers in the education field recognize that they lack sufficient training in dealing with mental health (21). Such circumstances make it necessary to evaluate the conceptions that university Education students possess in this regard, as well as those of professionals in this sector.
Nonetheless, although stigma is a global phenomenon, it must be recognized that it does vary depending on the culture, region, or education system (22–26). Similarly, university policy can also vary a great deal from country to country, making it necessary to conduct an analysis.
Despite the importance of this subject, literature is scarce in terms of dealing with stigma among education professionals, and there are even fewer transcultural studies that compare this problem between different countries (27). Therefore, the objective of the present study is to analyze the stigma that may exist among Education students who are preparing to become teachers in three countries with different education systems, namely Spain, Russia, and Canada. This study seeks to identify the stigma present among future education professionals in order to conduct a comparative analysis. For this purpose, we include as Supplementary Material the validation of the questionnaire in Russia and Canada, since the validation in the Spanish context is already published (28). Once the psychometric properties of the QSAS questionnaire were verified in the three countries, the objective of the study was to analyze if there were differences in stigma between the Education students of the three countries.
Methods
Participants
A total of 1,539 university students pursuing education studies were selected using an incidental non-probability sampling. Ultimately, the sample consisted of 513 men and 1,026 women (Canadian group: 239 men and 290 women; Russian group: 84 men and 220 women; Spanish group: 190 men and 516 women). The Canadian and Russian participants were the same as in Phase 1. The ages ranged between 18 and 58 years old (Mage = 19.91; SD = 3.69). There were no significant differences in terms of gender and age between the groups (p > 0.05). Students were only excluded from the sample if they refused to give their informed consent to participate. The participants received no incentive for taking part in the study.
Instruments
The Questionnaire on Students' Attitudes toward Schizophrenia (QSAS) (29) is comprised of 19 items divided between two factors: social distance (n = 12) and stereotypes (n = 7). The instrument follows the logic of the stigma process in which undesirable characteristics are stereotypically linked to a condition and serve to justify negative social reactions, i.e., stereotypes from the basis of behavioral intentions. A sample stereotype item is “Mostly, someone who has had schizophrenia comes from a family with little money.” Social distance items reflect the willingness to engage in social relationships with individuals with schizophrenia, for example, “If the person sitting next to me in class developed schizophrenia, I would rather sit somewhere else.” The items were scored based on a Likert scale with values of 0 (I disagree), 1 (unsure), to 2 (I agree). Sum scores for each subscale indicate the absence of stereotypes and social distance. The original validation of the QSAS was done with a sample of adolescents ages 14–18 years old. The questionnaire displays suitable psychometric properties and a similar structure, both in the Spanish version and in the versions applied in Russia and Canada, as shown in the Supplementary Material.
Procedure
Approval to conduct this study was granted from the Ethics Committee of the three universities that participated in this study (Almeria, Stavropol, and Winnipeg). This is a non-interventional, observational, cross-sectional, and analytic study. The corresponding version of the QSAS (29) was administered in each country in different courses levels of the various Schools of Education (in Teaching Degree studies) of the respective countries, particularly those were the teaching staff at each university facilitated access to the classrooms to administer the questionnaires prior to the beginning of class. Paper questionnaires were completed individually at the beginning of university lectures. The students filled out the questionnaires anonymously and respecting all standard ethical procedures. A member of the research group was present to answer questions from the participants. The average time to complete the questionnaire was 10 min. Students did not receive any extra credit or points in the class for participating in the study.
Statistical Analysis
By first verifying the normality and homoscedasticity of the data, it was initially confirmed that parametric tests could be used. In order to determine the existence of statistically significant differences in the stigma scores of the three countries ANOVA was applied, supplemented by eta squared indicating the size of the effect. Subsequently, a multivariate analysis was conducted using MANOVA to test the influence of education level within each country and gender in relation to stigma scores. The influence of age on stigma was also verified according to country. In this case, the size of the effect was quantified using eta squared.
Results
The analysis of the average differences between Russia, Canada, and Spain, as can be seen in Table 1, revealed the existence of statistically significant differences in stigma toward people with severe mental disorders, in terms of both total score and the two factors: stereotypes and social distance. By means of the eta squared statistic, it was verified that the differences between the three countries were notable in relation to all the variables. It is observed that Spain is the country with the highest average in stigma, while Canada has the lowest. When analyzed by factors (stereotypes and social distance), the same results are found. Post-hoc tests (Tukey) were also conducted which confirmed the differences between the countries in relation to stigma, as can be seen in Table 2.
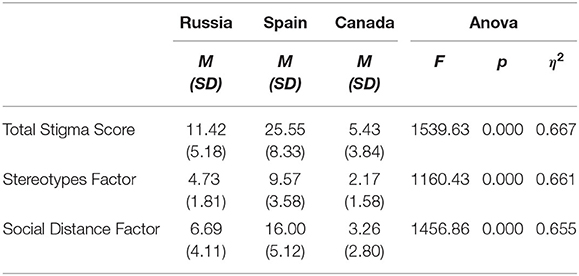
Table 1. ANOVA for the average differences of stigma among Canadian, Russian and Spanish students.
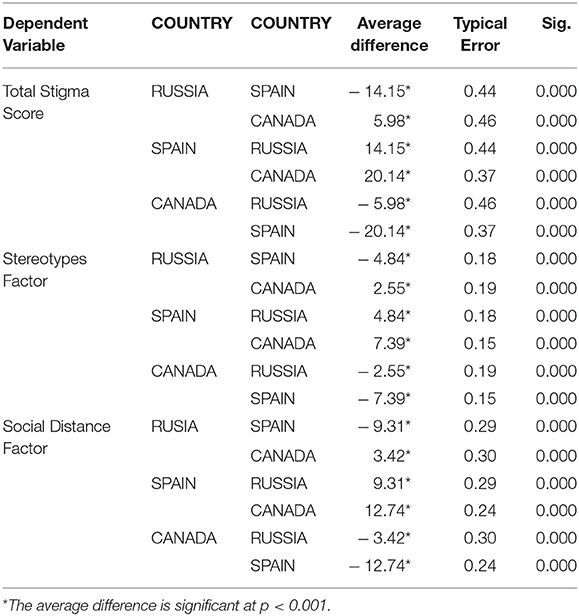
Table 2. Tukey HSD (post-hoc) for average differences of stigma between Canadian, Russian, and Spanish students.
Subsequently, the data were more closely scrutinized using a MANOVA to conduct inferential analysis between students from Russia, Canada, and Spain, but specifying the difference according to gender. Using Wilks's lambda, there was a significant difference stigma levels toward people with severe mental illness in relation to country [Wilks's Lambda = 0.345, F(4.000) = 537.25, p < 0.001; η2 = 0.412]. The size of the effect is large according to eta squared.
The differences were also significant by gender [Wilks's Lambda = 0.990, F(2.000) = 8.05, p < 0.001; η2 = 0.010]. However, the size of the effect was small, indicating that the difference was low. As can be observed in Table 3, women have lower scores in stigma than men, although in some cases the differences are minimal.
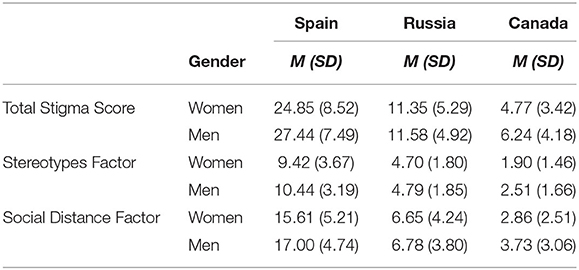
Table 3. Descriptive statistics for stigma between Spanish, Russian and Canadian students by country and gender.
Furthermore, there were no statistically significant differences in the country × gender interaction [Wilks's Lambda = 0.873, F(2.000) = 125.21, p = 0.088; η2 = 0.127] and the country × education level × gender interaction [Wilks's Lambda = 0.995, F(4.000) = 2.02, p = 0.011; η2 = 0.003].
An analysis was also conducted to determine whether the age of the participants had any influence on the differences in the stigma levels by countries. However, MANOVA once again revealed differences according to country [Wilks's Lambda = 0.383, F(4.000) = 312.46, p < 0.001; η2 = 0.381]. The size of the effect is large according to eta squared, but it did not reveal differences according to age [Wilks's Lambda = 0.997, F(2.000) = 1.65, p = 0.192; η2 = 0.003]. Furthermore, there were no statistically significant differences in the country × age interaction [Wilks's Lambda = 0.998, F(4.000) = 0.450, p = 0.772; η2 = 0.001].
Finally, the results obtained by the ANOVA and MANOVA are supported by the Multi-Group Confirmatory Factor Analysis. In this sense, there are significant differences in the comparison between the populations of the three countries (χ2 = 80.54; df = 34; ΔCFI = −0.005; ΔRMSEA = 0.004; p < 0.001). Similarly, significant differences can be seen when gender and country of origin are taken into account (χ2 = 65.29; df = 34; ΔCFI = −0.004; ΔRMSEA = −0.002; p < 0.01), as well as when gender, country of origin, and educational level are taken into account (χ2 = 72.83; df = 34; ΔCFI = −0.003; ΔRMSEA = 0.001; p < 0.01).
Discussion
Although stigma is known to be a universal phenomenon (30), its presence is not the same when examined in the context of transcultural criteria. Culture, tradition, and access to education are, among others, factors that can influence and shape perceptions of mental health (25, 31).
The first studies carried out based on this approach revealed that countries that were more developed displayed less fear, shame, and stigma toward mental health than developing countries (25, 32, 33). The present study compared stigma among Education students in three countries: Russia, Spain, and Canada. The validation of the QSAS was confirmed in Canadian and Russian contexts. Furthermore, the QSAS is a reliable tool to use with university students. The QSAS has suitable psychometric properties, with a similar factorial structure, for application in all three countries.
Upon comparing the results, it was found that Spain was the country where students displayed the most stigma. When compared with the scores obtained for the other two countries, the differences were statistically significant, both when the questionnaire was considered in its entirety and when examining the factors; stigma and social distance. In contrast, Canada displayed the least stigma, as its students demonstrated the least stigmatizing attitudes. In the original study using the QSAS (27) noted that a ceiling effect was evident and that the measure may not be sensitive to pick up on slight shifts in stigma toward mental health, the results from the Canadian sample reflect a similar ceiling effect.
The existence of statistically significant differences between the three countries coincides with other studies that maintain that certain societies are more tolerant than others (25, 34–36). The general attitude of the general population toward mental health problems and recovery influences interest in specific topics, which contributes to changes in education policies (37). This could be the case of Russia, where past studies found high levels of discrimination toward individuals with mental health problems; these levels have decreased in recent years due to political changes and the opening of this country (38).
As for Canada, it is the most tolerant country toward mental health problems and has the most active anti-stigma policies of the three education systems. In the case of Spain, not many works were found which closely analyze this topic, and most of these focus on students in secondary education (39–41). In this regard, more effort must be made in this country, unlike the strong initiatives carried out to address other issues, such as school bullying, substance abuse, and sexuality, among this age group (42). No specific programs for students were found at Spanish universities (43), and the research is aimed more at students enrolled in Schools of Health Science (Medicine, Psychology, and Nursing), but not in the Schools of Education (35, 44–46).
However, when comparing the results, it must be taken into account that they may be influenced by other uncontrolled variables in the study, such as social desirability. This aspect is closely related to stigma and also has a strong cultural component (2, 47). Thus, more studies are necessary to further investigate this possibility.
Therefore, university policies, related to general stigma among a population, can play a fundamental role—if the education of future professionals prioritized stigma as an essential subject during training (as occurs in Canada), such teachings would later influence the attitudes of students (15).
As for other aspects, the data collected in the study also reveal that women display lower levels of stigma toward people with mental disorders, albeit these differences are minor. These results may owe to women's greater propensity to show empathy when compared to men, as indicated in several studies (48).
In this study, age was not found to have a notable influence, probably due to the fact that the sample was a very homogeneous group. In other studies which compared stigma among students and professionals, it was indeed found to be a variable that could affect results (49), and various studies shows that older people tend to reveal more stigmatizing attitudes than young people (50, 51).
Among the limitations of this study, we highlight the relatively small sample used for the three countries and that no follow-up actions were conducted to verify whether the results remain consistent over time. Similarly, no other evaluation instruments were applied to validate the results from the stigma questionnaire utilized. Finally, other variables were not taken into consideration which may have also influenced the results, for example, prior contact with individuals with a mental disorder or if participants themselves or their relatives had received any psychiatric diagnosis. Similarly, the instrument utilized only analyzed stigma toward people with schizophrenia, not including the assessment of stigma toward other mental disorders.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the University of Almeria. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
JG and AC collaborated with the design of the study, and wrote the manuscript. JA and RT did the data analysis. NN entered the data. BG, KS, and MG applied the questionnaire in the different countries. All authors contributed to the article and approved the submitted version.
Funding
This work was funded by the Spanish Ministry of Science, Innovation and Universities: (PSI2017-84961-R AEI/FEDER, UE).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2020.587321/full#supplementary-material
References
1. Corrigan PW. On the Stigma of Mental Illness: Practical Strategies for Research and Social Change. Washington, DC: American Psychological Association (2005).
2. Mannarini S, Rossi A. Assessing mental illness stigma: a complex issue. Front Psychol. (2019) 9:2722 doi: 10.3389/fpsyg.2018.02722
3. Seeman N, Tang S, Brown AD, Ing A. 2016 World survey of mental illness Stigma. J Affect Disord. (2016) 190:115–21. doi: 10.1016/j.jad.2015.10.011
4. Corrigan PW, Penn DL. Lessons from social psychology on discrediting psychiatric stigma. Stigma Health. (2015) 1:2–17. doi: 10.1037/2376-6972.1.S.2
5. Schulze B, Angermeyer MC. Subjective experiences of stigma. A focus group study of schizophrenic patients, their relatives and mental health professionals. Soc Sci Med. (2003) 56:299–312. doi: 10.1016/S0277-9536(02)00028-X
6. Hansson L. Mental health and stigma-aspects of anti-stigma interventions. In: Bährer-Kohler S, Carod-Artal F, editors. Global Mental Health. Cam: Springer (2017). p.71–8.
7. Giralt R, Prat-Vigué G, Tort-Nasarre G. Attitudes and stigma toward mental health in nursing students: a systematic review. Perspect Psychiatr. (2019) C56:243–55. doi: 10.1111/ppc.12419
8. Horsfall J, Cleary M, Hunt GE. Stigma in mental health: clients and professionals. Issues Ment Health Nurs. (2010) 31:450–5. doi: 10.3109/01612840903537167
9. Mårtensson G, Jacobsson JW, Engström M. Mental health nursing staffs attitudes towards mental illness: an analysis of related factors. J Psychiatr Ment Health Nurs. (2014) 21:782–8. doi: 10.1111/jpm.12145
10. Navarro N, Triguero R. Estigma en los profesionales de la Salud Mental: una revisión sistemática. Psychol Soc Educ. (2019) 11:253–66. doi: 10.25115/psye.v11i2.2268
11. Olmo-Romero F, González-Blanco M, Sarró S, Grácio J, Martín-Carrasco M, Martinez-Cabezón AC, et al. Mental health professionals' attitudes towards mental illness: professional and cultural factors in the INTER NOS study. Eur Arch Psy Clin Neurosci. (2019) 269:325–39. doi: 10.1007/s00406-018-0867-5
12. Economou M, Peppou LE, Souliotis K, Lazaratou H, Kontoangelos K, Nikolaidi S, et al. Attitudes to depression and psychiatric medication amid the enduring financial crisis in Attica: comparison between 2009 and 2014. Int J Soc Psychiatr. (2019) 65:479–87. doi: 10.1177/0020764019858653
13. Hansson L, Jormfeldt H, Svedberg P, Svensson B. Mental health professionals attitudes towards people with mental illness: do they differ from attitudes held by people with mental illness? Int J Soc Psychiatr. (2013) 59:48–54. doi: 10.1177/0020764011423176
14. Wahl O, Aroesty-Cohen E. Attitudes of mental health professionals about mental illness: a review of the recent literature. J Community Psychol. (2010) 38:49–62. doi: 10.1002/jcop.20351
15. Wada M, Suto MJ, Lee M, Sanders D, Sun C, Le TN, et al. University students' perspectives on mental illness stigma. Ment Health Prev. (2019) 14:200159. doi: 10.1016/j.mph.2019.200159
16. Sadler K, Vizard T, Ford T, Marchesell F, Pearce N, Mandalia D, Goodman R. Mental Health of Children and Young People in England, 2017: Trends and Characteristics. (2018). Available online at: https://dera.ioe.ac.uk/32622/1/MHCYP%202017%20Summary.pdf [accessed July, 15, 2020].
17. Yamaguchi S, Wu SI, Biswas M, Yate M, Aoki Y, Barley EA, Thornicroft G. Effects of short-term interventions to reduce mental health-related stigma in university or college students: a systematic review. J Nerv Ment Dis. (2013) 201:490–503. doi: 10.1097/NMD.0b013e31829480df
18. Carr W, Wei Y, Kutcher S, Heffernan A. Preparing for the classroom: mental health knowledge improvement, stigma reduction and enhanced help-seeking efficacy in Canadian preservice teachers. Can J Sch Psychol. (2018) 33:314–26. doi: 10.1177/0829573516688596
19. Imran N, Rahman A, Chaudhry N, Asif A. World Health Organization School Mental Health Manual-based training for school teachers in Urban Lahore, Pakistan: study protocol for a randomized controlled trial. Trials. (2018) 19:290. doi: 10.1186/s13063-018-2679-3
20. Kutcher S, Wei Y, Gilberds H, Ubuguyu O, Njau T, Brown A, et al. A school mental health literacy curriculum resource training approach: effects on Tanzanian teachers' mental health knowledge, stigma and help-seeking efficacy. Int J Ment Health Syst. (2016) 10:50. doi: 10.1186/s13033-016-0082-6
21. Holtz KF. The Mental Health Literacy of High School Teachers. New York, NY: Columbia University (2017).
22. Chaudhry T, Chen SH. Mental illness stigma in South Asian Americans: a cross-cultural investigation. Asian Am J Psychol. (2019) 10:154–65. doi: 10.1037/aap0000141
23. Krol LM. The Relationship of Culture and the Stigma of Mental Illness. Master's Thesis. Hartford, Connecticut: University of Hartford (2010).
24. Zolezzi M, Alamri M, Shaar S, Rainkie D. Stigma associated with mental illness and its treatment in the Arab culture: a systematic review. Int J Soc Psychiatr. (2018) 64:597–609. doi: 10.1177/0020764018789200
25. Cheon BK, Chiao JY. Cultural variation in implicit mental illness stigma. J Cross Cult Psychol. (2012) 43:1058–62. doi: 10.1177/0022022112455457
26. Lauber C, Rossler W. Stigma towards people with mental illness in developing countries in Asia. Int Rev Psychiatr. (2007) 19:157–78. doi: 10.1080/09540260701278903
27. Kurumatani T, Ukawa K, Kawaguchi Y, Miyata S, Suzuki M, Ide H, et al. Teachers' knowledge, beliefs and attitudes concerning schizophrenia. Soc Psych Psych Epid. (2004) 39:402–9. doi: 10.1007/s00127-004-0758-0
28. Navarro N, Cangas A, Aguilar-Parra JM, Gallego J, Moreno-San Pedro E, Carrasco-Rodríguez Y, et al. Propiedades psicométricas de la versión en castellano del cuestionario de las actitudes de los estudiantes hacia la esquizofrenia. Psychol Soc Educ. (2017) 9:325–34. doi: 10.25115/psye.v9i2.865
29. Schulze B, Richter-Werling M, Matschinger H, Angermeyer MC. Crazy? So what! Effects of a school project on students' attitudes toward people with schizophrenia. Acta Psychiat Scand. (2003) 107:142–50. doi: 10.1034/j.1600-0447.2003.02444.x
30. Rüsch N, Angermeyer MC, Corrigan P. Mental illness stigma: concepts, consequences and initiatives to reduce stigma. Eur Psychiat. (2005) 20:529–39. doi: 10.1016/j.eurpsy.2005.04.004
31. Koschorke M, Evans-Lacko S, Sartorius N, Thornicroft G. Stigma in different cultures. In: Gaebel W, Rössler W, Sartorius N, editors. The Stigma of Mental Illness - End of the Story? Cham: Springer (2017). p.67–82. doi: 10.1007/978-3-319-27839-1_4
32. Linz SJ, Sturm BA. The phenomenon of social isolation in the severely mentally ill. Perspect Psychiatr Care. (2013) 49:243–54. doi: 10.1111/ppc.12010
33. Rüsch N, Corrigan PW, Heekeren K, Theodoridou A, Dvorsky D, Metzler S, Rössler W. Well-being among persons at risk of psychosis: the role of self-labeling, shame, and stigma stress. Psychiatr Serv (2014) 65: 483–9. doi: 10.1176/appi.ps.201300169
34. Abdullah T, Brown TL. Mental illness stigma and ethnocultural beliefs, values, and norms: an integrative review. Clin Psychol Rev. (2011) 31:934–48. doi: 10.1016/j.cpr.2011.05.003
35. Corrigan PW, Watson AC. Understanding the impact of stigma on people with mental illness. World Psychiatry. (2002) 1:16–20.
36. Pescosolido BA, Martin JK, Long S, Medina TR, Phelan JC, Link BG. A disease like anyother? A decade of change in publicreactions to schizophrenia, depression, and alcohol dependence. Am J Psychiatr. (2010) 167:1321–30. doi: 10.1176/appi.ajp.2010.09121743
37. López M, Laviana M, Fernández L, López-Pardo A, Rodríguez AM. Aparicio A. La lucha contra el estigma y la discriminación en salud mental: Una estrategia compleja basada en la información disponible. Rev Asoci Esp Neuropsiquiatr. (2008) 28:48–83. doi: 10.4321/S0211-57352008000100004
38. Wasserman E, Lapshina N. Educating Russian University students about psychiatric stigma. Bridg East West Psychiatr. (2006) 4:1–4.
39. De la Higuera J, Jiménez A, Zurita M, Candelas A, Fuica P, Martínez E, et al. Strategies for reducing stigma to mental illness in a school setting: preliminary study and pilot of the “lo hablamos” program. Psychol Soc Educ. 12:138–58. doi: 10.25115/psye.v10i1.3458
40. Andrés-Rodríguez L, Pérez-Aranda A, Feliu-Soler A, Rubio-Valera M, Aznar-Lou I, Serrano-Blanco A, et al. Effectiveness of the “What's Up!” intervention to reduce stigma and psychometric properties of the Youth Program Questionnaire (YPQ): results from a cluster non-randomized controlled trial conducted in Catalan High Schools. Front Psychol. (2017) 8:1608. doi: 10.3389/fpsyg.2017.01608
41. Casañas R, Arfuch V, Castellví P, Gil J-J, Torres M, Pujol A, et al. “EspaiJove.net”- a school-based intervention programme to promote mental health and eradicate stigma in the adolescent population: study protocol for a cluster randomised controlled trial. BMC Public Health. (2018) 18:939. doi: 10.1186/s12889-018-5855-1
42. Barbero FL. Alumnado con enfermedad mental. La asignatura pendiente. Educar. (2013) 49:245–66. doi: 10.5565/rev/educar.419
43. González-Badía J, Sala Mozos E, Hermoso EA. Mejora del Tratamiento de las Personas con Enfermedad Mental en las Universidades Públicas. Madrid: Ministerio de Sanidad, Servisios Sociales e Igualdad (2013).
44. Medina-Mesa Y, Cruces-Montes SJ, Merchán-Clavellino A, Romero-Moreno AF, Guil-Bozal R. La influencia de la formación en las actitudes hacia las personas con trastorno mental en una muestra de estudiantes universitarios. Int J Dev Educ Psychol. (2019) 5:309–20. doi: 10.17060/ijodaep.2019.n1.v5.1602
45. Granados G, Lopez MD, Corral A, Márquez VV. Attitudes and beliefs of nursing students toward mental disorder: the significance of direct experience with patients. Perspect Psychiatr Care. (2017) 53:135–43. doi: 10.1111/ppc.12147
46. Mullor D, Sayans P, Cangas AJ, Navarro N. Effect of a Serious Game (Stigma-Stop) on reducing stigma among Psychology students: a controlled study. Cyberpsychol Behav Soc Netw. (2019) 22:205–11. doi: 10.1089/cyber.2018.0172
47. Stier A, Hinshaw SP. Explicit and implicit stigma against individuals with mental illness. Aust Psychol. (2007) 42:106–17. doi: 10.1111/ap.2007.42.2.106
48. Angermeyer MC, Beck M, Matschinger H. Determinants of the public's preference for social distance from people with schizophrenia. Can J Psychiat. (2003) 48:663–8. doi: 10.1177/070674370304801004
49. Oliveira AM, Machado D, Fonseca JB, Palha F, Silva Moreira P, Sousa N, et al. Stigmatizing attitudes toward patients with psychiatric disorders among medical students and professionals. Front Psychiatry. (2020) 11:326. doi: 10.3389/fpsyt.2020.00326
50. Hansson L, Stjernsward S, Svensson B. Changes in attitudes, intended behaviour, and mental health literacy in the Swedish population 2009-2014: an evaluation of a national antistigma programme. Acta Psychiatrica Scand. (2016) 134(Suppl 446):71–9. doi: 10.1111/acps.12609
Keywords: rehabilitation, people with mental disorder, awareness, university students, Spain, Russia, Canada
Citation: Gallego J, Cangas AJ, Aguilar JM, Trigueros R, Navarro N, Galván B, Smyshnov K and Gregg M (2020) Education Students' Stigma Toward Mental Health Problems: A Cross-Cultural Comparison. Front. Psychiatry 11:587321. doi: 10.3389/fpsyt.2020.587321
Received: 25 July 2020; Accepted: 30 September 2020;
Published: 05 November 2020.
Edited by:
Leandro Fernandes Malloy-Diniz, Federal University of Minas Gerais, BrazilReviewed by:
Rui Mateus Joaquim, Federal University of Minas Gerais, BrazilAndré Luiz De Carvalho Braule Pinto, University of São Paulo, Brazil
Pedro Morgado, University of Minho, Portugal
Copyright © 2020 Gallego, Cangas, Aguilar, Trigueros, Navarro, Galván, Smyshnov and Gregg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adolfo J. Cangas, YWpjYW5nYXNAdWFsLmVz